
Abstract
Background:
Licorice, a commonly used traditional Chinese medicine in clinical practice, and pharmaceuticals with glycyrrhiza or glycyrrhiza extract as the main component play an important role in the treatment of hepatic and biliary system diseases and other conditions. Its dual identities as a traditional Chinese material medica and a natural phytocomponent have led to the underestimation of its latent adverse drug reactions (ADRs) in clinical and research.
Objective:
This study adopted a retrospective literature analysis method and stratified subgroups based on the inherent attribute differences of different study types, aiming to explore the characteristic differences in ADRs induced by glycyrrhiza-containing Chinese patent medicines under different study designs and considering the individual differences among patients.
Design:
A retrospective literature analysis was conducted in this study.
Methods:
This study adopted a retrospective study design. We searched PubMed, Web of Science, Scopus, Google Scholar, CNKI, Wanfang, and VIP Database from index inception to August 2025. Data on patient demographics, ADRs details, medication regimens, and outcomes were extracted and analyzed via SPSS 23.0.
Results:
A total of 120 articles were included (110 case reports, 10 clinical trials: 2 case series, 8 RCTs). Patient-related high-risk factors included males aged >60 years, hepatic insufficiency, or drug allergy history. Drug-related risk factors included off-label dosage, specific administration routes, and concomitant use with thiazide diuretics, drugs that induce arrhythmias or electrolyte disturbances, as well as agents with high plasma protein binding rates. All these factors were associated with the incidence and severity of ADRs. Most symptoms were alleviated following timely drug withdrawal and targeted treatment.
Conclusion:
ADRs induced by Glycyrrhiza-containing Chinese patent medicines involve multiple organ systems. Early detection and prompt drug withdrawal are crucial for symptom alleviation. In clinical practice, such preparations should be administered in conjunction with patients’ individual characteristics to ensure rational drug use.
Plain language summary
This study analyzed 135 cases of adverse drug reactions (ADRs) induced by glycyrrhiza-containing Chinese patent medicines, as well as 10 clinical trials. High-risk populations included patients aged ⩾60 years, male individuals, those with underlying comorbidities (e.g., hepatic/renal insufficiency, hypertension), and subjects with a history of drug allergies. Drug-related risk factors comprised supratherapeutic doses, intravenous infusion administration, and concomitant use with thiazide diuretics or drugs exhibiting high plasma protein binding rates. Primary ADRs involved endocrine/metabolic disorders (hypokalemia, pseudohyperaldosteronism), allergic reactions (including life-threatening anaphylactic shock), cardiovascular complications (hypertension, arrhythmias), as well as rhabdomyolysis and drug dependence (predominantly linked to compound glycyrrhiza tablets). The mechanistic basis lies in the inhibition of 11β-hydroxysteroid dehydrogenase type II (11β-HSDII) by glycyrrhiza metabolites (glycyrrhizic acid, glycyrrhetinic acid), which disrupts glucocorticoid metabolism and elicits aberrant renal cortisol activity. Most ADRs achieved resolution following drug withdrawal plus symptomatic management, with only one fatal case documented. Recommendations include allergy history assessment prior to administration, serial monitoring of serum potassium and blood pressure during treatment, avoidance of high-risk drug combinations, and strict adherence to recommended dosages and treatment durations.
Introduction
Licorice belongs to the Fabaceae family, and its medicinal parts are the roots and rhizomes. Pharmacological research primarily focuses on compounds such as glycyrrhizic acid, glycyrrhetinic acid, flavonoids, and polysaccharides. These compounds exhibit pharmacological effects including anti-inflammatory activity, immune modulation, inhibition of inflammatory mediators, promotion of hepatocyte repair, and antitussive and expectorant actions. Clinically, agents such as diammonium glycyrrhizinate and compound glycyrrhizin are commonly used to improve liver function in patients with liver diseases. Compound licorice preparations are frequently employed for cough suppression in respiratory conditions.1,2 In addition, because of the anti-inflammatory properties of its active components, licorice is often used for dermatologic conditions such as rashes and psoriasis. Thus, licorice is widely used clinically as a traditional Chinese medicine ingredient. However, precisely because it is a herbal component, the risk of adverse drug reactions (ADRs) is often overlooked in clinical use. Its most common side effect is pseudohyperaldosteronism, a clinical condition characterized by hypertension, hypokalemia, and suppression of plasma renin and aldosterone levels. 3 In 1946, Revers 4 first reported cases of hypokalemia and hypertension in Dutch children following consumption of licorice candy. This study used case reports as the core and combined them with baseline data of clinical trials to reveal the characteristics of rare or severe ADRs induced by glycyrrhiza-containing Chinese patent medicines. Through systematic literature retrieval, case reports and various types of clinical trial data associated with ADRs caused by glycyrrhiza-containing Chinese patent medicines were comprehensively collected, systematically collated, and integrated. On this basis, subgroups for case report data and clinical trial data were established, respectively. With a primary focus on subgroup analysis of case reports, this study integrated data on the same category of indicators from clinical trials to classify the occurrence patterns of ADRs, and further statistical tests were conducted to clarify the statistical significance of intergroup differences. Based on clinical trial data, the overall characteristics and general patterns of ADRs occurrence induced by glycyrrhiza-containing Chinese patent medicines were analyzed. Meanwhile, relying on case report data, a more detailed analysis was performed on ADRs of varying severity and rare ADRs triggered by special scenarios. The purpose of this study was to provide a reference for the rational clinical application of glycyrrhiza-containing Chinese patent medicines.
Methods
This literature-based case series and clinical trial analysis is a retrospective observational study, and the full text strictly follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline 5 as the core reporting framework (Supplemental Materials 1). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guideline 6 is only used as a supplementary methodological reference to standardize the whole process of literature search, screening, and data extraction, to ensure the comprehensiveness, repeatability, and transparency of literature retrieval, and to avoid selection bias and retrieval bias from the source. The specific application scope and compliance of PRISMA-ScR are detailed in Supplemental Materials.
Search strategy
PubMed, Web of Science, Scopus, and Google Scholar were systematically searched with the keywords “Licorice” OR “Glycyrrhiza” AND “glycyrrhizin” OR “Diammonium Glycyrrhizinate” AND “adverse reaction” OR “hypokalemia” OR “hypertension.” For Chinese databases, CNKI, Wanfang, and VIP were searched using the keywords “licorice,” “glycyrrhizin,” “Meineng,” “diammonium glycyrrhizinate,” “Ganlixin,” and “licorice zinc,” in combination with “adverse reaction,” “cause,” “induce,” “hypokalemia,” “hypertension,” and “allergic reaction.” This literature search was conducted and completed from August to December 2025, covering all relevant literature published from the inception of each database up to August 2025 that focused on ADRs associated with licorice preparations.
Inclusion and exclusion criteria
Literature inclusion criteria:
(1) The study population consists of individuals administered glycyrrhiza-containing Chinese patent medicines, including but not limited to diammonium glycyrrhizinate, compound licorice tablets, compound licorice mixture, compound licorice oral solution, licorzinc, magnesium isoglycyrrhizinate, etc.
(2) ADRs are clearly documented; in case reports, ADR records must contain detailed information, including clinical manifestations, onset time, and outcomes.
(3) The language of the literature is restricted to Chinese and English.
(4) Study types include case reports or small-scale case series of the aforementioned drugs, as well as clinical trial literature, such as RCTs, cohort studies, and cohort–case analyses.
(5) Publication timeframe: Literature published from the establishment date of each database to August 2025.
Literature exclusion criteria:
(1) Studies involving non-Chinese patent medicines containing glycyrrhiza, such as glycyrrhiza decoctions, nutritional products, and health supplements.
(2) Duplicate publications (only the version with the most complete data is retained). Reviews, meta-analyses, and theoretical discussion papers.
(3) Literature without ADR records or with unclear causality between ADRs and glycyrrhiza-containing Chinese patent medicines.
(4) Literature with incomplete data and missing no less than three items of key information (e.g., dosage, specific manifestations of ADRs).
(5) Others: Animal studies, production technology research, quality control studies, etc.
Subgroup-specific inclusion and exclusion requirements:
Case report subgroup:
Exclusion criteria: Case reports were excluded if patients concomitantly used drugs with definite hepatotoxicity/nephrotoxicity or other high-risk combined medications, and the causality of ADRs could not be assessed.
Inclusion criteria: Data on patients’ baseline characteristics (age, gender, underlying diseases, allergy history, etc.), medication dosage and administration, organ systems involved in ADRs and corresponding symptoms, as well as the onset and outcome time of ADRs were included.
Clinical trial subgroup:
Exclusion criteria: Clinical trials were excluded if they lacked placebo or positive controls, involved combined use of glycyrrhiza-containing Chinese patent medicines with other drugs, or failed to set ADR monitoring indicators.
Inclusion criteria: Data on ADR incidence rates and corresponding symptoms were included.
Study selection
The articles found in the database search were transferred to Endnote 2025 to identify and delete any duplicate articles. Two authors independently screened the titles and abstracts of all retrieved studies. Then, full-text screening of each potentially eligible study was independently done by two reviewers, and discrepancies were resolved through consensus. If the difference remained unresolved, a third reviewer adjudicated to reach a predefined consensus.
Data extraction
The double-independent data extraction method was adopted, where two researchers extracted data separately based on a pre-designed data extraction form. Discrepancies were resolved through discussion or arbitration by a third party. The extracted fields were divided into general fields and subgroup-specific fields:
General fields: Basic literature information, details of glycyrrhiza-containing Chinese patent medicines (drug name, dosage form, administration route), and basic characteristics of ADRs (involved organ systems, clinical manifestations).
Case report subgroup-specific fields: Patients’ baseline characteristics (age, gender, underlying diseases, allergy history), medication details (dosage and administration, concomitant medications), onset time, and remission time of ADRs. In addition, the causality of ADRs was evaluated according to the Naranjo Adverse Drug Reaction Probability Scale. The severity of ADRs was assessed and graded in accordance with the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) Version 4.03, 7 which categorized ADRs into grades 1–5: grade 1 denotes mild ADRs, grade 2 denotes moderate ADRs, grades 3–4 denote severe ADRs, and grade 5 denotes fatal ADRs. 5
Specific fields of the clinical trial subgroup: Study sample size, dosage and administration of the target drug, ADRs incidence proportion, and involved organ systems.
Quality assessment of included RCTs
The methodological quality of the included RCTs was evaluated using the Jadad scale, 8 a validated tool for assessing the quality of RCTs. RCTs were categorized based on the total score: low quality (⩽2 points) and high quality (⩾3 points). Two independent reviewers completed the quality assessment separately. Discrepancies in scores were resolved through discussion; if consensus was not reached, a third reviewer adjudicated.
Research methods
A retrospective approach was employed to extract and analyze relevant information, including patient age, gender, dosage and administration of licorice preparations, indications for licorice preparations, underlying medical conditions, concomitant medications, types of ADRs, timing of onset, timing of relief, management strategies, and outcomes.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). Quantitative data were expressed as mean ± standard deviation (x ± s) and analyzed by the t test. Qualitative data were presented as the number of cases (n) and percentage (%), and analyzed using the chi-square (χ2) test. A p value <0.05 was considered statistically significant.
Results
A total of 120 publications were included, among which 118 were in Chinese and 2 were in English. Of these, 108 were case reports or small-scale case series, corresponding to 135 ADRs cases in total (Supplemental Table A1), 8 commonly used clinical medications were identified: diammonium glycyrrhizinate (42 cases, 31.11%), compound glycyrrhiza mixture (9 cases, 6.67%), compound glycyrrhiza oral solution (8 cases, 5.93%), compound glycyrrhiza tablets (28 cases, 20.74%), monoammonium glycyrrhizinate compound (4 cases, 2.96%), glycyrrhizin compound (41 cases, 30.37%), licorice zinc (2 cases, 1.48%), and magnesium isoglycyrrhizinate (1 case, 0.74%).
A total of eight RCTs were identified, and all were assessed for methodological quality with the Jadad scale. Each trial achieved a score of 1–2 points, signifying low methodological quality, mainly due to insufficiently clear descriptions of randomization methods and deficiencies in blinding design in some studies. Thirty-five ADR cases derived from compound glycyrrhizin and 33 ADR cases from diammonium glycyrrhizinate across these studies. In addition, two cohort–case analyses were included, reporting 249 ADR cases induced by compound glycyrrhizin and 38 ADR cases induced by diammonium glycyrrhizinate (Supplemental Table A2). The medications involved in all included studies were compound glycyrrhizin and/or diammonium glycyrrhizinate.
The drugs included in the clinical trial subgroup were limited to diammonium glycyrrhizinate and compound glycyrrhizin. The incidence rate of ADRs induced by compound glycyrrhizin was 3.97% (284/7152), while that induced by diammonium glycyrrhizinate was 8.24% (71/862). Chi-square test showed a significant difference in ADRs incidence between the two drugs (p < 0.05); diammonium glycyrrhizinate was associated with a 2.17-fold higher ADRs risk than compound glycyrrhizin (OR: 2.17, 95% CI: 1.66–2.84). According to the statistical analysis of ADR distribution by involved organ systems, the top three affected systems among patients in the 120 publications were as follows: the skin, mucous membrane and appendage system (334 cases, 36.80%), the digestive system (119 cases, 23.60%), and the endocrine and metabolic system (57 cases, 10.71%).
Results of ADRs etiology and causality assessment
The causality between the herbal medicines containing glycyrrhizic acid and the reported ADRs was evaluated according to the Naranjo Adverse Drug Reaction Probability Scale (Table 1). Among the 135 patients in the case report subgroup, 90 cases were assessed as probable (34 cases with 5 points, 25 cases with 6 points, 28 cases with 7 points, and 3 cases with 8 points), and 45 cases were assessed as possible (10 cases with 3 points and 35 cases with 4 points). Of these ADR cases, 119 were directly induced by the glycyrrhiza component in the medications; 5 cases were attributed to other components in the compound preparations (e.g., morphine, alcohol); 8 cases were caused by concomitant medication; and 3 cases were jointly induced by the interaction between other components in the compound preparations and concomitant drugs.
Naranjo Adverse Drug Reaction Probability Scale.

Doubtful ADR (<2); possible ADR (2–4); probable ADR (5–8); definite ADR (⩾9).
ADR, adverse drug reaction.
Demographic and clinical information of the participants
The study included 135 patients who experienced ADRs due to licorice preparations. Males accounted for 60.74%, and females accounted for 39.26%. The mean age was 49.88 ± 20.35 years. The age distribution spanned a wide range, with the youngest patient being 1.5 years old and the oldest 92 years old (Table 2). A total of 108 cases (80.00%) had underlying diseases. The top five underlying diseases were as follows: hypertension (24 cases, 10.91%), viral hepatitis (23 cases, 10.45%), hepatic insufficiency (17 cases, 12.59%), elevated transaminase levels (12 cases, 5.45%), as well as diabetes mellitus, psoriasis vulgaris, and chronic bronchitis (7 cases, 3.18% for each). In addition, eight patients (5.92%) had a history of allergy.
Gender and age analysis of patients with ADRs induced by glycyrrhiza preparations (n = 135).
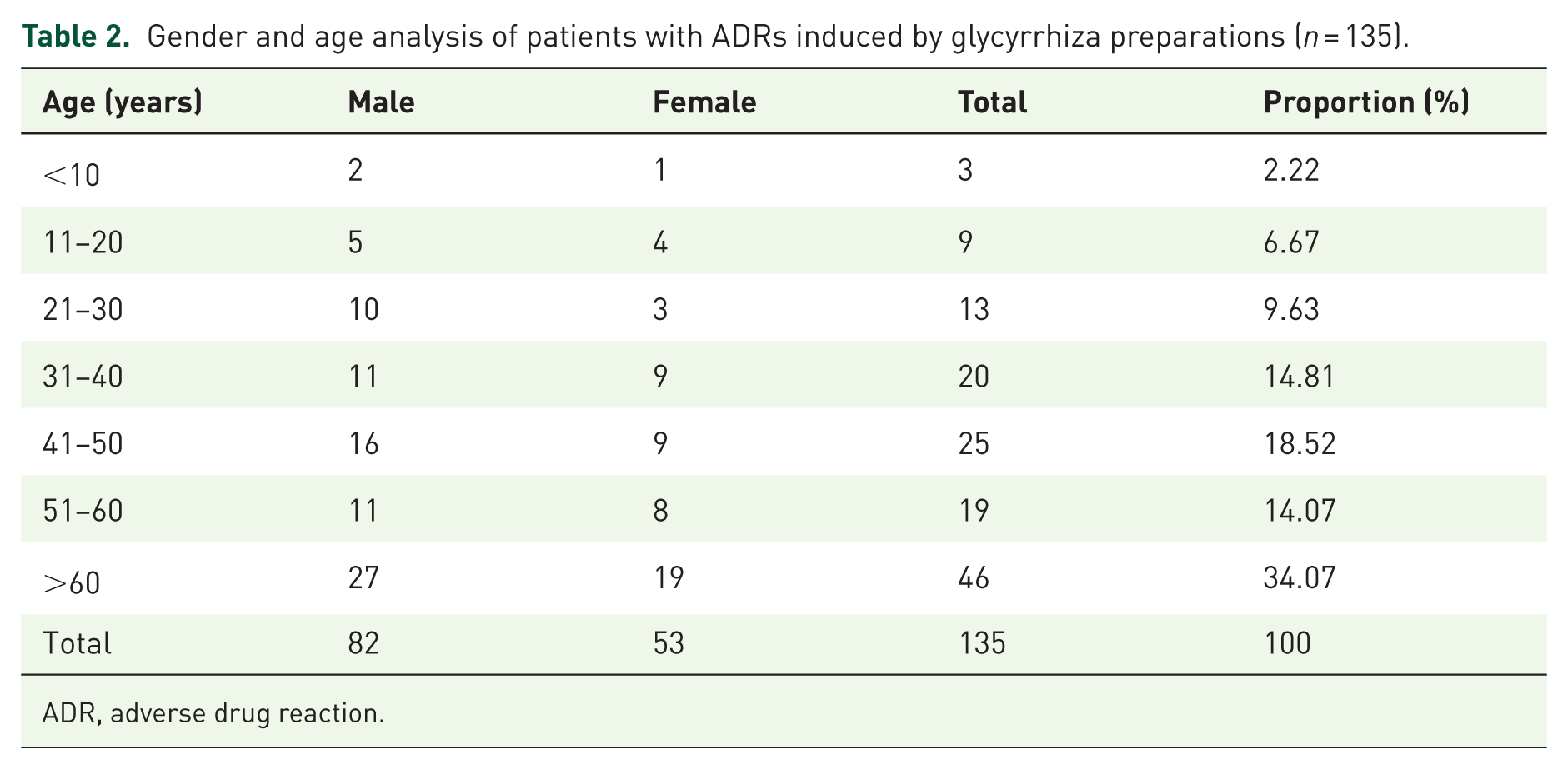
ADR, adverse drug reaction.
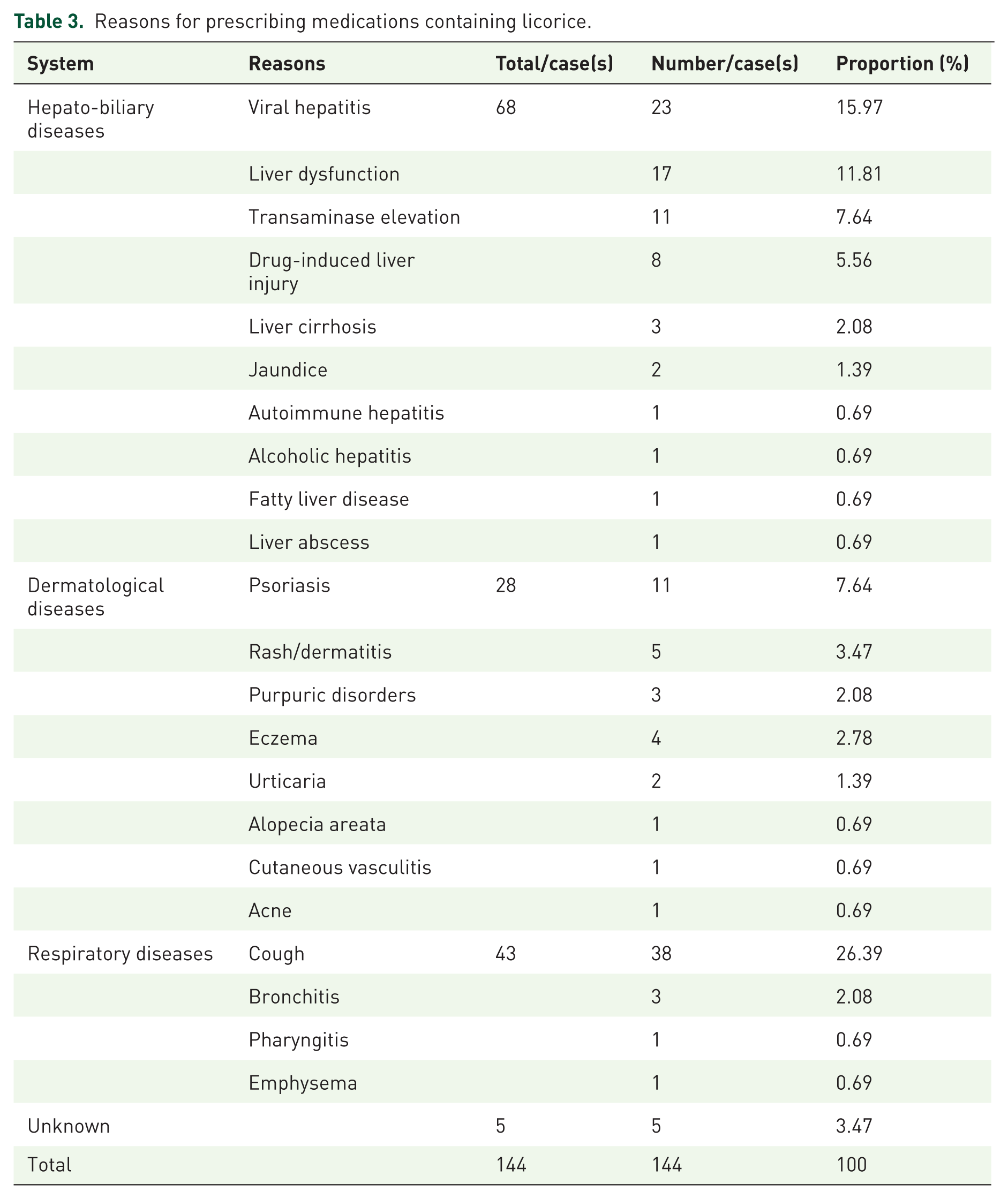
Reasons for patient medication use
The reasons for medication use showed marked clustering, primarily across hepatobiliary diseases, respiratory diseases, and dermatologic diseases (Table 3).
Reasons for prescribing medications containing licorice.
Route of administration and time of onset
The routes of administration were primarily categorized into three types: intravenous infusion (71 cases, 52.59%), oral administration (63 cases, 46.67%), and intramuscular injection (1, 0.74%). Compound licorice oral liquid, compound licorice tablets, compound licorice mixture, and licorice zinc were all administered orally. Diammonium glycyrrhizate, compound monoammonium glycyrrhizate, and magnesium isoglycyrrhizinate were primarily administered via intravenous infusion. Only one case used compound monoammonium glycyrrhizate via intramuscular injection.
By integrating the data of intravenous and oral administration from clinical trials, we analyzed the association between administration route and the risk of ADR occurrence. The results showed that the incidence rate of ADRs with oral administration was 10.31% (86/834), while that with intravenous administration was 3.87% (277/7155). Chi-square test showed a significant association between administration route and glycyrrhiza-containing preparation ADRs (p < 0.05); oral versus intravenous administration had an ADR OR of 0.350 (95% CI: 0.272–0.451), confirming significantly higher ADR risk with intravenous use.
The timing of ADRs varied widely, ranging from immediately after administration to as long as 3 years post-treatment. The highest incidence occurred 1–7 days after drug use, accounting for 33 cases (24.44%; Table 4).
Distribution of time of ADR onset.

ADR, adverse drug reaction.
Regarding the relationship between administration route and the time of onset (Figure 1): Intramuscular injection involved only one case, and it occurred within 10 min. When comparing oral administration with intravenous infusion, both routes showed the highest ADR incidence rate within 1–7 days. For intravenous infusion (68 cases), the proportion of ADRs occurring within ⩽7 days was 89.71% (61/68), which was higher than that of oral administration (49 cases) at 65.31% (32/49). Oral administration had a wider distribution of ADR onset time, ranging from ⩽10 min to >1 year; in contrast, the time of ADR onset for intravenous infusion was concentrated within ⩽1 month.

Time of onset of ADRs among different routes of administration.
Regarding the relationship between different drugs and the time of onset (Figure 2): Drugs with a relatively high proportion of ADRs occurring within ⩽1 h include compound licorice mixture, compound licorice oral liquid, diammonium glycyrrhizinate, and compound monoammonium glycyrrhizinate, while those with ADRs occurring between 1 h and 7 days include compound licorice oral liquid, compound monoammonium glycyrrhizinate, zinc glycyrrhizinate, and magnesium isoglycyrrhizinate, and drugs with ADR onset times exceeding 7 days were primarily compound licorice tablets.

Time of onset of ADRs among different drugs.
ADRs by systems and clinical manifestations
ADRs involved a total of eight organ systems and induced systemic fever reactions, with the endocrine and metabolic system accounting for the highest proportion (51 cases, 30.54%), followed by the allergic-related system (49 cases, 29.34%) and the dermatologic system (22 cases, 11.38%). Clinically, endocrine and metabolic system reactions typically cause hypokalemia, pseudohyperaldosteronism, and hypoglycemia. These manifestations could, in turn, trigger cardiovascular symptoms such as hypertension and arrhythmias, while hypokalemia further led to rhabdomyolysis in the musculoskeletal system. Allergic reactions, including anaphylaxis and anaphylactic shock, were also frequently reported. Furthermore, among the enrolled patients, one case of withdrawal reaction was identified, attributed to compound licorice tablets (Table 5).
ADRs affecting systemic and clinical manifestations.

ADR, adverse drug reaction.
Interestingly, however, observations of clinical trial cohorts revealed that, unlike the findings documented in case reports, the ADRs among patients in these studies predominantly involved the skin, mucous membranes, and their appendages, as well as the digestive system. Distribution of ADRs onset time across different organ systems (Table 6). Allergy-related reactions mostly occurred within 1 h, among which anaphylactic shock usually developed within 10 min. The ADRs occurring in the 1–7 days period were diverse in type, including hypokalemia, PHA, hypertension, and edema-related symptoms. Hypokalemia had a wide distribution of onset times, with cases reported either within 10 min or more than 1 day after administration.
Time of onset of ADRs.
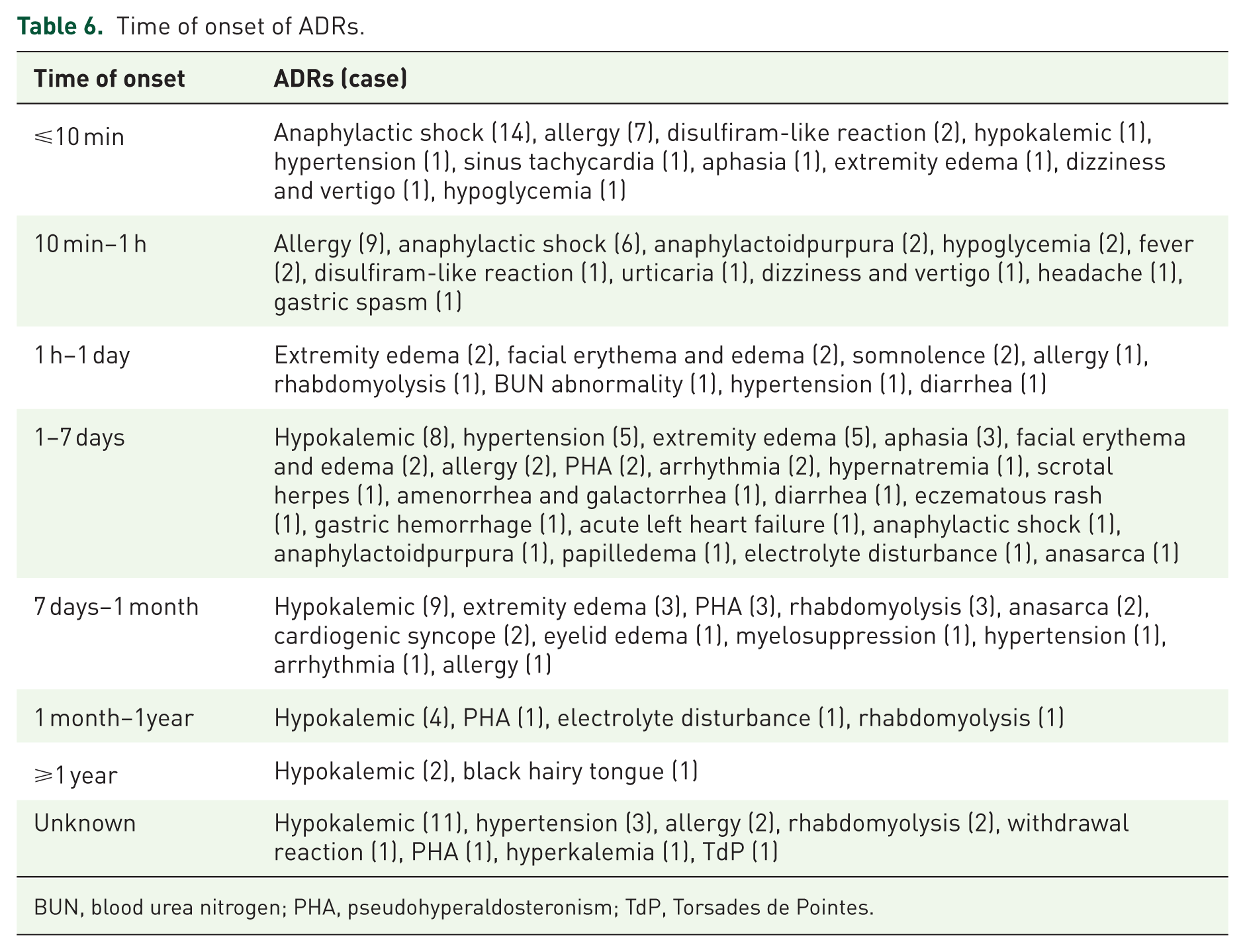
BUN, blood urea nitrogen; PHA, pseudohyperaldosteronism; TdP, Torsades de Pointes.
Severity of ADRs
Among the 135 ADR cases, 43 were mild (31.85%), 37 were moderate (27.41%), and 54 were severe (40.00%). One case resulted in death, 9 which was considered to be associated not only with drug-induced ADRs but also with the patient’s multiple comorbidities and poor baseline health status. The clinical trial subgroup was dominated by mild ADRs, only two cases of serious ADRs were documented.10,11
Treatment approach and outcomes
Regarding treatment approach, 108 patients (80.00%) underwent immediate discontinuation of medication with symptomatic treatment. Twenty-three patients (17.04%) discontinued medication without further intervention. Two patients (1.48%) received only symptomatic treatment and did not discontinue medication. The treatment approach for the remaining seven patients (4.38%) was not specified. Regarding outcomes, regardless of whether medication discontinuation or symptomatic treatment was administered, symptoms ultimately improved in 134 patients (99.26%). Only one patient, who had poor baseline health status, succumbed despite resuscitative efforts following the ADR onset and died on the third day after the ADR occurred (Figure 3).

Time of relief of ADRs among different drugs.
The remission time of ADRs related to the allergy-associated system ranged from 2 min to 7 days. For the endocrine, dermatologic, and cardiovascular systems, the ADRs resolved within several minutes to 1 month. By contrast, the ADRs involving the central and peripheral nervous system, hematological system, and digestive system subsided within 2 h to 7 days.
Combination therapy
The study identified 51 cases (37.78%) receiving combination therapy. Literature analysis identified 10 cases of ADRs clearly attributable to drug interactions, involving 8 distinct medications: azithromycin, nifuratel, methimazole, hydrochlorothiazide, losartan potassium and hydrochlorothiazide, cefoperazone and sulbactam, indapamide, and cilostazol.
Discussion
Licorice metabolites glycyrrhizic acid and glycyrrhetinic acid inhibit 11β-hydroxysteroid dehydrogenase type II (11β-HSDII), 12 a key glucocorticoid-metabolizing enzyme. This blocks cortisol inactivation, elevates renal local cortisol activity, and mediates licorice-related ADRs. Any factor reducing 11β-HSDII activity will further increase ADR risk.
This study evaluated the ADR characteristics of glycyrrhiza-containing Chinese patent medicines based on two complementary data sources: clinical trials and case reports. The two data sources reveal different but complementary dimensions of ADR characteristics: clinical trials can quantify the overall incidence and routine risk of ADRs with standardized medications, while case reports can describe the detailed clinical manifestations, high-risk scenarios, and full progression of rare and severe ADRs. Given the inherent differences in research design between the two types of studies, this study conducted independent descriptive analysis for each data source, respectively, and presented the results in parallel to form a complete safety evidence chain, rather than conducting forced statistical comparisons or integrated analysis across datasets.
Integrated characterization of ADR spectrum from complementary data sources
Clinical trial data provide a population-level, quantitative assessment of ADR risk under standardized clinical trial conditions. In the included clinical trials with unified medication regimens and strict inclusion/exclusion criteria, the overall incidence of ADRs induced by glycyrrhiza-containing preparations was 3.97% for compound glycyrrhizin and 8.24% for diammonium glycyrrhizinate, with a statistically significant difference in relative risk between the two drugs (OR: 2.17, 95% CI: 1.66–2.84, p < 0.05). The most common ADRs in this scenario were mild and transient reactions involving the skin, mucous membrane, and appendage system, as well as the digestive system, which reflects the most common ADR profile of the study drugs in the general population with standardized treatment.
Case report data complement the gaps in clinical trial evidence by detailing the full clinical spectrum, onset characteristics, progression, and outcomes of rare, severe ADRs that are not easily captured in conventional clinical trials. In the included case reports, ADRs involved multiple organ systems, with the highest proportion in the endocrine and metabolic system (30.54%), followed by the allergy-related system (29.34%). These data fully describe the clinical manifestations of severe ADRs such as hypokalemia, pseudohyperaldosteronism, anaphylactic shock, arrhythmias, and rhabdomyolysis, as well as the special high-risk scenarios of these severe events. The two data sources together form a complete ADR profile: clinical trials define the baseline risk of common ADRs in routine clinical practice, while case reports identify the full spectrum of severe and rare ADRs, providing a comprehensive safety reference for clinical medication.
Patient factors contributing to ADRs from licorice preparations
The integrated analysis of the two data sources consistently identifies the high-risk populations for ADRs induced by glycyrrhiza-containing preparations and clarifies the impact of patient-related factors on ADR risk from both population and individual dimensions.
Age
In the included case reports, patients aged over 60 years accounted for 44.44% of all ADR cases, the highest proportion among all age groups. This is mainly due to the age-related decline in 11β-HSDII activity, multiple comorbidities, and impaired physiological reserve in elderly patients, which increase their susceptibility to water and sodium retention and electrolyte disturbances induced by glycyrrhizic acid. 13 Case reports also supplement the clinical details of severe ADRs in elderly patients with multiple comorbidities, which cannot be fully evaluated in clinical trials with strict age and comorbidity restrictions.
Sex
Plasma concentrations of glycyrrhetinic acid depend on gastrointestinal transport rates. Individuals with slower transport rates exhibit higher reabsorption of glycyrrhetinic acid, resulting in elevated plasma concentrations. An epidemiological study by Ploeger et al. 14 demonstrated that women typically have slower gastrointestinal transit than men, making them more susceptible to ADRs from licorice preparations. Du 15 analyzed 75 Japanese patients with licorice-induced pseudoaldosteronism and found that female patients were more prone to this ADR than males. However, both case report and clinical trial data showed a higher proportion of male patients in ADR reports, which could be attributed to the higher prevalence of respiratory and hepatobiliary system diseases (the core indications of glycyrrhiza-containing preparations) in male patients due to unhealthy lifestyle habits (e.g., smoking and alcohol consumption), as confirmed by epidemiological statistics.16 –18
Underlying medical conditions
Patients with underlying conditions therefore exhibit heightened susceptibility, particularly those with cardiovascular disease, liver and renal insufficiency, and endocrine disorders.
Water and sodium retention, increased blood volume, and potassium loss induced by licorice preparations directly elevate blood pressure. In patients with preexisting hypertension or cardiac insufficiency, this may precipitate uncontrolled blood-pressure regulation, causing further vascular endothelial damage and increasing the incidence of drug-induced cardiovascular events.
In patients with hepatic insufficiency, reduced hepatic metabolic rate leads to elevated plasma glycyrrhizin concentrations and prolonged half-life, resulting in drug accumulation in the body. In addition, hepatic insufficiency is often accompanied by hypoalbuminemia, which decreases the binding rate of Glycyrrhizin (GL) to albumin and increases the proportion of free glycyrrhetinic acid, thereby facilitating its binding to the renal 11β-HSDII target to exert pharmacological effects. Yoshino et al. 13 have demonstrated that the incidence of ADRs in patients with hepatic insufficiency is 2–3 times higher than that in healthy individuals, with more severe clinical manifestations. For patients with hepatitis, accumulating evidence has indicated that increased susceptibility to ADRs in chronic inflammatory diseases may be mediated by the inhibition of 11β-HSDII and the stimulation of adrenocorticotropic hormone secretion by inflammatory cytokines. 14
In patients with renal insufficiency, reduced glomerular filtration and diminished potassium excretion capacity lead to compensatory hyperkalemia. Licorice preparations disrupt renal compensatory mechanisms, causing potassium imbalance and ultimately electrolyte disturbances. Renal insufficiency promotes water and sodium retention. Licorice preparations, through their pseudo-aldosterone effect, exacerbate hypertension and edema, further deteriorating renal function. A majority of drug package inserts do not provide clear instructions regarding dosage adjustment for patients with renal dysfunction, which necessitates more prudent medication practices in clinical settings. If patients have underlying conditions such as hypokalemia or hyperadrenocorticism, licorice use may aggravate these primary diseases and heighten drug sensitivity.
This study also documented a case report of ADRs in a hyperthyroidism patient following compound glycyrrhizinate administration. 19 Thyroid hormones (T4, T3) directly increase sodium-potassium pump synthesis and activity. In addition, patients with hyperthyroidism often exhibit hyperinsulinemia, and insulin strongly stimulates sodium-potassium pump activity. Hyperthyroidism is associated with upregulation of β-adrenergic receptors, further activating the sodium–potassium pump and increasing the risk of hypokalemia. Susceptibility to hypokalemia is heightened when combined with licorice preparations. Special caution is warranted in the management of thyrotoxic periodic paralysis, a complication characterized by acute-onset hypokalemia and flaccid muscle paralysis. 20
This study also identified eight patients with documented allergy histories, with allergens including penicillin, sulfonamides, and alcohol. Research indicates that patients with a history of trauma surgery, drug allergies, and elevated monocyte counts face a higher risk of ADRs. 21 Additional studies show that when treated with the same medication, patients with a history of allergies are 1.982 times more likely to experience ADRs than those without such a history. 22
Pharmacological factors contributing to ADRs from licorice preparations
The two data sources complement each other to fully clarify the impact of drug-related factors on ADR risk, from the quantitative assessment of overall risk in clinical trials to the detailed description of special risk scenarios in case reports.
Drug categories
Clinical trial data quantitatively confirm that diammonium glycyrrhizinate has a significantly higher ADR risk than compound glycyrrhizin. This is attributed to the fact that compound glycyrrhizin contains glycine and cysteine hydrochloride, which can attenuate the mineralocorticoid-like effect of glycyrrhizic acid and enhance liver detoxification; in addition, 13 the α-glycyrrhizic acid in diammonium glycyrrhizinate has a stronger inhibitory effect on 11β-HSDII than the β-glycyrrhizic acid in compound glycyrrhizin. 23 Case report data further support that compound glycyrrhizin tablets are the main preparation associated with long-term use-related drug dependence and withdrawal reactions, which are not captured in short-term clinical trials.
Dosage
Clinical trial data confirm that ADRs are generally mild and reversible at conventional therapeutic doses, whereas case reports detail severe clinical consequences resulting from non-standard dosage regimens. High-dose or long-term administration may lead to serious ADRs, including rhabdomyolysis, 24 Torsades de Pointes ventricular tachycardia, 25 and drug dependence, 26 with ADRs progressing gradually from single-system involvement to multi-system organ damage.27,28
Route of administration
Clinical trial data quantitatively compare the risk difference between intravenous infusion and oral administration, showing that intravenous administration is associated with a significantly higher ADR risk (OR: 0.350, 95% CI: 0.272–0.451, p < 0.05) for oral versus intravenous administration. This is mainly due to the 100% bioavailability of intravenous administration, which leads to a sharp increase in plasma drug concentration in a short period. Case report data further complement the onset characteristics of ADRs via different routes: intravenous administration is associated with a higher proportion of acute, severe anaphylactic shock occurring within 10 min after administration, while oral administration has a wider onset time window, with delayed severe ADRs such as hypokalemia and pseudohyperaldosteronism after long-term use.
Drug interactions
Licorice preparations, due to their specific active components, may cause more severe ADRs when used in combination with other medications. Drug–drug interactions include pharmacokinetic and pharmacodynamic interactions. In addition, some ADRs are induced by the non-glycyrrhiza components in compound preparations and concomitant medications. Conventional clinical trials, which typically exclude patients receiving complex concomitant medications, are unable to fully evaluate the risk of drug interactions, and case report data fill this critical research gap.
A subset of ADRs arises from the pharmacodynamic interactions between glycyrrhiza-containing drugs and other medications. Combining indapamide, hydrochlorothiazide, or other thiazide-containing diuretics (e.g., losartan potassium hydrochlorothiazide) with licorice preparations typically increases the incidence and severity of hypokalemia. As thiazide-like diuretics, these drugs promote sodium and potassium excretion by inhibiting sodium reabsorption in the distal renal tubules. The mineralocorticoid-like effects of licorice preparations further accelerate renal potassium excretion. The synergistic effect on potassium ion excretion leads to excessive potassium loss, causing hypokalemia and potentially severe ADRs such as arrhythmias.
Azithromycin blocks cardiac human Ether-à-go-go-Related Gene (hERG) potassium channels, inhibiting potassium efflux and delaying myocardial repolarization, thereby inducing arrhythmias manifested as QT interval prolongation on electrocardiograms. This mechanism explains the increased arrhythmia risk associated with azithromycin, other macrolides, and fluoroquinolones. When these drugs are co-administered with licorice preparations, licorice-induced hypokalemia further exacerbates myocardial electrophysiological disturbances, leading to more pronounced QT prolongation and potentially triggering life-threatening arrhythmias such as Torsades de Pointes ventricular tachycardia, which may ultimately be fatal.
Licorice preparations, due to their specific active components, may cause more severe ADRs when used in combination with other medications.
ADRs induced by other components contained in compound preparations. Some licorice preparations contain alcohol, such as compound licorice oral liquid and compound licorice mixture. When used concurrently with cephalosporin or nitroimidazole antibiotics, these drugs inhibit hepatic aldehyde dehydrogenase activity. The acetaldehyde produced during alcohol metabolism cannot be promptly metabolized and accumulates, leading to facial flushing, headache, nausea, palpitations, and dyspnea—a “disulfiram-like reaction.” This study identified three reported cases of disulfiram-like reactions caused by antibiotic combinations: one involved co-administration with cefoperazone/sulbactam, 29 and nifuratel. 30 Beyond these two classes, commonly used sulfonylurea and biguanide hypoglycemic agents may also induce disulfiram-like reactions when combined with alcohol-containing medications.
ADRs are induced by pharmacokinetic interactions. This study 31 reported a case in which cilostazol combined with compound glycyrrhizin induced pseudoaldosteronism and palpitations. Glycyrrhetinic acid and its metabolite 3-monoglucuronyl-glycyrrhetinic acid (3MGA) have serum albumin binding rates exceeding 90%, with 3MGA up to 99%, while cilostazol also exhibits high plasma protein binding. When used in combination, they compete for serum albumin, increasing free 3MGA and thereby ADRs. Research indicates that cilostazol increases intracellular cyclic adenosine monophosphate (cAMP) concentrations by inhibiting phosphodiesterase IIIa activity in cardiomyocytes, accelerating sinoatrial node automaticity and leading to tachycardia, palpitations, or even arrhythmias. 32 This mechanism may also contribute to an increased incidence or severity of cardiovascular ADRs when the two drugs are used in combination.
Prevention and management of ADRs
Based on the integrated findings of the two data sources, we put forward targeted recommendations for the clinical prevention and management of ADRs induced by glycyrrhiza-containing Chinese patent medicines. In routine clinical practice, the dosage, frequency, and treatment duration should be strictly controlled in accordance with the package insert, and off-label high-dose or long-term use should be avoided; intravenous administration should be used with caution, and patients should be closely monitored during infusion for acute allergic reactions. For high-risk populations, a detailed medical history inquiry should be conducted before administration, especially for elderly patients, those with hepatic/renal insufficiency, hypertension, hyperthyroidism, or a history of drug allergy; serum potassium, blood pressure, and creatine kinase should be monitored regularly during treatment. Concomitant use with potassium-depleting diuretics, drugs that prolong the QT interval, and high plasma protein-binding drugs should be avoided as much as possible.
For the management of ADRs that occur, timely drug withdrawal is the core measure for most ADRs. For acute allergic reactions, the drug should be discontinued immediately, anti-allergic treatment should be given, and epinephrine should be injected for severe anaphylactic shock. For hypokalemia and pseudohyperaldosteronism, drug withdrawal plus potassium supplementation and symptomatic antihypertensive treatment with spironolactone can achieve symptom relief in most patients. For severe complications such as rhabdomyolysis, fluid replacement and urine alkalization should be given in addition to drug withdrawal. The vast majority of ADRs can be resolved after timely drug withdrawal and targeted symptomatic treatment.
Limitations of the study
(1) Geographical bias may exist as all included literature was from China, limiting the generalizability of the findings. (2) The quality of the included analytical studies was relatively low, which may introduce potential selection bias or performance bias. (3) This study was limited to descriptive analysis of ADR distribution characteristics and cannot fully establish definitive causal relationships between related risk factors and ADR occurrence. (4) Although this study presents ADR data from case reports and clinical trials in parallel, the two types of studies have inherent differences in research design, leading to significant heterogeneity in population, medication regimen, and ADR monitoring methods between the two data sources. These differences make it impossible to perform a true integrated analysis of the two datasets. For this reason, we conducted only an independent analysis and a complementary presentation of the two data sources, without forced statistical comparisons.
Conclusion
In this study, a total of 135 cases of ADRs associated with glycyrrhiza-containing drugs were included, with relevant data from case series analyses and RCTs integrated. The results showed that male patients aged 60 years and above, those with underlying diseases such as hepatic or renal insufficiency or hypertension, and individuals with a history of drug allergy accounted for a relatively higher proportion of ADR cases. The risk of ADRs was significantly increased by supranormal dosage administration, intravenous administration route, and concomitant use with drugs prone to inducing electrolyte disturbances, hypertension, or arrhythmia, as well as drugs with high plasma protein-binding rates. ADRs induced by glycyrrhiza-containing Chinese patent medicines involved multiple organ systems and were closely correlated with both patient-related and drug-related factors. Specifically, mild ADRs mostly affected the skin, mucous membranes, and appendages, as well as the digestive system, whereas severe cases could induce symptoms involving the endocrine system, allergic reactions, and cardiovascular systems. The vast majority of ADRs were alleviated after drug withdrawal combined with symptomatic treatment; however, clinically, it is still necessary to conduct a detailed medical history inquiry, take into account the patients’ baseline health status, and implement individualized treatment regimens.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261446460 – Supplemental material for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials
Supplemental material, sj-docx-1-taw-10.1177_20420986261446460 for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials by Ziyi Yu, Danwei Wu, Yitong Xie, Lu Mao, Ziwei Jiang, Jiancun Zhen and Wei Zhang in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986261446460 – Supplemental material for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials
Supplemental material, sj-docx-2-taw-10.1177_20420986261446460 for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials by Ziyi Yu, Danwei Wu, Yitong Xie, Lu Mao, Ziwei Jiang, Jiancun Zhen and Wei Zhang in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-3-taw-10.1177_20420986261446460 – Supplemental material for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials
Supplemental material, sj-docx-3-taw-10.1177_20420986261446460 for Adverse drug reactions associated with glycyrrhiza-containing Chinese patent medicines: a literature-based analysis of individual case reports and clinical trials by Ziyi Yu, Danwei Wu, Yitong Xie, Lu Mao, Ziwei Jiang, Jiancun Zhen and Wei Zhang in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.