
Abstract
Background:
Congenital persistent hyperinsulinemic hypoglycemia (HH) is a rare disorder that can lead to severe and recurrent hypoglycemic episodes in neonates and infants. Management often requires intensive glucose infusion via central venous catheters (CVCs), which may increase the risk of thrombosis. While case reports suggest thrombosis can occur in HH, the incidence, risk factors, severity, and outcomes remain poorly understood.
Objectives:
This study aimed to determine the incidence of thrombosis in children with persistent HH and to evaluate potential risk factors associated with thrombotic complications.
Design:
A descriptive, retrospective cohort study of patients with persistent HH followed at a university pediatric endocrinology clinic between January 2000 and December 2025.
Methods:
Twenty patients with persistent HH were included. Data on demographics, clinical characteristics, laboratory results, treatment protocols, CVC use, timing and location of thrombosis were collected. Patients who developed thrombosis were compared with those who did not to identify risk factors.
Results:
Among 20 patients, 55% were male, with a median age at diagnosis of 1 day. A total of 23 CVCs were placed in 15 patients, with a median dwell time of 38 days. Thrombosis occurred in nine patients (45%), including six catheter-related and three catheter-independent intracranial thrombosis. Median age at thrombosis detection was 74 days. Patients who developed thrombosis experienced significantly more hypoglycemic episodes and more days with hypoglycemia (p < 0.05). No association was found between genetic mutations (ABCC8, KCNJ11, etc.) and thrombosis development. All four patients treated with enoxaparin achieved complete resolution without complications.
Conclusion:
Thrombosis is a frequent and clinically significant complication in persistent HH. Recurrent and severe hypoglycemic episodes are major risk factors. Routine thrombosis screening, particularly in patients with CVCs, may allow early detection and treatment even in asymptomatic cases.
Plain language summary
Persistent hyperinsulinemic hypoglycemia is a rare condition seen in newborns and infants in which the body produces too much insulin. This causes repeated episodes of low blood sugar, which can be dangerous for brain development if not treated quickly. Many of these children need high amounts of sugar given through a vein, often using a central venous catheter. Blood clots have been reported in some children with this condition, but how often they happen and what increases the risk has not been well studied. In this study, we reviewed the medical records of 20 children with persistent hyperinsulinemic hypoglycemia who were followed at our clinic over a 25-year period. We found that blood clots occurred in almost half of the patients. Some clots were related to the catheter, while others occurred in the brain without a direct link to the catheter. Children who developed blood clots had more frequent and longer-lasting episodes of low blood sugar compared with those who did not develop clots. Genetic differences did not appear to affect the risk of clot formation. All children who were treated with blood-thinning medication recovered fully, and no treatment-related problems were observed. Our findings show that blood clots are a more common complication of persistent hyperinsulinemic hypoglycemia than previously thought. Repeated low blood sugar episodes seem to play an important role in increasing this risk. Regular screening for blood clots, even when there are no clear symptoms, may help detect problems early and improve outcomes in these children.
Introduction
Hyperinsulinemic hypoglycemia (HH) is a heterogeneous group of disorders that constitute the most common cause of hypoglycemia in infants and neonates. It is characterized by dysregulated insulin secretion from pancreatic beta cells. 1 Because hypoglycemia can lead to severe, permanent brain damage, it is crucial to recognize and treat HH early and effectively. Clinically, the condition may be transient or persistent; persistent forms are typically congenital.
In the management of congenital HH, patients require central venous catheterization (CVC) due to the initial need for high-dose glucose infusion. Although CVC is an essential part of the treatment and care process of hyperinsulinism, it carries risks of complications such as thrombosis, phlebitis, catheter dislodgement or occlusion, and infection. 2 Thrombosis is one of the most frequent and serious complications. The incidence of thrombosis in childhood varies significantly according to age, underlying disease, and clinical setting.
There is currently no data regarding the development, frequency, and risk factors of thrombosis in patients with congenital persistent HH. It is hypothesized that the likelihood of thrombosis development is high in these cases due to the requirement for long-term intravenous therapy and frequent catheter interventions. The aim of our study is to emphasize the development of catheter-related thrombosis in persistent HH cases and to identify the predisposing factors that may lead to the development of thrombosis.
Method
This retrospective, cross-sectional, descriptive study included patients diagnosed with persistent HH and followed at our university’s Pediatric Endocrinology Clinic from January 2000 to December 2025. Inclusion criteria were defined as follows: diagnosis of persistent HH with negative blood ketones during hypoglycemia, fasting insulin > 2 mIU/mL, normal counter-regulatory hormone profiles (cortisol, growth hormone, ACTH), age < 18 years at diagnosis, and active follow-up at our institution. Patients diagnosed after age 18, those with other causes of hypoglycemia (fatty acid oxidation defects, gluconeogenesis disorders, glycogen storage diseases), or those with transient/secondary hyperinsulinism (IUGR, maternal diabetes, asphyxia, post-gastrointestinal surgery) were excluded.
Anthropometric measurements (weight, height, BMI, and respective SDS scores) and biochemical parameters at the time of hypoglycemia were recorded. Therapeutic interventions (octreotide, diazoxide, glucagon, calcium channel blockers), dosages, intravenous glucose infusion rates, and surgical history were documented. Catheter-related data, including type, duration of use, and the onset and management of thrombosis, were collected. Radiographic evaluations included abdominal ultrasonography (USG), echocardiography, and Doppler USG for catheter localization. Risk factors for thrombosis (catheter site, treatment duration, glucose infusion duration, and frequency of hypoglycemic episodes) and their association with specific mutations were analyzed.
Statistical analysis
Statistical Analysis Statistical analyses were performed using IBM SPSS Statistics software (version 22.0). Descriptive statistics for continuous variables are presented as mean ± standard deviation (SD), minimum, maximum, and median values. Categorical and ordinal variables are reported as frequencies and percentages. The normality of data distribution was assessed using the Shapiro–Wilk test.
For the comparison of two independent groups, the independent samples t-test was used for normally distributed data, while the Mann–Whitney U test was employed for nonnormally distributed data. The paired samples t-test was utilized for dependent group comparisons. Associations between categorical variables were analyzed using the Chi-square test. Multivariate regression analysis was performed to define the relationships between multiple variables and their impact on the dependent variable. For all statistical evaluations, a p-value of <0.05 was considered statistically significant.
Results
A total of 20 patients were included in the study, of whom 55% (n = 11) were male and 45% (n = 9) were female. The median age at diagnosis was 1 day (range: 1–195 days). Anthropometric characteristics at diagnosis are summarized in Table 1. Regarding birth weight categories, 50% (n = 10) of the cases were large for gestational age (LGA), while two cases were small for gestational age (SGA).
Anthropometric characteristics at diagnosis.
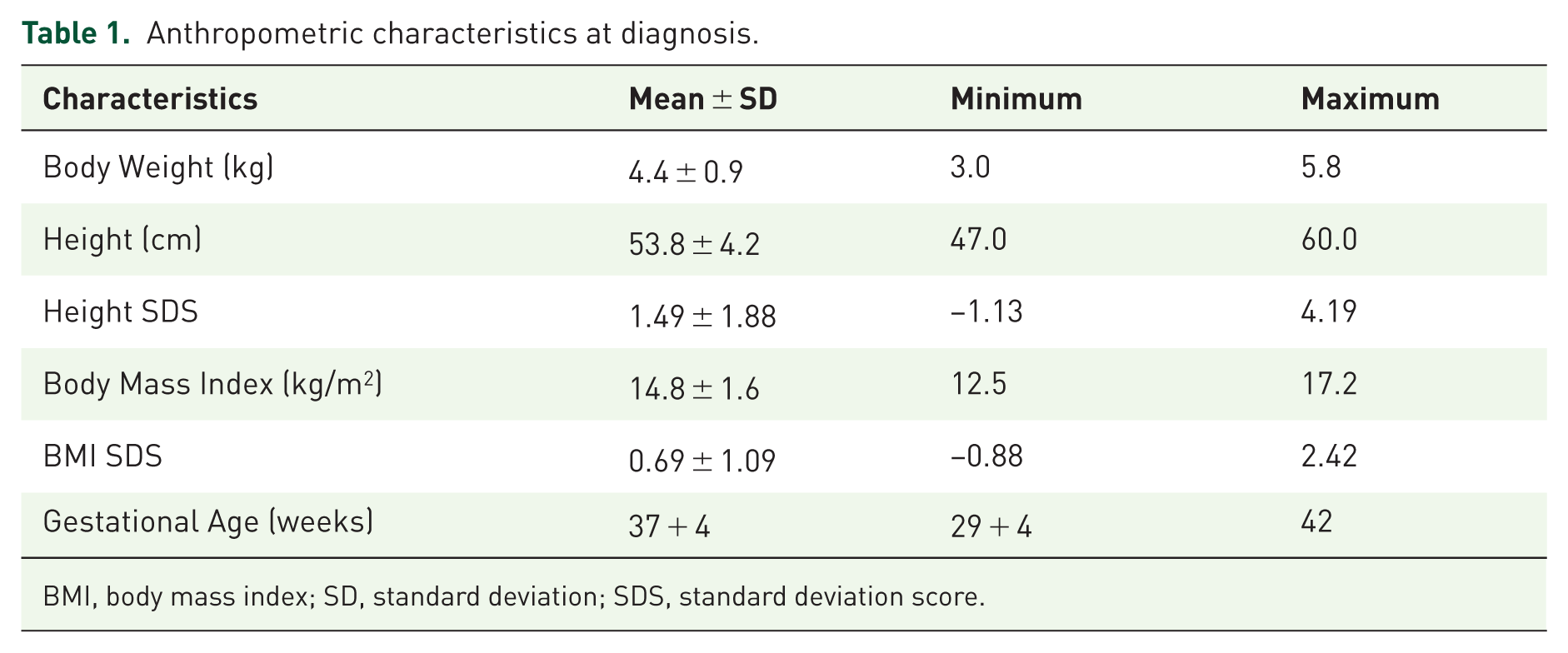
BMI, body mass index; SD, standard deviation; SDS, standard deviation score.
Laboratory evaluation during hypoglycemic episodes (blood glucose < 50 mg/dL) revealed negative blood β-hydroxybutyrate levels. Hyperinsulinism was confirmed by a mean fasting insulin levels of 16.6 mIU/mL (range: 2.6–62.7) and a mean C-peptide levels of 5.2 ng/mL (range: 0.6–8.6). Liver and kidney function tests, as well as counter-regulatory hormones (ACTH, cortisol, growth hormone), lactate, ammonia, organic acids, and acylcarnitine profiles, were within normal limits.
Genetic analysis identified ABCC8 mutations in eight cases, KCNJ11 mutations in five cases, and HADH mutations in one case. No mutations were detected in the remaining six cases. Focal involvement was present in one patient with a mutation, while diffuses involvement was observed in the others.
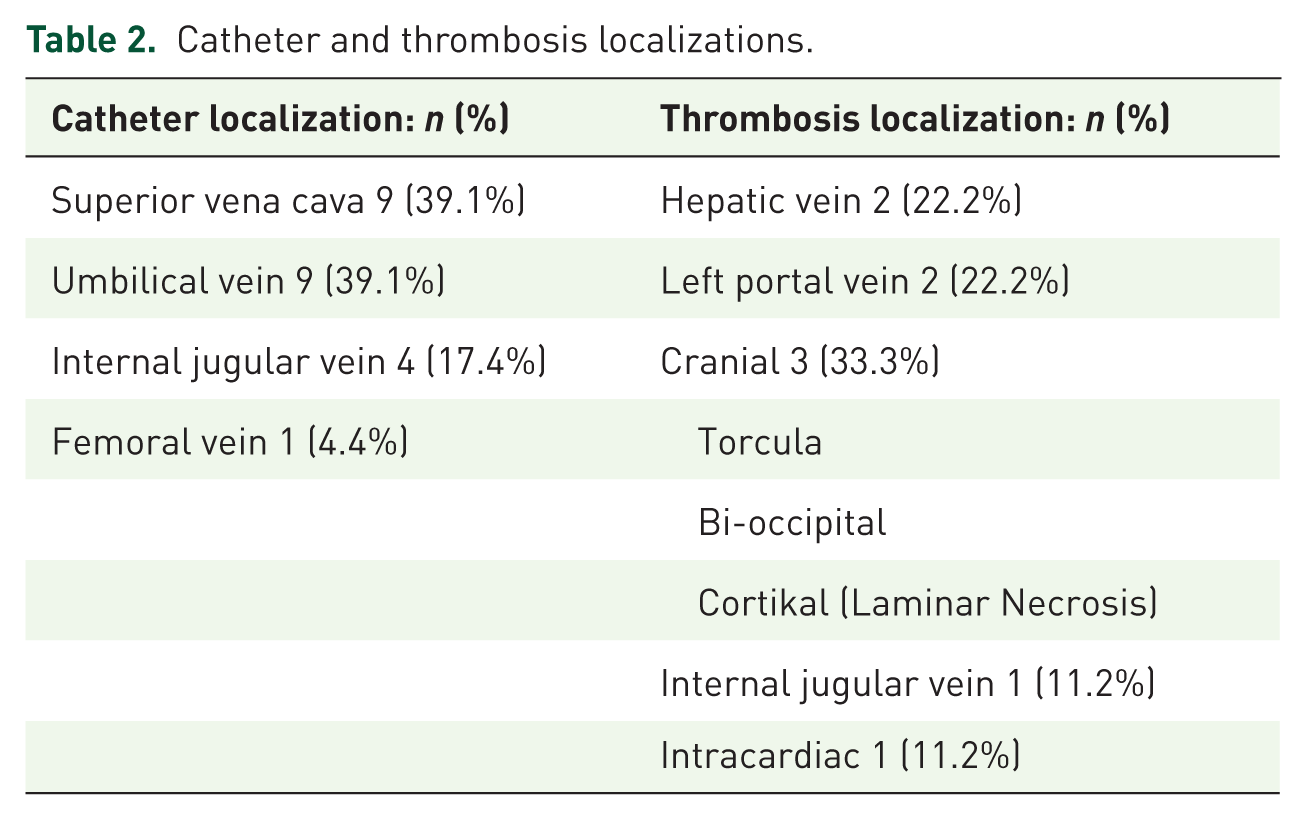
A total of 23 central venous catheterizations were performed in 15 cases, with a median catheter dwell time of 38 days. Thrombosis developed in nine cases, all of which were of venous origin. Catheter-related thrombosis was observed in six cases, while three cases presented with intracranial thrombosis independent of the catheter. The localization of the catheters and the origins of the thrombi are detailed in Table 2. The median age at the time of thrombosis detection was 74 days (range: 14 days–9 years); in two cases, thrombosis was identified during the chronic phase at an older age. Four cases (44.4%) received enoxaparin for thrombosis treatment, all of which achieved complete resolution. No complications were observed in any of the enoxaparin-treated cases. Among the cases that developed thrombosis, one was found to be heterozygous for Factor V Leiden and prothrombin mutations, indicating a predisposition to thrombophilia. Catheter-related infection occurred in five cases (33.3%), with cultures yielding Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Thrombosis was present in 80% of cases with catheter-related infections.
Catheter and thrombosis localizations.
No significant difference in mutation characteristics was observed when comparing cases with and without thrombosis (p > 0.05). The maximum glucose infusion rate, duration of glucose infusion, and maximum doses of diazoxide and octreotide did not differ significantly between the groups. However, the thrombosis group had a significantly higher number of days with hypoglycemia and total hypoglycemic attacks (p < 0.05). There was no statistically significant difference between patients who developed thrombosis and those who did not in terms of platelet counts and C-reactive protein levels measured within the first 24 h after a hypoglycemic episode (p = 0.139 and p = 0.681). Four cases of surgery were performed within the thrombosis group due to refractory hypoglycemia, and thrombosis was identified prior to the surgical intervention in three of these cases. The evaluation of potential risk factors for the development of thrombosis is presented in Figures 1–3.
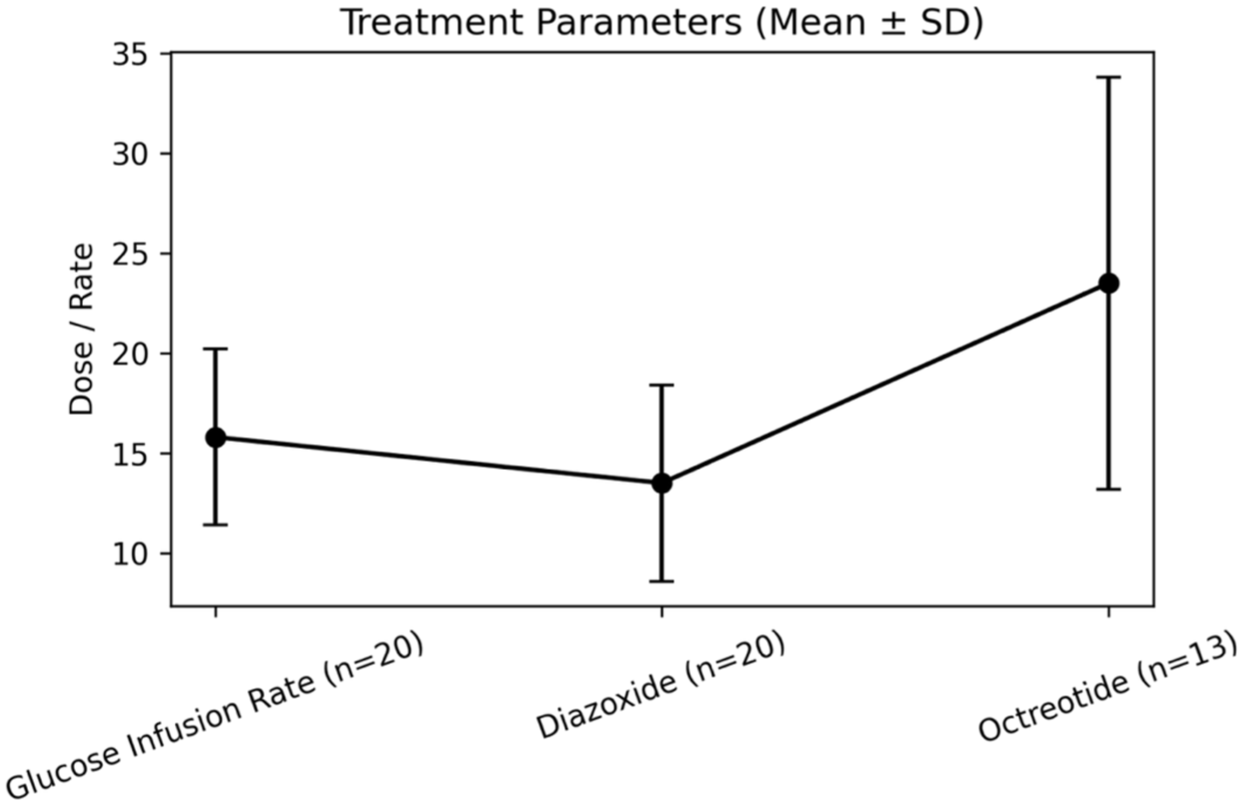
Maximum therapeutic doses.
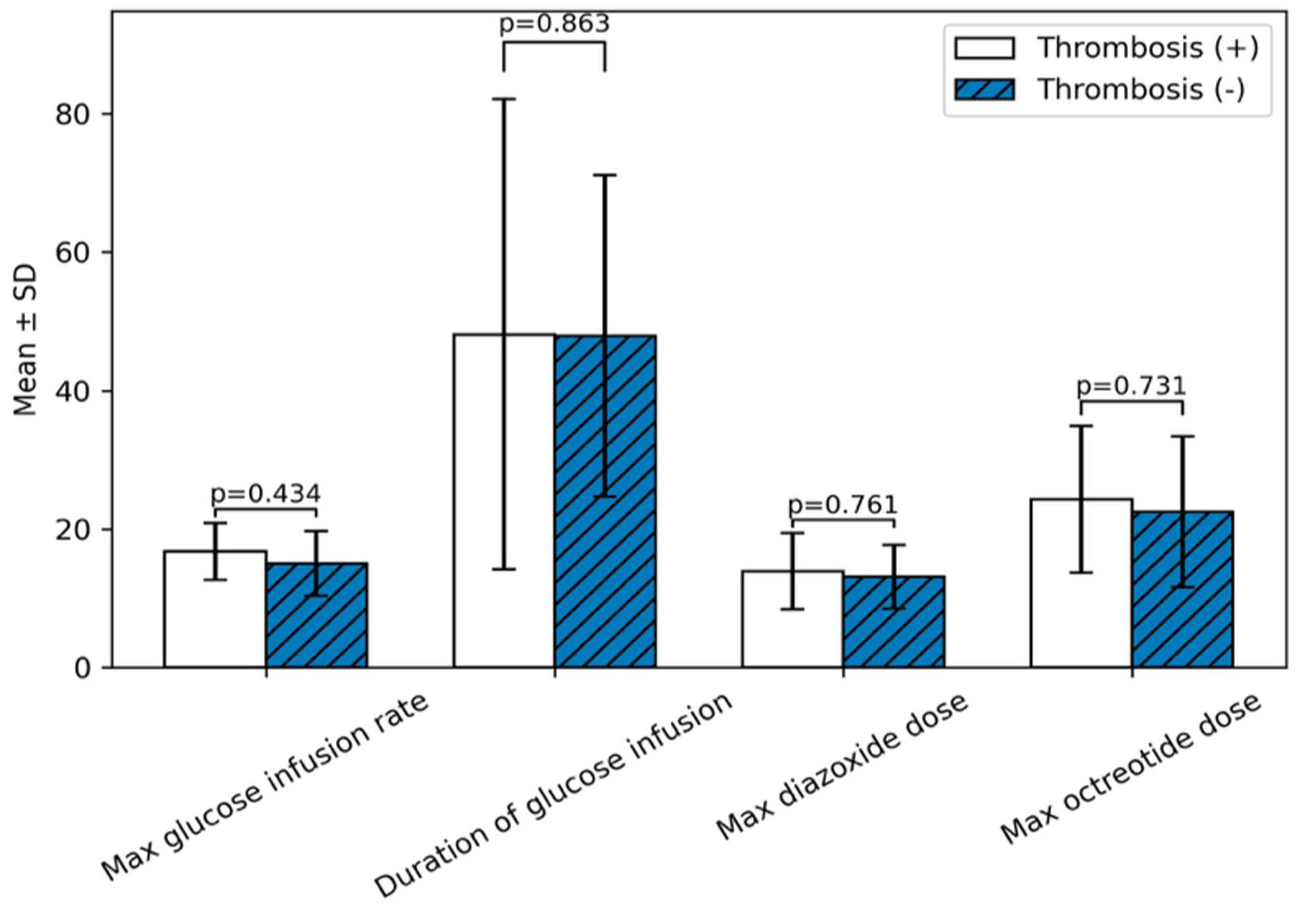
Comparison of treatment parameters between patients with and without thrombosis-1.
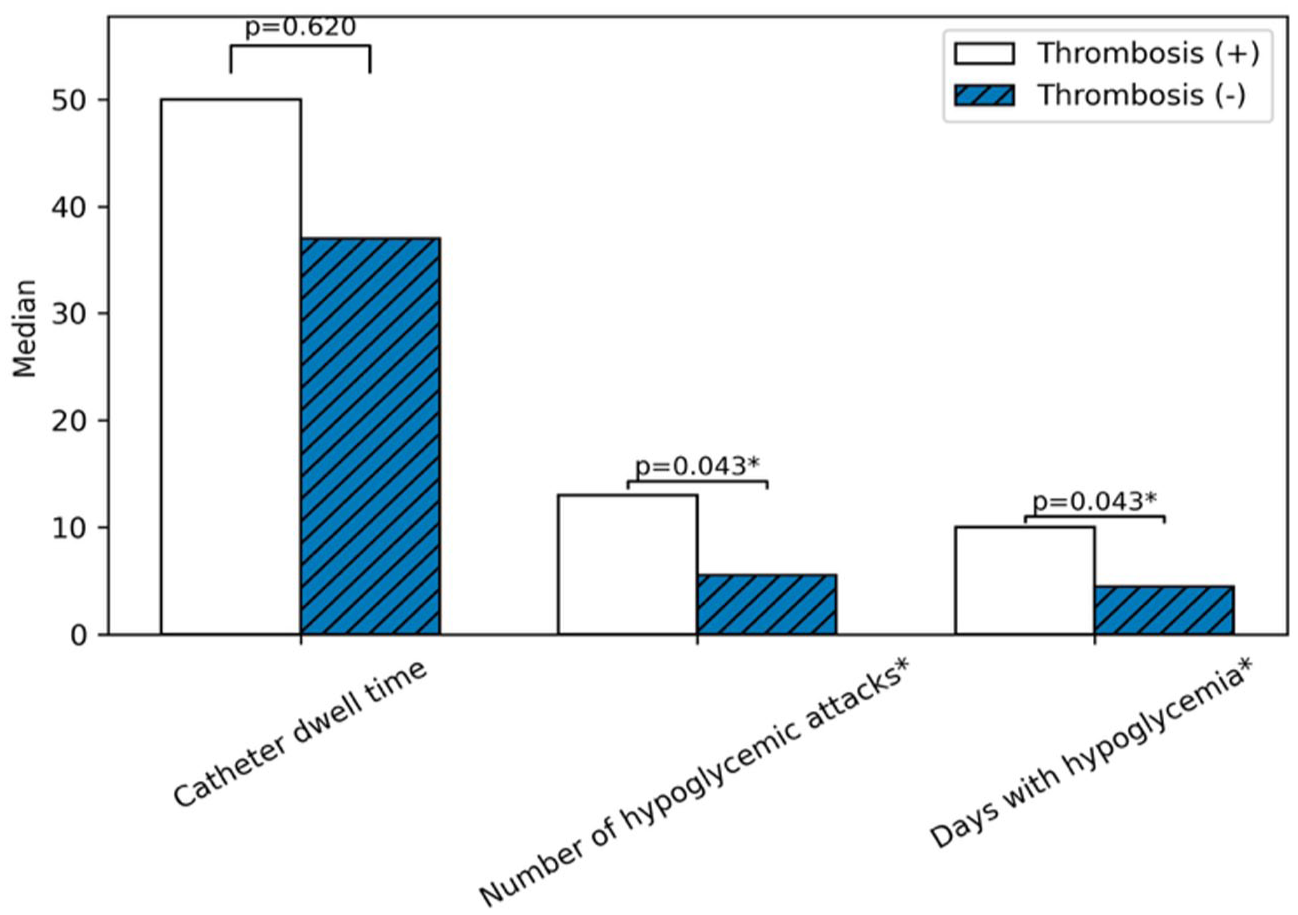
Comparison of treatment parameters between patients with and without thrombosis-2.
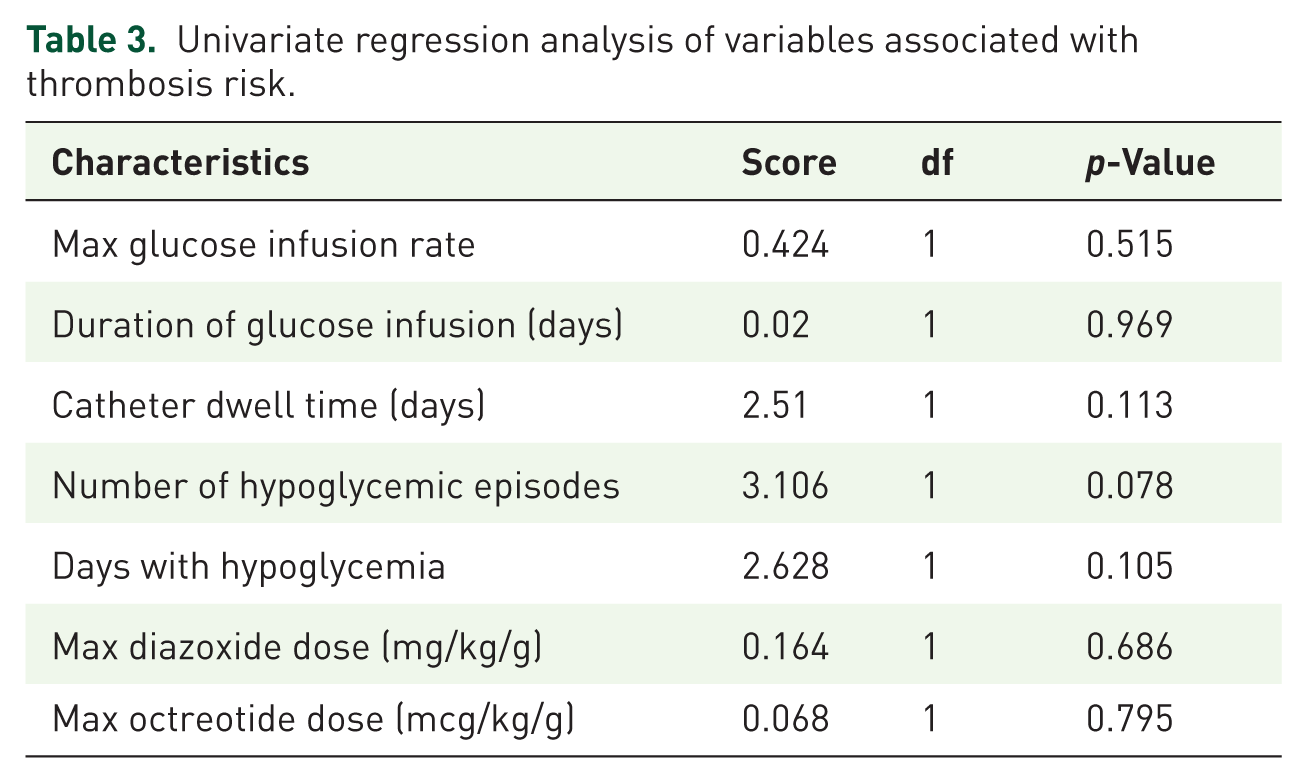
In the regression analysis conducted to evaluate risk factors contributing to the development of thrombosis, the number of hypoglycemic attacks was identified as the variable closest to the threshold of statistical significance (p = 0.078; Table 3).
Univariate regression analysis of variables associated with thrombosis risk.
During the follow-up period, one case was diagnosed with neuroblastoma, two cases developed diabetes mellitus following pancreatectomy, and one case underwent liver transplantation due to cholangitis and hepatic failure.
Discussion
The primary objective in the management of congenital persistent HH is to prevent recurrent and prolonged episodes of hypoglycemia, which can be clinically challenging. To prevent brain injury, serum blood glucose levels must be maintained above 70 mg/dL, 1 consequently, patients require high-rate intravenous glucose infusion at the onset of treatment, necessitating central venous catheterization. One of the most common and severe complications of central venous catheterization is thrombosis development. The aim of this study is to determine the risk of thrombosis and the predisposing factors associated with it in cases diagnosed with congenital HH.
In our study, catheter-related thrombosis was identified in six cases (26%), with an incidence rate of 9.2 per 1000 catheter days. In pediatric population studies, the frequency of catheter-related thrombosis ranges from 4% to 22%.3,4 This variation may be attributed to differences in clinical catheterization techniques, patient-specific risk factors, catheter types, and insertion sites. In a case series reporting on HH patients, the incidence of thrombosis was found to be 18%, or 4.2 per 1000 catheter days. 5 Compared to this initial report, the thrombosis rate in our study is slightly higher. Furthermore, three cases presented with intracranial thrombosis (bi-occipital, torcula, and laminar necrosis) independent of the catheter. This finding suggests the presence of predisposing factors that increase the risk of catheter-independent thrombosis in HH patients.
A study investigating the association between HH cases and thrombosis, homozygous or compound heterozygous ABCC8 and KCNJ11 mutations were found to correlate with thrombosis. 5 Although homozygous ABCC8 and KCNJ11 mutations were the most frequently detected genetic variants in our study, no significant association was observed between the type of mutation and the development of thrombosis. All cases of catheter-related thrombosis were asymptomatic; notably, two cases—one with portal vein thrombosis and the other with bi-occipital thrombosis—were diagnosed during the chronic phase. Regarding coagulation-related genes, Factor V Leiden and prothrombin heterozygosity were identified in only one case with thrombosis; however, these markers were not screened in cases without thrombosis. Levels of antithrombin III, protein-C, and protein-S were within normal limits. It has been demonstrated that homozygous mutations in Factor V Leiden or prothrombin increase the risk of catheter-related thrombosis fourfold. 6
Statistical analysis revealed no significant association between thrombosis risk and maximum glucose concentration, infusion duration, or peak doses of octreotide and diazoxide. While the mean duration of catheterization was higher in the thrombosis group compared to the nonthrombosis group, this difference did not reach statistical significance. However, the number of days with hypoglycemia and the frequency of hypoglycemic episodes were significantly higher in the group that developed thrombosis (p < 0.05). Studies indicate an association between severe, recurrent hypoglycemia and cardiovascular morbidity and mortality.7,8 Hypoglycemia has been shown to enhance atherothrombotic mechanisms, impair fibrinolytic balance, and lead to endothelial dysfunction.9,10 The higher frequency of hypoglycemic episodes in cases with thrombosis may be attributed to endothelial dysfunction and activation of the thrombotic cascade. Additionally, the administration of glucose boluses and continuous high-concentration glucose infusions to treat recurrent hypoglycemia may also contribute. High-concentration glucose infusions have been reported to increase the risk of catheter-related thrombosis. 11 In our study, the lack of difference in maximum glucose concentration and infusion duration between the groups suggests that thrombosis may be more closely related to recurrent hypoglycemic episodes and their acute correction with high-concentration fluids.
In addition, hematologic parameters measured within the first 24 h after the thrombotic event was reviewed. Platelet counts and C-reactive protein levels did not differ significantly between patients with and without thrombosis. However, it should be noted that hypoglycemia-related inflammatory and prothrombotic responses are typically transient and dynamic.12,13 Therefore, single measurements obtained after the thrombotic event may not adequately reflect the underlying pathophysiological processes. Prospective studies with serial measurements following hypoglycemic episodes would be more appropriate to clarify the relationship between hypoglycemia-related inflammatory activation and thrombosis risk.
Hyperinsulinemia is a condition that predisposes to thrombosis via coagulation and fibrinolytic systems, independent of other factors. It inhibits the fibrinolytic system by increasing PAI-1 levels, regardless of hyperglycemia. 14 Furthermore, a correlation has been established between insulin and various coagulation factors, including Factor VII and fibrinogen, which leads to clotting by activating the coagulation cascade.15,16 While this mechanism is well documented in patients with type 2 diabetes mellitus, a similar process may be present in patients with HH. This hyperinsulinemia-driven prothrombotic mechanism might be one of the predisposing factors for the three catheter-independent intracranial thrombosis observed in our study.
Although the catheter-related thrombosis in our cohort were asymptomatic, they were detected in the acute phase through ultrasonographic or echocardiographic imaging performed prior to catheter removal. Chronic thrombosis, however, were identified via Doppler ultrasonography or cranial magnetic resonance imaging during complication screening in long-term follow-up. While routine sonographic screening for catheter-related thrombosis is not recommended in neonatal and intensive care units, it is suggested for patients with a history of catheter-related infection or multiple catheterizations. 17
Conclusion
In this study, which highlights thrombosis as a prevalent comorbidity in HH, frequent hypoglycemic episodes were identified as a significant predisposing factor for thrombus development. It is anticipated that the inherent nature of the disease, along with prolonged and frequent central venous catheterization and high-dose glucose infusions, further elevates the risk of thrombosis. Therefore, performing routine sonographic screening in patients with HH—even in the absence of clinical symptoms—can facilitate early diagnosis and provide complication-free treatment options. In addition to the morbidity associated with hypoglycemia itself, the increased risk of thrombosis poses a further clinical burden in cases of congenital HH; consequently, patients with treatment-resistant hypoglycemia, in particular, should be closely monitored in this regard.
Supplemental Material
sj-docx-1-tae-10.1177_20420188261459825 – Supplemental material for Two threats in early life: congenital hyperinsulinemic hypoglycemia and thrombosis
Supplemental material, sj-docx-1-tae-10.1177_20420188261459825 for Two threats in early life: congenital hyperinsulinemic hypoglycemia and thrombosis by Ilkyaz Turktan, Sirmen Kızılcan Çetin, Gizem Senyazar, Seda Erisen Karaca, Sema Nilay Abseyi, Safak Demirtas, Elif Ozsu, Zehra Aycan, Merih Berberoglu and Zeynep Siklar in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.