
Abstract
Introduction
Differentiating ring-enhancing primary central nervous system lymphoma (PCNSL) from infections is critical yet challenging in clinical practice. This study aimed to evaluate the effectiveness of diffusion-weighted imaging (DWI) and susceptibility-weighted imaging (SWI) in differentiating ring-enhancing PCNSL from infections.
Material and Methods
We retrospectively reviewed 78 ring-enhancing lesions in 32 patients who underwent brain magnetic resonance imaging (MRI). Qualitative and quantitative assessments of the peripheral and central regions of ring-enhancing lesions were independently performed. The qualitative assessment involved evaluating restricted diffusion on DWI and intralesional susceptibility signal (ISS) on SWI. The quantitative assessment involved comparing the apparent diffusion coefficient average (ADCavg) ratio and apparent diffusion coefficient minimum (ADCmin) ratio of the peripheral and central regions with the final diagnosis.
Results
The lesions consisted of PCNSL (n = 21), tuberculosis (n = 17), and toxoplasmosis (n = 40). The qualitative assessment showed that diffusion was significantly more restricted at the periphery in PCNSL (p < .001) and that ISS positivity was significantly higher both peripherally (p < .001) and centrally (p = .001) in PCNSL than in infections. The quantitative assessment revealed that PCNSL had significantly lower ADCavg (peripheral, p < .001; central, p = .01) and ADCmin ratios (peripheral, p < .001; central, p = .025) compared to infections. A peripheral ADCavg ratio of <1.25 demonstrated the best diagnostic accuracy (area under the curve: 0.966, 95% confidence interval [CI]: 0.93–1.00, sensitivity: 85.7%, specificity: 89.5%, and accuracy: 88.5%) for differentiating PCNSL from infections.
Conclusion
Restricted diffusion on DWI, positive ISS on SWI, and ADC ratio measurements of ring-enhancing lesions demonstrate significant potential as adjunctive imaging features for distinguishing PCNSL from CNS infections.
Keywords
Introduction
Primary central nervous system lymphoma (PCNSL) is a hematologic malignancy with an annual incidence rate of seven cases per 1,000,000 people in the United States. 1 A significant risk factor for PCNSL is immunodeficiency, including human immunodeficiency virus (HIV) infection. 2 Early diagnosis and treatment improve survival rates and reduce sequelae, particularly when tumors are detected through imaging. 3 In immunocompetent patients, PCNSL typically appears on magnetic resonance imaging (MRI) as a solitary lesion with homogeneous enhancement in 90% of cases, most commonly located centrally within the cerebral hemisphere, periventricular white matter, or superficially adjacent to the meninges. 4 Conversely, the MRI appearance of PCNSL in immunocompromised hosts reveals a higher frequency of multiple lesions 5 with irregular or peripheral ring-like enhancement due to central necrosis.6,7 Although PCNSL may exhibit characteristic imaging findings on traditional computed tomography (CT) and MRI, none of these is sufficient to unequivocally differentiate PCNSL from other brain lesions. 8
Ring-enhancing lesions on conventional MRI sequences have a wide differential diagnosis, ranging from infectious processes to high-grade necrotic neoplasms. 9 PCNSL commonly presents a ring-enhancing pattern in approximately 75% of patients with Acquired Immunodeficiency Syndrome (AIDS) 8 and 29% of patients with immunodeficiency-associated central nervous system (CNS) lymphomas, such as post-transplant patients. 10 In immunocompromised patients, the common differential diagnoses for ring-enhancing CNS lesions include toxoplasmosis and tuberculosis. Distinguishing between PCNSL and opportunistic CNS infections is challenging, often leading to empirical treatment for infections. If the lesions resolve or decrease in size after treatment, they are presumed to be infectious, and therapy is continued until they resolve completely. However, if the subsequent clinical and radiographic responses are progressive or unsatisfactory, a diagnosis of PCNSL is favored, and a biopsy is recommended. These issues are crucial for ensuring accurate pre-therapeutic diagnosis, enabling prompt biopsy and specific therapy for patients with PCNSL, or avoiding unnecessary biopsies in patients with infection.
Diffusion-weighted imaging (DWI) is an MRI sequence used to measure the diffusion of water molecules in biological tissues. The apparent diffusion coefficient (ADC) is a quantitative value that describes the microscopic water diffusibility within tissues. The ADC, obtained from DWI using different degrees of diffusion weighting (b-values), is depicted on an ADC map, enabling measurement in the region of interest (ROI). Regions with more restricted diffusion show lower ADC values.11,12
Previous studies have shown restricted diffusion within lymphomatous lesions and bacterial abscesses in the brain, 6 but few studies have evaluated the diffusion characteristics of toxoplasmosis lesions. In PCNSL, restricted diffusion is thought to result from high cellularity, whereas toxoplasmosis lesions often demonstrate higher ADC values owing to necrosis and inflammatory changes that permit freer water movement. A previous study analyzed 21 patients, comparing ADC ratios of 13 toxoplasmosis and eight lymphoma lesions using ROI in the non-enhancing core of each lesion and the contralateral normal-appearing white matter. ADC ratios >1.6 were associated solely with toxoplasmosis, suggesting that the ADC ratio could aid in distinguishing between the conditions. 13 However, other studies have shown significant overlap in ADC ratios between toxoplasmosis and PCNSL, with variability even among different lesions in the same patient. 14 Therefore, the effectiveness of using ADC ratios to differentiate PCNSL from toxoplasmosis remains controversial.
Susceptibility-weighted imaging (SWI) utilizes blood oxygenation level-dependent principles to detect susceptibility effects via the paramagnetic properties of hemorrhage, venous blood, and physiological iron, as well as to identify calcium. SWI has been proven to be much more sensitive than CT or conventional gradient echo (GRE) T2* in detecting cerebral hemorrhage.15,16 Recent studies have identified abnormal SWI foci in most patients with neurotoxoplasmosis, which are presumably attributable to hemorrhage. 15 Conversely, microhemorrhage and calcification are rare in PCNSL. 8 Therefore, using the SWI sequence to differentiate these conditions may be beneficial.
This study aimed to 1) characterize DWI and SWI findings in ring-enhancing PCNSL and opportunistic infections and 2) differentiate between ring-enhancing PCNSL and opportunistic infections using DWI and SWI.
Materials and methods
The institutional review board approved this study (IRB number 472/62), which waived the requirement for obtaining informed consent owing to the retrospective nature of the study.
Patients
The retrospective data used in the analysis were obtained from electronic medical records and picture archiving and communication systems (PACS) recorded between June 2010 and June 2019. The inclusion criteria were: 1) pretreatment contrast-enhanced MRI of the brain, including DWI, ADC, and/or SWI sequences, with ring-enhancing lesions larger than 0.5 cm in diameter on post-contrast-enhanced sequences and 2) a final diagnosis of PCNSL confirmed via histopathology, toxoplasmosis indicated by positive serum Toxoplasma gondii antibodies, or tuberculosis confirmed via positive acid-fast bacilli from the cerebrospinal fluid, positive polymerase chain reaction (PCR) for tuberculosis, or favorable treatment response to anti-tuberculosis drugs after 2 months. 17 A ring-enhancing lesion is defined as a lesion with a rim of enhancement surrounding a non-enhancing portion on post-contrast-enhanced MRI.
The exclusion criteria included 1) post-biopsy lesions, 2) previously treated lesions, and 3) poor image quality.
MRI protocol and imaging analysis
MRI protocol
MRI scans, including routine multiplanar brain scans, were performed using 1.5-T and 3-T MRI scanners (Philips Ingenia [1.5 T] and Philips Ingenia [3 T]), both with a maximum gradient strength of 45 mT/m and using a 15-channel head coil. DWI and SWI, which are standard components of conventional brain MRI protocols, were conducted before administrating gadolinium-based contrast medium. DWI was performed in the axial plane using a spin-echo echo-planar imaging sequence with diffusion-gradient encoding in three orthogonal directions. The DWI parameters for 1.5 T were as follows: repetition time/echo time (TR/TE): 4217/76 ms; matrix: 144 × 134; field of view: 230 × 253 mm2; slice thickness: 5 mm; bandwidth 946 Hz/pixel; and b-values, 0 and 1000 s/mm2. The DWI parameters for 3 T were as follows: TR/TE: 5177/73 ms; matrix: 144 × 134; field of view: 230 × 253 mm2; slice thickness: 5 mm; bandwidth, 1731.6 Hz/pixel; and b-values, 0 and 1000 s/mm2. ADC maps were obtained by pixel-by-pixel calculations using the formula ADC = - [ln(Sb/S0)]/b, where b is the gradient b-factor (1000 s/mm2), Sb is the signal with b = 1000 s/mm2, and S0 is the signal without a diffusion-sensitizing gradient. SWI was performed on the 3-T scanner using an axial 3D multi-echo T2*-weighted gradient echo sequence with the following parameters: TR/TE1/deltaTE: 28/5.8/6.1 ms; number of echoes: 6; matrix: 360 x 296; field of view: 230 × 253 mm2; slice thickness: 2.5 mm; and bandwidth, 255.3 Hz/pixel.
Imaging analysis
All data were interpreted by two observers: 1) a neuroradiologist with 9 years of experience and 2) a radiology resident.
For qualitative assessment using both DWI and SWI sequences, the observers, blinded to clinical history, laboratory tests, and histopathological information, independently evaluated findings of restricted diffusion on DWI and intralesional susceptibility signal (ISS) of hemorrhage on SWI. The restricted diffusion lesion was defined as a lesion with high signal intensity on DWI and low ADC values. 18 The ISS was defined as a blooming signal within the lesion on SWI, 15 which could either be a vascular or dotted pattern. The vascular pattern is characterized by linear or tubular hypointensities, often continuous or streak-like, corresponding to blood vessels. The dotted pattern comprises small, discrete hypointense foci, indicative of microhemorrhages or small blood products. For each lesion, two locations were evaluated: 1) the central non-enhancing region and 2) the peripheral ring-enhancing region. Lesions were classified as either positive or negative for ISS. Any discrepancies in evaluations were resolved by consensus.
For quantitative assessment using only DWI sequence with ADC maps, the observers independently measured the ADC values of the ring-enhancing lesions. For each lesion, the ROIs were manually placed in two locations on a single slice that best represented the lesion’s features: 1) the central non-enhancing region and 2) the peripheral ring-enhancing region. For each location, the ROIs were delineated using two methods: 1) placing a freehand ROI surrounding the entire region to measure the average ADC value (ADCavg) and 2) placing a 5-mm2 ROI at the visually identified most hypointense region (indicating the most restricted water diffusion) to measure the minimum ADC value (ADCmin). Figure 1 shows a representative PCNSL case with four ROIs. The average ADC value from two independent observers was used to determine the ADC ratio. The ADC ratio was calculated as the ratio of the ADC value from the measured ROI to the ADC value from the contralateral normal-appearing brain. The contralateral ROI was matched in size and anatomical location, carefully avoiding any visible abnormalities and artifacts. The ADCavg and ADCmin ratios in both regions were analyzed for the final diagnosis. A 25-year-old male patient with HIV-related PCNSL. Axial contrast-enhanced T1-weighted imaging (A) shows a ring-enhancing lesion in the left basal ganglia (white arrow). Axial DWI (B) shows peripheral restricted diffusion (ADCavg ratio = 1.23, ADCmin ratio = 0.98) and no central restricted diffusion (ADCavg ratio = 1.74, ADCmin ratio = 1.00) (white arrow). Axial ADC maps (C-E) show regions of interest (ROIs) to measure ADCavg of the entire central non-enhancing region (C), ADCavg of the entire peripheral ring-enhancing region (D), ADCmin at the most restricted diffusion area of the central non-enhancing region and ADCmin at the most restricted diffusion area of the peripheral ring-enhancing region (E), and axial SWI shows positive intralesional susceptibility signal at peripheral ring-enhancing and central non-enhancing regions (white arrow) (F). PCNSL = primary central nervous system lymphoma; DWI = diffusion-weighted imaging; SWI = susceptibility-weighted imaging; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.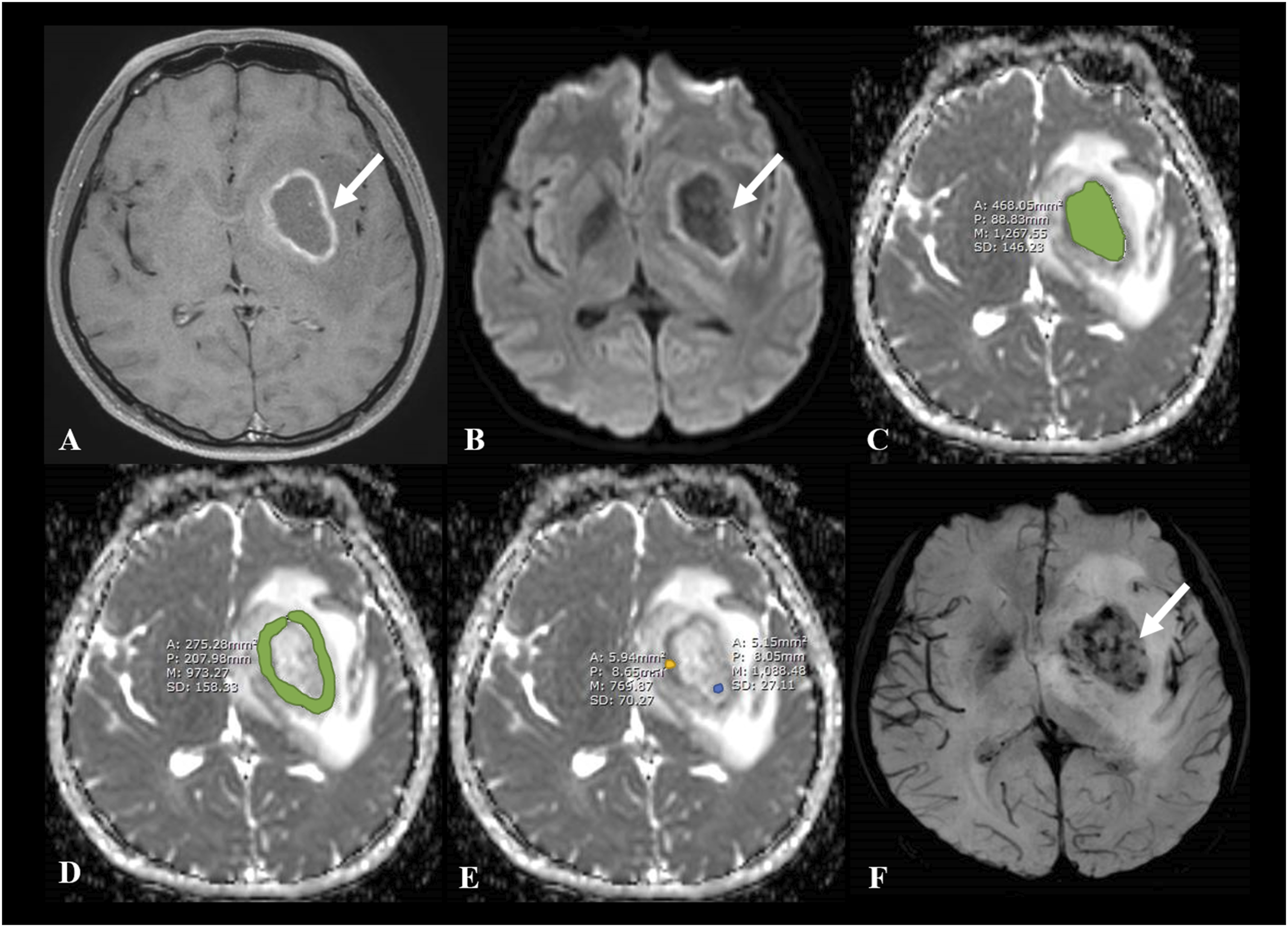
Statistical analysis
The Shapiro-Wilk test was applied to assess whether the data followed a normal distribution. The ADC ratios of PCNSL and infections were analyzed using an independent sample t-test. A subgroup analysis of ADC ratios among PCNSL, tuberculosis, and toxoplasmosis was conducted using one-way analysis of variance (ANOVA) with a post hoc test. A p-value of less than 0.05 was considered statistically significant. Diagnostic performance was assessed using the area under the curve (AUC) and receiver operating characteristic (ROC) curve analysis. The Youden index was used to determine the optimal cut-off point for maximum sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) for differentiating PCNSL from infections. The intraclass correlation coefficient (ICC) was used to assess inter-observer reliability. All statistical analyses were performed using SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA).
Results
Demographic data
We recruited 46 patients with ring-enhancing lesions who underwent brain MRI and were diagnosed with PCNSL, tuberculosis, or toxoplasmosis. 14 patients were excluded due to poor quality images (n = 6), lack of laboratory confirmation of toxoplasmosis or tuberculosis (n = 4), a history of PCNSL without current disease, and loss to follow-up (n = 1), a diagnosis of secondary CNS lymphoma (n = 2), and post-treatment imaging of toxoplasmosis (n = 1). The recruitment flow chart is presented in Figure 2. Recruitment flow chart. MRI = Magnetic resonance imaging; PCNSL = primary central nervous system lymphoma; CNS = central nervous system.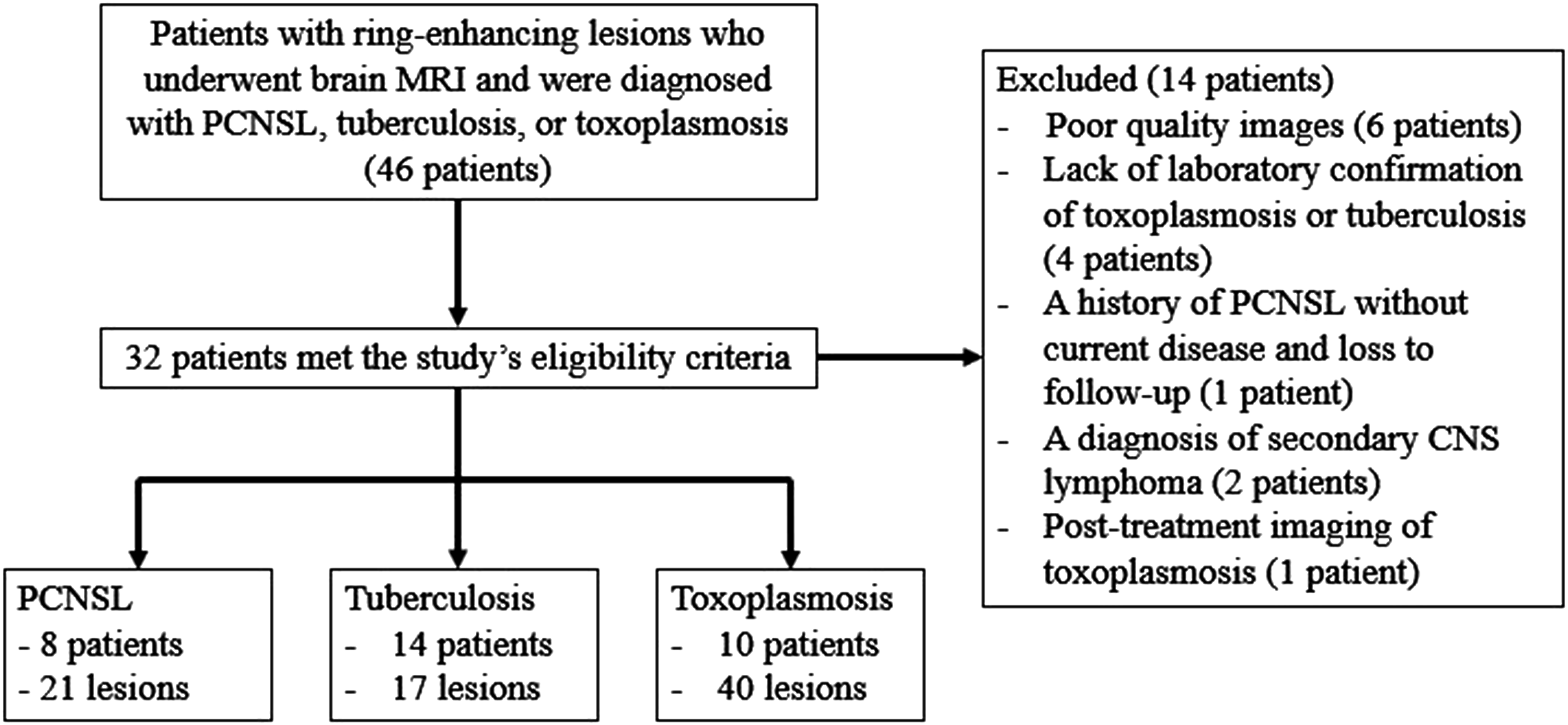
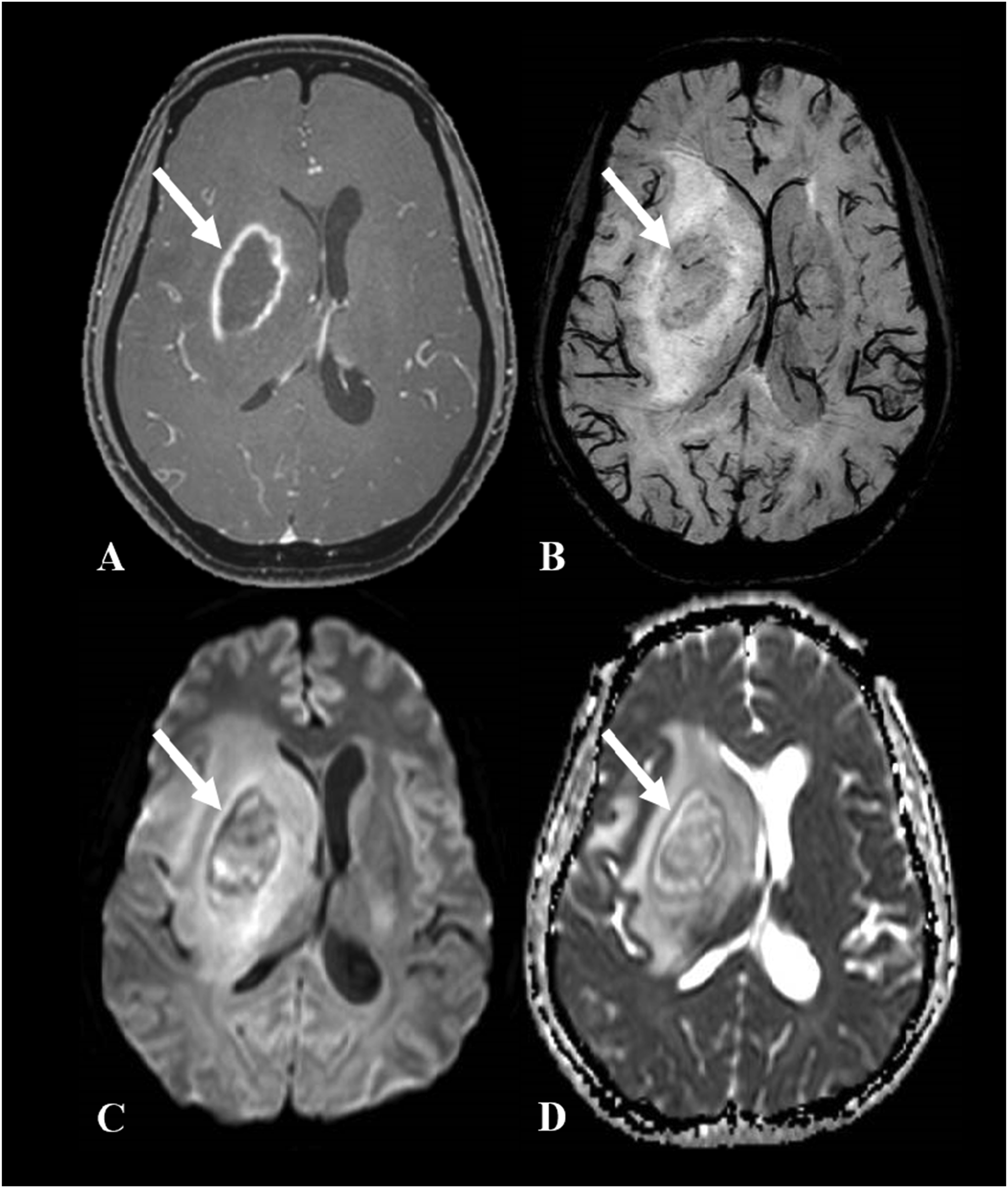
Data were collected from 32 patients with a total of 78 ring-enhancing lesions. Of these, 23 patients were immunocompromised, all with HIV infection, and nine patients were immunocompetent. This study included 22 males and 10 females. Among the eight patients with PCNSL, five were HIV-positive, and three were HIV-negative. Among the 14 patients with tuberculosis, eight were HIV-positive, and six were HIV-negative. All 10 patients with toxoplasmosis were HIV-positive. The mean age of the patients with PCNSL was 41 years (range: 25–63 years), whereas that of the patients with infections was 35 years (range: 17–56 years). Three patients with PCNSL and three patients with tuberculoma had a single brain lesion, while five patients with PCNSL, 11 patients with tuberculoma, and all 10 patients with toxoplasmosis had multiple lesions. The lesions consisted of 21 PCNSL and 57 infection-related lesions (tuberculosis: [n = 17]; toxoplasmosis: [n = 40]). Diagnoses were confirmed via histopathological examination in 14 patients (43.8%; 8 with diffuse large B-cell lymphoma and 6 with tuberculosis), positive PCR for tuberculosis in five patients, negative PCR for tuberculosis but favorable treatment response in four patients, and positive serum Toxoplasma gondii antibodies with favorable treatment response in 10 patients (42.9%). Figures 3 and 4 show the representative cases of infections. In total, 26 patients were scanned using a 3-T scanner, while the remaining 6 subjects were imaged on a 1.5-T scanner. Among the patients, 6 with PCNSL and 20 patients with infections were imaged using the 3-T scanner. DWI and ADC maps were obtained for all patients across both systems. SWI was performed exclusively on the 3-T scanner and was therefore available for 26 of 32 patients, corresponding to 64 of 78 lesions. A 26-year-old male patient with tuberculosis (A-D). Axial contrast-enhanced T1-weighted imaging (A) shows a smooth ring-enhancing lesion in the left lentiform nucleus (white arrow). Axial SWI (B) shows a negative intralesional susceptibility signal at both central and peripheral regions (white arrow). Axial DWI (C) and ADC map (D) show no restricted diffusion at both central (ADCavg ratio = 2.51, ADCmin ratio = 2.15) and peripheral regions (ADCavg ratio = 1.68, ADCmin ratio = 1.62) (white arrow). DWI = diffusion-weighted imaging; SWI = susceptibility-weighted imaging; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC. A 42-year-old female patient with toxoplasmosis (A-D). Axial contrast-enhanced T1-weighted imaging (A) shows a ring-enhancing lesion in the right basal ganglia. Axial SWI (B) shows positive intralesional susceptibility signals at the central non-enhancing region. Axial DWI (C) and ADC map (D) show no restricted diffusion at the peripheral ring-enhancing region (ADCavg ratio = 1.38, ADCmin ratio = 0.96) but at the central region (ADCavg ratio = 1.73, ADCmin ratio = 1.46). DWI = diffusion-weighted imaging; SWI = susceptibility-weighted imaging; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.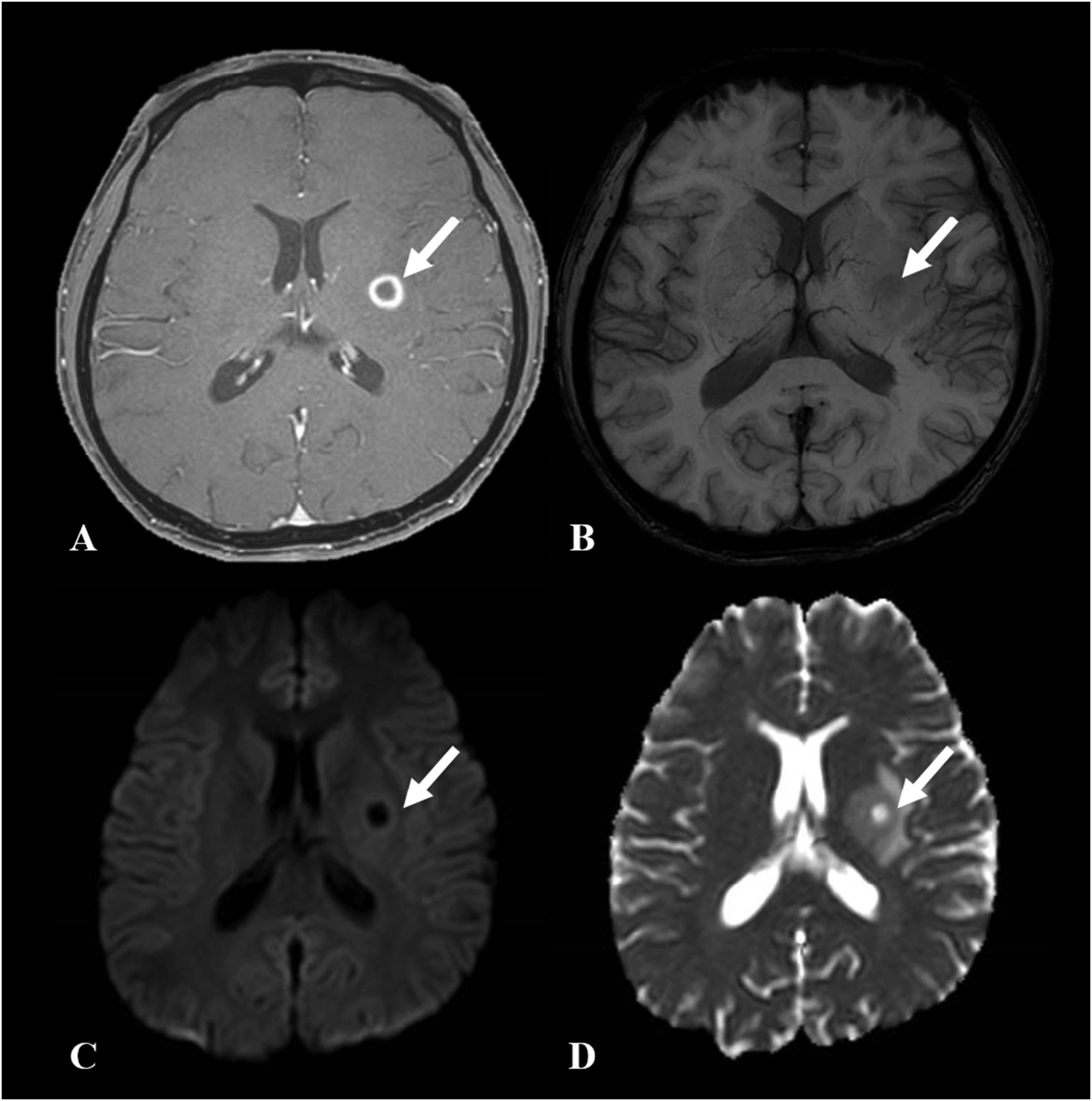
Results of qualitative assessment
Qualitative assessment of PCNSL and infection.
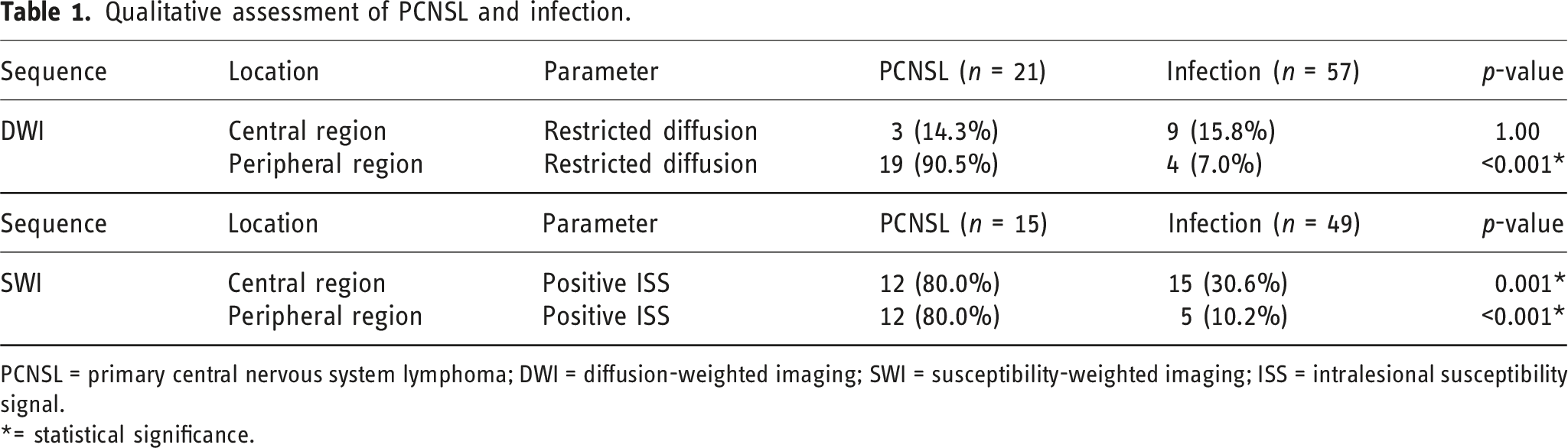
PCNSL = primary central nervous system lymphoma; DWI = diffusion-weighted imaging; SWI = susceptibility-weighted imaging; ISS = intralesional susceptibility signal.
*= statistical significance.
In the subgroup analysis, central restricted diffusion was observed in three PCNSL (14.3%), five tuberculosis (29.4%), and four toxoplasmosis (10.0%) lesions. Peripheral restricted diffusion was observed in 19 PCNSL (90.5%), two tuberculosis (11.8%), and two toxoplasmosis (5.0%) lesions. PCNSL lesions exhibited significantly more peripheral restricted diffusion than did tuberculosis (p < .001) and toxoplasmosis (p < .001) lesions. However, no significant difference in central restricted diffusion was found between PCNSL and tuberculosis (p = .43), PCNSL and toxoplasmosis (p = .68), or tuberculosis and toxoplasmosis (p = .11).
The results of the positive ISS parameter on the SWI sequence showed that the PCNSL exhibited significantly higher positive ISS in the central (p = .00) and peripheral regions (p < .001) than did infections.
In the subgroup analysis, positive ISS in the central region was observed in 12 PCNSL (80.0%), two tuberculosis (12.5%), and 13 toxoplasmosis (39.4%) lesions. In the peripheral region, positive ISS was noted in 12 PCNSL (80.0%), two tuberculosis (12.5%), and three toxoplasmosis (9.1%) lesions. PCNSL lesions demonstrated significantly more positive ISS in the central and peripheral regions than did tuberculosis (central: p < .001; peripheral: p < .001) and toxoplasmosis (central: p = .01; peripheral: p < .001). No significant differences in positive ISS were observed between tuberculosis and toxoplasmosis in the central (p = .10) or peripheral (p = 1.00) regions.
Results of quantitative assessment
ADC ratios of PCNSL and infection.
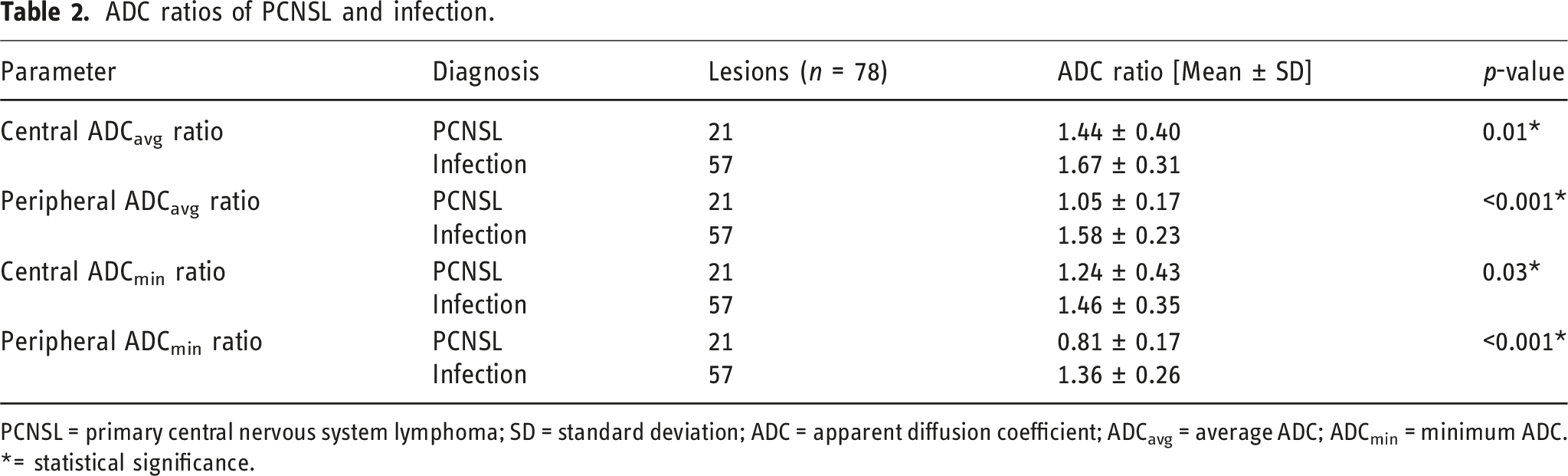
PCNSL = primary central nervous system lymphoma; SD = standard deviation; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.
*= statistical significance.
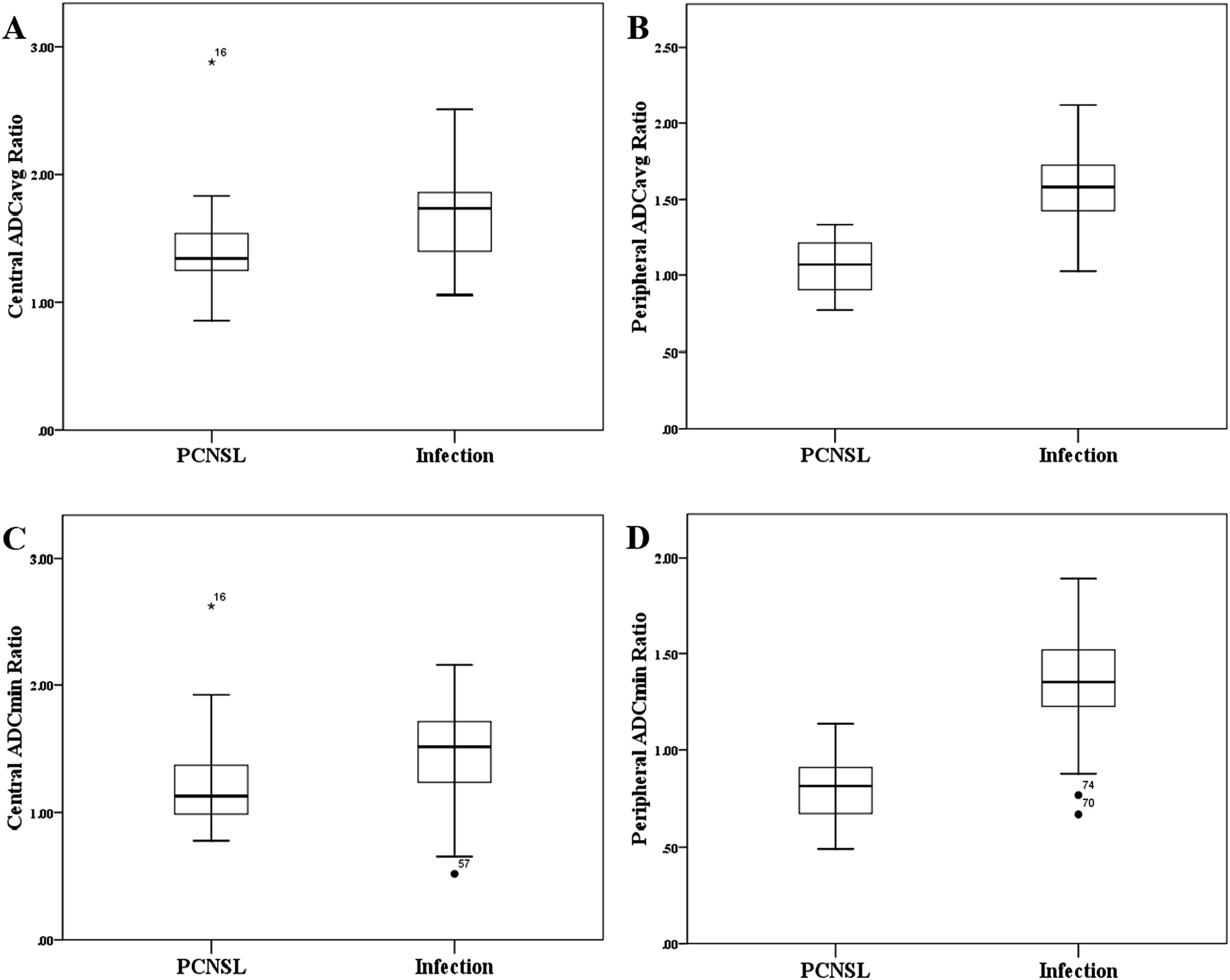
Box and whisker plots of ADC ratios of PCNSL and infections. (A) ADCavg ratio of the central non-enhancing region, (B) ADCavg ratio of the peripheral ring-enhancing region, (C) ADCmin ratio of the central non-enhancing region, and (D) ADCmin ratio of the peripheral ring-enhancing region. * = Statistical significance, N.S. = not statistical significance. PCNSL = primary central nervous system lymphoma; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.
ADC ratios of PCNSL, tuberculosis, and toxoplasmosis.
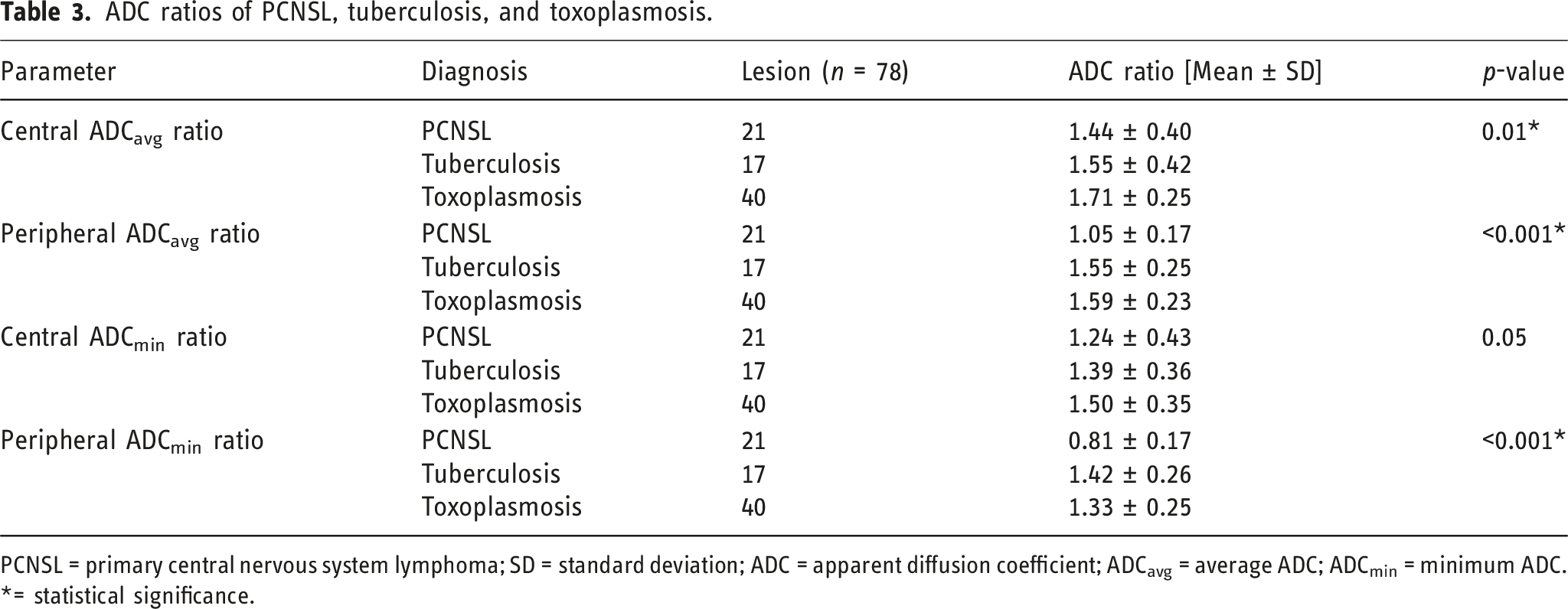
PCNSL = primary central nervous system lymphoma; SD = standard deviation; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.
*= statistical significance.
In the peripheral ring-enhancing region, PCNSL showed significantly lower ADC ratios than did tuberculosis (ADCavg and ADCmin ratios: p < .001) and toxoplasmosis (ADCavg and ADCmin ratios: p < .001). No significant differences in peripheral ADCavg and ADCmin ratios were observed between tuberculosis (p = .54) and toxoplasmosis (p = .22).
In the central non-enhancing region, PCNSL demonstrated significantly lower ADC ratios than did toxoplasmosis (central ADCavg ratio: p = .00; central ADCmin ratio: p = .02). No significant differences were observed in central ADCavg and ADCmin ratios between PCNSL and tuberculosis (central ADCavg ratio: p = .30; central ADCmin ratio: p = .24) or between tuberculosis and toxoplasmosis (central ADCavg ratio: p = .10; central ADCmin ratio: p = .33). Figure 6 displays the box and whisker plots of these ADC ratios. Box and whisker plots of ADC ratios in PCNSL, tuberculosis, and toxoplasmosis. (A) ADCavg ratio of the peripheral ring-enhancing region, (B) ADCmin ratio of the peripheral ring-enhancing region, (C) ADCavg ratio of the central non-enhancing region, and (D) ADCmin ratio of the peripheral ring-enhancing region. * = Statistical significance, N.S. = not statistical significance. PCNSL = primary central nervous system lymphoma; ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC.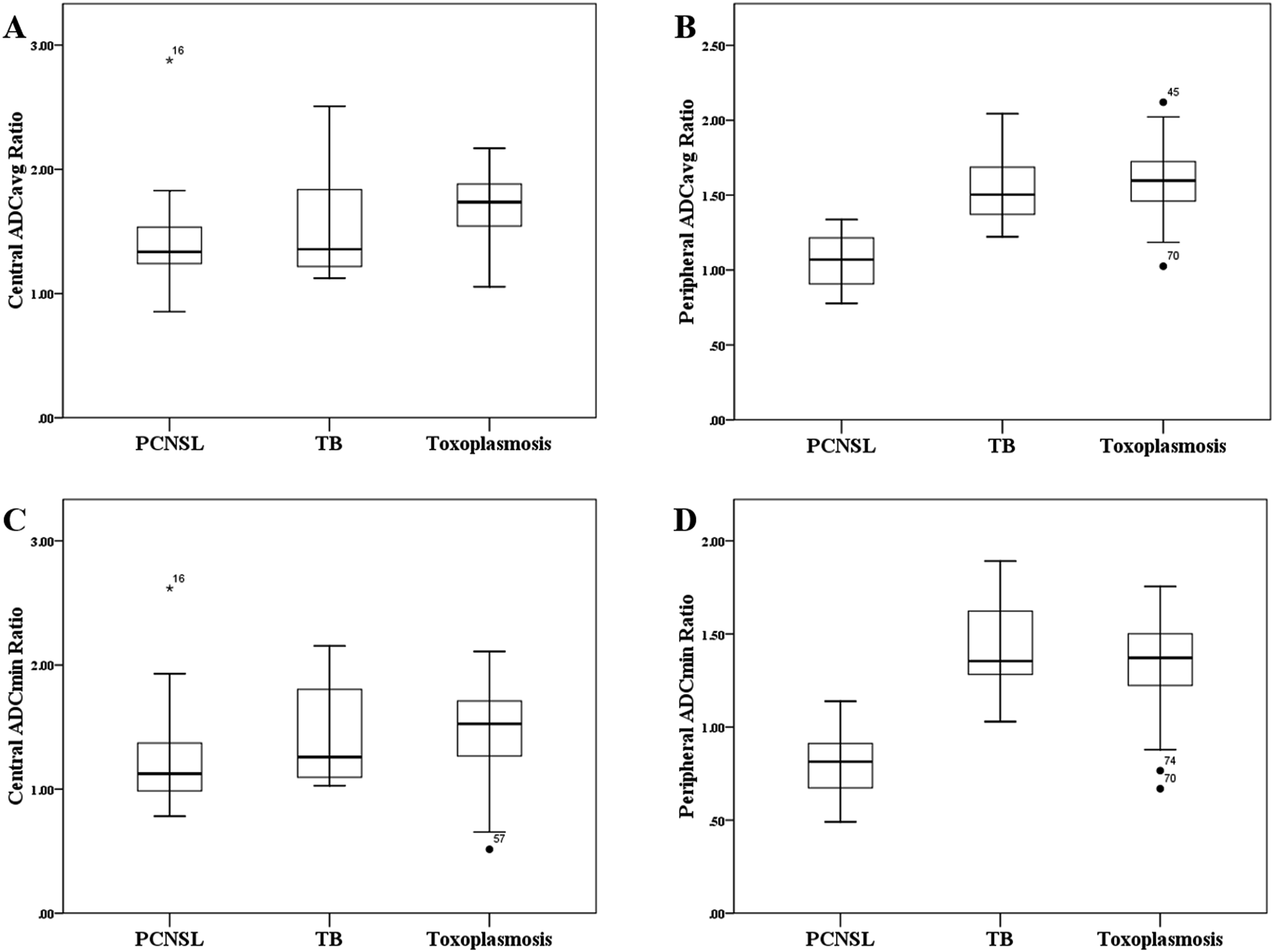
Using the Youden index to determine the optimal ADC ratio parameter for differentiating ring-enhancing PCNSL from infections, the diagnostic performance of the peripheral ADC ratios was evaluated. The AUC of the ROC analysis of the peripheral ADCavg ratios was 0.966 (95% confidence interval [CI]: 0.93–1.00), and that of the peripheral ADCmin ratios was 0.951 (95%CI: 0.91–0.99). The diagnostic performance of the central ADCavg ratio was also evaluated, showing an AUC of 0.734 (95%CI: 0.61–0.86) (Figure 7). When evaluating peripheral ADCavg, peripheral ADCmin, and central ADCavg ratios as the best three parameters for differentiating PCNSL from infections, the following cut-off points and diagnostic metrics were identified: peripheral ADCavg ratio <1.25 (sensitivity 85.7%, specificity 89.5%, accuracy 88.5%, PPV 75%, and NPV 94.4%); peripheral ADCmin ratio <1.00 (sensitivity 85.7%, specificity 91.2%, accuracy 89.7%, PPV 78.3%, and NPV 94.5%); and central ADCavg ratio <1.45 (sensitivity 66.7%, specificity 71.9%, accuracy 70.5%, PPV 46.7%, and NPV 85.4%). Table 4 shows a comparison of the diagnostic performance of these ADC ratios in the peripheral enhancing region. Receiver operating characteristic curve for differentiating PCNSL from infection. The area under the curve (AUC) of ADCavg ratio of the peripheral ring-enhancing region has the best diagnostic performance with an AUC of 0.966 (95%CI: 0.932–1.000). PCNSL = primary central nervous system lymphoma; ADC = apparent diffusion coefficient; ADCavg = average ADC; CI = confidence interval. Comparison of the diagnostic performance of ADC ratios. ADC = apparent diffusion coefficient; ADCavg = average ADC; ADCmin = minimum ADC; AUC = area under the receiver operating characteristic curve; PPV = positive predictive value; NPV = negative predictive value.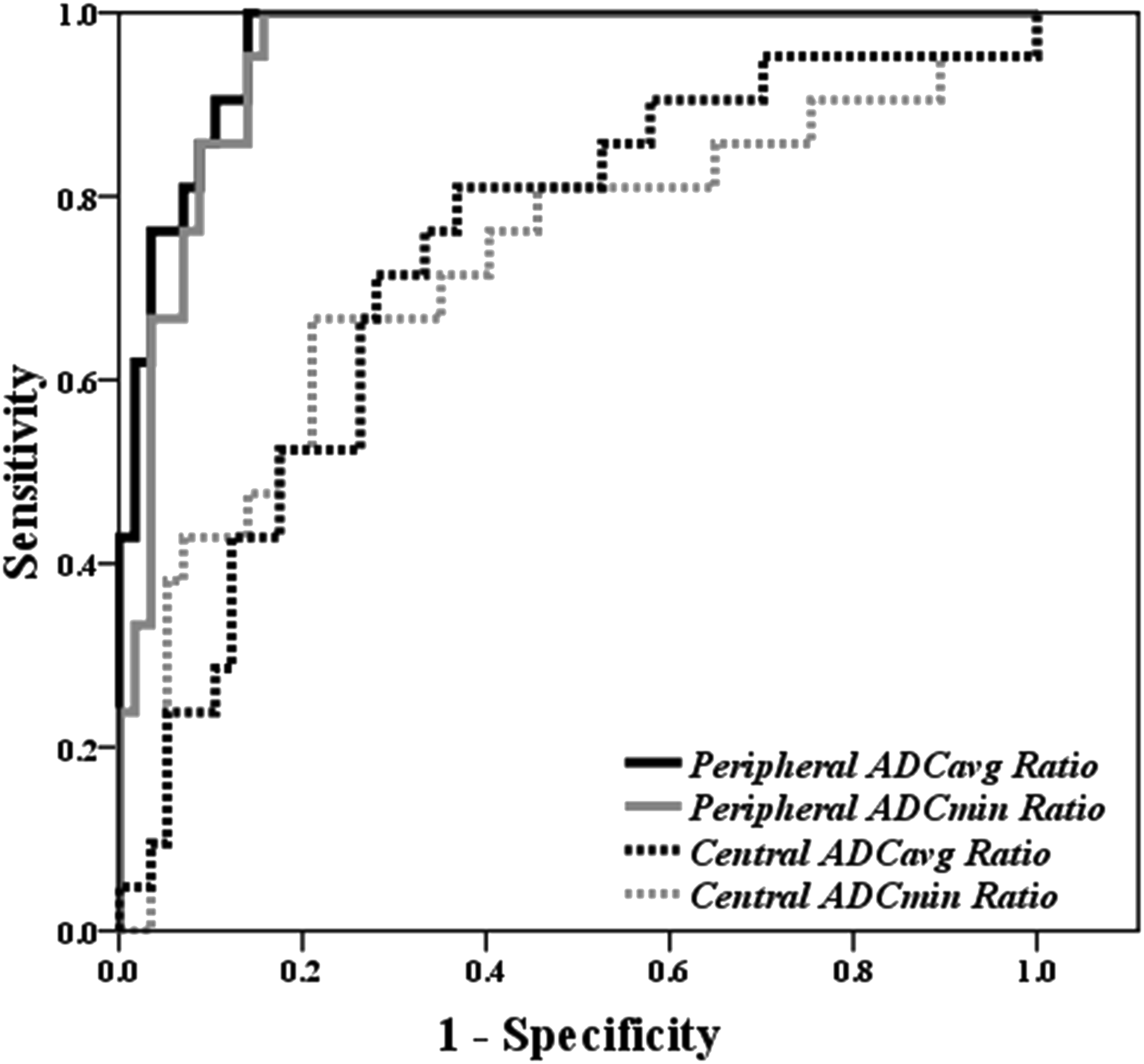

Analysis of inter-observer reliability for the ADC measurements obtained by two independent observers revealed a high degree of agreement. The ICC was estimated at 0.83, indicating a good level of reliability. ICC values below 0.5 suggest poor reliability, those in the 0.50–0.75 range indicate moderate reliability, those in the 0.75–0.90 range indicate good reliability, and values above 0.90 indicate excellent reliability. 19
Discussion
Ring-enhancing lesions are frequently observed on brain MRI and have a broad differential diagnosis. One of the key differential diagnoses is PCNSL, which can be challenging to distinguish from CNS infections such as bacterial and non-bacterial abscesses, toxoplasmosis, or fungal infections. 10 PCNSL is a hematologic malignancy that is sensitive to radiation and chemotherapy, with high-dose chemotherapy being the current first-line treatment.20,21 Conversely, tuberculosis and toxoplasmosis are treated with anti-tuberculosis drugs or multidrug regimens of anti-toxoplasmosis drugs. 22 Given the differing treatments for PCNSL and CNS infections, accurate imaging-based diagnosis of these conditions is essential.
In our study, we measured the ADC ratios in the central non-enhancing and peripheral ring-enhancing regions of each lesion. We found that PCNSL showed significantly lower ADC ratios than did infections. The three most effective parameters for differentiation were the peripheral ADCavg, peripheral ADCmin, and central ADCavg ratios. The cut-off points of peripheral ADCavg, peripheral ADCmin, and central ADCavg ratios were less than 1.25, 1.00, and 1.45, respectively, and demonstrated high specificity and accuracy in differentiating ring-enhancing PCNSL from infections.
A previous study by Camacho et al. 13 demonstrated the utility of DWI and ADC ratios in differentiating toxoplasmosis from lymphoma by analyzing ROIs in the non-enhancing core of the lesions and in the contralateral normal-appearing white matter. They found that no toxoplasmosis lesions had an ADC ratio greater than 1.6, suggesting the ADC ratio’s potential for differentiation. However, Schroeder et al. 14 used similar methods to those of Camacho et al. to compare the results and found overlapping ADC ratios for toxoplasmosis and PCNSL. They concluded that the diffusion characteristics of toxoplasmosis have a broad spectrum, making ADC ratios in the non-enhancing core of the lesions insufficient for definitive differentiation between lymphoma and toxoplasmosis.
Our results differ from those of Schroeder et al. 14 because we found a significant difference in the ADCavg ratio in the central region of the ring-enhancing lesion. However, the sensitivity and specificity of the central ADCavg ratio in differentiating between these two entities were relatively low compared with those of the peripheral ADC ratios. We also found a significant difference in restricted diffusion at the peripheral region of the ring-enhancing lesion between PCNSL and infections, supporting the use of peripheral ADC ratios for differentiating PCNSL from infections. We utilized DWI with quantitative ADC ratios because this imaging sequence is a standard sequence in most brain MRI protocols. This modality is noninvasive, rapidly performed, and easily processed, making it well-suited for clinical use.
The ring-enhancing pattern in PCNSL, which is commonly seen in patients with AIDS, is characterized by a dense cellular rim indicative of viable tumor cells with extensive central necrosis of the tumor mass.23,24 Histopathologically, the central region of PCNSL in immunocompromised patients exhibits low cellularity resulting from necrosis and may predominantly consist of fluid rather than cells. 25 Thus, restricted diffusion is often observed at the peripheral rim, leading to a relative decrease in the ADC value of the tumor.11,13
In contrast, most infectious lesions in our study, particularly toxoplasmosis lesions, showed increased diffusivity in the peripheral regions compared to the adjacent brain parenchyma, while PCNSL lesions exhibited restricted diffusion. Our study’s peripheral ADCavg and ADCmin ratios for infections were 1.58 ± 0.23 and 1.36 ± 0.26, respectively. Only approximately 6/57 (10.5%) lesions showed an ADC ratio less than 1.25 (ADCavg cut-off point), and 5/57 (8.8%) lesions had an ADC ratio less than 1.00 (ADCmin cut-off point).
Toxoplasmosis lesions in the CNS exhibit three morphologic types of pathologic lesions: necrotizing, organizing, and chronic abscesses, based on the host’s immune response. 26 Toxoplasmosis abscesses are characterized by an outer astroglial reaction that surrounds a proliferating zone of capillaries and fibroblasts, which then surrounds a central region of dead and dying brain tissues infiltrated by polymorphonuclear leukocytes and histiocytes. 5 The higher ADC ratio in toxoplasmosis compared to that in PCNSL likely reflects decreased viscosity within their concentric zone, which may be attributable to necrotic composition or impaired cellular immune response in immunocompromised patients. 13
Tuberculomas can present as caseating lesions with a solid necrotic center, showing a ring-enhancing appearance on imaging. Mature tuberculomas typically have a necrotic caseous center surrounded by a capsule containing fibroblasts, epithelioid cells, Langerhans giant cells, and lymphocytes. Caseating granulomas generally appear hypointense on T1- and T2-weighted MRI images due to their dense granulation and compressed glial tissue in the central core, resulting in greater cellular density than that in the adjacent brain parenchyma. 27 Parry et al. 28 reported a significant difference (p ≤ .001) between the ADC values of T2-weighted hypointense and hyperintense tuberculomas, with hypointense tuberculomas showing higher mean ADC values than those of hyperintense tuberculomas. Thus, tuberculosis usually exhibits variable ADC ratios in the central region. Our study, which included multistage tuberculosis cases, observed variations in the central ADC ratio. Additionally, we found no significant difference in restricted diffusion at the central region between PCNSL and tuberculosis (p = .43) but observed significantly restricted diffusion at the peripheral region of the lesion (p < .001). Therefore, the central region may be less helpful for distinguishing PCNSL from tuberculosis, and we recommend using the peripheral region to differentiate between these conditions.
Our study demonstrated that SWI can differentiate PCNSL from infections based on the presence of ISS. Spontaneous hemorrhage in PCNSL lesions may be more frequent in patients with AIDS than in those without, 8 with approximately 25% of spontaneous hemorrhage detected in PCNSL lesions in patients with AIDS. 29 Our study found that 80% of PCNSL lesions exhibited positivity for ISS in the central and peripheral regions. We identified two patterns of positive ISS in PCNSL: vascular and dotted. A previous study reported that the expression of vascular endothelial growth factor in lymphoma cells was significantly associated with tumor angiogenesis, 30 suggesting that a positive ISS with a vascular pattern may be related to vascular projection into the tumor, representing tumor angiogenesis. Thus, a positive ISS with a vascular pattern is more indicative of PCNSL than of infections, whereas a dotted pattern is more commonly associated with infections.
Previous studies have explored using SWI31,32 to differentiate between pyogenic brain abscesses and high-grade brain tumors, such as glioblastoma, by evaluating the presence and morphology of a hypointense rim on the SWI sequence. They found that a hypointense rim on SWI was typically present in pyogenic brain abscesses and concluded that SWI may assist in differentiating pyogenic abscesses from high-grade brain tumors. In our study, we used SWI to distinguish between tumors and infections. Our findings showed a significantly positive ISS at the periphery of PCNSL compared to infections.
Toxoplasmosis in the acute necrotizing abscess stage is characterized by acute inflammatory granulation tissue, a zone of necrosis, and petechial hemorrhage with free-living tachyzoites and encysted organisms. In the organizing abscess stage, a fibrous capsule with endarteritic vessels forms around the necrotic center, resembling a tuberculoma. The chronic stage presents a vascular fibrous scar with fewer toxoplasma tachyzoites. 26 This variability in stages likely contributes to toxoplasmosis lesions showing ISS on the SWI sequence due to the presence of blood products across all stages.
Although MRI features such as DWI and SWI provide valuable insights for distinguishing lymphoma from toxoplasmosis and tuberculoma, they should be considered adjunct tools rather than definitive diagnostic markers. The use of conventional MRI, with characteristic signs like the eccentric and concentric target signs, remains central to diagnosis. Additionally, advanced imaging techniques such as MR perfusion and MR spectroscopy offer further insights into the metabolic and hemodynamic properties of lesions. Ultimately, the final diagnosis should be based on a comprehensive evaluation that integrates clinical findings, laboratory results, conventional MRI, and advanced imaging techniques, ensuring the most accurate differentiation between these conditions.
This study has several limitations. First, the rarity of ring-enhancing PCNSL lesions resulted in a small and imbalanced cohort, with fewer PCNSL cases compared to infectious lesions, potentially biasing classification performance. Second, in patients with multiple lesions, biopsy was generally performed on the most clinically or radiologically significant lesion, with an assumption of homogeneity across lesions due to the impracticality of obtaining histopathological confirmation for each lesion. Third, the relatively recent adoption of SWI resulted in incomplete SWI data for some patients, whereas DWI was more consistently available, which may limit the generalizability of SWI-related findings. Fourth, analyses were conducted at the lesion level rather than the patient level, which may not fully represent clinical decision-making processes and introduces potential bias due to intra-subject correlation. Nonetheless, this approach was chosen to increase statistical power and explore lesion heterogeneity. Fifth, variations in MRI hardware and field strength can influence ADC measurements; while ADC ratios normalized to contralateral normal-appearing brain were employed to mitigate inter-subject variability, this method does not fully correct for differences in signal-to-noise ratio associated with scanner-specific factors, potentially affecting measurement reliability. Sixth, lesion quantification relied on two-dimensional ROIs drawn on representative slices, which may inadequately capture lesion heterogeneity compared to volumetric three-dimensional analyses. Finally, the qualitative interpretation of DWI and SWI is inherently subjective and susceptible to intra- and inter-observer variability, particularly in the absence of standardized or automated assessment protocols. Future large-scale, prospective, patient-level studies incorporating volumetric 3D ROI analyses and standardized imaging protocols are warranted to validate and extend these findings for clinical application.
Conclusion
Our findings indicate that restricted diffusion on DWI, positive ISS on SWI, and DWI with ADC ratios measured at ring-enhancing lesions may serve as valuable adjuncts in distinguishing ring-enhancing PCNSL from opportunistic CNS infections. Specifically, peripheral ADCavg, peripheral ADCmin, and central ADCavg ratios with cut-off points of less than 1.25, 1.00, and 1.45, respectively, were most effective in identifying PCNSL.
Footnotes
Author contributions
All authors contributed to the study’s conceptualization and design. Material preparation, data collection, and analysis were performed by Nutchawan Jittapiromsak, Phanuphong Sriinkua, Pornpattra Nimitpornsuko, and Pakrit Jittapiromsak. The first draft of the manuscript was written by Nutchawan Jittapiromsak, Phanuphong Sriinkua, and Pornpattra Nimitpornsuko. All authors commented on previous versions of the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.