
Abstract
Background
Chemotherapy is often associated with metabolic and functional disorders that may affect treatment outcomes in cancer patients. This study aimed to assess chemotherapy-induced changes in weight, body composition, nutritional status, biochemical parameters, and physical activity levels in Moroccan cancer patients.
Methods
This prospective cohort study involved 422 cancer patients treated by chemotherapy. Anthropometric measurements and bioelectrical impedance analysis were used to assess weight status and body composition. Nutritional status was evaluated using the Nutritional Risk Index, and biochemical parameters were obtained from the hospital's database. Physical activity levels were assessed by the International Physical Activity Questionnaire.
Results
After chemotherapy, there were significant reduction in fat-free mass and increase in body fat percentage (P < 0.001). The proportion of patients with moderate/severe malnutrition, sarcopenic obesity, and low muscle mass increased from 34.2%, 29.1%, and 49.1% pre-treatment to 50.0%, 39.3%, and 57.8% post-treatment, respectively. There was a significant decrease in total protein levels (P = 0.034). Physical activity and total energy expenditure decreased after chemotherapy (P < 0.001). Younger age (<60 years), low/moderate physical activity levels, and excessive body fat were independently associated with weight gain. Short disease duration (<12 months) and normal nutritional status were protective against moderate/severe weight loss, while non-excessive body fat increased such weight alteration. Non-malnourished patients and those without excess body fat had higher odds for low muscle mass.
Conclusions
Chemotherapy induced significant alterations in weight, nutritional status, body composition, and physical activity. Early implementation of nutritional and lifestyle interventions is needed in oncological care to prevent treatment-related malnutrition and adverse outcomes in cancer patients.
Keywords
Introduction
Cancer is a major global public health issue. Cancer is the second leading cause of death worldwide, and accounts for approximately 10 million deaths per year. About 30% of these deaths are due to five diet- and behavior-related risk factors, which are high body mass index (BMI), low intake of fruit and vegetable, low levels of physical activity, smoking, and alcohol consumption. 1
In Morocco, cancer is the second common cause of death (14%) just after cardiovascular diseases (38%). 2 Every year, an estimated 50,000 new cases are recorded in the country, and cancer-related mortality is considerable, though there are significant advancements in medical facilities and care. 3
Chemotherapy is a common treatment for cancer that reduces the risk of recurrence and improves overall outcomes. However, it may have several adverse side effects, such as alteration in weight and body composition, change in nutritional status, and reduced food intake.4,5 Such conditions may compromise treatment outcomes, affect quality of life, and increase the risk of comorbidities like cardiovascular diseases and diabetes.6,7
Cancer therapies also have been shown to cause significant impacts on nutritional status. In previous studies, it has been found that up to 40% of cancer patients may suffer from malnutrition and show lower survival rates compared to those with normal nutritional status for their cancer treatment.8,9 Some of the common nutritional disorders found during cancer are malnutrition, cachexia, or being overweight at various phases of the disease. 10
It is important for a patient with cancer, and particularly one undergoing chemotherapy, to maintain a healthy nutritional status. Cancer and its treatment can result in a loss of appetite, fatigue, gastrointestinal disturbances, vomiting, and muscular weakness. Some of these effects can lead to malnutrition, lowered chemotherapy tolerance, and poor quality of life. 11
From a therapeutic point of view, non-pharmacologic approaches like exercise can be highly beneficial as additional therapies for preserving normal nutritional status and body composition. Exercise can be employed to improve muscle volume status, metabolism, appetite, and reduce fatigue among cancer patients.12,13 Various studies have confirmed that even moderate exercises can avoid sarcopenia, lower systematic inflammation, and increase tolerance to cancer treatments. 12
Several tools have been standardized for the investigation of the patients’ nutritional status, especially in clinical settings. These tools include the use of anthropometric values weight and BMI), body composition parameters (fat mass and muscle mass), biochemical values (albumin, C-reactive protein, and glucose) and nutritional scoring systems known as nutritional risk indices. Of these, the nutritional risk index (NRI) is one of the most recognized and validated methods to determine which patients are at risk for nutritional complications. It is determined based on serum albumin levels, recent weight loss and therefore serves as an objective indicator for nutritional risk assessment. The use of NRI allows the early diagnosis of malnutrition and therefore the prompt provision of nutritional support with effective management of the treatment regimen.14,15
The purpose of this study was to assess chemotherapy- related changes in weight, body composition, biochemical markers, and physical activity levels among Moroccan cancer patients. It also aimed to investigate factors associated with abnormal nutritional status, weight gain, moderate to severe weight loss, and low muscle mass. Understanding such factors can help healthcare professionals to provide appropriate preventive measures, improve nutritional assessment, and effectively aid patients to cope with side effects triggered by chemotherapy cycles.
Methods
Study design
This prospective cohort study was carried out between February 2023 and December 2024 at Sidi Mohamed Iben Abdillah National Institute of Oncology (NIO) in Rabat, Morocco. The study involved patients with solid tumors who received adjuvant chemotherapy at the day hospital of the NIO. The eligibility criteria included histologically confirmed cancer diagnosis, indication of adjuvant chemotherapy, ability to respond to all questionnaires’ items, and compliance with follow-up. Exclusion criteria included significant diseases that may potentially impact nutritional status regardless of cancer, such as advanced renal disease, apparent acute infections, metastatic cancer, and mental impairments that affect communication. Only participants who provided written informed consent were involved. The minimum required sample size was calculated using the following Cochran's formula:
16

Data collection
Sociodemographic and clinical data
Data on sociodemographic parameters include age, sex, education level, and type of health insurance, while the clinical information needed in this study included cancer type, cancer stage, which was categorized from stage I to stage III, disease duration, follow-up duration, and comorbidities. These data were retrieved from the hospital's database.
Anthropometric measures
The anthropometric measurements were taken by standardized tools and procedures. Body weight was measured with a Seca digital scale, with a capacity of 150 kg and accuracy of 100 g, and height was measured using a portable adult stadiometer with a capacity of 200 cm and accuracy of 1 mm. 17 The patients’ body mass index (BMI) was calculated by the formula weight/height2. Based on the WHO criteria, subjects were classified as underweight (BMI<18.5 kg/m2), or normal weight (18.5 kg/m2 ≤BMI<25.0 kg/m2), or overweight (25.0 kg/m2 ≤BMI < 30.0 kg/m2), or obese (BMI≥30.0 kg/m2). 18
Body composition analyses
Body composition variables were determined by bioelectrical impedance analysis (BIA), using a multifrequency body composition analyzer (Nutriguard-MS; Germany), as recommended in current guidelines.
19
BIA measurements were conducted under standard settings with the placement of four self-adhesive electrodes on the back of the patient's right hand and right foot in supine position. According to the previous studies that explored BIA in assessing body composition in patients with cancer,
20
the Geneva equation was employed to estimate fat-free mass (FFM) of the subjects based on their resistance (R50) and reactance (Xc50) at 50 kHz frequency:
21
Fat Mass (FM), Body Fat Percentage (BF%), and Fat-Free Mass Index (FFMI) were calculated using the following formulas:



Excess body fat was defined based on BF% value by age and sex: (i) 20 to 39 years: >19% for men and >32% for women; (ii) 40 to 59 years: >21% for men and >33% for women; (iii) and 60 to 79 years: >24% for men and >35% for women. 22
Malnutrition was assessed according to the Global Leadership Initiative on Malnutrition (GLIM) criteria: (i) Low BMI (< 20 kg/m2 if age <70 years and < 22 kg/m2 if age ≥ 70 years); (ii) Weight loss during the previous six months (Moderate malnutrition: loss of weight > 5%; Severe malnutrition: loss of weight > 10%); and (iii) Low muscle mass (FFMI < 17 kg/m2 in male and FFMI < 15 kg/m2 in female). 23 Patients with both excess BF% 22 and low muscle mass 23 were diagnosed to have sarcopenic obesity.
Biochemical parameters
The biochemical parameters included in this study were albumin, total proteins, blood glucose levels, C-reactive proteins, urea levels, and creatinine levels. The values were obtained from the hospital's database. The Nutritional Risk Index (NRI) was calculated using the following formula:
24

On the basis of the NRI, patients were categorized into three groups: (i) No malnutrition (NRI>100); (ii) Moderate malnutrition (83.5 ≤ NRI≤100); and (iii) Severe malnutrition (NRI<83.5).
Physical activity
Data on physical activity were collected using the shortened version of the International Physical Activity Questionnaire (IPAQ), where the activity concerned the last seven days. The activity value was estimated in metabolic equivalent of task - minutes per week (in MET-min/week). According to the IPAQ manual scoring procedure, the total value in MET-min/week value was estimated by summing the minutes spent in vigorous, moderate, and walking activities with coefficients of 8.0 METs for vigorous activities, 4.0 METs for moderate activities, and 3.3 METs for walking activities.
25
The total energy expenditure expressed in MET-min/week was calculated using this formula:
Patients were then divided into three groups based on their values of the “Activity Level”: (i) Low activity level: less than 600 MET-min/week; (ii) moderate activity level: 600 to 3000 MET-min/week; and (iii) high activity level: more than 3000 MET-min/week.
Ethical considerations
The study protocol was approved by the Biomedical Research Ethics Committee of the Faculty of Medicine and Pharmacy, Rabat, Morocco (Approval N° 99/22). All participants were informed about the objectives and procedures of the study, and written consent was obtained from each subject. Participation in the study was strictly voluntary, on non-remunerated basis, and with the right to withdraw at any stage.
Statistical analyses
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS), version 22.0. The normality of variable distribution was checked by the Kolmogorov-Smirnov test. The results are presented as mean (± standard deviation) or as medians and interquartile ranges (25th–75th percentile) for continuous variables and proportions for categorical variables. Comparisons of continuous and categorical variables were done by Student's t-test and by Chi-square test, respectively. The Mann-Whitney U Test was used to compare values when the assumption of normality is not met. Binary logistic regression analyses were performed to identify the factors associated with weight gain, moderate to severe weight loss, and low muscle mass. We estimated the adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs). The models were adjusted for all independent variables, including age, education level, cancer type, disease stage, disease duration, follow-up period, weight status, body fat level, Nutrition Risk Index (NRI), comorbidities, and physical activity level. Statistical significance was set at P < 0.05.
Results
The study included 422 patients whose sociodemographic and clinical characteristics are summarized in Table 1. The mean age was significantly higher for men than for women (P < 0.001). Most women were aged between 40 and 59 years, whereas the majority of men were older than 60 years of age. More than half of the patients were illiterate (56.8%), and almost all of them had health insurance (96.9%), which also significantly differed by sex (P = 0.035). The cancer types significantly differed by sex, with gyneco-mammary cancers predominating among women, while gastrointestinal and urologic cancers were more common in men. Women were more frequently diagnosed with cancer at an early stage, whereas men were more often diagnosed at advanced stages. Comorbidities were also significantly more frequent in women than in men (P < 0.001).
Sociodemographic and clinical characteristics of the study population.
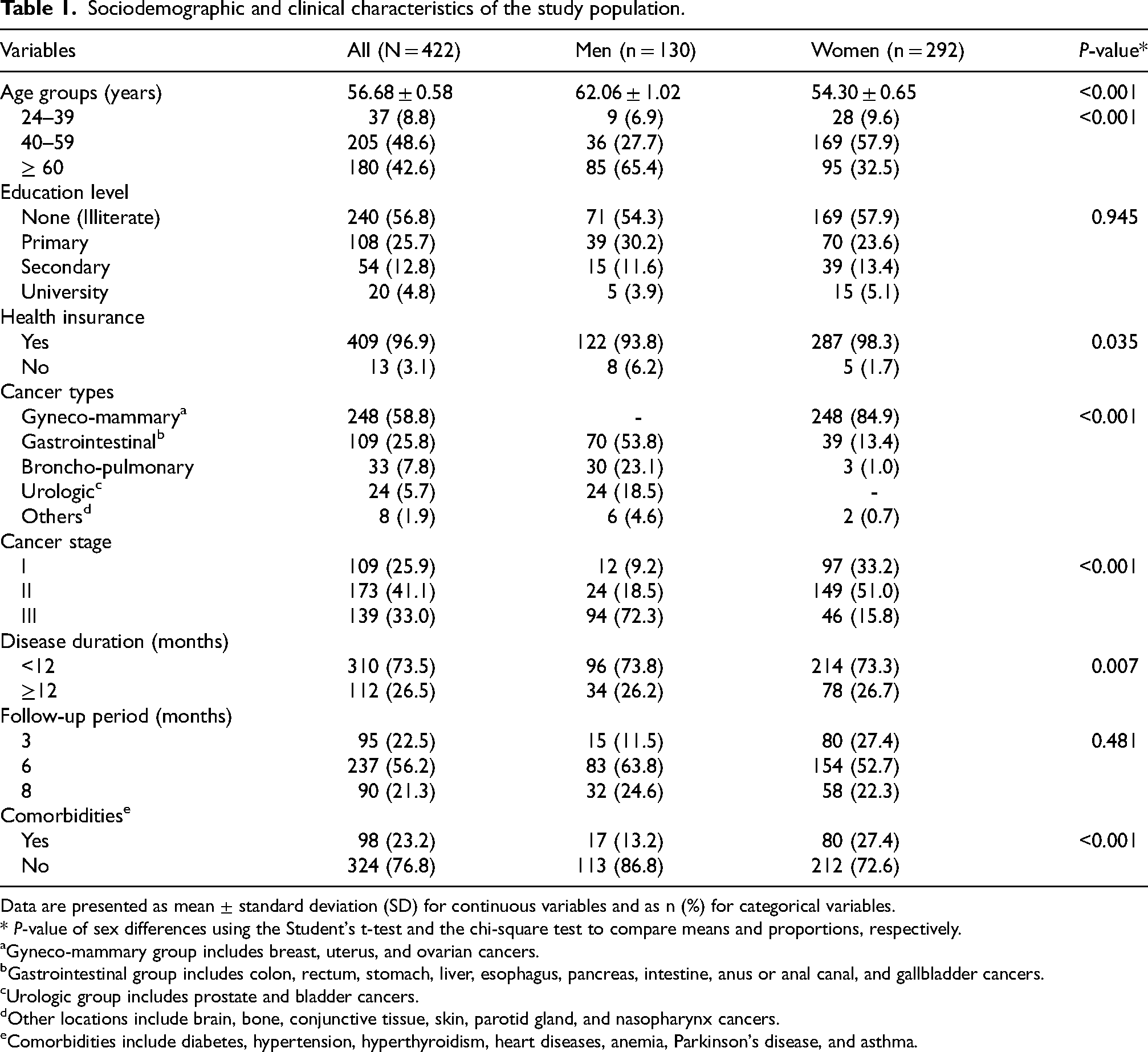
Data are presented as mean ± standard deviation (SD) for continuous variables and as n (%) for categorical variables.
* P-value of sex differences using the Student's t-test and the chi-square test to compare means and proportions, respectively.
Gyneco-mammary group includes breast, uterus, and ovarian cancers.
Gastrointestinal group includes colon, rectum, stomach, liver, esophagus, pancreas, intestine, anus or anal canal, and gallbladder cancers.
Urologic group includes prostate and bladder cancers.
Other locations include brain, bone, conjunctive tissue, skin, parotid gland, and nasopharynx cancers.
Comorbidities include diabetes, hypertension, hyperthyroidism, heart diseases, anemia, Parkinson's disease, and asthma.
After adjuvant chemotherapy, body weight significantly decreased in the overall sample (P < 0.001), whereas BMI did not differ significantly. Significant differences were observed in body composition parameters. In the overall sample, as well as in females, fat-free mass (FFM) and fat-free mass index (FFMI) were significantly reduced (P < 0.001). In contrast, fat mass (FM), fat mass index (FMI), and body fat percentage (BF%) significantly increased (P < 0.05). There were no significant differences in biochemical parameters after undergoing chemotherapy, except a significantly reduced total protein levels in the overall sample (P = 0.036). Albumin levels decreased, with a borderline statistical significance (P = 0.065). However, blood glucose, urea, creatinine, and C-reactive protein (CRP) levels increased, but with no significance. Energy expenditure was significantly lowered after undergoing chemotherapy (P < 0.001). The overall physical activity levels tended to decrease, with a significant increase in the low-activity level and a significant reduction in the high-activity level (P < 0.001) (Table 2).
Changes in weight, BMI, body composition, biochemical parameters, energy expenditure, and physical activity in cancer patients after receiving chemotherapy.
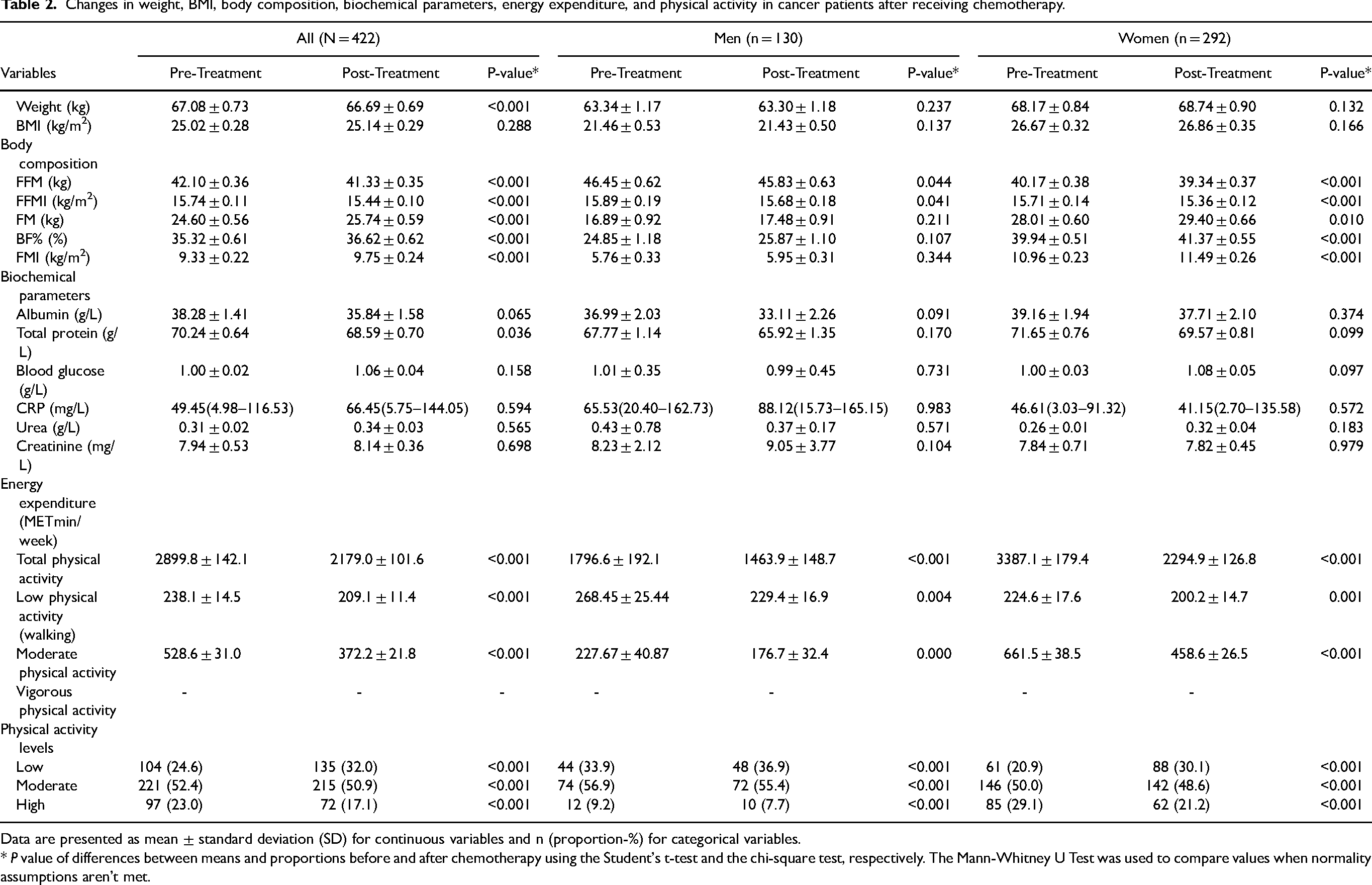
Data are presented as mean ± standard deviation (SD) for continuous variables and n (proportion-%) for categorical variables.
* P value of differences between means and proportions before and after chemotherapy using the Student's t-test and the chi-square test, respectively. The Mann-Whitney U Test was used to compare values when normality assumptions aren’t met.
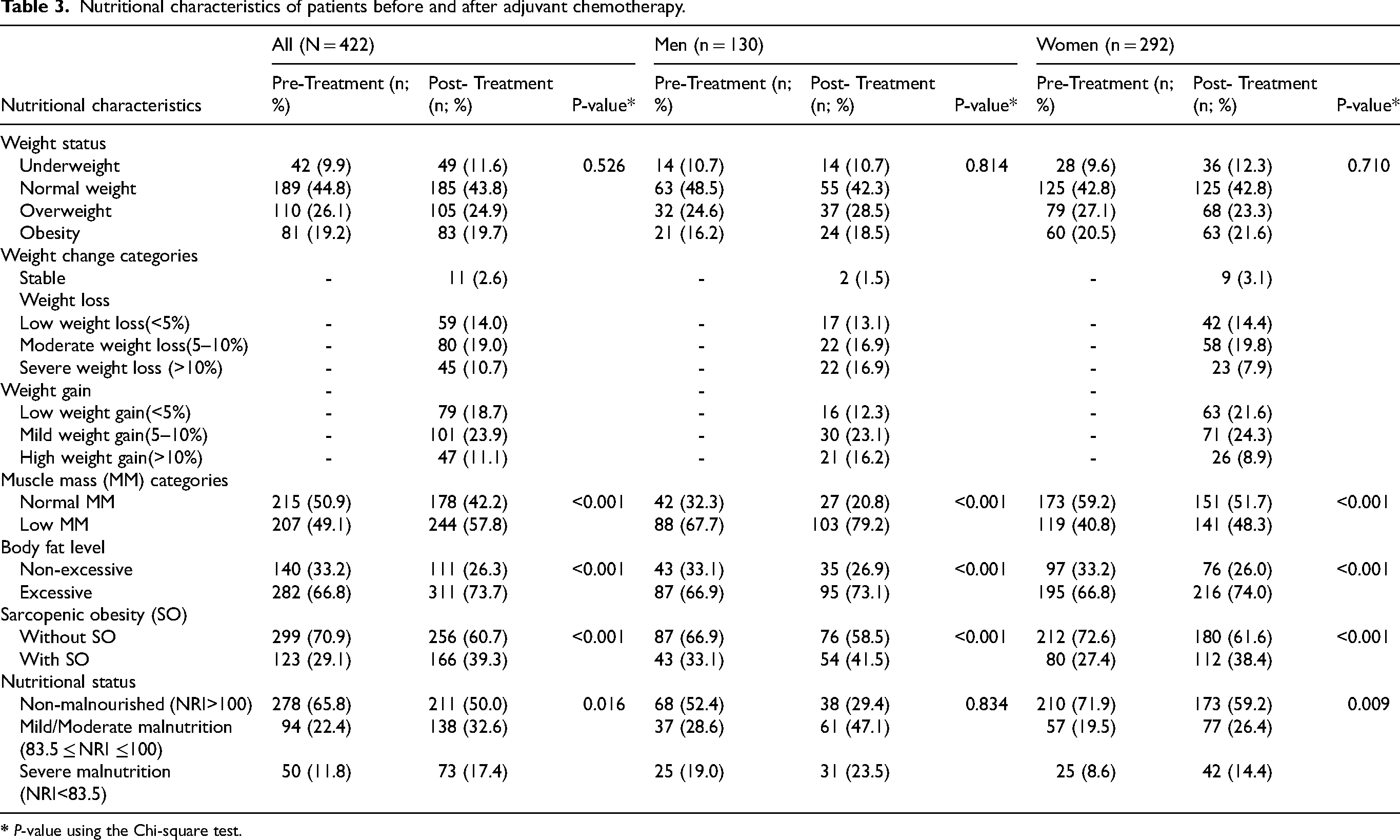
The nutritional characteristics of the study sample, before and after adjuvant chemotherapy, are presented in Table 3. Overall, 43.7% of patients experienced weight loss, while 53.7% gained weight. Weight gain was more frequently observed in women, whereas severe weight loss was more common in men. The prevalence of low muscle mass increased from 49.1% to 57.8% (P < 0.001), with a higher rise in men (from 67.7% to 79.2%). Excess body fat also increased from 66.9% to 73.1% in males and from 66.8% to 74.0% in females (P < 0.001). Similarly, the proportion of patients with sarcopenic obesity significantly increased among the study population, from 29.1% before chemotherapy to 39.3% after chemotherapy (P < 0.001), affecting both men (from 33.1% to 41.5%) and women (from 27.4% to 38.4%). The proportion of patients with moderate and severe malnutrition increased from 22.4% and 11.8% before chemotherapy to 32.6% and 17.4% after treatment, respectively.
Nutritional characteristics of patients before and after adjuvant chemotherapy.
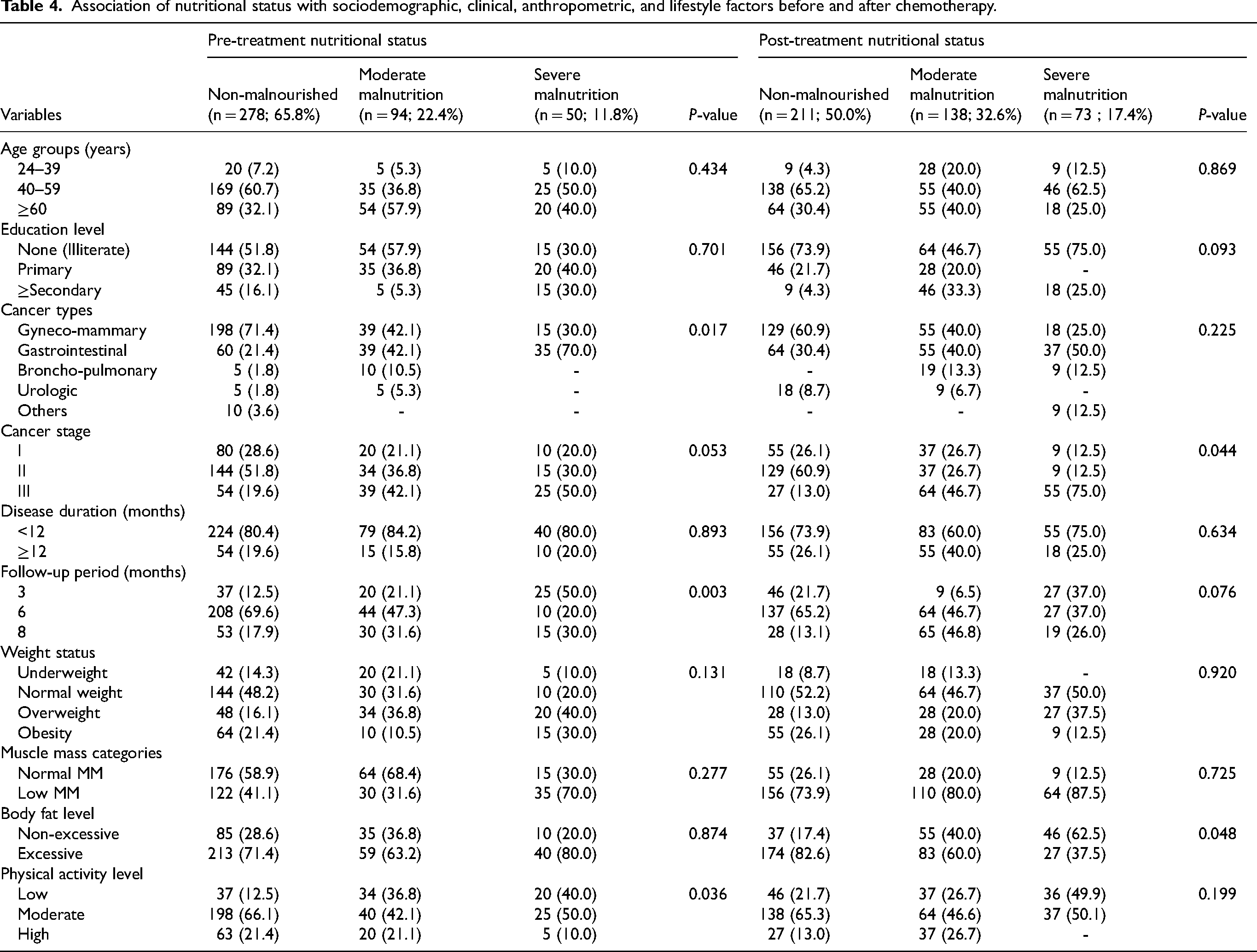
After chemotherapy, the overall proportion of patients with normal nutritional status decreased from 65.8% to 50.0%, while those with moderate- to-severe malnutrition increased from 34.2% to 50.0% (Table 4). Before treatment, nutritional status was significantly associated with cancer types (P = 0.017), follow-up period (P = 0.003), and physical activity level (P = 0.036). After treatment, nutritional status was significantly linked to cancer stage (P = 0.044) and body fat levels (P = 0.048).
Association of nutritional status with sociodemographic, clinical, anthropometric, and lifestyle factors before and after chemotherapy.
Logistic regression analysis showed that patients aged < 60 years and those with low/moderate physical activity levels had higher odds of gaining weight than patients aged ≥ 60 years and those with high physical activity levels (aOR = 4.55; 95% CI: 2.02–20.35; P = 0.047 and aOR = 3.20; 95% CI: 2.38–4.33; P < 0.001, respectively). Additionally, patients with no excess body fat had a lower likelihood of gaining weight than patients with excess body fat (aOR = 0.34; 95% CI: 0.15–0.78; P = 0.011).
Patients with a shorter disease duration (<12 months) and those who had normal nutritional status (NRI>100) were found to be significantly less likely to have moderate/severe weight loss compared to those with a longer disease duration and malnutrition (aOR = 0.36; 95% CI: 0.17–0.78; P = 0.009; and aOR = 0.31; 95% CI: 0.11–0.85; P = 0.023, respectively). In contrast, patients without excess body fat were found to have significantly higher odds of experiencing moderate/severe weight loss than those with excess body fat (aOR = 5.15; 95% CI: 2.70–12.63; P < 0.001).
In addition, for patients under 60 years old, underweight or normal weight, and without sarcopenic obesity, there was a significant reduction in the likelihood of having low muscle mass compared to those older than 60 years, overweight or obese, and with sarcopenic obesity (aOR = 0.43; 95% CI: 0.30–0.68; P = 0.026; aOR = 0.71; 95% CI: 0.54–0.98; P = 0.007; and aOR = 0.34; 95% CI: 0.15–0.65; P = 0.002, respectively). In contrast, patients without excess body fat and those who were non-malnourished had significantly higher odds of having low muscle mass (aOR = 1.85; 95% CI: 1.40–2.30; P = 0.008; and aOR = 2.57; 95% CI: 1.11–4.18; P = 0.028, respectively). (Table 5)
Predictors of weight gain, moderate/severe weight loss, and low muscle mass among cancer patients after chemotherapy.
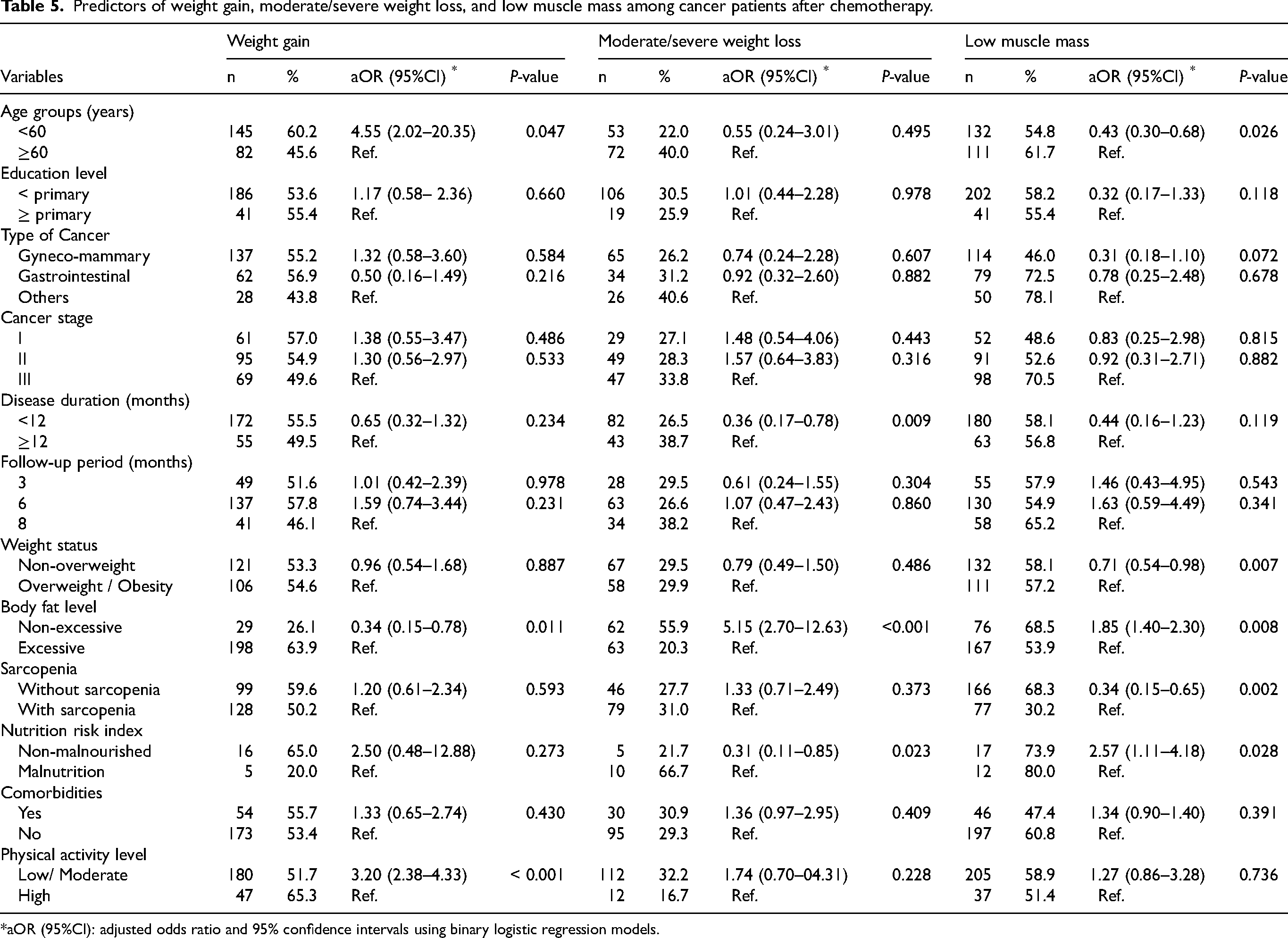
aOR (95%CI): adjusted odds ratio and 95% confidence intervals using binary logistic regression models.
Discussion
This prospective cohort study aimed to investigate chemotherapy-related changes in weight, body composition, nutritional status, biochemical markers, and physical activity levels in cancer patients. Overall, 43.7% of the patients lost weight, whereas 53.7% experienced weight gain. Moderate and severe weight loss was observed in 19.0% and 10.7% of the patients, respectively, with men being more affected than women. Our findings are consistent with other studies that found weight loss to be a common side effect of chemotherapy, particularly in patients with advanced tumor stages or gastrointestinal cancers.5,26–28 For example, a study conducted in Ethiopia reported that 35.8% and 42.2% of patients who received chemotherapy experienced severe and moderate weight loss, respectively. 5
Our results showed that 23.9% and 11.1% of the patients experienced mild and high weight gain, respectively. This is in line with several previous studies that have reported an increase in the proportion of patients who gained at least 5% of their body weight after receiving chemotherapy.29–32 It should be noted, however, that weight gain may vary depending on the type of cancer and treatment regimens. In fact, earlier studies have shown that weight gain of more than 5% was mainly seen in breast cancer patients (33.9%), 32 while only 5.7% of colorectal cancer patients gained weight. 30 These findings highlight the importance of early dietary interventions and weight change monitoring, particularly for vulnerable cancer patients who may experience significant weight loss.
Body composition analysis, after chemotherapy, indicated a significant decrease in fat-free mass (FFM) and an increase in fat mass (FM), particularly among women. The proportion of patients with sarcopenic obesity increased from 29.1% to 39.3%, whereas the proportion of patients with low muscle mass increased from 49.1% to 57.8%, with the largest rise seen in men, from 67.7% to 79.2%. Our findings are consistent with several previous studies that have shown a significant decrease in skeletal muscle mass during chemotherapy, with sarcopenia more common in men than in women.33,34,35 A recent meta-analysis of studies that included 81,814 patients with solid cancers found the baseline occurrence of sarcopenia to be 35.3%, but a marked increase to over 50% after chemotherapy was seen in patients with cancers such as esophageal cancer, urothelial carcinoma, and pancreatic cancer. 36 Sarcopenia is associated with increased treatment toxicity and poor prognosis. 37 Although large-scale studies are required to evaluate the effects of changes in FFM and FM in cancer patients treated by chemotherapy, our study emphasizes that it is essential to identify individuals with sarcopenia and sarcopenic obesity, as once detected, appropriate early healthcare interventions can be implemented.
Our study showed no major changes in biochemical parameters, except the significant decrease in total protein and a borderline reduction in albumin. This could be attributed to treatment effects on protein synthesis or nutritional intake, as reported in a previous study on the nutritional impact of chemotherapy in cancer patients. 38 There were slight increases in urea, creatinine, and CRP levels, but they were non-statistically significant. These findings suggest that renal function and CRP levels were not significantly affected, in line with previous studies reporting no major changes in these biochemical parameters after treatment. 39
The evaluation of nutritional status pre- and post-chemotherapy has shown that the proportion of patients with moderate to severe malnutrition increased significantly from 34.2% to 50.0%. Our findings support those reported in other studies, including one on patients undergoing head and neck cancer chemoradiotherapy which demonstrated a significant decrease in the number of non-malnourished patients (NRI ≥ 100) from 23 to 8 after the treatment. 40 These data emphasize the deleterious impact of chemotherapy on patients’ nutritional status. Given its sensitivity from both a functional and metabolic perspective, the nutritional risk index may be more informative for assessing the nutritional status of cancer patients than other commonly used indicators such as BMI.14,15
As shown in recent studies, the mechanisms underlying nutritional status changes and body composition during chemotherapy may not be limited to reduce energy intake. It is now well established that cancer- and treatment-related systemic inflammation, oxidative stress, and metabolic dysregulation are important contributors to malnutrition and muscle wasting in patients with cancer.11,41 Furthermore, chemotherapy-induced alterations in the gut microbiota may contribute to inflammatory and metabolic disturbances, which could lead to malnutrition and changes in body composition. Recent studies have highlighted complex interactions between the microbiome, diet, nutritional status, and muscle mass in patients with cancer. 42 In addition, alterations in the gut microbiota associated with cancer and chemotherapy have also been described. 43 These mechanisms may partly explain the alterations in weight, muscle mass, and nutritional parameters observed in the present study.
After chemotherapy, there was a significant decrease in both physical activity level and total energy expenditure (P < 0.001). Consistent with our results, a recent scoping study of 65 longitudinal and cross-sectional studies in cancer patients reported that 82% of studies showed a reduction in physical function following chemotherapy, independent of cancer type and age, highlighting the adverse effect of chemotherapy on physical performance. 44 The observed decline in physical activity is due to treatment-induced fatigue, a commonly reported side effect, that, in turn, may contribute to body fat accumulation and progressive muscle atrophy. The consequences of such a trend in physical activity not only impact functional ability but also accelerates detrimental effects on body composition. Importantly, these effects are reversible. Many previous studies have demonstrated that structured exercise programs during and/or after chemotherapy can mitigate the loss of physical function and help in maintaining a healthy body composition.45,46 In addition, Cormie et al. (2017) noted that regular exercise in cancer patients is associated with a decreased mortality rate, a lower chance of recurrence, and fewer side effects from treatment. 12 Thus, these findings underline the particular role of physical activity in oncology as an adjunct to chemotherapy, reducing the functional and metabolic impairments associated with anti-cancer treatments.
Logistic regression analysis revealed that younger age was a significant predictor of weight gain following chemotherapy, where patients under 60 years had increased odds of gaining weight (aOR = 4.55; 95% CI: 2.02–20.35; P = 0.047). Our results are consistent with evidence obtained from large mixed-gender cohort studies, indicating that young patients have higher chances of gaining weight after treatment.47,48 This association of younger age with post-treatment weight gain, observed among various cancer types in both men and women, suggests that age-related metabolic, hormonal or behavioral factors influence weight trajectories after therapy. On the other hand, young patients may tolerate treatment better and recover appetite more easily, and thus are more likely to gain weight.
Excess body fat and low to moderate physical activity levels were identified as predictors of weight gain. Patients with low to moderate levels of physical activity were three times more likely to gain weight (aOR = 3.20; 95%CI: 2.38–4.33; P < 0.001). Our findings support recent studies showing that lower levels of physical activity during chemotherapy contribute to increased adiposity and sarcopenic obesity. 49 Moreover, earlier research showed that structured physical activity interventions may decrease fat gain and loss of muscle mass from treatment, and improve muscle strength and metabolic health. 50
Patients with a shorter disease duration were significantly less likely to experience moderate to severe weight loss compared to those with long disease duration (≥12 months) (aOR = 0.36; 95% CI: 0.17–0.78; P = 0.009). This is in line with other studies which shows the advantages of early diagnosis and therapy to preserve nutritional status of cancer patients.51,52
Patients with normal body fat levels had a significantly higher likelihood of experiencing moderate/severe weight loss (aOR = 5.15; 95% CI: 2.70–12.63; P < 0.001) and low muscle mass (aOR = 1.85; 95%CI: 1.40–2.30; P = 0.008). These results are consistent with both our previous study 53 and a well-established association between a high BMI and improved cancer outcomes.54,55 Adipose tissue is thought to have a protective function, as macrophages confined within this tissue can suppress cachexia-related lipolysis and thus prevent weight loss. 56 However, this remains a temporary effect that might coexist with metabolic disorders or sarcopenia. 57
In this study, patients who were not malnourished had significantly lower odds of losing weight, but a higher likelihood of having low muscle mass. In contrast, other studies found that well-nourished patients had lower odds of low muscle mass compared to malnourished patients, 58 while anti-cancer treatment outcomes were also improved. 59 Although more longitudinal studies are required to validate these relationships, our observations underscore the importance of early and regular nutritional counseling as a front-line intervention to prevent and treat weight and muscle wasting in cancer patients, 60 regardless of their nutritional status.
Study limitations
This study has some limitations that should be considered. Firstly, the heterogeneity resulting from variations in cancer type, stage of the disease, and treatments may have affected nutritional status and body composition parameters differently among patients. Although it is acceptable for a cohort study, this heterogeneity limits tumor-specific and treatment-specific inferences and may reduce the generalizability of the findings. Secondly, despite its simplicity and common application in assessing body composition, bioelectrical impedance analysis could present measurement bias. Thirdly, the absence of detailed data on energy and nutrient intake limited the evaluation of the impact of energy and nutrient consumption on weight and muscle mass changes. Lastly, although CRP was measured as an inflammatory marker, other biomarkers such as interleukin-6, TNF-alpha, and indicators of insulin resistance were not assessed. Furthermore, other biological mechanisms known to contribute to nutritional deterioration during chemotherapy, including systemic inflammation beyond CRP, oxidative stress, immune–metabolic dysregulation, and microbiome alterations, were not evaluated. Recent evidence suggests that nutritional decline and muscle wasting in cancer patients are biologically mediated phenomena and are not solely related to reduced caloric intake or behavioral factors. Disease- and chemotherapy-associated microbiome alterations have been reported in breast cancer patients, 43 while chemotherapy-related changes in inflammatory and oxidative status have also been demonstrated. 61 In addition, current ESPEN guidelines emphasize that nutritional assessment in oncology should integrate inflammatory and metabolic alterations in addition to anthropometric measurements. 11 Therefore, the absence of a broader biological and metabolic assessment limits the mechanistic interpretation of the observed changes.
In addition, the exclusion of patients with metastatic disease, advanced renal dysfunction, and acute inflammatory conditions may have introduced selection bias, resulting in a relatively clinically stable study population. Therefore, the findings are likely to reflect treatment-related effects primarily in patients receiving adjuvant chemotherapy and may underestimate the magnitude of nutritional deterioration and body composition changes observed in more advanced cancer populations, particularly those at higher risk of cachexia and severe sarcopenia.
Conclusion
Our study identified significant changes in weight, body composition, nutritional status, biochemical parameters, and physical activity levels in patients with cancer receiving adjuvant chemotherapy. A high proportion of patients exhibited either significant weight loss or weight gain, in association with sarcopenia. Younger age, low/moderate physical activity levels, and excessive body fat were associated with increased odds of weight gain. Short disease duration and normal nutritional status were associated with lower odds of moderate/severe weight loss, whereas non-excessive body fat was associated with higher odds of such weight alterations. Similarly, younger age, non-overweight status, sarcopenic obesity, and gyneco-mammary cancers were associated with a reduced likelihood of low muscle mass, whereas normal nutritional status and non-excessive body fat were associated with a higher probability of muscle depletion. The biological mechanisms underlying the observed changes could not be assessed within the scope of this study. The observational nature of the study, the absence of a control group, the lack of mechanistic biomarkers, and the clinical heterogeneity of the cohort limit causal interpretation of the findings. Overall, our findings strongly emphasize the need for early, targeted nutritional and lifestyle interventions during chemotherapy to prevent the worsening of malnutrition and its associated adverse outcomes among patients with cancer.
Footnotes
Acknowledgments
The authors would like to thank the staff of the National Institute of Oncology (NIO) Sidi Mohammed Ben Abdellah, for the assistance they provided in data collection. They also would like to thank all the patients who took part in this research.
Ethical considerations
The study protocol was approved by the Biomedical Research Ethics Committee of the Faculty of Medicine and Pharmacy, Rabat, Morocco (Approval N° 99/22). All participants were informed about the objectives and procedures of the study, and written consent was obtained from each subject. Participation in the study was strictly voluntary, on non-remunerated basis, and with the right to withdraw at any stage.
Author contributions
AB, NE, DD contributed to the Data collection, Formal analysis, Software, Writing, Reviewing, and Editing. SM and SB contributed to the Conceptualization, Investigation, Supervision, Validation, Writing, Reviewing and Editing. SB, SL, HA, and ZE contributed to the Reviewing and Editing. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data of this study are available upon request to the corresponding author.