
Abstract
Background and purpose
Inter-hypothalamic adhesions (IHAs) are parenchymal tissue bridges traversing the third ventricle, previously reported only in the pediatric population. We aim to understand the prevalence of IHA in the adult population, assess their size and location, and ultimately investigate whether IHA volumes correlate with age.
Materials and methods
Patients who underwent routine high-resolution 3D T2WI MRI studies of the temporal bone/internal auditory canal at an otolaryngology clinic between 2008 and 2014 were consecutively selected. The presence of IHAs was confirmed when a parenchymal structure could be traced across the third ventricle, connecting bilateral hypothalamus, and was visible in at least two planes. They were classified based on their location within the third ventricle, considering their connection with hypothalamic nuclei. Patient clinical information were collected from electronic charts. The prevalence and volumes of IHAs were calculated. Associations between age and IHA volume, as well as between IHA type, age, volume, and gender, were analyzed.
Results
779 patients, with a mean age of 54.7 years were included. Among them, 44 IHAs were identified within 41 patients, resulting in a prevalence of 5.26% in our cohort. Type 1 IHA was the most frequently encountered type, comprising 70.5% of all cases. No significant correlation was observed between IHA volumes and age. Additionally, no associations were found between IHA type and age, volume, or gender.
Conclusion
IHAs are not exclusive to the pediatric population; they are also present in adults, with a prevalence of 5.26% in patients undergoing temporal bone/internal auditory canal MRI.
Keywords
Introduction
The term “inter-hypothalamic adhesion” (IHA) was first introduced in 2013 to describe a parenchymal bridge of tissue that traverses the third ventricle, connecting the bilateral hypothalamus. 1 To date, it has only been reported in the pediatric population1–7 and has never been documented in the adult population. On the other hand, inter-thalamic adhesions (ITAs), akin to IHAs, are glial bridges in the third ventricle that connect the medial thalamic surfaces and have undergone extensive investigation, with a reported prevalence ranging from 75% to 96% in the population.8–12 Variations in ITAs have been linked to various conditions, including schizophrenia, Chiari type 2, X-linked hydrocephalus, and Cornelia de Lange syndrome.13–16 Despite their similarities, IHAs have not garnered as much attention as ITAs, likely due to their much smaller size, lower prevalence, and the limited availability of high-resolution brain imaging. However, similar to ITAs, IHAs may also hold associations with a spectrum of pathological conditions. While some reports suggest a potential association between the presence of IHAs and congenital midline abnormalities, such claims rely on limited evidence from case reports or small case series.1,2 The clinical or pathological significance of IHAs, along with their potential use as imaging markers for brain pathologies, remains uncertain. 3
It is intriguing that IHAs have never been documented in the adult population thus far. This prompts the question of whether IHAs undergo morphological changes or involute as the brain grows and matures. Specifically, with ventricular enlargement and morphometric changes in brain parenchyma due to development and aging,17–19 IHAs might regress and become less detectable over time. If this is the case, they could serve for monitoring age-related changes or as indicators of age-related non-physiological alterations in the brain, a facet that has not been investigated before.
Given the scarcity of information in the literature concerning IHAs, especially within the adult population, our study aimed firstly to investigate their prevalence across all age groups. Additionally, we introduced a new categorization system based on their commonly encountered anatomical locations. Finally, we explored whether the volume of IHAs changes with age or if these categorizations are associated with age.
Materials and methods
Patient selection
The study was approved by the institutional review board, and informed consent was waived due to the nature of the study. Patients who underwent routine high-resolution T2WI MRI studies of the temporal bone/internal auditory canal at a tertiary academic-based otolaryngology clinic as a standard protocol between 2008 and 2014 were consecutively selected. The imaging was performed for various clinical indications, including, but not limited to, evaluating organic causes of hearing loss, tinnitus, clinical suspicion of tumors such as meningioma, acoustic schwannoma, cholesteatoma, inflammatory conditions, and postoperative evaluation following cochlear implantation. The end date of 2014 was chosen because the imaging protocol transitioned from coronally acquired to axially-acquired 3D T2WI, and the new sequence no longer covered the anatomical region of interest. The rationale for selecting this cohort was that they had T2-weighted High-Resolution CISS Coronal Thin and T2 SPACE Coronal thin sequences routinely available, as per institutional protocol, which provided excellent visibility of the third ventricle. Patients were excluded from the study if their field of view did not extend sufficiently anteriorly through the third ventricle, due to anatomical constraints that could hinder the accurate identification of adhesions, such as cases where the walls of the third ventricle were overlapping, either due to adjacent mass effect or a slit-like third ventricle; cases affected by metallic and motion artifacts, resulting in poor image quality that impeded adequate evaluation, were also excluded (Figure 1). Patient demographic information, along with their medical history and clinical data, were gathered from electronic archives. Patient selection flowchart FOV: Field of View, n: Number.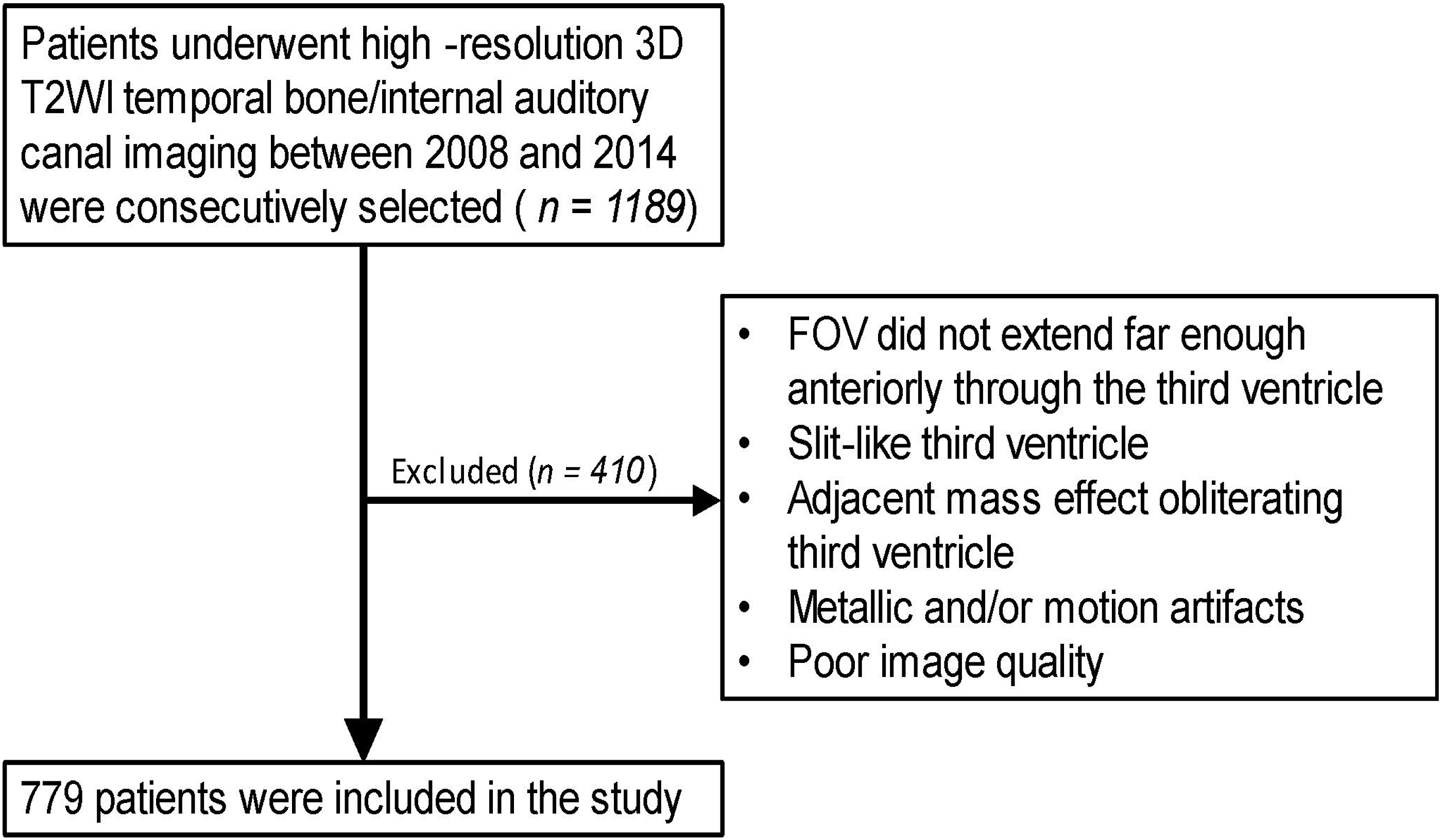
Image acquisition
The imaging studies were conducted using several MRI scanners, including the 3T Siemens Trio and Skyra, Siemens 1.5 T Avanto and Symphony, and Philips 1.5 T Intera. The following sequences were employed: T2 SPACE Coronal thin (matrix of 256 × 256, FOV of 130 mm with two signal averages, and TR/TE of 1000/205), T2 High Resolution CISS Coronal Thin (matrix of 256 × 192, FOV of 180 mm with one signal average, and TR/TE of 11.6/5.8). The Vitrea multi-planar reconstruction tool (Canon Medical Systems USA, Irvine, CA) was employed to reconstruct the coronally acquired images into axial and sagittal planes. Imaging review was conducted using Philips IntelliSpace® PACS (Koninklijke Philips NV, Amsterdam, Netherlands).
Image interpretation
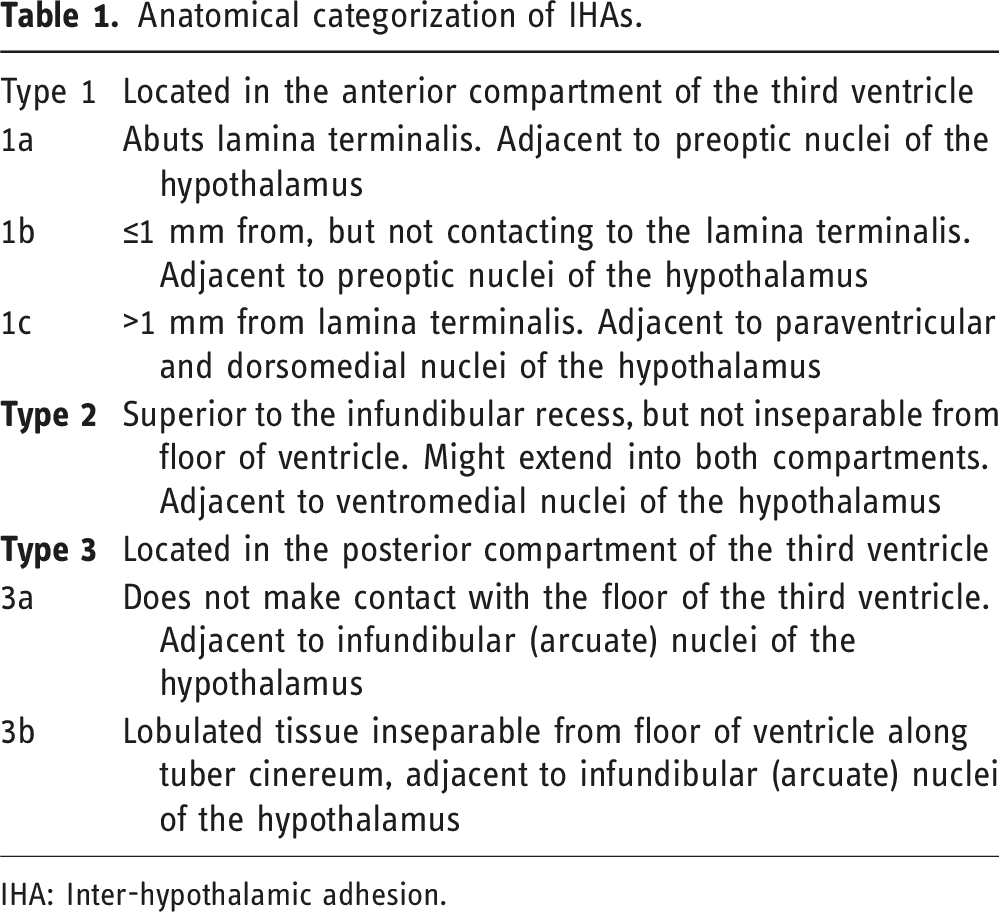
The presence of IHAs was confirmed when a parenchymal structure could be traced across the third ventricle, connecting the bilateral hypothalamus, and was visible in at least two planes (Figure 2). The assessment was conducted visually by a neuroradiologist with 15 years of expertise. Based on the observed anatomical localization patterns within the third ventricle, we propose a new classification system building upon our previous system
20
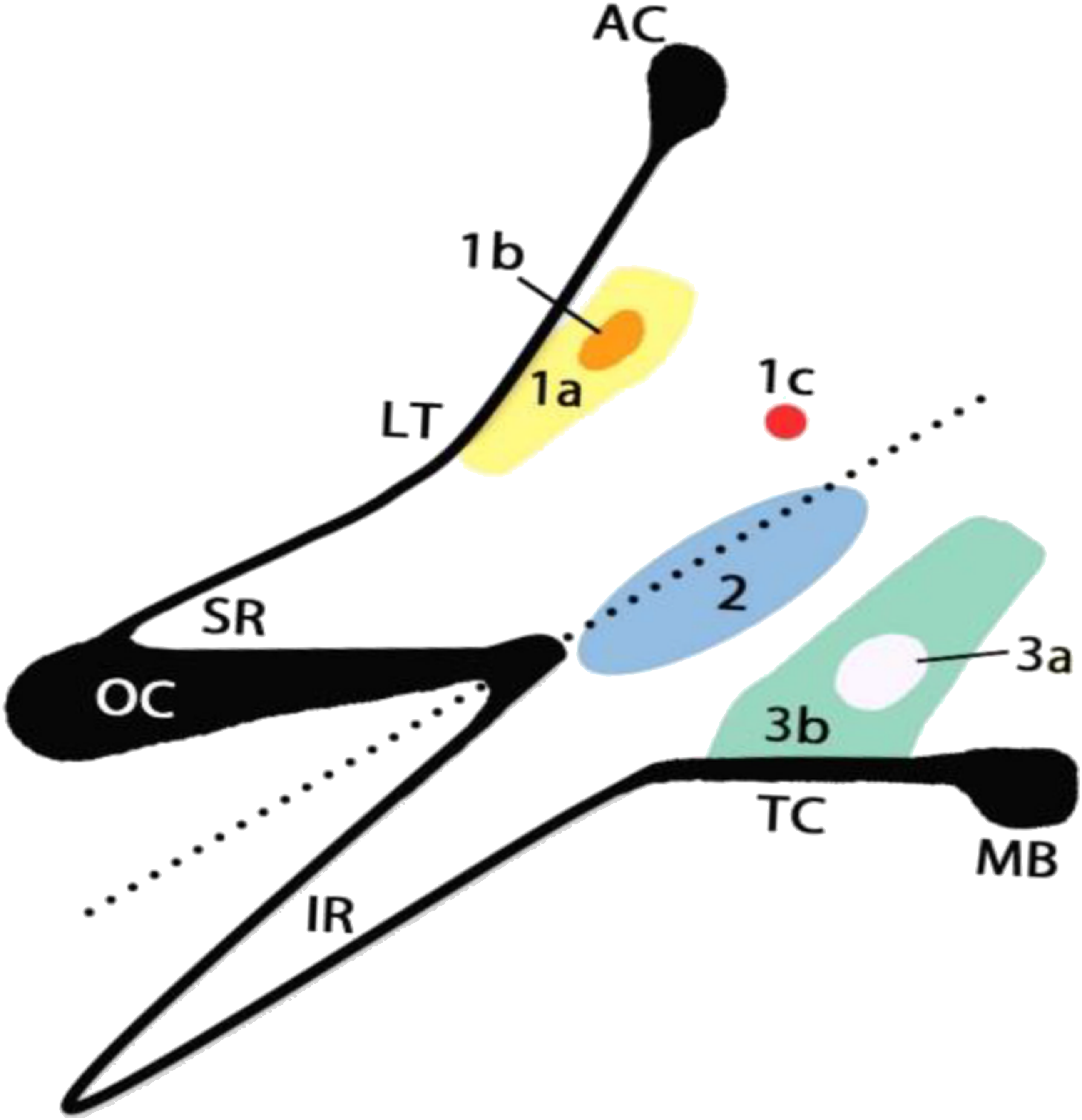
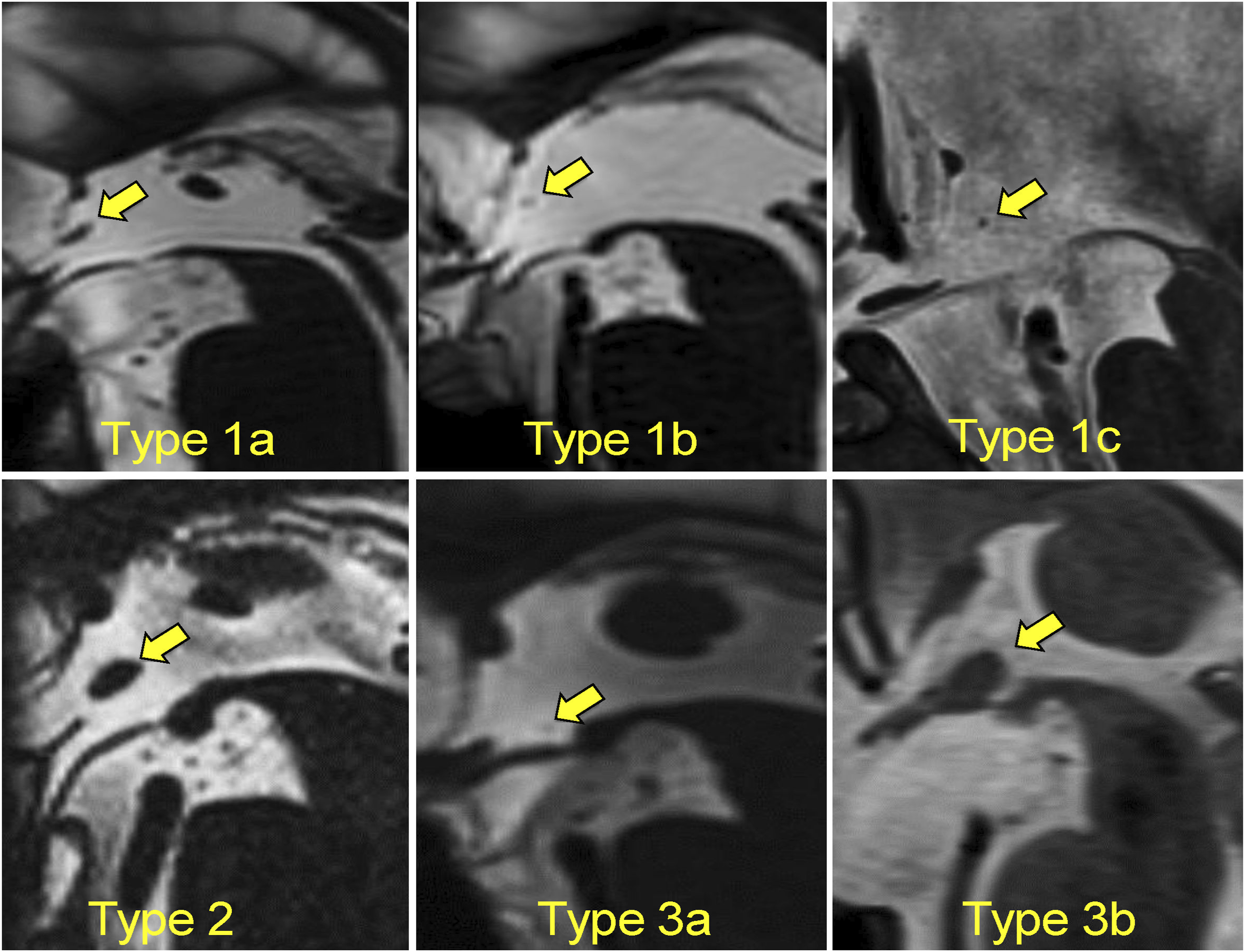
. This novel system includes subcategories 3a and 3b, reflecting variations exhibited by type 3 IHAs. The IHAs were classified according to their location along an imaginary oblique line separating the supraoptic recess from the infundibular recess, dividing the third ventricle into anterior-superior and posterior-inferior compartments. Additionally, their association with the hypothalamic nuclei was also considered. The groups were further subdivided based on the distance from the lamina terminalis or the distance from the floor of the ventricle (Figures 3 and 4) (Table 1). Visual evaluation of IHAs was conducted using high-resolution 3D T2WI MRI scans primarily acquired for imaging of the temporal bone/internal auditory canal but extending into the third ventricle. All patients underwent evaluation in three different planes: (A) coronal, (B) sagittal, and (C) axial. A positive result was considered if adhesions were visually identifiable in at least two different planes. White arrows show lamina terminals, yellow arrowheads show a type 1b IHA. IHA: Inter-hypothalamic Adhesion. Anatomical Categorization of IHAs. An imaginary oblique line between the SR and IR divides the third ventricle into anterior and posterior compartments. Type 1 IHAs are located in the anterior segment and are further subdivided based on their distance from the lamina terminalis (a: adjacent, b: ≤1 mm, c: >1 mm). Type 2 IHAs are located superior to the IR and might extend into both compartments. Type 3 IHAs are located in the posterior compartment (a: not contacting the floor, b: adjacent to the floor). IHA: Inter-hypothalamic Adhesion, AC: anterior commissure, LT: lamina terminalis, OC: optic chiasm, TC: tuber cinereum, MB: mammillary body, SR: supraoptic recess, IR: infundibular recess. Examples for each defined subtype. Anatomical categorization of IHAs. IHA: Inter-hypothalamic adhesion.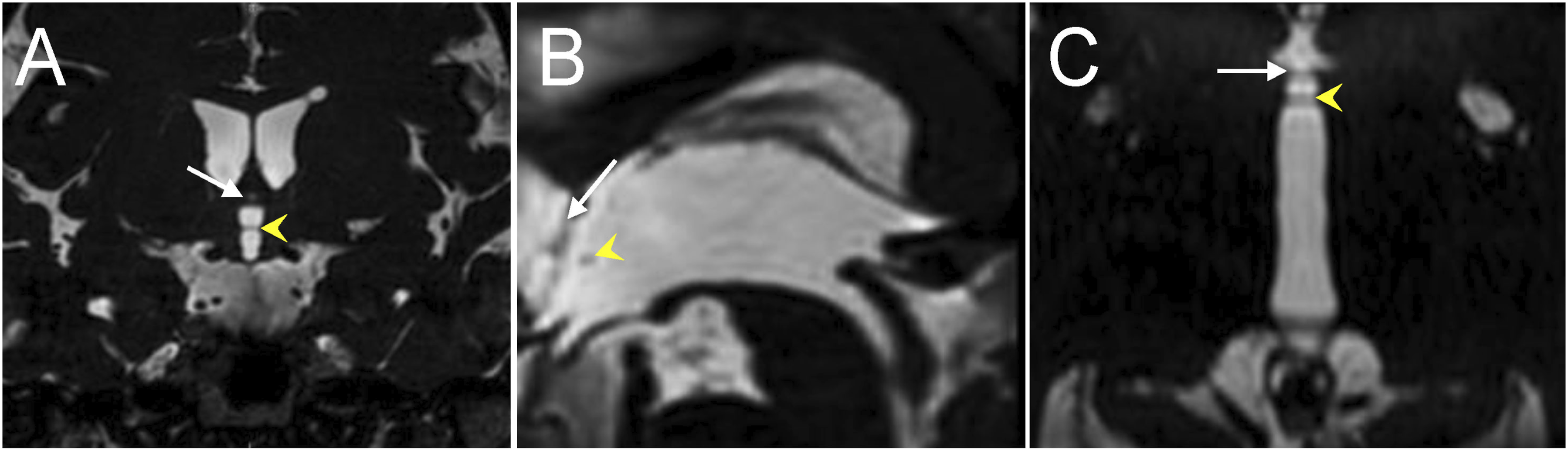
For volume measurement, the largest dimension of the IHA base (a) and the perpendicular diameter to this (b) were measured on the sagittal view. The height of the cylindroid (h) was estimated by the width of the third ventricle. All measurements were manually conducted on Philips IntelliSpace® Radiology PACS DICOM viewer using the standard ruler tool.
Volume(V) of the IHA was approximated using the volume of an elliptical cylinder, according to the following formula:
Statistical analysis
Descriptive statistics were calculated. Kolmogorov–Smirnov was applied to assess normal distribution. The Mann–Whitney U test or independent samples t test were employed for comparison numeric variables accordingly to normality distribution. Fisher’s exact test was used for comparison of categorical variables. Pearson’s correlation coefficient was utilized for assessing correlation between IHA volume and patient age. Kruskal–Wallis test was utilized for comparing IHA categories with age. Statistical significance was set at two-tailed p < .05. All statistical analyses were conducted using SPSS v.29 (IBM, New York).
Results
After exclusions (Figure 1), the study involved 779 consecutive patients, with a mean age of 54.7 years (range: 7 months to 95 years). Among them, inter-hypothalamic adhesions (IHAs) were identified in 41 individuals (5.26%). For patients with IHAs, the mean age was 52.38 years (range: 17 to 84 years), and there was no significant age difference between those with and without IHAs (p = .351) (Figure 5). The male-to-female ratio was 20:21 in people with IHAs, gender distribution did not statistically significant difference compared to no IHA group (p = .620). In our cohort, there were 19 pediatric patients (age <18 years) and 2 of them were positive for IHAs, corresponding to a prevalence of 10.53% in the pediatric age group. Population chart showing number of positive cases in each age. IHA: Inter-hypothalamic Adhesion.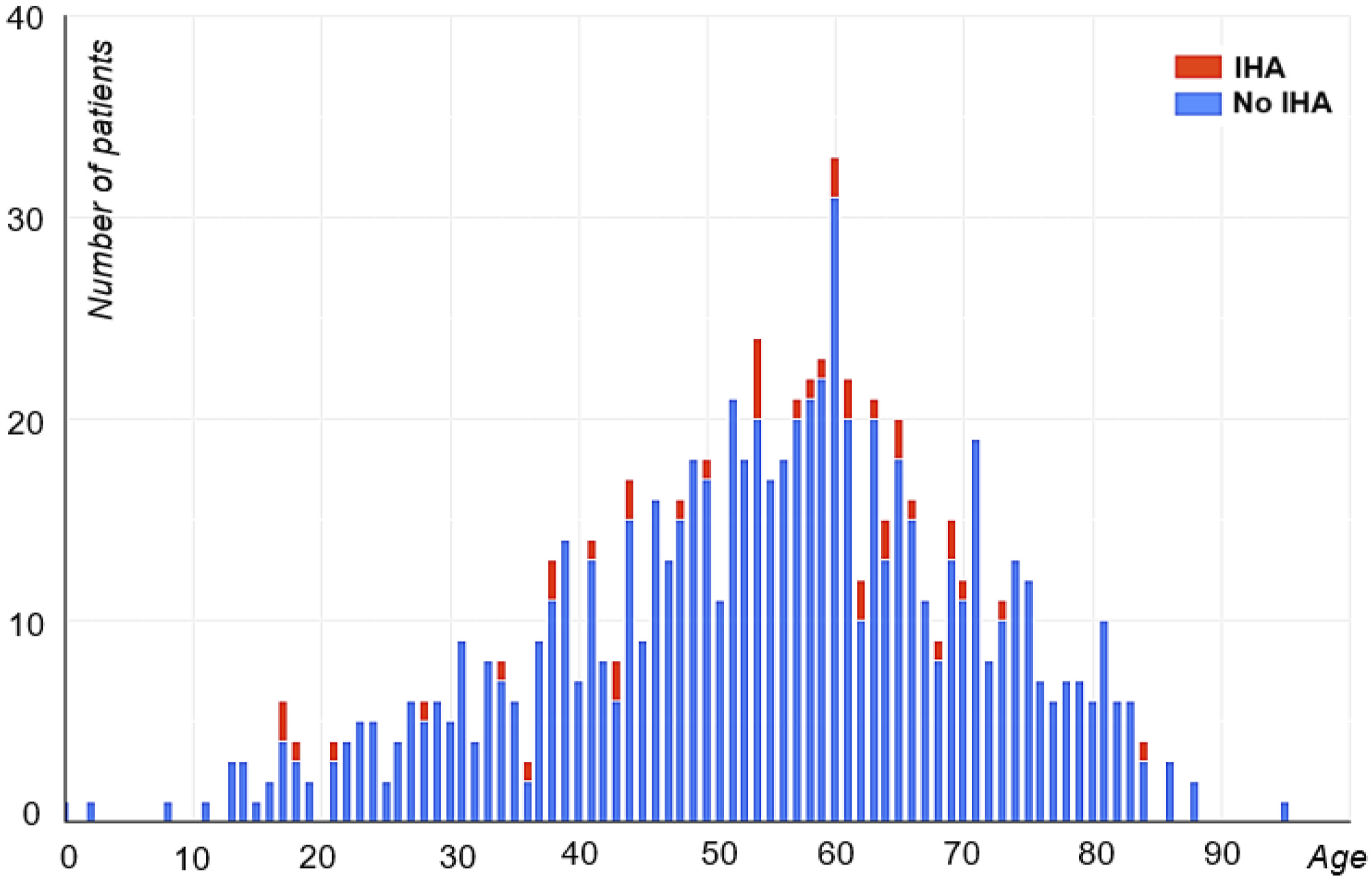
We identified a total of 44 IHAs among 41 patients, with three patients exhibiting two distinct IHAs (Type 1b and 3a; Type 1b and 2; Type 1b and 3b). The majority of the cases were type 1 IHAs, particularly type 1b. The distribution of IHAs among the categories was as follows: Type 1a (7 cases), Type 1b (27 cases), Type 1c (1 case), Type 2 (3 cases), Type 3a (2 cases), and Type 3b (4 cases).
The measured inter-hypothalamic adhesion (IHA) volumes varied between 0.37 mm³ and 21.03 mm³, with a mean volume of 5.74 mm³. No significant correlation was observed between IHA volume and age (Pearson correlation coefficient r = 0.065, p = .625) (Figure 6). Furthermore, gender did not exhibit any significant association with IHA volume (p = .357). Similarly, no statistically significant association was found between the IHA categories and patient age (p = .627). Volumetric assessment of each identified inter-hypothalamic adhesion is distributed by age. There was no correlation between age and IHA volume. IHA: Inter-hypothalamic adhesion.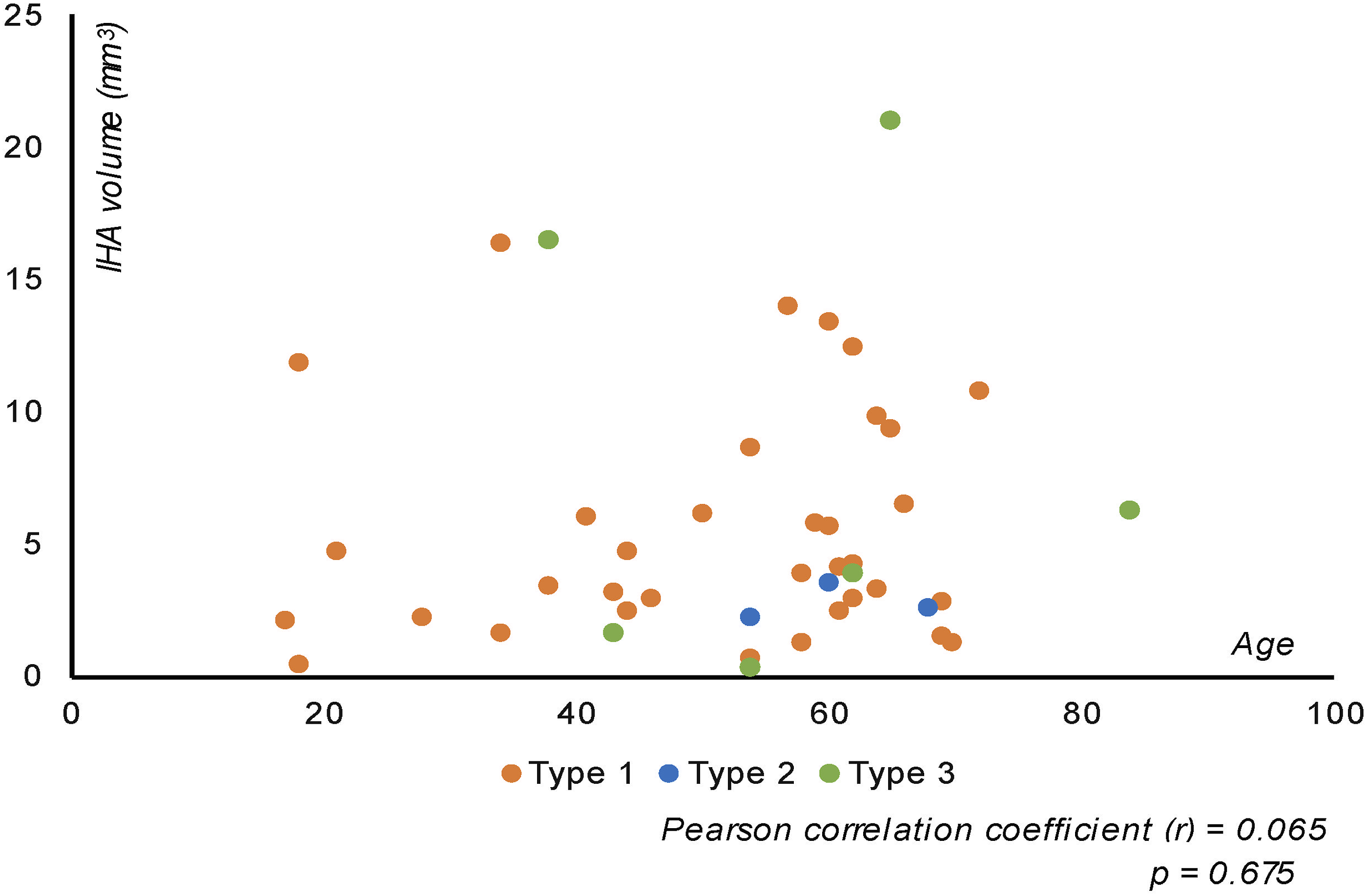
Upon reviewing the medical records of the 41 IHA patients, it was found that two cases had documented congenital heart defects or arrhythmias. One patient had undergone repair for a congenital encephalocele, and no other documented history of midline deformities was reported. Additionally, six patients exhibited thyroid disorders, including goiter and hypothyroidism. Among these patients, 10 cases had a documented history of acoustic neuromas, while 3 cases were diagnosed with meningiomas attributable to the cohort consisting of patients referred from an otolaryngology clinic.
Discussion
In this study, we investigated MRI studies from a cohort spanning from 7 months to 95 years of age and found an IHA prevalence of approximately 5.26%. We chose to evaluate MRI studies scanned with an internal auditory canal protocol, as this routinely had a high-resolution T2-weighted images with sufficient anatomic coverage, resolution, and ability to distinguish small brain structures from adjacent CSF. Our investigation extended beyond the previously reported pediatric population, aiming to discern whether IHA volume could indicate any age-related changes in the brain through volumetric assessment. However, we did not find a statistically significant correlation between IHA volumes and age, nor did we find any association between any IHA type and age or volume and gender. In our cohort, the pediatric age group exhibited a higher prevalence of IHAs compared to the overall prevalence (10.53% vs 5.26%). However, given the small pediatric sample size relative to the adult population in this cohort (n = 19 vs n = 760), it is not appropriate to infer that IHAs are more common in the pediatric age group based on this data. Moreover, in our recent study 20 on a pediatric population of 1,550 children, we reported a prevalence of 2.13%. This difference between the two studies is likely due to the higher spatial resolution of the MRI in the current study, which allowed for better detection of these small structures.
In the literature, IHAs have been addressed in a limited number of studies, all of which focused on the pediatric population.1–7 Some authors have suggested that upon encountering an inter-hypothalamic adhesion, a thorough examination of midline abnormalities should be conducted. After thorough evaluation of signs, symptoms, and a comprehensive brain examination, inter-hypothalamic adhesions can be deemed incidental and isolated findings. 21 On contrary some argue that neuroradiologists and other members of the care team should avoid unnecessary alarm, as these findings may be incidental in many patients. 22 Some studies have associated inter-hypothalamic adhesions with the CDK5RAP2 (MCPH3) mutation, an autosomal recessive primary microcephaly gene.23,24 However, the most comprehensive study on IHAs, conducted by Ahmed et al., 3 concluded that IHAs represented an isolated finding thought to be of no clinical significance. They suggested that it may result from incomplete hypothalamic cleavage, failed apoptosis, or abnormal neuronal migration, with the latter being potentially more likely, given the association they found with gray matter heterotopia discovered in 23 of 57 patients. Nevertheless, the evidence level in the current literature is insufficient to conclusively establish direct associations between IHAs and specific conditions.
Inter-thalamic adhesions (ITA) are structures similar to IHAs, but they connect the bilateral thalami instead of the hypothalami. They have been extensively studied, and alterations in this structure have been associated with a wide range of disorders in many studies.13–16,25–29 Considering their larger size and higher prevalence, it is understandable that IHAs have been much less investigated compared to ITAs. High-resolution imaging sequences are necessary for this investigation. However, IHAs can also serve as indicators of pathological conditions, which warrant further investigation.
In this study, we discovered that the majority of IHAs (70.5%) are situated within the anterior compartment (Type 1) of the third ventricle, closely associated with the lamina terminalis (LT). As the neural tube continues to develop, it bends and folds, shaping the primitive structures of the brain. The lamina terminalis becomes firmly established as the anterior wall of the third ventricle through the closure of the anterior neuropore.30,31 Subtle variations during the formation of LT might be contributing to the development of Type 1 IHAs.
Our study represents the first report on IHA prevalence in the overall population. We find it intriguing that IHAs have only been reported in the pediatric population so far. Consequently, we had initially hypothesized that IHAs might undergo changes in conjunction with the morphometric alterations of the brain. However, our study revealed that IHA are prevalent in both the adult and pediatric populations, and we found no association between volume and age.
In this study, we utilized imaging data from patients referred from an otolaryngology clinic with an IAC protocol MRI, most commonly for hearing loss. We chose this protocol specifically due to its high-quality T2-weighted imaging of the center of the brain rather than for any suspected link with hearing abnormalities. This protocol involved high-resolution 3D T2WI MRI studies of the temporal bone/internal auditory canal, but also captured the third ventricle in great detail. Many of the IHAs appeared very small, which may explain their previously underreported prevalence. However, utilizing this dataset introduces selection bias, as our cohort does not represent the normal population. Additionally, because hearing complaints are often associated with aging, the cohort is skewed toward older individuals, as evidenced by the smaller sample size in the pediatric age group. Furthermore, the reported prevalence of co-occurring tumors, particularly acoustic neuromas and meningiomas, cannot be directly attributed to the presence of IHAs, but rather to the study cohort comprising of patients referred from an otolaryngology clinic. Caution is warranted when proposing potential associations based on a cohort referred for various reasons, especially given that the clinical data were gathered retrospectively from medical charts, which can also introduce biases. The clinic’s affiliation with a tertiary academic institution may also lead to the referral of more complex cases, potentially increasing the observed prevalence of pathologies, independent of any association with IHAs. Prospective studies are needed to determine whether there is a true association between these pathologies and IHAs, or if IHAs could serve as an imaging marker for physiological or pathological changes.
Conclusions
This is the first study to demonstrate the presence of IHAs in adults. Our findings revealed a prevalence of 5.26% in patients undergoing temporal bone/internal auditory canal MRI due to various reasons. We identified multiple types of IHAs based on their location and associations with nearby structures. No relationship was observed between IHA volume or subtype and age. However, further research is imperative to determine whether IHAs could serve as potential indicators of underlying physiological or pathological conditions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board
Approved by University of Minnesota Institutional Review Board.
Informed consent
Informed consent was waived due to the nature of the study.