
Abstract
Burosumab is a monoclonal antibody targeting fibroblast growth factor 23 (FGF23) and is approved for the treatment of X-linked hypophosphatemia. Its use during pregnancy has not been studied, and fetal exposure may affect neonatal mineral metabolism. We report a neonate exposed to Burosumab throughout gestation who developed prolonged phosphate retention, suppressed parathyroid hormone, and transient hypercalcemia after birth. Serial biochemical monitoring demonstrated persistently elevated tubular phosphate reabsorption and low urinary phosphate excretion beyond the early neonatal period, consistent with sustained pharmacodynamic effects of FGF23 inhibition. These abnormalities gradually resolved over time, and the infant remained clinically well with normal growth and no evidence of nephrocalcinosis. Genetic testing excluded the familial pathogenic PHEX variant, confirming that the observed phenotype was due to transient pharmacologic exposure rather than intrinsic disease. This case demonstrates that antenatal Burosumab exposure can result in prolonged postnatal alterations in calcium–phosphate homeostasis. Careful biochemical monitoring is warranted in exposed infants, and continuation of Burosumab beyond mid-pregnancy should be approached with caution.
Plain language summary
Burosumab is a medication used to treat X-linked hypophosphatemia (XLH), a rare inherited disease that causes weak bones and low phosphate levels. It works by blocking a natural hormone called fibroblast growth factor 23 (FGF23), which normally lowers phosphate and vitamin D levels in the body. Although burosumab is effective for both children and adults, it has never been formally studied in human pregnancy, and it is unclear whether the drug crosses the placenta or affects the baby after birth. We describe the first known case of a baby exposed to burosumab throughout pregnancy. The mother, who has XLH, continued treatment to control severe bone pain and fatigue. The baby was born healthy at term but showed temporary high calcium levels and strong phosphate retention for several weeks after birth. These findings suggest that burosumab was transferred from the mother to the baby and remained active in the baby’s body after delivery. By six months of age, all laboratory values had returned to normal, and the baby remained well. This case shows that burosumab can have lasting effects on the newborn, even if the last dose is given before delivery. While no harm was observed in this infant, the results highlight the need for caution in future pregnancies, careful biochemical monitoring of newborns, and more research to guide the safe use of burosumab in women of childbearing age.
Keywords
Introduction
Burosumab is a fully human monoclonal IgG1 antibody directed against fibroblast growth factor 23 (FGF23), approved for the treatment of X-linked hypophosphatemia (XLH) in adults and children aged ⩾6 months.1,2 By binding and neutralizing circulating FGF23, Burosumab restores renal phosphate reabsorption and increases serum 1,25-dihydroxyvitamin D.3,4 Its use during pregnancy has not been studied in clinical trials. In preclinical studies, continuous FGF23 blockade during gestation in cynomolgus monkeys led to fetal nephrocalcinosis and soft-tissue calcifications, raising concern about potential developmental toxicity.5,6 Human IgG1 antibodies cross the placenta modestly during the second trimester and at increasing rates in the third trimester, allowing for progressive fetal exposure.7,8 The extent and persistence of pharmacologic activity in exposed neonates have not previously been characterized. We describe the first case of a neonate with prolonged postnatal phosphate retention and transient non-parathyroid hormone (PTH)-mediated hypercalcemia following continuous maternal Burosumab therapy throughout pregnancy, indicating sustained biologic activity after birth and delayed neonatal clearance. This case report was prepared in accordance with the CARE (CAse REport) guidelines (Supplemental Material). 9
Case presentation
The mother, with genetically confirmed XLH (a ~4.36 kb deletion within the PHEX gene [NM_000444.5] encompassing exon 2 with breakpoints in introns 1 and 2 and a minimal deletion boundary defined by aCGH at chrX:22,056,250–22,060,621 [GRCh37/hg19]), continued Burosumab therapy throughout pregnancy due to significant bone pain and fatigue experienced on conventional therapy after discontinuing Burosumab in her previous pregnancy. Following extensive counseling regarding potential fetal risks and the absence of safety data for Burosumab use during pregnancy, she reduced the Burosumab dose from 30 to 20 mg every 2 weeks after 26 weeks’ gestation while still experiencing good disease control. The final dose was administered on August 29, 2025, and delivery occurred on September 3, 2025. The infant was born at home via normal vaginal delivery at 38 weeks’ gestation, weighing 3.5 kg, in good clinical condition, without need for resuscitation.
Physical examination and investigations
Initial evaluation on day 6 of life showed a well-appearing newborn female with a blood pressure of 76/54 mmHg (≈95th percentile). Physical examination was normal, including a length of 50.2 cm (47th percentile), weight 3.595 kg (70th percentile), and head circumference of 36 (75th percentile). Laboratory values revealed serum phosphate 1.85 mmol/L (normal 1.30–2.60 mmol/L), calcium 2.91 mmol/L (normal 1.89–2.59 mmol/L), ALP 201 U/L (normal 83–248 U/L), PTH <0.6 pmol/L (normal 1.8–7.9 pmol/L), and creatinine 26 µmol/L (normal <53 µmol/L). Fractional phosphate excretion was 1.5%, tubular reabsorption of phosphate (TRP) 98.5% (normal 85%–95%), and tubular maximum phosphate reabsorption per unit of glomerular filtration rate (TmP/GFR) 1.82 mmol/L (normal 1.02–2.00 mmol/L), consistent with maximal tubular phosphate reabsorption. At no time was there any hypercalciuria. A skeletal survey was normal, without evidence of skeletal dysmorphology or calcifications.
A follow-up at 6 weeks of life revealed a thriving baby, without concerns for her developmental or feeding statuses. Unfortunately, no anthropometry was obtained at this time. Laboratory evaluations confirmed persistent suppression of urinary phosphate excretion (FEp 0.5%, TmP/GFR 2.16 mmol/L (normal 1.02–2.00 mmol/L)) and normalization of serum calcium (2.59 mmol/L (normal 2.25–2.75 mmol/L)) and PTH (1.1 pmol/L (normal 1.8–7.9 pmol/L)). At 10 weeks of age, serum phosphate remained within the high–normal range (1.89 mmol/L) with continued evidence of phosphate retention (TmP/GFR 1.87 mmol/L; TRP 98.9%), while fractional phosphate excretion remained <1%. PTH had normalized (1.6 pmol/L). These findings suggested ongoing Burosumab-related renal handling effects beyond the early neonatal period. Renal ultrasound remained normal (without calcifications), though mild aortic dilation was noted on the first echocardiogram (also in the absence of calcifications). There was no evidence of subcutaneous calcifications on physical examination. Overall, the biochemical course supported ongoing Burosumab activity in the neonate up to 6 weeks postpartum.
Key serial biochemical findings are summarized in Table 1 at 6 days of life, as well as up to 26 weeks of life. Figure 1 depicts the longitudinal changes of serum calcium, intact PTH, serum phosphate, TmP/GFR, TRP, and urinary calcium/creatinine ratio. Unfortunately, 1,25-hydroxyvitamin D levels were requested but not successfully acquired in this infant due to a lack of sufficient quantities at procurement (except at 6 weeks of life, when the level was within the normal range at 100 pmol/L). At 6 months of age, all initially abnormal laboratory parameters had normalized, and there was still no evidence of nephrocalcinosis. Genetic testing performed at that time did not identify the familial pathogenic PHEX variant. A heterozygous variant of uncertain significance (c.*231A>G) was identified in a non-coding region of PHEX, without established functional or clinical relevance. In the context of complete biochemical normalization and normal clinical development without signs of skeletal abnormalities, these findings suggested that the infant was unaffected by XLH.
Serial biochemical parameters in the newborn following antenatal Burosumab exposure.
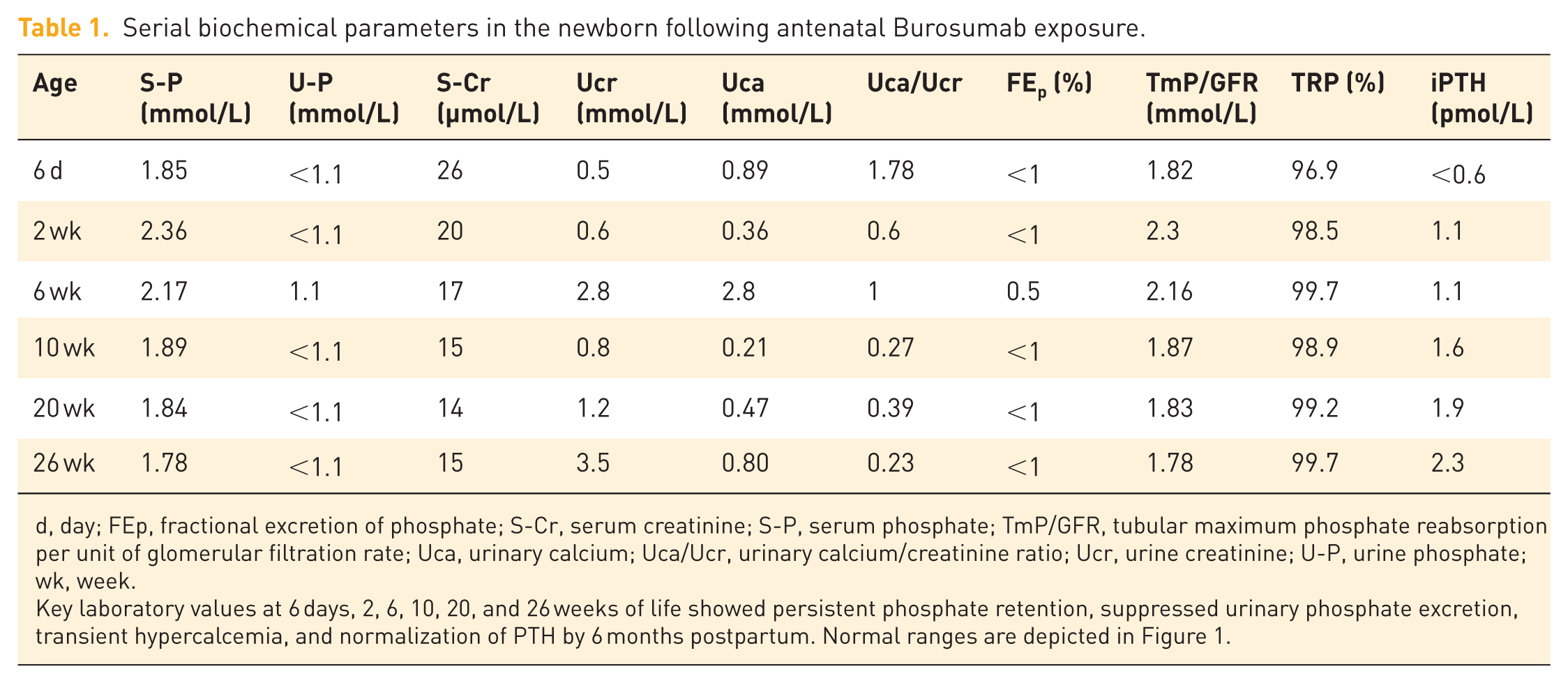
d, day; FEp, fractional excretion of phosphate; S-Cr, serum creatinine; S-P, serum phosphate; TmP/GFR, tubular maximum phosphate reabsorption per unit of glomerular filtration rate; Uca, urinary calcium; Uca/Ucr, urinary calcium/creatinine ratio; Ucr, urine creatinine; U-P, urine phosphate; wk, week.
Key laboratory values at 6 days, 2, 6, 10, 20, and 26 weeks of life showed persistent phosphate retention, suppressed urinary phosphate excretion, transient hypercalcemia, and normalization of PTH by 6 months postpartum. Normal ranges are depicted in Figure 1.
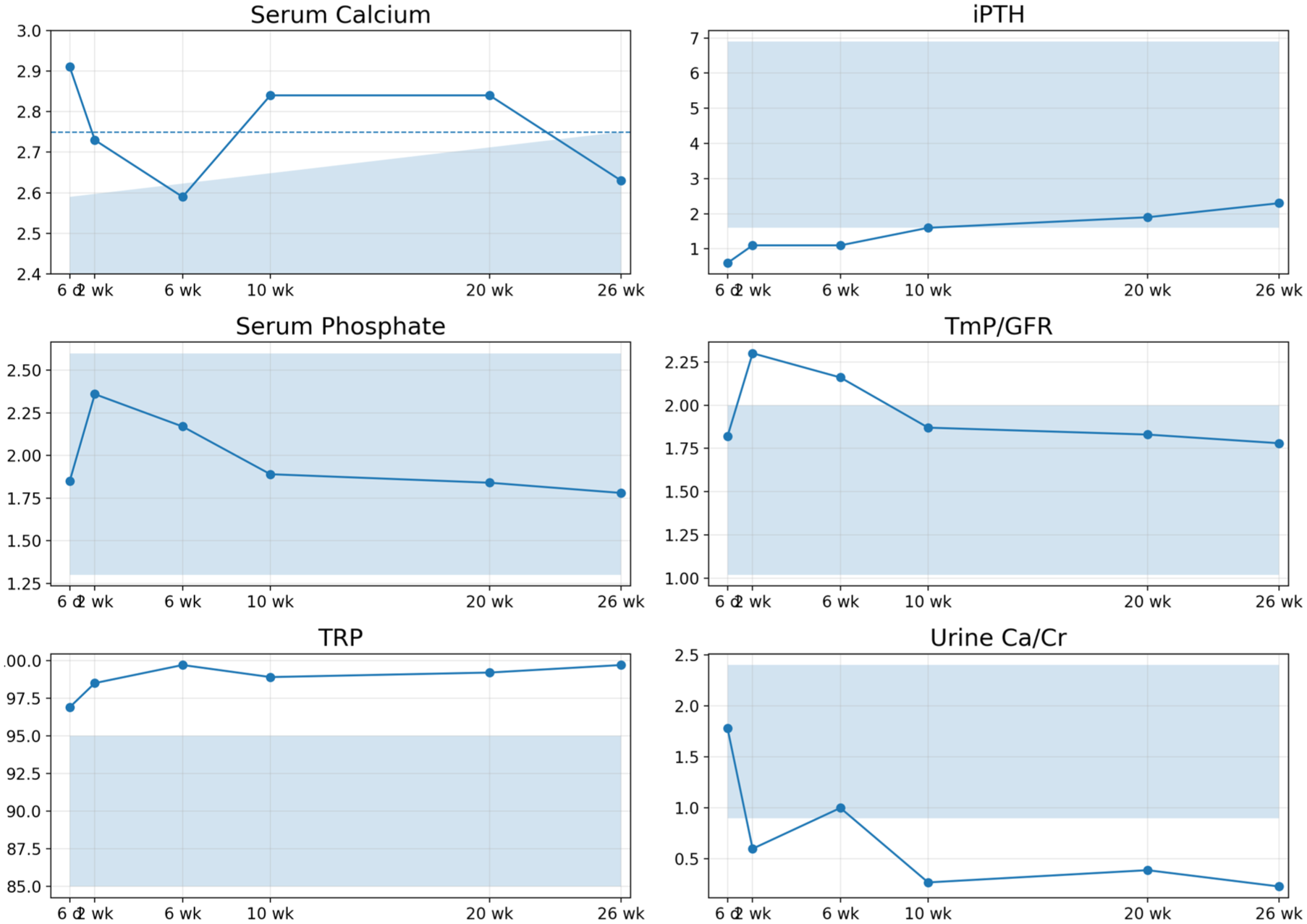
Evolution of serum calcium (orange), intact parathyroid hormone (purple), serum phosphate (blue), and TmP/GFR (red), TRP (green), and urinary calcium/creatinine ratio (bluish green) from 6 days to 6 weeks of life; shaded areas denote neonatal reference ranges.
Discussion
The persistence of suppressed urinary phosphate and elevated TmP/GFR 20 weeks after birth is consistent with ongoing Burosumab activity. With a terminal elimination half-life of approximately 19 days for Burosumab, 3 and given the well-described FcRn-mediated recycling mechanism that extends IgG half-life from days to weeks, 10 it is plausible that not all Burosumab had been cleared from the baby. Preclinical studies in cynomolgus monkeys demonstrated transplacental transfer of burosumab, with measurable drug levels persisting in neonatal circulation for up to 6 weeks postpartum (corresponding to approximately 20%–25% of maternal serum concentrations). 6 However, no comparable data are available in humans. The complete normalization of biochemical parameters by 6 months of age, together with the absence of the known pathogenic familial PHEX variant, confirmed that the observed phenotype represented a transient pharmacologic effect rather than an intrinsic disorder of phosphate metabolism.
The non-PTH-mediated hypercalcemia at 6 days of life, albeit transient, was also in line with Burosumab exposure, likely due to a spike in 1,25-dihydroxyvitamin D. Unfortunately, due to insufficient quantity, we were not able to obtain a 1,25-dihydroxyvitamin D level in this infant except at 6 weeks of life (at which time it was within the normal range). We therefore postulate, based on the known mechanism of action of Burosumab (release of inhibition on renal 1α-hydroxylase) together with the observed hypercalcemia but no hypercalciuria (Figure 1), that 1,25-dihydroxyvitamin D levels were elevated transiently in the early neonatal period. Vitamin D metabolites measured during follow-up were within reference ranges; however, in the context of suppressed PTH and high tubular phosphate reabsorption, a normal 1,25-dihydroxyvitamin D level may be physiologically inappropriate and compatible with partial FGF23 pathway disinhibition.
To place these findings in context, it is important to distinguish biochemical effects observed following antenatal exposure from those reported after postnatal initiation of Burosumab therapy. Interestingly, our prior work also identified hypercalciuria (along with new-onset nephrocalcinosis) in a small subset of children with XLH (2/13) who had recently initiated Burosumab. In this series, the children experienced a significant drop in their serum PTH levels within 4–8 weeks following transition from conventional therapy to Burosumab. 11 whereas on conventional therapy, these children had no evidence of nephrocalcinosis, suppressed PTH or elevated serum or urinary calcium levels. 11 Although the fact that their normal, pre-Burosumab renal ultrasound was obtained several months before the first Burosumab dose precludes absolute certainty that the nephrocalcinosis developed as a direct consequence of Burosumab therapy, it is nevertheless interesting to note that we observed non-PTH-mediated hypercalciuria (with nephrocalcinosis) in another context. Together, these observations speak to the clinical importance of the release of inhibition on renal 1α-hydroxylase brought about by Burosumab. While these postnatally treated children differ fundamentally from the present case in timing and developmental context, the shared biochemical features underscore the central role of FGF23 pathway modulation in calcium–phosphate homeostasis.
Clinical significance and management considerations
The biochemical abnormalities observed in this infant were interpreted in the context of established neonatal endocrine and nephrology practice. Although transient hypercalcemia was documented, serum calcium concentrations remained below thresholds typically associated with acute toxicity or mandating pharmacologic intervention in asymptomatic neonates. The infant exhibited no clinical features attributable to hypercalcemia, including feeding intolerance, irritability, dehydration, cardiac manifestations, or impaired growth. Renal function remained stable, and there was no clinical or biochemical evidence of nephrocalcinosis or other end-organ complications during follow-up.
Given the absence of symptoms, preserved renal function, and the expectation of gradual physiological adaptation, a conservative management strategy with close biochemical surveillance was adopted rather than active intervention. This approach is consistent with standard neonatal practice, in which asymptomatic biochemical perturbations are monitored while avoiding unnecessary treatment that may disrupt ongoing mineral homeostasis. The prolonged nature of the biochemical signal, however, underscores the importance of structured follow-up in infants with antenatal exposure.
The adverse drug reaction was reported to the manufacturer in accordance with pharmacovigilance requirements. A targeted search of publicly available pharmacovigilance databases, including FAERS and VigiBase summaries, did not identify comparable neonatal cases with detailed biochemical follow-up. This absence underscores the novelty and clinical relevance of the present report.
Consideration of alternative explanations for phosphate retention and suppressed PTH
Several alternative explanations for suppressed PTH levels and phosphate retention in early life were considered, including normal neonatal adaptation of mineral metabolism, maternal vitamin D status, feeding-related factors, and transient renal immaturity. Transitional alterations in calcium–phosphate handling are well described in the immediate neonatal period; however, these changes typically resolve within the first weeks of life as renal tubular function and endocrine regulation mature.
In the present case, the degree and persistence of phosphate retention—characterized by near-complete tubular phosphate reabsorption (TRP consistently approaching 99%), fractional phosphate excretion below 1%, and elevated TmP/GFR—extend beyond what is usually observed during physiological neonatal adaptation. Importantly, these findings persisted beyond the early neonatal period, including at 10 weeks of age, when transitional mineral handling would be expected to have normalized.
Suppressed or low-normal PTH concentrations in this context are likewise atypical for common neonatal conditions associated with hyperphosphatemia. When considered together with the temporal relationship to antenatal exposure and the prolonged biochemical trajectory, the observed pattern is less consistent with nonspecific neonatal physiology and more compatible with sustained alteration of FGF23-mediated phosphate regulation. While causality cannot be definitively established in a single case, the findings support biological plausibility for prolonged pharmacodynamic effects following antenatal exposure.
Given the mechanistic effects of Burosumab on renal phosphate handling, isolated serum measurements may be insufficient to detect prolonged pharmacodynamic activity. We therefore propose a structured monitoring framework (Box 1) that includes paired serum and urine measurements, allowing calculation of TRP and TmP/GFR. These indices provide critical insight into renal phosphate handling and may help distinguish transient neonatal adaptation from sustained effects following antenatal Burosumab exposure.
Suggested monitoring framework for infants with antenatal burosumab exposure.
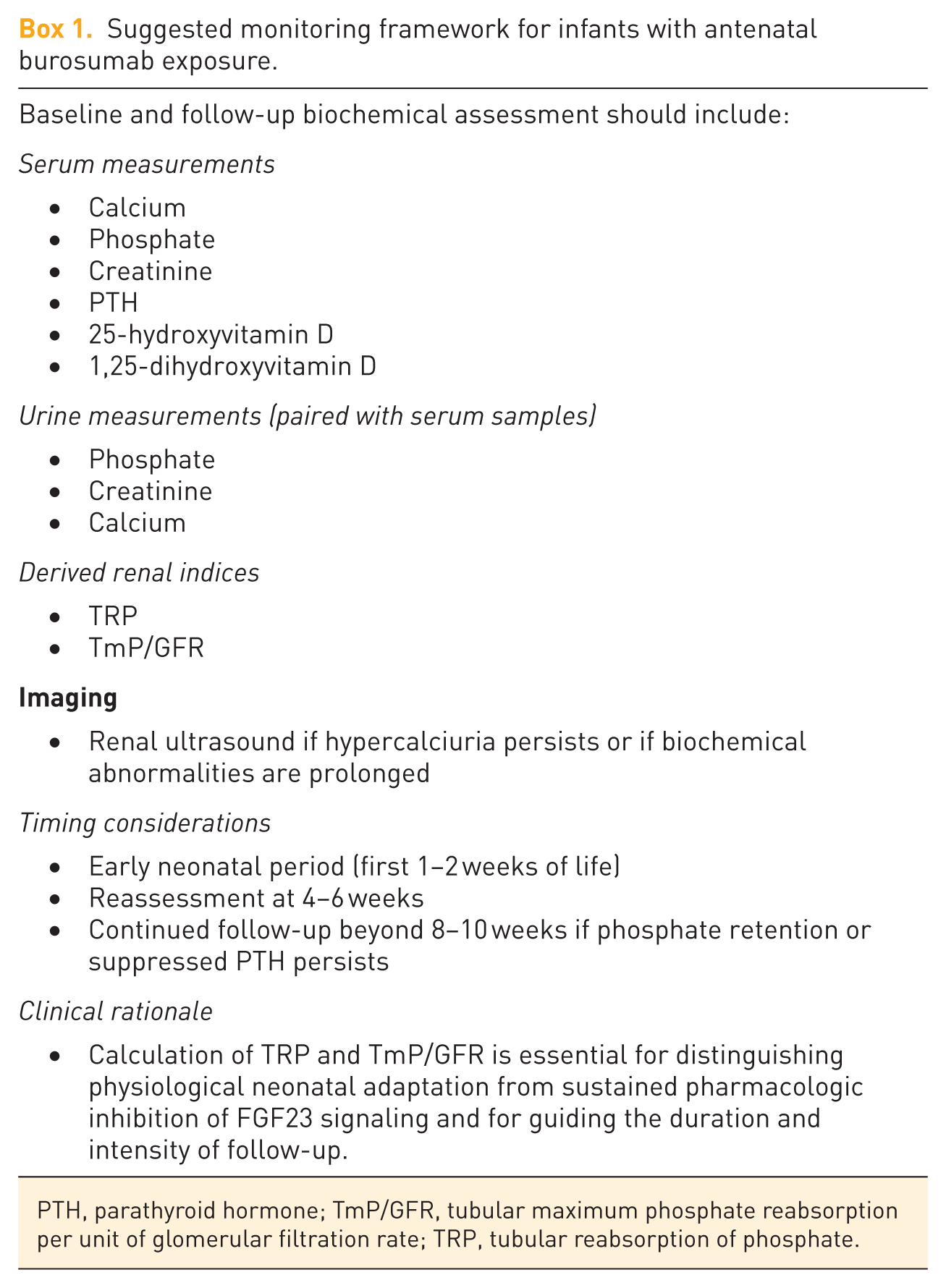
PTH, parathyroid hormone; TmP/GFR, tubular maximum phosphate reabsorption per unit of glomerular filtration rate; TRP, tubular reabsorption of phosphate.
We propose that this case demonstrates placental transfer of active drug, neonatal pharmacologic effect, and delayed normalization of biochemical parameters of bone and mineral ion metabolism similar to what was described in preclinical models. 6 Given that the maternal dose was administered only 5 days before delivery, ongoing neonatal biochemical effects are pharmacologically plausible within the known elimination half-life of Burosumab. On the other hand, cardiac, subcutaneous, and renal calcifications were absent, and there was no evidence of growth restriction or skeletal dysmorphology. Recent consensus guidance explicitly discourages continuation of Burosumab beyond 20 weeks’ gestation due to uncertain fetal safety.12,13 The management guidelines and systematic review further highlight knowledge gaps in long-term safety, particularly in reproductive contexts.12,13
The complete normalization of biochemical parameters by 6 months of age, in conjunction with the absence of a pathogenic PHEX variant, confirms that the observed phenotype represents a transient pharmacologic effect rather than an intrinsic disorder of phosphate metabolism.
Conclusion
Continuation of Burosumab beyond 20 weeks of gestation may lead to prolonged phosphate retention and hypercalcemia in the newborn. Our data discourage the continuation of Burosumab treatment throughout pregnancy because it crosses the placenta and phosphate retention persists for at least 10 weeks after delivery.
Learning points
Burosumab crosses the placenta in late pregnancy, leading to sustained neonatal biochemical effects.
Prolonged phosphate retention and transient hypercalcemia may occur postpartum.
Monitoring of neonatal mineral metabolism is essential after antenatal exposure.
Caution regarding maternal continuation of Burosumab beyond 20 weeks of gestation is meritorious given the biochemical abnormalities observed in this report.
Pharmacovigilance reporting remains paramount for the use of biologics during pregnancy.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261450017 – Supplemental material for Prolonged neonatal phosphate retention and transient hypercalcemia following antenatal Burosumab exposure: a pharmacovigilance alert
Supplemental material, sj-docx-1-taw-10.1177_20420986261450017 for Prolonged neonatal phosphate retention and transient hypercalcemia following antenatal Burosumab exposure: a pharmacovigilance alert by Guido Filler, Funmbi Babalola, Andrea Cowan, Tayyab Khan and Leanne Ward in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We are grateful to the patient’s mother for sharing her experience to help expand medical knowledge in an area with limited existing data.
Declarations
Patient perspective
The mother noticed substantially fewer XLH-related symptoms compared to the previous pregnancy when she stopped the Burosumab injections at 20 weeks of gestation and reported a lot more energy. A formal offspring perspective was not included, as the infant is not of an age to provide subjective input.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.