
Abstract
Introduction
Food literacy is increasingly recognized as an important determinant of healthy aging; however, its relationship with adherence to the Mediterranean diet and successful aging remains insufficiently explored, particularly among older adults participating in lifelong learning programs. This study aimed to evaluate the relationship between food literacy, adherence to the Mediterranean diet, and successful aging among University of the Third Age (U3A) students.
Methods
This cross-sectional study was conducted between November 2024 and February 2025 with 120 individuals aged
Results
Adherence to the Mediterranean diet was positively associated with food literacy in the simple model (β = 0.202, p = 0.027). Successful aging showed a stronger association (β = 0.485, p < 0.001). In the multiple model, successful aging remained significant (β = 0.452, p < 0.001), while BMI was negatively associated (β = −214, p = 0.007). The association between MEDAS and food literacy was not significant after adjustment.
Conclusions
Successful aging was more strongly associated with food literacy than with adherence to the Mediterranean diet. While MEDAS showed a significant association in the unadjusted model, this association did not remain after adjustment. These findings suggest the potential importance of multidimensional approaches to promoting healthy aging.
Introductıon
Aging is a universal life process, and the global population is rapidly aging. It is estimated that the proportion of individuals aged 60 years and older will reach 22% by 2050. 1 Similar trends are observed in Turkey, where improvements in healthcare, along with declining fertility and mortality rates, have led to significant demographic changes, resulting in an increasing proportion of older adults in the population. 2 This demographic transition has intensified the focus on achieving longer and healthier lives. As the population ages, the need for disease prevention and management increases, making healthy aging a global priority. 3 Healthy aging involves not only the absence of disease but also the maintenance of physical independence, functional ability, and overall well-being. 4 In this context, the concept of successful aging has gained increasing importance. Successful aging is a multidimensional construct that includes the absence of serious illness, the preservation of physical and cognitive functions, and active social engagement. 5 While genetic factors play a role, modifiable lifestyle factors and individual attitudes toward aging are also critical determinants. Self-care aimed at increasing the education and awareness of older adults, thinking that they can still learn and be active, is one of the building blocks of this process. 6 Factors such as body mass index (BMI), physical activity, and adherence to the Mediterranean diet have been associated with this concept. 7 Promoting a healthy lifestyle is therefore essential for supporting healthy aging outcomes and protecting public health. 8 In this context, University of the Third Age (U3A) programs have been suggested to support successful aging by promoting lifelong learning, social participation, and active engagement among older adults. 9
Nutrition is a key modifiable factor associated with successful aging. The Mediterranean diet, characterized by high consumption of fruits, vegetables, whole grains, legumes, and olive oil, and limited intake of red and processed meats, has been shown to reduce the risk of chronic diseases and support cognitive health in older adults.10,11 However, successful aging is not determined solely by dietary patterns, but also by individuals’ knowledge, skills, and awareness related to food and nutrition. 12 In this context, food literacy has emerged as an important concept. Food literacy is a multidimensional concept that encompasses the knowledge, skills, beliefs, and practices required to improve individuals’ health and quality of life. 13 It enables individuals to make informed decisions about the foods they consume and their potential effects on health. 14 A study conducted in Japan reported that higher levels of food literacy were associated with better diet quality among individuals aged 19–80 years. 15 Food literacy has been suggested to promote healthy eating behaviors, and higher levels of food literacy among older adults may be associated with greater adherence to the Mediterranean diet, a healthy dietary pattern. Findings from food literacy interventions in younger populations have emphasized the need to evaluate food literacy in broader populations, including adults and vulnerable groups.16,17 Although previous studies have examined adherence to the Mediterranean diet, chronic diseases in older adults, and successful aging, the relationship between food literacy, adherence to the Mediterranean diet, and successful aging in older adults remains underexplored. This study aimed to examine the association between food literacy, adherence to the Mediterranean diet, and successful aging among students enrolled in the U3A.
Methods
Location of the study and sample selection
The sample for this study consists of U3A students aged 60-85 at Alanya Alaaddin Keykubat University (Antalya, Türkiye). All 120 students enrolled in the program were included in the study. Research data was collected through face-to-face interviews between November 2024 and February 2025. Participants aged ≥60 years who were enrolled in the U3A program, were literate, and voluntarily agreed to participate were included in the study. Individuals with end-stage or severe chronic diseases (e.g., advanced cancer or end-stage renal disease) that could significantly affect their general health status and participation were excluded. The study data were collected using a questionnaire form. The questionnaire form included individuals’ sociodemographic information, dietary habits, anthropometric measurements, the Self-Perceived Food Literacy Scale (SPFL), the Mediterranean Diet Adherence Scale (MEDAS), and the Successful Aging Scale (SAS).
Questionnaire form
The general information section of the survey form used to collect research data included questions about the age, sex, income, education level, occupation, etc. of elderly individuals, as well as information about their diagnosed chronic diseases and use of medication or nutritional supplements. The section on eating habits includes questions about the number of main and snack meals, skipping meals, and diet practices.
Self-perceived food literacy scale (SPFL)
The Self-perceived Food Literacy Scale (SPFL), developed by Poelman et al. 18 and adepted into Turkish by Tarı Selçuk et al., 19 is used to assess individuals’ food literacy levels. The SPFL consists of 29 items and 8 sub-dimensions: food preperation skills (items 1–6), resilience and resistance (items 7–12), healthy snack styles (items 13–16), social and conscious eating (items 17–19), examining food labels (items 20–21), daily food planning (items 22–23), healthy budgeting (items 24–25), and healthy food stockpiling (items 26–29). The scale is rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). Items 2, 10, 12, 19, 26, 27, 28, and 29 are reverse-coded. The total score, obtained by summing all items, ranges from 29 to 145 and indicates the level of perceived food literacy, with high scores indicating a high level of food literacy. The Cronbach's alpha coefficient for the overall scale is 0.83.
Mediterranean diet adherence screener (MEDAS)
The Mediterranean Diet Adherence Screener (MEDAS) was developed by Martínez-González et al. 20 to assess adherence to the Mediterranean diet. In this study, the Turkish version adapted by Özkan Pehlivanoğlu et al. 21 was used, with a Cronbach's alpha coefficient is 0.829. The scale consist of 14 items evaluating dietary habits such as the type of oil used in cooking, daily fruit and vegetable intake, consumption of margarine, butter, and red meat, as well as weekly consumption of foods such as wine, legumes, and seafood. Each item is scored as 0 or 1, resulting in a total score ranging from 0 to 14. High scores indicate greater adherence to the Mediterranean diet. Scores are classified as low (<7), moderate (7–8), and high (≥9) adherence. 21
Successful aging scale (SAS)
The Successful Aging Scale (SAS), developed by Demir-Çelebi and Yüksel, 22 is used to assess successful aging in individuals aged 60 years and older. The scale consists of 19 items and a single dimension, and is rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). There are no reverse-coded items, and total scores range from 19 to 95. The Cronbach's alpha coefficient for the scale was determined to be 0.96 and 0.90. High scores indicate a high level of successful aging.
Anthropometric measurements
The height (cm) and body weight (kg) measurements of the elderly individuals were obtained from current student registration forms. BMI was calculated using body weight (kg) and height (m2) information. Participants were categorized according to the BMI categories published by the World Health Organization (WHO) as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (≥30 kg/m2). 23
Data analysis
The data from the study were analyzed using the SPSS (25.0) program. The normality of the data distribution was examined using the Kolmogorov—Smirnov test, skewness and kurtosis values, histograms, and probability plots. Categorical variables are presented with frequency (n) and percentage (%), while continuous variables are presented with mean (X̄) and standard deviation (SD). The Independent Samples t-test was used for comparisons between two independent groups showing a normal distribution, and one-way ANOVA was used for comparisons between three independent groups. Before applying the one-way ANOVA test, Levene's test was applied to evaluate the homogeneity of the groups. If the test result was “p > 0.05,” the analysis was applied. The “Post-hoc Tukey HSC” test was used to determine which group the difference originated from. The relationships between numerical variables were determined using the Pearson correlation test. Linear regression models were used to determine the variables predicting food literacy. The significance level was set at 0.05.
Ethical approval
Prior to collecting the study data, ethical committee approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Alanya Alaaddin Keykubat University, dated October 8, 2024, with decision number 2024/20. The study was conducted in accordance with the Declaration of Helsinki, and voluntary informed consent was obtained from all participants.
Results
The general characteristics of the participants are presented in Table 1. Of the participants, 51.7% were aged 60–68 years (mean age: 68.9 ± 5.3 years), 79.2% were female, 55.8% were married, 46.7% had a university degree or higher, and 83.3% were retired. Additionally, 44.2% reported having an income below their expenses, 69.2% reported living with others, and 77.5% reported having at least one chronic disease. Hypertension (23.4%) was the most commonly reported chronic disease. Among the reported conditions, issues related to inadequate vitamin and mineral intake (31.1%) were also observed. A total of 72.5% of participants reported regular daily medication use, with antihypertensive and anticoagulant medications being the most frequently used (32.9% and 22.8%, respectively). Furthermore, 42.5% of participants reported using dietary supplements, with vitamin D (32.5%) and vitamin B12 (27.8%) being the most commonly used. The mean BMI was 27.9 ± 4.8 kg/m2, and 51.6% of participants were classified as overweight. The mean MEDAS score was 5.6 ± 1.9, and 67.5% of participants had low adherence to the Mediterranean diet. The mean SAS and SPFL scores were 84.7 ± 8.9 and 111.4 ± 14.0, respectively.
General characteristics of the participants (n = 120).
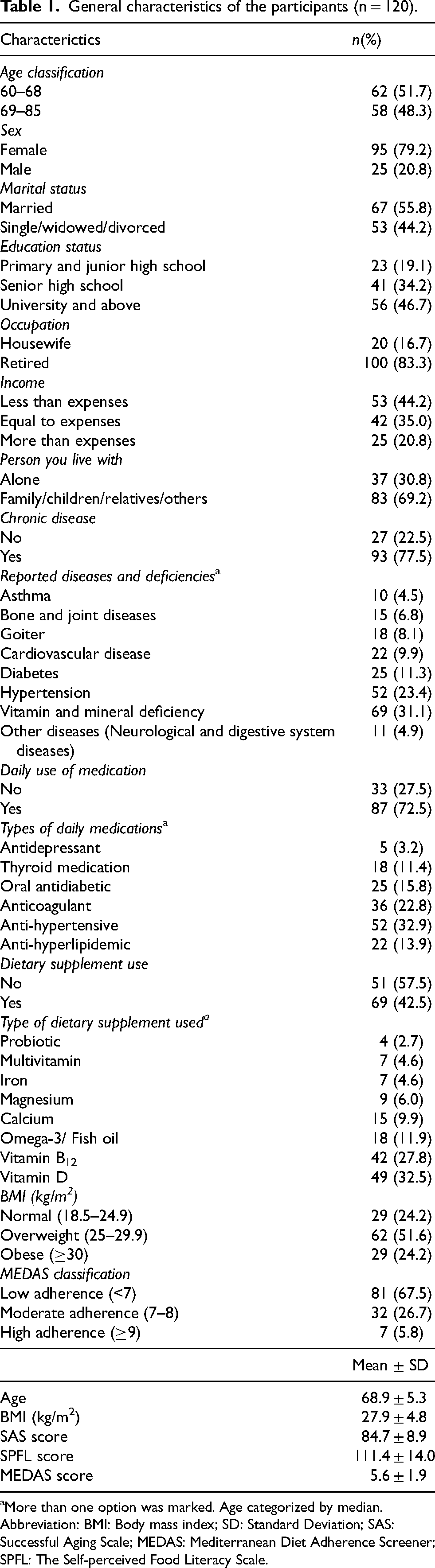
More than one option was marked. Age categorized by median.
Abbreviation: BMI: Body mass index; SD: Standard Deviation; SAS: Successful Aging Scale; MEDAS: Mediterranean Diet Adherence Screener; SPFL: The Self-perceived Food Literacy Scale.
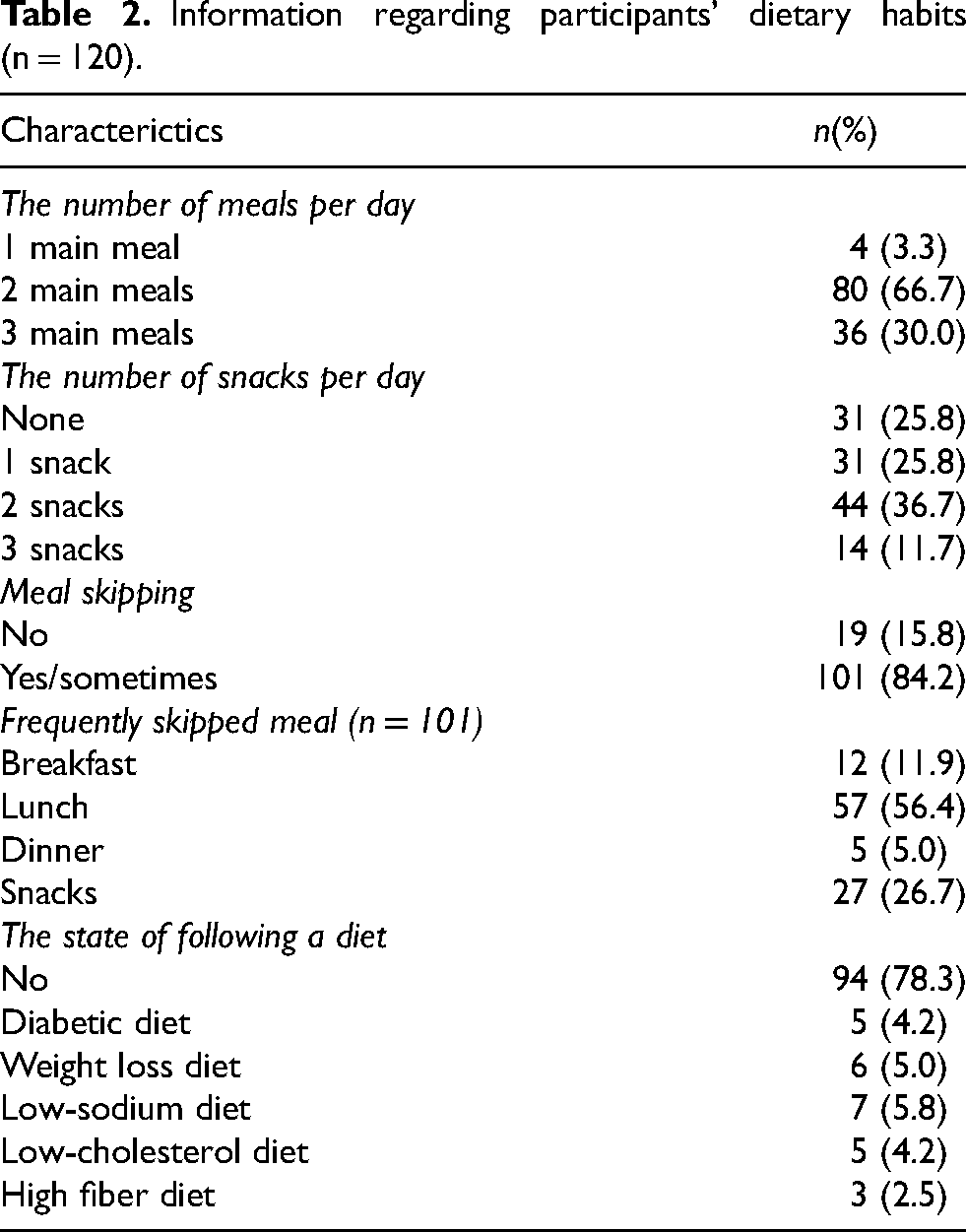
Information regarding participants’ dietary behaviors is presented in Table 2. Among the participants, 66.7% reported consuming two main meals per day and 36.7% reported consuming two snacks, while 84.2% reported skipping meals. Among those who skipped meals, lunch was the most frequently skipped meal (56.4%). Additionally, 78.3% of participants’ reported not following any specific diet.
Information regarding participants’ dietary habits (n = 120).
Information on MEDAS, SAS, and SPFL scores according to selected variables is presented in Table 3. A statistically significant difference in MEDAS scores was observed according to educational level and number of main meals (p < 0.05). Participants with a university degree or higher had significantly higher MEDAS scores compared to those with primary or secondary education (p < 0.05), while no significant difference was observed between primary and secondary education groups (p > 0.05). No significant difference in MEDAS scores was observed between participants consuming one main meal per day and other groups (p > 0.05). However, participants consuming two main meals per day had higher MEDAS scores compared to those consuming three main meals (p < 0.05). SAS and SPFL scores were significantly higher in women and in those with a BMI <25 kg/m2 (p < 0.05). No significant differences in MEDAS, SAS, and SPFL scores were observed according to age, marital status, income level, or presence of chronic disease (p > 0.05).
MEDAS, SAS and SPFL scores according to some variables.
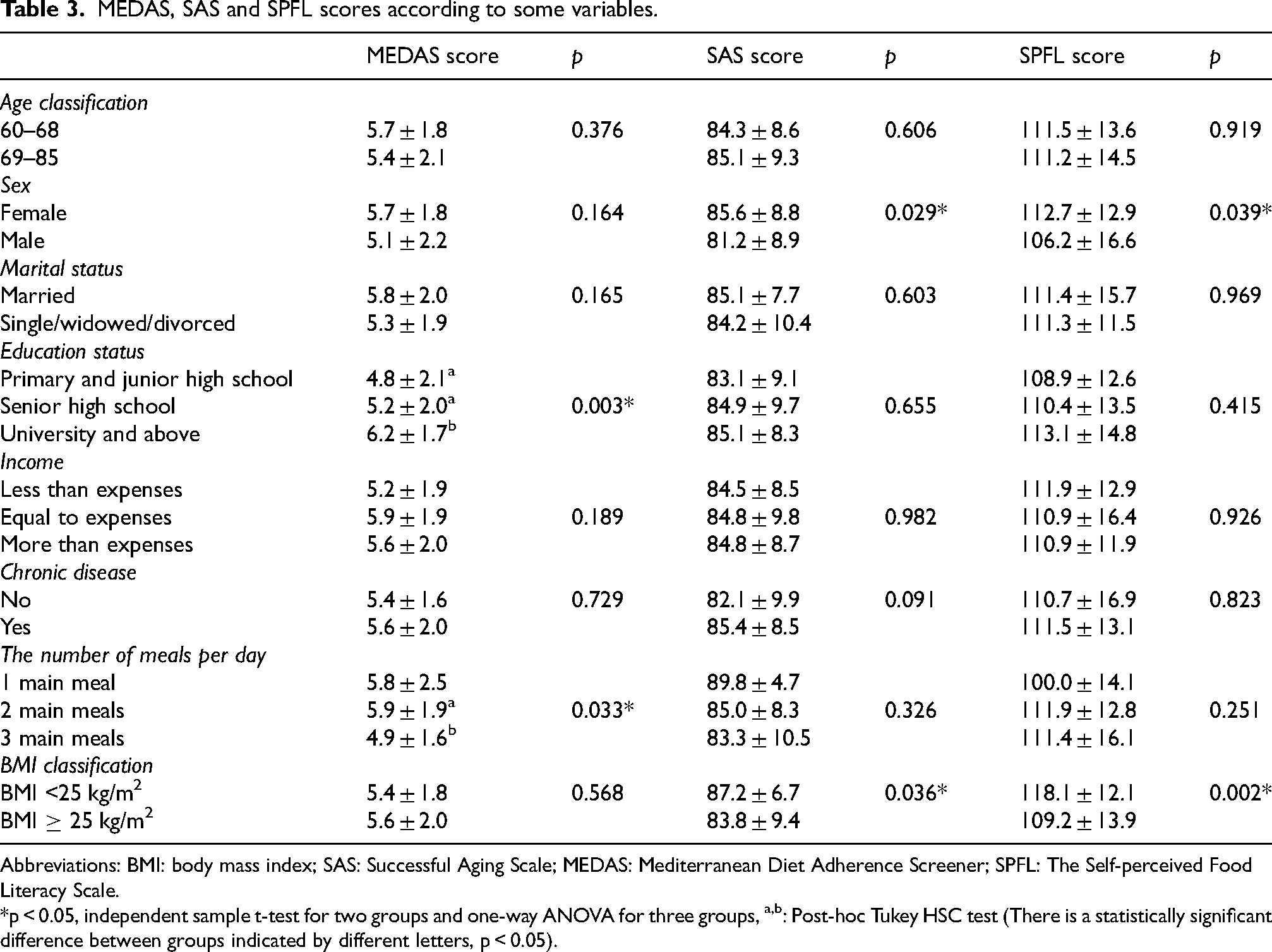
Abbreviations: BMI: body mass index; SAS: Successful Aging Scale; MEDAS: Mediterranean Diet Adherence Screener; SPFL: The Self-perceived Food Literacy Scale.
*p < 0.05, independent sample t-test for two groups and one-way ANOVA for three groups, a,b: Post-hoc Tukey HSC test (There is a statistically significant difference between groups indicated by different letters, p < 0.05).
The correlations between the study variables are presented in Table 4. The SPFL total score was positively correlated with all SPFL sub-dimensions, including food preparation skills (r = 0.660, p < 0.01), resilience and resistance (r = 0.718, p < 0.01), healthy snack styles (r = 0.672, p < 0.01), social and conscious eating (r = 0.493, p < 0.01), examining food labels, (r = 0.646, p < 0.01), daily food planning (r = 0.590, p < 0.01), healthy budgeting (r = 0.590, p < 0.01), and healthy food stockpiling (r = 0.439, p < 0.01). In addition, SPFL score were positively correlated with the MEDAS (r = 0.202, p < 0.05) and SAS scores (r = 0.485, p < 0.01), and negatively correlated with BMI (r = -0.241, p < 0.01). Among the SPLF sub-dimensions, food preparation skills were positively correlated with MEDAS (r = 0.292, p < 0.01) and SAS scores (r = 0.398, p < 0.01). Resilience and resistance were positively correlated with SAS scores (r = 0.231, p < 0.05) and negatively correlated with BMI (r = -0.325, p < 0.01). Healthy snack styles were positively correlated with MEDAS (r = 0.196, p < 0.05) and SAS scores (r = 0.414, p < 0.01).
Relationships between the variables in the study.
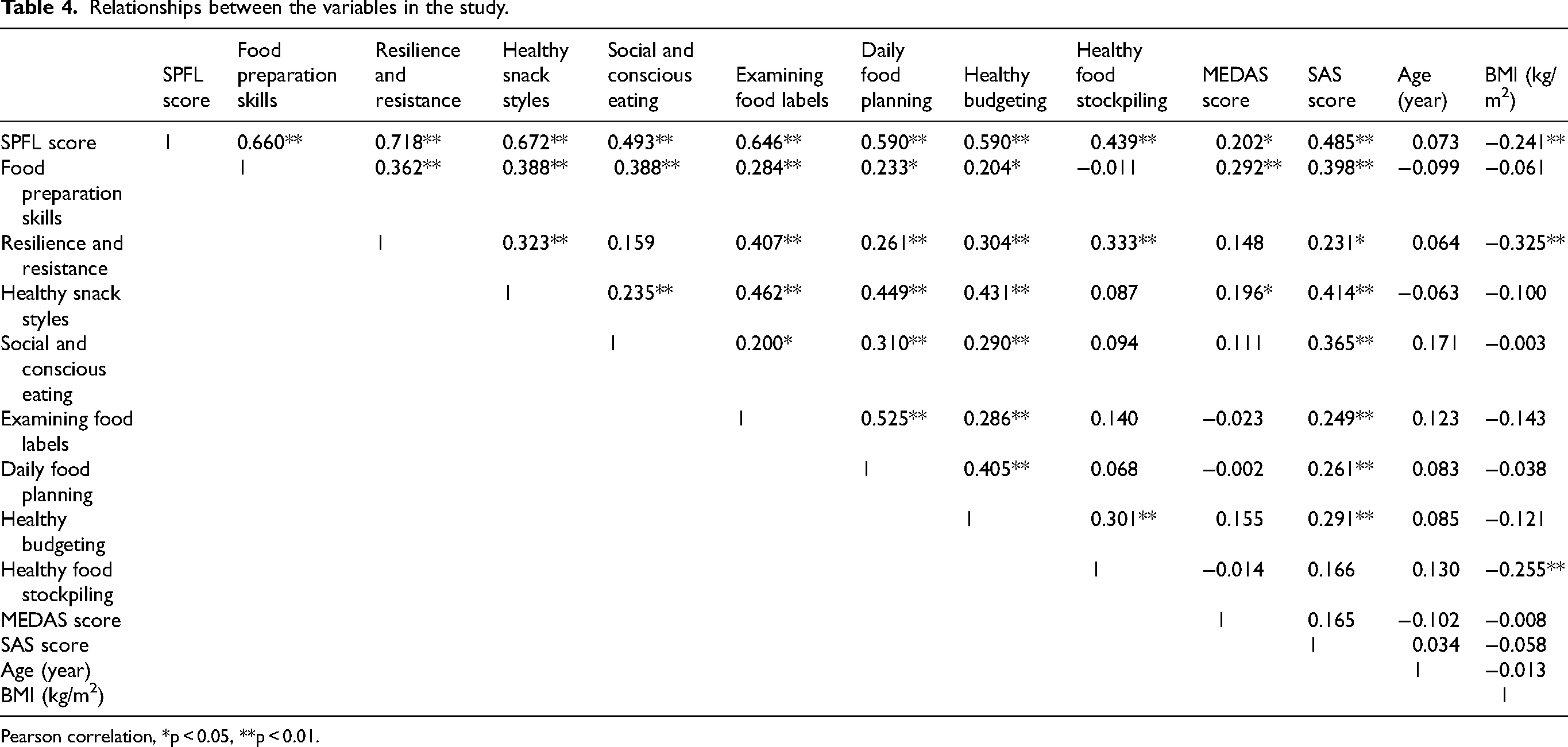
Pearson correlation, *p < 0.05, **p < 0.01.
Social and conscious eating, examining food labels, daily food planning, and budgeting on healthy foods were all significantly correlated with the SAS scores (r = 0.365, r = 0.249, r = 0.261, and r = 0.291, respectively; p < 0.01). Healthy food stockpiling was negatively correlated with BMI (r = -0.255, p < 0.01).
Linear regression analyses were conducted to examine the predictors of SPFL (Table 5). In Model 1, MEDAS was positively associated with SPFL (β=0.202, p = 0.027), explaining 4.1% of the variance. In Model 2, SAS was more strongly associated with SPFL (β=0.485, p < 0.001), accounting for 23.6% of the variance. In Model 3, which included MEDAS, SAS, and BMI as independent variables, SAS remained a significantly associated with SPFL (β=0.452, p < 0.001), while BMI was negatively associated with SPFL (β=-0.214, p = 0.007). However, the association between MEDAS and SPFL was not statistically significant (p = 0.113). The final model explained 29.7% of the variance in SPFL. Durbin—Watson values (1.629–1.765) indicated no evidence of autocorrelation in the regression models.
Linear regression analyses predicting food literacy.
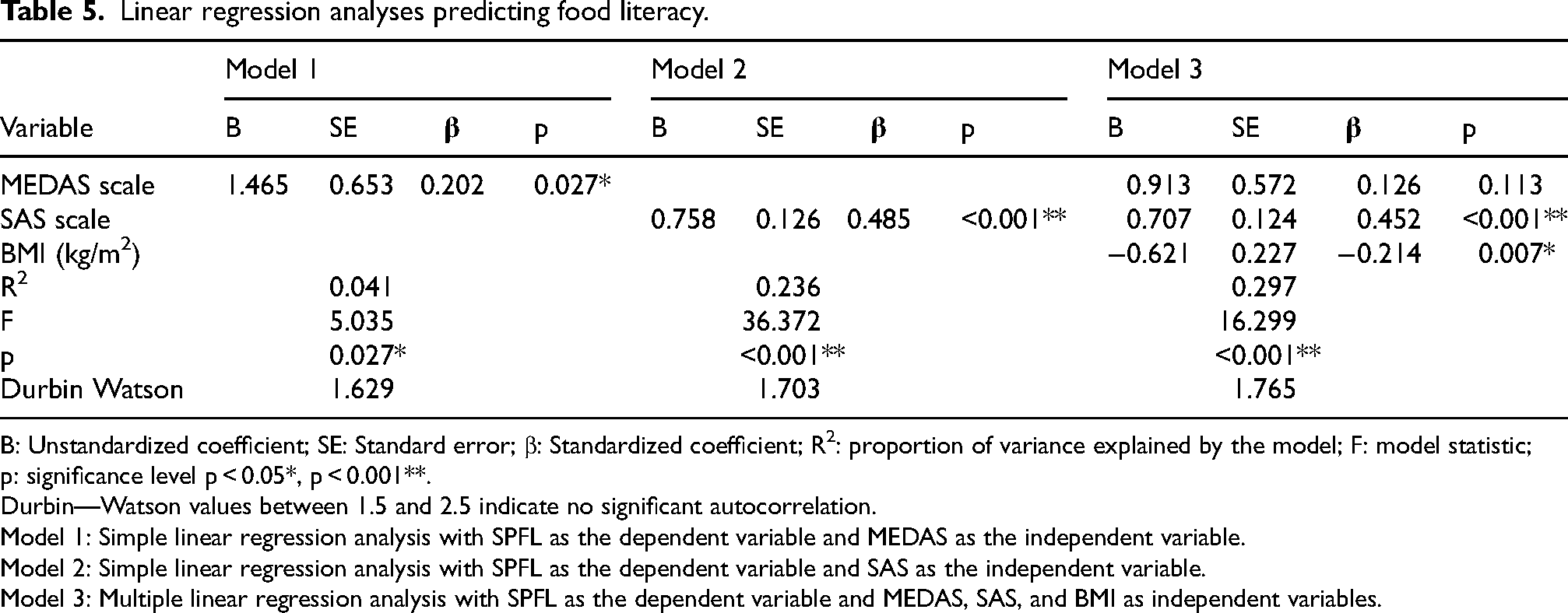
B: Unstandardized coefficient; SE: Standard error; β: Standardized coefficient; R2: proportion of variance explained by the model; F: model statistic; p: significance level p < 0.05*, p < 0.001**.
Durbin—Watson values between 1.5 and 2.5 indicate no significant autocorrelation.
Model 1: Simple linear regression analysis with SPFL as the dependent variable and MEDAS as the independent variable.
Model 2: Simple linear regression analysis with SPFL as the dependent variable and SAS as the independent variable.
Model 3: Multiple linear regression analysis with SPFL as the dependent variable and MEDAS, SAS, and BMI as independent variables.
Discussion
This study aimed to examine the association between food literacy, adherence to the Mediterranean diet, and successful aging among U3A students. The findings indicated that food literacy was positively associated with adherence to the Mediterranean diet and successful aging, and negatively associated with BMI. Notably, successful aging showed the strongest association with food literacy. However, this relationship should be interpreted with caution, as the cross-sectional design of the study does not allow for conclusions regarding directionality. Individuals with higher levels of successful aging may have better food literacy due to greater functional capacity, social engagement, and health awareness. Conversely, higher food literacy may also support successful aging by promoting healthier dietary behaviors and lifestyle choices. Therefore, a bidirectional relationship between these variables may be considered.
Food literacy, which encompasses individual behaviors related to the planning, selection, preparation, and consumption of healthy foods, is considered an important factor for achieving optimal nutrition.24,25 Given its close relationship with healthy eating behaviors, food literacy has been suggested to be associated with obesity and may play a role in maintaining a healthy body weight. 26 Previous studies examining the relationship between food literacy and BMI in adults have reported a negative association between these variables.27,28 Consistent with these findings, the present study showed that individuals with a BMI <25 kg/m2 had higher food literacy scores, and SPFL scores were negatively correlated with BMI. These findings are in line with previous literature suggesting that higher food literacy may be associated with more favorable body weight outcomes.
Additionally, our findings indicated that females had higher levels of food literacy compared to males. In a study evaluating the impact of sex on sustainable food literacy, greater involvement in meal preparation and cooking was associated with higher levels of food literacy, with this pattern more frequently observed among female participants. 29 However, the literature presents inconsistent findings, with some studies reporting higher food literacy levels among males, 30 while others have found no significant differences between sexes.31,32 Given this variability, the relationship between food literacy and sex remains inconclusive. Therefore, further studies with larger and more diverse populations are needed to better understand this association.
Healthy eating is one of the key factors in maintaining health and supporting successful aging in an aging population.33,34 In addition to social engagement, adherence to healthy dietary patterns such as the Mediterranean diet has been associated with successful aging and increased life expectancy. 35 In the present study, the mean Mediterranean diet adherence score was 5.6 ± 1.9, and 67.5% of participants showed low adherence. Several factors, including the high cost of healthy foods, limited accessibility, and time required for meal preparation, have been reported as barriers to adherence to the Mediterranean diet among older adults. 36 The majority of participants in this study were retired (83.3%) and a considerable proportion reported low income levels (44.2%), suggesting that socioeconomic factors may be associated with lower adherence to the Mediterranean diet. Consistent with our findings, a study conducted among U3A students in Antalya reported a mean Mediterranean diet adherence score of 7.58 ± 1.76, with 26.6% of participants showing low adherence. 37 Similarly, a study conducted among older adults in Australia reported a mean adherence score of 5.4 ± 2.4. 38 Furthermore, only 23.7% of older adults in Spain were reported to have high adherence to the Mediterranean diet, indicating that adherence may be declining even in Mediterranean countries. 39 Food insecurity has been identified as a potential barrier to adherence to the Mediterranean diet by limiting access to healthy foods 40 ; this factor was not directly assessed in the present study. Although the present study was conducted in the Mediterranean region, the relatively low adherence observed should be interpreted carefully and may be associated with socioeconomic and environmental factors affecting food access among older adults.
Other factors that may hinder adherence to the Mediterranean diet include limited knowledge about foods and inadequate food preparation skills. 41 In the present study, higher food preparation skills, one of the SPFL sub-dimensions, were associated with higher MEDAS scores. Consistent with these findings, a study conducted among Portuguese adults reported that higher cooking skills were associated with greater adherence to the Mediterranean diet. 42 However, evidence on the relationship between cooking skills and Mediterranean diet adherence among older adults remains limited. Food literacy, which is closely related to knowledge and education, has been suggested to influence eating behaviors. 43 In line with this, participants with higher educational levels in the present study had higher MEDAS scores. Additionally, a weak but significant positive correlation was observed between SPFL and MEDAS scores (r = 0.202), indicating a low-strength association whereby higher food literacy was related to greater adherence to the Mediterranean diet. This finding is consistent with a previous study suggesting that individuals with higher levels of food literacy may show greater adherence to the Mediterranean diet. 43 In light of all these findings, the results of the regression analysis indicated that adherence to the Mediterranean diet was positively associated with food literacy. This finding suggests that individuals who adopt healthier dietary patterns may have higher levels of nutritional knowledge. High food literacy has been identified as one of the factors associated with adherence to the Mediterranean diet. 36 Therefore, improving food literacy in older adults may represent a potential strategy for enhancing adherence to the Mediterranean diet.
In addition, recent studies conducted in Mediterranean populations have highlighted that adherence to the Mediterranean diet is also associated with contextual factors such as food security, which may influence individuals’ ability to access and maintain healthy dietary patterns.44,45 These findings suggest that, beyond individual knowledge and skills, broader environmental and socioeconomic factors may also play a role in shaping dietary adherence in older adults. Furthermore, evidence from Mediterranean settings also indicates that greater adherence to the Mediterranean diet may be associated with more favorable aging outcomes, supporting its potential role in successful aging.
Successful aging is influenced by multiple factors, including socio-demographic characteristics, lifestyle habits, and overall health status. 46 Although BMI is closely related to overall health status and has been associated with adverse health outcomes, 47 the evidence regarding the relationship between BMI and successful aging remains inconsistent. In British adults aged 42–63 years, individuals with a BMI ≥30 kg/m2 were reported to have lower successful aging rates compared to those with a BMI of 18.5–25 kg/m2. 48 In contrast, among Chinese individuals aged 60 years and older, obesity was positively associated with successful aging in men, whereas underweight women showed a negative association compared to those with normal BMI. 49 Similarly, in French adults aged 65–75 years, higher BMI was reported to be negatively associated with successful aging. 50 These inconsistent findings may be explained by differences in study populations and methodologies, including variations in age range, sex distribution, baseline BMI levels, general health status, and the presence of chronic diseases. In addition, differences in sample size and whether BMI was analyzed as a categorical or continuous variable may also contribute to the heterogeneity of the findings. In the present study, higher successful aging scores were observed among individuals with a BMI <25 kg/m2. However, this finding should not be interpreted as indicating that lower BMI directly promotes successful aging. The predominance of female participants in the study sample, the fact that most participants were classified as overweight, and the relatively small sample size may limit the generalizability of this finding. Furthermore, successful aging in older adults is likely shaped by a complex interaction of factors, including body composition, overall health status, and lifestyle behaviors, rather than BMI alone.
Women's responsibilities related to household duties, as well as social disadvantages such as lower educational attainment and socioeconomic status, limited access to healthcare services, and the presence of morbidities, have been reported as barriers to successful aging. 51 Previous studies have indicated that successful aging levels are higher in males than in females.7,52,53 However, in our study, successful aging scores were higher among females. This finding may be related to the characteristics of the study population, which consisted largely of women attending U3A programs, who may have higher levels of awareness and engagement in lifelong learning. However, these characteristics were not directly assessed in the present study and should therefore be interpreted with caution. In addition, females in this study demonstrated higher levels of food literacy, which may also be associated with successful aging. In the present study, the mean SAS score of the participants was 84.7 ± 8.9. Considering that the maximum possible score on the scale is 95, participants generally demonstrated relatively high levels of successful aging. This may be associated with active participation in university-based lifelong learning activities, increased awareness through educational initiatives, and continued social engagement with peers of similar age; however, these interpretations should be considered as hypothetical. In addition, optimizing opportunities for health, participation, and security in order to enhance quality of life with increasing age is closely related to the concept of active ageing. 6 Lifelong learning environments, such as U3A programs, have been reported to be associated with increased social participation, cognitive engagement, and improved well-being among older adults.54,55 These findings suggest that continued engagement in educational and social activities may contribute to successful ageing.
Successful aging has been associated with healthy eating behaviors, and identifying levels of food literacy related to knowledge and skills in this area is important for supporting healthy eating. Food literacy encompasses multiple components, including food preparation skills, daily food planning, healthy food choices, conscious eating, examining food labels, and budgeting for healthy foods. 19 Previous studies have suggested that cooking skills training is associated with greater adherence to healthy dietary patterns and may contribute to successful aging. 56 Additionally, a study conducted in Korea reported that older adults with higher food literacy had more adequate nutrient intake and significantly higher consumption of fresh fruits and vegetables. 57 Similarly, the Israel National Health and Nutrition Survey of Older Adults found that better nutritional quality was positively associated with successful aging among individuals aged 65 years and older. 58 Therefore, successful aging may be promoted through higher levels of food literacy, as individuals with greater food literacy tend to make healthier food choices.
The findings of the study showed that all SPFL sub-dimensions, except for healthy food stockpiling, were positively associated with successful aging. These results suggest that individuals with higher levels of food literacy may be more likely to make appropriate food choices, apply healthier cooking methods, and adopt behaviors associated with successful aging. In addition, the observed positive association between food literacy and successful aging indicates that individuals who are able to integrate healthy eating skills into their daily lives may be more likely to achieve healthier aging outcomes. The increase in explained variance from Model 1 to Model 2 suggests that successful aging was more strongly associated with food literacy compared to the other variables included in the models. In Model 3, which included adherence to the Mediterranean diet, successful aging, and BMI, these variables remained independently associated with food literacy. Moreover, the relatively strong association between SAS and food literacy suggests that food literacy is not only related to nutritional knowledge but may also be associated with factors such as individuals’ health status and quality of life. Therefore, higher levels of food literacy in older adults may be associated with the adoption of healthier dietary patterns, as well as with successful aging and weight management.
Limitations
Our study has several limitations. First, the use of WHO standard adult BMI cut-off points constituted a limitation, as physiological aging is associated with changes in body composition—specifically, a decrease in muscle mass and an increase in fat mass—even when body weight remains stable. These changes suggest that BMI may not be a sufficiently sensitive or adequate indicator on its own for assessing nutritional status and body composition in older adults, and therefore should be interpreted with caution. It is recommended that BMI be supported by additional anthropometric measurements that assess muscle mass and fat distribution. Although this study demonstrated associations between food literacy, adherence to the Mediterranean diet, and successful aging among individuals aged 60 years and older, no educational intervention was implemented; therefore, changes in behaviors aimed at improving food literacy could not be evaluated. Furthermore, physical activity levels were not assessed, which represents another limitation. In addition, the sample was predominantly composed of female participants, and the relatively small sample size (n = 120) may have limited the generalizability of the findings. Moreover, the study was restricted to U3A students aged 60 years and older, and its cross-sectional design limited the ability to generalize the results to the broader older adult population, as this group may have had higher levels of awareness and cognitive functioning. Finally, as the data were based on self-reports, recall bias and social desirability bias may have been present.
Conclusions
The results of this study indicate that higher food literacy among U3A students was associated with greater adherence to the Mediterranean diet, higher levels of successful aging, and lower BMI. These findings suggest that promoting food literacy may contribute to improved knowledge and more positive attitudes toward health eating among older adults. In this context, food literacy may play a supportive role in encouraging healthy dietary behaviors, facilitating the management of chronic diseases, and promoting successful aging. However, further longitudinal and interventional studies are needed to better understand the direction and causality of these relationships.
Footnotes
Acknowledgments
We would like to thank the U3A students who participated in our study.
Ethical considerations
Prior to data collection, ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Alanya Alaaddin Keykubat University, October 8, 2024, with decision number 2024/20.
Consent to participate
The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants included in the study.
Consent for publication
Not applicable
Author contributions
CŞK: conceptualization, methodology, investigation, formal analysis, writing – original draft, writing – review and editing; EE: writing – review and editing, formal analysis; HG, ÖN: data curation; MS: supervision. All authors approved the manuscript in its current form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.