
Abstract
Intervertebral disc degeneration (IVDD) is a multifactorial and clinically heterogeneous condition involving disturbances in oxidative balance, mitochondrial homeostasis, inflammatory signaling, susceptibility to regulated cell death, extracellular matrix integrity, and biomechanical function. Although biomaterial-based strategies have shown significant promise in preclinical studies, their clinical translation remains hindered by pathological heterogeneity, insufficient mechanistic validation, and frequent reliance on simplified experimental models. These models often fail to fully replicate the chronic, mechanically complex, and clinically diverse nature of human disc degeneration. In addition, current biomaterial strategies are commonly classified according to material composition or isolated molecular targets, potentially obscuring their functional objectives and limiting mechanistic comparisons across therapeutic platforms. This review presents a mechanism-guided framework for interpreting biomaterial interventions in IVDD. Biomaterial strategies are discussed based on their primary pathological targets and therapeutic intentions, including inflammatory regulation, restoration of redox homeostasis, mitochondrial protection, ferroptosis modulation, extracellular matrix preservation, and multifunctional microenvironment-responsive interventions. This framework acknowledges that these pathological processes are interconnected and vary in their relative dominance across clinical and pathological contexts and patient populations. We further analyze current biomaterial strategies according to mechanistic intervention layers, including upstream sensing and initiation-level control, restraint of intracellular amplification, organelle stabilization, regulation of execution checkpoints, and integration with higher-order structural organization. This layered perspective emphasizes that the efficacy of biomaterials depends not only on their composition but also on the pathological context, depth of regulatory influence, mechanistic specificity, and compatibility across intervention layers. Collectively, this review provides an integrated, mechanism-oriented framework for biomaterial design, preclinical evaluation, and translational development in IVDD therapy.
Keywords
1. Introduction
1.1. Clinical burden, asymptomatic degeneration, and painful disc disease
Low back pain (LBP) remains one of the leading causes of disability worldwide, imposing substantial socioeconomic and healthcare burdens in both developed and developing regions. 1 In 2020, LBP affected approximately 619 million people globally, and the number of prevalent cases is projected to reach 843 million by 2050. 1 Among its multifactorial etiologies, IVDD is widely recognized as an important pathological contributor.2,3 The intervertebral disc comprises the gelatinous nucleus pulposus (NP), fibrous annulus fibrosus (AF), and cartilaginous endplates, which collectively maintain spinal flexibility and distribute loads.4,5 Progressive deterioration of this complex tissue may contribute to chronic pain, functional limitations, and reduced quality of life. 6
Clinically, IVDD is typically assessed and graded using magnetic resonance imaging (MRI), which provides detailed evaluations of disc structure, signal intensity, and morphological alterations. 7 However, imaging-defined disc degeneration does not necessarily indicate symptomatic disease. Disc degeneration is a common age-related finding and frequently occurs in individuals without associated pain or functional impairment.8,9 A systematic review of imaging studies in asymptomatic populations found that disc degeneration prevalence increased from 37% at age 20 to 96% by age 80, suggesting that many degenerative imaging findings represent age-related structural changes rather than active pain generators. 8 This distinction is clinically relevant because imaging abnormalities are often incidental findings whose severity does not consistently correlate with the intensity of pain or level of disability.6,8 Consequently, the clinical challenge is not merely to identify morphological degeneration but to differentiate painful degenerative disc disease or discogenic LBP from asymptomatic, age-related structural alterations. 10 The clinical significance of IVDD thus depends not only on imaging abnormalities but also on symptom manifestation, local pathological activity, and structural or biomechanical deterioration.11,12 Degenerative disc changes become meaningful therapeutic targets when associated with persistent symptoms, evidence of local biological activity such as inflammation or Modic changes, structural deterioration, or biomechanical dysfunction, especially after ruling out other primary pain sources.2,13 To identify appropriate candidates for disease-modifying interventions, relevant clinical features include chronic discogenic LBP typically lasting more than 12 weeks (3 months),14,15 imaging findings suggestive of clinically relevant disc pathology or local biological activity, such as annular disruptions, high-intensity zones, endplate abnormalities, inflammatory endplate signals, or Modic changes,16–18 and insufficient response to appropriate conservative management.19,20 These features should be interpreted within a comprehensive clinical evaluation rather than used as rigid eligibility criteria, including exclusion of other major spinal or extraspinal pain sources such as facet joint pain, sacroiliac joint disorders, spinal stenosis, nerve root compression, or muscular dysfunction.21,22
Despite advances in imaging, molecular biology, and biomaterials engineering, IVDD remains difficult to reverse once structural collapse and matrix disorganization occur. 23 Although multiple clinical interventions exist, their ability to modify the degenerative microenvironment or address interconnected pathological mechanisms remains limited.24,25 Therefore, disease-modifying strategies, including potential intradiscal biomaterial interventions, should be considered within a well-defined clinical context. Such strategies may be appropriate for carefully selected symptomatic patients with biologically active or symptomatically relevant disc pathology but should not be applied to asymptomatic, imaging-defined degeneration alone.12,26,27 The increasing burden of LBP and clinically significant disc disorders among aging populations underscores the need for therapeutic approaches tailored to the pathological complexity of disc degeneration.28,29
1.2. Current clinical management and unresolved limitations
Current clinical management of symptomatic IVDD or discogenic LBP generally follows a stepwise approach rather than immediately resorting to invasive interventions. 12 Existing treatments are broadly classified as conservative and pharmacological management, interventional pain procedures, and surgical options. 30
Conservative and pharmacological management typically represents the first-line approach. This includes patient education, activity modification, exercise-based rehabilitation, physiotherapy, lifestyle changes, and pharmacological pain management, such as non-steroidal anti-inflammatory drugs or other analgesics as appropriate. 31 For patients with persistent symptoms or identified pain sources, interventional procedures, such as epidural steroid injections, intradiscal injections, nerve blocks, or radiofrequency-based therapies, may be considered. 32 Surgical interventions, including discectomy, decompression, spinal fusion, or total disc replacement, are generally reserved for patients with refractory symptoms, neurological compromise, segmental instability, or severe structural pathology.33,34 Although these treatments can alleviate symptoms, enhance function, relieve neural compression, or provide mechanical stabilization in carefully selected patients, their capacity to restore disc cellular homeostasis, rebuild extracellular matrix integrity, or reverse established degenerative changes remains limited.35,36 Specifically, conservative and pharmacological therapies primarily target pain relief and functional improvement rather than addressing the underlying degenerative environment. Interventional procedures may temporarily control inflammation and pain, but their long-term disease-modifying efficacy remains uncertain37. Surgical interventions may alter spinal biomechanics, accelerate adjacent-segment degeneration, and introduce procedure-related complications. 38
Given these therapeutic limitations, there is a clear need for disease-modifying strategies that target underlying pathological mechanisms of degeneration rather than simply managing symptoms. This review defines the primary clinical goal of biomaterial-based intradiscal interventions as reducing symptom-associated discogenic pain and functional impairment, rather than addressing asymptomatic, age-related imaging findings. Mechanistically, these interventions aim to modulate local degenerative processes associated with pain and tissue deterioration, including inflammation, oxidative stress, mitochondrial dysfunction, susceptibility to regulated cell death, and extracellular matrix disruption. Biomaterial-based interventions should thus be viewed as potential disease-modifying approaches for clinically significant disc pathology rather than treatments intended to fully reverse imaging-defined degeneration.
In this context, biomaterial-based approaches are being explored to overcome existing therapeutic limitations. Compared with systemic pharmacological therapies or purely mechanical surgical stabilizations, biomaterials offer advantages such as localized retention, sustained drug release, reduced systemic exposure, minimally invasive or injectable delivery, and combined biological and structural support within the disc space. Various biomaterial systems, including hydrogels, nanoparticles, exosome-inspired delivery platforms, gene-delivery constructs, and responsive scaffolds, have been developed to target inflammation, oxidative stress, mitochondrial dysfunction, regulated cell death pathways, and extracellular matrix remodeling.39–41 Notably, microenvironment-responsive biomaterials can be engineered to react specifically to pathological cues such as acidic pH, excessive reactive oxygen species, enzymatic activity, or inflammatory mediators, thus enabling more precise spatial and temporal therapeutic control. 42 Collectively, these properties position biomaterials not merely as structural fillers or drug-delivery vehicles but as platforms for sustained biological modulation within the degenerative disc environment.
Nevertheless, biomaterial-based IVDD therapies remain largely at the preclinical phase, and their clinical efficacy has not been widely validated. Although promising in preclinical models, many systems target isolated molecular pathways without adequately considering the broader pathological network.43–45 In addition, many studies rely on simplified inflammatory or oxidative stress models that fail to capture the chronic, mechanically complex, and heterogeneous nature of human IVDD.46–49 Consequently, biomaterials that appear effective under simplified experimental conditions may provide limited insight into their true therapeutic potential, clinical relevance across distinct pathological scenarios, or translational viability.
A critical limitation is the classification of biomaterials based solely on composition, which has led to repetitive ROS-scavenging or anti-inflammatory designs while obscuring meaningful mechanistic distinctions.50–52 Moreover, mechanistic attribution is often incomplete, as therapeutic effects are frequently not supported by rigorous causal validation such as rescue experiments, pathway-specific perturbations, or multi-level verification.53–55 These limitations suggest that future advances depend on improved material design, greater mechanistic precision, more pathologically relevant models, and evaluations better suited for translational contexts.
1.3. Rationale and scope of this review
Despite recent advances in biomaterial-based treatments for IVDD, therapeutic outcomes remain highly context-dependent. This variability reflects the marked pathological heterogeneity within degenerative disc tissues, where inflammatory signaling, oxidative stress, mitochondrial dysfunction, metabolic imbalance, susceptibility to regulated cell death, extracellular matrix remodeling, and biomechanical instability coexist in varying combinations and relative prominence.24,56,57 Consequently, biomaterials targeting a single mechanism may achieve different degrees of therapeutic success depending on the prevailing pathological context, experimental model, and degenerative state of the disc. Although several existing reviews have summarized biomaterial strategies for IVDD, but many adopt a primarily materials-centered perspective, potentially obscuring their functional therapeutic objectives.58,59 The inconsistent outcomes observed among similar biomaterial systems may therefore partly result from insufficient alignment between biomaterial functions, intended therapeutic goals, and targeted underlying pathological mechanisms.
In this review, therapeutic strategies for IVDD focus specifically on biomaterial-based interventions addressing clinically significant, symptom-associated, or biologically active degenerative disc pathology rather than asymptomatic, age-related imaging findings. Based on this clinical boundary, we propose a mechanism-guided framework to interpret biomaterial approaches for IVDD. Current strategies are organized according to their primary therapeutic aims and mechanistic targets: inflammatory regulation, restoration of redox homeostasis, mitochondrial protection, modulation of ferroptosis, preservation of extracellular matrix integrity, and multifunctional microenvironment-responsive interventions. This approach clarifies how biomaterial designs can better align with pathological heterogeneity, mechanistic complexity, and functional therapeutic requirements. Structural severity and local biological activity are discussed as contextual descriptors for interpreting pathological heterogeneity rather than as criteria for biomaterial classification, patient stratification, or treatment indication. Through this mechanism-oriented perspective, we aim to offer a more clinically cautious and translationally relevant interpretation of biomaterial-based IVDD therapies.
2. Clinical and pathological heterogeneity of IVDD
IVDD is a clinically and biologically heterogeneous condition characterized by diverse local cellular, biochemical, and biomechanical abnormalities.60,61 During degeneration, oxidative imbalance, inflammatory activation, mitochondrial dysfunction, matrix destabilization, and regulated cell death susceptibility do not occur in isolation. Instead, these processes coexist, interact, and vary in relative importance depending on the specific disease context.62–65 Recognizing these context-dependent pathological patterns is crucial for rational therapeutic design, as biomaterial-based interventions are unlikely to be equally effective across all degenerative conditions. Therefore, effective strategies must align with the dominant pathological features, therapeutic objectives, and biological constraints of the degenerative disc.
2.1. Pathological heterogeneity beyond imaging-defined degeneration
MRI plays a central role in IVDD assessment, and imaging-based grading systems, particularly the widely used Pfirrmann classification, provide practical references for describing structural and signal changes such as NP dehydration, disc height loss, annular disruption, and endplate alterations.66–68 These imaging features are valuable for characterizing morphological severity and providing a standardized basis for comparing experimental findings and therapeutic approaches.
However, structural degeneration represents only one aspect of the degenerative process. Discs with similar imaging characteristics may differ significantly in local biological activity, such as redox status, mitochondrial function, inflammation intensity, extracellular matrix remodeling, susceptibility to regulated cell death, and residual reparative potential.69–72 These biological differences are especially important for biomaterial-based therapies, as the effectiveness of a biomaterial depends not only on structural degeneration severity but also on the specific pathological processes active within the disc microenvironment.
Accordingly, IVDD should be viewed as a heterogeneous pathological continuum in which multiple biological processes coexist and interact with variable prominence.2,73 Oxidative stress, mitochondrial dysfunction, inflammatory activation, susceptibility to regulated cell death, extracellular matrix breakdown, and biomechanical instability may arise in distinct combinations across patients, anatomical regions, and experimental models. 74 This heterogeneity helps explain why biomaterials targeting similar mechanisms may yield different therapeutic outcomes in distinct degenerative scenarios.
Building upon this perspective, the following section summarizes the primary overlapping pathological axes in the degenerative disc environment: redox imbalance and oxidative stress, mitochondrial instability and susceptibility to regulated cell death, and inflammatory activation combined with catabolic remodeling. These axes establish a mechanistic foundation for the subsequent discussion of biomaterial strategies organized by therapeutic function. Importantly, greater structural severity alone does not necessarily indicate active pathological progression or the need for intervention, particularly if the degenerative segment is clinically stable or pain-free. Structural severity thus should be interpreted as a contextual descriptor rather than a direct indication for biomaterial treatment.
2.2. Overlapping pathological axes in the degenerative disc environment
IVDD involves substantial remodeling of the disc microenvironment beyond structural degeneration. Physiologically, the intervertebral disc environment is characterized by hypoxia, limited nutrient diffusion, high osmotic pressure, and minimal vascularity.75,76 During degeneration, these intrinsic limitations become exacerbated, destabilizing local disc homeostasis.55,77 (1) Redox imbalance and oxidative stress
Oxidative stress is a core pathological feature in IVDD, although its intensity and downstream effects vary by disease context.78,79 Mechanical stress, metabolic disturbances, and impaired mitochondrial function synergistically contribute to ROS overproduction, disrupting cellular redox equilibrium.65,80,81 Elevated ROS levels further promote mitochondrial membrane depolarization, impair electron transport chain activity, and initiate lipid peroxidation cascades, thereby linking oxidative imbalance directly to organelle dysfunction and subsequent cellular injury.82–84 (2) Mitochondrial instability and regulated cell death susceptibility
Mitochondrial dysfunction represents another significant degenerative axis in IVDD. As degenerative stress persists, mitochondrial quality control mechanisms, including mitophagy, mitochondrial fission–fusion dynamics, and biogenesis regulation, become increasingly dysregulated.85–87 This mitochondrial dysfunction not only intensifies ROS production but also enhances disc cell vulnerability to regulated cell death pathways, especially ferroptosis, characterized by iron-dependent lipid peroxidation.88–90 Intracellular iron accumulation (Fe2+), glutathione depletion, and suppressed GPX4 enzymatic activity further amplify susceptibility to ferroptotic injury,91,92 leading to progressive loss of viable NP cells. (3) Inflammatory activation and catabolic remodeling
Inflammatory and catabolic signaling constitutes another major pathological axis, particularly when tissue damage, extracellular matrix breakdown, and biomechanical instability become more pronounced. Key inflammatory pathways, including NF-κB and MAPK cascades, become activated by mechanical stress, oxidative injury, matrix degradation products, and cytokine stimulation.93,94 Pro-inflammatory cytokines, particularly IL-1β and TNF-α, stimulate the production of matrix-degrading enzymes, including matrix metalloproteinases and aggrecanases, accelerating extracellular matrix deterioration.95–97 The resulting degradation fragments can themselves act as damage-associated molecular patterns (DAMPs), reinforcing inflammatory signaling loops and perpetuating microenvironmental instability.98,99 Ultimately, this interaction creates a self-sustaining cycle involving oxidative stress, mitochondrial dysfunction, and inflammatory exacerbation.100–102
Mechanism-oriented pathological contexts and biomaterial design considerations in IVDD.
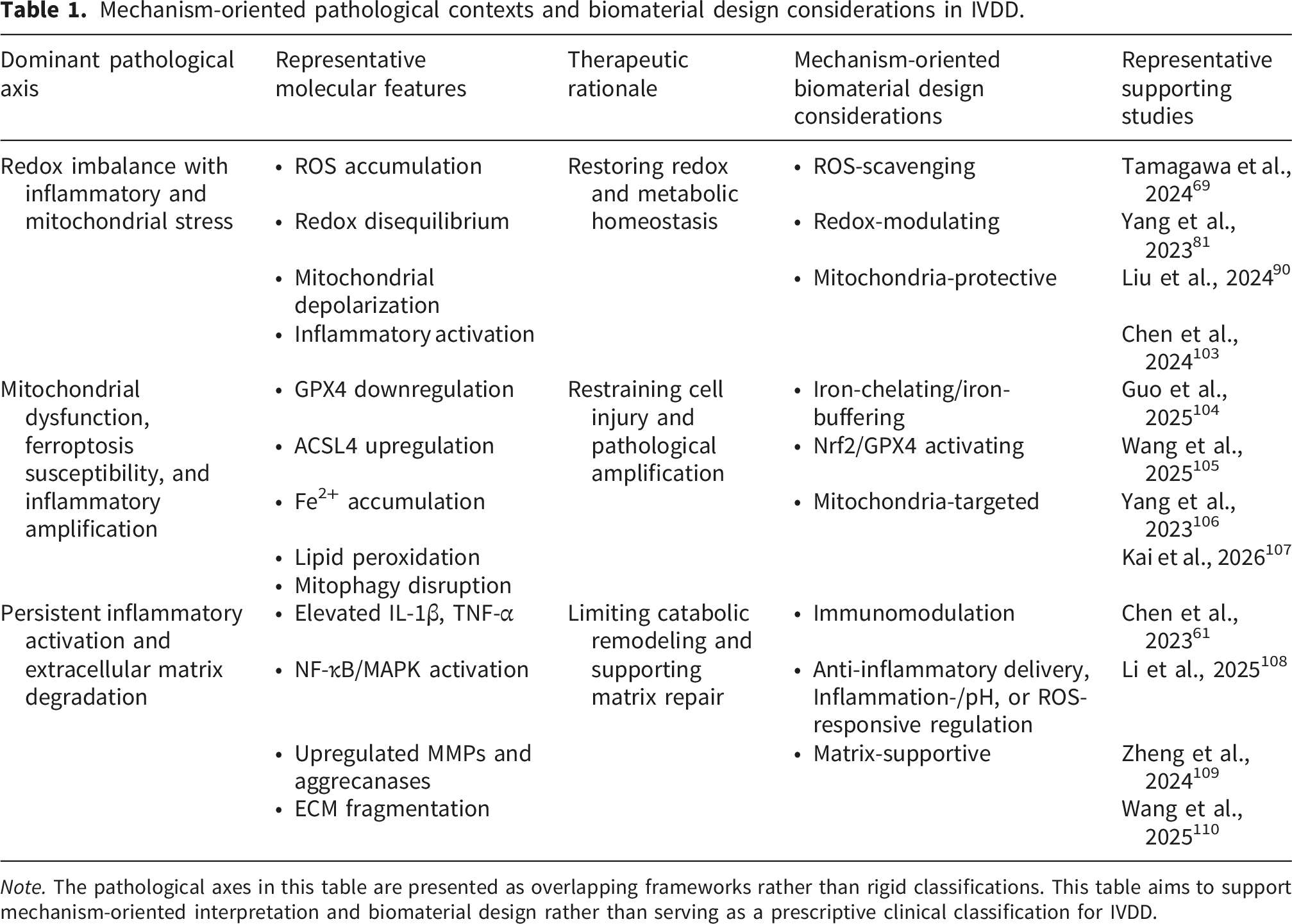
Note. The pathological axes in this table are presented as overlapping frameworks rather than rigid classifications. This table aims to support mechanism-oriented interpretation and biomaterial design rather than serving as a prescriptive clinical classification for IVDD.
Figure 1 summarizes the relationships among structural degeneration, overlapping pathological axes, and mechanism-oriented biomaterial strategies. Mechanism-oriented pathological contexts and biomaterial design considerations in IVDD.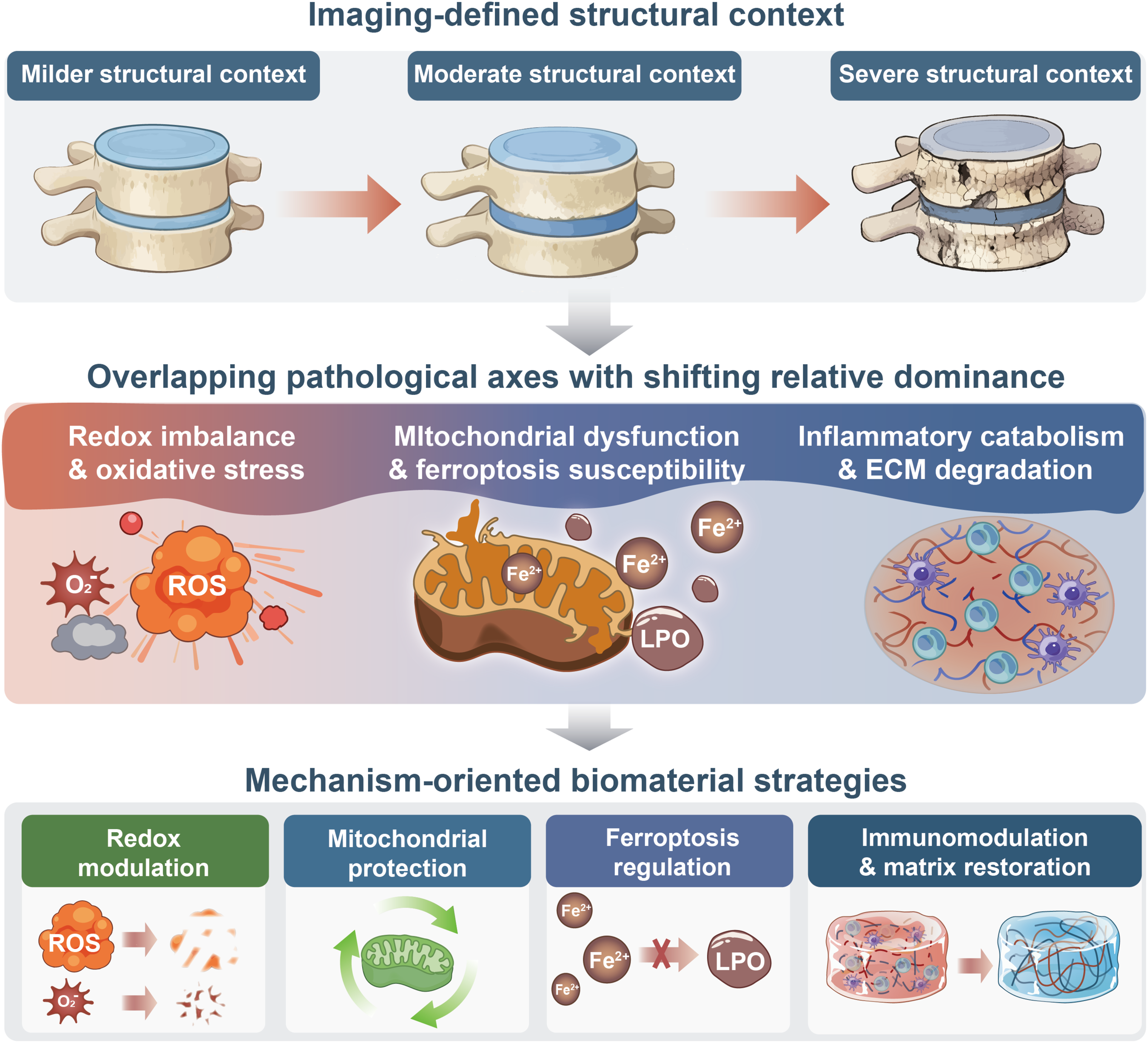
This schematic illustrates IVDD as a heterogeneous degenerative process, where structural degeneration serves primarily as an approximate context. Redox imbalance, mitochondrial dysfunction, ferroptosis susceptibility, inflammatory activation, and extracellular matrix disruption may coexist and interact, with varying degrees of prominence across degenerative contexts. Biomaterial strategies are aligned with these mechanisms, including redox modulation, mitochondrial protection, ferroptosis regulation, immunomodulation, and matrix-supportive designs. These associations guide interpretation and material design, not prescriptive clinical treatments.
3. Function-oriented classification of biomaterial strategies
In IVDD research, biomaterial strategies can be more meaningfully evaluated by the functional logic underlying their design rather than classifications based solely on chemical composition or structural features.111,112 Traditional, material-centered taxonomies can obscure the mechanistic rationale and complicate comparisons between systems designed with different formulations but aiming toward similar biological outcomes.113,114
In this review, functional intention refers to the primary biological process or pathological mechanism targeted by a given biomaterial system. Accordingly, subsequent sections are organized into major functional categories, including inflammatory signaling modulation, oxidative stress and mitochondrial dysfunction regulation, ferroptosis-related injury inhibition, and multifunctional strategies supporting extracellular matrix homeostasis. This framework clarifies biomaterial strategies according to their mechanistic roles in disc degeneration.
3.1. Inflammation-modulating biomaterials
Inflammation-modulating biomaterials attenuate excessive inflammatory signaling and the associated catabolic remodeling of disc tissues. In IVDD, inflammatory mediators such as IL-1β and TNF-α activate signaling cascades, including NF-κB and MAPK, promoting cytokine production, matrix-degrading enzyme expression, and extracellular matrix disruption.108,115–117 Given the close relationship between inflammatory activation and oxidative stress, mitochondrial dysfunction, and matrix catabolism, inflammation-modulating biomaterials should be evaluated according to their targeted signaling networks and downstream biological processes.118,119
3.1.1. Suppressing inflammatory amplification at initiation
Inflammatory signaling in IVDD frequently intertwines with oxidative stress, mitochondrial dysfunction, and matrix disturbances, creating an interconnected inflammatory–catabolic network rather than isolated pathological events.120,121Pro-inflammatory cytokines like IL-1β, TNF-α, and IL-6 act as key upstream mediators, triggering catabolic signaling cascades and disrupting matrix equilibrium.122,123 Biomaterials aimed at this functional intention primarily suppress inflammatory amplification, maintain extracellular matrix homeostasis, and disrupt self-reinforcing inflammatory-catabolic cycles.
A representative example of cytokine-targeted delivery was demonstrated by Loepfe et al., 124 who designed electrosprayed gelatin microparticles for local delivery of epigallocatechin-3-gallate (EGCG) into degenerated intervertebral discs. EGCG is known to inhibit IL-1β-induced inflammatory pathways through attenuation of IRAK1-NF-κB and MAPK signaling, thus reducing pro-inflammatory cytokine production and expression of matrix-degrading enzymes. Encapsulating EGCG within crosslinked gelatin microparticles maintained its biological activity and facilitated sustained local release. In inflammatory disc-cell culture models, EGCG-loaded microparticles significantly decreased IL-6, IL-8, and COX-2 expression, accompanied by pronounced suppression of matrix-degrading enzymes, including MMP-1, MMP-3, and MMP-13. Although the gelatin matrix itself was biologically inert regarding inflammatory modulation, its deliberate structural design ensured localized and sustained EGCG presentation. This demonstrates that even passive carrier platforms can effectively modulate cytokine-driven inflammation when guided by explicit functional objectives.
In addition to cytokine-targeted approaches, bioactive hydrogels containing anti-inflammatory agents have shown promise in IVDD models. Wu et al. 125 created an injectable composite hydrogel combining mesoporous bioactive glass nanoparticles and sodium alginate to enable sustained delivery of melatonin, an agent noted for its antioxidant and anti-inflammatory properties. The mesoporous bioactive glass facilitated effective drug loading and controlled release, while the alginate scaffold provided injectable properties compatible with the mechanical conditions of intervertebral discs. Melatonin released from this composite significantly inhibited inflammatory responses in NP cells by suppressing NF-κB signaling and reducing expression of inflammatory mediators. Moreover, melatonin receptor activation in NP cells improved extracellular matrix homeostasis by increasing anabolic factors and decreasing catabolic activity. These findings indicate that biomaterial-enabled prolonged release of anti-inflammatory molecules can effectively suppress these pathological responses and simultaneously support extracellular matrix integrity in the IVDD-associated disc microenvironment.
Beyond sustained anti-inflammatory agent delivery, certain biomaterial systems may also directly mitigate the upstream inflammatory response by reducing cellular responsiveness to inflammatory stimuli. Isa et al. 126 developed a cross-linked, high-molecular-weight hyaluronic acid (HA) hydrogel and examined its anti-inflammatory properties in an IL-1β-induced NP cell inflammation model. Instead of serving primarily as a passive drug carrier, the hydrogel itself suppressed expression of the inflammatory receptor IL-1R1 and its downstream adaptor MyD88, reducing NP cell responsiveness to inflammatory signals at receptor-adaptor initiation levels. This effect was accompanied by reduced expression of neurotrophins NGF and BDNF, which are associated with inflammation-mediated sensitization in degenerative disc tissues. The authors proposed that this protective mechanism might, at least partially, result from HA-CD44 interactions. Collectively, these findings expand the concept of inflammation-modulating biomaterials beyond passive cytokine sequestration or sustained anti-inflammatory molecule delivery, suggesting that early receptor-mediated signal initiation may be more effectively managed at the receptor-mediated signaling initiation level.
Overall, biomaterials targeting the initiation phase of inflammatory signaling primarily aim to restrain inflammatory amplification and maintain local tissue homeostasis.
3.1.2. Regulating immune cell behavior and inflammatory phenotypes
Immune cell recruitment, macrophage activation, and phenotypic polarization frequently accompany inflammatory responses within disc microenvironments.127,128 Therapeutic strategies regulating immune cell behavior offer additional functional pathways to control inflammatory amplification beyond direct cytokine suppression. Biomaterials may directly interact with immune cells, influencing their activation and phenotype, rather than simply acting as passive carriers for anti-inflammatory substances. 129 By carefully controlling material composition, surface chemistry, and physical characteristics, biomaterial systems can effectively modulate immune cell recruitment and polarization, reshaping inflammatory phenotypes within diseased tissues.130,131
A representative example of immune cell–targeted biomaterial design was reported by Jiang et al., 132 who developed an injectable hydrogel system capable of locally releasing Mg2+ ions. Sustained presentation of Mg2+ promoted macrophage polarization toward the anti-inflammatory M2 phenotype while concurrently inhibiting pro-inflammatory M1 activation, resulting in significant shifts in local inflammatory profiles. By establishing an immunoregulatory niche, this hydrogel actively modulated macrophage responses within the inflammatory microenvironment, extending beyond the typical role of passive drug carriers.
Furthermore, biomaterials may reshape inflammatory profiles by preserving immune-privileged niches and restricting inflammatory cell infiltration, in addition to modulating immune activation or macrophage polarization states. Wang et al. 133 developed a synthetic mucin-based hydrogel (Muc-gel) for post-discectomy applications. This hydrogel created an immune-suppressive environment at surgical sites, significantly reducing macrophage infiltration and M1 polarization. In subcutaneous implantation and rat tail degeneration models, Muc-gels effectively decreased pro-inflammatory gene expression and alleviated inflammatory damage, suggesting that biomaterials may control immune cell behavior through instructive cues while simultaneously remodeling the local immune microenvironment.
Collectively, these studies support a conceptual shift from direct suppression of inflammatory mediators toward proactive immune cell reprogramming through rational biomaterial design. These approaches underscore the potential of immunoregulatory biomaterials to control inflammation by modulating immune cell infiltration, macrophage polarization, and local immune phenotypes.
3.1.3. Microenvironment-responsive inflammatory regulation
Inflammatory abnormalities in IVDD frequently involve oxidative stress, local acidosis, enzymatic dysregulation, and extracellular matrix disruption.74,100 Microenvironment-responsive materials are designed to exploit endogenous cues, including acidic pH, oxidative stress, and enzymatic dysregulation, to achieve on-demand anti-inflammatory activity. This approach aims to enhance therapeutic precision while minimizing unnecessary disruption of residual physiological processes.134–136 By responding adaptively to pathological biochemical signals, biomaterials can synchronize anti-inflammatory effects with local redox, pH, and matrix homeostasis.
An illustrative example of microenvironment-responsive modulation was reported by Zheng et al., 109 who developed hydrogen ion–capturing hydrogel microspheres (GMNP, GelMA-based mineralization microspheres) to reverse chronic inflammaging in degenerated intervertebral discs. This system was designed to neutralize pathological acidosis through a CaCO3 mineralization layer, while concurrently reducing ROS levels and inhibiting the NLRP3/Caspase-1/IL-1β signaling axis. In vitro, GMNP reduced inflammatory activation and promoted extracellular matrix synthesis in NP cells. In vivo, it established a stable microenvironment that suppressed inflammaging and facilitated disc regeneration, highlighting the need for biomaterials that restore microenvironmental and matrix homeostasis in addition to exerting anti-inflammatory effects.
Another representative example was reported by Wang et al., 110 who developed a hydrogel-based drug delivery system (HPPC, Hydrogel–Polydopamine–pH/ROS-responsive Composite) for microenvironment-responsive anti-inflammatory intervention. This system incorporates celecoxib-loaded polydopamine nanoparticles within a dynamically crosslinked HA–based hydrogel network formed via Schiff-base and boronic ester linkages, enabling dual responsiveness to elevated ROS and acidic pH in degenerative disc tissues. Under pathological conditions, excessive ROS and acidosis destabilize the dynamic crosslinks, triggering controlled celecoxib release while providing intrinsic antioxidant activity through polydopamine. This coordinated response effectively suppresses inflammatory and oxidative stress signaling in NP cells, primarily via modulation of the COX2–PGE2–NF-κB and TNF-α–p38 MAPK pathways. In vivo studies further demonstrated that the responsive hydrogel reduced inflammatory mediator expression, restored extracellular matrix balance, and alleviated disc degeneration. Compared with conventional drug delivery systems, this approach emphasizes the advantage of coupling drug release to local biochemical signals such as ROS accumulation and acidosis.
Overall, these studies advocate shifting from continuous, nonspecific drug delivery toward adaptive strategies activated by endogenous pathological cues. By responding specifically to oxidative stress, acidic pH, and other inflammation-associated disturbances, such biomaterials enable precise and timely anti-inflammatory interventions while simultaneously supporting local redox, pH, and extracellular matrix homeostasis.
These approaches exemplify how microenvironment-responsive biomaterials integrate anti-inflammatory therapy with local biochemical modulation, effectively managing inflammatory–oxidative disturbances in IVDD.
3.2. Redox-modulating material strategies
Redox-modulating biomaterials aim to attenuate excessive ROS accumulation, restore redox equilibrium, and minimize oxidative damage to disc cells and extracellular matrix components.120,137 Excessive ROS in IVDD not only directly mediates oxidative injury but also amplifies inflammation and mitochondrial dysfunction.138,139 Elevated ROS production activates NF-κB/MAPK inflammatory pathways, destabilizes mitochondrial membranes, and impairs respiratory chain function, perpetuating oxidative–mitochondrial injury cycles.140–143 Current redox-modulating biomaterials thus integrate ROS scavenging, redox regulation, and interruption of ROS-driven inflammatory and mitochondrial amplification loops.
3.2.1. Direct ROS-neutralizing strategies
Initial biomaterial strategies addressing redox imbalance primarily aimed to directly scavenge ROS, with some systems additionally attenuating ROS-associated inflammatory and catabolic signaling.144–146 Direct ROS neutralization serves as an initial functional focus for redox-modulating biomaterials, although many systems also integrate signal regulation, responsive release, or immune modulation. For example, Wang et al. 147 developed a ROS-scavenging nanoplatform that reduced oxidative stress and suppressed NF-κB activation in degenerative disc cells. This antioxidant intervention decreased pro-inflammatory cytokine and matrix-degrading enzyme expression while restoring extracellular matrix homeostasis. In vivo, the treatment effectively maintained disc height and collagen II content, demonstrating that direct correction of oxidative imbalance can attenuate redox-driven degenerative signaling cascades.
Expanding on direct ROS-scavenging methods, Wang et al. 148 introduced a tannic acid nanoparticle (TA NP)-encapsulated hydrogel for gene delivery targeting degenerative NP tissue. In this system, tannic acid nanoparticles provided inherent ROS-scavenging capability and suppressed TNF-α/NF-κB signaling, whereas antagomir-21 contributed to restoring extracellular matrix metabolism via PTEN–MAPK/ERK pathway modulation. The hydrogel, responsive to pH and ROS, facilitated cue-triggered release and prolonged local retention in vivo, effectively integrating oxidative stress mitigation with signaling-level therapeutic correction.
In another advancement, Bai et al. 149 engineered a ROS-responsive hydrogel capable of locally scavenging H2O2 and simultaneously releasing rapamycin in response to ROS stimuli. By inhibiting mTORC1 signaling and promoting anti-inflammatory macrophage polarization, this hydrogel disrupted the ROS–NF-κB feedback loop and preserved disc structure in vivo. These studies collectively demonstrate that redox-modulating biomaterials extend beyond passive ROS elimination, effectively integrating direct oxidative stress mitigation with targeted suppression of inflammatory, immune, and catabolic signaling pathways associated with redox imbalance in IVDD.
3.2.2. ROS-responsive and mitochondria-targeted systems
Recent advancements in redox-modulating systems have increasingly emphasized targeted, organelle-specific, and stimulus-responsive designs, moving beyond generalized ROS scavenging. Chen et al. 103 developed a metal-phenolic nanoparticle (PGA-Mn-TP04) exhibiting mitochondrial targeting and catalytic ROS-scavenging activity. Through Mn2+/Mn3+ redox cycling, this nanoparticle demonstrated SOD- and catalase-mimetic activities, enabling efficient decomposition of ·O2- and H2O2 near their primary intracellular origins. In addition to reducing oxidative stress, this intervention restored mitochondrial membrane potential and ATP synthesis, and normalized mitochondrial dynamics by downregulating DRP1 and upregulating OPA1, MFN1, and MFN2 expression. This stabilization of mitochondria was associated with decreased oxidative stress–induced apoptosis, enhanced extracellular matrix integrity, and reduced disc degeneration in vivo.
Multifunctional redox-modulating platforms have also emerged, addressing oxidative microenvironments alongside inflammation, senescence, and tissue regeneration. Wang et al. 150 engineered a nucleus pulposus-mimetic hydrogel incorporating engineered microalgae, targeting oxidative stress and senescence-related disc cell dysfunction. Transcriptomic analysis indicated significant attenuation of oxidative stress-mediated inflammatory responses, including reduced TNF-α production and lower expression of senescence-associated secretory phenotype factors such as IL-6. In vivo, local injections of engineered microalgae delayed disc degeneration in rat models, while microalgae-hydrogel composites effectively repaired NP defects in goat models. These innovative systems thus move beyond basic antioxidant buffering, integrating oxidative stress control with inflammatory suppression, senescence modulation, and tissue reconstruction.
Overall, emerging redox-modulating strategies emphasize transitioning from generalized oxidative buffering toward targeted regulation of redox-sensitive inflammatory signaling, mitochondrial dysfunction, and stress-associated microenvironmental instability. Rather than merely acting as antioxidant reservoirs, these systems function as mechanism-oriented platforms that integrate redox control, organelle protection, catalytic ROS neutralization, and coordinated regulation of inflammation, senescence, and extracellular matrix remodeling responses.
3.3. Ferroptosis-related interventions
Ferroptosis-targeting interventions aim to limit iron-dependent lipid peroxidation, preserve mitochondrial integrity, and protect disc cells from ferroptosis-associated injury.151,152 Ferroptosis is an iron-dependent form of regulated cell death characterized by excessive phospholipid peroxidation and membrane damage.88,153,154 In degenerative disc cells, oxidative and inflammatory stress are associated with expansion of the labile iron pool, depletion of glutathione, impaired GPX4 activity, and accumulation of lipid ROS. 155 Accordingly, current biomaterial strategies can be broadly categorized into three functional interfaces: limiting lipid peroxide accumulation and propagation, modulating upstream ferroptosis-related signaling pathways, and restoring endogenous antioxidant defenses.
Recent studies have increasingly emphasized material systems that restore GPX4-dependent antioxidant capacity, reflecting the central role of lipid peroxidation in ferroptosis regulation. For instance, Yang et al. 106 developed a ferroptosis-targeted platform aimed at suppressing lipid ROS and maintaining membrane integrity in degenerative disc cells. This intervention significantly reduced malondialdehyde levels, restored GPX4 expression, and alleviated iron-induced oxidative damage. Mechanistic analyses further demonstrated that inhibition of lipid peroxide propagation improved mitochondrial morphology and restored extracellular matrix homeostasis both in vitro and in vivo. These findings indicate that targeting the GPX4–lipid peroxidation axis represents a potential strategy for interrupting ferroptotic cascades in IVDD.
Beyond direct inhibition of lipid peroxidation, subsequent studies have extended this regulatory logic to include upstream signaling regulation. Li et al. 156 identified osteopontin (OPN) as a ROS-responsive regulatory node linking oxidative stress to ferroptosis in degenerative discs. Mechanistically, ROS-induced OPN upregulation promoted ferroptotic responses in NP cells, as evidenced by reduced GPX4 and FTH1 expression, mitochondrial shrinkage, and increased intracellular iron levels. To disrupt this ROS–OPN–ferroptosis axis, quercetin, a small-molecule antioxidant, was employed due to its ability to directly bind OPN, as confirmed by molecular docking and surface plasmon resonance analyses. To enhance quercetin bioavailability and retention, a phenylboronic acid-modified dendrimer nanocarrier was incorporated into a ROS-responsive injectable hydrogel, enabling stimuli-responsive drug release under oxidative conditions. In vivo, this system effectively preserved disc height, extracellular matrix integrity, and ferroptosis-related protein expression compared with systemic administration. These results suggest that targeting upstream signaling nodes offers a complementary approach to mitigating ferroptotic amplification in IVDD.
In addition to suppressing lipid peroxidation and regulating upstream pathways, restoration of endogenous antioxidant systems represents another key strategy for ferroptosis modulation. Lin et al. 157 developed a dual-crosslinked ROS-responsive injectable hydrogel (HP@ICA) to improve the solubility and local retention of icariin, a natural activator of Nrf2 signaling. By integrating cyclodextrin-modified polyvinyl alcohol with phenylboronic acid-functionalized HA, the system enabled pH/ROS-responsive release of icariin within degenerative disc tissues. Mechanistically, released icariin activated the Nrf2–GPX4 axis, restored glutathione levels, increased GPX4 and xCT expression, and reduced intracellular Fe2+ accumulation, lipid peroxidation, and malondialdehyde production. In vivo, HP@ICA preserved disc height, enhanced type II collagen expression, and improved MRI signal intensity compared with non-drug-loaded controls. These findings highlight a biomaterial-based strategy in which ferroptosis inhibition is achieved through both exogenous antioxidant support and sustained activation of endogenous redox regulatory networks, thereby supporting extracellular matrix restoration.
Overall, ferroptosis-targeted strategies in IVDD cover multiple mechanistic aspects, including lipid peroxidation inhibition, upstream pathway modulation, and restoration of the Nrf2–GPX4 axis. These studies demonstrate that ferroptosis can be effectively regulated through biomaterials that integrate iron homeostasis control, lipid peroxide suppression, activation of endogenous antioxidants, and mitochondrial protection.
3.4. Multi-functional and responsive systems
Multifunctional and responsive biomaterials integrate multiple therapeutic functions within a single platform, addressing interconnected oxidative, inflammatory, ferroptotic, metabolic, and matrix-remodeling abnormalities in IVDD. These biomaterials do not treat extracellular matrix support as an isolated function but rather as an outcome of coordinated suppression of inflammation-driven catabolism, oxidative injury, ferroptotic cell loss, and biomechanical instability. Typically, these systems combine ROS scavenging, anti-inflammatory action, ferroptosis inhibition, hypoxia alleviation, drug delivery, matrix preservation, or structural reinforcement rather than targeting isolated molecular events.
Lu et al. 145 developed an injectable ROS-responsive hydrogel embedding dual-functional nanoparticles designed for synergistic modulation of oxidative stress and inflammation in IVDD. The hydrogel matrix included ROS-sensitive linkers allowing degradation and controlled drug release under elevated oxidative conditions, thus ensuring stimulus-triggered therapeutic activation. Mechanistically, the embedded nanoparticles demonstrated intrinsic ROS-scavenging activity while concurrently suppressing NF-κB-driven inflammatory signaling, resulting in reduced TNF-α and IL-6 expression. This dual regulatory function attenuated mitochondrial dysfunction, decreased lipid peroxidation, and restored extracellular matrix homeostasis in NP cells. In vivo, the responsive system significantly improved disc height index and collagen II expression compared to non-responsive controls, demonstrating the efficacy of combining oxidative stress neutralization and immunomodulation within a unified biomaterial platform.
Multifunctional ferroptosis-targeting platforms have expanded beyond single-mechanism inhibition toward integrated control of multiple pathological processes. Wang et al. 107 developed a self-stiffening polysaccharide-based hydrogel (CS/OHA@Cur-MNPs) simultaneously combining iron chelation, antioxidant pathway activation, and biomechanical reinforcement. In this system, macrophage membrane-coated ZIF-8 nanoparticles provided inflammatory cytokine scavenging and pH-responsive curcumin delivery under acidic pathological conditions. The released curcumin activated the Nrf2/HO-1/GPX4 axis, restored glutathione metabolism, and suppressed lipid peroxidation. Concurrently, dynamic Schiff-base linkages chelated excess Fe2+, reducing Fenton-driven ROS accumulation while converting iron overload into additional crosslinking points, thus increasing hydrogel stiffness. This iron-responsive mechanical reinforcement created a self-reinforcing protective loop in which ferroptosis suppression and mechanical stabilization synergistically promoted extracellular matrix integrity. Such designs exemplify biomaterial-based strategies that integrate redox regulation and structural adaptation for degenerative disc treatments.
Another representative multifunctional strategy integrates mitochondrial targeting, ROS scavenging, iron chelation, and ferroptosis regulation within a locally retained hydrogel. Guo et al. 104 designed an injectable nanocomposite hydrogel incorporating gallic acid-derived PGA-Cu nanoparticles modified with the mitochondrial-targeting peptide SS08. These PGA-Cu@SS08 nanoparticles were embedded in a BSA/gelatin hydrogel matrix, enabling sustained local release after intradiscal injection. PGA-Cu@SS08 localized to mitochondria, effectively scavenged various ROS species, and preserved mitochondrial function under oxidative stress. Furthermore, the abundant phenolic hydroxyl groups on PGA-Cu, along with histidine residues in SS08, endowed the nanoparticles with iron-chelating capabilities, reducing labile iron accumulation. Mechanistically, PGA-Cu@SS08 activated the NRF2–HO-1 pathway, increased GPX4 and FSP1 expression, inhibited ferritinophagy-associated iron release, and reduced mitochondrial lipid peroxidation. In vivo, this nanocomposite hydrogel restored disc height, maintained tissue hydration, and preserved extracellular matrix integrity, illustrating a multifunctional biomaterial that integrates redox modulation, mitochondrial protection, iron homeostasis, and ferroptosis inhibition.
Collectively, these studies demonstrate how multifunctional, responsive biomaterials can incorporate diverse regulatory mechanisms, including redox modulation, inflammatory control, ferroptosis inhibition, hypoxia correction, matrix preservation, and structural reinforcement. Importantly, matrix-supportive effects are achieved not only through direct environmental reinforcement but also by mitigating upstream inflammatory-catabolic and oxidative-ferroptotic injuries that drive matrix degradation. Such systems highlight the advantages of mechanism-oriented, integrated biomaterial designs for IVDD therapy.
4. Mechanistic intervention layers revealed by current biomaterial studies
Beyond functional classification, current biomaterial research has identified distinct mechanistic intervention levels within IVDD-related pathological processes. These include upstream sensing and initiation, intracellular amplification control and organelle stabilization, and execution checkpoints that limit terminal damage. This layered approach provides an analytical framework to understand biomaterial regulation at different nodes within inflammatory, oxidative, mitochondrial, ferroptotic, and matrix-disruptive signaling networks. Figure 2 summarizes representative biomaterial interventions across these regulatory layers. The subsequent sections detail biomaterial interventions at upstream danger-signal sensing, intracellular stress amplification, organelle dysfunction, and downstream injury execution interfaces. Representative biomaterial intervention layers targeting regulatory signaling, organelle dysfunction, and terminal injury responses in IVDD.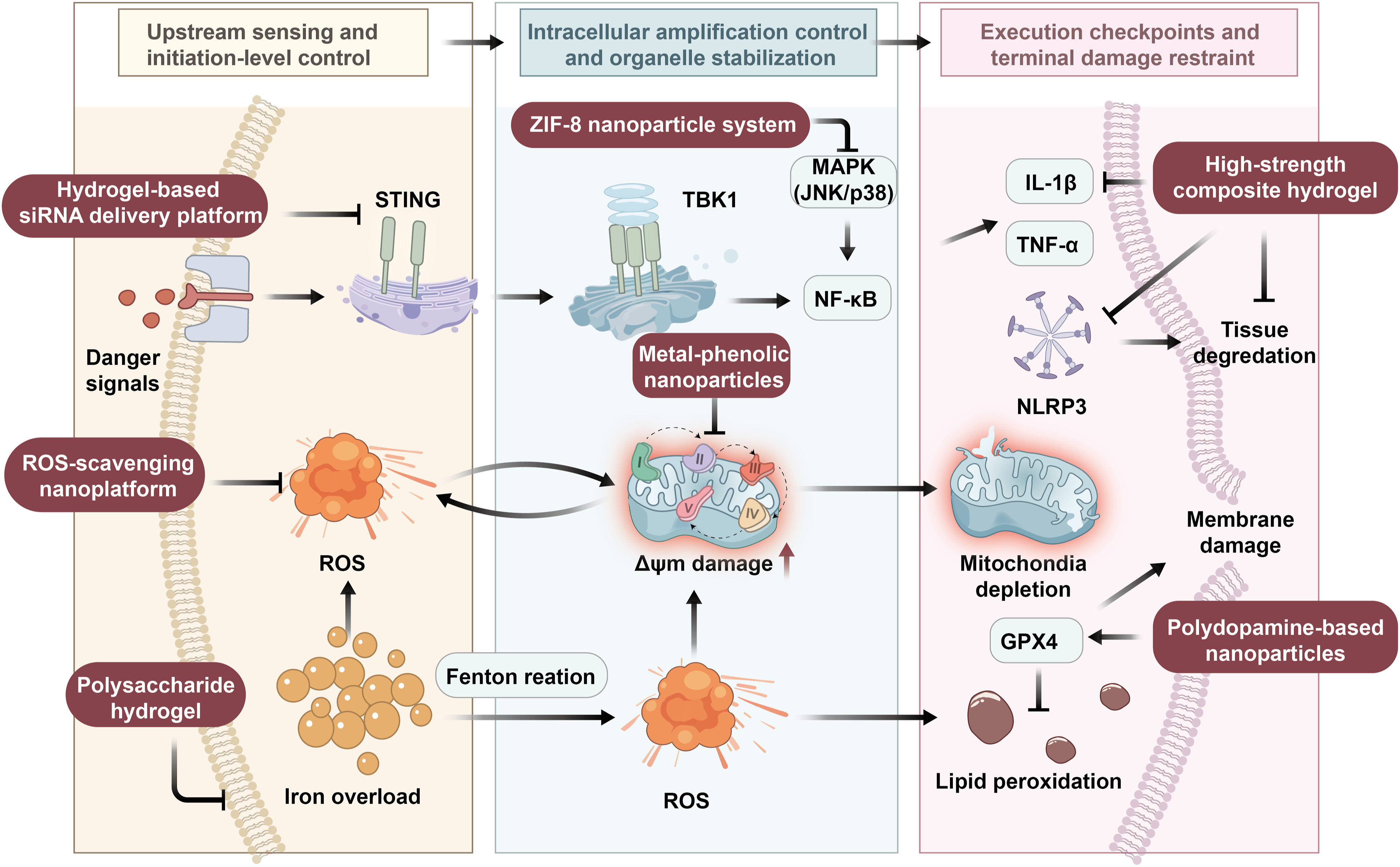
This schematic summarizes representative biomaterial interventions acting across major mechanistic layers in IVDD, including upstream sensing and initiation-level control, intracellular amplification control and organelle stabilization, and execution checkpoints with terminal damage restraint. Upstream regulation targets danger-signal sensing, STING-associated inflammatory initiation, ROS accumulation, and iron overload. Intracellular amplification control focuses on stress-propagation processes, including MAPK/NF-κB signaling, ROS-driven amplification, and mitochondrial membrane potential (Δψm) disruption. Execution-level regulation targets injury-associated interfaces, including NLRP3 activation, inflammatory cytokine release, GPX4-associated antioxidant failure, lipid peroxidation, membrane damage, and tissue degradation. Together, these layers provide a mechanistic lens for interpreting how biomaterial interventions engage distinct regulatory nodes within IVDD-associated pathological networks. Higher-order structural integration and network coupling are discussed separately in the subsequent section.
4.1. Upstream initiation and sensing-level control
Initiation-level regulation refers to interventions aimed at restraining upstream pathogenic signals before they propagate into broader inflammatory, oxidative, or ferroptotic pathways. Within this review, this regulatory level primarily encompasses material strategies that modulate initial inflammatory sensing or reduce ferroptotic susceptibility through iron availability regulation. Adaptor-associated signaling pathways, including those involving STING and MyD88, represent proximal regulatory nodes through which inflammation can be specifically attenuated at the signal initiation level.158,159 Supporting this concept, Chen et al. 160 demonstrated that sustained silencing of STING via an injectable hydrogel-based siRNA delivery system effectively attenuated STING–TBK1–NF-κB signaling, reduced pro-inflammatory cytokine expression, and preserved extracellular matrix integrity in vivo. These results indicate that targeting adaptor-level signaling upstream of cytokine production enables precise inflammatory modulation.
A parallel rationale applies to ferroptotic initiation. Dysregulated iron metabolism in degenerative disc tissues is a primary upstream event that lowers the threshold for ferroptosis induction.161–163 An expanded labile iron pool increases available redox-active Fe2+, promoting Fenton reactions, accelerating lipid radical generation, and priming cells for phospholipid peroxidation even before the complete impairment of GPX4-dependent antioxidant defenses.155,164 Thus, iron overload should be viewed as a critical initiation-level factor in ferroptotic susceptibility, not merely as a consequence of oxidative stress.165,166 Recent biomaterial systems have integrated iron-chelating or iron-buffering motifs to directly reduce labile Fe2+ concentrations within degenerative disc tissue. Besides direct iron regulation, upstream ROS accumulation also acts as a priming signal linking oxidative stress with ferroptosis and inflammation. For example, a ROS-responsive nanozyme-functionalized hydrogel effectively disrupted the ROS–ferroptosis–inflammation loop by scavenging excessive ROS and inhibiting IL-6/STAT3 signaling, thereby reducing ferroptotic susceptibility. 105 Similarly, a magnetically responsive hydrogel capable of adsorbing excess iron and modulating cellular iron metabolism successfully suppressed ferroptosis and promoted intervertebral disc regeneration. 167
Collectively, these studies illustrate that biomaterial strategies effectively intervene at initiation-level checkpoints by disrupting inflammatory signaling, iron-dependent ferroptotic priming, or ROS-driven pathological activation before these signals propagate downstream.
4.2. Intracellular amplification control and organelle stabilization
Intracellular amplification control and organelle stabilization strategies target processes responsible for converting upstream stress signals into sustained inflammatory, oxidative, and mitochondrial disturbances. This layer includes biomaterial systems designed to attenuate NF-κB/MAPK-associated signal propagation or to maintain mitochondrial functionality under oxidative stress.110,168
At the signaling-amplification level, inflammatory signals initiated upstream propagate through kinase cascades, notably MAPK and NF-κB pathways. 143 These phosphorylation cascades serve as intracellular amplification hubs, converting initial danger signals into prolonged transcriptional activation of inflammatory mediators.169,170 Materials capable of attenuating kinase phosphorylation consequently reduce inflammatory escalation without entirely blocking upstream sensing events. Supporting this mechanism, Yang et al. 171 reported that melatonin-loaded ZIF-8 nanoparticles inhibited p38 and JNK phosphorylation in LPS-stimulated NP cells, thereby reducing NF-κB activation and downstream TNF-α and IL-1β expression. This example highlights how biomaterial interventions selectively dampen intracellular inflammatory amplification by specifically targeting kinase-driven signaling rather than solely suppressing cytokine release.
A related amplification mechanism involves mitochondrial dysfunction. In degenerative disc tissues, excessive ROS production disrupts mitochondrial membrane potential, ATP synthesis, and respiratory chain activity, further intensifying mitochondrial ROS generation and exacerbating cellular injury.80,172,173 Biomaterials addressing this level stabilize mitochondrial bioenergetics and maintain organelle integrity under oxidative stress, complementing antioxidant interventions. 174 Consistent with this approach, mitochondria-targeted metal–phenolic nanoparticles restored mitochondrial membrane potential, normalized mitochondrial fission–fusion dynamics, and reduced oxidative stress-induced apoptosis in disc cells. 103 By mitigating ROS generation at its primary intracellular source and preserving mitochondrial integrity, these interventions interrupt the oxidative–mitochondrial injury cycle associated with disc degeneration and extracellular matrix breakdown.
These findings collectively suggest that biomaterial strategies may effectively reduce intracellular amplification by inhibiting kinase-dependent inflammatory propagation or by protecting mitochondrial function.
4.3. Execution checkpoints and terminal damage restraint
Execution checkpoints and terminal damage restraint approaches focus on downstream molecular interfaces where accumulated inflammatory, oxidative, or ferroptotic stresses convert into cellular injury and tissue disruption.175–177 This level includes biomaterial systems designed to inhibit inflammasome-mediated inflammatory execution or to stabilize the GPX4–lipid peroxide defense axis.178,179
One critical execution node is the inflammasome-dependent inflammatory machinery. At this downstream inflammatory interface, activation of the NLRP3 inflammasome leads to cytokine maturation and subsequent inflammatory tissue damage, transforming sustained signaling into destructive biological outcomes.180,181 Materials designed to suppress inflammasome assembly or activation therefore intervene at a terminal execution checkpoint within inflammatory cascades. Supporting this approach, Wei et al. 182 showed that a mechanically robust composite hydrogel reduced NF-κB/NLRP3 activation and inhibited IL-1β maturation in AF cells and a rat degeneration model. By specifically targeting inflammasome activation, this system effectively mitigated inflammatory execution and subsequent tissue degradation, emphasizing the therapeutic potential of interventions at these critical molecular interfaces.
A parallel execution checkpoint occurs during ferroptosis, wherein collapse of the GPX4–glutathione antioxidant system results in uncontrolled accumulation and propagation of membrane phospholipid peroxides.178,183,184 GPX4 acts as the key enzymatic safeguard, converting toxic phospholipid hydroperoxides into harmless lipid alcohols, and its destabilization signals a critical transition toward irreversible ferroptotic cell death.88,185 Biomaterials targeting this mechanistic checkpoint seek to preserve or restore endogenous defense pathways that protect against lipid peroxide-associated membrane damage, beyond mere oxidative buffering. Supporting this concept, polydopamine-based nanoparticles capable of inhibiting GPX4 ubiquitination preserved GPX4 protein expression while simultaneously reducing intracellular iron accumulation and lipid peroxidation in degenerative NP cells. 106 Similarly, ROS-responsive injectable hydrogels delivering Nrf2 activators promoted glutathione synthesis, enhanced cystine uptake, and increased GPX4 and xCT expression in degenerative disc cells. 157 These biomaterial systems reinforce intrinsic antioxidant defenses at critical lipid-peroxidation control points, surpassing the limited effects of external radical scavenging alone.
Collectively, emerging evidence indicates that current biomaterial approaches can effectively restrain downstream injury-execution processes by inhibiting inflammasome-mediated injury and strengthening endogenous ferroptosis-defense checkpoints.
4.4. Higher-order integration across intervention layers
The previous sections detailed specific intervention layers, including initiation-level control, amplification restraint, and execution checkpoint regulation. However, these layers are interconnected through higher-order regulatory interfaces that coordinate organelle homeostasis, adaptive stress responses, and cross-pathway signaling. This section addresses these integration points, bridging layer-specific biomaterial interventions and broader network coupling, discussed in subsequent sections.
At the integration level, representative regulatory nodes include ROS-responsive signaling hubs, mitochondrial quality-control systems, inter-organelle communication interfaces, and metal-ion homeostasis mechanisms.174,186,187 As previously discussed in Section 3.3, the OPN-targeted hydrogel represents an integration-level strategy because it modulates a ROS-responsive signaling node positioned at the intersection of oxidative stress, iron dysregulation, and ferroptosis progression. 156 By targeting such a hub, biomaterial intervention may influence not only a single downstream pathway, but also the coupling between redox imbalance and ferroptotic susceptibility.
Another critical integration level involves mitochondrial quality control and inter-organelle communication. Sustained oxidative stress in degenerative discs impairs mitophagy, disrupts mitochondrial fission–fusion dynamics, and alters organelle contact mechanisms, all essential for mitochondrial renewal, structural integrity, and long-term stress resilience.188,189 Emerging evidence particularly highlights mitochondria-associated endoplasmic reticulum membranes (MAMs) and mitochondrial metal-ion homeostasis as fundamental determinants of mitochondrial stability and adaptive capacity. 190
Supporting this perspective, Song et al. 190 demonstrated that degenerative NP cells exhibit diminished MAM formation accompanied by mitochondrial Zn2+ overload and accelerated cellular senescence. Mechanistically, the loss of the MAM-tethering protein SYNJ2BP impaired NLRX1–SLC39A7 interactions, thereby disrupting mitochondrial Zn2+ homeostasis and organelle functionality. Thus, mitochondrial regulation in IVDD may require strategies extending beyond simple antioxidant buffering to include stabilization of organelle interactions and upstream structural mediators involved in stress adaptation.
Emerging evidence indicates that biomaterial-based IVDD therapies increasingly target higher-order integration points, coordinating mitochondrial quality control, organelle communication, redox adaptation, and ferroptosis-related stress responses across multiple pathological pathways.
5. Crosstalk and convergence among intervention layers
Although the preceding section distinguished biomaterial interventions according to mechanistic regulatory levels, these mechanistic layers do not function independently within IVDD-associated pathological networks. IVDD is increasingly recognized as a complex, interconnected pathological system where oxidative stress, inflammation, mitochondrial dysfunction, and ferroptosis interact through reciprocal amplification loops.153,191 In the avascular and nutritionally constrained disc environment, these interactions are particularly significant, as limited metabolic support impairs the capacity of disc cells to withstand persistent stress.192,193 Consequently, interventions targeting a single pathological layer can be either reinforced or undermined by unresolved instability in interconnected layers. Understanding these inter-pathway interactions is crucial to explain why interventions targeting isolated mechanisms frequently yield incomplete therapeutic benefits, and why coordinated disruption of interacting amplification loops may provide more durable therapeutic effects. The major amplification loops and convergence relationships discussed in this section are illustrated in Figure 3. Crosstalk and convergence among major pathological loops and biomaterial intervention nodes in IVDD.
This schematic illustrates the major feedback interactions among oxidative stress, inflammation, mitochondrial dysfunction, and ferroptosis in IVDD. ROS and inflammatory signaling form a reciprocal amplification loop, while mitochondrial dysfunction promotes ferroptotic susceptibility through impaired bioenergetics, iron dysregulation, and lipid peroxidation. In turn, ferroptotic damage further enhances inflammatory propagation through oxidized lipids and danger-associated signals. These coupled processes indicate that IVDD should be understood as an interconnected pathological network rather than a set of isolated mechanisms, highlighting the need for biomaterial strategies capable of coordinated, multi-node intervention and loop interruption.
5.1. Redox–inflammation amplification loop
A primary example of pathological convergence involves reciprocal interactions between oxidative stress and inflammatory signaling. ROS serve as critical signaling mediators linking mitochondrial dysfunction and inflammatory activation.81,194 In degenerative disc cells, mitochondrial ROS production can activate NF-κB- and MAPK-dependent inflammatory cascades, thereby elevating pro-inflammatory mediator expression.195,196 Conversely, inflammatory cytokines may exacerbate mitochondrial dysfunction, including the loss of mitochondrial membrane potential, further intensifying oxidative imbalance and promoting additional intracellular ROS generation.197,198 This bidirectional interaction creates a self-sustaining feedback loop wherein oxidative stress and inflammatory signaling mutually reinforce each other.199,200 Such interconnected signaling explains why ROS scavenging alone may be insufficient for completely resolving degenerative pathology, as inflammatory activation can persist despite ROS.
5.2. Mitochondrial dysfunction–ferroptosis coupling
Mitochondria represent structural and metabolic convergence points within the pathological network of degenerative discs.187,201 Iron accumulation, impaired electron transport, defective mitophagy, and prolonged oxidative stress collectively promote lipid peroxide propagation and ferroptosis susceptibility.86,202,203 Conversely, ferroptotic lipid peroxidation and membrane damage can exacerbate mitochondrial structural injury, further amplify mitochondrial ROS production, and disrupt cellular bioenergetic homeostasis.204,205 Together, these mechanisms establish a self-perpetuating mitochondrial dysfunction–ferroptosis loop, wherein mitochondrial instability heightens ferroptotic susceptibility, and ferroptotic damage further intensifies mitochondrial impairment. This integrated network logic helps elucidate why mitochondrial-targeted interventions may concurrently influence oxidative stress, ferroptotic vulnerability, and broader cellular stress resilience.
5.3. Inflammation–ferroptosis interaction
Inflammatory signaling further modulates ferroptotic susceptibility by altering iron metabolism, glutathione homeostasis, and GPX4 expression.206,207 Conversely, ferroptotic cell death can release oxidized lipid fragments and DAMPs, thereby amplifying innate immune responses.208,209 This reciprocal interaction functions as a threshold-regulating loop: once inflammatory intensity surpasses a critical threshold, ferroptotic execution becomes increasingly probable, and initiated ferroptosis further enhances inflammatory propagation via secondary danger signaling. 210 Consequently, ferroptosis should be considered an integrated stress-responsive program embedded within broader inflammatory and oxidative networks, rather than as an isolated death mechanism. This interplay also suggests that anti-inflammatory approaches and ferroptosis-directed interventions may offer improved therapeutic efficacy when implemented together rather than separately.
5.4. Systems-level implications of pathological coupling
These interactions indicate that IVDD is best conceptualized not as multiple independent mechanisms, but as a regulatory network in which instability within one component can propagate across multiple pathological pathways.62,191,211Single-axis interventions may temporarily stabilize specific pathological nodes but fail to resolve other amplification loops, limiting long-term efficacy. This interconnected structure explains why therapeutic benefits from isolated interventions often remain partial, transient, and difficult to sustain. Biomaterial strategies that simultaneously target redox modulation, inflammation control, mitochondrial protection, ferroptosis inhibition, and matrix stabilization may offer more robust and durable network-level benefits than single-target approaches.
6. Design implications of mechanism-oriented biomaterial strategies
6.1. From mechanistic analysis to design principles
Based on the pathological features (Section 2) and mechanistic analyses (Sections 3-5) outlined previously, we propose evaluating biomaterial strategies for IVDD primarily by the pathological processes they address and the mechanistic depth of their therapeutic actions, rather than material composition alone. This shift emphasizes how specific biomaterial functions interact with pathological drivers, regulatory layers, and interconnected signaling networks.
6.2. Principles for mechanism-oriented material design
Based on this rationale, three principles can guide biomaterial selection and design:
First, biomaterial interventions should directly target the principal pathological drivers relevant to their intended therapeutic effect. Material selection should be informed by the dominant destabilized regulatory axis rather than solely by novelty or general targeting preferences. Intervention priorities may thus vary depending on the prevailing pathological conditions, encompassing oxidative imbalance, mitochondrial dysfunction, ferroptotic vulnerability, or chronic inflammatory–catabolic loops.212–214
Second, mechanistic specificity should be rigorously validated alongside phenotypic rescue. Assertions regarding pathway modulation must be supported by causal evidence rather than solely inferred from downstream biomarker changes or general histological improvements. Genetic knockdown studies, pharmacologic inhibition experiments, rescue assays, and multi-omic analyses should be employed whenever feasible to distinguish true mechanistic engagement from indirect compensatory responses.215,216
Third, biomaterial designs should be evaluated for their network-level compatibility across interacting pathological pathways. Strategies addressing a single pathological axis while neglecting related instabilities may provide only partial or temporary benefits.216,217 Therefore, material systems should be assessed based not only on primary effects but also on their broader influence on redox balance, inflammation, mitochondrial health, ferroptosis regulation, and extracellular matrix remodeling.
6.3. Implications for future material design
Given the multifactorial, clinically heterogeneous, and mechanistically interconnected nature of IVDD, future biomaterial design should move beyond isolated functional optimization to emphasize pathological context, mechanistic precision, and translational relevance.24,60 Although biomaterial-based strategies have demonstrated significant preclinical promise, their effective clinical translation remains constrained by pathological heterogeneity, incomplete mechanistic validation, and poorly representative experimental models.55,218
Future biomaterial designs should prioritize adaptive regulation of key pathological drivers, rigorous causal validation of therapeutic mechanisms, and the use of experimental models that more accurately replicate the biochemical, mechanical, and cellular complexity of degenerative discs. Progress in this field will additionally depend upon developing translationally meaningful outcome measures capable of connecting mechanistic efficacy with sustained structural and functional improvements.213,215,219
7. Challenges and future perspectives
7.1. Translational challenges
Despite significant advances in biomaterial-based strategies for IVDD, several translational barriers continue to limit clinical advancement.220,221
First, pathological heterogeneity in IVDD complicates the identification of a universally effective therapeutic target. Degenerative discs vary significantly in structural integrity, inflammatory profiles, metabolic vulnerabilities, biochemical imbalances, and biomechanical dysfunction; however, preclinical studies frequently assess biomaterials under simplified or uniform experimental conditions.222,223 This discrepancy restricts the ability to predict therapeutic efficacy across diverse clinical scenarios.
Second, mechanistic attribution remains insufficiently rigorous in many studies. Although biomaterials often claim modulation of pathways such as NF-κB, Nrf2, mitochondrial signaling, or ferroptosis, causal validation frequently remains incomplete.41,224,225 Without employing pathway-specific rescue experiments, genetic manipulations, or systems-level validation, it is challenging to differentiate direct target engagement from secondary compensatory responses.226,227
Third, current experimental models do not fully recapitulate the chronic, mechanically intricate, and biologically heterogeneous characteristics of human disc degeneration.228,229 Commonly employed in vitro inflammatory models and small-animal puncture models are useful for mechanistic evaluations; however, they inadequately represent long-term extracellular matrix remodeling, biomechanical dysfunction, and clinical heterogeneity.228,230,231 In addition, many studies rely predominantly on short-term molecular or histological endpoints, with insufficient assessment of biomechanical restoration, durability, or functional recovery.219,232
Future progress therefore requires enhanced biomaterial designs, improved experimental models relevant to human pathology, rigorous mechanistic validation, and the development of outcome measures with greater translational significance.
7.2. Emerging opportunities
(1) Development of responsive and adaptive biomaterials
Materials designed to respond to pathological signals such as oxidative stress, acidic pH, enzymatic activity, or inflammatory stimuli could enable more precise signal-triggered therapeutic effects. These responsive systems may minimize unnecessary interference with residual physiological processes while enhancing therapeutic specificity within the local pathological microenvironment. (2) Multifunctional and sequential intervention platforms
Given that IVDD involves interconnected disruptions in redox homeostasis, mitochondrial function, inflammation, ferroptosis susceptibility, and extracellular matrix integrity, future biomaterial systems could benefit from combining multiple therapeutic functions or enabling sequential intervention. Multi-cargo delivery strategies or temporally controlled release may be particularly beneficial for addressing interacting pathological processes through coordinated or stepwise regulation. (3) Integration with biologically active therapies
Combining biomaterials with biologically active components, such as cells, extracellular vesicles, nucleic acid therapeutics, or bioactive small molecules, may enhance therapeutic versatility and regenerative potential. Such integrative approaches could bridge the gap between local pathological control and structural regeneration. (4) Improvement of pathology-relevant and translationally informative models
A key opportunity lies in the development of experimental models that better represent disease heterogeneity, biomechanical loading conditions, nutritional limitations, inflammatory profiles, metabolic dysfunction, and extracellular matrix remodeling. More accurate in vitro and in vivo models are essential for determining whether promising biomaterials maintain efficacy under clinically relevant conditions.
7.3. Concluding remarks
IVDD is a clinically heterogeneous condition characterized by interconnected inflammatory, oxidative, mitochondrial, ferroptotic, and matrix-remodeling processes. Although biomaterial-based strategies have shown substantial promise in preclinical studies, effective clinical translation remains hindered by disease heterogeneity, incomplete mechanistic validation, and inherent limitations of current experimental models. Future progress will require closer alignment of biomaterial functions with specific pathological mechanisms, interconnected regulatory networks, and therapeutic goals, supported by rigorous causal validation and clinically meaningful assessment systems. Continued advances in adaptive biomaterial design, mechanistic precision, and translational modeling may bring biomaterial-based interventions closer to achieving durable, clinically relevant disc repair in IVDD.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Department of Orthopedics at the Affiliated Hai’an Hospital of Nantong University and the Department of Orthopedic Surgery at the Second Affiliated Hospital of Soochow University for providing a supportive academic environment and essential resources for this review work.
Author Contributions
Jianpeng Chen: Conceptualization, Investigation, Writing - original draft. Wenhao Deng: Investigation, Visualization, Formal analysis. Shiran Zhou: Visualization, Investigation. Jun Yan: Funding acquisition, Resources, Supervision. Kai Chen: Funding acquisition, Supervision, Writing - review & editing. Qianliang Wang: Conceptualization, Supervision, Writing - review & editing. Shujun Lv: Project administration, Supervision, Writing - review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant Nos. 81902239 and 81971036), the Medical Research Project of Jiangsu Provincial Health and Wellness Commission (No. MQ2024038 to Kai Chen), and the Horizontal Research Project of the Second Affiliated Hospital of Soochow University (Contract No. 04030929).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.