
Abstract
Introduction
The prevalence of neurodegenerative diseases has significantly increased, necessitating a deeper understanding of their symptoms, diagnostic processes, and prevention strategies. Frontotemporal dementia (FTD) and Alzheimer’s disease (AD) are two prominent neurodegenerative conditions that present diagnostic challenges due to overlapping symptoms. To address these challenges, experts utilize a range of imaging techniques, including magnetic resonance imaging (MRI), diffusion tensor imaging (DTI), functional MRI (fMRI), positron emission tomography (PET), and single-photon emission computed tomography (SPECT). These techniques facilitate a detailed examination of the manifestations of these diseases. Recent research has demonstrated the potential of artificial intelligence (AI) in automating the diagnostic process, generating significant interest in this field.
Materials and Methods
This narrative review aims to compile and analyze articles related to the AI-assisted diagnosis of FTD and AD. We reviewed 31 articles published between 2012 and 2024, with 23 focusing on machine learning techniques and 8 on deep learning techniques. The studies utilized features extracted from both single imaging modalities and multi-modal approaches, and evaluated the performance of various classification models.
Results
Among the machine learning studies, Support Vector Machines (SVM) exhibited the most favorable performance in classifying FTD and AD. In deep learning studies, the ResNet convolutional neural network outperformed other networks.
Conclusion
This review highlights the utility of different imaging modalities as diagnostic aids in distinguishing between FTD and AD. However, it emphasizes the importance of incorporating clinical examinations and patient symptom evaluations to ensure comprehensive and accurate diagnoses.
Keywords
Introduction
Neurodegenerative diseases (ND) represent a substantial global health challenge, particularly among the elderly population. These conditions result in neuronal dysfunction and loss, manifesting in a diverse array of clinical symptoms.1,2
Common NDs include frontotemporal dementia (FTD), Alzheimer’s disease (AD), dementia with Lewy bodies (DLB), Parkinson’s disease (PD), and Huntington’s disease (HD). 1
FTD specifically affects the anterior temporal and frontal lobes, 3 resulting in behavioral and personality changes (behavioral variant, bvFTD) or language impairments (primary progressive aphasia, PPA). 4
FTD is highly heritable, and specific patterns of cognitive decline have been observed in genetic carriers. 5 Whilst administrative function deficits seem usual across the different genetic groups, specific patterns of cognitive decline have been known at a presymptomatic stage in MAPT, GRN and C9orf72 carriers. 6 The progression of FTD involves stages of atrophy, starting in the anterior frontal cortex and hippocampus, followed by involvement of the orbitofrontal gyrus, basal ganglia, posterior temporal lobe, and ultimately severe atrophy in frontotemporal, hippocampal, thalamic, and basal ganglia regions. 7
AD is the most prevalent form of neurodegenerative dementia, affecting millions of individuals worldwide and exerting a profound impact on caregivers and households. 8 In the United States alone, there are currently 5.4 million diagnosed cases of AD, with the majority of those affected being over the age of 65. 9 While the majority of AD cases occur sporadically, mutations in three genes (amyloid precursor protein, presenilin 1, and presenilin 2) can cause a rare familial form of AD (fAD) that accounts for less than 0.5% of cases. 10 The prodromal stage of AD, known as Mild Cognitive Impairment (MCI), is widely recognized as a diagnostic label. 11 Many individuals with MCI may progress to AD within a few years. 12
At present, there are no definitive treatments available for FTD. It is important to note that acetylcholinesterase inhibitors, commonly prescribed for individuals with AD, may actually worsen symptoms in individuals with FTD. 13 Therefore, accurate diagnosis of FTD and AD is crucial to avoid negative treatment outcomes. Additionally, reducing misdiagnosis is essential for clinical trials that aim to differentiate between these two diseases. 14 However, accurate diagnosis presents a significant challenge due to the overlapping clinical symptoms and impaired cognitive domains observed in both FTD and AD. 15 Despite their distinct clinical and biological presentations, both disorders ultimately lead to functional decline and loss of independence.16–21
Neuroimaging methods provide essential tools for the diagnosis and management of dementia, contributing significantly to the understanding of the underlying neurobiology of various neurodegenerative disorders. These advanced imaging techniques enable clinicians and researchers to visualize and monitor structural and functional changes in the brain, facilitating the identification of disease-specific biomarkers and pathophysiological mechanisms. Moreover, neuroimaging plays a critical role in assessing the efficacy of therapeutic interventions, allowing for the objective evaluation of treatment outcomes and the optimization of therapeutic strategies. Through these applications, neuroimaging enhances the precision of diagnostic processes, enriches our comprehension of disease progression, and supports the development of more effective clinical interventions. 22
Machine learning (ML) is a systematic and interdisciplinary field that focuses on the development of algorithms and statistical models enabling computers to learn from and make predictions or decisions based on data.23,24 Machine learning (ML) involves the creation of algorithms designed to analyze and interpret datasets effectively, emphasizing the learning aspect of artificial intelligence (AI). This field focuses on developing models that can autonomously learn and improve from experience without explicit programming. Through iterative processes, these models refine their performance by adapting to new data, thereby enhancing their predictive accuracy and decision-making capabilities. 25
Deep learning (DL), an advanced technique within the field of machine learning (ML), has demonstrated exceptional performance compared to traditional ML methods, particularly in recognizing intricate patterns in high-dimensional data. This is especially evident in the domain of computer vision, where deep learning models have achieved remarkable success in tasks such as image classification, object detection, and facial recognition. By utilizing neural networks with multiple layers, DL methods can automatically extract and learn hierarchical features from raw data, enabling them to handle complex data representations and achieve superior accuracy in various applications. 26
The purpose of this review is to compile and analyze articles that utilize ML and DL methods to classify AD and FTD groups of diseases.
Materials and methods
We conducted a comprehensive look within the PubMed, Scopus, Web of Science, ScienceDirect, Embase, and Google Scholar databases, utilizing particular Mesh terms and keywords related to our subject of intrigued.
The search key words are; ((((((frontotemporal dementia) OR (FTD)) OR (frontotemporal degeneration)) OR (frontotemporal labor degeneration)) AND (((Alzheimer) OR (AD)) OR (Alzheimer’s disease))) AND (((((convolutional neural network) OR (CNN)) OR (classification)) OR ((deep learning) OR (DL))) OR ((machine learning) OR (ML)))) AND ((((((computed tomography) OR (CT)) OR ((positron emission tomography) OR (PET))) OR ((single photon emission computed tomography) OR (SPECT))) OR ((magnetic resonance imaging) OR (MRI))) OR (neuroimaging)).
The search was constrained to as it were the English dialect and publication dates from 2012 to 2024.
After the removal of duplicate and unrelated articles, a total of 39 articles were reviewed. Thirteen articles were subsequently excluded from the study for several reasons. Five articles were eliminated due to the classification of patients using methods other than imaging, such as genetic information or cerebrospinal fluid levels. Three articles were excluded because the classification of patients was performed by a radiologist. Additionally, three articles were removed due to the absence of Alzheimer’s disease patients in the study; these articles appeared in the initial search solely because they mentioned Alzheimer’s disease in their text. Finally, two articles were excluded because they utilized classification methods other than machine learning techniques. Consequently, 26 articles were included for further analysis. Final studies were screened, and systematic and non-systematic review articles were excluded. A flow chart below (Figure 1) shows the Search strategy and article selection process. PRISMA flow chart of study selections.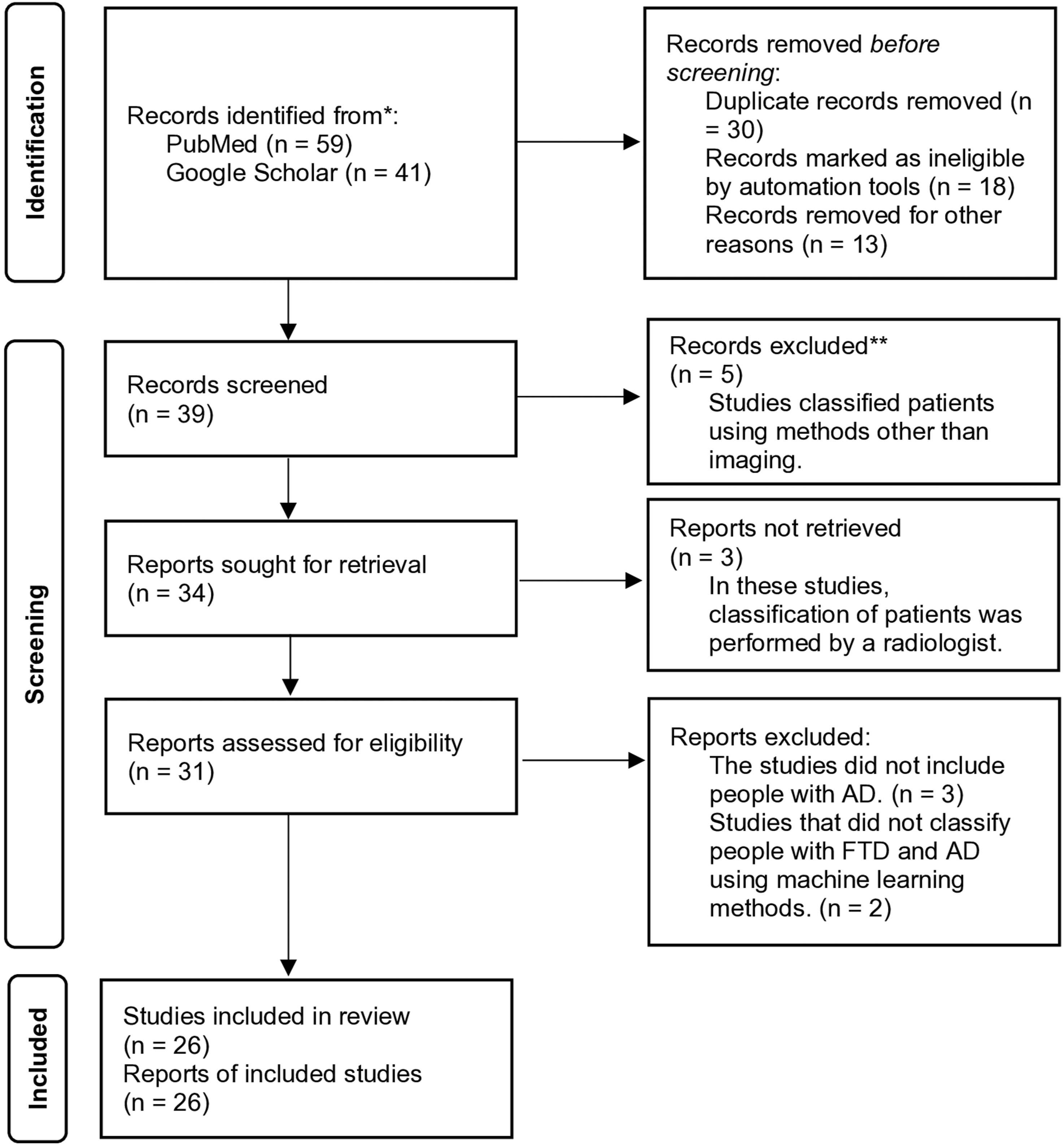
Results
Neuroimaging is widely recognized as a highly effective approach for the diagnosis of neurodegenerative disorders. Various MRI imaging techniques, alongside other modalities such as PET and SPECT, are employed in the differential diagnosis of Alzheimer’s disease (AD) and frontotemporal dementia (FTD). Given the overlapping clinical manifestations of these two neurodegenerative disorders, reliance solely on conventional MRI techniques proves insufficient in the diagnostic process. While advanced imaging modalities like functional MRI (fMRI), diffusion-weighted imaging (DWI), and diffusion tensor imaging (DTI) have enhanced our understanding of these conditions, the incorporation of artificial intelligence (AI) in imaging diagnosis offers a promising frontier.
AI-assisted diagnostic approaches, particularly those leveraging machine learning (ML) and deep learning (DL), present significant potential in integrating complex neuroimaging data for more accurate differential diagnoses of AD and FTD. These methodologies can process vast amounts of imaging data, identifying subtle patterns and anomalies that might be overlooked by traditional techniques.
The subsequent sections provide a comprehensive overview of various diagnostic imaging modalities. Emphasis is placed on how the integration of these modalities with advanced machine learning and deep learning techniques has yielded promising results in the differential diagnosis of AD and FTD. Through the synthesis of neuroimaging data and AI-driven analytical tools, these approaches aim to enhance diagnostic accuracy, thereby improving clinical outcomes for patients suffering from these debilitating conditions.
Integrating machine learning and deep learning techniques with neuroimaging data
In numerous specialty areas, the accurate and prompt evaluation of clinical images is essential for both diagnosis and treatment. Consequently, quality assessment parameters such as accuracy, sensitivity, and specificity of clinical images are critical in healthcare operations. Therefore, the development of computer-based vision algorithms is imperative to aid in the analysis of biomedical images. 27
Machine learning is a computational strategy that uncovers optimal problem solutions by defining methods and parameters that are typically determined, inferred, and devised by an experimenter. 28 The use of ML has become widespread across various fields offering reliable guidance for decision making and reducing manual function. 29 Unsupervised and supervised learning are machine learning techniques and here we talk more about these two categories.
Unsupervised machine learning is like setting a data detective loose on your dataset without telling them what to look for. Unlike supervised methods, which have specific labels or outcomes to guide their work, unsupervised methods sift through raw data independently, finding patterns, structures, or groups on their own. For example, clustering—one unsupervised method—can group similar items together, such as identifying clusters of customers with similar purchasing habits or categorizing text documents based on thematic content.
On the other hand, supervised learning is employed when the objective is to predict or classify a specific outcome of interest. Supervised learning techniques have been applied to large datasets, incorporating demographic and clinical predictors, to develop risk scores for predicting the onset of diseases.30–34
As automated systems technology continues to advance across various medical fields, machine learning systems play a crucial role in assisting physicians with the automated diagnosis of diseases. 35
Deep learning, a branch of machine learning, involves the automatic extraction of features directly from data. In deep learning, a deep architecture is constructed with multiple linear units to capture high-level abstractions that exist within the data. 36 A commonly used type of neural network in medical imaging for image analysis and training is the convolutional neural network (CNN). 37 CNNs demonstrate exceptional proficiency in rapidly identifying visual patterns directly from raw image pixels. In some instances, minimal preprocessing is performed before inputting the images into the CNN. These deep networks utilize multi-layered neurons to analyze small portions of the input image known as receptive fields, and they utilize shared weights within each convolutional layer. CNNs incorporate three architectural concepts to achieve some level of scale, change, and distortion invariance. 38
Neuroimaging modalities
This section provides a summary of several neuroimaging modalities utilized in the differential diagnosis between AD and FTD, The modalities discussed include structural magnetic resonance imaging (sMRI), functional magnetic resonance imaging (fMRI), diffusion-weighted imaging (DWI), diffusion tensor imaging (DTI), positron emission tomography (PET), and single-photon emission computed tomography (SPECT). Each of these techniques offers unique insights into the pathophysiological differences between AD and FTD, enhancing the accuracy and reliability of differential diagnosis in clinical settings.
Structural magnetic resonance imaging (sMRI)
Magnetic resonance imaging (MRI) has emerged as an invaluable diagnostic tool, facilitating the non-invasive visualization of internal organs and yielding significant clinical benefits. This advanced imaging technique utilizes a powerful superconducting magnet in conjunction with three magnetic gradients to generate detailed images of body structures. 39 By adjusting parameters related to the transmission and reception of radiofrequency (RF) pulses, MRI can acquire various tissue contrasts, resulting in the formation of T1-weighted and T2-weighted images. T1-weighted images are typically employed as anatomical references due to their detailed depiction of anatomical structures, while T2-weighted images provide excellent tissue contrast, enhancing the differentiation of various tissue types. In clinical practice, both T1 and T2-weighted images are often obtained to maximize the diagnostic information available through their differing contrasts. This dual approach allows for a more comprehensive assessment of tissue characteristics and pathologies. 40 In AD, significant atrophy is often observed in the medial temporal lobes, including the hippocampus, while FTD typically presents with atrophy in the frontal and anterior temporal lobes. These patterns can aid in distinguishing between the two conditions, although overlap in atrophy patterns can limit the specificity of sMRI alone.41,42
Diffusion weighted imaging (DWI)
Different tissues in the human body exhibit distinct diffusion properties due to variations in the Brownian motion of water molecules between cells and within extracellular compartments. Diffusion-weighted imaging (DWI) leverages these differences to generate diffusion-weighted images. This imaging method is instrumental in investigating the molecular function of various tissues, offering both quantitative and qualitative information about their diffusion characteristics. By analyzing the diffusion properties of tissues, DWI can provide valuable insights into their microstructural organization and pathology, making it a critical tool in the diagnosis and evaluation of numerous medical conditions. 43
Diffusion tensor imaging (DTI)
Diffusion tensor imaging (DTI) is an advanced neuroimaging technique that utilizes diffusion weighting along with three-dimensional display algorithms and tensor formalism to produce detailed visual representations of tissue microstructure. This method generates diffusion tensor images, which provide crucial information about diffusion anisotropy, reflecting the directional dependence of water diffusion in tissues. DTI offers various quantitative measures, including mean diffusivity (MD), fractional anisotropy (FA), radial diffusivity (RD), and axial diffusivity (AD). These metrics are instrumental in assessing and characterizing the integrity and organization of white matter tracts, making DTI a valuable tool in the study of neurological disorders and brain connectivity.44,45 DWI highlights areas of restricted water diffusion, which can indicate acute pathology, while DTI provides detailed information on white matter microstructure. These techniques have revealed distinct patterns of white matter degeneration in AD and FTD, offering additional diagnostic value. For instance, AD is often associated with changes in the posterior cingulum bundle, whereas FTD typically affects the uncinate fasciculus.46,47
Functional magnetic resonance imaging (fMRI)
Functional magnetic resonance imaging (fMRI) is a specialized imaging modality designed to display sectional, time-varying alterations in brain metabolism.48,49 These changes can occur due to task-induced cognitive condition alterations or as a consequence of spontaneous activity in the resting brain. Since its inception in 1990, fMRI has been utilized across various fields, including cognitive neuroscience, clinical psychology, and presurgical planning. The popularity of fMRI stems from its widespread accessibility, non-invasive nature (requiring no injections), relatively low cost, and high spatial resolution. These attributes make fMRI an invaluable tool for studying brain function and aiding in clinical and research applications. 50 In AD, disruptions are often seen in the default mode network, whereas FTD may show alterations in the salience network. Despite its potential, fMRI’s variability and complexity necessitate advanced analytical techniques for reliable differentiation.51,52
Resting state fMRI (Rs-fMRI)
The field of brain functional studies has a long and diverse history of experimental projects primarily focused on investigating task-related activities. These endeavors have significantly advanced our understanding of the intricate workings of the human brain. Similarly, resting-state functional MRI (Rs-fMRI) has emerged as a powerful tool for investigating brain functions and exploring the complexities of the human brain. Unlike task-related fMRI, which captures brain activity induced by specific tasks, resting-state BOLD signals have the potential to capture “automatic” neural processes occurring during rest. The contrasting results observed between Rs-fMRI and task-related fMRI studies underscore the existence of distinct underlying neurobiological mechanisms. 53 Due to its non-invasive nature and high sensitivity, Rs-fMRI has garnered significant attention for its utility in investigating functional brain networks, offering valuable insights into the brain’s intrinsic connectivity and organization. 54
Positron emission tomography (PET)
Positron emission tomography (PET), a non-invasive imaging technique, is extensively employed to evaluate the pathophysiology of various brain disorders, including neurodegenerative diseases. As a functional or molecular imaging tool, PET is highly sensitive and maps the positron emission of administered radiopharmaceuticals, enabling the study of the biological functions of tissues. One such radiopharmaceutical, 18F-fluorodeoxyglucose (FDG), was developed to study glucose metabolism and is currently used in neurology as a clinically approved diagnostic tool. 55 F-18 FDG PET imaging is particularly valuable in detecting frontotemporal hypometabolism, which can be identified in the prodromal stages of frontotemporal dementia (FTD), marked by early behavioral and cognitive symptoms. Consequently, PET imaging is essential for diagnosing potential FTD during the dementia stage, adhering to established diagnostic criteria. 56 AD is characterized by widespread amyloid plaques and tau tangles, detectable with specific PET tracers. In contrast, FTD often lacks significant amyloid deposition but may show tau or TDP-43 pathology depending on the subtype. PET imaging thus provides critical biomarker evidence that can support the differential diagnosis. 57
Single-photon emission computed tomography (SPECT)
Since the advent of radioactive tracers for medical applications, there has been an increasing interest in precisely visualizing the distribution and quantification of these tracers’ uptake within the body. During the 1960s and 1970s, advancements in single-photon emission computed tomography (SPECT) technology reached a level where it became clinically feasible and commercially available. The employment of functional neuroimaging using SPECT has been instrumental in investigating diverse biochemical and metabolic alterations occurring within the brain. This imaging modality provides valuable insights into early and differential diagnosis, as well as facilitating a deeper understanding of the underlying pathological processes. 58 Various molecular radiotracers have been employed to assess brain functions, including regional blood flow, neurotransmitter deductions, and glucose metabolism. 59 Patterns of hypoperfusion can differentiate AD, which typically shows posterior parietal and temporal hypoperfusion, from FTD, where anterior frontal and temporal hypoperfusion are more common. However, the lower spatial resolution of SPECT compared to PET can be a limitation. 60
Several studies have undertaken the integration of machine learning (ML) and deep learning (DL) techniques with neuroimaging data to address the complex challenge of differential diagnosis between Alzheimer’s disease (AD) and frontotemporal dementia (FTD), which often present with overlapping clinical symptoms and morphological patterns. The studies have been organized based on the different modalities utilized in their research.
Structural MRI studies
Studies based on deep learning
Da Ma et al. (2020) 61 developed a sophisticated diagnostic system using brain volume and cortical thickness as features. They implemented a range of classifiers including Generative Adversarial Networks (GANs), multi-type and multi-scale feature deep neural networks (MMDNN), and traditional techniques like SVM and PCA. GANs, which involve simultaneous training of two neural networks—one for image generation and the other for discrimination—proved effective in this context. The study reported accuracies of 83.06% with PCA and SVM (multi-type), 85.97% with MDNN and volume features, and up to 88.28% with GANs (multi-type).
In 2021, Hu et al. 62 assessed the capability of a ResNet Convolutional Neural Network (CNN) to differentiate between AD and FTD using structural MRI images. ResNet, known for its residual learning models and advanced activation functions, was evaluated under nine different scenarios, achieving a remarkable diagnostic accuracy of 98.61% in the best-performing scenario.
Furthermore, Nguyen et al. (2022) 63 advocates for the application of two specific biomarker categories: structural grading and structural atrophy. They propose the training of a robust ensemble of 3D U-Nets to accurately differentiate between healthy brain patterns and those indicative of dementia. This approach produces an interpretable 3D grading map that effectively highlights regions of abnormality in the brain. Furthermore, this map can be leveraged to improve classification tasks through the implementation of graph convolutional networks. The classification accuracy achieves 89.7%.
One year later again Nguyen et al. (2023) 64 presents an innovative deep grading framework designed for both binary and multi-disease classification concerning Alzheimer’s Disease and FTD. The framework not only classifies disease types but also identifies specific brain regions related to these conditions through the use of color mapping. It focuses on two types of biomarkers: structural grading, which evaluates anatomical similarities, and structural atrophy, which assesses abnormalities in brain structure. By combining U-Nets, multi-layer perceptron (MLP) and SVM models, the method enhances disease detection and differential diagnosis accuracy. (accuracy = 93%) The findings demonstrate that the proposed ensemble model surpasses current state-of-the-art methods across various classification tasks and shows generalizability when tested on out-of-domain datasets.
Based on the studies reviewed, the classifier that demonstrates the best performance is the ResNet convolutional neural network, achieving an impressive diagnostic accuracy of 98.61%. 62 In contrast, ensemble model (U-Nets, MLP, and SVM) reported a slightly lower accuracy of 93.3%. 64 The selection of critical features, like brain volume and structural grading, is essential for enhancing model efficacy, and the use of diverse algorithms, including ensemble methods, has improved both classification and interpretability outcomes.
Studies based on machine learning
Muñoz-Ruiz et al. (2012) 65 devised a diagnostic system to distinguish between patients with FTD, AD, and mild cognitive impairment (MCI) using structural MRI images. The system utilized features from voxel-based morphometry (VBM), hippocampal volumetry (HV), and tensor-based morphometry (TBM). A regression classifier was employed, and the results demonstrated robust discriminatory capacity, particularly with the application of voxel-based morphometry (VBM) with the highest accuracy.
Recognizing the overlapping morphometric patterns between normal aging and neurodegenerative diseases such as AD and FTD, Raamana et al. (2014) 66 introduced a novel classifier using features derived from structural MRI images, including shape invariants, volumes, and local displacements of the lateral ventricles and hippocampus. For the classification they used support vector machine (SVM) and Bayes Net, and results showed that local atrophy in the lateral ventricles was a good biomarker for distinguishing between FTD, AD, and normal controls.
Furthermore, Möller et al. (2014) 67 harnessed the discriminative prowess of SVM classifiers in elucidating distinctive neuroanatomical alterations characteristic of behavioral variant FTD (bvFTD) and AD, the results suggested that SVM could effectively distinguish between these disorders, reporting an accuracy of 78.7% for diagnosing Alzheimer’s disease, and fostering insights into the pathophysiological underpinnings of these neurodegenerative disorders.
Concurrently, Klöppel et al. (2015) 68 investigates automated MRI diagnostic methods, particularly a linear SVM, for distinguishing various types of dementia, such as AD and FTD. The method demonstrates impressive accuracy (AUC = 97%) in differentiating healthy aging from dementia in training datasets, although its performance declines in real-world scenarios (AUC < 80%). These results indicate the promise of incorporating MRI-based tools into clinical settings and underscore the importance of continual methodological enhancements.
In a subsequent study, Wang et al. (2016) 69 scrutinized the diagnostic utility of neuropsychological examination and MRI-derived morphometric features in distinguishing AD from bvFTD. They examined brain atrophy in eight regions using MRI images and assessed 17 neuropsychological features, employing a Naïve Bayes classifier for classification. The study found that neuropsychological characteristics provided greater diagnostic accuracy in distinguishing between AD and bvFTD, and integrating gray matter atrophy with neuropsychological characteristics achieved a classification accuracy of 61.47%, illuminating the synergistic role of clinical and neuroimaging data in refining diagnostic accuracy.
Koikkalainen et al. (2016) 70 delved into the discriminative potential of structural MRI features across AD, LBD, FTD, vascular dementia, and healthy individuals. Quantitative features, including volume, vascular, and morphology characteristics, were extracted and classified using a multi-class Disease State Index (DSI) classifier. The study demonstrated structural differences between AD/FTD and healthy individuals using voxel-based and tensor-based morphometry, achieving a balanced accuracy of 69.1%, highlighting the nuanced neuroanatomical signatures indicative of AD, FTD, vascular dementia, and healthy aging, thus facilitating refined diagnostic algorithms.
In a study by Kim et al. (2019), 71 authors aim to classify individual patients with FTD and AD using a machine learning approach instead of traditional group analysis. All of the participants underwent volumetric MRI scans to assess cortical thickness. To enhance data quality and reduce dimensionality, the researchers employed the Laplace Beltrami operator, followed by principal component analysis (PCA) and linear discriminant analysis (LDA) for classifier development. The resulting hierarchical classification system achieved an overall accuracy of 75.8%, surpassing non-hierarchical approaches. The accuracies for specific classification steps varied between 86.1% and 92.1%.
Later, Poonam et al. 72 present an automated hierarchical classification model that employs Artificial Intelligence (AI) to improve the diagnostic accuracy of FTD and AD through the analysis of MRI data. The results demonstrated high classification accuracies, achieving 86.5% with SVM, 76% with LDA, and 72.7% with Naive Bayes, surpassing traditional multi-class models. These findings highlight the potential of AI methods to assist clinicians in effectively distinguishing between dementia subtypes, thereby facilitating timely diagnosis and intervention.
Chague et al. (2021) 73 proposed integrating artificial intelligence into clinical workflows for diagnosing dementia, using atrophy patterns to classify early-onset Alzheimer’s disease (EOAD), late-onset Alzheimer’s disease (LOAD), depression and FTD with an SVM classifier. The study found that incorporating SVM weight maps significantly enhanced diagnostic accuracy.
Similarly, in 2022, Pérez-Millan et al. 74 employed both supervised and unsupervised machine learning methodologies to differentiate between EOAD and FTD. Using cortical thickness and subcortical gray matter volume, they trained PCA and SVM classifiers, achieving classification accuracies of 87.2% for healthy individuals and EOAD, 80.8% for healthy individuals and FTD, and 66.5% for EOAD and FTD. The three-group classification accuracy was 65.2%.
At the same year, Koutsouleris et al. (2022) 75 evaluated sMRI patterns in patients with AD, MCI, schizophrenia, bvFTD, and healthy individuals. They used gray matter volume maps for training and employed NeuroMiner software to generate four diagnostic classifiers. The classification results using original non-recovery labels for distinguishing bvFTD from healthy individuals showed higher accuracy compared to other groups, with a balanced accuracy (BAC) of 78.7%, specificity of 67.4%, and sensitivity of 89.8%.
We propose Deep Grading, a novel framework for diagnosing neurodegenerative diseases such as AD and FTD. They utilize multi-channel Disease’s Coordinate maps to identify disease-specific patterns in different brain regions, enhancing classification accuracy. Using MRI data from diverse databases, the framework demonstrates strong performance and generalization across various tasks.
In 2023, Lampe et al. 76 employed atlas-based volumetry on MRI scans from 426 patients and 51 controls diagnosed with different neurodegenerative syndromes. Using SVM classifier, the study achieved high accuracy rates in both binary (71–95%) and multi-syndrome classifications. Disease-specific atrophy patterns played a key role in determining feature importance. Classification performance varied among syndromes, with better results seen in syndromes exhibiting regionally specific atrophy. Accuracy in disease classification improved with increased disease severity and duration, pinpointing optimal diagnostic windows.
In the same year Pérez-Millan et al. 77 utilizes machine learning methods with both cross-sectional and longitudinal MRI data to distinguish between AD and FTD. With a cohort of 339 subjects and advanced techniques for feature reduction, the study employs a support vector machine classifier. Results show that the longitudinal approach surpasses the cross-sectional method in accurately classifying AD and FTD, achieving accuracy rates between 83.3% and 95%. Emphasizing the significance of longitudinal data for enhanced accuracy and insight into disease progression, the algorithm identifies key brain regions influencing classification outcomes.
In summary, the research demonstrates substantial progress in utilizing advanced machine learning techniques with MRI for distinguishing AD and FTD, with
PET studies
Study based on deep learning
In 2022, Noella et al. 78 focused on differentiating between Parkinson’s disease (PD), FTD, and AD through the analysis of PET brain scans. They trained a Deep CNN (DCNN) with a generative adversarial architecture on FDG-PET datasets, achieving a classification accuracy of 97.7%, with both sensitivity and specificity at 97%.
Studies based on machine learning
Thiele et al. (2013) 79 explored the utility of F-18 FDG PET imaging in classification tasks using partial least squares (PLS) as the classifier. PLS, a dimension reduction method, was employed to handle datasets with numerous variables effectively, achieving commendable accuracy rates approaching 94%, indicative of its diagnostic efficacy. 80
In a subsequent study, Xia et al. (2014) 81 used FDG-PET images to classify individuals with AD, FTD, and controls, employing features like average glucose metabolism in cortical volumes, asymmetry, and spatial variation rates. They utilized the genetic algorithm-multiple kernel learning (GA-MKL) algorithm, achieving a diagnostic accuracy of 94.62% for classifying different types of dementia. GA is known for its efficiency in multi-objective optimizations, making it a cost-effective method for reducing feature dimensionality and improving classification accuracy. 82
Further advancing this field of study, Díaz-Álvarez et al. (2022) 83 aimed to distinguish between bvFTD and AD, as well as differentiate various subtypes of primary progressive aphasia (PPA), using genetic algorithms combined with NB and K-Nearest Neighbor (KNN) classifiers. They trained their model using PET image features and achieved high accuracies: 95.28% with KNN and 92.13% with NB for AD versus healthy controls, 96.67% with KNN and 95.83% with NB for bvFTD versus healthy controls, and around 90-91% for PPA variants classification. Continuing this trajectory, García-Gutierrez et al. 84 utilized PET datasets to classify individuals using SVM and Bayesian networks (Naive Bayes) classifiers. The study reported accuracies of 88.1% for Naive Bayes and 88.5% for SVM, with high precision and sensitivity.
The
SPECT study
Wang et al. (2013) 85 evaluated the performances of principal component analysis (PCA) and PLS methods for feature extraction from SPECT images to classify individuals with FTD, AD, and healthy controls. It investigates the potential of machine learning algorithms, combined with neuroimaging and neuropsychological clinical features, to improve differentiation between the two diseases. PCA transforms multivariate datasets into uncorrelated variables arranged by explained variance, 86 whereas PLS handles datasets with many variables by generating new components. For classification, tree classifiers, including elastic-net logistic regression (ENLR), SVM, and multiple discriminant analysis (MDA), were utilized. The study found that the PCA-based method, particularly PCA-ENLR, demonstrated higher consistency and reliability compared to PLS-based methods. The findings suggest that, at the time of presentation, the machine learning classification primarily relies on cognitive characteristics rather than imaging data.
fMRI studies
Hu et al. (2021) 87 proposed a novel framework for functional connectivity analysis has been introduced, emphasizing multi-band functional connectivity biomarkers. This approach decomposes Blood Oxygenation Level Dependent (BOLD) signals into various frequency bands using discrete wavelet transform, subsequently integrating them into a parameter-free multi-band fusion model. This model generates a sparsely-connected Functional Connectivity Network (sparse FCN) for each individual, facilitating closeness among similar sparse FCNs while maintaining distance from the most different ones. Additionally, the framework employs l1-SVM for simultaneous selection of brain regions and disease diagnosis. This model achieves the highest accuracy for all diseases: 90.18% for AD and 86.48% for FTD.
Multimodal studies
Studies based on machine learning
Bron et al. (2014) 88 adopted a multimodal approach that combined arterial spin labeling (ASL) with MRI techniques. They used cerebral blood flow (CBF) from ASL and gray matter atrophy from MRI scans as diagnostic markers, applying linear SVM for classification. This method provided important insights into the hemodynamic and structural changes associated with AD, FTD and control groups. Their findings highlighted CBF as a valuable diagnostic biomarker for dementia; however, the integration of ASL with structural MRI data did not significantly improve diagnostic performance, achieving an AUC of 91%.
In parallel, Muñoz-Ruiz et al. (2016) 89 advocated for the clinical utility of Disease State Index (DSI) algorithms in diagnosing FTD and AD. DSI is a statistical analysis technique that combines different data features to provide overall and individual evaluations for disease classification.90,91 The analysis included regional MRI volumes, regional cerebral blood flow ratios from SPECT data, levels of phosphorylated Tau-181 (P-Tau), amyloid β42 (Aβ42), total Tau (T-Tau) from CSF samples, and APOE genotype. DSI classification achieved an AUC of 89% for distinguishing two disease groups.
In the next year, Bron et al. (2017) 92 assessed the additional diagnostic benefits of ASL and DTI when used alongside structural MRI for computer-aided classification of these two diseases. SVMs employed for various classification tasks. The results demonstrated that the combination of ASL and DTI with structural MRI significantly enhanced classification accuracy for distinguishing between AD and FTD (AUC = 84%)
Later in 2018, Bouts et al. 93 conducted a multimodal study to design a differential diagnosis system for AD and bvFTD. They extracted features such as gray and white matter density from structural MRI, FA, MD, RD, and AxD from DTI images, and correlation (Corr) and partial correlation (pcor) from Rs-fMRI. These features were used to train an elastic net regression classifier. The combination of MD, corr, and FA maps yielded the highest AUC for diagnosing AD versus bvFTD (Accuracy = 78%).
Moguilner et al. (2022) 94 used a combination of neuropsychological data, MRI, EEG, and fMRI to design a classification system for AD, bvFTD, and cognitively normal individuals. They applied an eXtreme gradient boosting (XGBoost) classifier. The multimodal model exhibited excellent performance in distinguishing bvFTD and AD with an AUC of 92%.
The mentioned investigations, including those by Bron et al. (2017), 92 Bouts et al. (2018), 93 Chague et al. (2021), 73 Moguilner et al. (2022), 94 and Koutsouleris et al. (2022), 75 have further elucidated the diagnostic landscape through innovative methodologies such as multimodal fusion frameworks, elastic net regression classifiers, and integration of artificial intelligence into clinical workflows, collectively advancing the frontier of precision medicine in dementia diagnosis.
Summary of recent studies on the classification of AD and FTD using various MRI protocols and classifiers. The first four rows correspond to deep learning articles. The rest of the articles are based on machine learning.
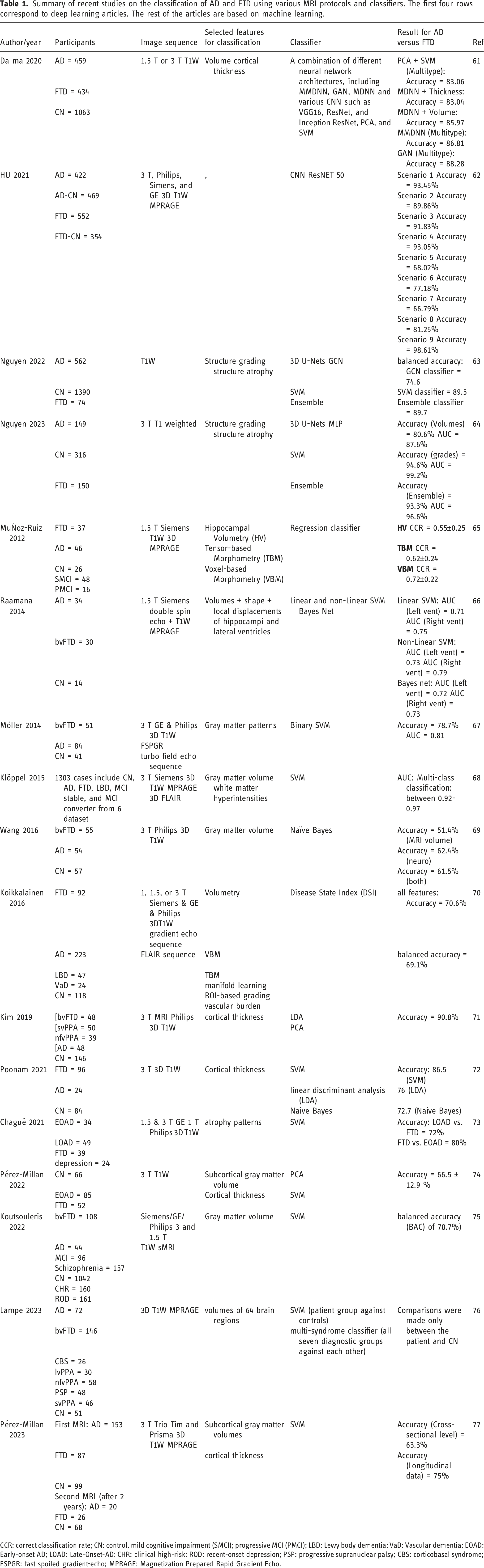
CCR: correct classification rate; CN: control, mild cognitive impairment (SMCI); progressive MCI (PMCI); LBD: Lewy body dementia; VaD: Vascular dementia; EOAD: Early-onset AD; LOAD: Late-Onset-AD; CHR: clinical high-risk; ROD: recent-onset depression; PSP: progressive supranuclear palsy; CBS: corticobasal syndrome; FSPGR: fast spoiled gradient-echo; MPRAGE: Magnetization Prepared Rapid Gradient Echo.
Summary of recent studies on the classification of AD and FTD using PET scans.
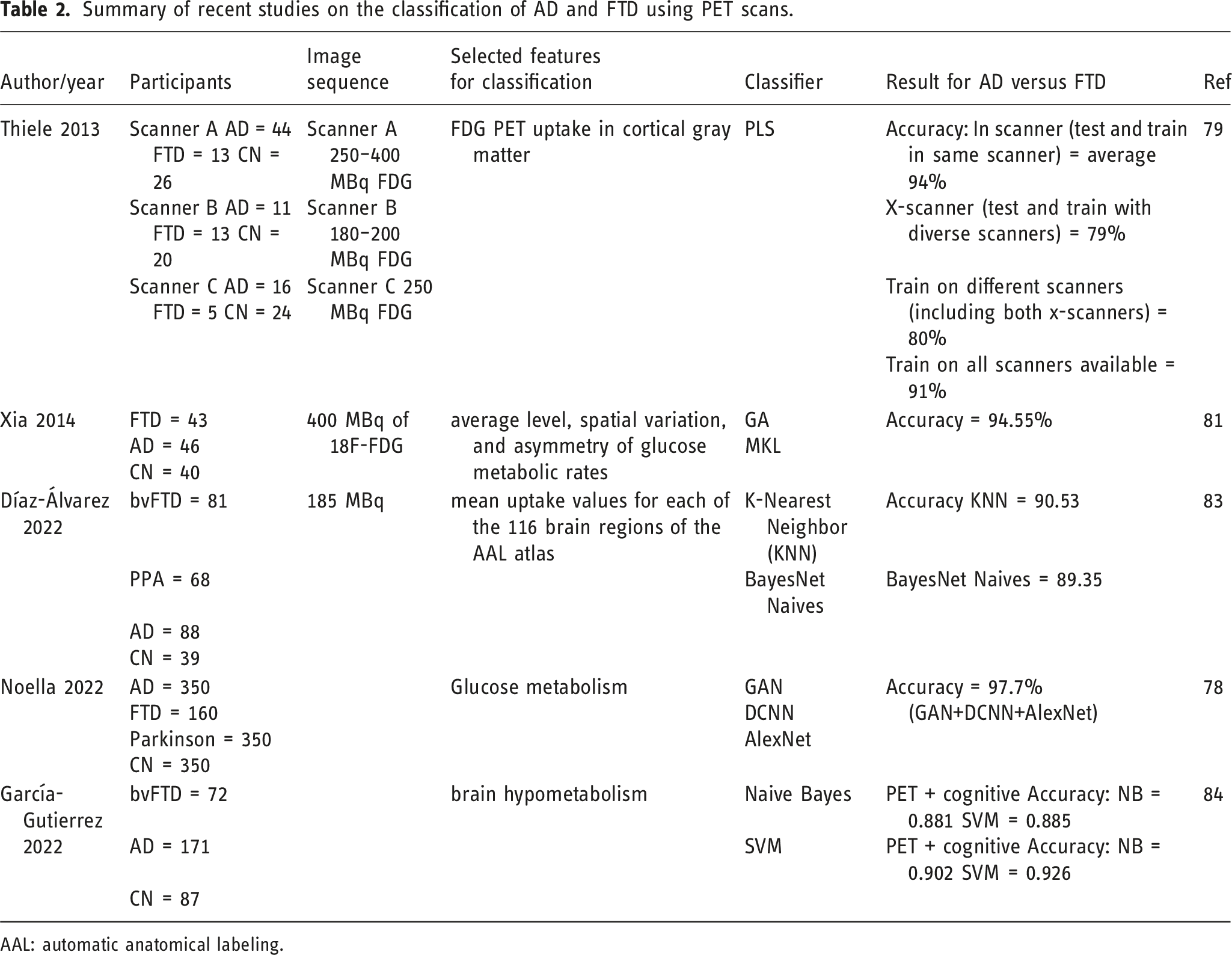
AAL: automatic anatomical labeling.
Summary of study on the classification of AD and FTD using SPECT.

Summary of study on the classification of AD and FTD using fMRI.
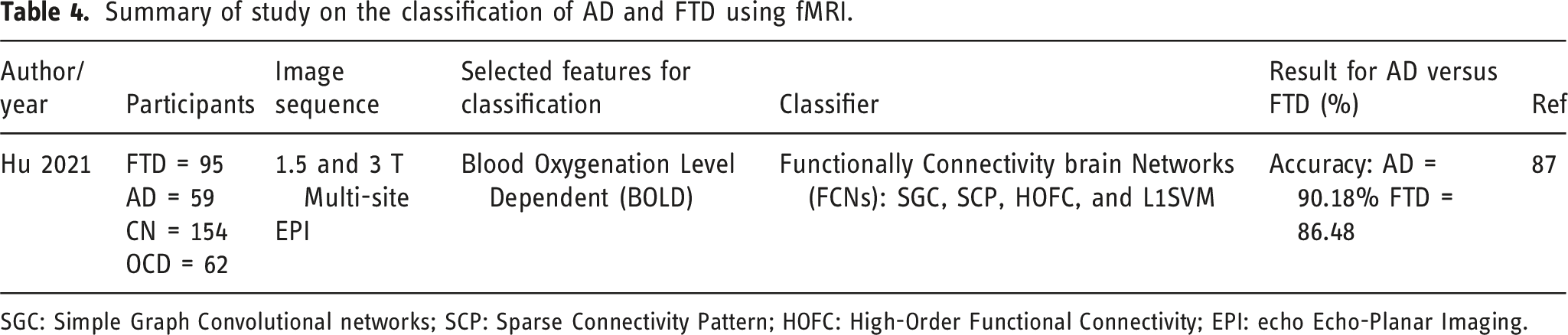
SGC: Simple Graph Convolutional networks; SCP: Sparse Connectivity Pattern; HOFC: High-Order Functional Connectivity; EPI: echo Echo-Planar Imaging.
Summary of study on the classification of AD and FTD using multi-modalities.
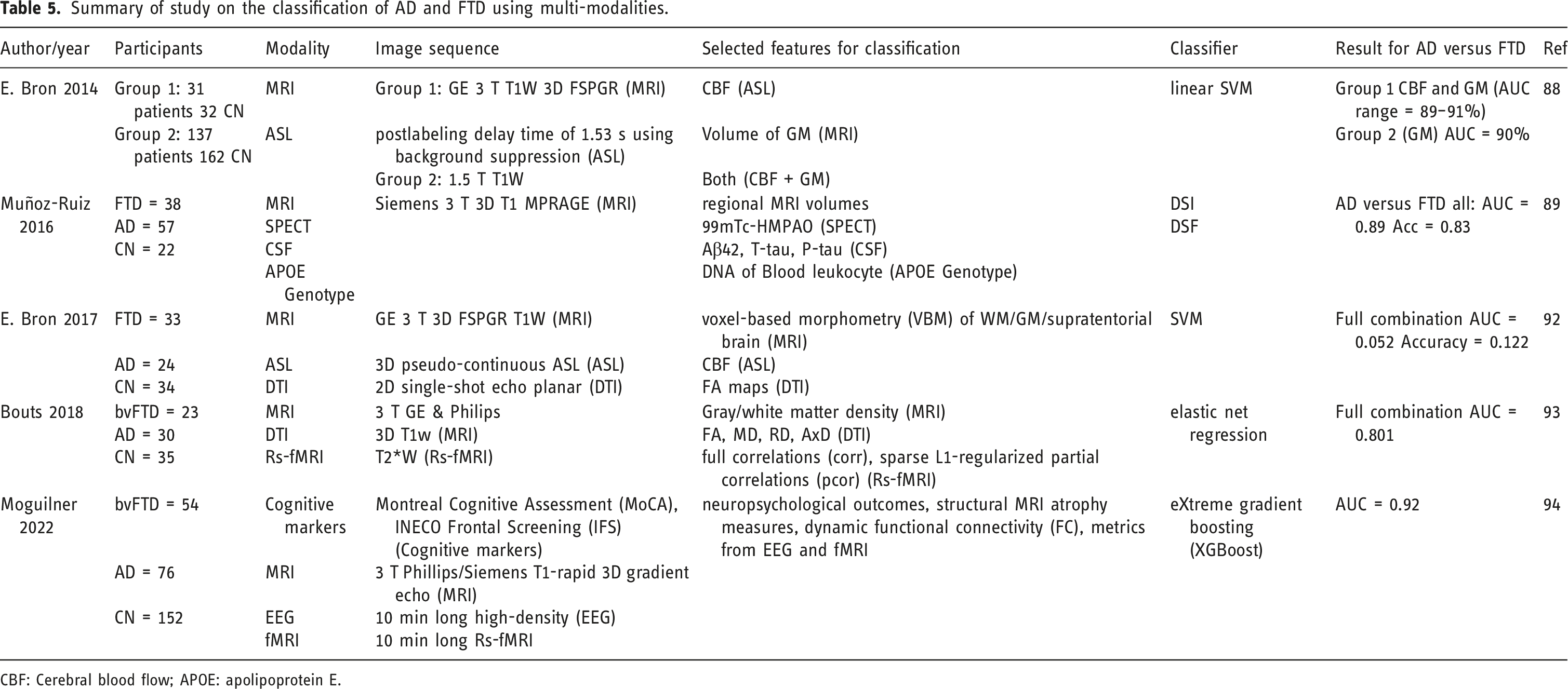
CBF: Cerebral blood flow; APOE: apolipoprotein E.
Discussion
The increasing prevalence of neurodegenerative diseases, particularly FTD and Alzheimer’s disease, underscores the urgent need for improved diagnostic methodologies. This narrative review highlights significant advancements in the application of artificial intelligence, especially machine learning and deep learning, in the differential diagnosis of these conditions. The integration of advanced neuroimaging techniques with AI has the potential to enhance diagnostic accuracy, facilitating timely and appropriate interventions for patients.
Best classifier and modality
Among the classifiers reviewed, the ResNet convolutional neural network stood out as the most effective, achieving the highest accuracy of 98.61%. The Support Vector Machine (SVM) classifier also demonstrated strong performance, particularly in studies employing traditional ML techniques. While MRI and PET showed promising results, further exploration of other imaging modalities would be beneficial. • •
Advantages and disadvantages of previous articles
The articles reviewed highlight several advantages, including the potential for enhanced diagnostic accuracy and the ability to leverage large datasets to train sophisticated models. However, they also reveal drawbacks, such as the necessity for comprehensive clinical evaluations alongside imaging data to ensure accurate diagnoses. Many studies did not adequately incorporate clinical assessments, which are crucial for understanding the complete clinical picture.
In conclusion, the integration of ML and DL techniques with neuroimaging data offers a promising avenue for the differential diagnosis of AD and FTD. Future research should prioritize refining these AI models, validating their performance in various clinical settings, and ensuring they complement traditional diagnostic methods. This multidisciplinary approach will be vital for advancing the diagnosis and treatment of neurodegenerative disorders, ultimately enhancing patient outcomes. The combination of traditional neuroimaging modalities with AI-driven analytical methods can significantly improve the differential diagnosis of AD and FTD. Techniques such as structural MRI, fMRI, DWI, DTI, PET, and SPECT each provide valuable insights, and their integration with ML and DL techniques has the potential to enhance diagnostic precision. Ongoing efforts should focus on refining these AI models and validating their effectiveness across diverse clinical contexts to fully harness their potential in diagnosing neurodegenerative diseases.
The findings from the review of ML and DL applications in diagnosing AD and FTD suggest a promising future for clinical practice, characterized by enhanced diagnostic accuracy and efficiency. However, addressing barriers related to data quality, integration challenges, resistance to change, ethical considerations, and financial implications is crucial for the successful implementation of these technologies in healthcare settings. Ongoing research, collaboration, and advocacy for regulatory frameworks will be key to overcoming these obstacles and realizing the full potential of AI in neurodegenerative disease diagnosis.
Limitations of the reviewed studies
Despite these encouraging results, several limitations warrant consideration. Many studies had relatively small sample sizes, which may restrict the generalizability of the findings. To validate the effectiveness of the proposed models across diverse populations, larger and more varied cohorts are necessary. Additionally, variations in methodologies—including differences in imaging protocols and classification techniques—complicate direct comparisons and the establishment of standardized diagnostic protocols.
Another significant limitation is the dependence on the quality of imaging data. Variations in imaging protocols, scanner types, and patient demographics can introduce biases that may influence model performance. While AI models can enhance diagnostic accuracy, they should not replace comprehensive clinical evaluations, genetic testing, and neurological assessments, which are critical for accurate diagnosis. Researchers should analyze biomarkers from various imaging modalities while considering patients’ clinical manifestations and incorporating findings from genetic and neurological examinations. This holistic approach will ensure a more thorough assessment of neurodegenerative diseases, ultimately leading to improved diagnostic precision and better patient outcomes.
Footnotes
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research Department at Mashhad University of Medical Sciences to support this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.