
Abstract
Introduction
Sickle cell disease (SCD) confers a three-to fivefold increase in the prevalence of intracranial aneurysms (IA). Flow diversion (FD) requires mandatory dual antiplatelet therapy (DAPT), yet perioperative transfusion to reduce hemoglobin S (HbS) risks delayed hemolytic transfusion reaction (DHTR). No guidelines address this conflict between DHTR-associated coagulopathy and mandatory DAPT. We report the largest FD series in SCD.
Methods
Retrospective single-center case series of SCD patients undergoing FD for IA (2017 to 2026). Of 12 SCD patients treated for aneurysms, seven received FD and comprised the analytic cohort.
Results
Seven patients (5 HbSS, 2 HbS/β0-thalassemia; median age 38; 71% female) harbored 29 aneurysms; 12 were treated with FD across 8 procedures using 15 devices. HbS <30% was achieved in 3 of 7 (43%); one patient underwent FD at HbS 78.5% due to alloimmunization. Clopidogrel hyporesponsiveness was identified in 2 of 4 TEG-tested patients (50%). Procedure-related mortality was 14% (1/7): fatal DHTR with DIC on postoperative day 8, the first reported DHTR-DAPT collision. Procedure-related morbidity included one intraoperative thrombus and one vasospasm episode, both resolved without sequelae (2/8 procedures, 25%). Additional events included asymptomatic in-stent stenosis and delayed stroke from SCD vasculopathy. At last follow-up, 5 of 6 survivors maintained mRS 0 to 1.
Discussion and Conclusion
FD is technically feasible in SCD, but the 14% procedure-related mortality from a fatal DHTR exposes the unresolved conflict between transfusion-associated hyperhemolysis and mandatory DAPT. CYP2C19-mediated clopidogrel resistance and alloimmunization pose additional challenges that require predefined protocols and prospective multicenter registries.
Keywords
Introduction
Sickle cell disease (SCD) affects approximately 100,000 Americans, with cerebrovascular complications representing a leading cause of morbidity. 1 Intracranial aneurysm prevalence in SCD is estimated at 5% to 11%, approximately 3 to 5 times the general population rate.2–5 Flow diversion has emerged as the preferred treatment for wide-neck paraclinoid aneurysms but requires mandatory dual antiplatelet therapy (DAPT), introducing unique challenges in SCD. The inherent prothrombotic state of SCD elevates the risk of device-related thrombosis,6–8 while perioperative transfusion to reduce hemoglobin S (HbS) per American Society of Hematology (ASH) guidelines carries the risk of delayed hemolytic transfusion reaction (DHTR), which occurs in approximately 4% of episodically transfused SCD adults and can be fatal.9,10 When DHTR-associated coagulopathy develops in a patient on mandatory DAPT, the resulting management dilemma has no published guidance.
Published experience with flow diversion in SCD is limited. Grin et al. reported Pipeline embolization in 14 hemoglobinopathy patients (5 SCD) with zero complications but limited perioperative detail. 11 Pelcher et al. found that the 3 SCD patients in their 11-patient hematologic disorder series were the only subgroup with complications (67% stroke rate). 12 This series reports the largest dedicated flow diversion experience in SCD (7 patients, 8 procedures, 15 devices), with emphasis on the DHTR-DAPT conflict, antiplatelet pharmacogenomics, and alloimmunization as barriers to perioperative optimization.
Methods
Study design and patient selection
We retrospectively identified all SCD patients who underwent flow diversion for IA at a single academic center between July 2017 and February 2026 (Figure 1). During the study period, 12 SCD patients underwent 16 procedures for IA. Five were excluded (2 non-flow-diversion endovascular, 3 surgical clipping only), yielding 7 patients who received at least one flow diverter. This study was conducted in accordance with STROBE guidelines.
13
Institutional review board approval was obtained. Eligible patients had confirmed SCD (HbSS or HbS/β0-thalassemia), verified by hemoglobin electrophoresis. The rationale for grouping HbSS and HbSβ0 is detailed in Supplemental Tables. This study represents Level IV evidence (case series without comparison group). Patient selection flow diagram.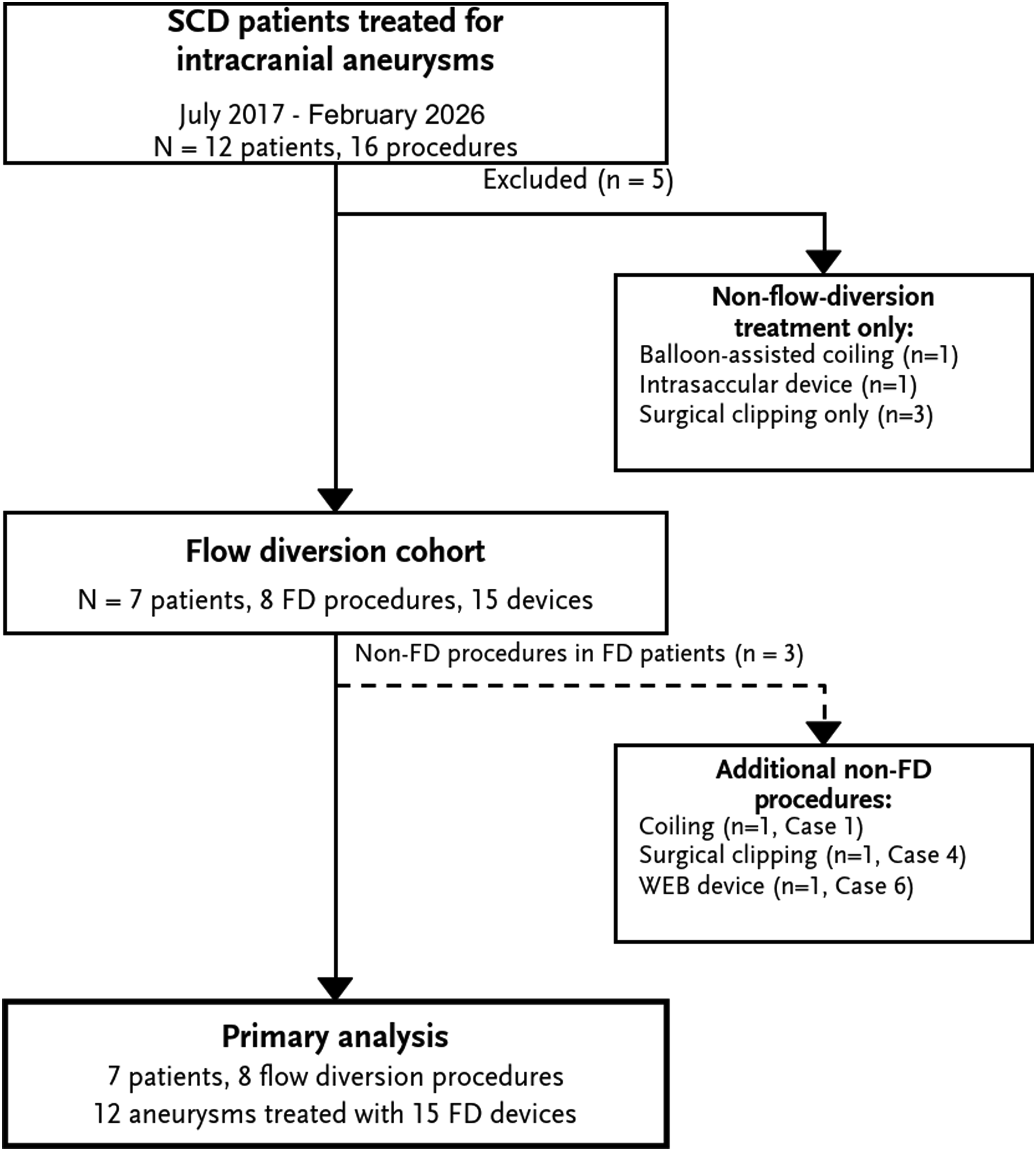
Perioperative protocol
Preoperative hematology consultation was obtained. The target HbS was <30% per ASH guidelines. 9 Transfusion strategy was individualized: exchange transfusion for baseline HbS >60%, simple transfusion or exchange for HbS 30% to 60%. Extended red blood cell phenotyping and alloantibody review were performed for all patients. DAPT (aspirin 81–325 mg plus clopidogrel 75 mg) was initiated 5 to 7 days preprocedure; cilostazol was substituted for aspirin intolerance. Thromboelastography (TEG) with platelet mapping assessed ADP-receptor inhibition (adequate: >30%); subtherapeutic patients were switched to prasugrel.14,15 Intraoperative anticoagulation consisted of weight-based heparin (activated clotting time goal 250–300 s). Postoperatively, patients were monitored with daily hemolysis markers for 3 to 5 days for signs of DHTR. 10
Outcome assessment
Outcomes were reported per patient, per procedure, and per aneurysm. Angiographic outcomes were graded using the O’Kelly–Marotta (OKM) scale. 16 Clinical outcomes were assessed by modified Rankin Scale (mRS). Adverse events were classified into four categories: procedure-related mortality, procedure-related morbidity (intraprocedural events requiring active intervention), device-related radiographic findings (asymptomatic imaging abnormalities not requiring intervention), and disease-related events (attributable to underlying SCD progression rather than the procedure). Given the sample size, all analyses were descriptive; no inferential statistical testing was performed.
Results
Cohort and aneurysm characteristics
Patient characteristics and clinical outcomes.
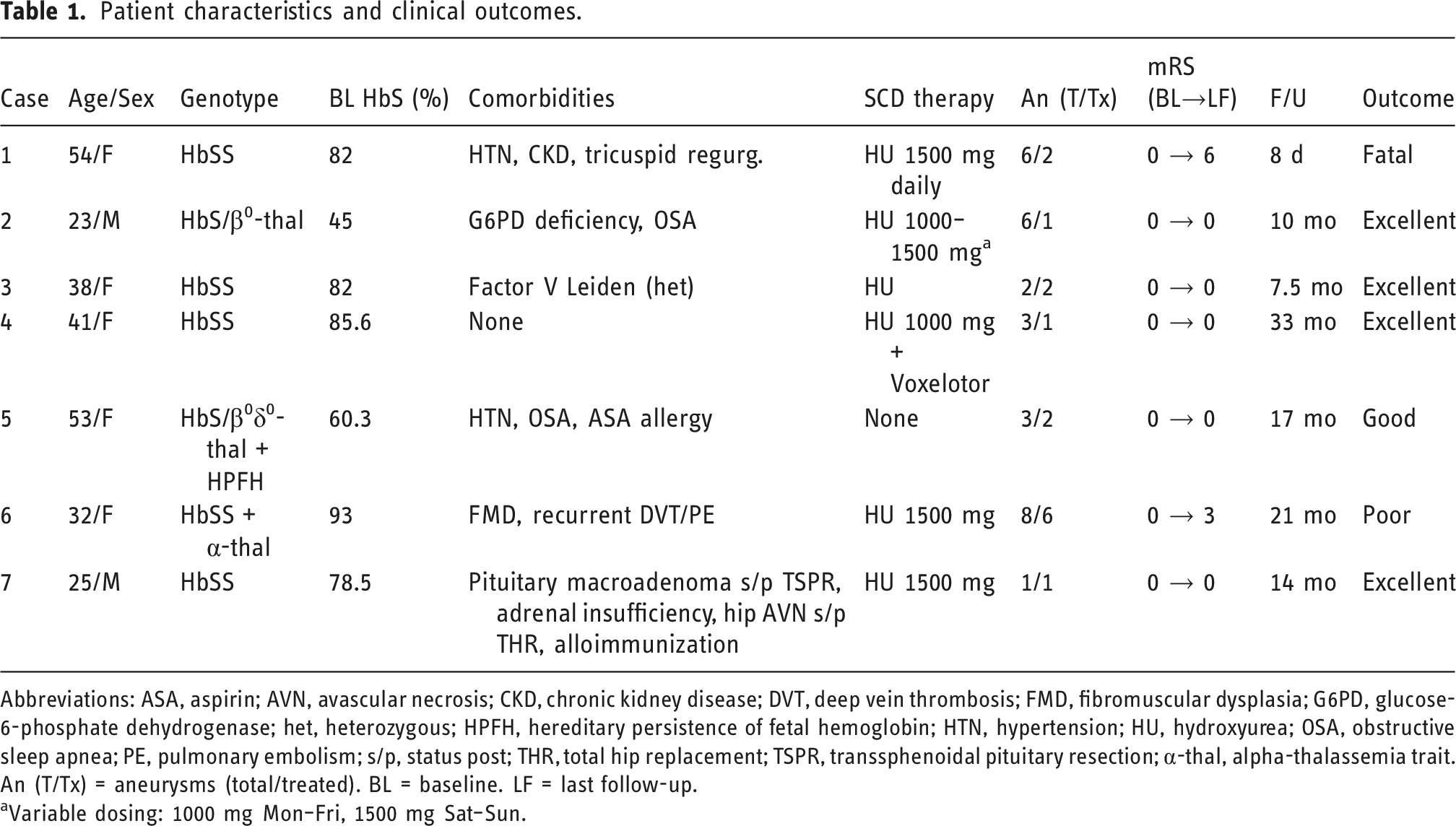
Abbreviations: ASA, aspirin; AVN, avascular necrosis; CKD, chronic kidney disease; DVT, deep vein thrombosis; FMD, fibromuscular dysplasia; G6PD, glucose-6-phosphate dehydrogenase; het, heterozygous; HPFH, hereditary persistence of fetal hemoglobin; HTN, hypertension; HU, hydroxyurea; OSA, obstructive sleep apnea; PE, pulmonary embolism; s/p, status post; THR, total hip replacement; TSPR, transsphenoidal pituitary resection; α-thal, alpha-thalassemia trait.
An (T/Tx) = aneurysms (total/treated). BL = baseline. LF = last follow-up.
aVariable dosing: 1000 mg Mon–Fri, 1500 mg Sat–Sun.
Flow diversion procedures (N = 8 procedures in 7 patients).
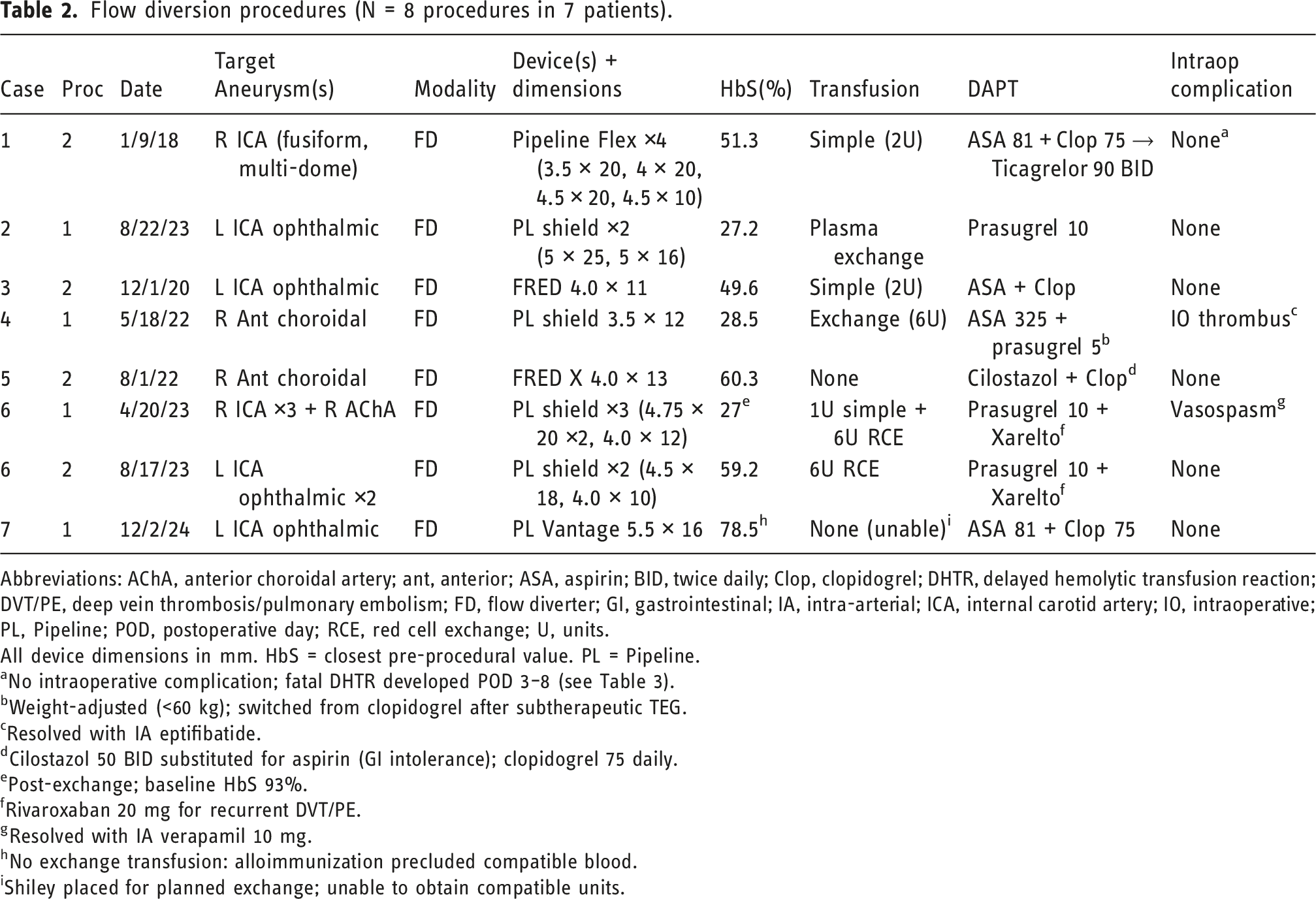
Abbreviations: AChA, anterior choroidal artery; ant, anterior; ASA, aspirin; BID, twice daily; Clop, clopidogrel; DHTR, delayed hemolytic transfusion reaction; DVT/PE, deep vein thrombosis/pulmonary embolism; FD, flow diverter; GI, gastrointestinal; IA, intra-arterial; ICA, internal carotid artery; IO, intraoperative; PL, Pipeline; POD, postoperative day; RCE, red cell exchange; U, units.
All device dimensions in mm. HbS = closest pre-procedural value. PL = Pipeline.
aNo intraoperative complication; fatal DHTR developed POD 3–8 (see Table 3).
bWeight-adjusted (<60 kg); switched from clopidogrel after subtherapeutic TEG.
cResolved with IA eptifibatide.
dCilostazol 50 BID substituted for aspirin (GI intolerance); clopidogrel 75 daily.
ePost-exchange; baseline HbS 93%.
fRivaroxaban 20 mg for recurrent DVT/PE.
gResolved with IA verapamil 10 mg.
hNo exchange transfusion: alloimmunization precluded compatible blood.
iShiley placed for planned exchange; unable to obtain compatible units.
Adverse events and clinical outcomes.
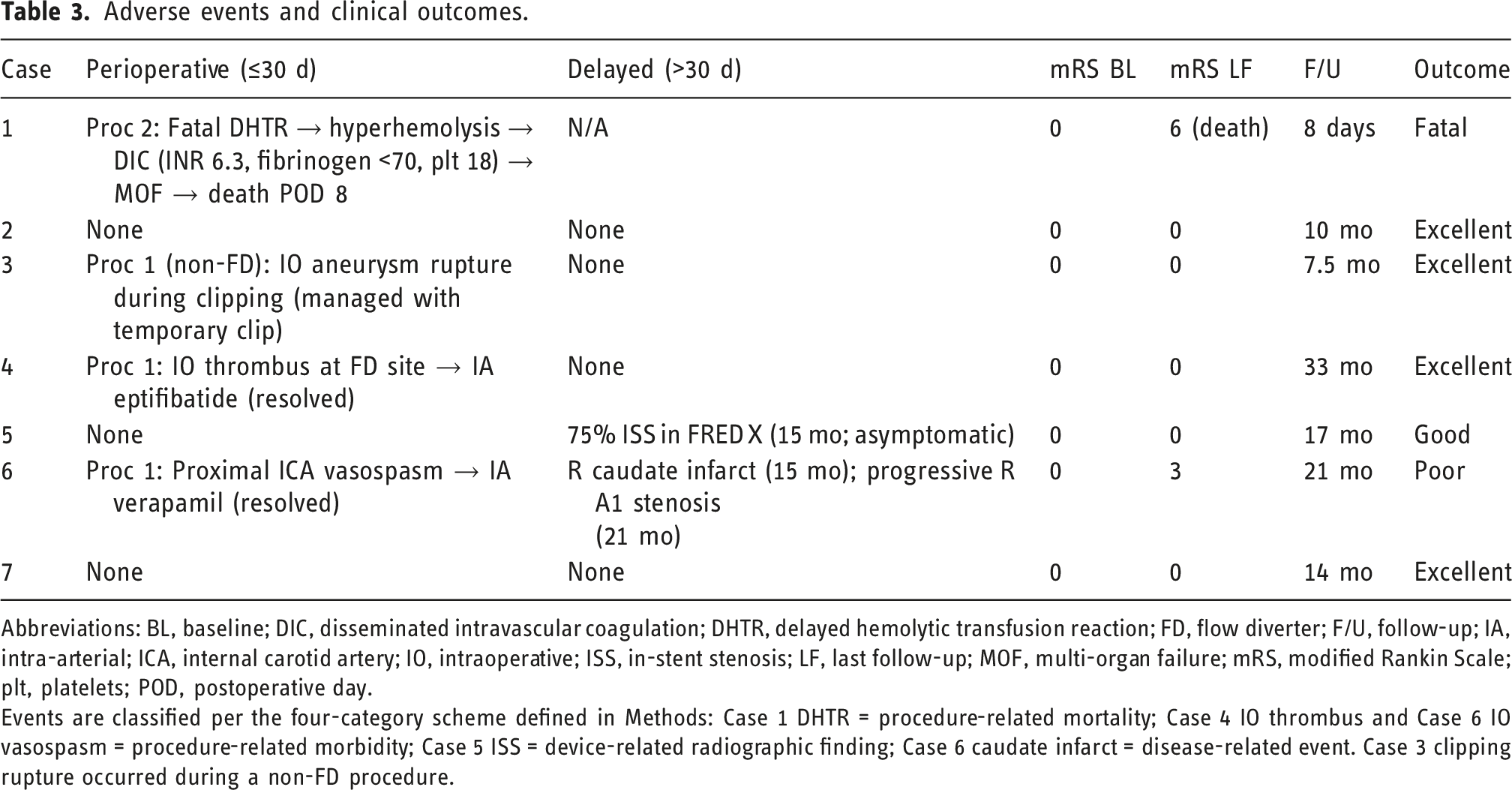
Abbreviations: BL, baseline; DIC, disseminated intravascular coagulation; DHTR, delayed hemolytic transfusion reaction; FD, flow diverter; F/U, follow-up; IA, intra-arterial; ICA, internal carotid artery; IO, intraoperative; ISS, in-stent stenosis; LF, last follow-up; MOF, multi-organ failure; mRS, modified Rankin Scale; plt, platelets; POD, postoperative day.
Events are classified per the four-category scheme defined in Methods: Case 1 DHTR = procedure-related mortality; Case 4 IO thrombus and Case 6 IO vasospasm = procedure-related morbidity; Case 5 ISS = device-related radiographic finding; Case 6 caudate infarct = disease-related event. Case 3 clipping rupture occurred during a non-FD procedure.
Perioperative management
Transfusion was performed in 5 of seven patients (71%). The HbS target of <30% was achieved in 3 (43%): Cases 2 (27.2%), 4 (28.5%), and 6 (27%). Case 7 could not receive exchange transfusion because of alloimmunization (homozygous variant RHCE genotype) and underwent flow diversion at HbS 78.5%. Case 5 (HbS/β0δ0-thalassemia with hereditary persistence of fetal hemoglobin [HPFH], baseline HbS 60.3%) did not receive transfusion. TEG platelet mapping was performed in 4 of seven patients (57%); 2 of 4 (50%) demonstrated subtherapeutic clopidogrel response (ADP inhibition 15.1% and 12.9%). One was switched to prasugrel; the other was not switched and had no thromboembolic events.
Complications and outcomes
Technical success was achieved in all eight procedures (100%). The sole procedure-related death was a fatal DHTR in Case 1, a 54-year-old woman who underwent Pipeline Flex placement for bilateral paraclinoid ICA aneurysms following simple transfusion. On postoperative day 3, she developed progressive hyperhemolysis (hemoglobin nadir 3.8 g/dL, LDH 3741 U/L) and DIC (INR 6.3, fibrinogen <70 mg/dL, platelets 18 K/µL), progressing to multi-organ failure and death on day 8 (Figure 2). To our knowledge, this is the first reported case of DHTR-associated coagulopathy colliding with mandatory DAPT after flow diversion. One intraoperative thrombus during flow diverter deployment (Case 4) was managed with eptifibatide without sequelae; this occurred in the context of subtherapeutic clopidogrel response (ADP inhibition 15.1%). Intraoperative proximal ICA vasospasm in Case 6 (Procedure 1) was managed with intra-arterial verapamil and resolved without sequelae (procedure-related morbidity: 2/8, 25%). Two additional events were classified outside procedure-related complications. Asymptomatic 75% in-stent stenosis was identified within the FRED X flow diverter at 15 months in Case 5 (device-related radiographic finding); the non-standard DAPT (cilostazol plus clopidogrel for aspirin intolerance) and non-surface-modified device may have contributed. A right caudate infarct at 15 months in Case 6 (Figure 3) was attributed to progressive A1 stenosis from SCD vasculopathy rather than device thrombosis (disease-related event, mRS 3); the flow diverter remained patent on imaging. Among 11 FD-treated aneurysms with follow-up, the adequate occlusion rate (OKM C or better) was 82%. The 30-days mortality was 14% (1/7). At last follow-up (median 10 months), 5 of 6 survivors (83%) maintained mRS 0 to 1. Laboratory trajectory of fatal delayed hemolytic transfusion reaction (Case 1). Representative case of endovascular flow diversion for intracranial aneurysms in a patient with sickle cell disease.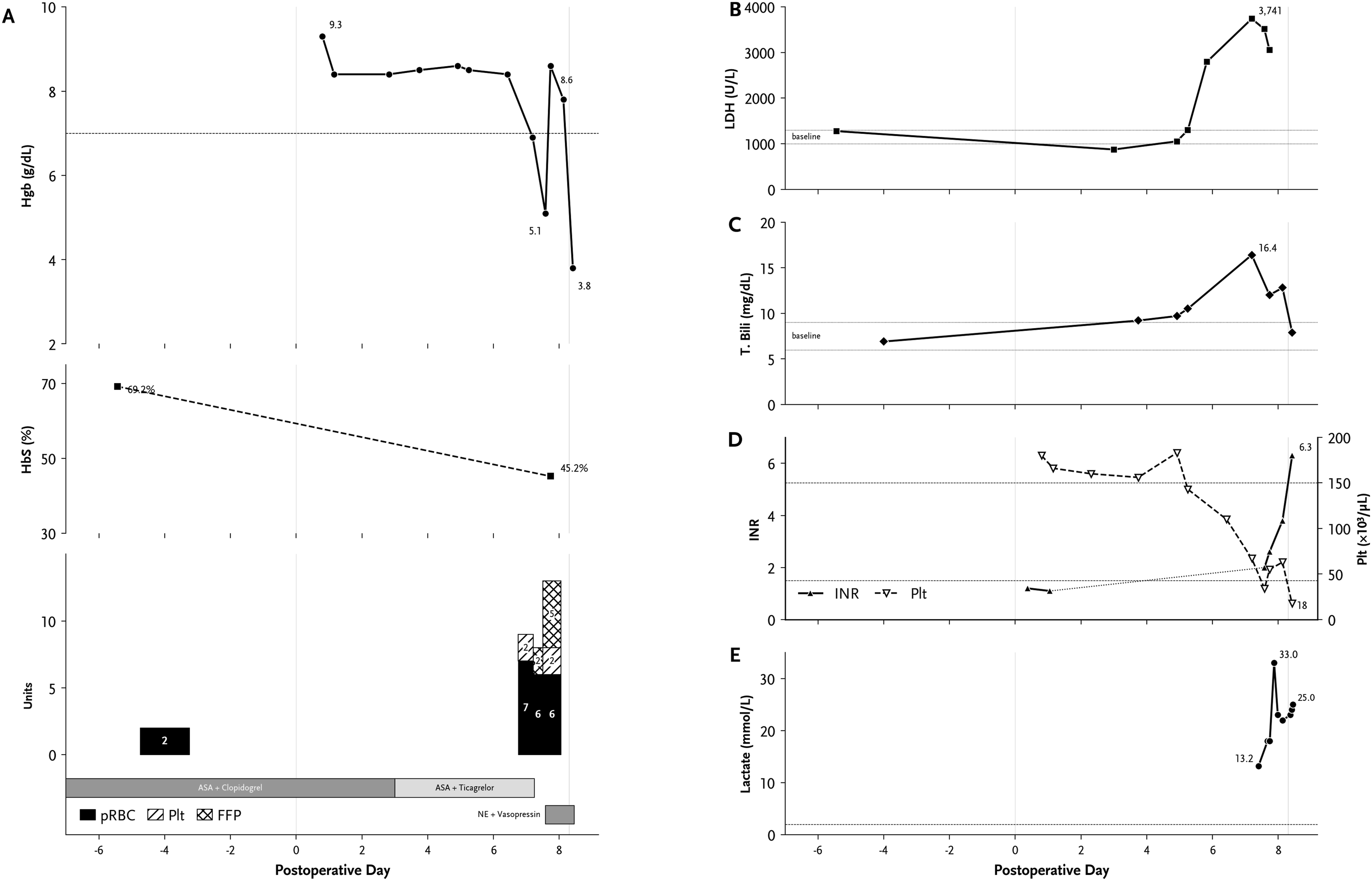

Discussion
This series constitutes the largest reported FD experience in SCD and the first to document the interaction between DHTR-associated coagulopathy and mandatory DAPT. As Level IV evidence, the procedure-related mortality from a fatal DHTR warrants careful appraisal and should be viewed as hypothesis-generating. The fatal DHTR in Case 1 illustrates a management dilemma specific to flow diversion in SCD. DHTR occurs in approximately 4% of episodically transfused SCD adults, develops without detectable alloantibodies in 30% of cases, and is therefore unpredictable. 10 When DHTR produces DIC, as occurred in Case 1, the clinician confronts simultaneous hemorrhagic coagulopathy and the ongoing requirement for DAPT to prevent in-stent thrombosis. No published guidance addresses this specific dilemma. The uncomplicated courses of non-FD endovascular patients at our institution who did not require mandatory DAPT support the hypothesis that the DAPT-SCD interaction, rather than the endovascular procedure itself, drives much of the excess risk. We propose that centers performing flow diversion in SCD patients establish predefined DHTR response protocols, including immediate hematology involvement, avoidance of further transfusion, initiation of IVIG and corticosteroids, and explicit criteria for DAPT modification when DIC develops.
The rate of subtherapeutic clopidogrel response observed in our cohort is consistent with the approximately 37% prevalence of CYP2C19 loss-of-function alleles in individuals of African descent.14,15 Inadequate platelet inhibition in a population already predisposed to thrombosis compounds this risk, as the intraoperative thrombus in Case 4 demonstrates. We recommend either CYP2C19 genotyping or empiric prasugrel/ticagrelor as first-line P2Y12 inhibition, with mandatory TEG platelet mapping, for SCD patients undergoing flow diversion. The uncomplicated outcome in Case 7, who underwent flow diversion without exchange transfusion due to alloimmunization, challenges the assumption that the ASH-recommended HbS <30% is an absolute prerequisite. Alloimmunization, present in up to 50% of chronically transfused SCD patients, remains a practical barrier that perioperative protocols must address. 9 The low rate of HbS target achievement in our cohort illustrates how often clinical circumstances prevent adherence to guideline recommendations. The occurrence of in-stent stenosis exclusively in the patient receiving a non-surface-modified device with non-standard DAPT, while no Pipeline Shield-treated patient developed clinically significant stenosis, aligns with in vitro data showing reduced thrombogenicity with surface-modified devices.17,18 Surface-modified flow diverters may be particularly advantageous in the prothrombotic milieu of SCD. Contextualizing our results (Table S2): Grin et al. reported zero complications in 14 hemoglobinopathy patients (5 SCD), 11 while Pelcher et al. reported 67% postoperative stroke in their 3 SCD patients. 18 Our procedure-related mortality falls between these extremes. The heterogeneity likely reflects differences in perioperative protocols, device selection, and SCD severity—the very variables that future registries must capture.
Considering the lethal potential of the DHTR-DAPT interaction, flow diversion in SCD should be approached with caution and reserved for aneurysms that cannot be adequately addressed by alternative techniques. When the anatomy is favorable, conventional stent-assisted coiling, intrasaccular flow disruption with the WEB device, or surgical clipping should be considered first; the latter two options in particular avoid the obligatory DAPT exposure that appears to drive much of the excess risk in this population. Flow diversion remains a reasonable option for wide-neck or otherwise complex aneurysms in which these alternatives are not feasible, provided that a multidisciplinary perioperative plan is in place.
Limitations
As a retrospective single-center series of seven patients, this study provides Level IV evidence. The sample size precludes inferential statistics or risk factor analysis; reported rates carry wide confidence intervals. Selection bias, heterogeneous protocol adherence, variable follow-up, and the absence of a comparison group substantially constrain the conclusions. CYP2C19 genotyping was not performed. These findings should be interpreted as hypothesis-generating. CYP2C19 genotyping was not performed. These findings should be interpreted as hypothesis-generating. The retrospective design further limited the completeness and uniformity of data collection. The flow diverters used were heterogeneous (Pipeline Shield, Pipeline Vantage, Pipeline Flex, FRED, and FRED X), and the antiplatelet regimens varied across patients, including substitution of cilostazol for aspirin intolerance and prasugrel for subtherapeutic clopidogrel response. In addition, no standardized follow-up imaging protocol was applied, and the duration of follow-up varied between patients. This device and pharmacologic heterogeneity, together with the lack of a uniform follow-up schedule, may have influenced the observed outcomes and limits direct comparison across cases.
Conclusion
As the largest reported flow diversion series in SCD, these data demonstrate technical feasibility with adequate angiographic occlusion, but the procedure-related mortality from a fatal DHTR serves as a stark reminder of the lethal potential when DHTR and mandatory DAPT collide. Three priorities emerge: (1) predefined DHTR response protocols for patients on mandatory DAPT; (2) pharmacogenomically guided antiplatelet therapy given the high CYP2C19 loss-of-function allele prevalence in this population; and (3) prospective multicenter registries capturing genotype, transfusion strategy, antiplatelet regimen, and long-term outcomes. Given these risks, flow diversion in SCD should be reserved for aneurysms that are not amenable to stent-assisted coiling, intrasaccular flow disruption with the WEB device, or surgical clipping. Until such data exist, flow diversion in SCD should involve multidisciplinary consensus and frank acknowledgment of current uncertainty.
Supplemental material
Supplemental Material—Flow diversion for intracranial aneurysms in patients with sickle cell disease
Supplemental Material for Flow diversion for intracranial aneurysms in patients with sickle cell disease by Bluyé DeMessie, Muhammed Amir Essibayi, Alireza Karandish, Shreya Nandi, Dhrumil Vaishnav, Lyanna Gomez, Kainaat Javed, Adisson Fortunel, Nathan Farkas, Kaitlin L. Strumph, Deepa G. Manwani, Mandana Behbahani, Deepak Khatri, David Altschul in The Neuroradiology Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.