
Abstract
Although the effectiveness of thrombectomy has become clear, there is no consensus on whether sedation should be performed under general anesthesia or procedural sedation. Midazolam is used to achieve mild sedation during invasive treatments and examinations. This study aimed to investigate the treatment outcomes of thrombectomy under mild sedation using midazolam and report them retrospectively. This study included 100 cases of acute occlusion of the anterior circulation of intracranial vessels with a National Institutes of Health Stroke Scale (NIHSS) score of 10 or more who underwent thrombectomy under sedation using midazolam at our hospital between 2023 and 2024. The average age of the patients was 79.0 ± 12.2 years, and the preoperative NIHSS score was 19.8 ± 6.4. In total, 92 cases (92.0%) with modified Thrombolysis in Cerebral Infarction 2B or higher recovered with an average time from puncture to recanalization of 32 ± 23 min, and 52 cases (52.0%) had a favorable outcome (modified Rankin Scale 0–2) 3 months later. Anesthesia-related complications included postoperative pneumonia in seven cases (7.0%), and procedural complications included symptomatic intracranial hemorrhage due to perforation of intracranial vessels by the microguidewire in one case (1.0%). Nine patients (9.0%) died 3 months after surgery. Thrombectomy under procedural sedation using midazolam achieves favorable outcomes owing to favorable and rapid recanalization. In addition, there are few procedural complications due to body movement and few anesthesia-related complications due to sedation, making this a safe method.
Introduction
The effectiveness of thrombectomy for acute cerebral infarction has been demonstrated in various large-scale studies, and its use has become widespread worldwide.1–3 However, there is no consensus on the optimal sedation method for thrombectomy. Thrombectomy should be performed under procedural or general anesthesia. When performing thrombectomy under general anesthesia, it may take time to retrieve the thrombus because it takes time to perform anesthesia induction, including intubation, before the procedure is initiated. However, it has the advantage of reducing the patient’s body movement, which may shorten the procedure time and ensure airway security. Furthermore, some anesthetics may promote cerebral ischemic resistance by suppressing cerebral oxygen metabolism 4 and may protect the ischemic area by increasing cerebral blood flow and reducing cerebral vascular resistance. 5 When performing thrombectomy under procedural sedation, on the other hand, there is a risk of complications such as perforator branch perforation due to unexpected movements of the catheter operation caused by the patient’s body movement and the procedure time may be extended, but the time to proceed to the procedure is relatively short. Furthermore, it may be possible to avoid worsening the prognosis of cerebral infarction due to a drop in blood pressure caused by general anesthesia. A report summarizing comparatively large studies examining the differences between these techniques reported that thrombectomy under general anesthesia correlated with a good functional prognosis; however, the level of evidence is by no means high, and there have been no established reports on the use of specific anesthetics.6–9
Midazolam is a benzodiazepine sedative that takes effect within 10 s to 2 min when administered intravenously and lasts for several hours. 10 It is used worldwide for mild sedation during dental treatments or gastrointestinal endoscopy.11–14 Furthermore, when neurological findings are difficult to obtain after the administration of sedatives during endovascular treatment, it is possible to quickly reverse sedation using flumazenil, a benzodiazepine drug antagonist. 15 There have been comprehensive reports of endovascular treatment of aneurysms using midazolam, which can be said to be highly safe.16–18 However, there are no comprehensive reports of thrombectomy performed under procedural sedation with midazolam. In recent years, our institution has been performing thrombectomies under mild sedation with midazolam, with a focus on its rapid efficacy and safety. This study aimed to investigate the safe and favorable treatment outcomes of thrombectomy after acute cerebral infarction under midazolam sedation at our institution.
Methods
Patient selection
This study included 176 patients who underwent thrombectomy at our hospital from 2023 to 2024. Of these, 168 cases were included, excluding one case in which a safe airway was required due to impaired consciousness, one case in which simultaneous cervical spine surgery was required, five cases in which a reliable airway was required to perform direct cervical artery puncture, and one case in which midazolam could not be administered due to severe renal failure requiring dialysis. After excluding 68 cases, 100 cases with anterior circulation lesions and a National Institutes of Health Stroke Scale (NIHSS) score of 10 or more based on past studies were selected as eligible patients. Data on patient background, procedure method, blood pressure fluctuations during the procedure, and postoperative conditions were extracted from electronic medical records. In addition, the site of vascular occlusion and patency status after thrombectomy were evaluated using angiography. The site of vascular occlusion and patency status were evaluated individually by each surgeon and the first author; when the evaluations differed, the judgment of the other co-author was followed.
Sedation method
After arriving at the hospital, for patients who were judged to require thrombectomy based on head computed tomography (CT) or head magnetic resonance imaging (MRI), an intravenous line was established and midazolam (0.06 mg/kg body weight) was administered as a bolus over 1 min, followed by continuous administration at 0.06 mg/h/kg of body weight, and pentazocine (15 mg) was administered intravenously for pain control. The sedation depth during surgery was monitored based on the patient’s respiratory status and physical movement, and the dosage of midazolam was changed if necessary. After the procedure, continuous administration of midazolam was terminated, and if the patient was not awakened or the surgeon judged that early confirmation of neurological findings was necessary, 0.2 mg flumazenil was administered intravenously, and re-administration was performed every 4 min up to a maximum of 1 mg until awakening was achieved. There were no established criteria for flumazenil administration; therefore, the decision was made at the surgeon’s discretion.
Procedure
The procedure was performed via the right femoral artery approach, and an upper-arm approach was used depending on the surgeon’s judgment. A balloon-guiding catheter was guided to the target blood vessel, a distal access catheter and a microcatheter were inserted near the occluded blood vessel, and a lesion crossing was performed using a microguidewire. While retrieval using the combined technique is the norm, retrieval using the direct aspiration first-pass technique (ADAPT) was performed at the surgeon’s discretion. There were no guidelines for determining whether to employ a combined technique or ADAPT as a method of thrombectomy. The surgeon decided which stent was to be used in the combined technique. The thrombectomy procedure was performed by adequately experienced surgeons who were instructors or specialists at the Japanese Society of Neuroendovascular Therapy.
Evaluation method
Patient background information, age, sex, medical history, and smoking history were obtained from the electronic medical records.
Image evaluation was performed using head CT and MRI at the time of consultation and diffusion-weighted image (DWI)-Alberta Stroke Program Early CT Score (ASPECTS) and CT-ASPECTS. The site of occlusion was evaluated from the results of angiography at the time of thrombectomy.
Functional evaluation was performed using the modified Rankin Scale (mRS) before the procedure, the mRS 3 months after surgery, the NIHSS score immediately before surgery, and the NIHSS score 24 h after surgery from electronic medical records. The mRS was assessed based on the patient’s condition in the electronic medical record and was independently assessed by the first author and one co-author, with a third co-author providing judgement in case of discrepancy.
Complications were evaluated for the presence or absence of anesthesiologic and interventional complications using electronic medical records and radiological images. Anesthesiologic complications were defined as complications related to anesthesia, such as postoperative pneumonia, or cases in which general anesthesia was administered due to excessive sedation. Complications are defined as follows: Postoperative pneumonia was defined as a complication that occurred within 48 h after surgery, in which images showed clear signs of pneumonia, the patient had a fever, and the attending physician administered antibiotics. Interventional complications were defined as those that occurred because of the patient’s movement during surgery that affected the patient’s outcome.
The vascular occlusion site, thrombectomy method, time of onset or last healthy time, time of arrival at the hospital, time of puncture, and time of recanalization were also evaluated from the electronic medical and radiological image records. Recanalization status was evaluated using the modified Thrombolysis in Cerebral Infarction (mTICI) scale.
Dichotomous variables were presented as the number of individuals and percentages. Continuous variables are presented as mean ± standard deviation or median and interquartile range.
Results
Patient characteristics
Characteristics of patients with acute ischemic stroke in midazolam sedation undergoing thrombectomy.
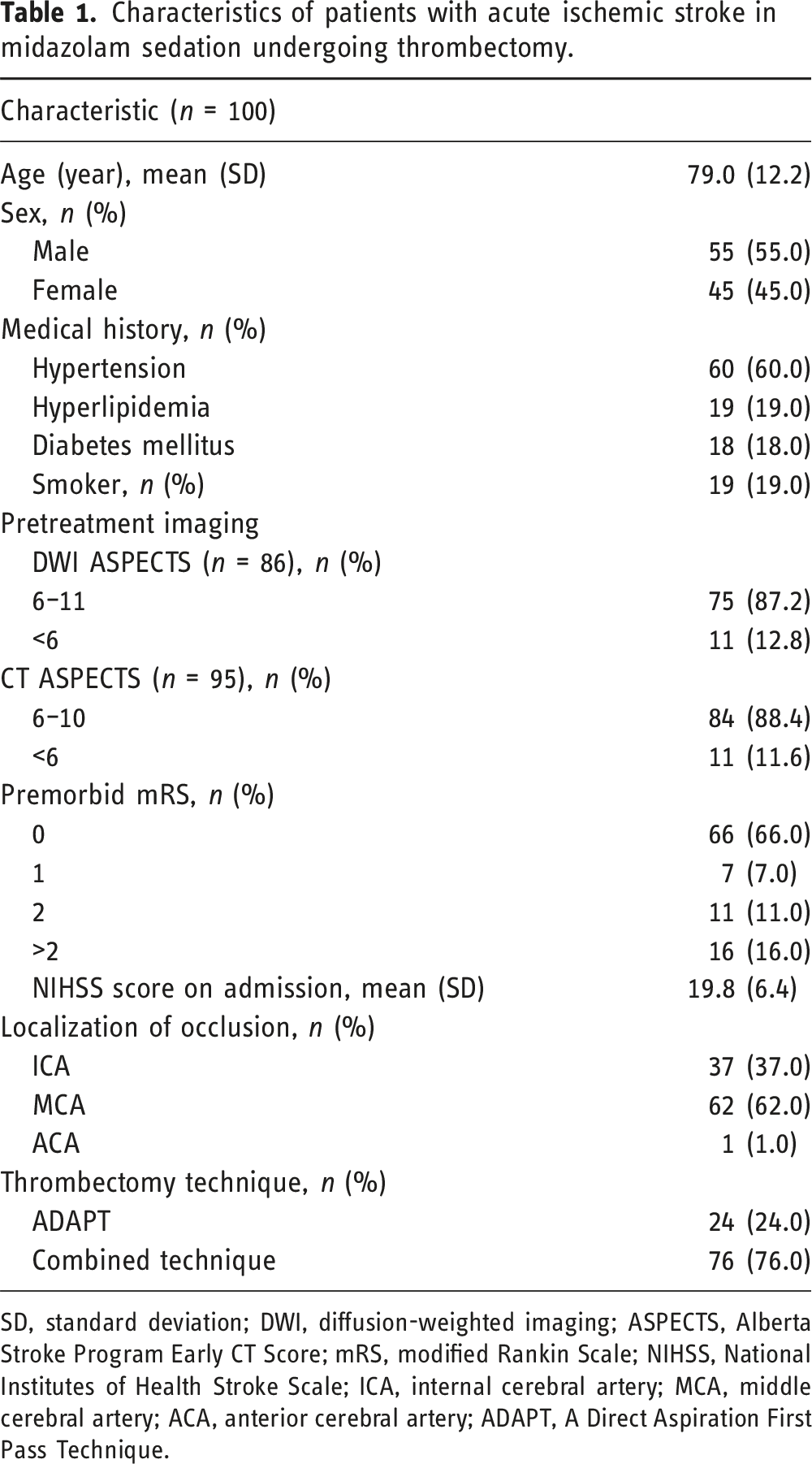
SD, standard deviation; DWI, diffusion-weighted imaging; ASPECTS, Alberta Stroke Program Early CT Score; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; ICA, internal cerebral artery; MCA, middle cerebral artery; ACA, anterior cerebral artery; ADAPT, A Direct Aspiration First Pass Technique.
Outcomes
Outcomes of midazolam sedation in acute ischemic stroke patients undergoing thrombectomy.
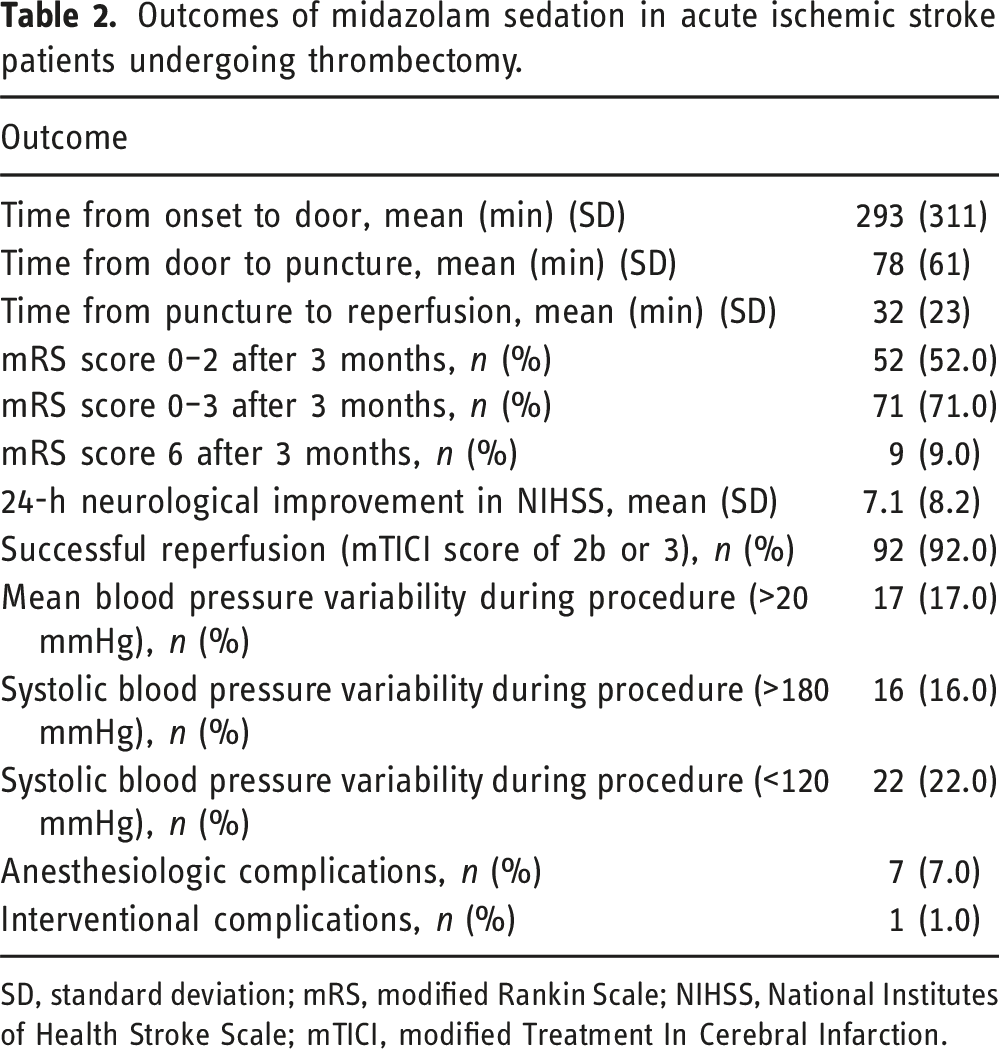
SD, standard deviation; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; mTICI, modified Treatment In Cerebral Infarction.
Discussion
Comparison of outcomes following thrombectomy for acute ischemic stroke between this study and previous studies.
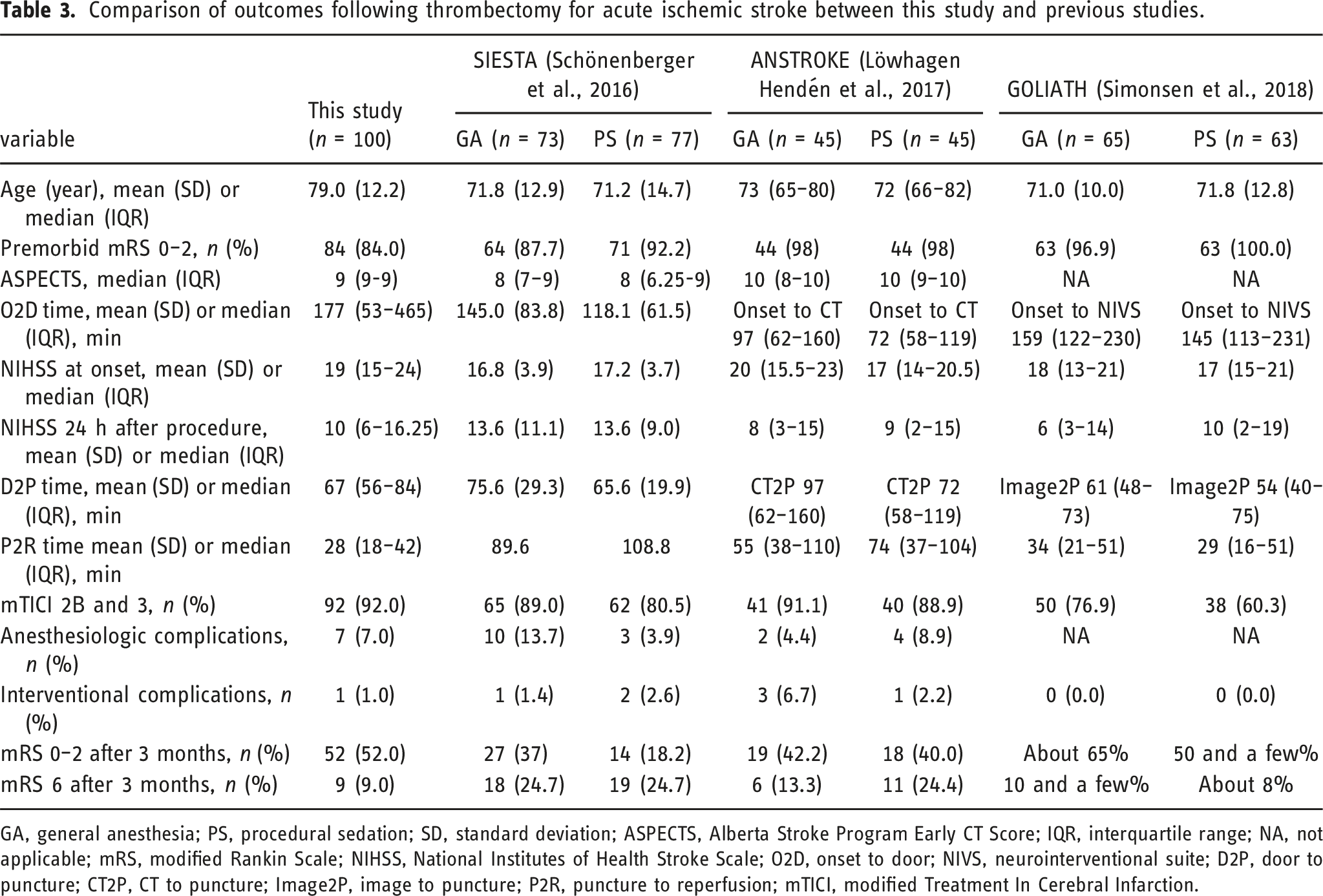
GA, general anesthesia; PS, procedural sedation; SD, standard deviation; ASPECTS, Alberta Stroke Program Early CT Score; IQR, interquartile range; NA, not applicable; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; O2D, onset to door; NIVS, neurointerventional suite; D2P, door to puncture; CT2P, CT to puncture; Image2P, image to puncture; P2R, puncture to reperfusion; mTICI, modified Treatment In Cerebral Infarction.
In terms of treatment outcomes, the favorable recovery rate of mTICI 2B or higher was 92.0%, which was equal to or better than the 76.9%–89.0% recovery rate of mTICI 2B or higher in the general anesthesia group in previous reports, which is expected to have a favorable recovery due to less body movement. The favorable recovery rate in this study is thought to be due to the effective sedation by midazolam, the minimal patient body movement, and the procedure being performed under favorable conditions. However, 52.0% of the cases achieved a favorable outcome of mRS 0–2 at 3 months after surgery, which is similar to the previous results of 18.2%–65%. The favorable outcome, despite the subjects being relatively old with a relatively poor preoperative mRS in our study, is thought to be due to the favorable recovery rate. In a previous report comparing general anesthesia with procedural sedation, the improvement in the NIHSS score after 24 h was not statistically significant but tended to be better under general anesthesia. 9 This may be due to the brain-protecting effect of the anesthetics used in general anesthesia, which reduces the demand for oxygen consumption in the brain.4,8 Midazolam, a benzodiazepine drug that was also used as a sedative in this study, has been reported to reduce cerebral oxygen metabolism 4 and increase cerebral ischemic resistance by reducing cerebral vascular resistance and ensuring cerebral blood flow. 5 Our patients achieved the same level of improvement in NIHSS as previous subjects who underwent thrombectomy under general anesthesia.
From a time perspective, the median time from arrival at the hospital to puncture was 67 min at our hospital, whereas the median time in previous reports on light sedation groups was 54–72 min, giving the impression that it took a little longer to puncture. At our hospital, the CT or MRI room is directly connected to the emergency arrival point; therefore, the time from hospital arrival to image acquisition is short. This suggests that the time required for the puncture was due to the large number of MRI sequences. In cases where acute cerebral infarction was diagnosed based on CT alone and puncture was performed, there was no significant difference in the average time from previous reports. In the future, in cases where thrombectomy is clearly indicated, such as in cases of hemiplegia in patients with atrial fibrillation, MRI examinations should be skipped or MRI should be performed with a specific sequence. Notably, the median time from puncture to recanalization in our hospital was 28 min, which is shorter than the 29–74 min in previous studies performed under general anesthesia. This is thought to be because there was little body movement due to the good sedation provided by midazolam and that our staff is well-versed in thrombectomy techniques due to the large number of cases of acute cerebral infarction in our hospital.
From the viewpoint of safety, there were seven cases of postoperative pneumonia (7.0%), which is lower than the 3.9%–13.7% reported in previous studies. Aspiration pneumonia due to oversedation with midazolam is a complication that may be feared but may occur less frequently than expected. Another important point is that when performing endovascular cerebrovascular surgery under procedural sedation, the patient may become restless or transition to general anesthesia due to the worsening of neurological symptoms during the procedure. 19 However, at our institution, all procedures were completed under procedural sedation using midazolam, except for five cases in which the patient was forced to transition to general anesthesia because of direct cervical artery puncture due to severe vascular tortuosity. Regarding interventional complications, our hospital was able to perform using a microguidewire in one case (1.0%). This is comparable to the 0%–6.7% reported in previous studies. Furthermore, the 3-month mortality rate was 9% in this study, while other studies have comparable or higher mortality rates of 8%–24.7%. Thus, thrombectomy using midazolam is considered safe.
This study has some limitations. First, this was a single-center study. Future multicenter studies are necessary to demonstrate the efficacy and safety of thrombectomy under midazolam sedation.
Second, this study did not have a comparative participant group for analysis. Although thrombectomy under midazolam sedation was performed in all cases at our institution, a randomized controlled trial must be conducted to demonstrate its efficacy and observe statistically significant differences. Further verification is required to demonstrate midazolam’s efficacy and safety using a comparative population. Finally, this is a retrospective study. Future prospective studies are needed to clarify the efficacy of thrombectomy under procedural sedation with midazolam.
Conclusion
Thrombectomy using midazolam sedation is highly safe and effective with few complications, as well as shortens the time from puncture to recanalization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Informed consent
Informed consent from each of the eligible patients was substituted by the opt-out method.
Data Availability Statement
All supporting data are available from the corresponding author according to reasonable request.