
Abstract
Background:
The optimal extent of surgery for patients with unilateral multifocal papillary thyroid carcinoma (PTC; ⩽4 cm) and limited lymph node metastasis remains uncertain.
Objectives:
To compare recurrence risk between lobectomy and total thyroidectomy in this population.
Design:
Retrospective cohort study with inverse probability weighting regression adjustment (IPWRA) and non-inferiority analysis.
Methods:
This study included unilateral multifocal PTC (⩽4 cm) patients without bulky nodes (all metastatic <3 cm) treated from 2008 to 2024. IPWRA estimated the average treatment effect (ATE) of lobectomy versus total thyroidectomy on recurrence. A non-inferiority analysis with a prespecified margin of 3% was performed. Sensitivity analyses included traditional multivariable logistic regression, 1:1 propensity score matching, weighted logistic regression, and a 5-year landmark analysis. Recurrence-free survival was analyzed using Kaplan–Meier methods and multivariable Cox regression.
Results:
A total of 1373 patients were included (524 lobectomy, 849 total thyroidectomy). After IPWRA, all covariates achieved excellent balance. Over 52.4 months median follow-up, 36 recurrence events occurred (2.6%). The ATE of lobectomy versus total thyroidectomy was 1.19% (95% confidence interval (CI): −1.44% to 3.81%; p = 0.375), indicating no statistically significant difference in recurrence risk between the two procedures. The upper bound of the 90% CI (3.39%) marginally exceeded the prespecified non-inferiority margin of 3%. The 5-year landmark analysis showed a near-zero difference (ATE 0.01%, p = 0.994), and three of four sensitivity analyses yielded nonsignificant results. Subgroup analyses were directionally consistent but underpowered. The multivariable Cox regression was underpowered (minimum detectable hazard ratio (HR): 2.61) and yielded an inconclusive result (HR: 2.04, 95% CI: 0.91–4.62, p = 0.085).
Conclusion:
In patients with unilateral multifocal PTC (⩽4 cm) without bulky nodal metastases, lobectomy showed no significant difference in recurrence risk compared with total thyroidectomy, supporting that lobectomy may be a safe alternative in this intermediate-risk population.
Plain language summary
Papillary thyroid cancer is the most common type of thyroid cancer. For patients with multiple cancer spots (all ⩽4 cm) on one side of the thyroid and without bulky lymph node metastases (all involved nodes <3 cm), doctors disagree on whether to remove only the affected side (lobectomy) or the whole thyroid (total thyroidectomy). This study compared cancer recurrence between these two operations.
We reviewed records of 1,373 patients treated at Xijing Hospital in China between 2008 and 2024. All had papillary thyroid cancer, multiple tumors on one side (largest ⩽4 cm), and no bulky lymph node metastases (all involved nodes <3 cm). Of these, 524 had lobectomy and 849 had total thyroidectomy. Because the two groups differed in many ways – including treatment period, tumor size, microscopic spread, number of metastatic nodes, and BRAF mutation – we used inverse probability weighting to create balanced groups for a fair comparison.
After more than 4 years of follow-up, only 36 patients (2.6%) had recurrence – 10 in the lobectomy group (1.9%) and 26 in the total thyroidectomy group (3.1%). After adjusting for differences, the absolute risk difference was 1.19% (95% CI: –1.44% to 3.81%; P = 0.375), meaning no statistically significant difference in recurrence between the two operations. We also tested whether lobectomy was “not worse than” total thyroidectomy by a 3% margin. The result fell just short of proving this (upper bound 3.39% vs. 3%). However, most additional sensitivity analyses – including a 5-year landmark analysis that equalised follow-up time – consistently showed no meaningful difference in recurrence.
For patients with multiple thyroid cancer spots up to 4 cm on one side and without bulky lymph node metastases, lobectomy appears to be a safe alternative to total thyroidectomy regarding cancer recurrence.
Keywords
Introduction
Over the past decade, the optimal extent of surgery for papillary thyroid carcinoma (PTC) has progressively shifted from routine total thyroidectomy toward more individualized, risk-adapted strategies. 1 As the most prevalent histologic type of differentiated thyroid cancer, accounting for over 90% of cases, 2 PTC represents the primary focus of ongoing debates regarding surgical de-escalation. The 2025 American Thyroid Association (ATA) Management Guidelines for Adult Patients with Differentiated Thyroid Cancer represent a landmark evolution in this paradigm, refining the risk stratification system from the traditional three-tiered model to a more nuanced four-tiered classification—low, low-intermediate, intermediate-high, and high risk of recurrence. 3 This subdivision specifically addresses the heterogeneity within the former intermediate-risk category, incorporating detailed histopathologic features such as multifocality, the anatomical extent of lymph node metastasis, and quantitative nodal burden. The clinical imperative underlying this refinement is to better identify which patients genuinely benefit from more aggressive surgical approaches, while sparing others the avoidable surgical complications of overtreatment.4,5
For high-risk PTC patients, total thyroidectomy remains the standard of care with a well-established consensus. 3 For low-risk papillary thyroid microcarcinoma (PTMC), the safety of lobectomy is well established; accumulating evidence now further extends this paradigm to selected intermediate-risk patients, including those with lateral neck metastasis (N1b). In patients with unilateral multifocal node-negative PTMC, Jeon et al. 6 reported comparable locoregional recurrence between lobectomy (3.15%) and total thyroidectomy (0.78%; p = 0.244) over a median follow-up of 94.8 months. At the higher end of the risk continuum, a growing body of evidence challenges the traditional mandate for total thyroidectomy in patients with lateral neck metastasis.7,8 Ji et al. 9 extended these observations to T1-2 N1b disease, reporting comparable recurrence-free survival (RFS) between total thyroidectomy and lobectomy in patients with unilateral lateral neck metastasis. Similarly, Saito et al. 10 reported comparable 15-year RFS in cN1b patients undergoing lobectomy with ipsilateral lateral neck dissection versus total thyroidectomy (hazard ratio (HR): 1.10, 95% confidence interval (CI): 0.35–3.47). Two meta-analyses have further supported these findings: Cao et al. 11 confirmed no significant difference in recurrence outcomes between total thyroidectomy and lobectomy in patients meeting the 2015 ATA intermediate-risk criteria, while Li et al. 12 specifically pooled 2462 patients with lateral lymph node metastasis and demonstrated similar RFS (HR: 1.16, 95% CI: 0.63–2.12). However, these aggregate-level analyses were unable to isolate the specific subgroup of patients with unilateral multifocal disease and limited nodal burden, whose distinct risk profile and surgical considerations remain incompletely characterized.
A critical evidence gap therefore persists for precisely this population: intermediate-risk patients with unilateral multifocal PTC (tumor size 1–4 cm) whose nodal status ranges from node-negative to limited metastatic involvement (all metastatic foci <3 cm). According to the 2025 ATA framework, these patients occupy a transitional zone within the refined intermediate-risk category. 3 Patients whose only risk factor is unilateral multifocality fall within the low-intermediate risk stratum. However, when unilateral multifocality coexists with additional low-intermediate risk factors—such as microscopic extrathyroidal extension (ETE), cN1a with >2 mm or >5 metastatic nodes, or limited lateral metastasis—patients may be reclassified into the intermediate-high risk stratum based on cumulative risk burden. No dedicated study has systematically examined this population, whose risk profile spans the boundary between these two strata. Prior investigations rarely provided the anatomical compartment and quantitative nodal counts—information essential for understanding whether the effect of surgical extent varies with nodal burden or concomitant risk factors such as microscopic ETE.
To address this gap, we conducted a retrospective cohort study of 1373 patients with unilateral multifocal PTC (⩽4 cm) who met strict eligibility criteria: absence of gross ETE, distant metastasis, and bulky lymph nodes (all metastatic foci <3 cm). This cohort encompasses the full spectrum of nodal involvement—from node-negative to limited central or lateral metastases—and includes patients with or without microscopic ETE, reflecting the transitional risk profile described above. We aimed to compare recurrence risk between lobectomy and total thyroidectomy in this precisely defined population, with particular attention to the anatomical distribution and quantitative burden of lymph node metastases. By providing evidence specific to this understudied subgroup, this study aims to inform risk-stratified surgical decision-making for PTC patients occupying the boundary between low-intermediate and intermediate-high recurrence risk categories, helping to balance oncological safety with the avoidance of unnecessary surgical morbidity.
Methods
Study population and design
We conducted a retrospective cohort study of consecutive patients with unilateral multifocal PTC who underwent surgery at the Department of Thyroid, Breast, and Vascular Surgery, Xijing Hospital, between January 2008 and December 2024. Clinical and pathological data were retrospectively collected from electronic medical records and operative reports. Age was categorized as ⩽35, 35–55, and >55 years to retain the established 55-year prognostic threshold while distinguishing younger patients, who may have distinct clinical features.
Inclusion and exclusion criteria
Patients were eligible if they met all the following criteria: (1) postoperative pathological diagnosis of PTC; (2) postoperative pathological confirmation of multifocal tumors (⩾2 independent foci) within a single thyroid lobe; (3) a maximum diameter of the largest lesion of ⩽4.0 cm based on postoperative pathology; (4) absence of gross ETE as documented in surgical records; (5) no distant metastasis (M0); (6) initial surgery consisting of either lobectomy or total/near-total thyroidectomy; and (7) availability of regular postoperative follow-up data for ⩾12 months. Patients were excluded for any of the following: (1) maximum tumor diameter >4.0 cm; (2) cervical lymph node metastasis ⩾3 cm in maximum diameter (The 2025 ATA guidelines classify metastatic lymph nodes ⩾3 cm as a high-risk feature); (3) presence of gross ETE (pT3b or pT4); (4) bilateral or unilateral unifocal carcinoma; (5) pre-existing distant metastasis (M1); (6) history of prior malignant thyroid surgery or neck radiotherapy; or (7) missing crucial data on pathology, including focality, tumor size, or nodal status. As this was a retrospective cohort study, the sample size was determined by the inclusion of all consecutive eligible patients during the study period. A detailed flowchart of patient selection is shown in Figure 1.
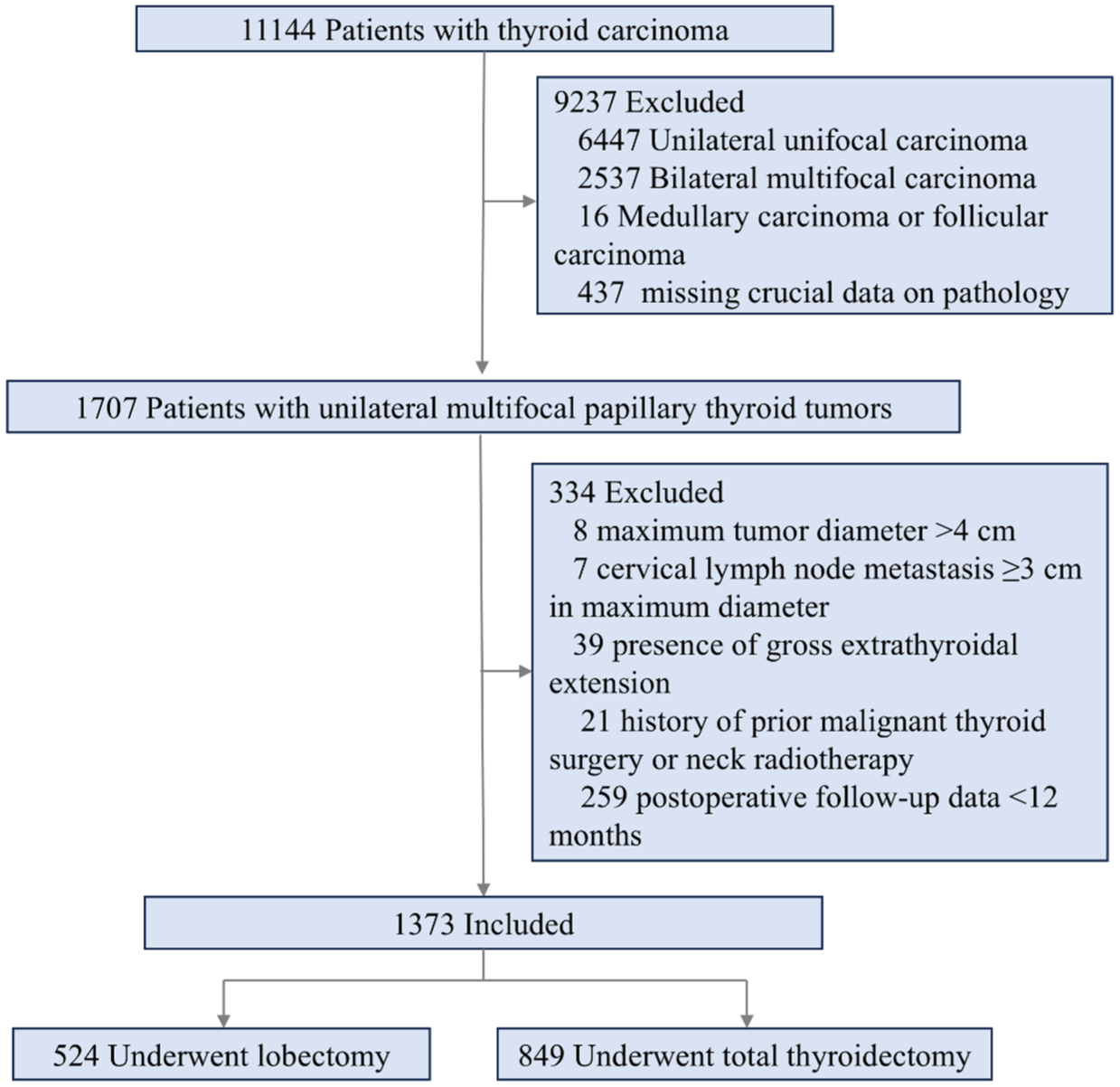
Flowchart of patient inclusion and exclusion.
Study definitions, follow-up, and outcome assessment
We used the STROBE reporting guideline to draft this manuscript. 13 Patients were categorized based on the extent of thyroid resection. The lobectomy group comprised individuals who received lobectomy, regardless of whether isthmectomy was performed; those who underwent lobectomy with concomitant nodule enucleation were also classified into this group. The total thyroidectomy group included patients who had total, subtotal, or near-total thyroid resection.
During the study period (2008–2024), surgical extent was determined according to the evolving ATA guidelines (2006, 2009, and 2015 editions) and the 2012 Chinese national guidelines for differentiated thyroid carcinoma. Total thyroidectomy was recommended for patients with high-risk features, including tumor size >4 cm, gross ETE, bilateral multifocal disease, high-burden lateral neck metastasis, distant metastasis, or high-risk pathological subtypes. For lobectomy, the indications were stratified by tumor size. For tumors ⩽1 cm, lobectomy was considered appropriate when all of the following conditions were met: unifocal disease confined to one lobe, no ETE, no lymph node metastasis, no history of head and neck radiation, and no family history of thyroid cancer. For tumors 1–4 cm, lobectomy could be considered in the absence of gross ETE, distant metastasis, and high-burden nodal disease, particularly when the contralateral lobe was free of nodules. For patients with intermediate-risk features—such as unilateral multifocal disease or limited nodal metastasis—either lobectomy or total thyroidectomy could be considered, and the final decision reflected a combination of physician judgment and patient preference. Consistent with the broader surgical paradigm shift toward de-escalation reflected in successive guideline editions, the adoption of lobectomy at our institution increased progressively over the study period (Table 1). The treatment period was dichotomized at 2020 to provide approximately balanced patient numbers across the two-time intervals (2009–2019, n = 565; 2020–2024, n = 808). This cutoff was chosen for descriptive purposes and does not correspond to a specific institutional policy change. All procedures were performed via a standardized open approach by senior surgeons in a single surgical department.
Patient demographic, clinical, and pathologic characteristics according to the extent of surgery (N = 1373).
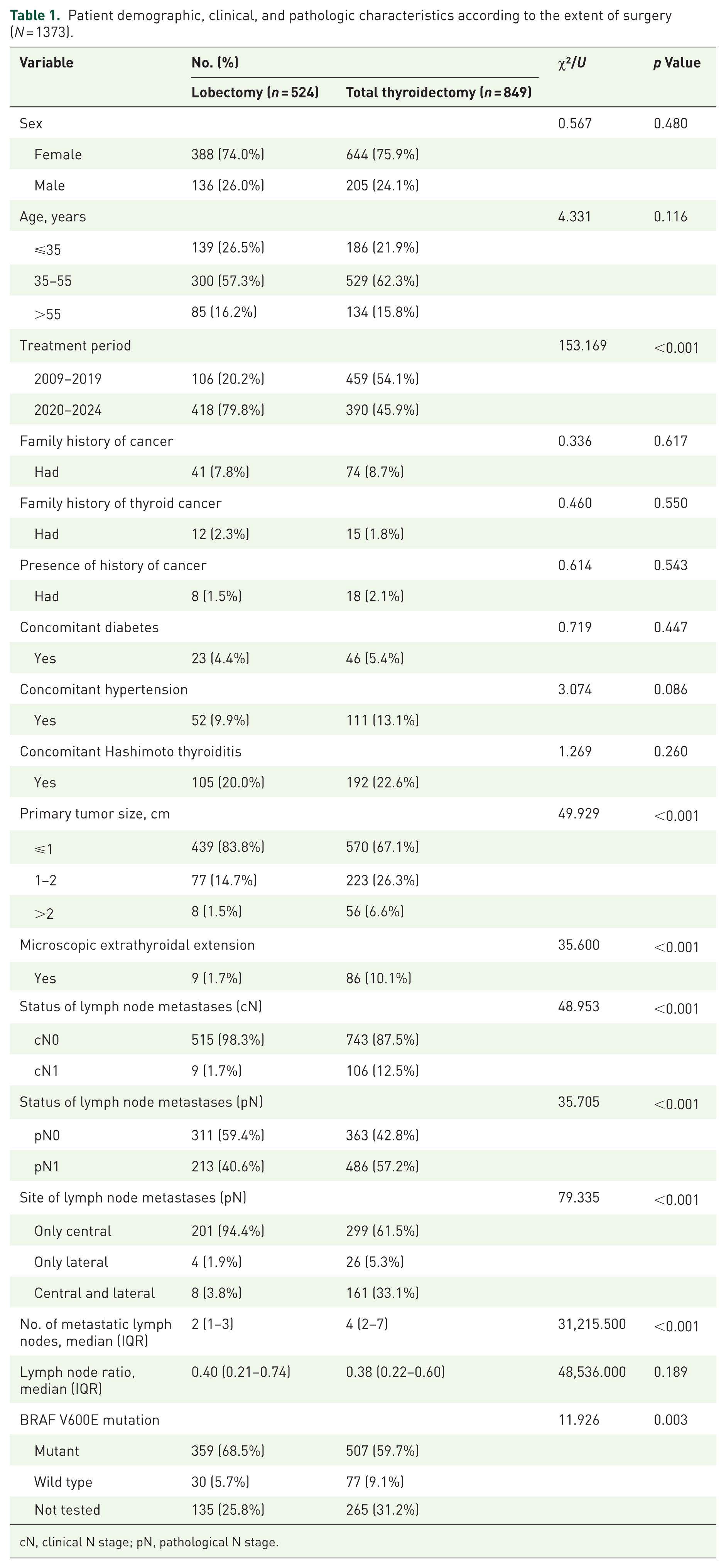
cN, clinical N stage; pN, pathological N stage.
Follow-up information was obtained via annual telephone interviews and review of outpatient records, with time calculated from the date of surgery. The primary outcome was structural recurrence, defined as structural evidence confirmed histopathologically or by imaging on two consecutive examinations. Biochemical abnormalities alone (elevated serum thyroglobulin or anti-thyroglobulin antibodies) were not considered recurrence.
Statistical analysis
The primary analysis employed inverse probability weighting regression adjustment (IPWRA) to estimate the average treatment effect (ATE) of lobectomy versus total thyroidectomy on recurrence risk. Propensity scores were estimated using logistic regression that included sex (categorical), age (continuous), tumor size (continuous), microscopic ETE (continuous), number of metastatic lymph nodes (continuous), lymph node metastasis ratio (continuous), BRAF mutation status (categorical), and treatment period (categorical). Inverse probability of treatment weights was derived from the propensity scores to balance baseline covariates between groups. These variables were selected as factors known to influence surgical decision-making in PTC. Covariate balance was assessed using standardized mean differences (SMD), with post-weighting SMD <0.15 considered adequate.
To assess the robustness of our primary findings, we performed three sensitivity analyses: (1) traditional multivariable logistic regression adjusting for all covariates; (2) 1:1 nearest-neighbor propensity score matching without replacement; and (3) inverse probability weighting (IPW). A power calculation for the multivariable Cox regression was performed. Given the total number of recurrence events (n = 36), the proportion of patients in the lobectomy group (38.2%), a two-sided α of 0.05, and a target power of 80%, the minimum detectable HR was estimated using the standard formula for Cox regression power: the detectable ln(HR) equals (Zα/2 + Zβ) divided by the square root of (events × proportion in treatment group × (1 − proportion in treatment group)). This threshold was compared with the observed HR to assess whether the analysis was adequately powered to detect clinically meaningful differences in recurrence risk by surgical extent.
To address the imbalance in follow-up duration without relying on weighting assumptions, a 5-year landmark analysis was performed. The cohort was restricted to patients with at least 60 months of follow-up, and the primary IPWRA model was re-estimated in this subgroup.
RFS was analyzed using Kaplan–Meier methods with the log-rank test. Multivariable Cox proportional hazards regression was used to identify independent predictors of recurrence. Subgroup analyses were performed to evaluate potential effect modification by sex, age, tumor size, local invasion, BRAF status, and ATA risk stratum. A non-inferiority margin of 3% absolute risk difference (RD) was prespecified based on the 2025 ATA risk stratification framework and margins adopted in contemporary thyroid cancer de-escalation trials. Non-inferiority was assessed using the IPWRA model by computing the two-sided 90% CI for the RD (lobectomy minus total thyroidectomy), which corresponds to a one-sided test at α = 0.05. Non-inferiority would be declared if the upper limit of the 90% CI was below the 3% margin. All analyses were conducted using Stata version 19.5 (StataCorp, College Station, TX, USA), with two-sided p < 0.05 considered statistically significant.
Results
Patient characteristics before and after IPW
A total of 1373 patients with unilateral multifocal differentiated thyroid carcinoma were included, of whom 524 (38.2%) underwent lobectomy, and 849 (61.8%) underwent total thyroidectomy (Figure 1). Table 1 presents the baseline characteristics. Before IPW, significant intergroup differences were observed. Compared with the total thyroidectomy group, the lobectomy group had a higher proportion of patients treated in the recent period, smaller tumor size, and a lower frequency of microscopic ETE (all p < 0.001). Regarding pathological lymph node status, the lobectomy group exhibited a lower prevalence of lymph node metastases (p < 0.001) and, among patients with lymph node involvement, a significantly higher proportion of metastases confined to the central compartment (p < 0.001). The number of metastatic lymph nodes was also markedly lower in the lobectomy group (p < 0.001). In addition, the lobectomy group demonstrated a higher prevalence of the BRAF V600E mutation (p = 0.003).
To mitigate confounding by baseline imbalances and obtain a more valid estimate of the comparative effectiveness of lobectomy versus total thyroidectomy on recurrence risk, we applied IPW to balance baseline covariates between the two groups. After applying IPW, all measured covariates achieved balance. As shown in Table 2, the post-weighting SMDs for all variables were below the prespecified threshold of 0.15, with several below 0.10. Substantial improvements were noted for the initially imbalanced variables: treatment period (SMD decreased from 0.748 to −0.139), tumor size (from −0.421 to −0.143), microscopic ETE (from −0.362 to −0.141), and number of metastatic lymph nodes (from −0.602 to 0.120). The substantial reduction in SMDs after weighting, as visualized in Figure 2, further supports the effectiveness of the weighting approach in achieving covariate balance.
Covariate balance before and after propensity score weighting (N = 1373).
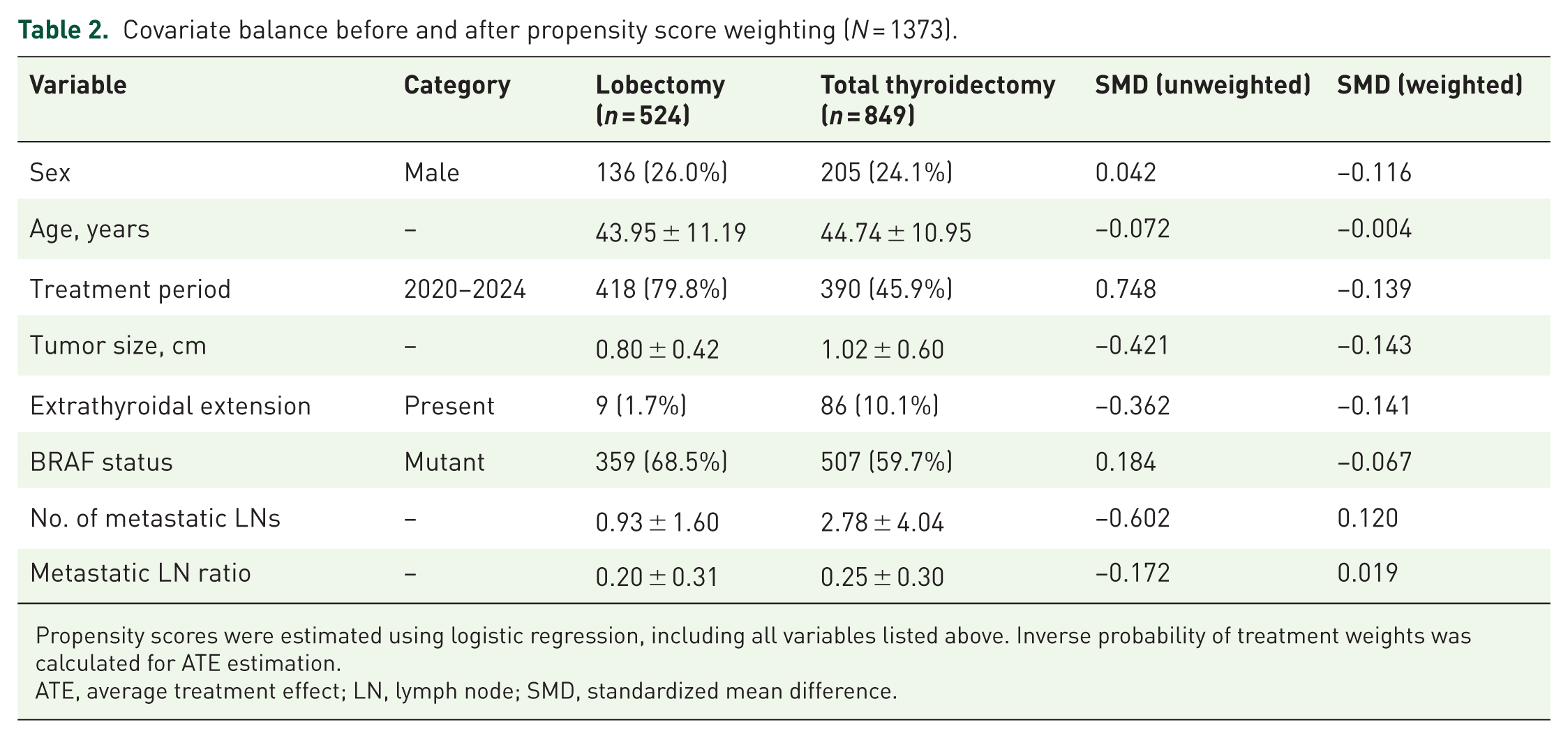
Propensity scores were estimated using logistic regression, including all variables listed above. Inverse probability of treatment weights was calculated for ATE estimation.
ATE, average treatment effect; LN, lymph node; SMD, standardized mean difference.
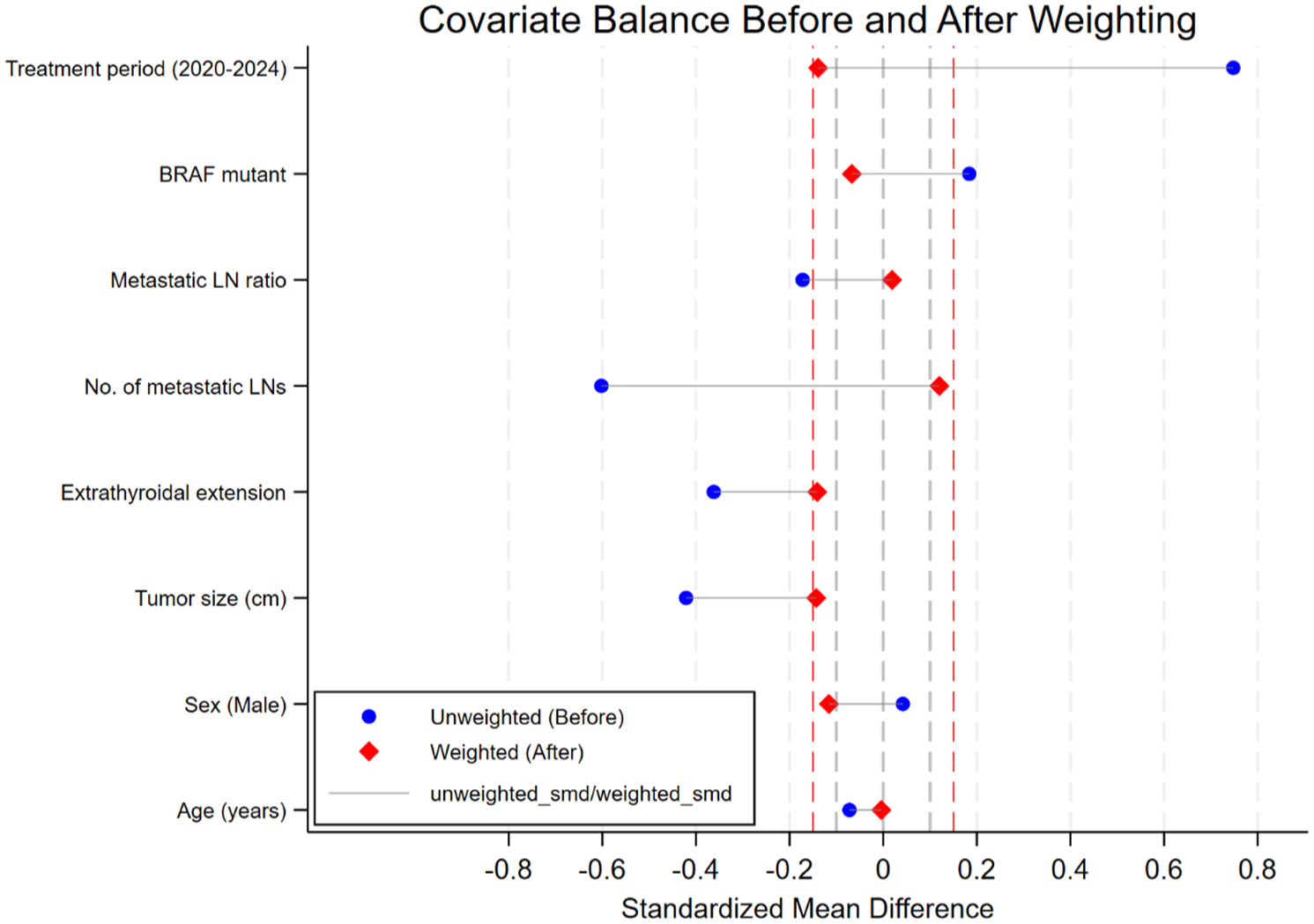
Standardized mean differences before and after inverse probability weighting.
RFS analysis
Median follow-up for the entire cohort was 52.4 months (range 12.1–201.6 months). The lobectomy group had a shorter median follow-up than the total thyroidectomy group (40.8 months (range 12.1–201.6) vs 66.2 months (range 12.1–201.6)). During follow-up, 36 recurrence events occurred, yielding an overall recurrence rate of 2.6% (36/1373). The recurrence rate was 1.9% (10/524) in the lobectomy group and 3.1% (26/849) in the total thyroidectomy group. When categorized by the 2025 ATA risk system, 1084 (79.0%) patients were at low-intermediate risk and 289 (21.0%) at intermediate-high risk. Recurrence occurred in 14 (1.3%) of low-intermediate-risk patients and 22 (7.6%) of intermediate-high-risk patients. Unadjusted RFS rates at predefined time points are presented in Table 3. The 5-year RFS rates were 97.10% (95% CI: 95.51%–98.14%) for total thyroidectomy and 97.34% (95% CI: 94.63%–98.69%) for lobectomy. At 10 years, the RFS rates were 96.56% (95% CI: 94.72%–97.76%) and 95.54% (95% CI: 89.31%–98.18%), respectively. The corresponding 15-year RFS rates were 89.46% (95% CI: 79.58%–94.71%) for total thyroidectomy and 95.54% (95% CI: 89.31%–98.18%) for lobectomy. No significant differences were observed at any time point.
Unadjusted recurrence-free survival rates at specific time points by surgical extent.
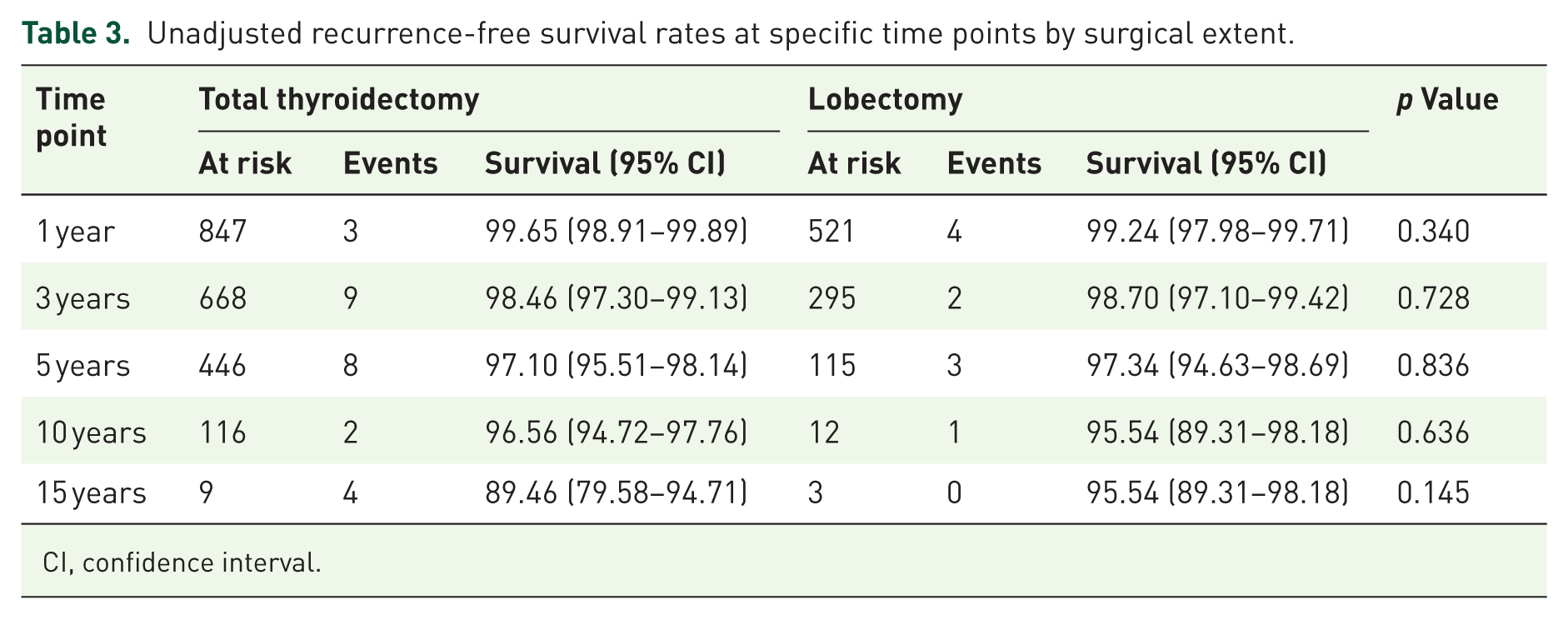
CI, confidence interval.
Figure 3 illustrates the Kaplan–Meier curves for RFS according to surgical extent before and after IPW. In the unadjusted analysis (Figure 3(a)), the log-rank test showed no significant difference between the lobectomy and total thyroidectomy groups (p = 0.857). After weighting, the survival curves remained closely overlapping, and the weighted log-rank test similarly demonstrated no significant difference (p = 0.086; Figure 3(b)).
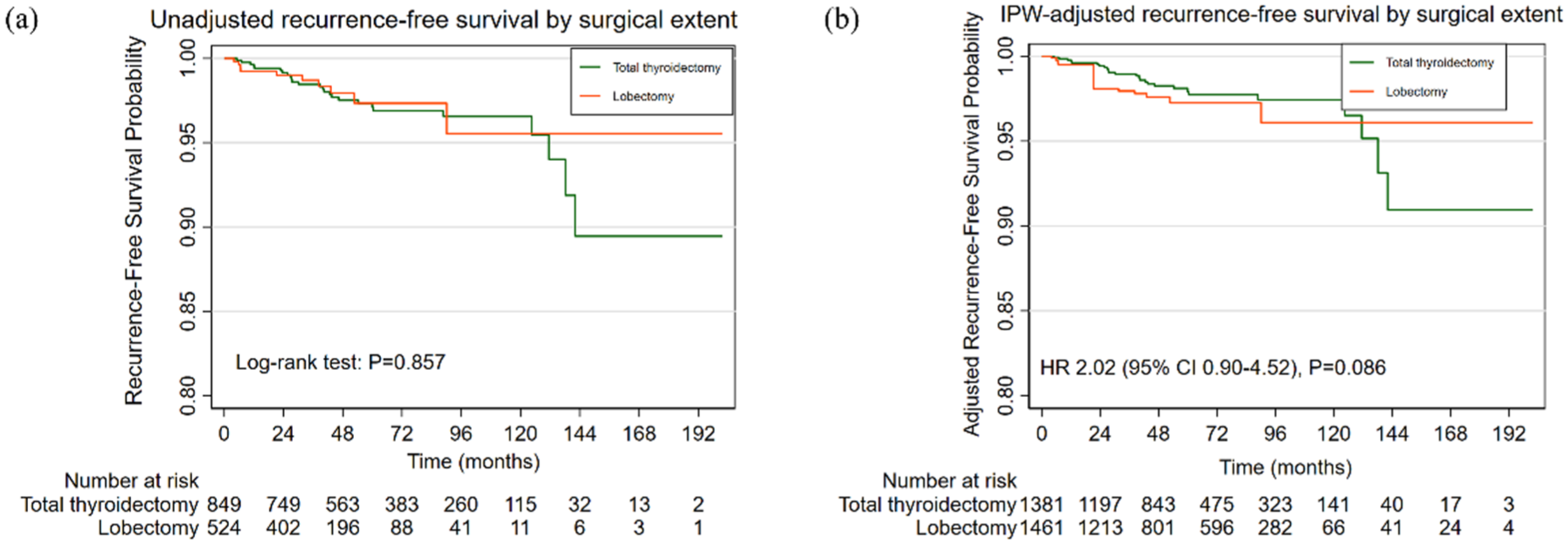
Recurrence-free survival of the enrolled patients before (a) and after adjustment (b).
The IPWRA analysis further corroborated these findings, revealing no statistically significant difference in recurrence risk between the two surgical groups (absolute RD, 1.19% (95% CI: −1.44% to 3.81%); p = 0.375), corresponding to an ATE of 0.0119 (Table 4). The estimated baseline recurrence rate in the total thyroidectomy group was 2.07% (95% CI: 1.27%–2.86%). In the non-inferiority analysis, the upper bound of the two-sided 90% CI for the RD was 3.39%, which marginally exceeded the prespecified 3% margin. Therefore, formal non-inferiority was not established.
IPWRA analysis of the effect of lobectomy versus total thyroidectomy on recurrence risk in papillary thyroid cancer (N = 1373).
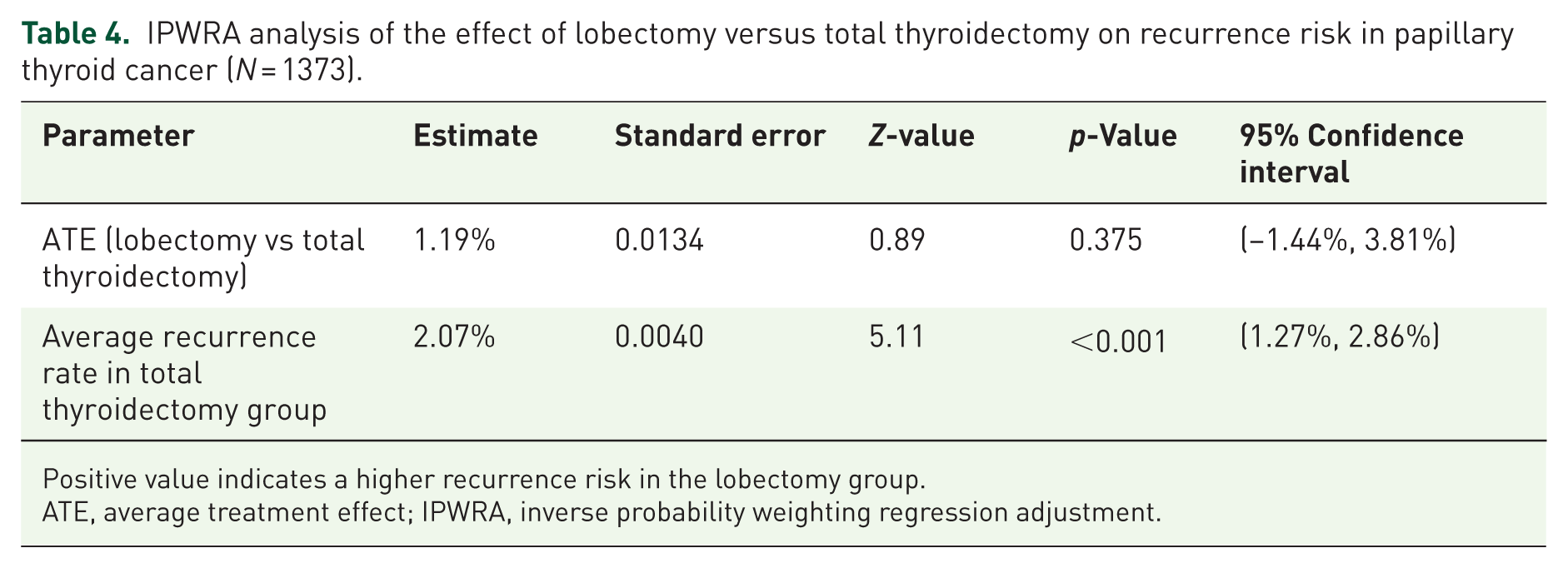
Positive value indicates a higher recurrence risk in the lobectomy group.
ATE, average treatment effect; IPWRA, inverse probability weighting regression adjustment.
To assess the robustness of our primary finding, we conducted sensitivity analyses using alternative statistical approaches. The RD estimates were non-significant in three of the four methods (Table 5): traditional multivariable logistic regression (RD = 1.48%, 95% CI: 0.89%–3.85%, p = 0.221), weighted logistic regression with trimmed weights (RD = 1.28%, 95% CI: −0.74% to 3.30%, p = 0.215), and the primary IPWRA analysis (RD = 1.19%, p = 0.375). The 1:1 propensity score matching yielded a significant RD (1.91%, 95% CI: 0.74%–3.08%, p = 0.001), which likely reflects the loss of 344 unmatched total thyroidectomy patients and reduced effective sample size. In the 5-year landmark analysis (n = 559), the ATE of lobectomy versus total thyroidectomy was 0.01% (95% CI: −2.30% to 2.32%; p = 0.994), confirming that the shorter follow-up in the lobectomy group did not materially bias recurrence estimates.
Sensitivity analysis of the effect of lobectomy versus total thyroidectomy on recurrence risk.
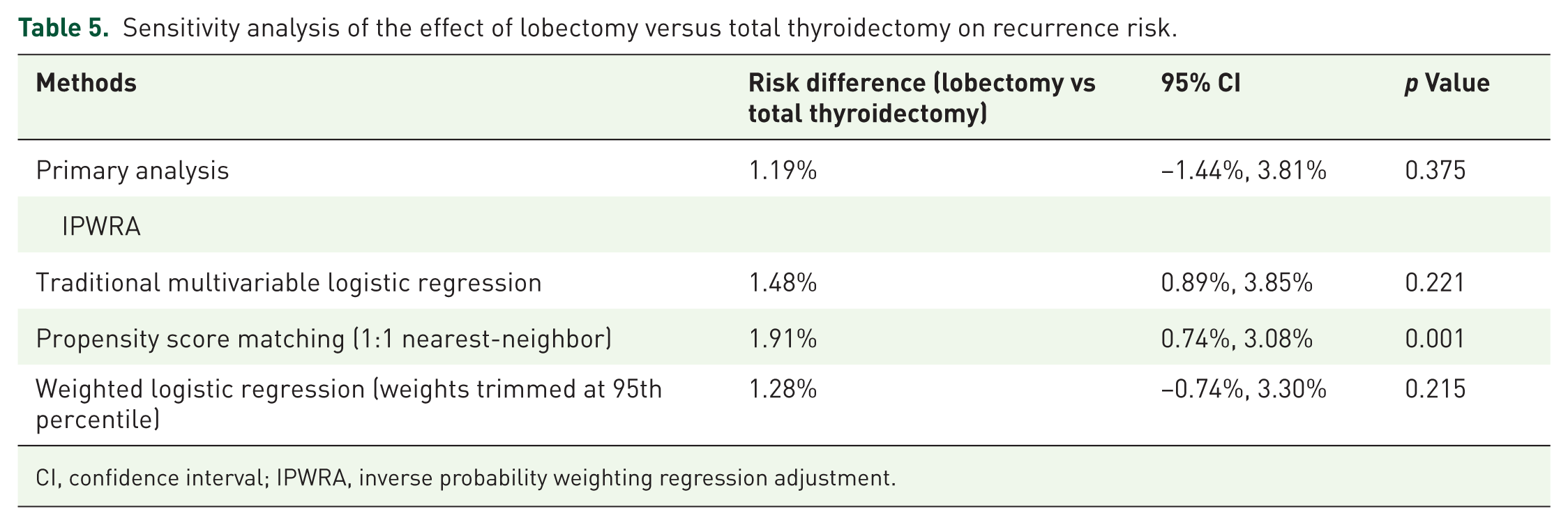
CI, confidence interval; IPWRA, inverse probability weighting regression adjustment.
Multivariable and subgroup analyses
In the multivariable Cox proportional hazards model adjusting for relevant covariates, the HR for lobectomy versus total thyroidectomy was 2.04, but the CI was wide (HR = 2.04, 95% CI: 0.91–4.62, p = 0.085; Table 6). A power calculation indicated that with 36 recurrence events, the model had 80% power to detect only HRs ⩾2.61; the observed point estimate therefore falls below the reliably detectable threshold. Independent predictors of recurrence included larger tumor size (1–2 cm: HR = 2.69, 95% CI: 1.13–6.39, p = 0.025; >2 cm: HR = 3.86, 95% CI: 1.12–13.29, p = 0.032), and presence of microscopic ETE (HR = 3.20, 95% CI: 1.23–8.29, p = 0.017). Radioactive iodine (RAI) was administered to 263 of 849 total thyroidectomy patients (31.0%). Within the total thyroidectomy group, RAI was not independently associated with recurrence (HR 1.37, 95% CI: 0.45–4.17; p = 0.582). When added to the overall Cox model, RAI remained non-significant (HR 1.41, 95% CI: 0.47–4.23; p = 0.544), and the HR for lobectomy was materially unchanged (HR 2.28 vs 2.04).
Multivariable Cox proportional hazards analysis for recurrence-free survival.
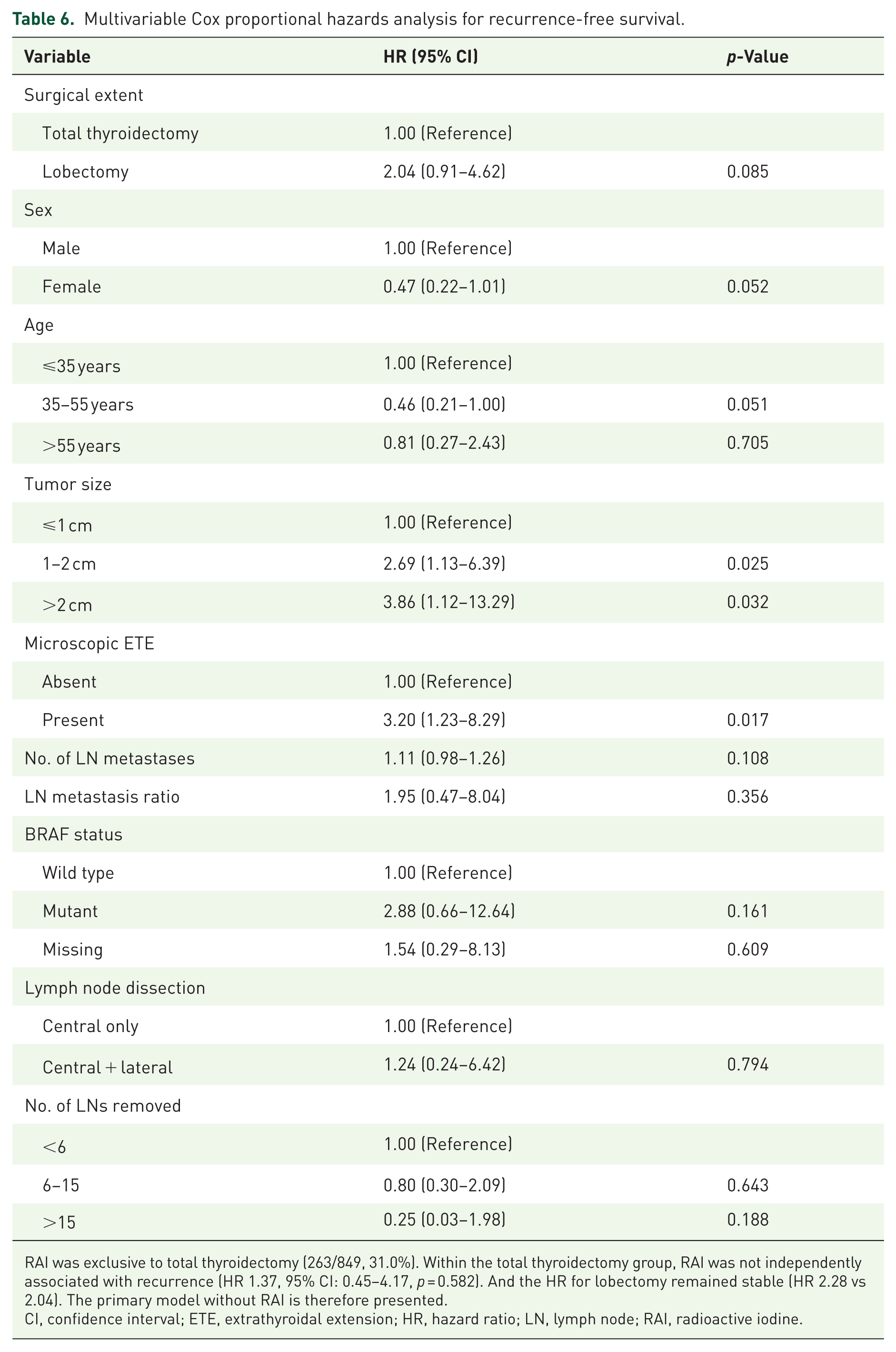
RAI was exclusive to total thyroidectomy (263/849, 31.0%). Within the total thyroidectomy group, RAI was not independently associated with recurrence (HR 1.37, 95% CI: 0.45–4.17, p = 0.582). And the HR for lobectomy remained stable (HR 2.28 vs 2.04). The primary model without RAI is therefore presented.
CI, confidence interval; ETE, extrathyroidal extension; HR, hazard ratio; LN, lymph node; RAI, radioactive iodine.
Subgroup analyses were performed to evaluate potential heterogeneity in the treatment effect across strata defined by sex, age, tumor size, local invasion, BRAF status, and the ATA risk stratum. As shown in the forest plot (Figure 4), no statistically significant interactions were observed; all HR CIs crossed unity. These findings indicate that the absence of a significant difference in recurrence risk between lobectomy and total thyroidectomy was consistent across all patient subgroups examined. However, given the limited number of total recurrence events (n = 36), these exploratory analyses are underpowered.
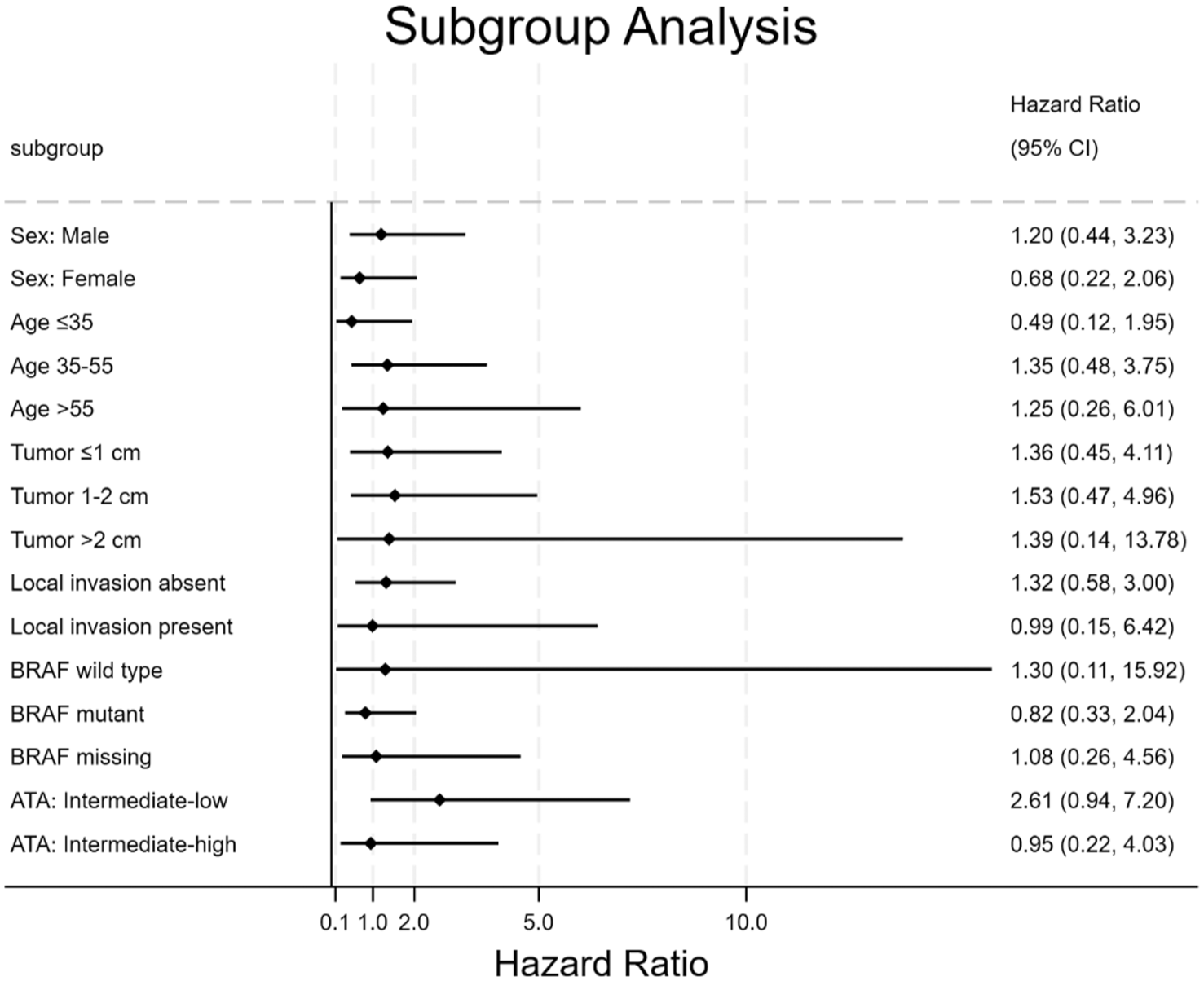
Forest plot of subgroup analyses for recurrence risk: lobectomy versus total thyroidectomy in patients with unilateral multifocal thyroid cancer.
Discussion
In this large cohort study of patients with unilateral multifocal PTC (⩽4 cm) and no bulky lymph node metastasis (all metastatic foci <3 cm), we found no significant difference in recurrence risk between lobectomy and total thyroidectomy after IPW adjustment. A non-inferiority analysis with a prespecified margin of 3% yielded a 90% CI upper bound of 3.39%, which marginally exceeded the margin; therefore, formal non-inferiority was not established. However, the 5-year landmark analysis demonstrated a near-zero difference between groups, and the consistency of findings across sensitivity analyses supports the robustness of the primary result. Directionally consistent treatment effects were observed across key clinical subgroups, including patients with varying tumor sizes, nodal status, the presence or absence of microscopic ETE, and the 2025 ATA risk stratum (low-intermediate vs intermediate-high). Though these subgroup analyses are exploratory, underpowered due to the limited number of recurrence events (n = 36), and should not be used to guide clinical decision-making. The multivariable Cox regression was similarly underpowered and is not relied upon for the primary conclusions. Collectively, based on the IPWRA analysis and the consistency observed across sensitivity analyses, these results suggest that for this precisely defined population—occupying the boundary between low-intermediate and intermediate-high risk strata in the 2025 ATA guidelines—surgical de-escalation may be safely considered without compromising oncologic outcomes.
A fundamental challenge in retrospective studies is that treatment allocation is non-random, intertwining true treatment effects with confounding bias because of baseline differences between groups. 14 To address this, we employed IPWRA, a doubly robust method within the propensity score framework. 15 IPWRA first constructs a propensity score model for the likelihood of undergoing lobectomy versus total thyroidectomy, then weights each observation by the inverse probability of the received treatment. This weighting creates a pseudo-population in which measured covariates are balanced between the surgical groups, approximating the conditions of a randomized trial and enabling estimation of the marginal ATE. 16 A key advantage of IPWRA is its double-robustness property: it yields consistent estimates of the ATE if either the treatment model or the outcome model is correctly specified, offering greater robustness than propensity score matching or conventional multivariable adjustment alone. 17 In our study, IPWRA successfully achieved excellent covariate balance, with all post-weighting SMD falling below 0.15, supporting the validity of our causal interpretation. To further assess robustness, we performed four complementary sensitivity analyses—traditional multivariable logistic regression, 1:1 nearest-neighbor propensity score matching, weighted logistic regression, and a 5-year landmark analysis. Three of the four methods yielded non-significant RD estimates consistent with the primary analysis, while the 1:1 PSM yielded a nominally significant result that likely reflects post-matching sample attrition. These consistency methods substantially reduce the likelihood that our conclusions are artifacts of any single analytical approach. Beyond baseline imbalance, the substantial difference in median follow-up (40.8 vs 66.2 months) raised the concern that late recurrences might have been missed in the lobectomy group. To address this, we performed both inverse probability of censoring weighting (IPCW) and a 5-year landmark analysis. The IPCW model yielded unstable estimates due to extreme weights, a recognized limitation with rare events. By contrast, the landmark analysis—which equalizes follow-up by restricting to patients with ⩾60 months of observation—showed a near-zero difference between groups (ATE 0.01%, p = 0.994). These complementary approaches confirm that neither baseline imbalance nor differential follow-up meaningfully biased our conclusions.
While subgroup analyses in our study provide a qualitative description of treatment effects across patient strata and allow comparison with prior studies, they are exploratory and underpowered; the following observations should therefore be interpreted as hypothesis-generating rather than confirmatory. In our cohort, the absence of interaction between surgical extent and tumor size categories (⩽1, 1–2, >2 cm) provides a preliminary suggestion that lobectomy remains comparable to total thyroidectomy across the 1–4 cm range. This aligns with Song et al., 18 who demonstrated in a 10-year propensity-matched analysis that lobectomy is feasible for 1–4 cm PTC without compromising disease-free survival. Even when stratified at 2–4 cm, no differential effect of surgical extent emerged in their study or ours. Our analysis incorporated two quantitative nodal metrics—number of metastatic lymph nodes and lymph node ratio—neither of which demonstrated a significant interaction with surgical extent in subgroup analyses. This finding, though limited by power, suggests that the comparative effectiveness of lobectomy versus total thyroidectomy may not vary according to nodal burden, specifically in patients with all metastatic foci <3 cm who undergo systematic lymph node dissection of the involved compartments. While our primary finding emphasizes equivalence across nodal strata, nodal burden itself remains a powerful prognostic factor. Previous studies have consistently shown that high-burden nodal disease—characterized by multiple involved nodes, larger metastatic foci, or elevated lymph node ratio—is associated with increased recurrence risk.19 –21 These observations are not contradictory to our findings; rather, they highlight that nodal burden determines baseline recurrence risk irrespective of surgical extent. In our study, the total thyroidectomy group had significantly higher nodal burden (median 4 vs 2 metastatic nodes; 33.1% vs 3.8% lateral involvement). That no recurrence difference emerged after weighting provides an exploratory signal that adequate nodal dissection may neutralize the prognostic impact of nodal burden, at least within our inclusion criteria. This interpretation aligns with studies in N1b disease showing that features such as extranodal extension or maximum node diameter—not thyroid resection extent—drive recurrence, 22 and that lobectomy is feasible for selected patients with lateral metastasis when nodal disease is appropriately managed.9,23 Similarly, microscopic ETE did not significantly interact with surgical extent in our exploratory analysis, consistent with large studies reporting no recurrence difference between lobectomy and total thyroidectomy after accounting for mETE. 24 However, mETE may influence outcomes indirectly by promoting nodal dissemination. It is independently associated with lateral lymph node metastasis. 25 In patients with lateral metastasis, mETE has been identified as a marker of tumor aggressiveness. Ji et al. 9 found that minor ETE, together with lymph node ratio >0.49, independently predicted structural recurrence, whereas the extent of thyroidectomy was not a significant factor. These observations position mETE as a biological marker of tumor aggressiveness rather than a direct indicator for more extensive thyroid resection. Once mETE is accounted for through appropriate nodal management—as achieved by weighting in our analysis—lobectomy and total thyroidectomy remain comparable. Collectively, these findings reinforce that within the 1–4 cm range, the cumulative burden of risk features—including tumor size, quantitative nodal metrics (number and ratio), and mETE—should inform postoperative risk stratification and surveillance intensity. Collectively, these exploratory findings suggest directions for future investigation rather than establishing definitive conclusions. They reinforce the importance of integrating detailed nodal and pathologic features into risk assessment, but do not independently justify surgical decision-making.
Limitations
Several limitations of this study should be acknowledged. First, its retrospective, single-center design inherently carries the potential for selection bias, despite our rigorous adjustment using IPWRA and multiple sensitivity analyses. Unmeasured confounding—such as surgeon experience, patient preference, or details of lymph node dissection completeness—cannot be entirely excluded. Second, the relatively small number of recurrence events (n = 36), while consistent with the indolent nature of PTC, limited statistical power for subgroup analyses; these exploratory analyses should therefore not be used to guide clinical decision-making. The robustness of the primary conclusion is supported by the consistency of findings across the IPWRA-based sensitivity analyses and the landmark analysis, rather than by subgroup precision. Third, our study population was derived from a single institution in China, which may limit generalizability to other populations with different genetic backgrounds, iodine intake, or clinical practice patterns. Fourth, we did not systematically collect data on postoperative complications, quality-of-life measures, or patient-reported outcomes, which are essential for fully understanding the trade-offs between surgical approaches. Finally, our exclusion of patients with lymph nodes ⩾3 cm means that our findings cannot be extrapolated to those with bulky nodal disease, for whom total thyroidectomy remains standard. Future multicenter prospective studies with longer follow-up and comprehensive collection of oncologic and patient-centered outcomes are warranted to validate and extend our observations.
Conclusion
In this large, rigorously adjusted cohort study of patients with unilateral multifocal PTC (⩽4 cm) and no bulky lymph node metastasis (all involved nodes <3 cm), no significant difference in recurrence risk between lobectomy and total thyroidectomy after IPW adjustment. Although formal non-inferiority within the prespecified 3% margin was not established, the primary analysis, the 5-year landmark analysis, and the majority of sensitivity analyses consistently showed no statistically significant difference between the two surgical approaches. The multivariable Cox regression was underpowered and inconclusive in this regard. Directionally consistent treatment effects were observed across key subgroups, though these subgroup analyses are underpowered and should not guide clinical practice. Collectively, based on these findings, our results extend the evidence for surgical de-escalation to this specific intermediate-risk population—those occupying the boundary between low-intermediate and intermediate-high risk strata in the 2025 ATA guidelines. For such patients, lobectomy with systematic compartment-oriented lymph node dissection may offer a safe alternative that balances oncological safety with the potential avoidance of excess surgical morbidity. These findings support individualized, risk-stratified decision-making and underscore the importance of integrating detailed nodal and pathologic features—rather than relying on categorical rules based on any single factor—when determining the appropriate extent of thyroid resection.