
Abstract
Vulvar Leiomyoma is an extremely rare benign tumor of smooth muscle origin, accounting for a small fraction of Vulvar neoplasms. It often mimics Bartholin’s cyst or other soft tissue masses, posing diagnostic challenges. We present a case of a 19-year-old unmarried woman with a Vulvar mass. Histopathological examination confirmed the diagnosis of Vulvar Leiomyoma with no evidence of malignancy. Vulvar leiomyoma’s should be considered in the differential diagnosis of Vulvar masses. Accurate diagnosis requires histopathological analysis. Complete surgical excision is the treatment of choice. This case report is presented in accordance with the CARE guidelines.
Introduction
Leiomyomas are benign tumors arising from smooth muscle tissue, most commonly found in the uterus. However, when these tumors occur outside the uterus, they are referred to as extra uterine leiomyoma’s and are considered rare. Among these, vulvar leiomyomas are extremely uncommon, representing less than 0.03% of all gynecological neoplasms and approximately 0.07% of all benign soft tissue tumors in women.1,2 These tumors are thought to originate from smooth muscle cells in the walls of blood vessels, erectile tissue, the round ligament, or remnants of the dartos muscle in the labia majora. 3
Due to their rarity, vulvar leiomyomas often pose a diagnostic challenge. Clinically, they can be mistaken for Bartholin’s gland cysts, epidermoid cysts, or other benign mesenchymal tumors such as lipomas or fibromas.4,5 They typically present as slow-growing, firm, well-circumscribed masses, and while many are asymptomatic, some patients may report discomfort, dyspareunia, or local pressure effects depending on the size and location.5–8
Diagnostic imaging, such as ultrasound or MRI, may assist in characterizing the mass, but definitive diagnosis is only possible through histopathological examination, which identifies the classical features of bland, spindle-shaped smooth muscle cells arranged in intersecting fascicles without evidence of malignancy.9–11
Given the potential for recurrence and rare cases of malignant transformation into leiomyosarcoma, complete surgical excision with clear margins remains the mainstay of treatment.12,13
This case report highlights a rare presentation of vulvar leiomyoma in a 19-year-old woman and reinforces the importance of histological confirmation in the evaluation of vulvar masses.
Methodology
This is a single-patient clinical case report. The reporting of this study conforms to the CARE guidelines. 14 All patient details were fully de-identified to ensure confidentiality. The patient was selected consecutively after presentation to the gynecology outpatient department. Written informed consent for participation and publication was obtained. The study was conducted in accordance with the Declaration of Helsinki (1975), as revised in 2024.
Ethical approval
Ethical approval was obtained from the Quality Assurance and Ethical Review Committee of Woldia Comprehensive Specialized Hospital, Ethiopia (Approval No: ወሆ/WCSH/25154/2017; approved on 08/09/2017 E.C (15 May 2025).
Case presentation
A 19-year-old young woman in her late teens presented in 24/10/2014E.c. or (01 july 2022 G.c.) with a painless vulvar mass that had been progressively enlarging over approximately one year. She was unmarried and not sexually active. The mass had been progressively enlarging over a period of several months. She denied any associated symptoms such as pruritus, vaginal discharge, dyspareunia, or systemic signs like fever or weight loss. There was no history of trauma, infection, weight loss, or systemic symptoms. Menstrual cycles were regular. Based on clinical findings, a provisional diagnosis of Bartholin’s cyst or another benign soft tissue mass was considered. The decision was made to proceed with surgical excision for diagnostic and therapeutic purposes. The excised mass was sent for histopathological evaluation.
Clinical evaluation
On physical examination, a firm, mobile, non-tender, and well-defined mass was palpated on the right labia majora. The overlying skin appeared normal without signs of inflammation, ulceration, or discoloration. There was no regional lymphadenopathy. Per-speculum and per-vaginal examinations were not performed due to the patient’s virgin status. External genital examination showed a normal vaginal introitus and cervix was not examined. Rectovaginal examination was unremarkable (Figure 1). The mass was located on the right labia majora, approximately 0.5 cm from the clitoris and 4 cm from the anal verge. Preoperative Vulvar Leiomyoma. Preoperative clinical photograph showing a well-circumscribed and non-ulcerated mass arising from the right labia majors. The overlying skin appears normal, with no signs of inflammation or discoloration. The lesion is located several centimeters from the clitoris and anal verge.
Pre-operative workup
Preoperative evaluation included clinical examination and basic laboratory investigations. Due to the small size, superficial location, and benign clinical features, advanced imaging was not performed. Leiomyosarcoma was considered in the differential diagnosis; however, absence of rapid growth, ulceration, fixation, or lymphadenopathy reduced suspicion. Advanced imaging (MRI/PET) was not pursued due to limited resources and low clinical suspicion. Preoperative biopsy was not performed to avoid tumor seeding and because complete excision was feasible and diagnostic.
Surgical intervention
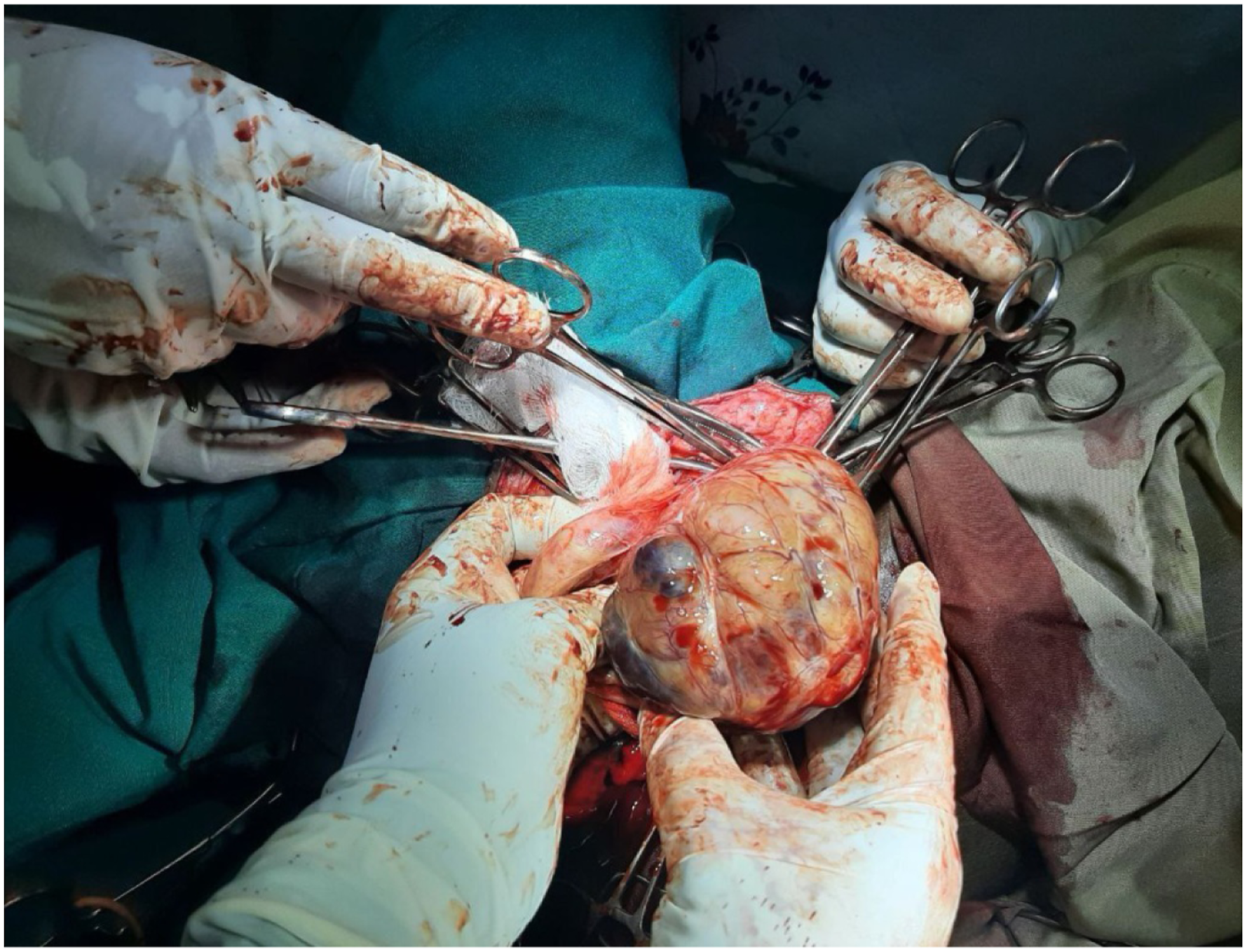
The mass was surgically excised under spinal anesthesia with clear margins (Figures 2 and 3). Intraoperative Leiomyoma. Intraoperative photograph demonstrating the vulvar mass following surgical exposure. The lesion appears well encapsulated and clearly demarcated from surrounding tissues, facilitating complete excision. Intraoperative Leiomyoma case report image in Woldia comprehensive specialized hospital, 2025. Intraoperative image showing mobilization of the vulvar mass during surgical excision at Woldia Comprehensive Specialized Hospital. The tumor demonstrates a smooth surface and firm consistency, suggestive of a benign soft-tissue lesion.
Pathology report summary
Microscopic examination
The gross specimen was sent for histopathological evaluation. Sections revealed interlacing bundles of bland smooth muscle cells arranged in fascicles. Areas of hyalinization and degeneration were noted. No features of atypia, mitotic figures, or necrosis were identified (Figure 4). Microscopic Leiomyoma. Histopathological section showing interlacing fascicles of bland spindle-shaped smooth muscle cells with eosinophilic cytoplasm and elongated nuclei. No cytologic atypia, mitotic figures, or tumor necrosis are identified (hematoxylin and eosin stain, ×200 magnification).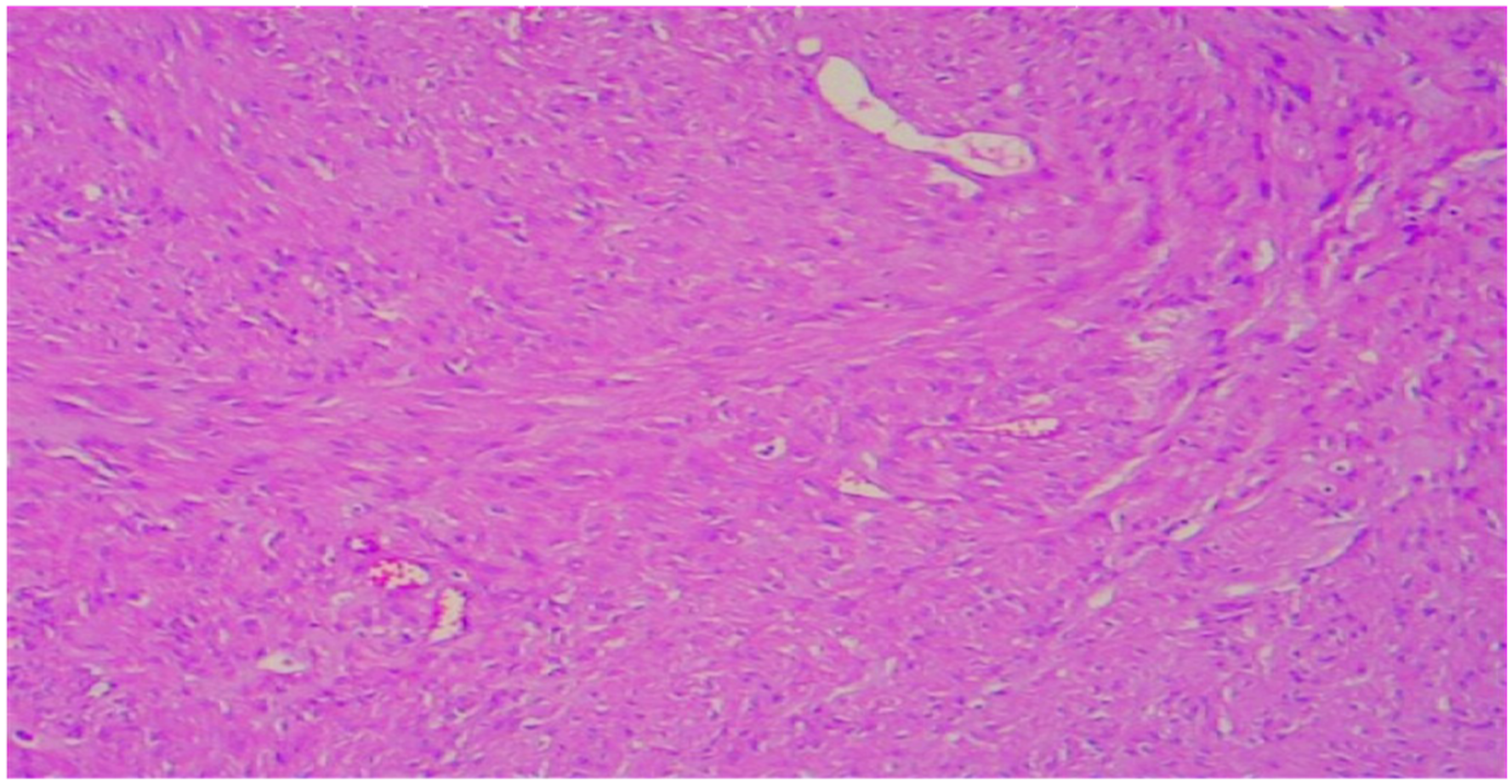
Pathology findings
The gross specimen was a well-circumscribed, firm mass with a homogenous cut surface. Histologic sections revealed interlacing bundles of bland smooth muscle cells arranged in fascicles, with areas of hyalinization and degeneration. No cellular atypical, mitotic activity or necrosis was observed. These findings were consistent with a diagnosis of Leiomyoma. Immunohistochemistry was not required as the morphology was characteristic (Figure 5). Gross Pathology Leiomyoma. Gross pathology specimen of the excised vulvar mass demonstrating a well-circumscribed, firm lesion with a homogeneous gray-white cut surface, consistent with leiomyoma.
Post-operative prognosis and follow up
The patient recovered well postoperatively and was discharged the same day. The urinary catheter was removed on postoperative day one. The patient passed stool on postoperative day two. No wound complications were observed. At six-month follow-up, there was no evidence of recurrence.
Differential diagnosis
Differential diagnoses included Bartholin’s cyst, lipoma, fibroma, aggressive angiomyxoma, and leiomyosarcoma.
Discussion
Leiomyomas are benign neoplasms arising from smooth muscle cells and are most commonly found in the uterus. Extra uterine leiomyomas, though histologically identical, are considerably rarer and can occur in unusual sites such as the gastrointestinal tract, skin, and genitourinary tract. Among these, Vulvar leiomyomas are exceptionally rare, accounting for less than 1% of all benign Vulvar tumors.1,2
Due to their rarity and nonspecific presentation, Vulvar leiomyomas are often misdiagnosed preoperatively. The most common clinical misdiagnosis is a Bartholin’s gland cyst, especially when the lesion is located in the posterolateral aspect of the vulva.15,16
In this case, the 19-year-old patient presented with a slow-growing, painless, firm Vulvar mass, which is typical for benign soft tissue tumors of this type. The absence of inflammatory signs or ulceration, and the mobility of the lesion, was suggestive of a benign process. However, given that clinical features alone cannot reliably distinguish between various Vulvar masses, surgical excision and histopathological evaluation were essential.
Histologically, Vulvar leiomyomas are characterized by spindle-shaped smooth muscle cells arranged in interlacing fascicles, often accompanied by areas of hyalinization, as seen in our case. The lack of cellular atypical, necrosis and a low mitotic index are key features distinguishing benign leiomyomas from leiomyosarcomas, which carry a poorer prognosis and require more aggressive treatment.3,17,18
Some authors propose diagnostic criteria for differentiating benign from malignant smooth muscle tumors in the vulva, based on mitotic activity, cytologic atypia, and tumor necrosis. According to Nielsen et al., a tumor may be diagnosed as a leiomyosarcomas if it shows ≥5 mitoses per 10 high-power fields, moderate-to-severe atypia, and coagulative tumor cell necrosis. If none of these features is present, the tumor is classified as a Leiomyoma.19,20
While imaging modalities such as ultrasound and MRI can help in preoperative assessment by delineating the size, depth, and consistency of the mass, they are not diagnostic. MRI, in particular, is useful in identifying the origin and composition of soft tissue masses and can be especially helpful in large or recurrent tumors to assess local infiltration. 9 However, these tools were not necessary in our case due to the small size and superficial location of the mass.
Surgical excision with clear margins remains the definitive and curative treatment for Vulvar leiomyomas. Incomplete excision may result in recurrence, though this is rare in benign cases. In our patient, the mass was completely excised, and no recurrence was noted at the six-month follow-up. Given the benign nature and complete excision, long-term surveillance may not be necessary, although some authors advocate for periodic clinical follow-up.3,16
The young age of our patient is notable, as Vulvar leiomyomas are more commonly diagnosed in women aged 30–60 years. The etiology remains unclear, but hormonal influence particularly estrogen is suspected to play a role in tumor development and growth, as seen in uterine leiomyomas. Some studies report tumor expression of estrogen and progesterone receptors, suggesting a potential hormonal dependency.21,22 However, receptor status was not assessed in this case, which may be a limitation in evaluating recurrence risk and potential hormonal management options.
Immunohistochemical staining, including smooth muscle actin (SMA), desmin, and h-caldesmon, is often used to confirm smooth muscle origin and differentiate leiomyoma from aggressive angiomyxoma or leiomyosarcoma. Although immunohistochemistry was not performed in this case due to classical morphology, its role is well established in diagnostically challenging cases.
This case underscores the importance of considering Vulvar Leiomyoma in the differential diagnosis of Vulvar masses, especially when clinical presentation is nonspecific. It also highlights the necessity of histopathological confirmation to ensure accurate diagnosis and guide appropriate.
Conclusion
Vulvar leiomyoma, although rare, should be considered in the differential diagnosis of vulvar masses in young women. Histopathological examination is essential for definitive diagnosis, and complete surgical excision offers excellent outcomes with minimal risk of recurrence.
Footnotes
Acknowledgments
We acknowledge the surgical team of Woldia Comprehensive specialized hospital involved in the management of the case.
Ethical considerations
Ethical approval was obtained from the Quality Assurance and Ethical Review Committee of Woldia Comprehensive Specialized Hospital, Ethiopia (Approval No: ወሆ/WCSH/25154/2017; approved on 08/09/2017 E.C (15 May 2025). All experimental protocols were conducted in accordance with the ethical standards and relevant guidelines and regulations set forth by the IRB.
Consent to participate
Informed consent for participation in the study was obtained from the patient’s after a full explanation of the purpose, procedures, risks, and benefits of the study. Written informed consent for treatment and publication was obtained from the patient.
Consent for publication
Written informed consent to publish identifying information and images was also obtained from the patient’s parent/legal guardian for publication in an online open-access journal. All patient identifiers have been removed, and no identifiable facial features were included in any images.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable request. No custom code or software was used in the preparation or analysis of this manuscript.
Use of Artificial Intelligence
No scientific content, data, or analysis was generated using AI.