
Abstract
Dural venous sinus injury (DVSI) can occur after traumatic brain injury and lead to impaired cerebral venous outflow through extrinsic compression, intraluminal thrombosis, or mixed mechanisms. It can progress to a sinus tear or transection with hemorrhage. On noncontrast-enhanced head CT, DVSI may be subtle and can be confounded by adjacent fractures, extra-axial blood products, and filling defects such as arachnoid granulations. Although the reported incidence of severe head injury is 1–4%, modern trauma imaging has revealed a substantially higher burden of DVSI and dural venous sinus thrombosis (DVST) in patients with skull base and calvarial fractures, particularly when fractures cross or overlie major sinuses or the jugular bulb. This narrative review focuses on acute post-traumatic dural venous sinus injury and synthesizes current knowledge on the angiographic anatomy. We also highlight the strengths and limitations of CT venography (CTV), MR venography (MRV), and adjunctive digital subtraction angiography in detecting DVSI, differentiating intraluminal thrombus from extrinsic compression, and characterizing collateral pathways. Finally, we review management strategies, including neurosurgical decompression for mechanically compressed sinuses, the non-standardized use of systemic anticoagulation for DVST in the presence of a hemorrhage, and the role of detailed venographic mapping for operative planning. Timely recognition of these injuries and their complications, guided by a systematic venographic approach, is essential for mechanism-based management that may reduce the risk of serious sequelae including venous infarction.
Keywords
Introduction
The dural venous sinuses are channels formed where the periosteal and meningeal layers of the dura mater separate. They are essential for the venous drainage of blood from the brain to the internal jugular veins.1,2 Dural venous sinus injuries (DVSIs) typically occur secondary to acute traumatic head injuries (TBIs).3,4 DVSI is a term that can include a spectrum of injury mechanisms including extrinsic sinus compression, intraluminal thrombosis (dural venous sinus thrombosis; DVST), and frank sinus laceration or transection.3,5,6 The reported incidence of traumatic DVSI varies substantially by population and injury type.4,7 Post-traumatic DVST appears to occur in about 4% of all-comer TBI populations. In higher-risk patients with skull fractures adjacent to or traversing a dural venous sinus, reported prevalence is substantially higher, including 13.9% in a recent prospective intensive care unit (ICU) cohort, 23% to 40.7% in retrospective computed tomography venography (CTV) cohorts, and 26.2% in a meta-analysis.7–11 However, detection of these injuries is increasing due to the use of dedicated venographic imaging in acute trauma settings.7,8 Dural venous sinus thrombosis (DVST) is a thrombotic manifestation of DVSI that is also being diagnosed with a consistently increasing frequency in patients with skull fractures, regardless of age group or brain injury severity.7,11,12 Outcomes for DVSI are variable and depend on the injury site and extent, with injuries in the posterior third of the sinus system having the highest mortality rates.8,13 Early imaging-based diagnosis of DVSIs is crucial for addressing potentially treatable complications and improving patient outcomes. 14 Additionally, DVSI on initial noncontrast CT can be obscured by adjacent trauma and unrecognized outflow obstruction can rapidly progress to venous infarction or hemorrhage.3,5,15,16 This narrative review focuses on acute post-traumatic dural venous sinus injury, excluding non-traumatic and spontaneous cerebral venous thrombosis, and summarizes the angiographic anatomy of the major dural venous sinuses, highlights the role of CTV in diagnosing DVSI, describes key radiologic signs, discusses the anatomic basis and proposed pathophysiology of these injuries, outlines management considerations, and presents illustrative cases of DVSI secondary to TBI.
Methods
A literature search was conducted using PubMed and Google Scholar using keywords such as dural venous sinus injury, traumatic dural venous sinus thrombosis, cerebral venous thrombosis, traumatic brain injury, skull fracture, depressed skull fracture, CT venography, MR venography (MRV), digital subtraction angiography, superior sagittal sinus, transverse sinus, sigmoid sinus, cavernous sinus, jugular bulb, torcular Herophili, venous sinus compression, venous sinus occlusion, venous infarction, anticoagulation, blunt cerebrovascular injury, epidural hematoma, arachnoid granulation, sinus thrombosis classification, and venographic anatomy. Illustrative cases were selected from institutional teaching files if they demonstrated acute post-traumatic dural venous sinus injury on CT venography, including examples of extrinsic compression, intraluminal thrombosis, mixed injury patterns, or associated complications such as venous infarction. Cases were excluded if dedicated venographic imaging was unavailable, if the imaging findings were non-diagnostic or indeterminate, or if the injury pattern did not illustrate a distinct mechanism or teaching point relevant to the scope of this review.
Anatomic considerations
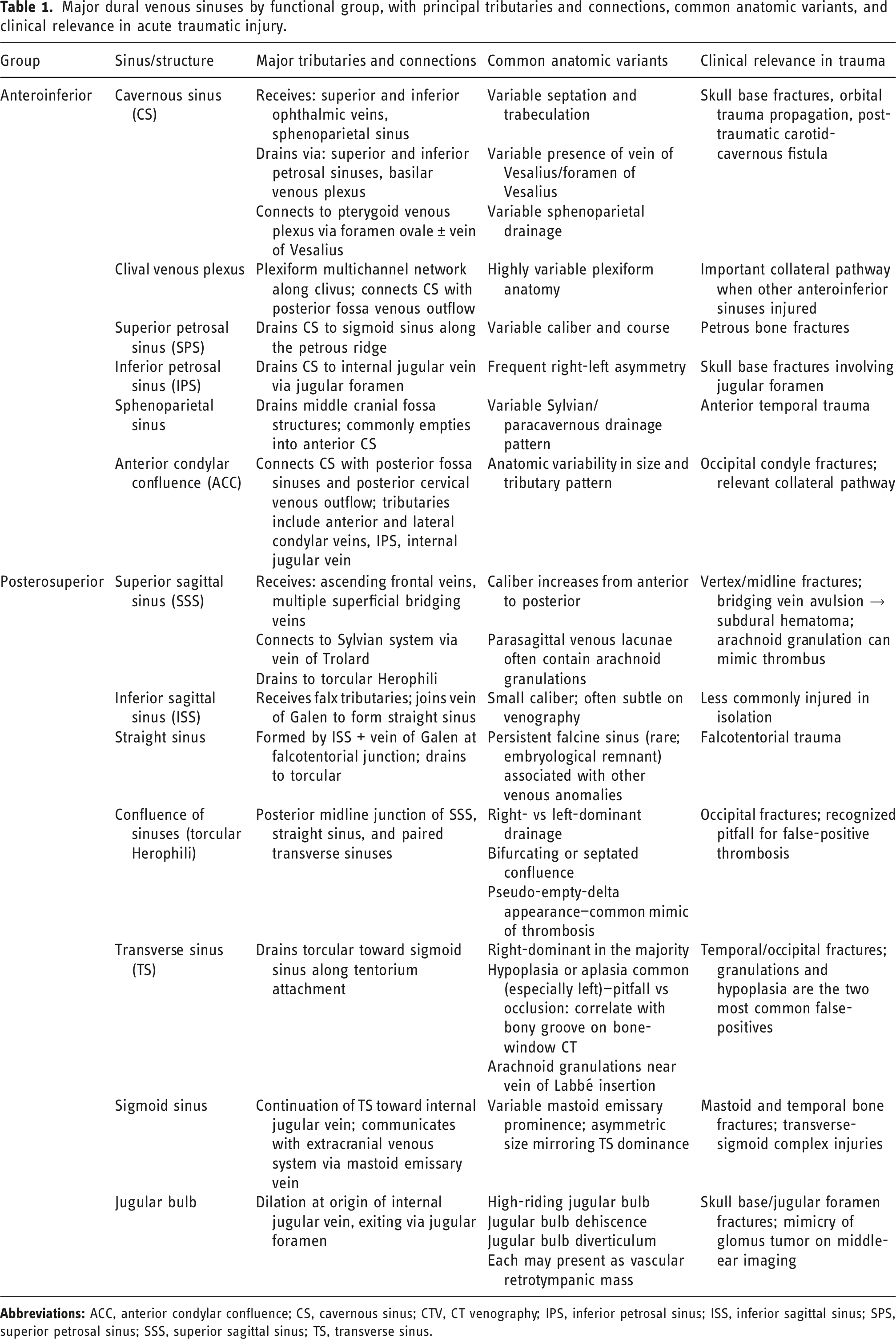
Major dural venous sinuses by functional group, with principal tributaries and connections, common anatomic variants, and clinical relevance in acute traumatic injury.
Anteroinferior dural venous sinus group
The anteroinferior group of dural venous sinuses includes the cavernous sinus (CS), the clival venous plexus (CVP), the superior and inferior petrosal sinuses (SPS and IPS), and the sphenoparietal sinus (SpPS) (Figure 1).25,26 The paired set of cavernous sinuses surrounds the pituitary fossa and communicates via the anterior and posterior intercavernous channels (Figure 1(B)).1,25,26 The CVP is a plexiform, fenestrated, multichannel venous network along the clivus that provides critical collateral pathways by connecting the CS with posterior fossa venous outflow at the skull base.1,25–27 The CS is a significant part of the anteroinferior dural venous sinus group, as it receives orbital, facial, meningeal, and skull base venous drainage.25,26 A. DSA AP view, B. Petrosal venogram, and C. lateral DSA demonstrating structures of the anteroinferior group of dural sinuses including the cavernous sinus (CS), superior petrosal sinus (SPS), inferior petrosal sinus (IPS), clival venous plexus (CVP), and the intercavernous (IC) sinus connecting both CSs. The sphenoid emissary vein (vein of Vesalius, V) can be seen draining the cavernous sinus (C) into the pterygoid venous plexus (PVP). Other structures demonstrated in the images include the internal jugular veins (IJV), the jugular bulb (J), the sigmoid sinus (SigS), transverse sinus (TS), and vertebral artery (VA).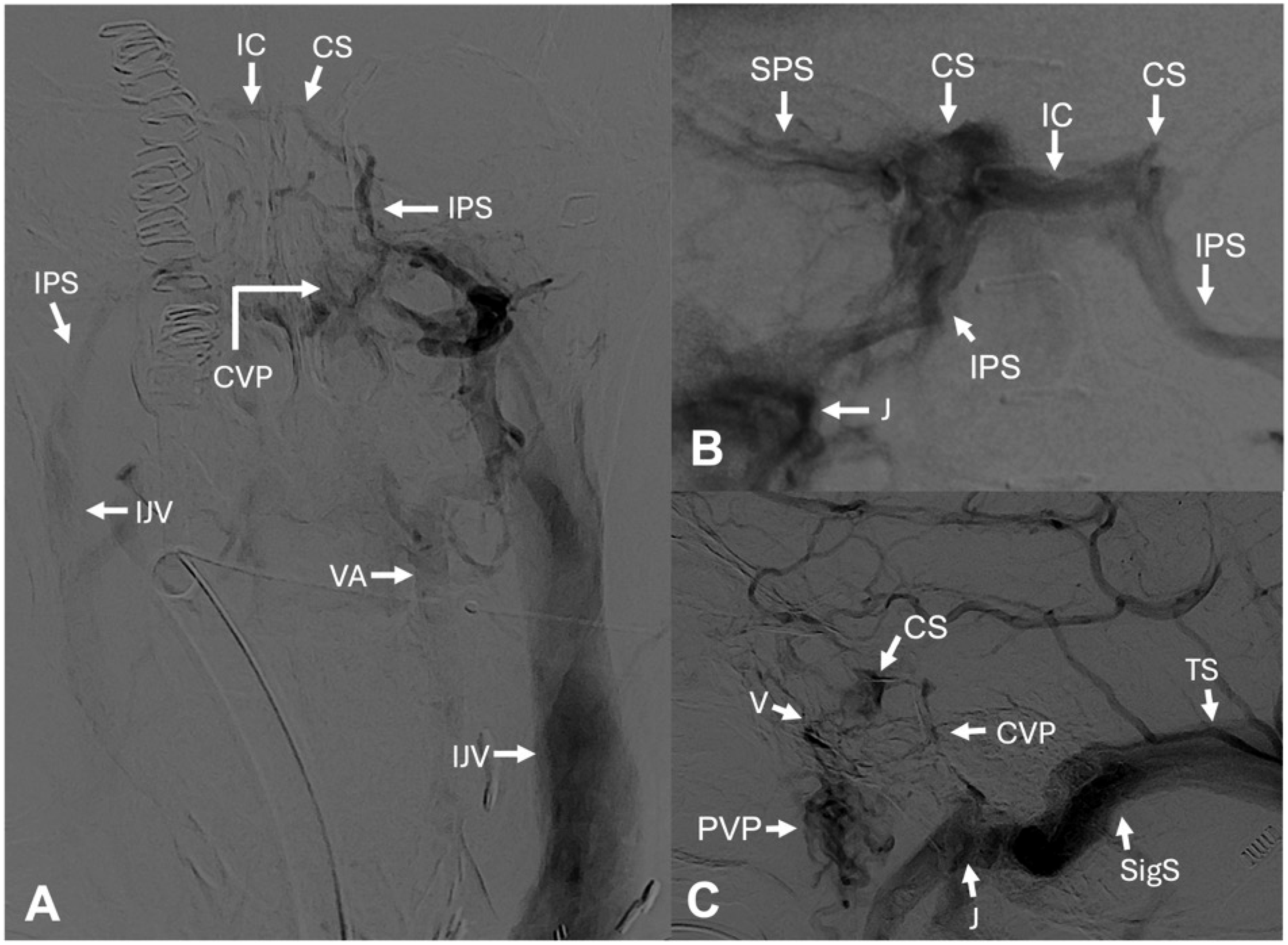
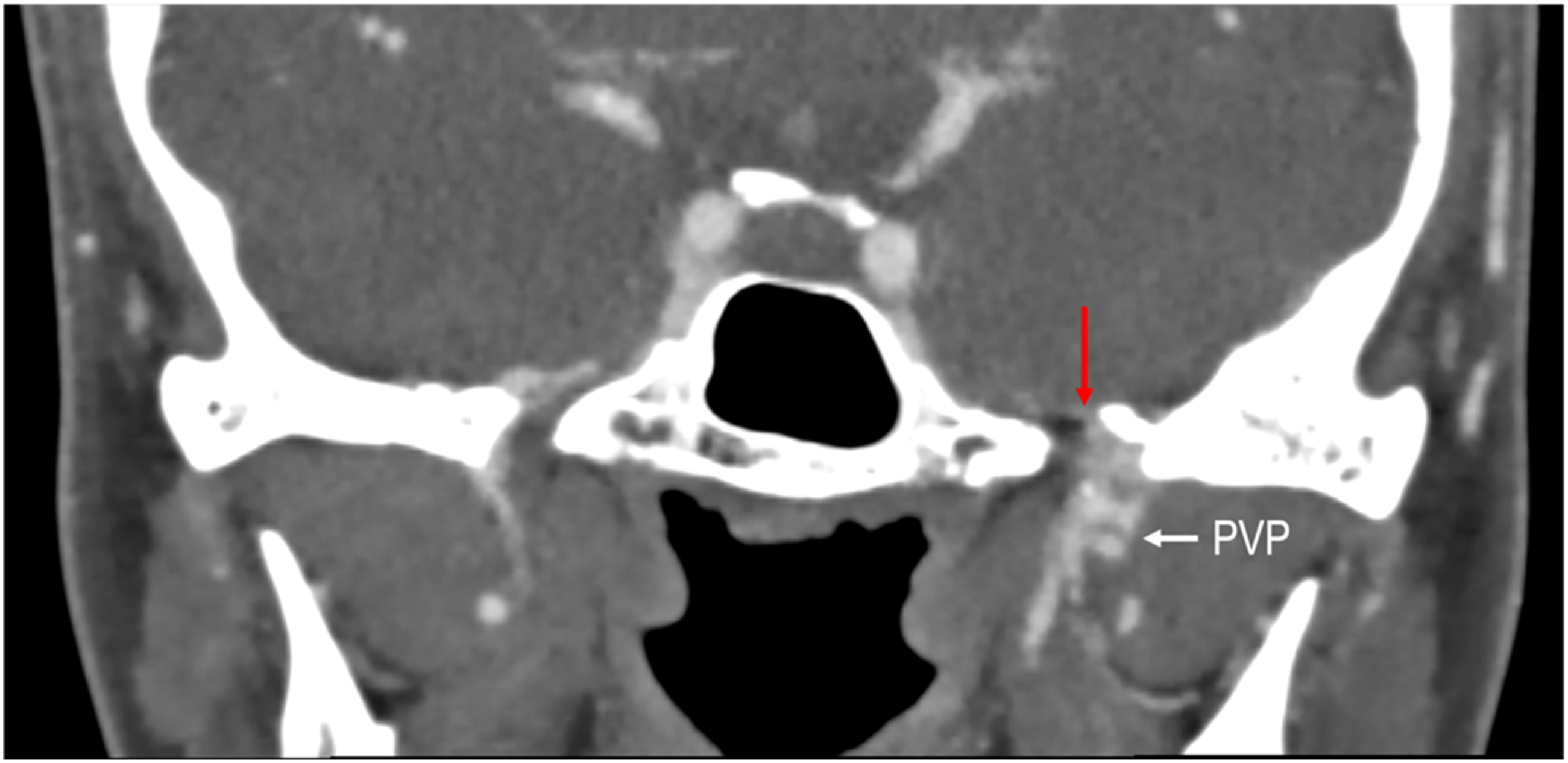
Anteriorly, orbital and facial drainage reaches the CS predominantly via the superior and inferior ophthalmic veins; inferiorly, the CS communicates with the pterygoid venous plexus through emissary veins traversing the skull base foramina, most often the foramen ovale and, when present, the foramen of Vesalius (Figures 2 and 3).3,25,26,28 Posteriorly, the CS drains via the superior and inferior petrosal sinuses toward the sigmoid sinuses and internal jugular veins, with additional collateral pathways through the basilar venous plexus and the anterior condylar confluence (ACC).1,14,25,26 Axial head CT depicting a corticated foramen of Vesalius (red arrow). A, B. Coronal head CT angiogram showing the venous plexus (red arrow) contained within the foramen ovale that drain into the pterygoid venous plexus (PVP) (white arrow).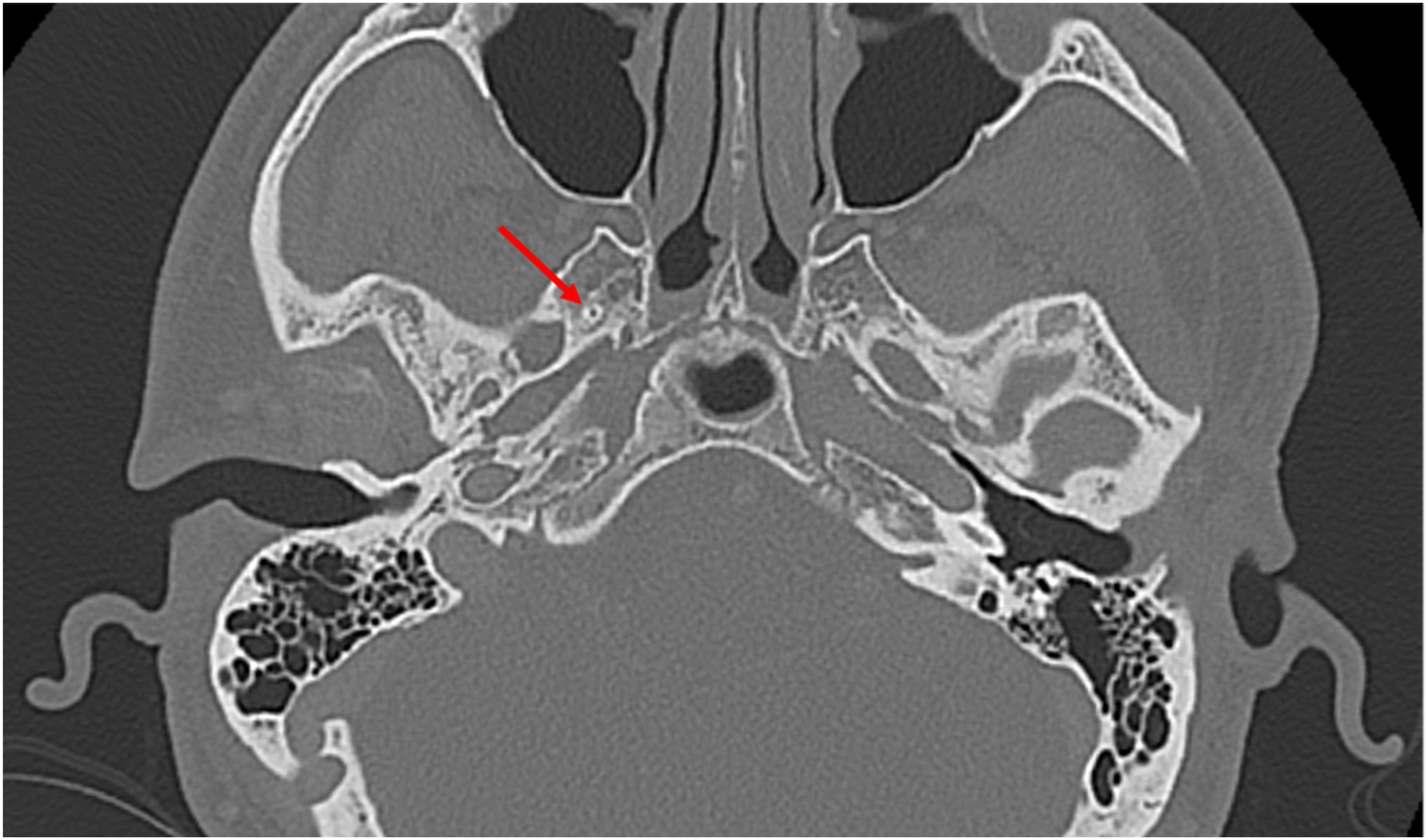
Posterosuperior dural venous sinus group
Another important group of the dural venous sinuses is the posterosuperior group, which includes the superior sagittal sinus (SSS), inferior sagittal sinus (ISS), straight sinus (SS), sinus confluence (torcular Herophili [TH]), transverse sinuses (TS), sigmoid sinuses (SigS), and jugular bulbs (J) (Figure 4).
17
The SSS is a large midline dural venous sinus that originates anteriorly from the ascending frontal veins and travels along the superior margin of the falx cerebri, which parallels the inner calvarial vault.
17
The caliber of the SSS increases along its course from the anterior cranial fossa to the confluences of sinuses in the posterior skull.
17
Along its course, the SSS receives venous drainage from numerous small superficial (bridging) veins.
17
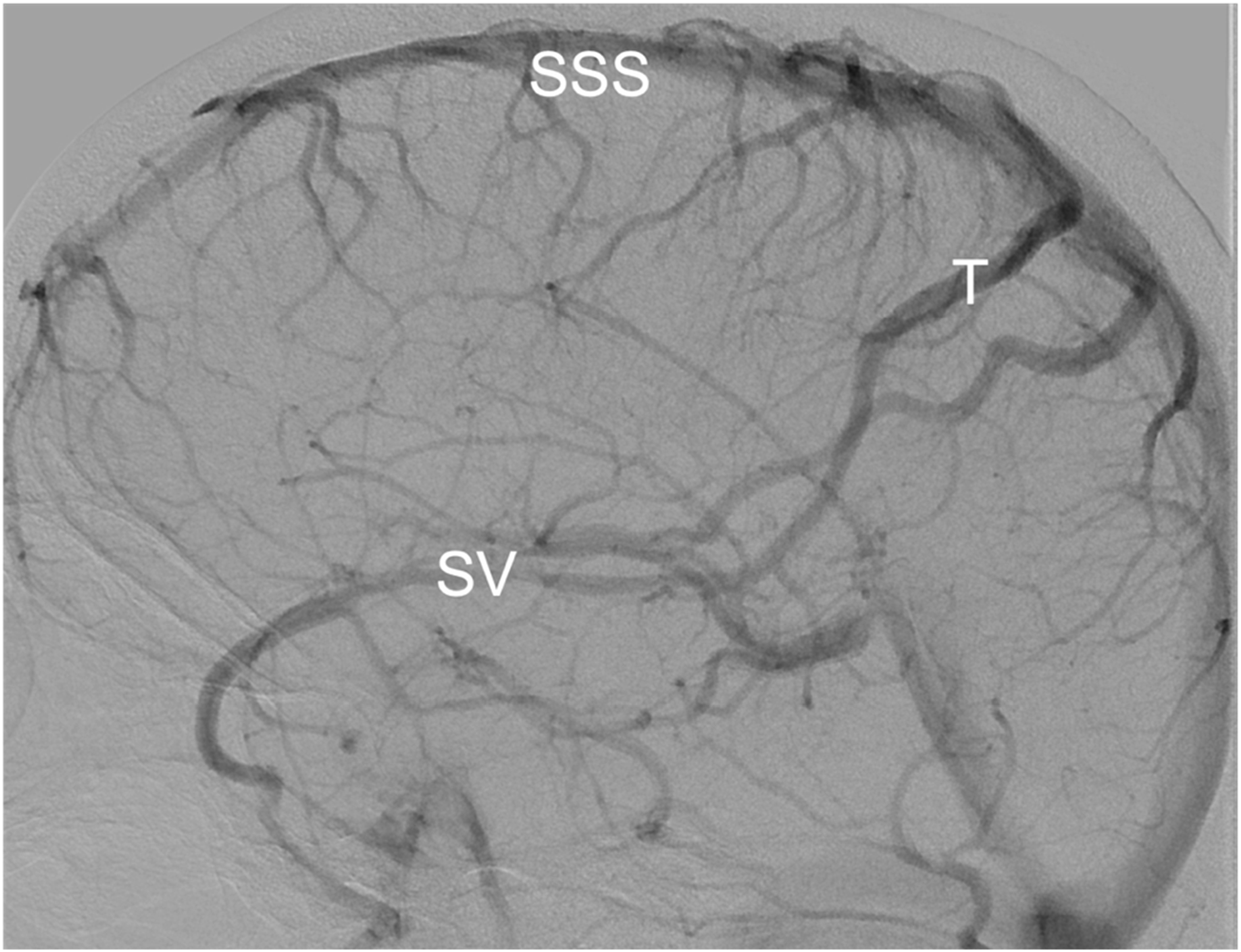
Adjacent to the SSS are parasagittal venous lacunae that can contain arachnoid granulations.29,30 These arachnoid granulations participate in CSF resorption and can be seen as physiologic filling defects on venography.29,30 The SSS is also connected to the superior middle cerebral (Sylvian) venous system by major superficial anastomotic pathways, such as the superior anastomotic vein of Trolard (Figure 5).
17
Sagittal cross-section illustration of the skull demonstrating the posterosuperior dural venous sinus group including the superior sagittal sinus (SSS), inferior sagittal sinus (ISS), straight sinus (SS), sinus confluence (torcular Herophili [TH]), transverse sinuses (TS), sigmoid sinuses (SigS), and jugular bulbs (J). Digital subtraction angiography (DSA) during the venous phase depicting the superior sagittal sinus (SSS) and superior anastomotic vein of Trolard (T), that is connected to the superficial middle cerebral vein or Sylvian vein (SV).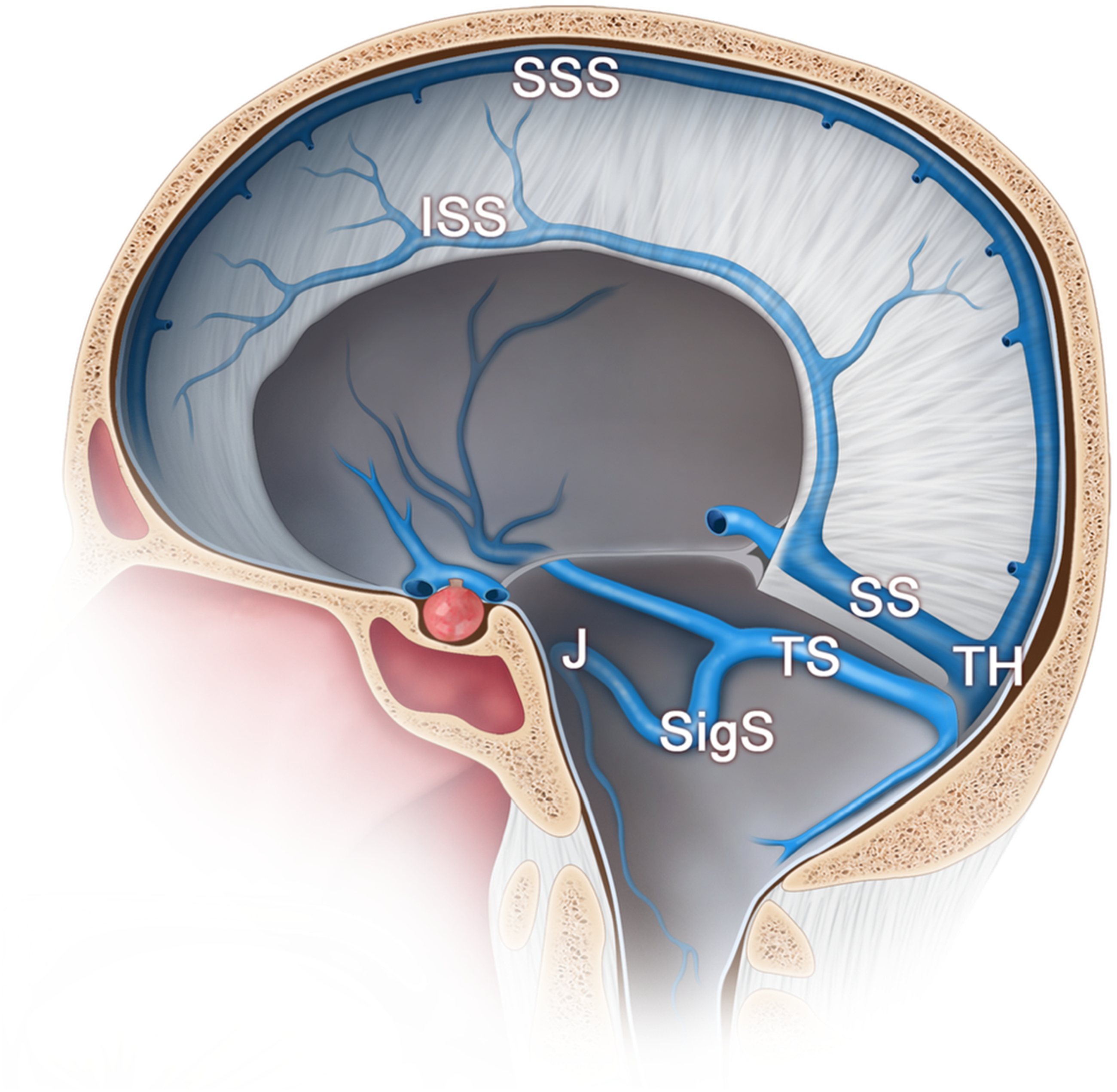
The ISS is relatively small when compared to the SSS and lies midline, coursing along the inferior margin of the falx cerebri.
17
Venous blood from the internal cerebral and basal veins drains into the great cerebral vein (vein of Galen), which anastomoses with the ISS at the falcotentorial junction to form the straight sinus (Figure 6(A)).1,17 The straight sinus then travels posteroinferiorly along the junction of the falx cerebri and tentorium cerebelli.
17
The straight sinus can receive numerous small tributaries from the falx and tentorium and later drain towards the confluence of sinuses (torcular Herophili [TH]), where it interfaces with the transverse sinus system.
17
A. Lateral and B. posterior view digital subtraction angiography (DSA) in the venous phase depicting the transverse sinuses (TS), the sinus confluence (TH) (white arrow), sigmoid sinus (SigS), jugular bulbs (J), and internal jugular veins (IJV).
The confluence of sinuses is the posterior midline venous junction where the superior sagittal sinus and straight sinus connect with the pair of transverse sinuses.1,21,24,31 The confluence of sinuses has several anatomical variants, including asymmetry due to right- or left-dominance and bifurcating or septated confluence patterns. From the torcular, the transverse sinuses travel laterally along the margin of the tentorium cerebelli toward the petrous temporal bone, where they turn inferiorly in the sigmoid sulcus and become the sigmoid sinuses. 17 The transverse and sigmoid sinus systems can also communicate with the extracranial venous system through emissary veins, such as the mastoid emissary vein.20,32 The sigmoid sinuses are the inferior continuation of the transverse sinuses, which descend posterior to the petrous temporal bone and terminate by becoming the internal jugular veins (Figure 6(B)). 17 The jugular bulbs are superior dilatations at the origin of the internal jugular veins, which can exhibit several anatomic variants (e.g., high-riding jugular bulb, dehiscence, or a diverticulum), which are essential to recognize because they can present as vascular retrotympanic masses and be misdiagnosed as a glomus tumor or other vascular middle-ear or internal auditory canal lesions.19,31,33
Imaging of dural venous sinus injuries
Currently, there is no universally accepted algorithm for the imaging evaluation of acute post-traumatic dural venous sinus injury (DVSI), and practices vary between institutions and clinical scenarios.15,30,34 In traumatic brain injury, a skull fracture or epidural hematoma overlying a dural venous sinus increases the risk for developing DVST and should prompt evaluation with venographic imaging.15,35,36 Because thrombosis and occlusive sinus injury are challenging to identify on noncontrast-enhanced CT imaging alone, venographic imaging is often required for adequate characterization and differentiation.37,38 When DVSI is suspected, CTV or MRV are the primary imaging modalities used to define the extent of injury and detect thrombosis.1,9,39 Patterns of non-opacification on CTV/MRV can help differentiate between the mechanism of injury, including intraluminal thrombosis, extrinsic compression/stenosis, or a combination of both.3,5,40 In the setting of acute trauma, CTV is often favored over MRV because it offers fast image acquisition and can be integrated into pre-existing CT-based trauma protocols.9,24,41 Furthermore, CTV post-processing with thin-section multiplanar reformats, maximum-intensity projections, and 3D renderings can improve anatomic depiction and help define the length and severity of injury.24,28,31 Additionally, advanced CT post-processing techniques, including dual-energy bone-removal CT venography, may further enhance diagnostic confidence by improving separation of contrast-opacified dural venous sinuses from adjacent skull base bone.28,31 Distinguishing true intraluminal thrombosis from adjacent extra-axial hemorrhagic compression still relies primarily on multiplanar venographic assessment. 42
Comparison of imaging modalities for evaluation of acute post-traumatic dural venous sinus injury.
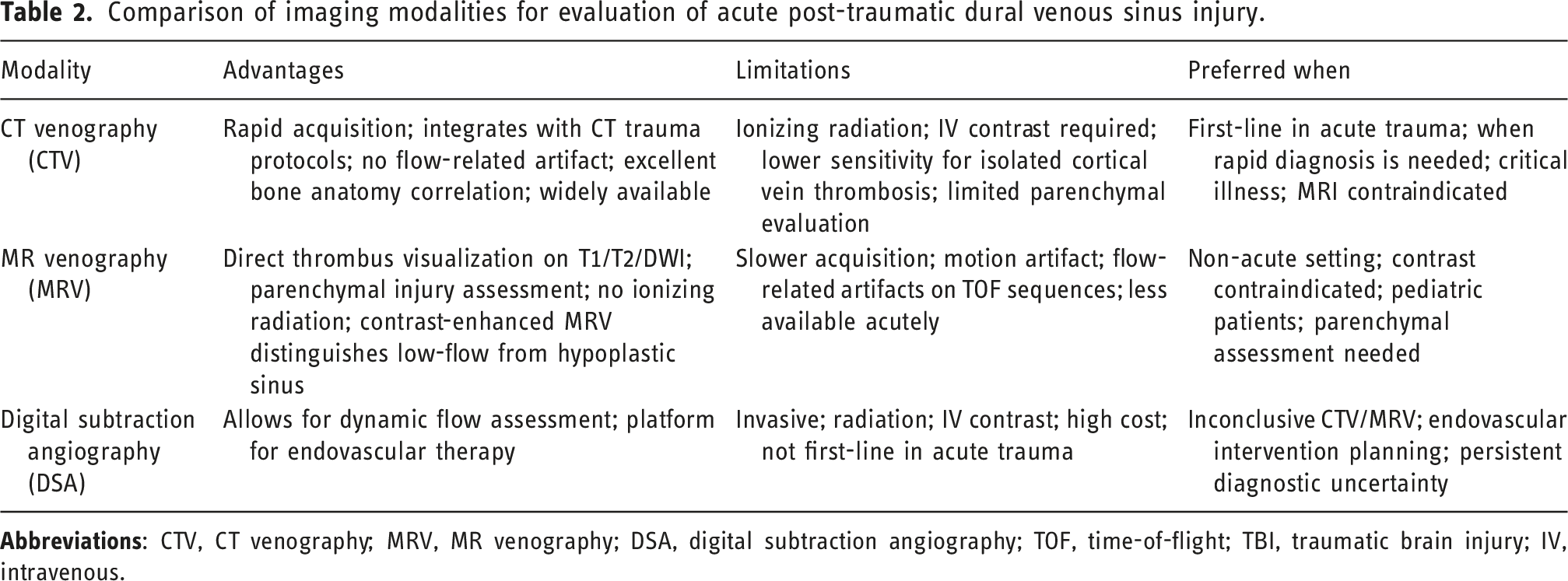
MRI/MRV can be used to characterize parenchymal sequelae and cortical vein involvement.1,39,41 However, time-of-flight and phase-contrast MRV sequences can be susceptible to flow-related artifacts.1,22,45 Contrast-enhanced MRV can better depict accurate luminal filling and help distinguish decreased flow from a hypoplastic sinus.1,22,45 MRV can be suited for long-term follow-up imaging and may be preferred in cases where contrast administration or ionizing radiation is undesirable, especially in pediatric patients.15,23,39,46,47
Additional imaging with digital subtraction angiography (DSA) is usually reserved for cases in which venographic imaging is inconclusive or for planning/performing endovascular interventions.19,39,45 Ultimately, venographic imaging helps distinguish intraluminal thrombus from extrinsic compression and detect complications, including venous congestion, infarction, or hemorrhage.3,6,11
Radiologic signs of acute traumatic dural venous sinus injury
Direct and indirect radiologic signs of acute traumatic dural venous sinus injury, with the best imaging modality for detection and the most clinically relevant mimics or interpretive pitfalls.
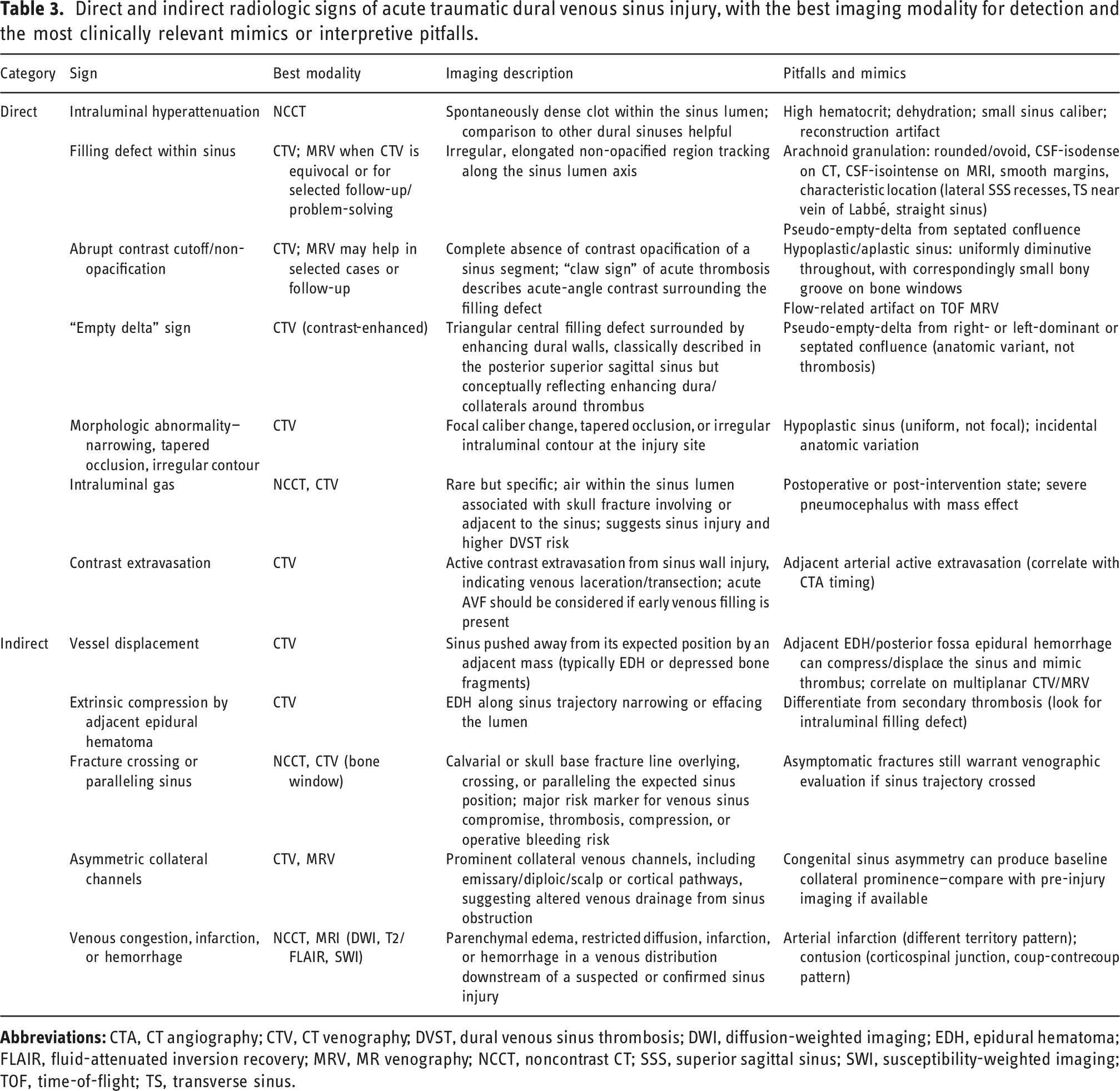
Direct signs of DVSIs can manifest as abnormalities in blood flow (opacifications) and vessel morphology.5,39 A key finding associated with venous injury is the lack of filling or complete occlusion of a sinus segment, which may appear as an abrupt cutoff of contrast on CTV (Figure 7).
5
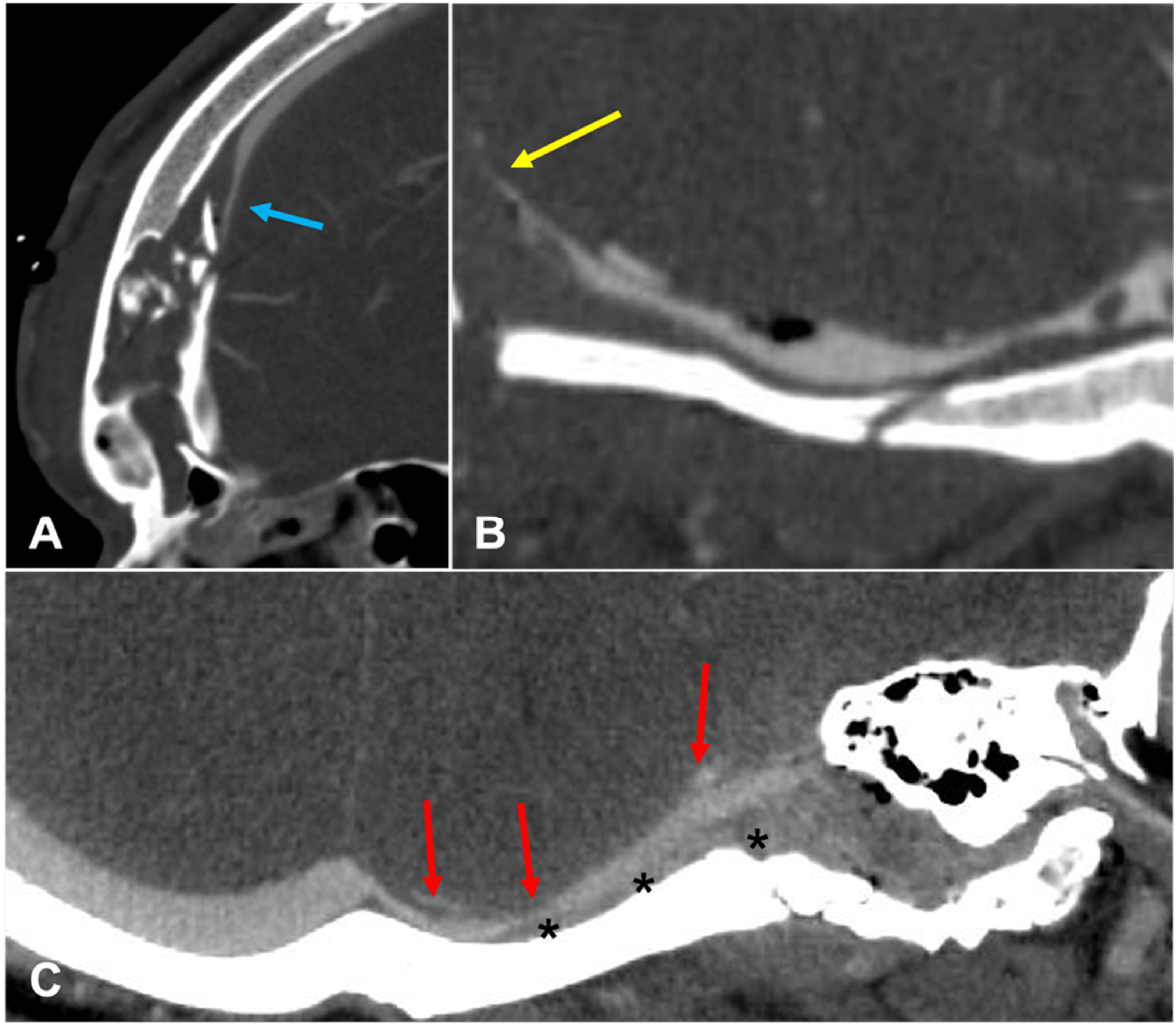
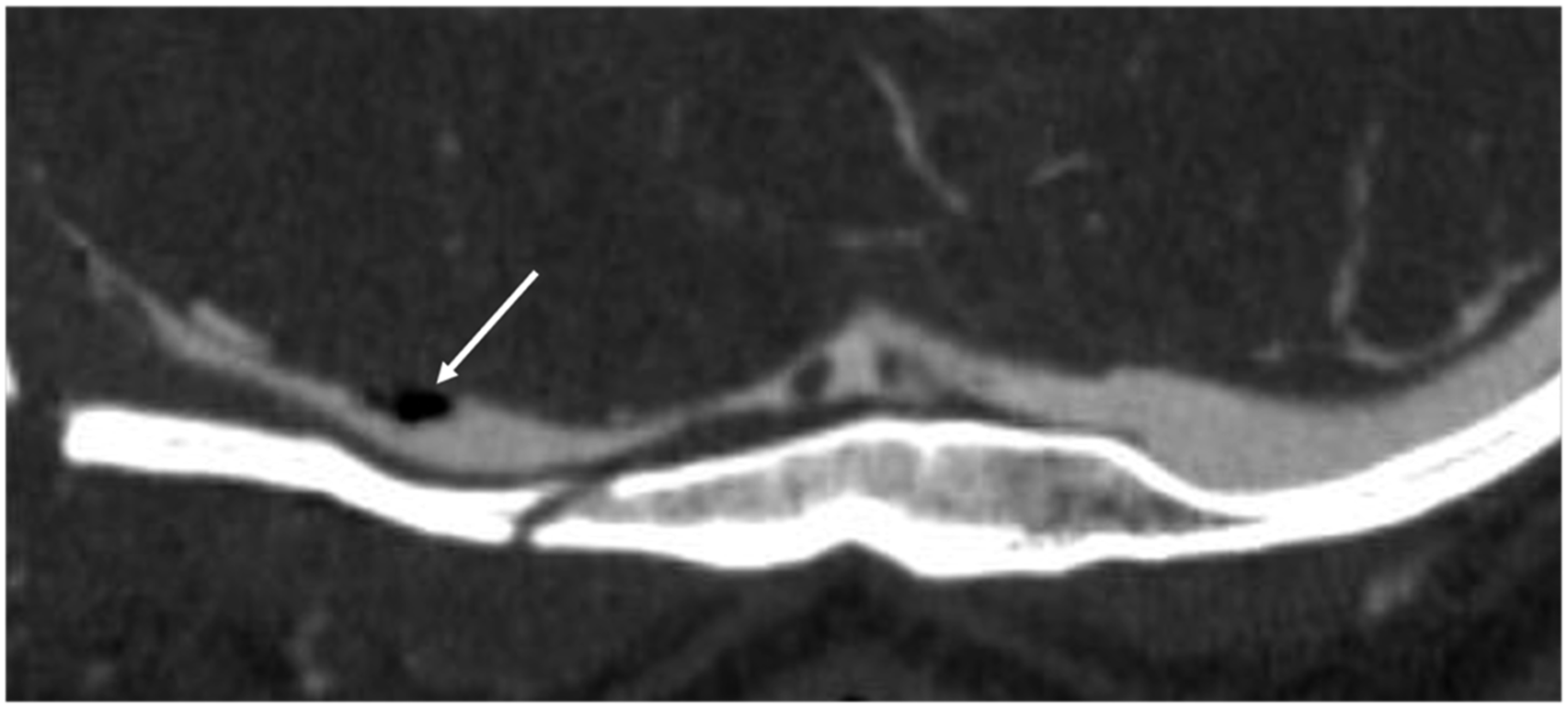
For example, an intraluminal thrombosis may present as a hyperattenuating clot within the sinus on noncontrast CT and as a filling defect on CTV (classically described as an “empty delta” appearance in some cases).48,50 Furthermore, morphologic changes such as narrowing, tapered occlusion, and an irregular contour are additional direct indicators of venous injury (Figure 8).5,43 Another rare but specific sign of venous injury is the presence of intraluminal gas (Figure 9).48,49 A. Axial noncontrast-enhanced CT demonstrating a hyperattenuating clot (red arrow). B. CT venogram demonstrating the corresponding filling defect (red arrows) and associated diastatic fracture (yellow arrow). A–C. CT venogram demonstrating a change in caliber and narrowing (blue arrow), tapered occlusion (yellow arrow), and irregular contour (red arrows) with vessel displacement (asterisks). Axial CT venogram demonstrating intraluminal gas (arrow).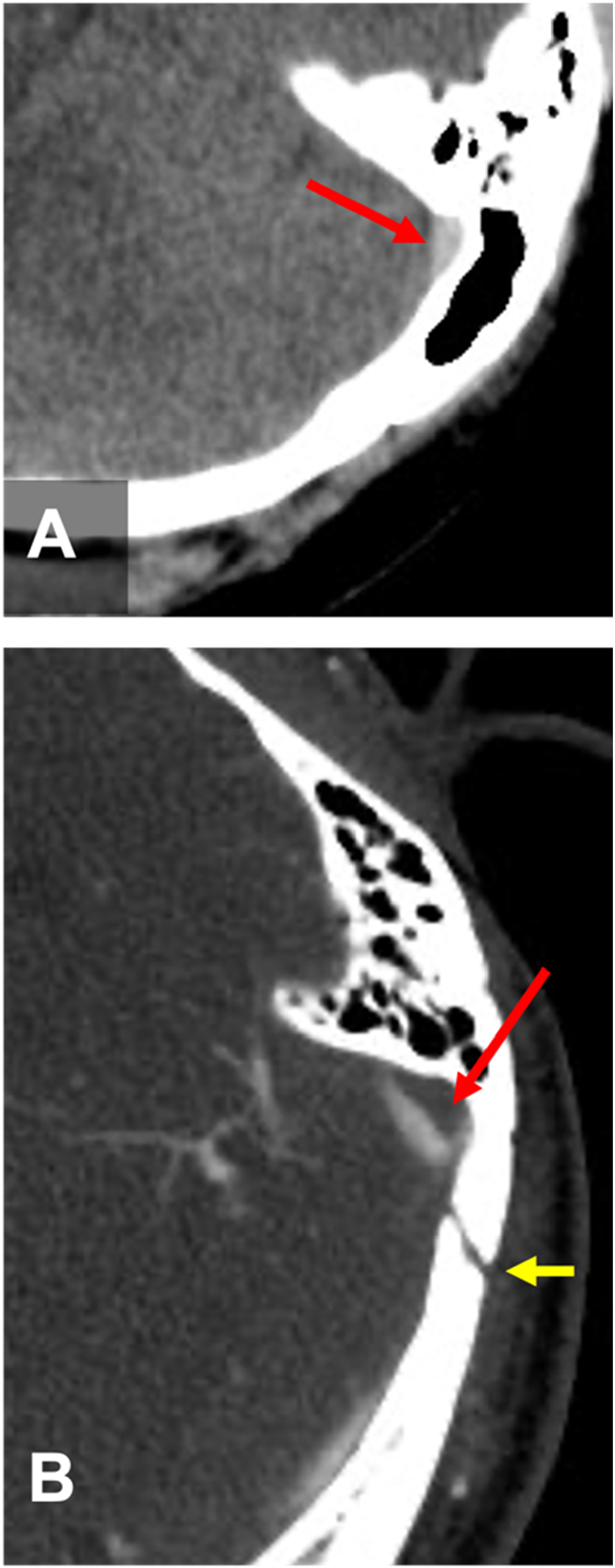
Indirect signs of DVSIs reflect secondary effects on the dural sinuses from injury to surrounding structures.
5
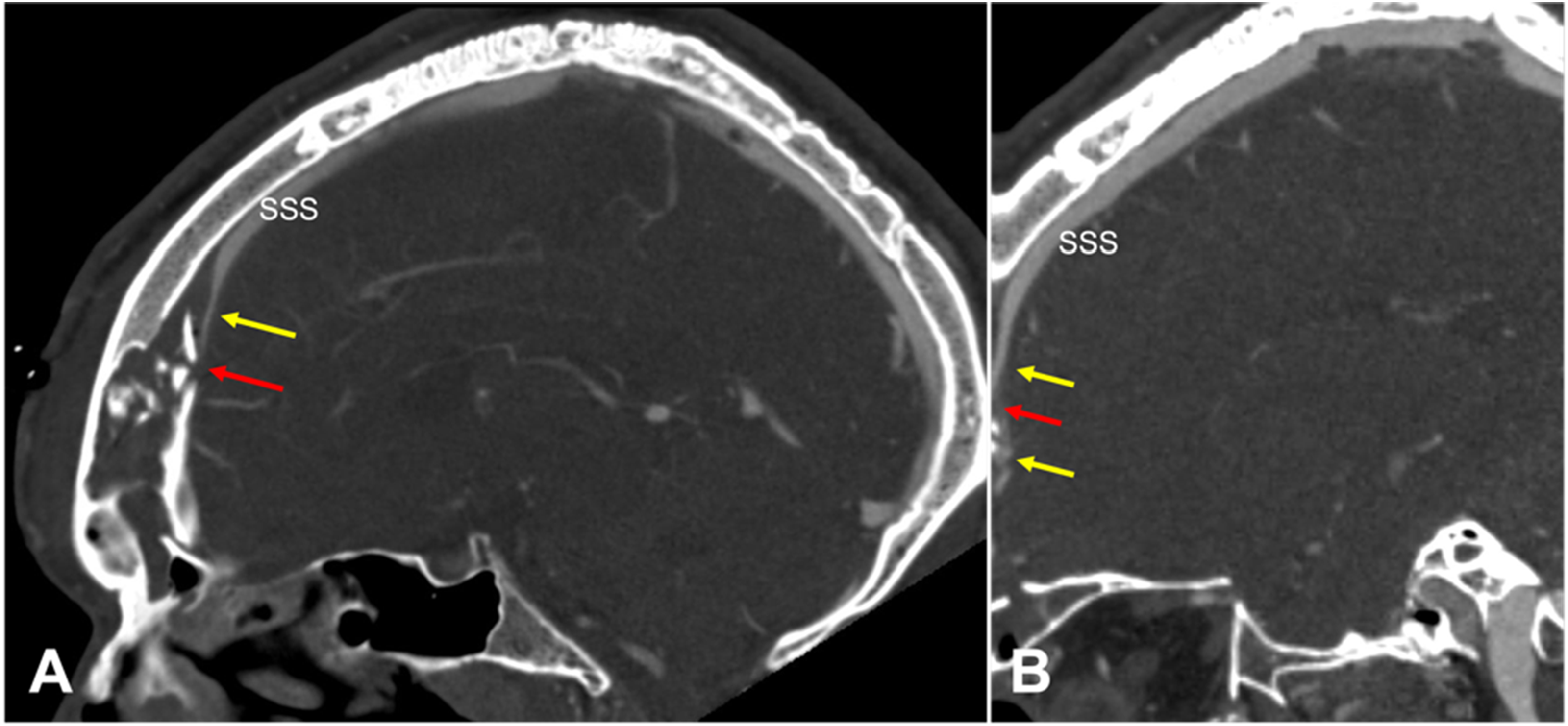
Vessel displacement and extrinsic compression are significant indirect findings that are frequently caused by an adjacent epidural hematoma due to a calvarial fracture overlying the sinus (Figures 10 and 11).5,51 The presence of a diastatic or depressed skull fracture that crosses or lies parallel to a dural sinus is another critical indirect finding and primary risk factor for both laceration and secondary thrombotic or compressive injury.50–52 When present, asymmetric collateral venous channels or distal reconstitution can further support a focal traumatic abnormality rather than a global timing or technique issue.11,51 A. Axial CT venogram and B. 3D reconstruction demonstrating vessel displacement (red arrows) by venous epidural hematoma (white arrows). A. Sagittal CT venogram, B. axial head CT, and C. 3D reconstruction demonstrating a calvarial fracture (yellow arrows) with epidural hematoma (EDH) (white arrow in panel A) causing extrinsic compression and narrowing of the superior sagittal sinus (SSS).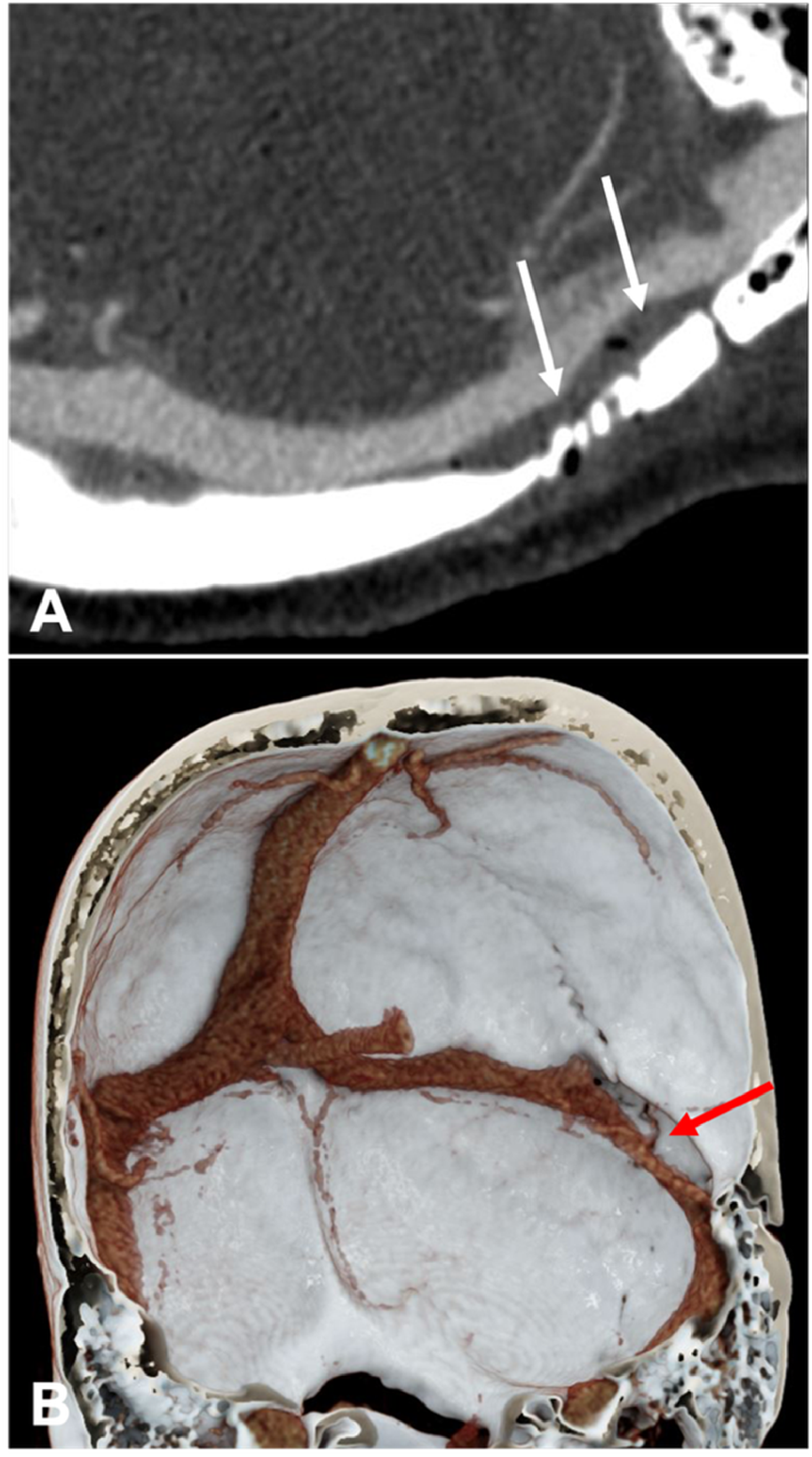
There are two important imaging pitfalls: arachnoid (Pacchionian) granulations and congenital transverse sinus hypoplasia or atresia. First, arachnoid (Pacchionian) granulations typically appear as focal rounded filling defects with CSF-like attenuation on CT and signal intensity similar to CSF on MRI.1,16,18,19 Giant arachnoid granulations may not parallel CSF on all MRI sequences. They are commonly seen in the transverse sinus, especially laterally near the vein of Labbe or lateral tentorial sinus.1,16,18,19 Giant arachnoid granulations have also been described in the superior sagittal and straight sinuses.1,16,18,19 In contrast, an intraluminal thrombus typically appears elongated or irregular, extending along the sinus rather than forming a short rounded defect.1,5,18 An acute venous thrombosis may appear as an elongated hyperattenuating clot on noncontrast CT, and intrinsic thrombus on CTV may produce an acute-angle “claw sign” of contrast partially or completely surrounding the thrombus.1,5,18 Second, a hypoplastic or atretic transverse sinus can simulate sinus occlusion, particularly on time-of-flight MR venography, where stagnation of blood flow in a normal but small nondominant transverse sinus may mimic thrombosis.1,16 Correlation with bone-window CT helps differentiate congenital hypoplasia from thrombosis.5,19,31 One important distinction is that congenitally small transverse or sigmoid sinuses are expected to have small jugular foramina or sigmoid sinus grooves, whereas thrombosed sinuses may be discrepant with the osseous anatomy and show intraluminal thrombus or absent contrast filling on CTV.5,19,31 Contrast-enhanced MR venography and CT venography can also help resolve this limitation because they are less susceptible to time-of-flight (TOF) flow gaps, and CT venography may directly show a patent hypoplastic transverse sinus.16,23
Classification and pathophysiology of dural venous sinus injuries
DVSIs can be classified by mechanism of injury. 5 Type A injuries are due to external compression from blood, air, or bone fragments, leading to a nonocclusive luminal narrowing. 5 Type B injuries involve a thrombosis of the venous sinus. 5 Finally, type C injuries are considered mixed, involving both compression and thrombus formation. 5 DVSI can also be classified by the extent of flow limitation. 5 Type 1 DVSI is non-occlusive and characterized by a narrowed but patent venous sinus. In contrast, type 2 DVSI occurs when there is complete luminal occlusion without contrast filling in the injured segment of the sinus. 5 Finally, type 3 injuries involve a transection or tear of the venous sinus with contrast extravasation and can cause the formation of an acute arteriovenous fistula. 5 This two-axis classification system was introduced by Schwartz et al. as a standardized radiologic grading scheme for traumatic dural venous sinus injury on CT venography. 5 However, the Schwartz grading scheme has not yet been externally validated or widely adopted into standard clinical practice, and other classification approaches remain in use. 5 Nevertheless, the system provides a descriptive structure: Type A (extrinsic compression), Type B (intrinsic thrombosis), and Type C (mixed). In selected cases compression or occlusion of the sinus may warrant neurosurgical evaluation, whereas thrombotic injury may raise consideration of anticoagulation, with treatment individualized to balance hematoma expansion against thrombus propagation or venous infarction.5,9,30,50,53
Acute post-traumatic dural venous sinus thrombosis (DVST) is a potentially fatal complication of traumatic brain injury and can be associated with venous congestion, hemorrhage, and worse clinical outcomes. 7 DVST more commonly occurs when depressed skull fractures or epidural hematomas are near a dural venous sinus, leading to a mechanical disruption of venous outflow and promoting thrombus formation.7,54 Overall, the risk of DVST is highest when a fracture extends to the dural sinus or jugular bulb. 11 Fractures of the petrous bone that extend towards the transverse sinus, sigmoid sinus, or jugular bulb have also been associated with the formation of DVST.11,55 When venous outflow obstruction is substantial, the resulting venous congestion can progress to edema, venous infarction, and hemorrhage. 15
Although the exact mechanism of DVST formation has not been fully defined, it may parallel Virchow’s triad: (1) endothelial injury from direct damage to the sinus wall, (2) hypercoagulability after trauma/TBI, and (3) venous stasis when depressed fracture fragments and/or an epidural hematoma compress the sinus. 7 One potential complication of DVST is venous hypertension, which can have a nonspecific clinical presentation and be masked by coexisting traumatic brain injury and other intracranial hemorrhage symptoms, making early imaging-based recognition important. 56 Because traumatic DVSI can present with intraluminal thrombus, external compression, or both, distinguishing these mechanisms is essential for subsequent monitoring and management.5,35
Several anatomic injury patterns are associated with increased risk of DVSI/DVST and other associated complications. In blunt head trauma, skull base fractures that extend to the dural venous sinus or the jugular bulb/foramen carry a high risk for developing post-traumatic dural venous sinus thrombosis or occlusion.10,11,54 Similarly, comminuted fractures of the mastoid, temporal, and adjacent occipital bone can damage the transverse-sigmoid sinus complex, especially when the fracture line (or associated epidural hematoma) overlies the dural venous sinus.3,9,40 Furthermore, temporal bone fractures can involve the otic capsule and are clinically significant because they can be associated with a higher likelihood of complications such as facial nerve injury and CSF leak.48,57,58 Compared with fractures that spare the otic capsule, otic capsule-violating fractures are more often associated with otologic and neurologic complications and therefore require early recognition.48,57,58
Penetrating cranial trauma can injure a dural venous sinus along the projectile path, leading to sinus wall disruption, intraluminal thrombosis, or extrinsic compression from adjacent hemorrhage.8,12,59,60 Projectile-related injuries, such as gunshot wounds, to the cranial sinuses are classically associated with severe hemorrhage and sinus thrombosis, warranting prompt evaluation due to the risk of massive blood loss and high perioperative mortality risk.8,12,59,60
Trauma causing midline/parasagittal calvarial fractures (especially depressed fractures) or vertex/parasagittal extra-axial hematomas overlying the sinus can lead to superior sagittal sinus injuries.8,13 Extensive venous outflow occlusion, particularly involving the middle or posterior third of the SSS, can be associated with venous congestion or infarction.50,60 Therefore, a targeted venographic assessment is warranted in cases of midline fractures with suspected dural sinus involvement to identify potential complications.11,40,41
Illustrative cases of dural venous sinus injuries: Imaging patterns
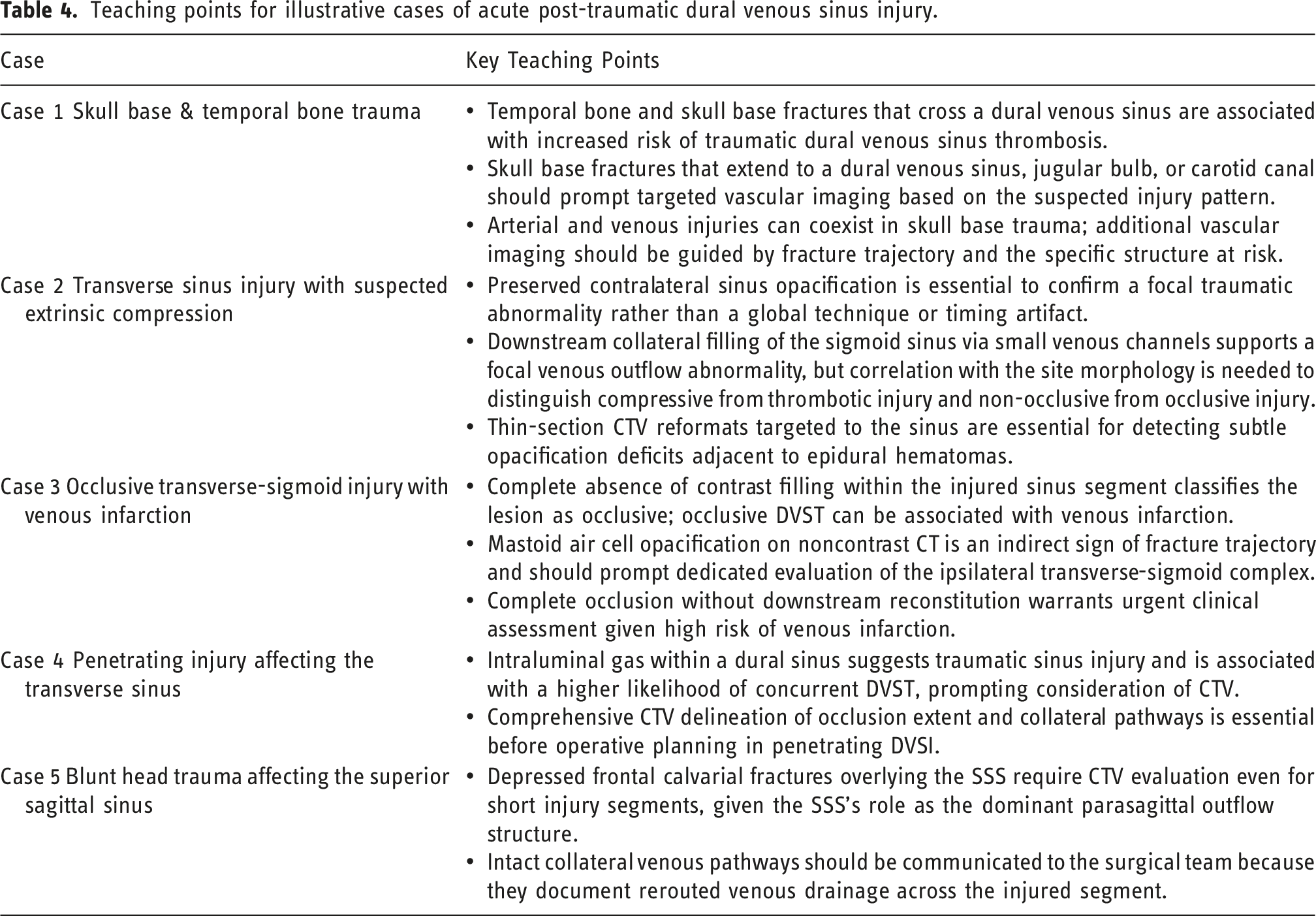
Teaching points for illustrative cases of acute post-traumatic dural venous sinus injury.
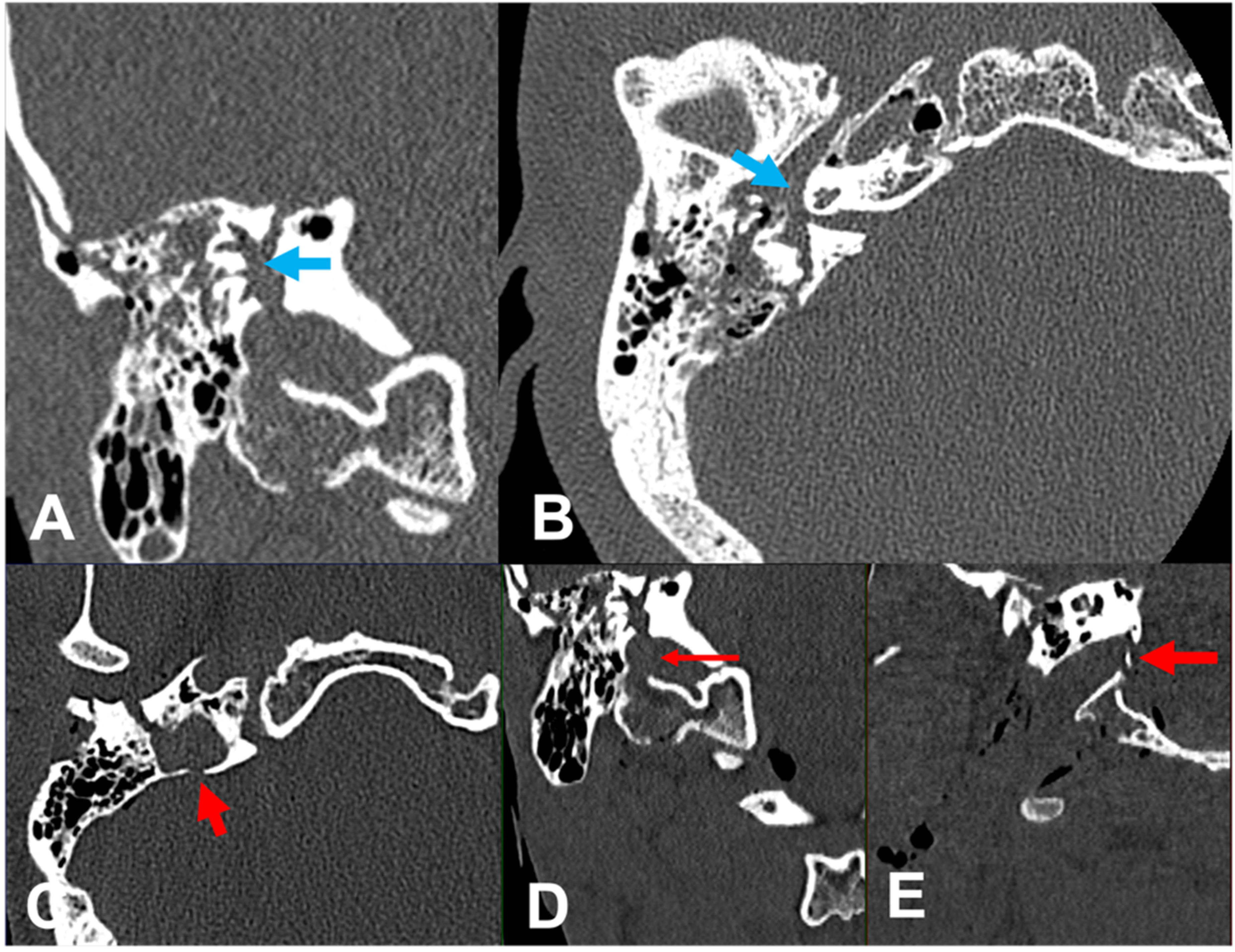
Case 1: Skull base and temporal bone trauma
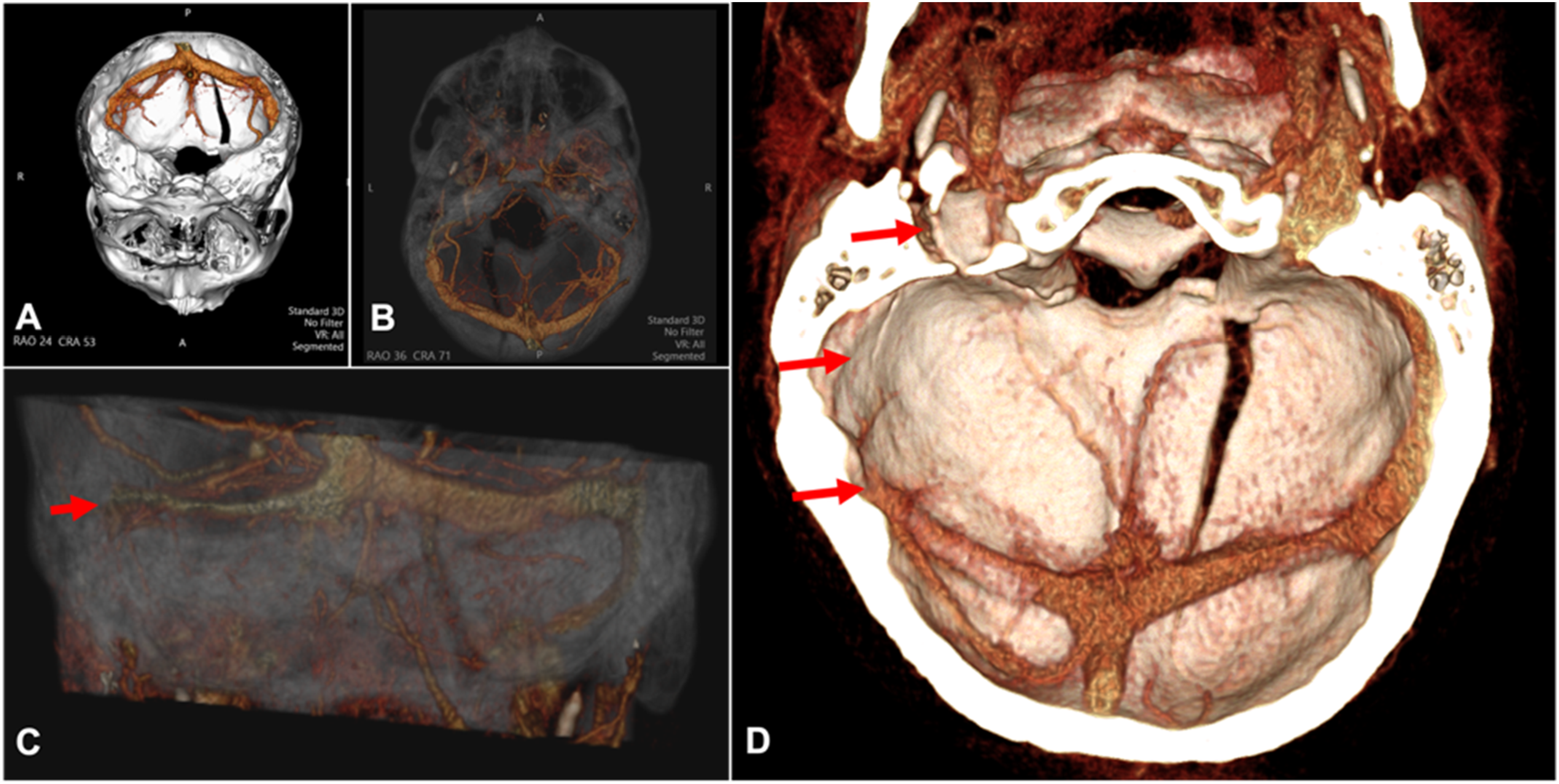
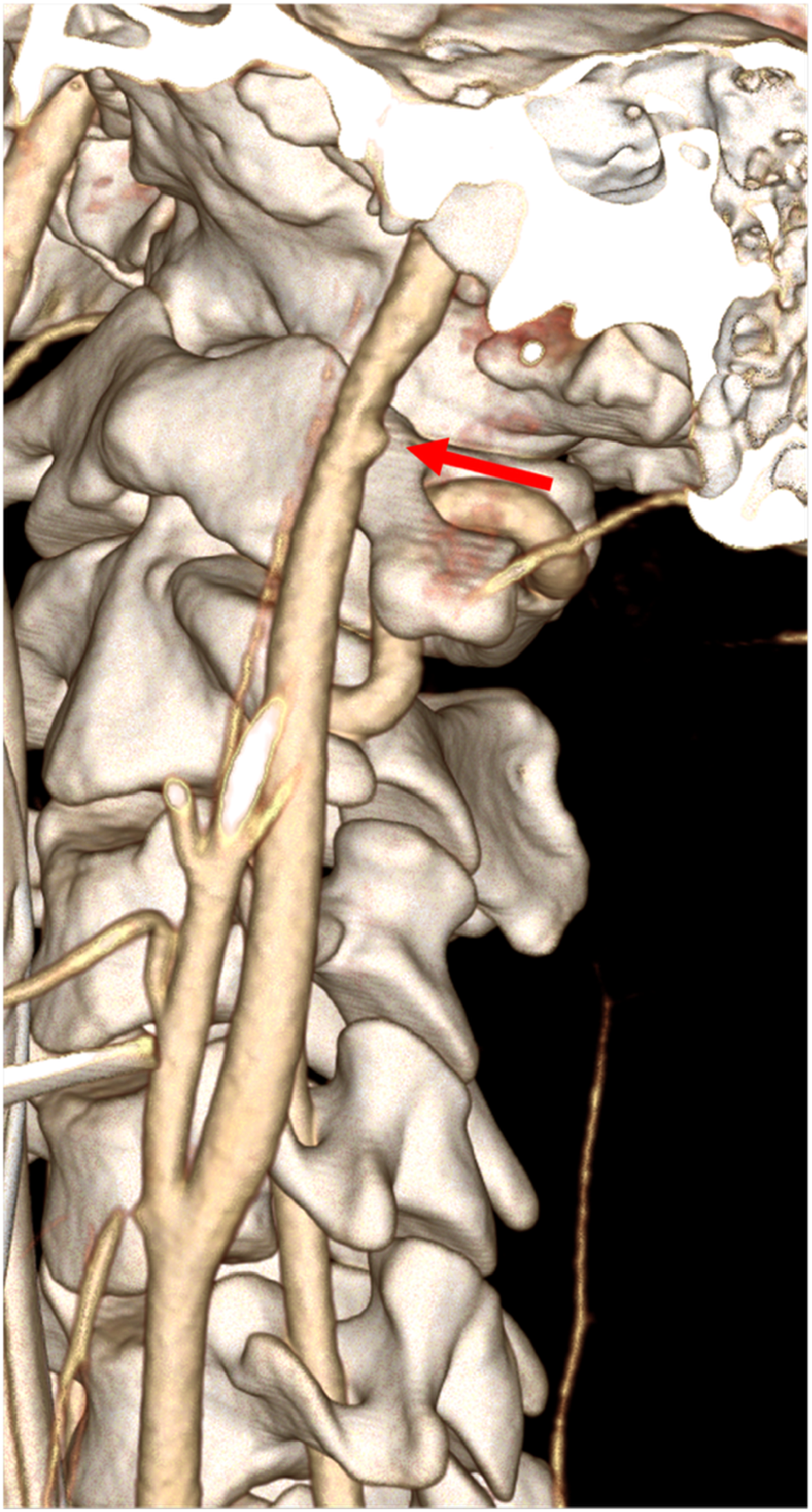
In this case, a male patient was involved in a motor vehicle accident (Figure 12). CT imaging demonstrates a temporal bone fracture that violates the otic capsule with associated fracture through the jugular fossa, including otologic complications, venous outflow injury, and concomitant arterial injury (Figure 13; blue arrows, Figures 14 and 15). Because skull base fractures can meet screening criteria for blunt cerebrovascular injury (BCVI), a computed tomography angiogram (CTA) can be used to identify concomitant arterial injury, such as an internal carotid artery pseudoaneurysm (BCVI grade III) (Figure 16).4,52,61 This case highlights the importance of targeted venography and arterial screening when fracture trajectories involve the skull base. Head CT 3D reconstruction demonstrating the skull and skull base fractures traversing the jugular foramen (red arrow). A–E Temporal bone CT demonstrating otic capsule violating temporal bone fracture (blue arrows) with an associated fracture through the jugular fossa (red arrows). A–D. CT venogram demonstrating absence of filling of the sigmoid sinus and jugular bulb on the right (red arrows) with normal filling of the left sigmoid sinus and jugular bulb (yellow arrows). CT venogram 3D reconstructions demonstrating a tapered occlusion at the distal right transverse sinus and sigmoid sinus with lack of filling of the jugular bulb (red arrows). CT angiography with 3D reconstruction demonstrating a small pseudoaneurysm of the distal left internal carotid artery (ICA) representative of a grade III arterial injury (red arrow).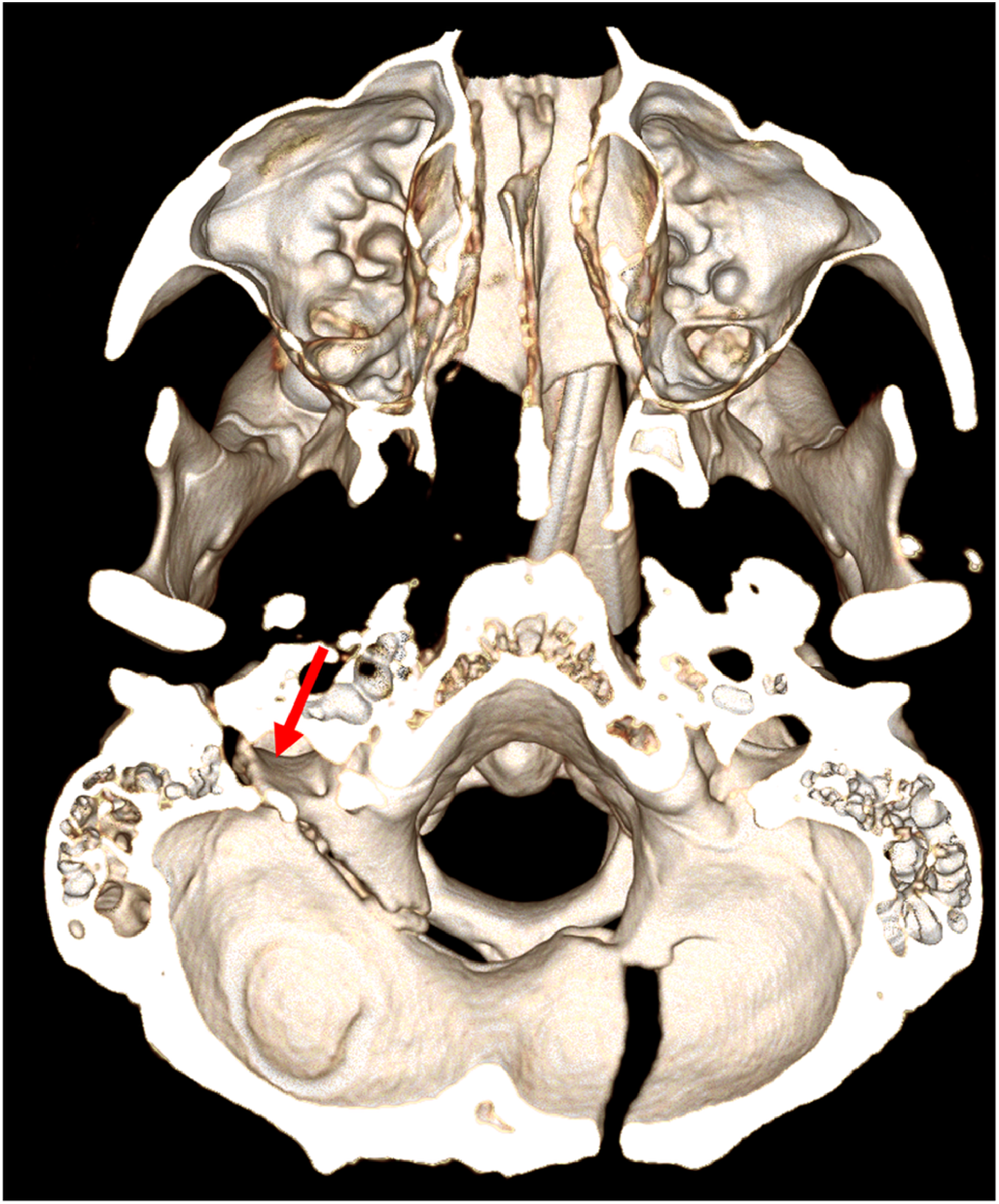
Case 2: Transverse sinus injury with suspected extrinsic compression
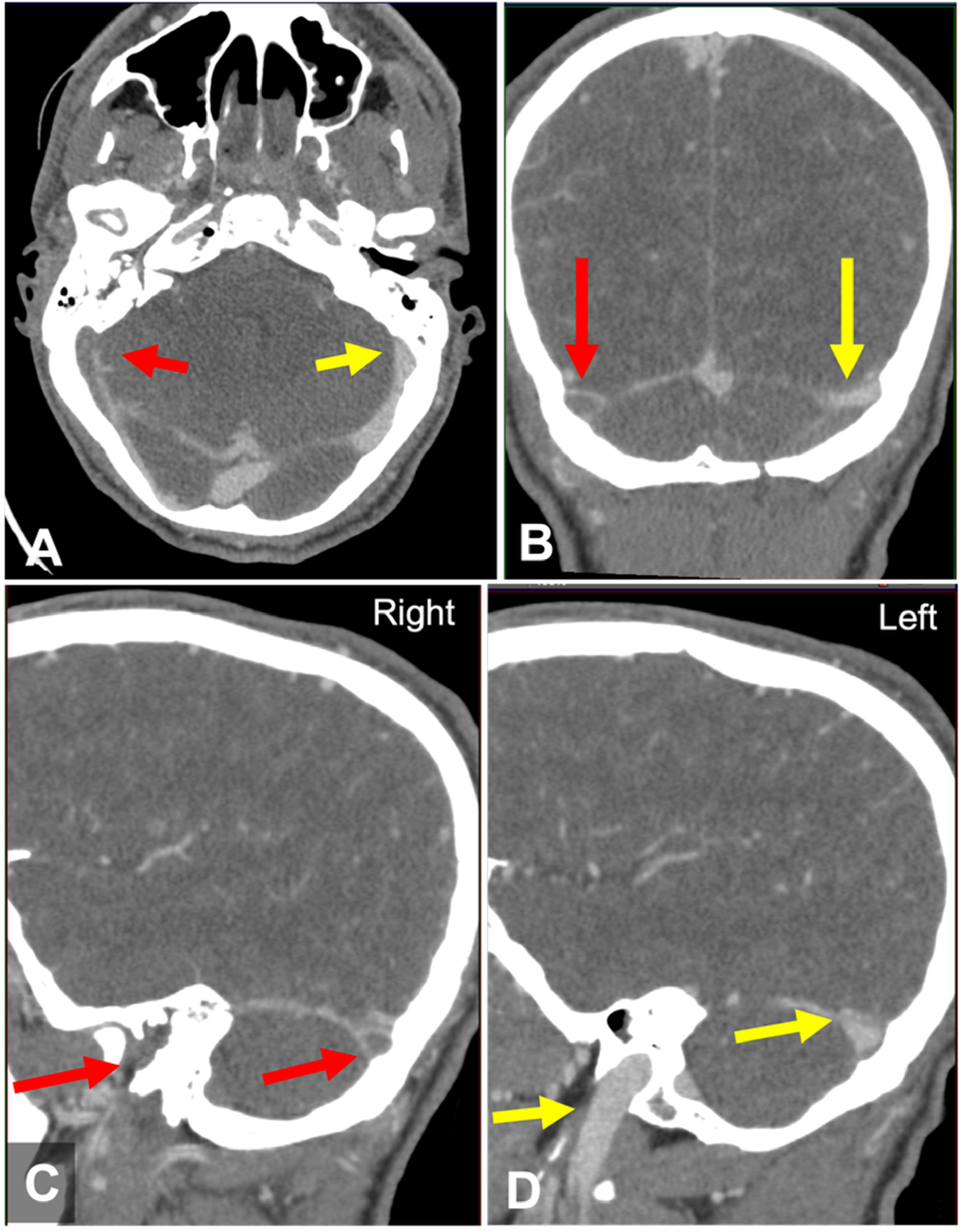
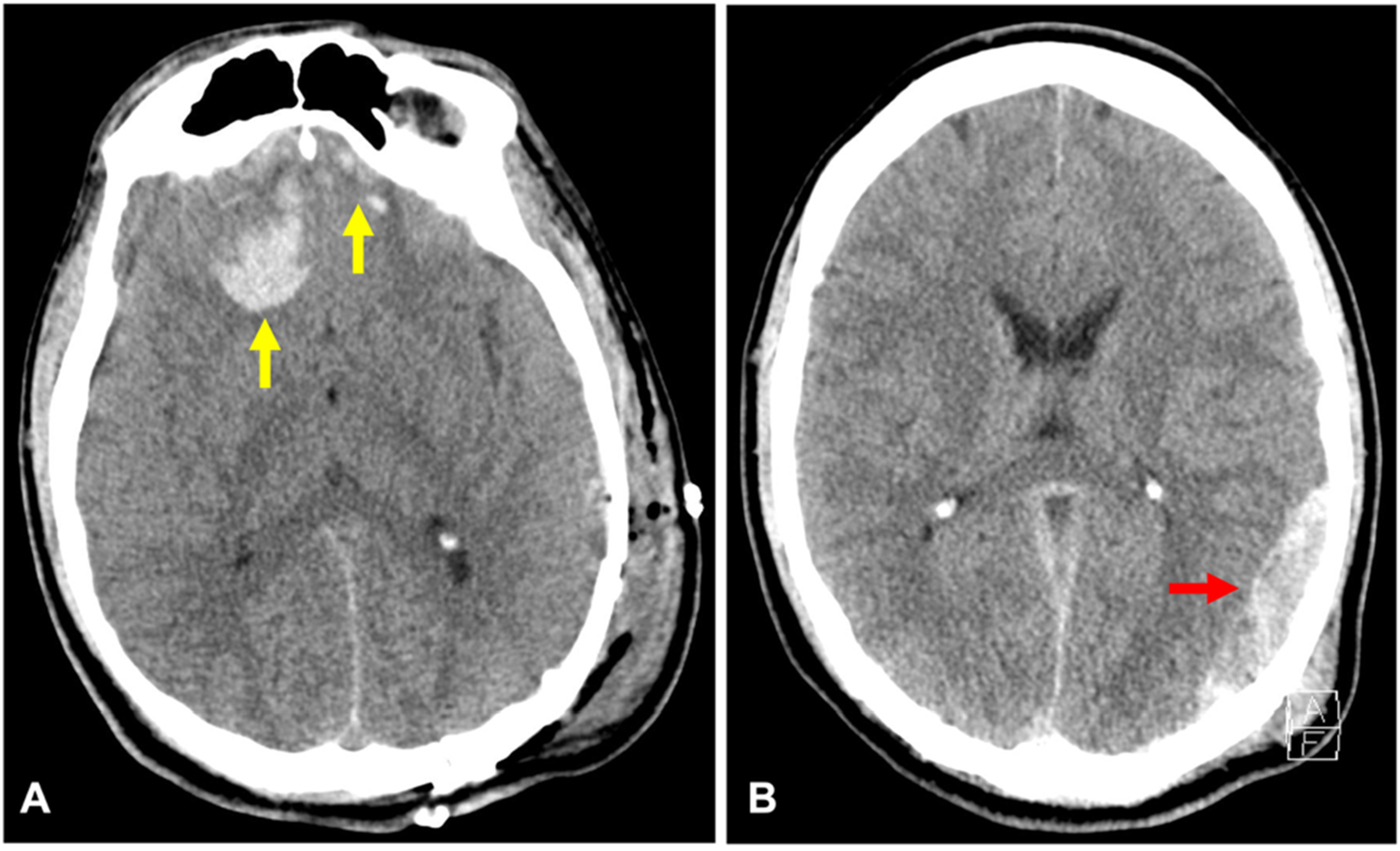
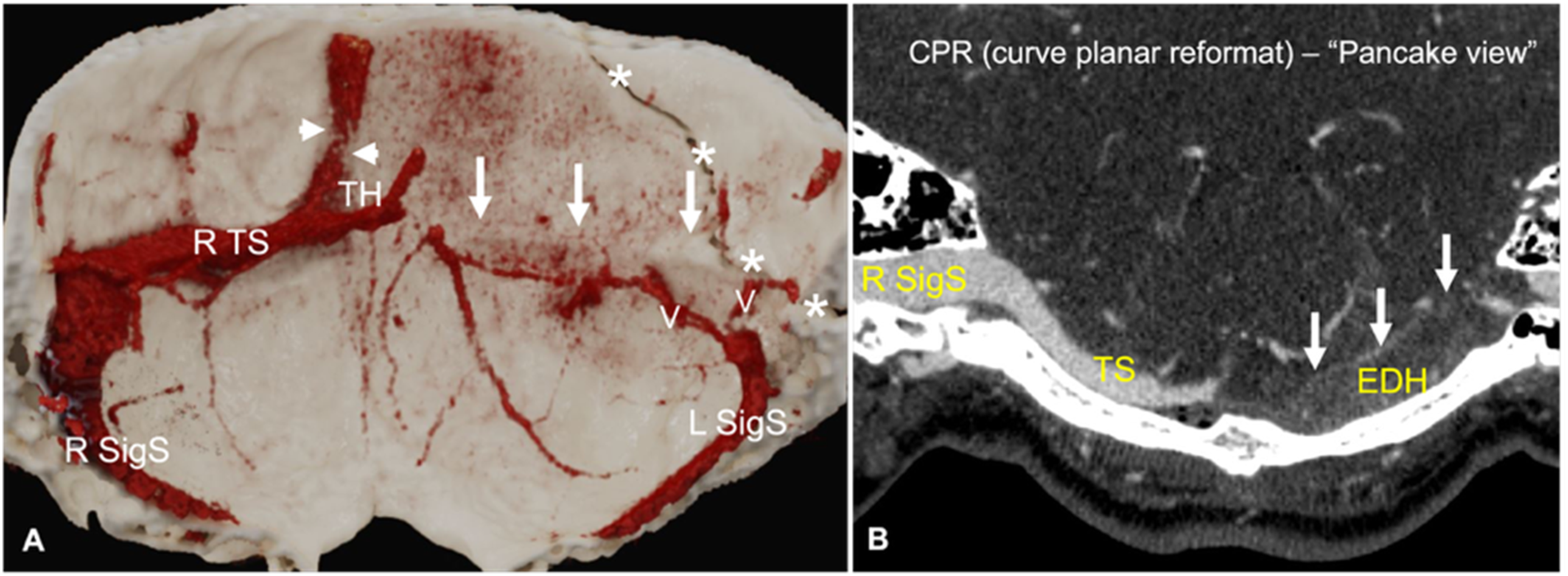
In this case, a 29-year-old male suffered blunt head trauma after being hit with a baseball bat and was run over by a vehicle. Noncontrast-enhanced CT imaging demonstrates a fracture of the left mastoid portion of the temporal bone with an associated occipital fracture (Figure 17) and coexisting traumatic intracranial hemorrhagic injuries, including bilateral frontal hemorrhagic contusions and a right convexity epidural hematoma (Figure 18). CTV with thin-section reformats and targeted post-processing reveals a lack of opacification and possible occlusion of the left transverse sinus with downstream filling of the left sigmoid sinus via small venous collaterals (Figure 19; white arrow). This imaging pattern supports a mechanical compression of the transverse sinus in the region of the epidural hematoma. A. 3D rendering of maxillofacial CT showing a displaced fracture of the mastoid segment of the left temporal bone (black arrows). B. Temporal bone CT demonstrating comminuted fractures of the left mastoid with widened fracture lines (white arrows) with another fracture present in the adjacent occipital bone (yellow arrow). A–B. Axial brain CT showing hemorrhagic contusions in the bilateral inferior frontal lobes (yellow arrows) with an epidural hematoma along the right convexity (red arrow). A. CT venogram and B. CT with curve planar reformation depicting lack of opacification of the left transverse sinus (white arrows) with an epidural hematoma (EDH) obliterating the left transverse sinus. There is filling of the left sigmoid sinus (L SigS) from venous collaterals (V). There is also an irregularity and narrowing at the posterior segment of the superior sagittal sinus (arrowheads) extending to the torcular (TH). The right transverse sinus (R TS) and right sigmoid sinus (R Sigs) demonstrate normal filling. Asterisks delineate a fracture in the occipital bone and mastoid bone.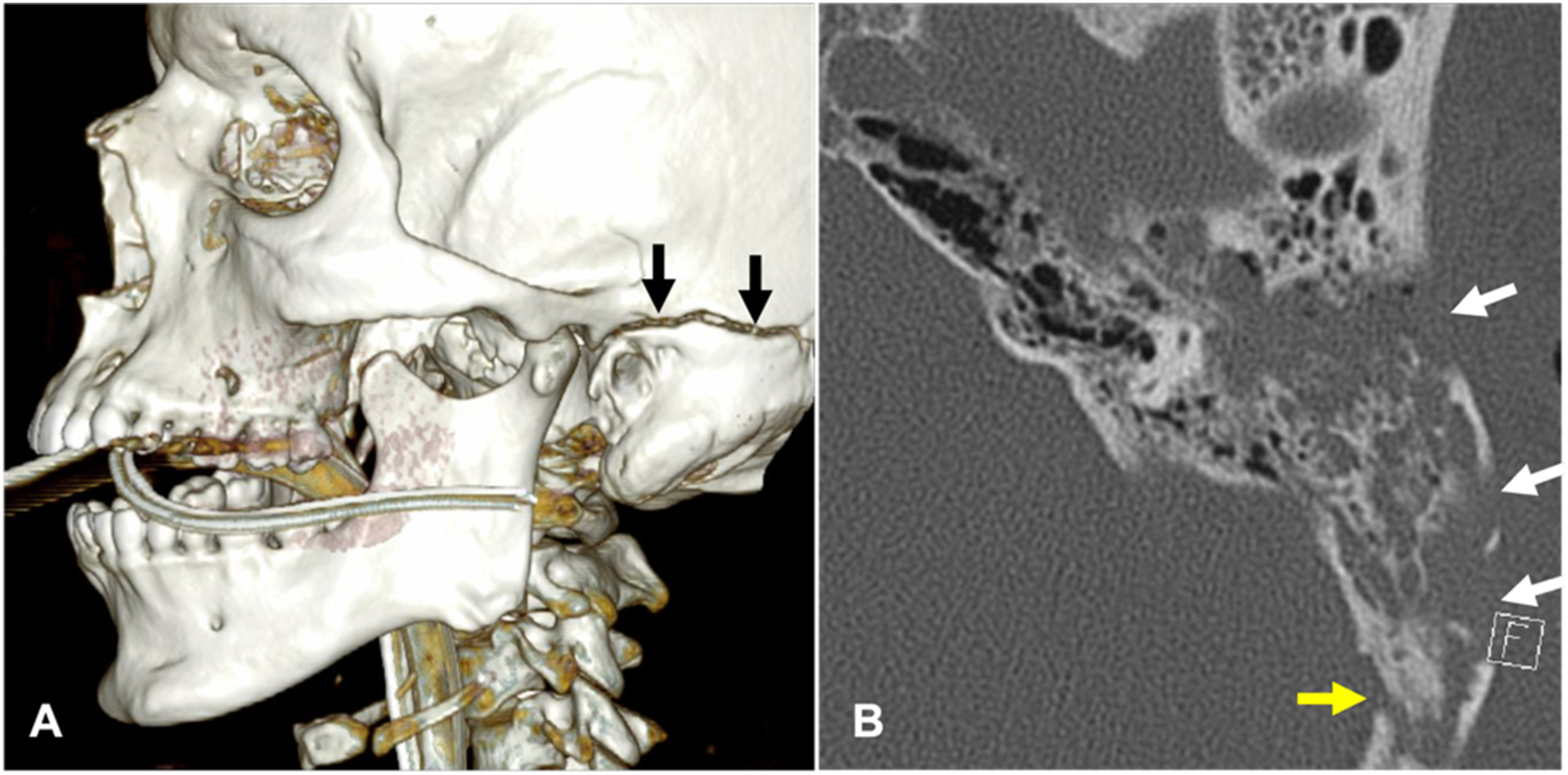
Case 3: Occlusive transverse-sigmoid sinus injury with venous infarction
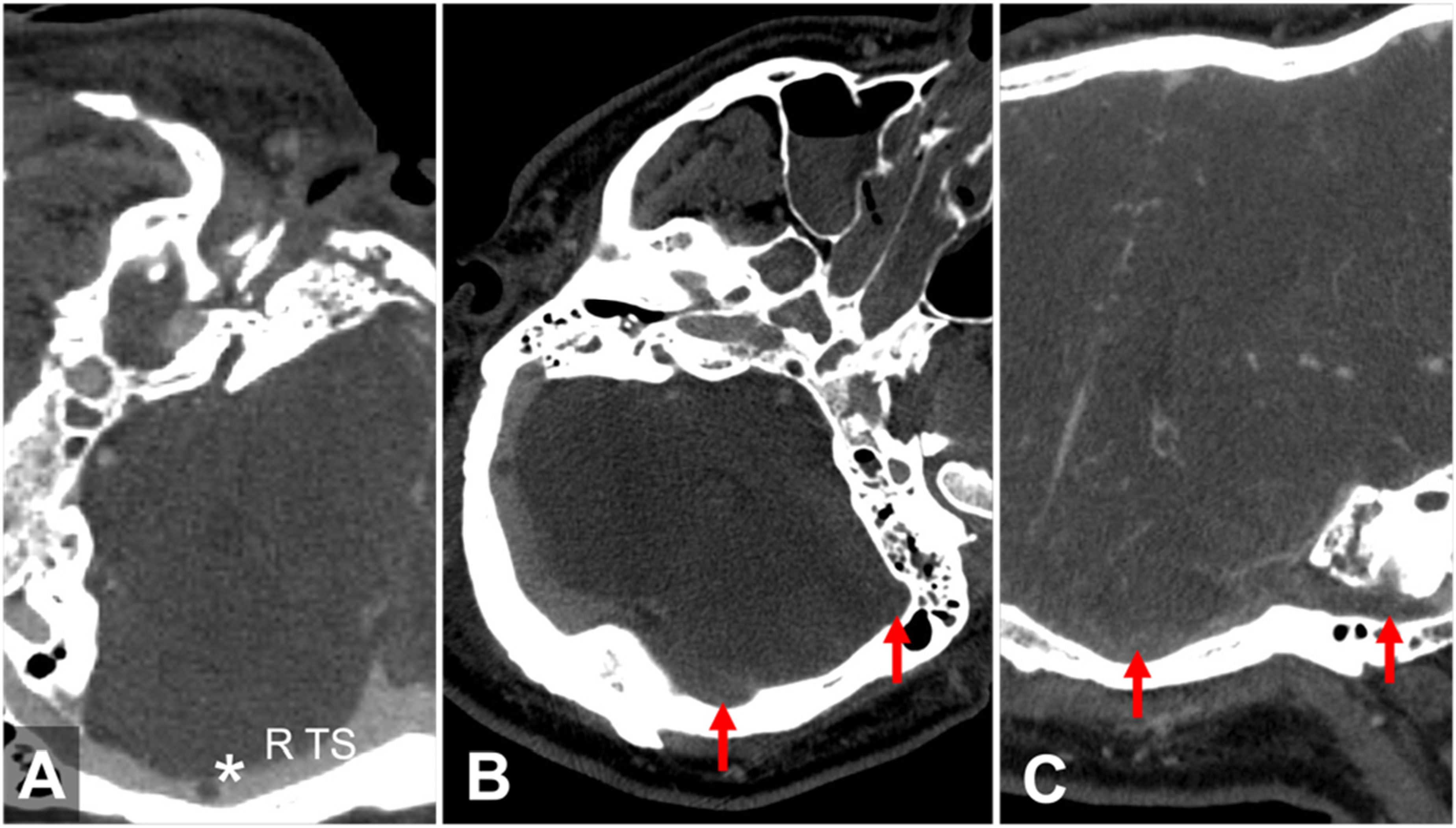
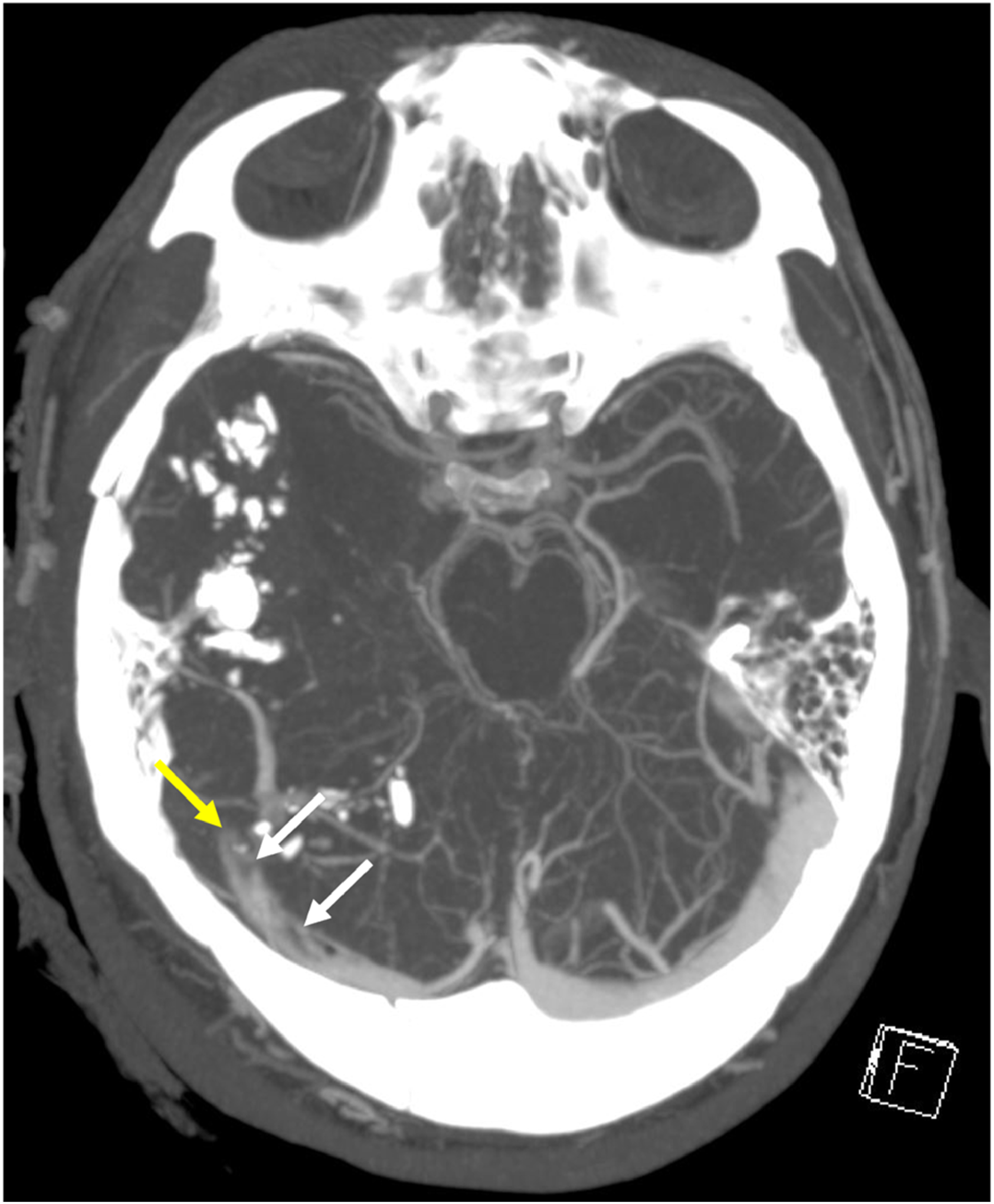
In this case, a 42-year-old male sustained head injuries after jumping out of a moving vehicle. CT imaging demonstrates a fracture of the left mastoid bone with opacification of the mastoid air cells (Figure 20; yellow arrows). Imaging with CTV reveals lack of opacification of the left transverse-sigmoid sinus complex, consistent with an occlusive injury (Figure 21; red arrows). The CTV also depicts a lack of distal reconstitution of venous flow, leading to the development of a venous infarct (Figure 22 A - B; red arrows; Figure 22 C; yellow arrows). Axial temporal bone CT showing comminuted fracture and opacification (blood) of the left mastoid air cells (yellow arrows). A–C. CT venogram showing lack of opacification (occlusion) of the left transverse-sigmoid sinus complex (red arrows) and a filling defect in the right transverse sinus (R TS) which represent an arachnoid granulation (asterisk). A. Curved Planar Reformation (CPR) and B. 3D volume rendering showing occlusion of the left transverse-sigmoid sinus complex (red arrows) without distal collateral reconstitution. C. MRI demonstrating a secondary venous infarct on the adjacent left cerebellum (yellow arrow).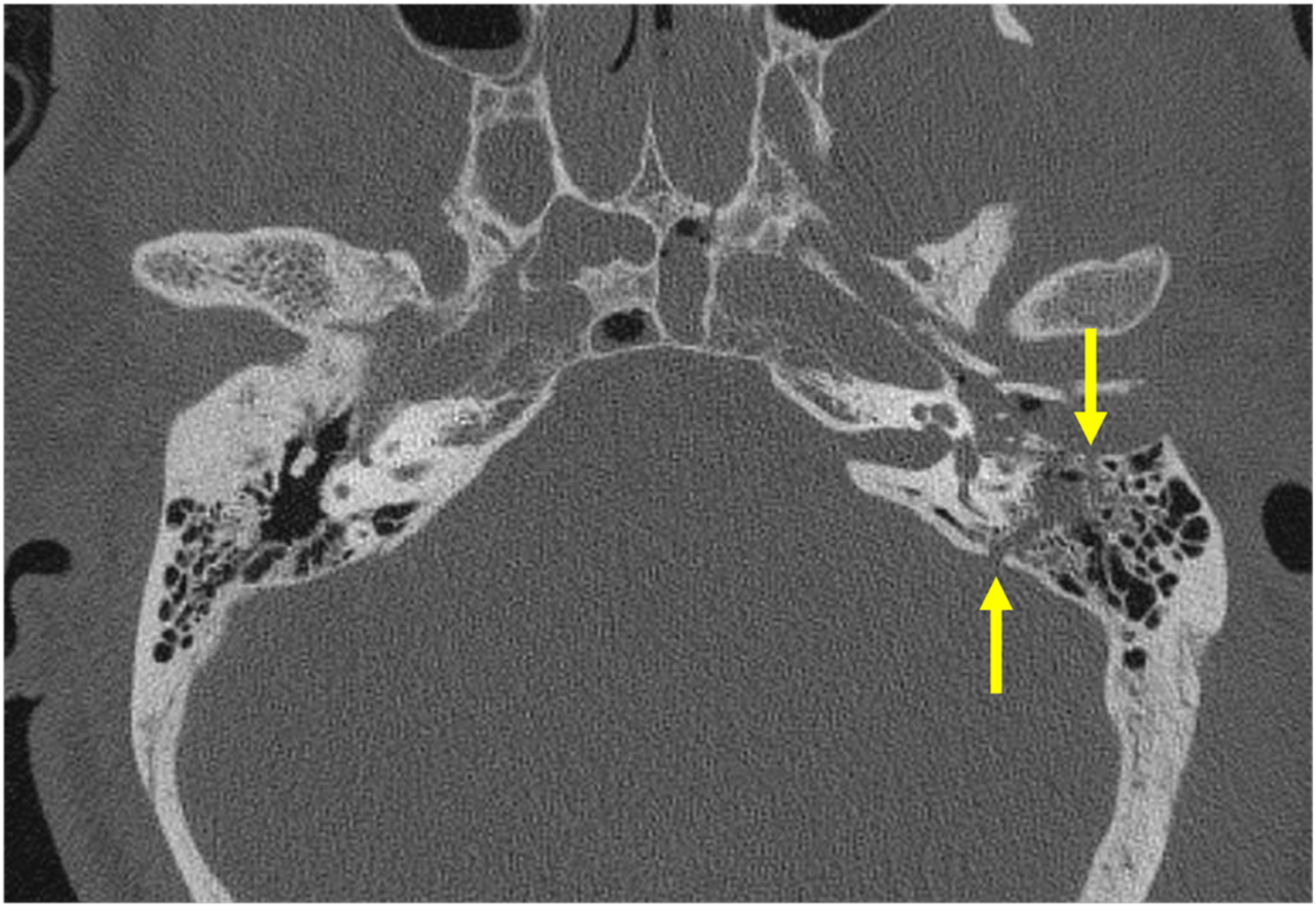
Case 4: Penetrating injury affecting the transverse sinus
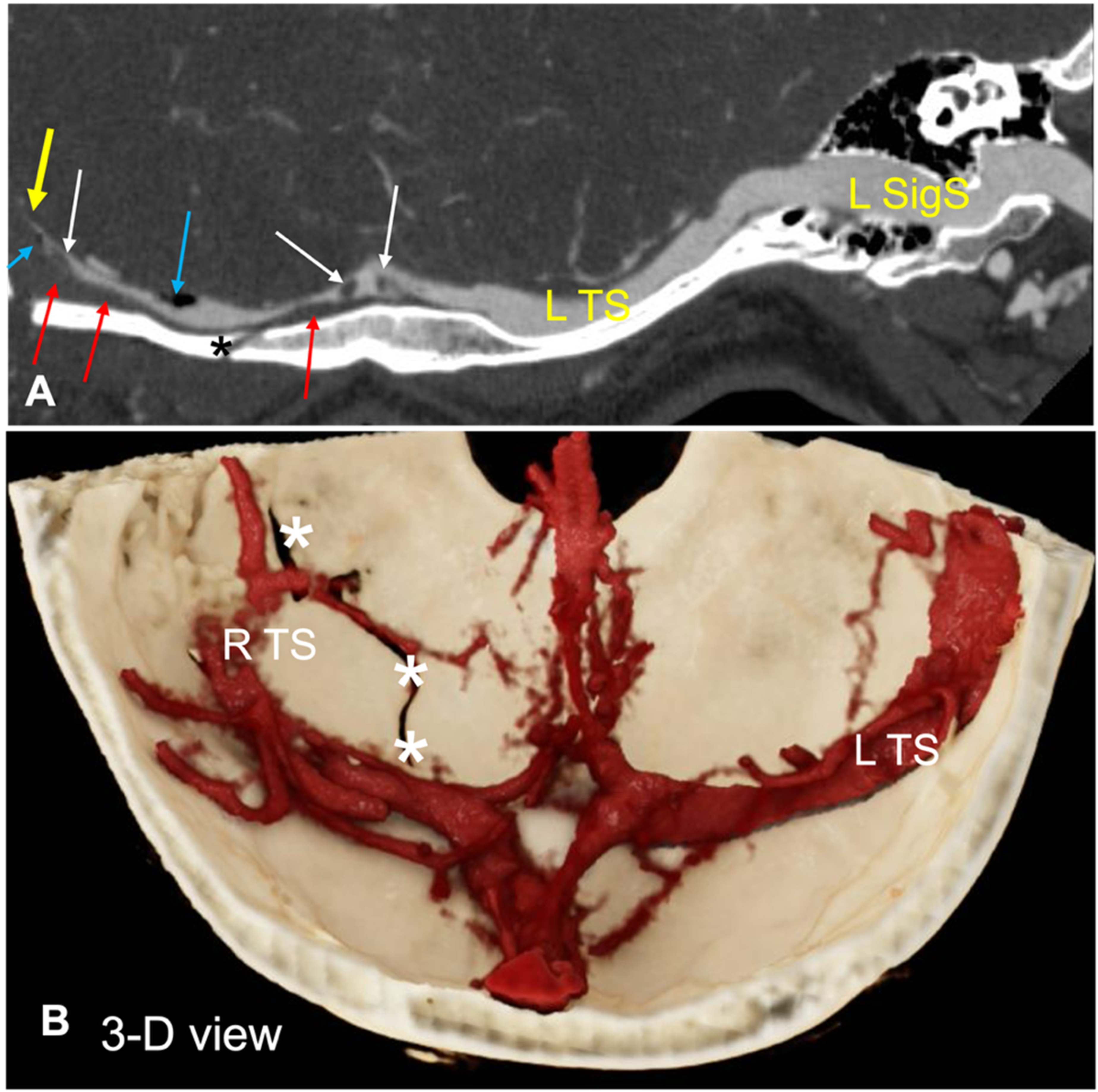
In the following case, a 22-year-old presented with a gunshot wound to the head. The CT images show multiple comminuted skull base and facial fractures along the projectile’s trajectory, affecting the right mastoid and right occipital calvarium (Figure 23). The CTV demonstrates abnormal right transverse sinus opacification with intraluminal filling defects compatible with clot/thrombus formation (Figure 24; white arrows), intraluminal gas, and distal tapered cutoff/occlusion, best appreciated with thin-section curved planar reformats (“pancake view”) and 3D volume rendering (Figure 25; blue arrows). Axial head CT demonstrating multiple comminuted fractures of the skull base and facial bones, along the projectile trajectory (dashed line), involving the right mastoid (M) and right occipital bone (O). CT venogram showing irregular opacification and filling defects (white arrows) within the right transverse sinus with distal cutoff of flow (yellow arrow). A. CT venogram depicting irregular opacification with filling defects representative of clot formation within the right transverse sinus (white arrows), intraluminal gas (blue arrows), distal tapered occlusion (yellow arrow), and a venous epidural hematoma (red arrows) slightly displacing the right transverse sinus away from the calvarium. B. 3D reconstruction demonstrating fractures through the skull base and calvarium (asterisks). L TS, left transverse sinus; R TS, right transverse sinus; L SigS, left sigmoid sinus.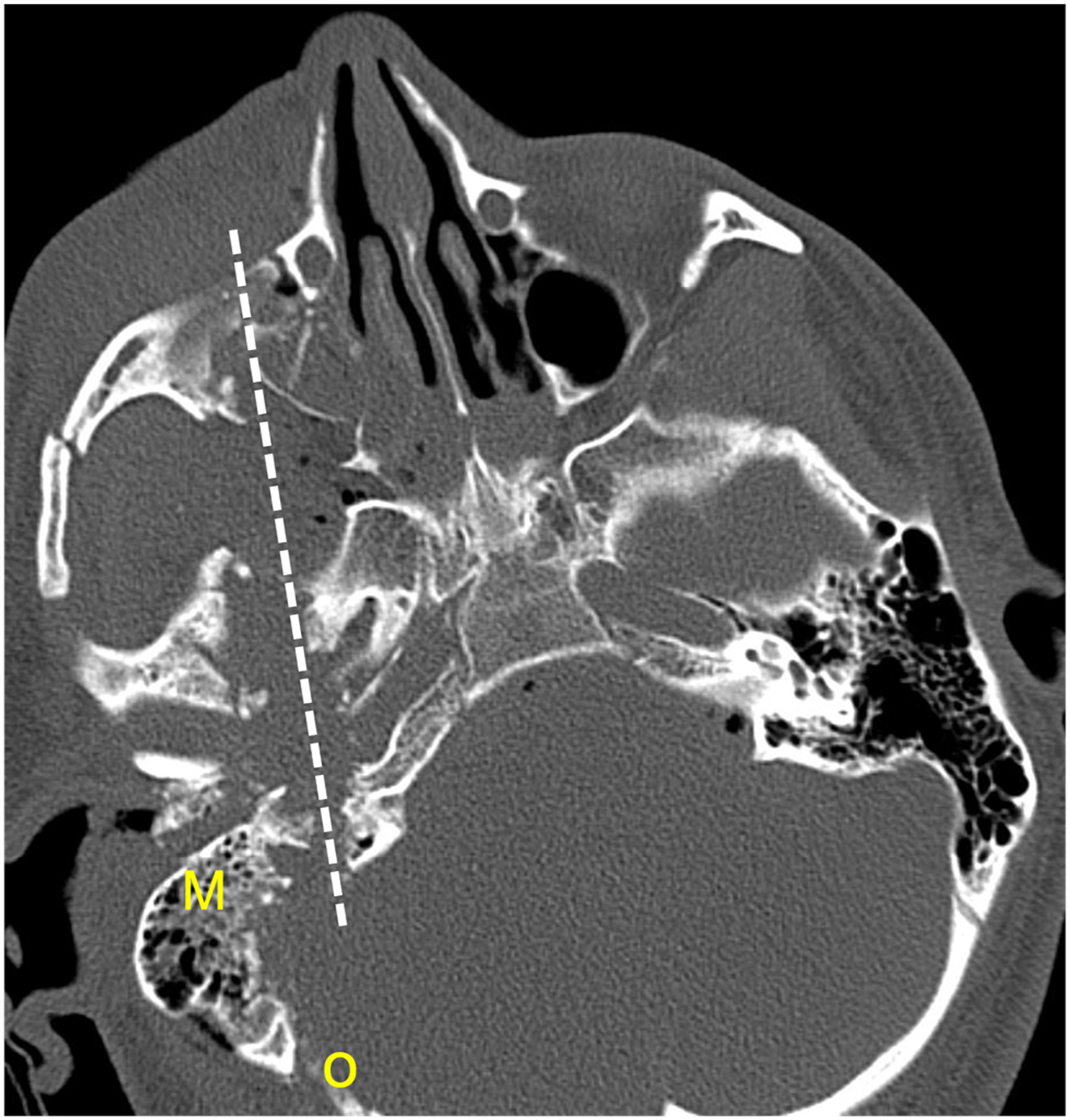
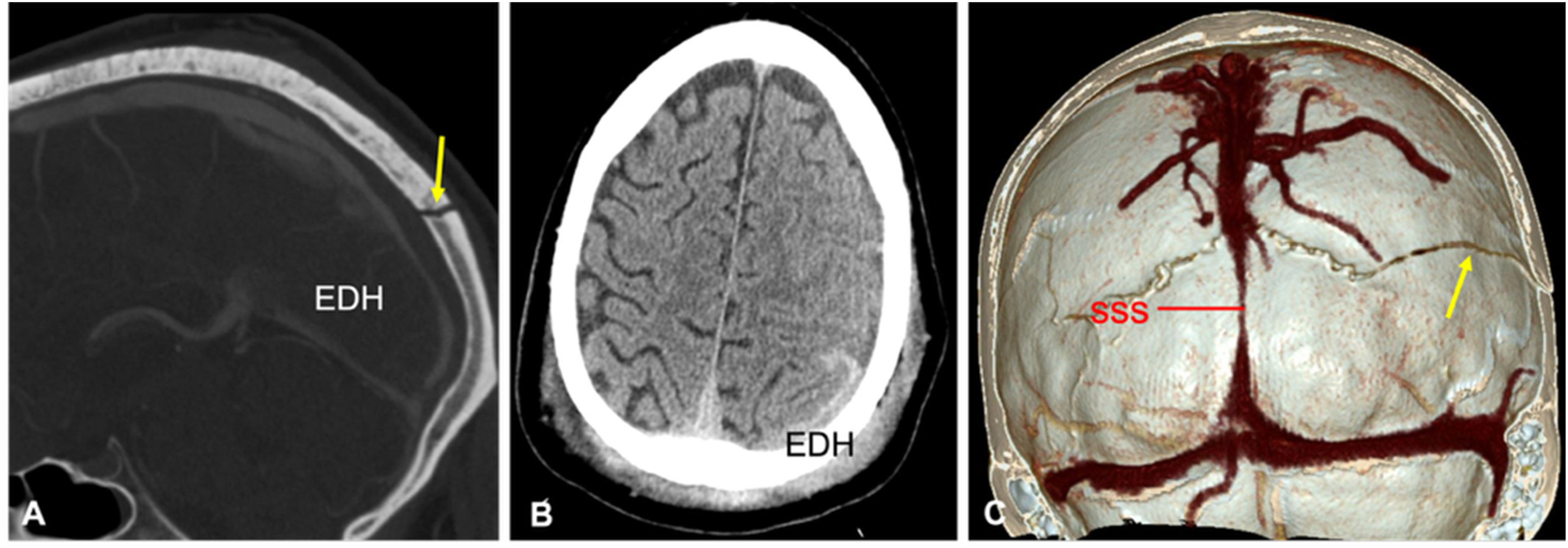
Case 5: Blunt head trauma affecting the superior sagittal sinus
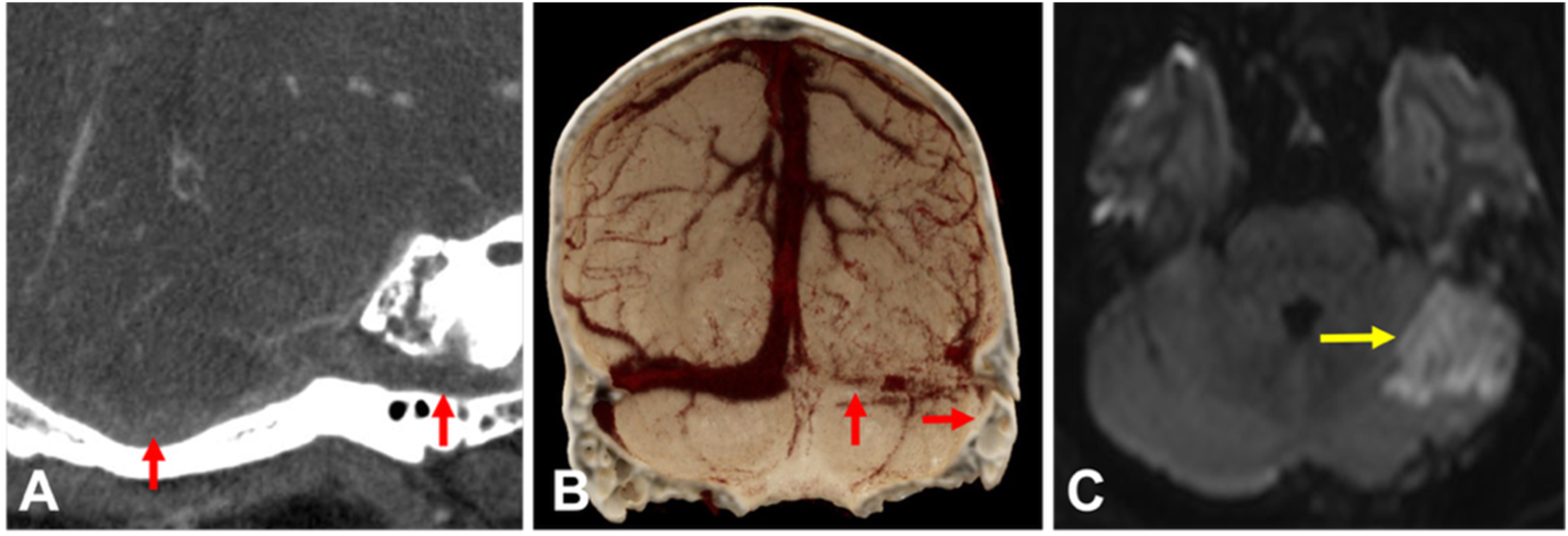
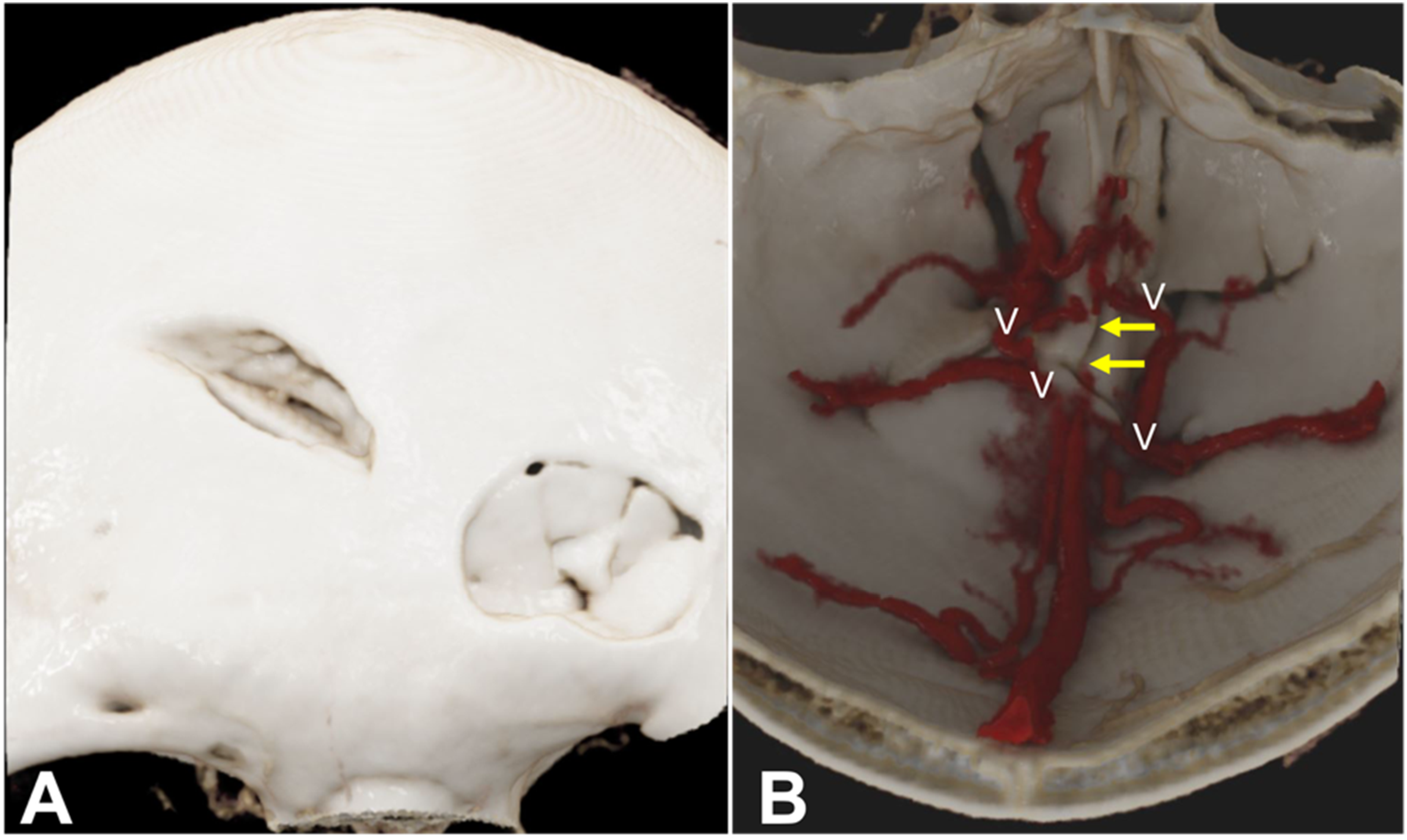
In this case, a 26-year-old male was assaulted with a crowbar. Noncontrast CT with 3D surface rendering demonstrates comminuted, depressed bilateral frontal calvarial fractures with small adjacent extra-axial hematomas (Figure 26; yellow arrows). CTV shows abrupt vessel caliber change with focal narrowing and discontinuity involving a short segment of the anterior SSS, consistent with traumatic injury/occlusion in the setting of a direct calvarial impact (Figure 27; yellow and red arrows). 3D post-processing with “external view” demonstrates the fracture configuration, while the “internal view” highlights collateral venous pathways that bypass the injured segment (Figure 28). The “internal view” reconstruction is helpful when the damaged segment is short and partially obscured by adjacent bone or hematoma on standard planar views. A. Axial CT head showing comminuted, depressed fractures of the bilateral frontal calvarium with subjacent small subdural hematomas (yellow arrows). A–B. CT venogram demonstrating change in caliber (yellow arrows) with narrowing and slight displacement of the anterior segment of the superior sagittal sinus (SSS) and focal discontinuity of the SSS (red arrows). A. 3D surface rendering (“external view”) showing comminuted, depressed fractures of the bilateral frontal calvarium. B. CT venogram with 3D volume rendering (“internal view”) showing venous collaterals (V) reconstituting the occluded, damaged short segment (arrows) of the anterior portion of the superior sagittal sinus.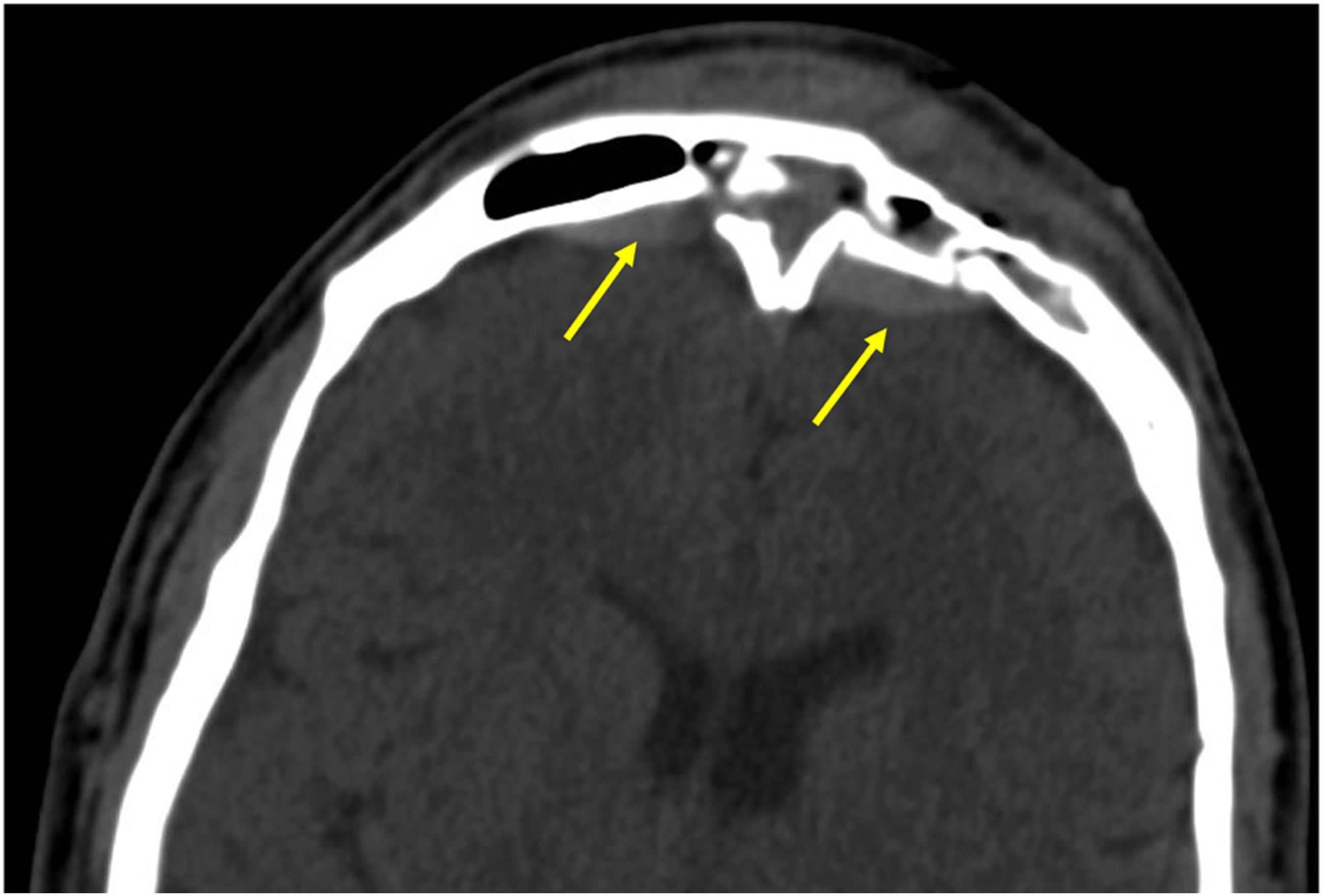
Management of dural venous sinus injuries
Proposed mechanism-based management approach for acute post-traumatic dural venous sinus injury.
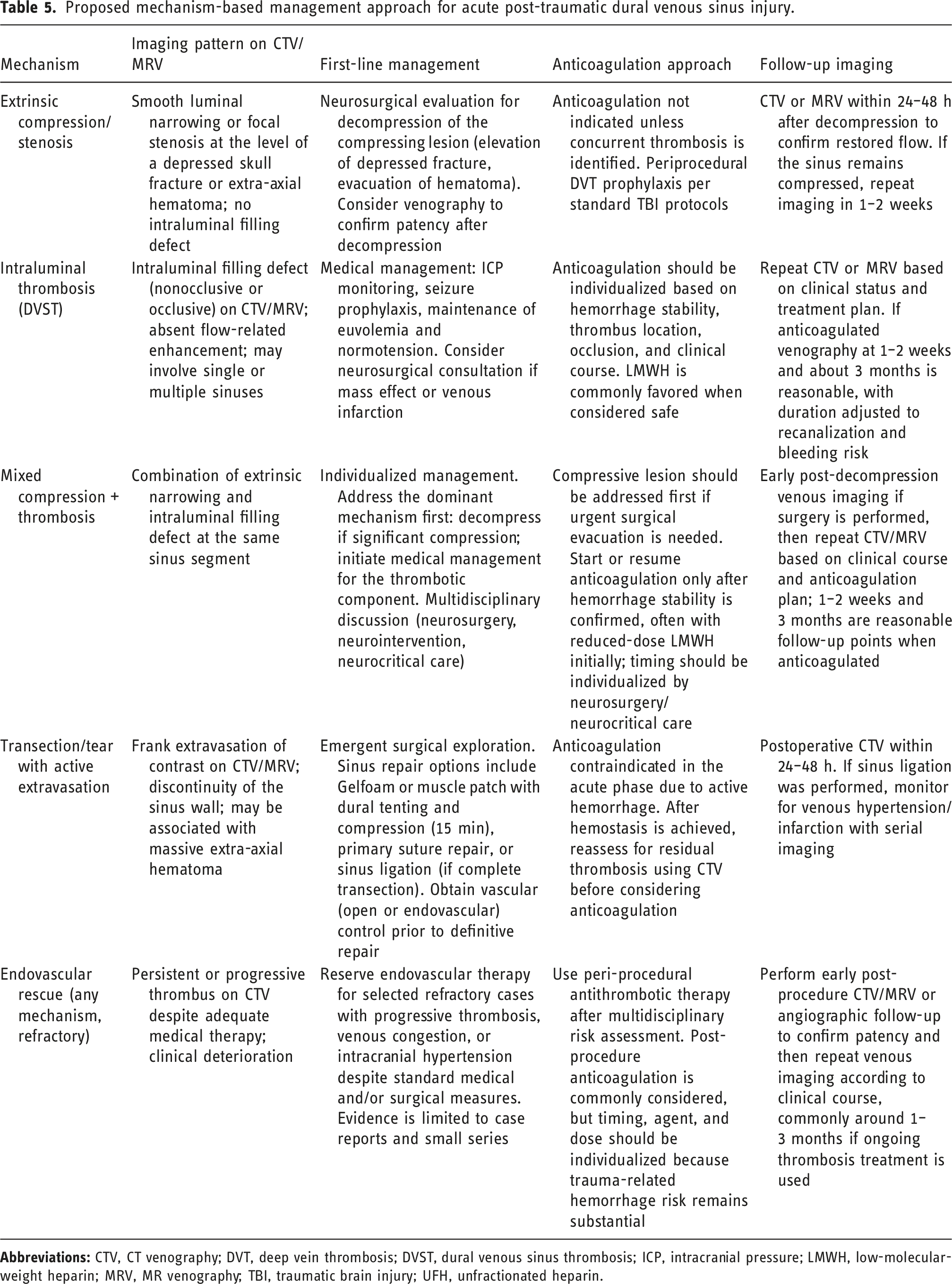
Currently, there is limited data about the management of DVST, and no consensus has been reached regarding optimal treatment strategies. 62 One challenge when managing DVST is that it often presents in conjunction with cerebral contusions, parenchymal hemorrhages, and subdural and epidural hematomas. 54 General practice favors systemic anticoagulation with low-molecular-weight heparin (LMWH) to prevent clot propagation, even in the presence of intracranial hemorrhage. 54 The 2024 American Heart Association scientific statement and the European Stroke Organization guidelines similarly recommend LMWH over unfractionated heparin in the acute phase of cerebral venous thrombosis, noting that venous hemorrhage is not a contraindication to anticoagulation; however, these recommendations are based on spontaneous cerebral venous thrombosis (CVT) populations, and specific guidelines for traumatic DVST are lacking.15,39,45 In the traumatic setting, limited observational data suggest that delaying anticoagulation until interval CT documents stability of hemorrhagic lesions may reduce the risk of hemorrhagic complications. 15 One adult series had 58% of patients with DVST treated with anticoagulation.30,63 Of these, 50% demonstrated thrombus resolution at 3 months.30,63 However, the study reported a rate of complications of 14% including gastrointestinal bleeding, and an additional 14% developed new or worsening intracranial hemorrhage with a mortality of 4.5%.30,63 A United Kingdom and Ireland survey of neurosurgical and critical care practice found substantial variation: 73.2% of clinicians used anticoagulation in selected cases only, 17.1% used no anticoagulation, and 9.8% used anticoagulation in all cases, with no respondents reporting an established departmental protocol for traumatic cerebral venous sinus thrombosis (tCVST) management. 34 It is important to note that there are no standardized guidelines for the timing, dosing, or duration of anticoagulation therapy for DVST. 12 Moreover, the benefits of anticoagulation therapy must be weighed against the risk of progression of hemorrhagic parenchymal contusions and epidural and subdural hematomas.42,54 Follow-up CT venography at 1 to 2 weeks and at 3 months after injury may be considered to assess recanalization and guide treatment duration; complete recanalization in adult or all-age TBI series has been reported in 41–80% of cases across published series. 15 Endovascular intervention, such as intrasinus thrombolysis or mechanical thrombectomy, is reserved as a rescue option for patients with clinical deterioration despite adequate medical therapy, and current evidence does not support routine endovascular treatment over standard anticoagulation.39,64
Conclusion
Systematic evaluation of the dural venous sinuses should be part of the diagnostic algorithm in head trauma, particularly when fractures or extra-axial hematomas occur along sinus trajectories (e.g., temporal/mastoid–transverse-sigmoid region, or vertex/frontal-parietal injuries near the superior sagittal sinus). Because DVSI and DVST can present subtly (or not at all) in noncontrast CT, the use of CTV/MRV with thin-section and targeted post-processing can aid diagnosis. Venographic imaging can distinguish between thrombus and extrinsic compression, characterize lesion extent, and define collateral pathways and downstream patency. Ultimately, timely recognition of these injuries, guided by a systematic venographic approach, is important for directing mechanism-based management and reducing the risk of severe sequelae such as venous infarction. However, prospective multicenter studies with standardized imaging protocols are needed to define anticoagulation strategies for traumatic DVST with intracranial hemorrhage and to establish the role of follow-up imaging in assessing recanalization and guiding treatment duration.
Footnotes
Ethical consideration
This is a review article for educational purposes.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Declaration of conflicts of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.