
Abstract
Orthognathic surgery represents a fundamental therapeutic approach for correcting severe skeletal jaw deformities that cannot be resolved through orthodontic treatment alone. Beyond restoring occlusal function, it also enhances speech, mastication, breathing, and facial aesthetics. The procedure generally involves repositioning the maxilla, mandible, or both, requiring close collaboration between orthodontists and maxillofacial surgeons to ensure optimal outcomes. However, the postoperative phase presents significant challenges, particularly related to nutrition and metabolic stress. Surgical trauma induces a catabolic state that accelerates protein breakdown and lean mass loss, with the most pronounced weight reduction occurring within the first two postoperative weeks. Patients often experience restricted mandibular mobility for 3–4 weeks, necessitating a transition to liquid or semi-liquid diets. This limitation, combined with increased energy and protein requirements—estimated at 2500–3000 kcal and 1–1.5 g/kg protein per day—places individuals at high risk of inadequate intake. Poor nutritional support may impair wound healing, prolong recovery, and negatively affect body composition and biochemical parameters. Clinical studies consistently document significant postoperative weight loss, averaging between −2.5 and −5 kg, with marked reductions in fat mass during the initial month after surgery. Given these findings, nutritional management emerges as a critical determinant of surgical success. Evidence suggests that supplementation with compact, high-calorie, high-protein oral nutritional supplements (ONS) or nutrient-dense natural shakes, in combination with structured dietary counselling, can mitigate postoperative weight loss and preserve lean body mass. This study therefore aims to evaluate the efficacy of targeted nutritional interventions—providing an average of 325 kcal and 20 g protein per serving—in improving anthropometric and body composition outcomes compared with standard care. By addressing the interplay between surgical stress, dietary limitations, and metabolic demands, the research highlights the importance of personalized perioperative nutrition as an integral component of orthognathic surgery management.
Introduction
Orthognathic surgery is a treatment modality designed to correct severe skeletal deformities of the jaws that cannot be managed with orthodontic treatment alone. Orthognathic surgery addresses both functional and aesthetic needs caused by skeletal deformities.The primary goal of orthognathic surgery is to achieve a balanced and functional occlusion, which enhances the patient's ability to speak, chew, and breathe, while also improving facial symmetry and overall appearance. The procedure typically involves the repositioning of the upper jaw (maxilla), lower jaw (mandible), or both, depending on the patient's specific condition. 1 Close collaboration between the orthodontist and the maxillofacial surgeon is crucial for an effective treatment planning and execution. 2 However, the postoperative period is complex and may involve complications that impact the patient's nutritional status and quality of life. The surgery induces metabolic stress, increasing protein catabolism and resulting in significant lean muscle mass loss.3–6 As nutrition is often compromised in patients undergoing maxillofacial surgery, adequate nutritional management is essential for promoting recovery.7,8 The majority of this weight loss occurs within the first two postoperative weeks. After surgery, energy and protein requirements increase to support healing and to manage surgical stress. Current recommendations suggest a daily intake of 2500–3000 kcal/10,450– 12,540 kJ and 1–1.5 g/kg of protein.2,9,10 Mandibular mobility is restricted after surgery for 3–4 weeks, necessitating a modified diet, predominantly liquid or semi-liquid. 10 Insufficient nutritional intake can negatively affect weight, body composition, and biochemical parameters. Successful orthognathic surgery depends not only on surgical expertise, but also on personalized nutritional management that addresses dietary challenges and meets the patient's increased needs. 11 Studies have shown significant weight loss in the first postoperative month. 12 A survey at Queen Elizabeth Hospital reported an average reduction of −4.96 kg (range: −9.6 to +3.0 kg) and a decrease in body fat mass of −3.07% (range: −5.80% to +2.30%) within the first four weeks. 13 A systematic review of 4836 patients confirmed a mean weight loss of −2.53 kg (95% CI = -0.24 to −4.81). 14 Given the observed weight loss and changes in nutritional status in patients undergoing orthognathic surgery,13,14 this study aims to evaluate the efficacy of supplementation with compact, high-calorie, high-protein oral nutritional supplements (ONS) or natural shake-based alternatives, combined with dietary counselling for a modified consistency diet, providing an average intake of 325 kcal and 20 g of protein to reduce postoperative weight loss.7,10 Also, it aims to investigate changes in anthropometric measures and body composition during the postoperative period, comparing a control group with intervention groups.
Materials and methods
Study design and participants
This randomized controlled study was conducted at the Maxillofacial Surgery Unit of the University Medical Center of Padua between December 2023 and September 2024. Twenty-six patients (16 males and 10 females) scheduled for orthognathic surgery were enrolled after providing written informed consent. Inclusion criteria were age between 18 and 40 years and eligibility for elective orthognathic surgery. Exclusion criteria included type 1 or type 2 diabetes mellitus, galactosemia, chronic kidney disease, history of gastric or gastrointestinal surgery, eating or neurological disorders, oncological disease, and pregnancy. Participants were randomly allocated to one of three groups using a 1:1:1 allocation ratio.Randomization was performed using computer-generated random number sequences from Research Randomizer software version 4.0. Allocation concealment was maintained through sequentially numbered, opaque, sealed envelopes prepared by a researcher not involved in patient recruitment or assessment. Due to the nature of the intervention, participants and dietitians could not be blinded to group assignment; however, maxillofacial surgeons and researchers conducting measurements were blinded to minimize bias. The three groups were designated as Group A, the natural food smoothie group (n = 9), Group B, the oral nutritional supplement group (n = 9), and Group C, the control group (n = 8).
Nutritional intervention and study protocol
All participants in both intervention and control groups received standardized nutritional counselling delivered by dietitians. The counselling session was conducted on postoperative day 2 (T1) and lasted 45 min as an individual session. The dietary counselling protocol included detailed instruction on texture progression: weeks 1 to 2 required a full liquid diet including broths, strained soups, milk, yogurt, fruit juices, and nutritional supplements; weeks 3 to 4 allowed progression to pureed and creamy consistency foods including blended vegetables, pureed meats, mashed potatoes, puddings, and smoothies; from week 4 onwards, gradual introduction of soft foods based on clinical evaluation and jaw mobility. Nutritional targets were established based on postoperative metabolic stress and current recommendations for orthognathic surgery patients. Energy intake target was approximately 25–30 kcal/kg/day and a protein intake of 1.0–1.5 g/kg/day. Fluid intake target was a minimum of 2 liters per day. Practical recommendations included consuming 5 to 6 small frequent meals per day, cautious use of straws, maintaining oral hygiene and monitoring for signs of malnutrition. All participants received written materials including dietary guidelines, food texture charts, sample meal plans, and dietitian contact information.
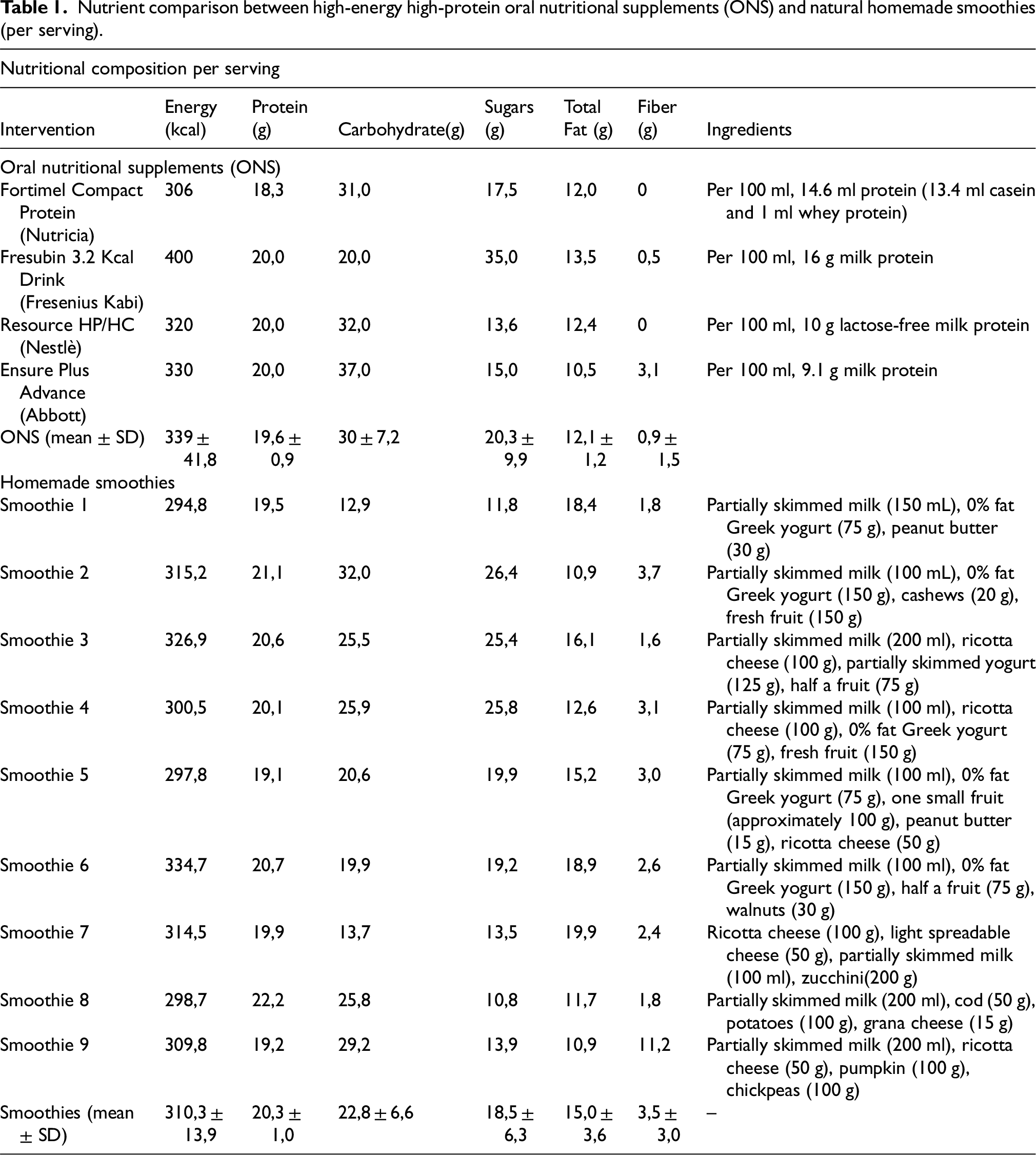
Participants were allocated to one of three groups: an ONS group (n = 9), receiving dietary counseling plus commercially available high protein, high energy oral nutritional supplements providing a mean of 325 kcal and 20 g of protein per serving, with instructions to consume 1–2 servings per day for 4 weeks; a natural food (recipe) group (n = 9), receiving dietary counseling plus individualized homemade smoothies based on natural foods designed to provide a similar nutritional content (approximately 300 kcal and 20 g of protein per serving) (Table 1), consumed 1–2 times per day for 4 weeks; and a control group (n = 8), receiving dietary counseling alone without nutritional supplementation. Compliance with dietary recommendations and supplementation was assessed using 24-h dietary recalls and food diaries.
Nutrient comparison between high-energy high-protein oral nutritional supplements (ONS) and natural homemade smoothies (per serving).
Assesstmments, measurements and statistical analysis
Assessments were conducted at three time points: T0 (preoperative baseline, 1 day before surgery), T1 (early postoperative, day 2 at 48 ± 6 h after surgery), and T2 (one- month postoperative, 28 ± 3 days after surgery). The preoperative assessment included obtaining written informed consent, collecting medical and surgical history, conducting 24- hour dietary recall, performing anthropometric measurements and body composition
analysis, and completing nutritional risk screening using NRS-2002 and GLIM criteria. The early postoperative assessment included anthropometric measurements, body composition analysis, the nutritional counselling session, group assignment revelation, and distribution of supplements and food diaries. The one-month assessment included 24- hour dietary recall, collection of food diaries, anthropometric measurements, body composition analysis, adherence assessment questionnaires, and clinical evaluation.
All anthropometric measurements were performed by trained dietitians using standardized techniques according to World Health Organization guidelines. Anthropometric measurements included body weight, height, body mass index (BMI), arm circumference, and waist circumference, obtained using standardized equipment (SECA scale with stadiometer and SECA measuring tape). Body composition was assessed by bioelectrical impedance analysis using a Metadieta analyzer (METEDA s.r.l., serial number A00092030, software version 1.2.6), evaluating fat-free mass, fat mass, and phase angle. Nutritional risk was assessed using the NRS-2002 tool and GLIM criteria.
The primary outcome was postoperative weight change (absolute and percentage variation) between T0 and T2. Secondary outcomes included changes in BMI, arm circumference, waist circumference, phase angle, fat-free mass, and fat mass. Continuous variables were expressed as medians and interquartile ranges (IQR), while categorical variables were reported as absolute numbers and percentages. Differences between T0 and T2 within each group were analyzed using the Mann–Whitney U test, with statistical significance set at p < 0.05.
Results
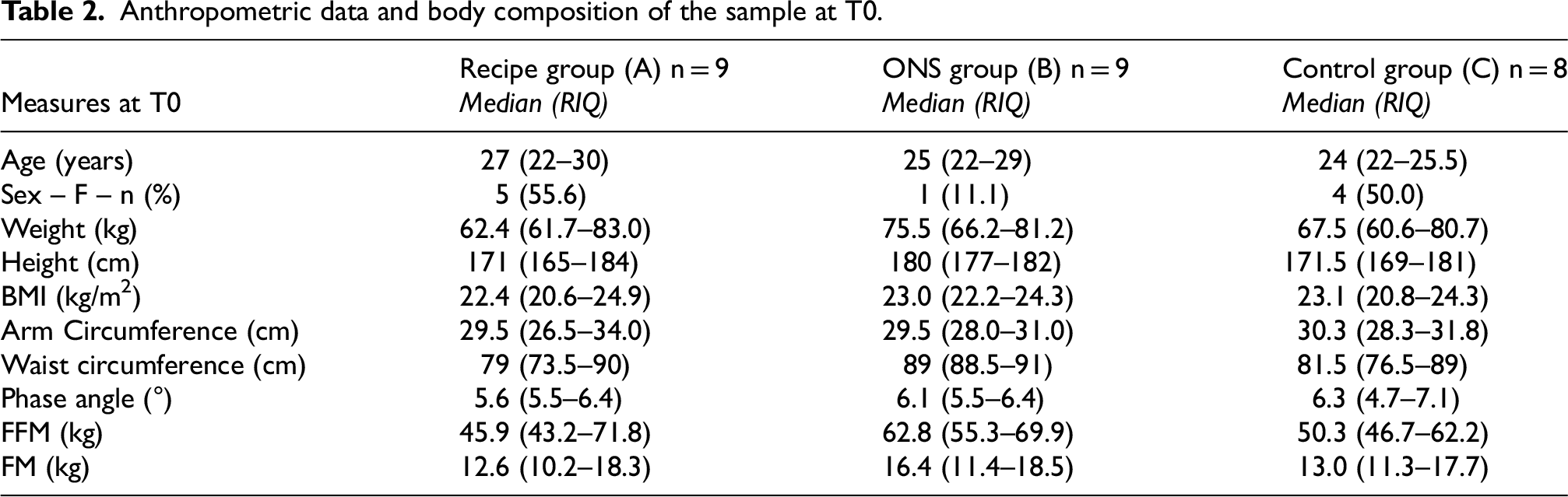
Analysis of anthropometric measures and body composition at T0 (Table 2) showed a balanced distribution of age and participant numbers across the groups. The ONS group had a median age of 25 years (IQR: 22–29), the control group 24 years (IQR: 22–25.5), and the natural food group was slightly older, with a median age of 27 years (IQR: 22–30). Sex distribution was similar between the control and natural food groups (4 and 5 women, respectively), whereas the ONS group included only 1 woman, which explains the observed differences in median weight and height. The ONS group had a higher median weight of 75.5 kg (IQR: 66.2–81.2) compared to the control group (67.5 kg, IQR: 60.6–80.7) and the natural food group (62.4 kg, IQR: 61.7–83). Median BMI was similar across the groups, falling within the normal weight range: 23.0 kg/m2 (IQR: 22.2–24.3) in the ONS group, 23.1 kg/m2 (IQR: 20.8–24.3) in the control group, and 22.4 kg/m2 (IQR: 20.6–24.9) in the natural food group. One participant in the natural food group had a BMI > 29.9 kg/m2 (obesity), and one participant in the control group had a BMI > 24.9 kg/m2 (overweight). Body circumferences were similar between the natural food and control groups: arm circumference was 29.5 cm (IQR: 26.5–34.0) and 30.3 cm (IQR: 28.3–31.8), respectively, and waist circumference was 79 cm (IQR: 73.5–90) and 81.5 cm (IQR: 76.5–89.5), respectively. The ONS group had a larger waist circumference (89 cm, IQR: 88.5–91), likely attributable to the different gender distribution. Body composition analysis showed a higher lean mass (fat-free mass, FFM) in the ONS group (62.8 kg, IQR: 55.3–69.9) compared to the control group (50.3 kg, IQR: 46.7–62.2). However, the percentage of FFM was similar in the two groups (80.4% and 80.2%, respectively). Fat mass (FM), while differing in absolute quantity, was also comparable in percentage. The natural food group had lower FFM (45.9 kg, IQR: 43.2–71.8) and FM (12.6 kg, IQR: 10.2–18.3), likely due to the higher proportion of women in this group. Median phase angle was similar between the ONS (6.1°, IQR: 5.5°–6.4°) and control (6.3°, IQR: 4.7°–7.1°) groups. This similarity allows for accurate examination of changes in phase angle related to cellular health and muscle mass integrity. However, the median phase angle in the natural food group was lower (5.6°, IQR: 5.5°–6.4°), likely due to the greater proportion of females, who tend to have lower values than males
Anthropometric data and body composition of the sample at T0.
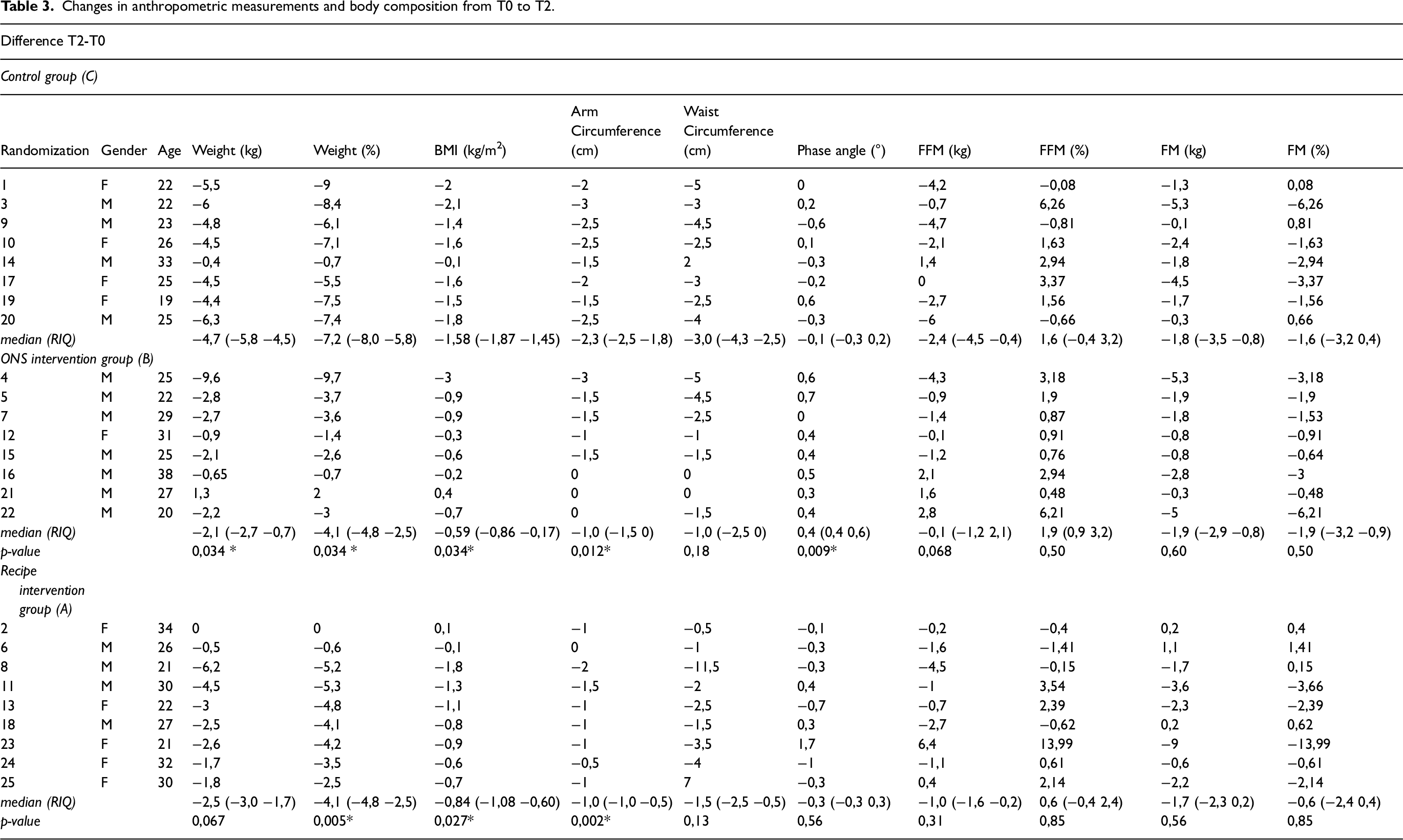
One month postoperatively (T2), patients were re-evaluated to analyze changes in anthropometric measures and body composition compared to the preoperative period (T0) (Table 3). Significant differences between groups were found for weight loss (both absolute and percentage), BMI reduction, arm circumference reduction, and phase angle in the ONS group. The ONS group experienced a median weight loss of −2.1 kg (IQR: −2.7 to −0.7; p = 0.034), representing a percentage reduction of −4.1% (IQR: −4.8% to −2.5%; p = 0.034). The natural food group showed a median weight loss of −2.5 kg (IQR: −3.0 to −1.7; p = 0.067), equivalent to −4.1% (IQR: −4.8% to −2.5%; p = 0.005), while the control group showed a greater loss of −4.7 kg (IQR: −5.8 to −4.5), equivalent to −7.2% (IQR: −8.0% to −5.8%). For BMI, the ONS group had a median reduction of −0.59 kg/m2 (IQR: −0.86 to −0.17; p = 0.034). The natural food group also showed a decrease of −0.84 kg/m2 (IQR: −1.08 to −0.60; p = 0.027), while the control group had a larger decrease of −1.58 kg/m2 (IQR: −1.87 to −1.45). Similarly, non-dominant arm circumference decreased by −1.0 cm (IQR: −1.5 to 0; p = 0.012) in the ONS group and −1.0 cm (IQR: −1.0 to −0.5; p = 0.002) in the natural food group, while the reduction was more pronounced in the control group (−2.3 cm, IQR: −2.5 to −1.8). Although not statistically significant, waist circumference reductions were −1.0 cm (IQR: −2.5 to 0; p = 0.18) for the ONS group, −1.5 cm (IQR: −2.5 to −0.5; p = 0.13) for the natural food group, and −3.0 cm (IQR: −4.3 to −2.5) for the control group. Body composition analysis showed a significant improvement in phase angle in the ONS group, with a median increase of +0.4° (IQR: + 0.4° to +0.6°; p = 0.009), indicating improved cellular health and muscle mass. The control group showed a phase angle decrease of −0.1° (IQR: −0.3° to +0.2°), while the natural food group showed a decrease of −0.3° (IQR: −0.3° to +0.3°; p = 0.56). Lean mass was better preserved in the ONS group, with a median reduction of −0.1 kg (IQR: −1.2 to 2.1; p = 0.068), while the control group experienced a greater reduction of −2.4 kg (IQR: −4.5 to −0.4). In the natural food group, FFM decreased by −1.0 kg (IQR: −1.6 to −0.2; p = 0.31), but these differences were not statistically significant. Finally, fat mass showed no significant differences between the groups: the ONS group recorded a reduction of −1.9 kg (IQR: −2.9 to −0.8; p = 0.60), the natural food group −1.7 kg (IQR: −3.5 to +0.8; p = 0.85), and the control group −1.8 kg (IQR: −3.5 to −0.8). Analysis of food diaries and medical histories revealed that during the postoperative period (first 2–3 weeks), participants primarily followed a liquid or creamy diet, resulting in lower-than-necessary nutritional intake. With reduced swelling, a semi-solid diet was possible by one month (T2), but nutritional requirements were still not fully met. ONS group patients showed good compliance during the first three weeks, but adherence decreased in the fourth week due to the broadening of dietary consistencies. Additionally, supplement procurement issues were reported due to high costs and industrial processing. Patients consuming natural smoothies used the supplements 1–2 times per day for approximately 4 weeks, discontinuing them with improved chewing ability. The main challenges encountered were large volumes, lack of appetite and motivation, which reduced compliance. However, natural smoothies offer advantages such as low cost, use of natural ingredients, high palatability, and recipe variety, reducing dietary monotony.
Changes in anthropometric measurements and body composition from T0 to T2.
Discussion
As reported in the literature, surgical interventions induce metabolic stress and protein catabolism, leading to a reduction in lean mass and increased energy requirements for tissue healing.4,5,11 In patients undergoing orthognathic surgery, these effects are compounded by chewing difficulties during the 4-week postoperative period, necessitating dietary counseling and modifications in consistency (Giridhar VU)10,15 This study evaluated 26 patients (16 male, 10 female) at the Maxillofacial Surgery Unit of University of Padova Medical Center, assigned to three groups: the ONS group, receiving supplements providing 325 kcal/1359 kJ and 20 g of protein; the natural food group, consuming smoothies of similar nutritional value (300 kcal/1254 kJ, 20 g of protein); and the control group, receiving only dietary counselling.
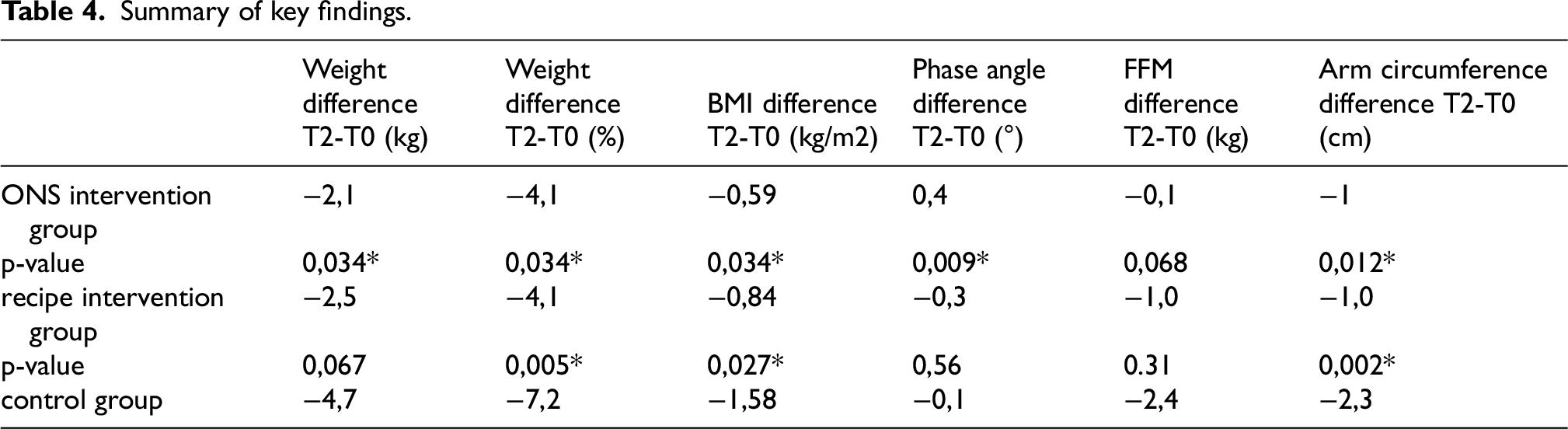
Both intervention groups demonstrated better preservation of body weight compared to the control group. In the ONS group, weight loss was −2.1 kg (IQR: −2.7 to −0.7; p = 0.034), equivalent to −4.1% (IQR: −4.8% to −2.5%; p = 0.034), with a BMI reduction of −0.59 kg/m2 (IQR: −0.86 to −0.17; p = 0.034). The natural food group experienced a weight loss of −2.5 kg (IQR: −3.0 to −1.7; p = 0.067), equivalent to −4.1% (IQR: −4.8% to −2.5%; p = 0.005), and a BMI reduction of −0.84 kg/m2 (IQR: −1.08 to −0.60; p = 0.027). The control group showed a greater decrease: −4.7 kg (IQR: −5.8 to −4.5), equivalent to −7.2% (IQR: −8.0% to −5.8%), and a BMI decrease of −1.58 kg/m2 (IQR: −1.87 to −1.45). Non-dominant arm circumference decreased less in the ONS group (−1.0 cm, IQR: −1.5 to 0; p = 0.012) compared to the control group (−2.3 cm, IQR: −2.5 to −1.8). Bioimpedance analysis revealed significant differences in phase angle only in the ONS group (+0.4°, IQR: + 0.4° to +0.6°; p = 0.009), indicating improved cellular health and muscle mass, while the control group showed a decrease of −0.1° (IQR: −0.3° to +0.2°). The natural food group showed a reduction of −0.3° (IQR: −0.3° to +0.3°; p = 0.56). The change in lean mass was minimal in the ONS group (−0.1 kg, IQR: −1.2 to +2.1; p = 0.068), greater in the natural food group (−1.0 kg, IQR: −1.6 to −0.2; p = 0.31), and more pronounced in the control group (−2.4 kg, IQR: −4.5 to −0.4). Although the difference in FFM was not statistically significant, the small sample size may have limited statistical power. The p-value near the significance threshold in the ONS group suggests that a larger sample size could confirm the efficacy of supplementation. In conclusion, the combination of nutritional supplementation and dietary counselling appears to promote postoperative recovery, improving weight retention and muscle mass (Table 4).
Summary of key findings.
This study has some limitations, primarily the small sample size, which may have influenced the statistical significance of the results. Future studies with larger samples are needed to confirm these findings and increase the robustness of the data. Another important consideration is the variability in patient compliance with nutritional recommendations. During the first three weeks, when the diet was primarily liquid or creamy, adherence was good due to the use of ONS and natural food smoothies. However, the transition to firmer food textures led to a decline in supplement intake, potentially reducing nutritional intake and negatively impacting lean body mass recovery and metabolic function. ONS demonstrated significant benefits: balanced nutritional intake in reduced volumes and ease of use for patients, improving compliance in the initial weeks. However, their high cost and limited availability can restrict access. Furthermore, the processed nature of these products may be a drawback for individuals preferring fresh, minimally processed foods. While cost-effective, palatable, and versatile, natural food smoothies also present challenges. The required volumes were often high, and reduced appetite and motivation among patients negatively impacted compliance. The nutritional content of smoothies is also less standardized than that of commercial ONS, increasing the risk of suboptimal intake. To improve long-term compliance, increased motivational support and targeted education are crucial. Future studies should explore more accessible and sustainable solutions to ensure adequate nutritional support throughout the recovery period.
Conclusion
This study demonstrated the efficacy of nutritional supplementation with oral nutritional supplements (ONS) and natural food smoothies, combined with dietary counselling, in improving nutritional management of patients undergoing orthognathic surgery during the postoperative period. Compared to the control group, the intervention groups maintained body weight, BMI, and arm circumference more effectively.
ONS supplementation promoted improved body composition, as evidenced by reduced lean mass loss and an improvement in phase angle, a key indicator of cellular health and muscle quality. These results support the role of ONS in meeting increased energy and protein requirements, thereby promoting postsurgical metabolic and functional recovery. However, adherence to nutritional supplements decreased with the introduction of firmer food textures. This suggests the need for strategies to improve compliance, such as enhanced motivational support and targeted educational interventions. Furthermore, the high cost and limited availability of ONS highlight the need to develop more accessible and sustainable protocols. Compliance with natural food smoothies was limited by large volumes, reduced motivation, and decreased appetite. This underscores the importance of tailoring nutritional solutions to individual preferences and needs through personalized dietary counselling. Future research, with larger sample sizes, and addressing the identified challenges, will help consolidate these findings and contribute to the development of more effective and targeted nutritional strategies for postoperative support in orthognathic patients.
Footnotes
Ethical approval statement
The approval was issued by the Ethics Committee “Comitato Etico Territoriale Area Centro-EST Veneto” on September 5th, 2024. CET-ACEV: 537n/AO/24.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.