
Abstract
Arteriovenous fistulas (AVFs) involving the inferior petroclival vein (IPCV) are extremely rare and may mimic cavernous sinus (CS) dural arteriovenous fistulas (DAVF) because of shared venous drainage patterns. A 72-year-old man presented with diplopia and left ocular chemosis. Carotid angiography revealed retrograde venous drainage into the superior ophthalmic vein via the inferior petrosal sinus (IPS) and CS. The initial findings suggested a CS-DAVF; however, three-dimensional angiography, including multiplanar reconstruction and maximum intensity projection analyses, identified shunt pouches in the IPCV and anterior condylar vein. Transvenous embolization via the IPS allowed the selective coil embolization of the IPCV shunt pouch while preserving the IPS. The IPCV-AVF resolved completely. Although the anterior condylar vein dural AVF remained, it was classified as Borden type I and was managed conservatively. The present case highlights the importance of detailed three-dimensional angiographic analysis to distinguish IPCV-AVF from CS-DAVF and guide effective treatment.
Keywords
Introduction
The inferior petroclival vein (IPCV) courses along the extracranial surface of the petroclival fissure. 1 Its rostral end communicates with the venous plexus surrounding the carotid artery or the cavernous sinus (CS), and its caudal end connects to the internal petrosal sinus (IPS) or anterior condylar vein (ACV). 1 The IPCV has been described as a potential venous route for accessing the CS during endovascular procedures. 1 However, arteriovenous fistulas (AVFs) involving the IPCV are extremely rare, and only two cases have been previously reported in the literature.2,3
Herein, we present a rare case of IPCV-AVF that was successfully treated with selective transvenous coil embolization. We emphasize the importance of detailed three-dimensional (3D) angiographic evaluation to distinguish IPCV-AVF from CS dural arteriovenous fistula (DAVF), which may present with similar clinical and imaging features.
Case presentation
A 72-year-old man presented with diplopia and left conjunctival chemosis. He initially consulted an ophthalmologist, who noted ocular proptosis, elevated intraocular pressure, decreased visual acuity, and nearly complete ophthalmoplegia in the left eye. Brain magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) suggested a DAVF, prompting referral to our department. Neurological examination additionally revealed left hypoglossal nerve palsy and no pulsatile tinnitus. MRI confirmed left-sided proptosis. Time-of-flight MRA demonstrated a markedly dilated left superior ophthalmic vein (SOV) and multiple detailed abnormal vessels suggestive of feeders. Left external carotid angiography showed multiple fine feeding arteries arising from the left ascending pharyngeal artery, middle meningeal artery, accessory meningeal artery, and artery of the foramen rotundum. The shunt flow drained into the left internal jugular vein and also demonstrated retrograde flow into the SOV via the IPS and CS (Figure 1(a, b)). On the basis of these findings and the patient’s ocular symptoms, a CS-DAVF was initially suspected. However, right external carotid angiography demonstrated that the shunt point fed by neuromeningeal branch of the ascending pharyngeal artery appeared to be located inferior to the CS (Figure 1(c)). The careful review of 3D external carotid angiograms, including multiplanar reconstruction (MPR) and maximum intensity projection (MIP) analyses, identified the shunt pouches in the IPCV and ACV, adjacent to the IPS (Figure 1(d, e)). (a, b) Left external carotid angiography (a: AP view, b: lateral view) revealing multiple reticular feeders and retrograde drainage from the shunt into the internal jugular vein and SOV. (c). Right external carotid angiography demonstrating that the shunt point fed by neuromeningeal branch of the APA appeared to be located inferior to the CS. (d, e). Three-dimensional left external carotid angiograms (d: multiplanar reconstruction, e: maximum intensity projection) showing the shunt pouch at the IPCV near the IPS.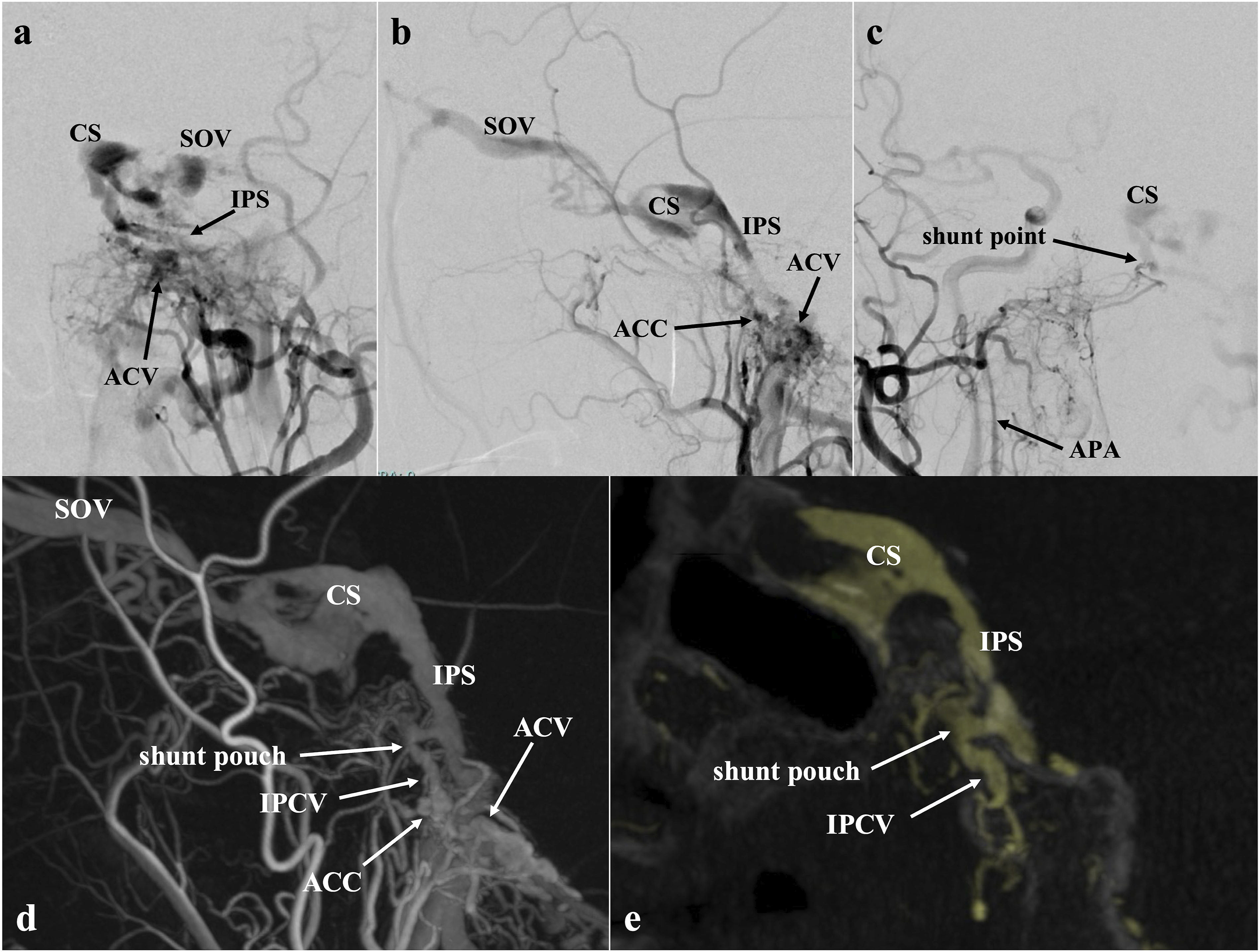
The patient underwent transfemoral transvenous embolization under general anesthesia. A microcatheter was navigated from the left internal jugular vein through the IPS to the shunt pouch of the IPCV (Figure 2(a)). Selective coil embolization was then performed using four detachable coils, successfully obliterating the IPCV shunt pouch while preserving the IPS (Figure 2(b)). Post-embolization angiography confirmed the complete obliteration of the IPCV-AVF. Although the ACV-DAVF remained, it was classified as Borden type I and was managed conservatively (Figure 2(c)). Post-operative computed tomography showed the coil mass within the IPCV in an extracranial location (Figure 2(d)). All symptoms resolved promptly following the embolization procedure. Follow-up MRI and MRA at 1 month demonstrated the complete resolution of the ACV-DAVF. No recurrence of either AVF was observed on follow-up MRA during the 10-month follow-up period. (a) Imaging during transvenous embolization showing a microcatheter positioned at the IPCV shunt pouch via the IPS. (b). Native image showing the coil mass within the selectively embolized shunt pouch. (c). Post-embolization angiogram showing complete disappearance of the IPCV-AVF; the residual ACV-DAVF (Borden type I) remained. (d). Post-operative computed tomography image showing the coil mass within the IPCV in an extracranial location.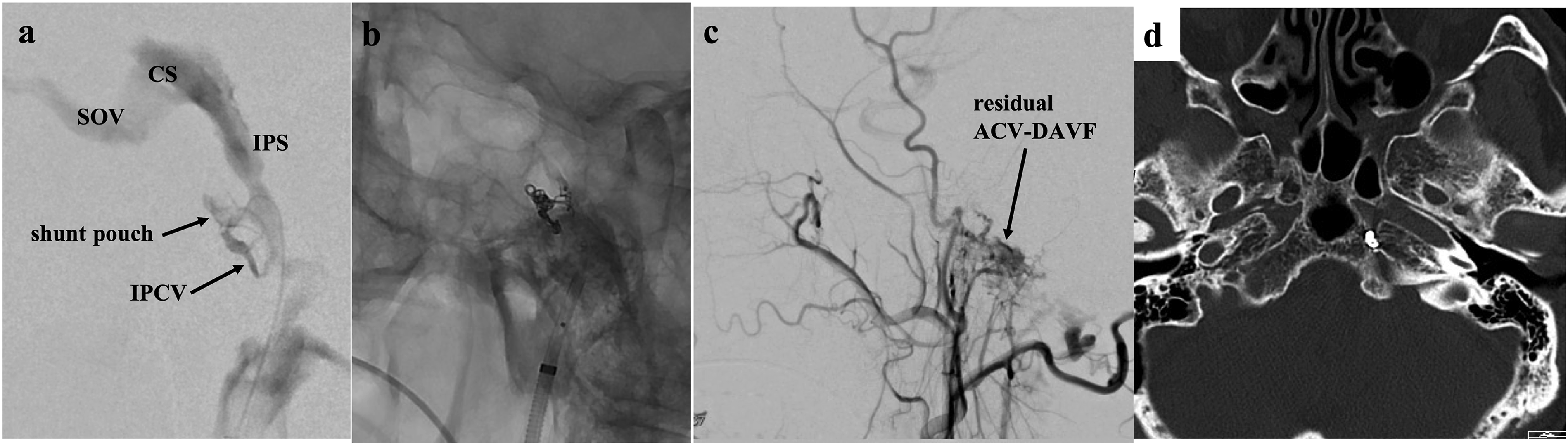
Discussion
DAVFs located around the hypoglossal canal (HC) region, including those involving the ACV and anterior condylar confluence, account for approximately 3%–4% of all intracranial DAVFs.4,5 DAVFs in this region have been described using various terminologies, including anterior condylar confluence DAVF, ACV-DAVF, and HC-DAVF, reflecting the complex venous anatomy around the HC. 6 Mizutani et al. reported that one-third of these HC-DAVFs originate from the ACV, and another one-third were located in the jugular tubercle venous complex, superior to the HC. 6 AVFs involving the IPCV, which is located above the HC, may therefore be considered part of the spectrum of HC-DAVFs; however, they appear to exhibit distinct clinical features.
Including our case, only three patients with IPCV-AVFs have been reported in the literature. All three presented with retrograde venous drainage through the CS to the SOV, leading to ocular symptoms such as chemosis, ophthalmoplegia, or proptosis—symptoms that are typically associated with CS-DAVFs.2,3 By contrast, most HC-DAVFs present with pulsatile tinnitus and fewer ocular symptoms.4,5 Notably, in all three reported IPCV-AVF cases, the shunt pouch received arterial supply from the contralateral ascending pharyngeal artery, which may represent a characteristic angiographic feature of IPCV-AVFs. Such contralateral arterial supply has also been described in HC-DAVFs, 5 suggesting a close anatomical relationship between IPCV-AVFs and HC-DAVFs. Recognition of this angiographic feature may therefore aid in the precise localization of the shunt point. Selective embolization was successfully performed in all reported IPCV-AVF cases.
In the present case, two distinct shunt pouches were identified: one in the IPCV and one in the ACV.2,3 This anatomical configuration differed from the two previously reported IPCV-AVFs in that a separate ACV-DAVF was also present.2,3 In our case, the IPCV was in direct anatomical connection with the IPS, and the high-flow shunt likely promoted retrograde drainage into the CS and SOV, producing the severe ocular manifestations. The use of 3D angiographic reconstruction (specifically, MPR and MIP) played a crucial role in identifying the exact locations of the shunt points. These modalities provided enhanced visualization of the intraosseous venous anatomy and were instrumental in differentiating the IPCV-AVF from a CS-DAVF. Precise anatomical localization of the shunt points allowed for effective, selective coil embolization while preserving important venous structures such as the IPS.
The residual ACV-DAVF after the embolization of the IPCV-AVF, which primarily caused retrograde drainage into the CS and SOV, demonstrated only antegrade drainage into the internal jugular vein without cortical venous reflux, corresponding to a low-risk Borden type I lesion. Therefore, conservative management of the ACV-DAVF was considered appropriate. The spontaneous resolution of the ACV-DAVF observed on follow-up imaging may have been related to reduced shunt flow and subsequent thrombosis caused by hemodynamic changes following occlusion of the dominant IPCV shunt.
Conclusions
We report a rare case of an AVF involving the IPCV that clinically and radiographically mimicked a CS-DAVF. Selective transvenous coil embolization via the IPS resulted in the complete obliteration of the IPCV-AVF, with the associated resolution of ocular symptoms. Because IPCV-AVFs may present with clinical and angiographic features similar to those of CS-DAVFs, careful interpretation of 3D angiography, particularly MPR and MIP analyses, is essential for accurate localization of the shunt point and appropriate treatment planning. In addition, selective angiography of the contralateral ascending pharyngeal artery may aid in the identification of the shunt location.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board of Nakamura Memorial Hospital (Approval No. 2025080801).
Consent to participate
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Author contributions
Conceptualization and study design: YT, HE, and TF.
Data collection and curation: YT and TF.
Writing—original draft preparation: YT and TF.
Writing—review and editing: YT and HE.
Supervision and overall responsibility: OT and HN.
Funding acquisition: None.
All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.