
Abstract
Background:
Routinely collected electronic healthcare data have created new opportunities for active, near real-time post-marketing drug safety surveillance. Sequential analysis offers a natural framework for periodic signal detection as data accrue and may facilitate earlier identification of emerging safety concerns. However, its application in drug safety surveillance has not been comprehensively characterized.
Objective:
To systematically identify and characterize empirical applications and methodological developments of sequential analysis for safety signal detection in post-marketing drug surveillance using electronic healthcare data and to summarize key methodological approaches and evidence gaps in the literature.
Eligibility criteria:
Eligible studies included empirical observational studies that applied sequential analyses to periodically monitor prespecified drug-outcome pairs, and methodological studies that proposed or evaluated sequential approaches for post-marketing surveillance.
Sources of evidence:
Six databases (PubMed, EMBASE, the Cochrane Library, CNKI, WanFang, and VIP) were searched from inception to 21 July 2025.
Charting methods:
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews. Two reviewers independently screened studies and extracted data using a standardized form. Findings were mapped to predefined analytical dimensions and synthesized narratively.
Results:
Forty-six studies were included, comprising 20 empirical observational studies and 26 methodological studies. All empirical studies were conducted in high-income countries, predominantly the United States, and 80% were pilot or feasibility assessments. Electronic health/medical records and administrative claims were the primary data sources. Considerable methodological heterogeneity was observed in study designs, analytical frequency, and sequential approaches. Two broad paradigms were identified: sequential testing and sequential risk estimation. Methodological studies were largely motivated by challenges inherent to observational settings, particularly confounding control.
Conclusion:
Despite growing interest and methodological development, the application of sequential analysis in post-marketing drug safety surveillance remains limited. Future work should prioritize stronger approaches to confounding, clearer implementation standards, and better integration of sequential monitoring into routine pharmacovigilance practice.
Plain language summary
After medicines are approved, it is important to continue monitoring their safety using real-world healthcare data. Sequential analysis is a useful approach that allows researchers to repeatedly check for potential safety problems as new data become available, which may help detect risks earlier than traditional methods. However, it is not clear how this approach has been used in practice.
We carried out a scoping review to understand how sequential analysis has been used for post-marketing drug safety surveillance and to identify important research gaps. We searched six databases and included both real-world studies that used sequential analysis to monitor specific drug-outcome pairs and methodological studies that developed or evaluated these approaches.
We included 46 studies. Most real-world studies were from high-income countries, especially the United States, and many were pilot or feasibility studies rather than routine surveillance programs. The main data sources were electronic medical records and administrative claims databases. We found wide differences across studies in how often data were checked, which study designs were used, and which sequential methods were applied. Two main approaches were used: repeated statistical testing and continuous estimation of risk over time. Many methodological studies focused on problems that are especially important in observational setting, such as confounding.
Although interest in sequential analysis is increasing, its use in drug safety monitoring is still limited. The review identifies important barriers and highlights priorities for future methodological and operational development before these approaches can be more widely used in routine pharmacovigilance practice.
Keywords
Introduction
Adverse drug events (ADEs) pose a major threat to patient safety worldwide and may lead to serious outcomes, including hospitalization, disability, and even death.1,2 This challenge is equally pressing in China. According to the National Medical Products Administration (NMPA), approximately 2.6 million ADE reports were submitted annually in recent years, with an increasing proportion classified as serious. 3 In addition, ADEs account for a substantial proportion of hospital admissions, with estimates ranging from 0.16% to 15.7%, depending on study design, population, and detection methods. 4 Higher risks have been consistently observed among vulnerable populations, particularly pediatric and elderly patients.5,6 These findings underscore the urgent need for more effective and timely drug safety surveillance strategies. Post-marketing drug safety surveillance plays a critical role in the continuous evaluation of risks after a medication enters into routine clinical practice. Traditionally, such surveillance has relied primarily on spontaneous reporting systems, such as the Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) or the National Adverse Drug Reaction Monitoring System (NADRMS) in China, through which healthcare professionals, pharmaceutical companies, and patients voluntarily report suspected ADEs to regulatory authorities. Although these systems provide broad population coverage and remain indispensable for identifying rare or serious adverse events, they are inherently limited by substantial underreporting, reporting bias, and the lack of appropriate denominator data.7,8 These limitations constrain the timely and comprehensive identification of potential safety signals.
While signal detection methods based on spontaneous reporting continue to evolve, the increasing availability of large-scale electronic healthcare databases has significantly expanded the data resources for post-marketing drug safety surveillance. These databases typically encompass diverse data sources, including electronic health records (EHRs), administrative claims, disease registries, and pharmacy dispensing records, capturing detailed longitudinal information on patient demographics, diagnoses, procedures, and medication exposures across millions of individuals in real-world setting. 9 For instance, the Clinical Practice Research Datalink (CPRD) provides anonymized primary care medical records from 674 practices in the United Kingdom, covering over 11.3 million individuals, and has been widely used to investigate drug utilization and safety in routine clinical practice. 10 Similarly, administrative claims databases such as Medicare in the United States, as well as nationwide health insurance databases in countries such as Denmark and South Korea, have enabled large-scale population-based studies, particularly for evaluating rare or long-term drug safety outcomes.11–13 The availability of these large, longitudinal data sources has facilitated numerous pharmacoepidemiologic studies and enhanced the capacity for timely and robust detection of drug safety signals. In response, several active surveillance initiatives have been established worldwide, including the Sentinel Initiative 14 and the Observational Health Data Sciences and Informatics (OHDSI) network 15 in the United States, the Exploring and Understanding Adverse Drug Reactions by integrative mining of clinical records and biomedical knowledge (EU-ADR) project 16 in Europe, and the Asian Pharmacoepidemiology Network (AsPEN) 17 in Asia. Collectively, these efforts have promoted a paradigm shift from passive to active surveillance and stimulated substantial methodological advancements in the detection, refinement, and evaluation of drug safety signals.
In routine surveillance settings, electronic healthcare data accrue continuously and can be analyzed repeatedly as new data become available, creating a natural context for sequential analysis. Sequential analysis is well established in clinical trials, where it enables interim analyses while rigorously controlling the overall type I error rate, thereby providing a principled framework for evaluating accumulating evidence. 18 When adapted to post-marketing surveillance, sequential analysis allows for near real-time evaluation of pre-specified adverse events following the introduction of a medical product. 19 It therefore serves a dual purpose: facilitating early detection of emerging safety concerns while simultaneously providing reassurance to regulators and the public through ongoing monitoring. To date, sequential analysis has been most extensively applied in vaccine safety surveillance,20,21 notably within initiatives such as the Vaccine Safety Datalink (VSD), where it underpins near real-time monitoring commonly referred to as rapid cycle analysis. 22 Recent studies have explore the extension of similar sequential methodology to therapeutic drugs.23–25 Nevertheless, a systematic overview of how these methods have been implemented and adapted in post-marketing drug safety surveillance is still lacking.
The objective of this scoping review is to systematically identify and characterize empirical applications and methodological developments of sequential analysis for safety signal detection in post-marketing drug surveillance based on routinely collected electronic healthcare data, and to summarize key methodological approaches and evidence gaps in the literature. This synthesis thereby provides a structured overview to inform future methodological development and regulatory practice in near-real-time drug safety surveillance.
Methods
This scoping review was conducted in accordance with the methodological framework proposed by Arksey and O’Malley 26 and reported following the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for scoping reviews, checklist provided in the Supplemental File). 27 The review question and eligibility criteria were structured using the PICO framework. The population comprised individuals represented in electronic healthcare databases; the intervention referred to sequential analysis methods for post-marketing drug safety surveillance; the outcomes included drug safety endpoints and methodological performance measures. The comparator was not mandatory. The study protocol was pre-registered on the Open Science Framework (OSF) platform (https://doi.org/10.17605/OSF.IO/UZGSW).
Search strategy
We systematically searched three English-language databases (PubMed, EMBASE, and the Cochrane Library) and three Chinese databases (CNKI, WanFang, and VIP). The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords related to drug safety, post-marketing surveillance, sequential analysis, and electronic healthcare data. The detailed strategy is provided in the Supplemental File. In addition, reference lists of included studies were manually screened to identify additional relevant publications. The literature search was conducted from database inception to 21 July 2025. All retrieved records were imported into EndNote X9 for reference management, and duplicate records were removed.
Eligibility criteria and literature screening
Based on the PICO framework, two categories of studies were eligible for inclusion. First, empirical observational studies were included if they: (i) used routinely collected electronic healthcare data within a population-based monitoring setting; (ii) evaluated the safety of one or more drugs in relation to pre-specified adverse outcomes; (iii) employed an observational study design; and (iv) conducted repeated or periodic analyses as data accrued over time. Second, given that the application of sequential analysis in post-marketing drug safety surveillance remains at an early stage, methodological studies were also eligible if they: (i) proposed, extended, or evaluated novel or improved sequential statistical methods for post-marketing drug safety surveillance; or (ii) compared the signal detection performance of different sequential approaches. We excluded studies based exclusively on spontaneous reporting systems, review or opinion articles, studies for which the full text was unavailable, and studies focusing solely on vaccine safety.
Study selection was conducted in two stages. Titles and abstracts were screened first, followed by full-text review to determine final eligibility. Screening was performed independently by two researchers (Q.D. and H.N.), and any disagreements were resolved through discussion with a third researcher (Y.S.).
Data extraction and synthesis
A standardized data extraction form was developed based on relevant prior reviews,20,28 and the RECORD Pharmacoepidemiology Checklist. 29 For empirical observational studies, we extracted information on authors, year of publication, study setting and period, primary objectives, data sources, study population, evaluated drugs and outcomes, sequential analysis framework, statistical approaches, frequency of assessment, and main findings. In line with methodological guidance for scoping reviews, 30 study quality was characterized by extracting and discussing key quality-related parameters rather than by conducting a formal methodological quality or risk-of-bias assessment. These parameters included study design, sample size, outcome identification criteria, case validation methods, confounder control strategies, consideration of data-accrual lags, and reported methodological challenges. For methodological studies, additional data were collected on proposed or extended sequential methods, optimization strategies, performance evaluation metrics, and comparative assessments across different approaches. Detailed descriptions of the data extraction form are provided in Tables S1 and S2.
Extracted data were subsequently mapped to predefined analytical dimensions to facilitate a structured synthesis of the evidence. These dimensions encompassed basic study characteristics, real-world data features, pharmacovigilance objectives, methodological aspects of sequential analysis, and key adaptations addressing confounding, data uncertainty, and other challenges. A narrative approach was used to synthesize findings across included studies. Data extraction and synthesis were conducted independently by two researchers (Q.D. and Y.S.), with discrepancies resolved through discussion.
Results
Study selection
A total of 3712 records were identified through database searches after duplicates removal. Following title and abstract screening, 3583 records were excluded as not relevant to the research question, leaving 129 articles for full-text review. Seven additional studies were identified through manual screening of reference lists. Ultimately, 46 studies met the eligibility criteria and were included in the final synthesis. The detailed study selection process is illustrated in the PRISMA-ScR flow diagram (Figure 1).
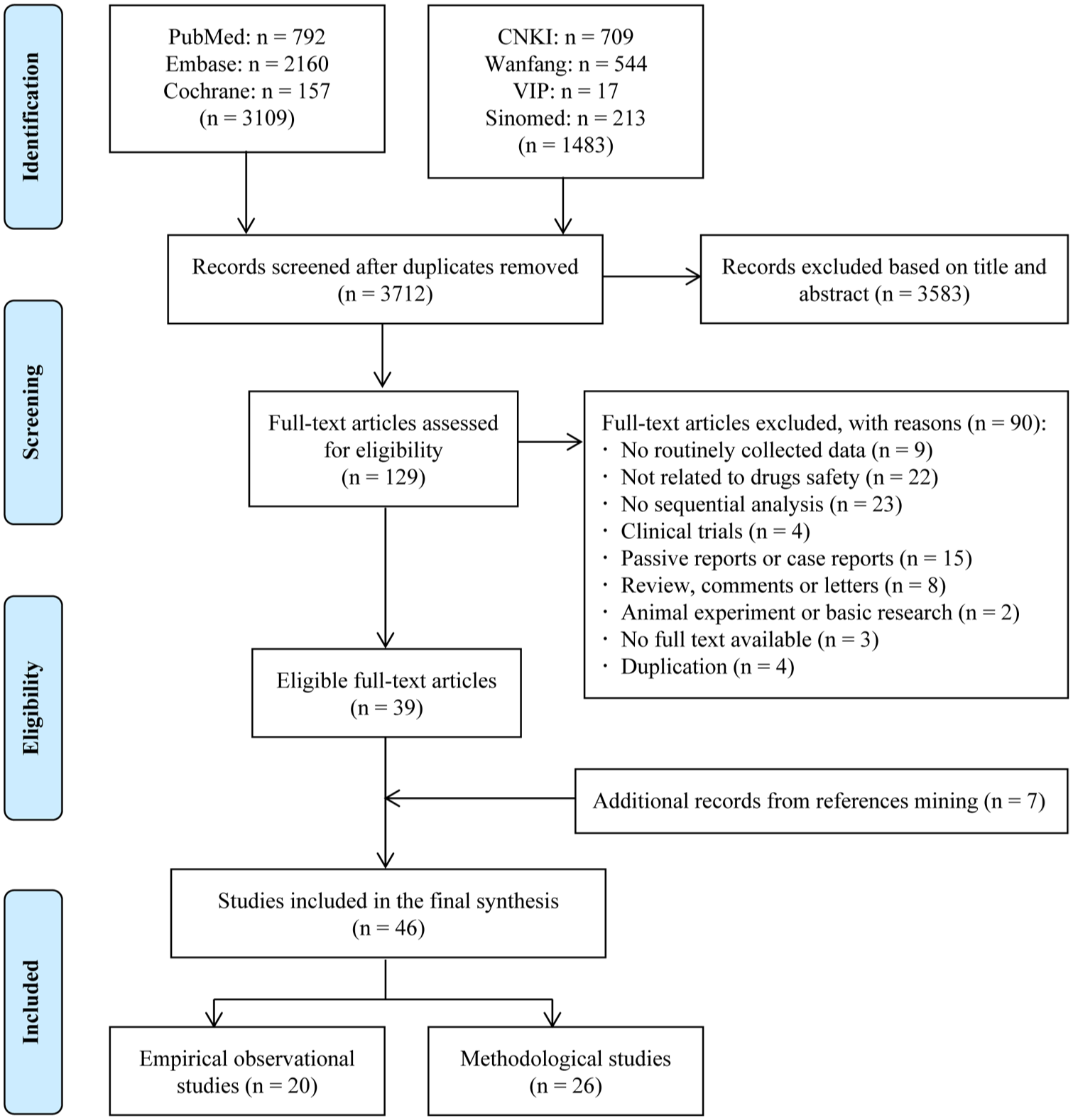
Flow diagram showing study selection process.
Of the 46 included studies, 20 were empirical observational studies. Most of these (n = 16, 80%) were pilot or feasibility studies primarily aimed at evaluating the implementation of sequential methods and identifying key methodological considerations, whereas only four studies (20%) focused on detecting safety signals for specific drugs. In addition, 26 methodological studies were included to comprehensively capture the development of sequential approaches in post-marketing drug safety surveillance. Basic information of all included articles is provided in Table S3.
Characteristics of included empirical observational studies
Data source, drugs and ADEs studied
The earliest application of sequential analysis for post-marketing drug safety surveillance was reported in the United States in 2007. 31 Subsequently, 13 additional studies were conducted in the United States, along with six studies carried out in five other high-income countries. Most investigations were performed within well-established active surveillance systems or large healthcare data networks, including the Sentinel Initiative, the HMO Research Network, and several national or commercial healthcare databases. Two main types of data sources were used: electronic health or medical records (EHRs/EMRs) in 12 studies (60%) and administrative claims data in eight studies (40%).
Across these studies, a variety of therapeutic drugs were monitored after licensure for pre-specified ADEs using fixed risk windows. Lipid-lowering agents were the most frequently evaluated drug class (n = 5), followed by antihypertensive drugs, non-steroidal anti-inflammatory drugs, anticoagulants, and antibiotics (each n = 4). ADEs were typically selected based on safety concerns arising from spontaneous reporting systems or pre-licensure clinical trials. Cardiovascular outcomes received the greatest attention. Most studies identified ADEs using algorithms based on International Classification of Diseases (ICD) diagnosis codes applied to automated data to enable near real-time analysis. Only one study defined outcomes using laboratory test results rather than diagnostic codes. 32 Approximately half of the studies conducted case validation through medical chart review, reporting positive predictive values generally exceeding 80%.23–25,33–39 Across all empirical studies included in this review, 26 statistically elevated drug–event pairs (signals) were identified (Figure 2), eight of which corresponded to known associations used primarily for methodological validation across seven studies. An overview of study characteristics is presented in Table 1, with additional details provided in Table S4.
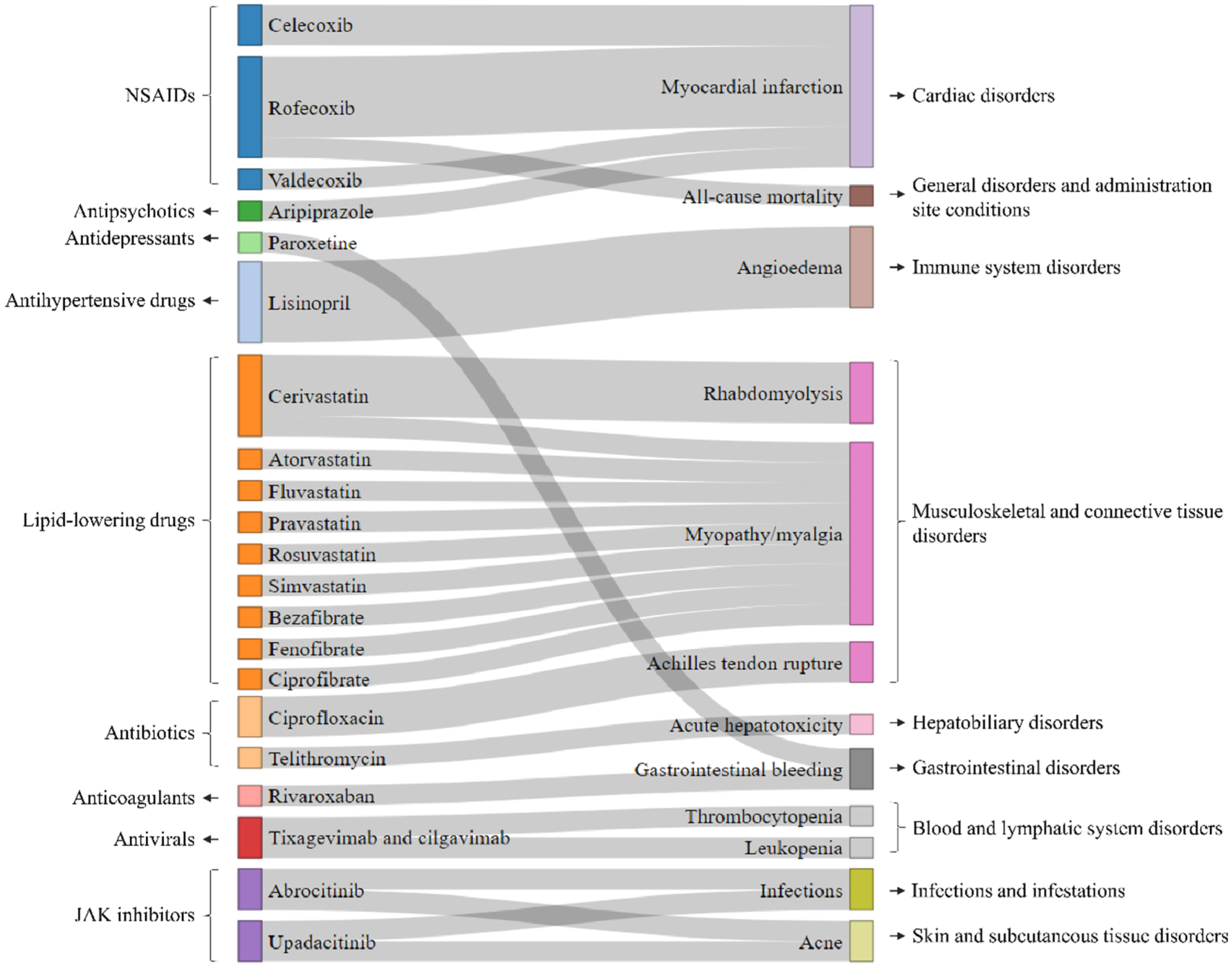
Statistically elevated drug–event pairs (signals) in the included studies. Drug notes and event nodes are colored according to their corresponding therapeutic classes and SOC categories, respectively. The width of each link represents the relative number of drug–event pairs reported across studies.
Summary of basic characteristics of empirical observational studies (n = 20).
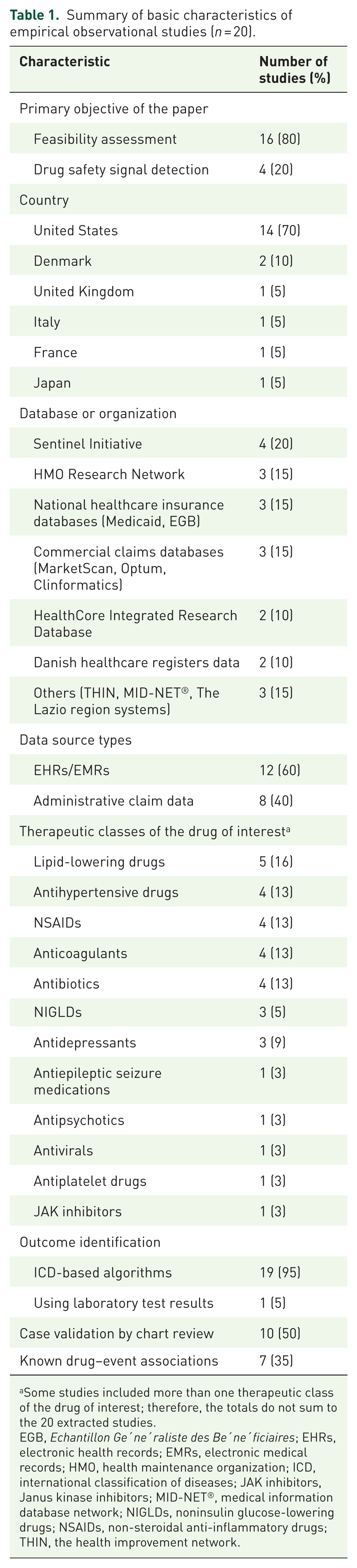
Some studies included more than one therapeutic class of the drug of interest; therefore, the totals do not sum to the 20 extracted studies.
EGB, Echantillon Ge′ne′raliste des Be′ne′ficiaires; EHRs, electronic health records; EMRs, electronic medical records; HMO, health maintenance organization; ICD, international classification of diseases; JAK inhibitors, Janus kinase inhibitors; MID-NET®, medical information database network; NIGLDs, noninsulin glucose-lowering drugs; NSAIDs, non-steroidal anti-inflammatory drugs; THIN, the health improvement network.
Sequential methodologies
Cohort designs with concurrent or parallel comparison were the most frequently used study design (n = 16), followed by self-controlled designs (n = 4), including case-crossover and case-time-control studies (Table 2). Two studies applied more than one study design within the same surveillance framework. Sequential analysis was implemented in two principal paradigms: (i) as sequential testing approaches (n = 6), which involved periodic hypothesis testing such as the maximized sequential probability ratio test (MaxSPRT) or group sequential methods; and (ii) as sequential risk estimation (n = 17), which involved repeatedly fitting regression models as new data accrued to update effect estimates such as the hazard ratios (HRs). Three studies employed both sequential testing and sequential risk estimation strategies. The analysis frequency was largely determined by the update cycle of the data sources. Most studies (90%) conducted analyses at fixed calendar-based intervals, with quarterly monitoring being the most common approach. Two studies (10%) adopted irregular, information-based analysis schedules. Detailed methodological features of individual studies are provided in Table S5.
Summary of sequential methodology of empirical observational studies (n = 20).
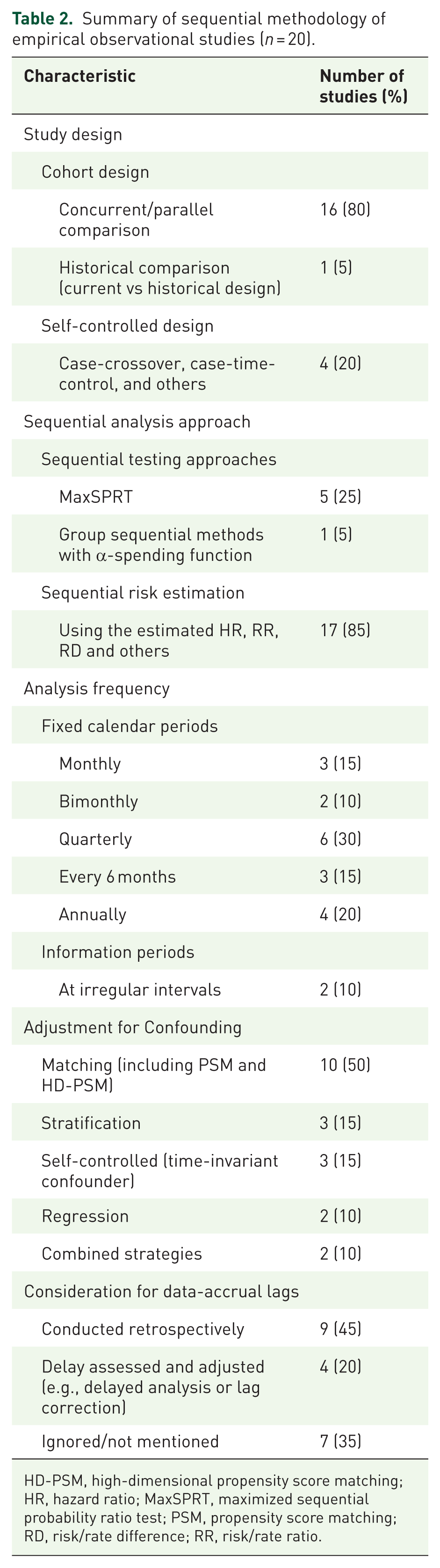
HD-PSM, high-dimensional propensity score matching; HR, hazard ratio; MaxSPRT, maximized sequential probability ratio test; PSM, propensity score matching; RD, risk/rate difference; RR, risk/rate ratio.
Confounder adjustment and potential challenges
All included studies reported strategies for confounder control (Table 2). Most approaches were design-based (n = 18, 90%) and included, either alone or in combination: (i) matching baseline confounders, using traditional and high-dimensional propensity score methods; (ii) stratification by key confounder categories; and (iii) self-controlled designs, which inherently account for time-invariant confounding. Only two studies (10%) relied primarily on analysis-based strategies using regression modeling. Commonly considered confounders included age, sex, study site, seasonality, temporal trends, comorbidities, concomitant medications, and other outcome-related risk factors.
Only four prospective studies (20%) explicitly addressed data-accrual lags, most often by delaying analyses for several months to allow for data stabilization. Additional challenges frequently reported across studies included multiple testing arising from repeated analyses, rare outcomes, time-varying population characteristics and exposure patterns, and outcome misclassification.
Characteristics of included methodological studies
Methodological advances in sequential analysis for drug safety surveillance have largely been motivated by challenges observed in empirical applications. As shown in Figure 3, fifteen studies proposed novel or extended sequential testing methods, which inherently control the inflation of type I error arising from multiple testing. These approaches can be broadly classified into continuous sequential methods, such as MaxSPRT (n = 4); group sequential methods, such as the conditional sequential sampling procedure (CSSP) (n = 9); and Bayesian sequential methods (n = 2). The former two fall within frequentist frameworks, whereas the latter is grounded in Bayesian inference. Seven studies focused on refinements to the design and operational aspects of sequential monitoring, particularly with respect to bias adjustment, handling of data uncertainty, and enhancing the feasibility of workflows and implementation.
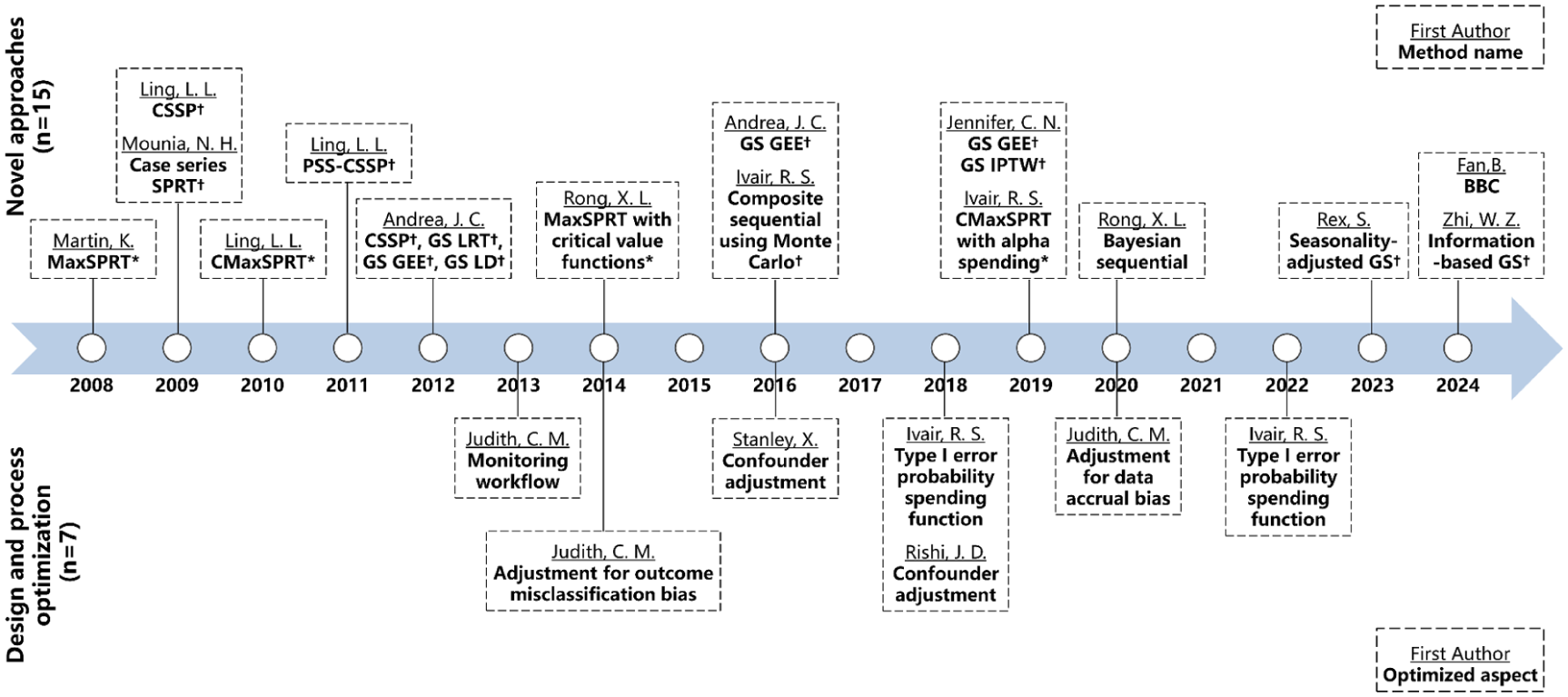
Timeline of advances in sequential methodology for drug safety surveillance.
Nine studies conducted comparative evaluations of signal detection performance across different methods (Table S6). The evaluation metrics could be broadly categorized into three domains: (i) accuracy (n = 6), encompassing both signal detection performance, such as type I and type II error rates and statistical power, as well as the reliability of effect estimates; (ii) timeliness (n = 6), referring to the ability of a method to detect signals early and primarily assessed using time to signal; and (iii) operational feasibility (n = 5), reflecting the practical implementation of sequential methods and including metrics related to time to surveillance end (i.e., maximum sample size required in the absence of a signal) and computational efficiency. Among the included studies, one study comparing sequential and non-sequential analyses indicated that sequential approaches could detect safety signals earlier, or at least as quickly as non-sequential analyses, highlighting their practical value for timely post-marketing risk management. 40 Another study compared continuous versus group sequential approaches and reported that continuous sequential methods consistently achieved shorter expected times to signal when data were updated frequently. 41 The remaining seven studies focused on comparisons of specific sequential methods, including MaxSPRT, CSSP, and other recent methods. These studies consistently showed that newer approaches incorporating flexible modeling or bias adjustment—such as group sequential generalized estimating equations (GS GEE) or Bayesian sequential with bias correction (BBC)—tended to offer improved statistical power, better control of type I error, and faster signal detection compared with classical alternatives. Overall, the performance of sequential monitoring is strongly influenced by the specific methodological choice, particularly in settings characterized by confounding or rare outcomes.
Discussion
To our knowledge, this scoping review provides the first comprehensive synthesis of published evidence that used sequential analysis to detect drug safety signals in near real-time within post-marketing surveillance. This review aimed to systematically identify and characterize empirical applications and methodological developments of sequential analysis in this context, while summarizing key methodological approaches and evidence gaps. Our findings indicate that although sequential methods are conceptually well aligned with the needs of near real-time pharmacovigilance, their empirical application to therapeutic drugs remains limited. Most observational studies were conducted as pilot or feasibility evaluations rather than as fully operational, prospective surveillance programs for specific drugs. Furthermore, all identified studies were performed in high-income countries, predominantly in the United States. The overwhelming concentration highlights the substantial infrastructural, computational, and governance requirements necessary to support timely data availability and periodic monitoring. Besides, heterogeneity was observed in study designs, analytical frequencies, and sequential methods, indicating the absence of a standardized methodological framework for sequential drug safety monitoring. Overall, the current evidence suggests that sequential analysis has not yet been fully integrated into routine pharmacovigilance practice for drugs, despite its potential to support near real-time safety assessment.
In contrast, sequential analysis has become well established in vaccine safety surveillance. 42 A prominent example was its use in the early detection of an increased risk of seizures following measles-mumps-rubella-varicella vaccination (USA, 2011, population-based sequential surveillance study, 9.2 million people in the VSD), which ultimately informed changes to national vaccination policy. 22 Additionally, sequential analysis has proven particularly valuable in contexts characterized by rapid exposure accrual, such as seasonal influenza and COVID-19 vaccination campaigns, where urgent public health demands necessitated near real-time safety evaluation.43,44 These methods have also been applied in settings where safety concerns existed due to experiences with earlier versions of vaccines, such as rotavirus vaccination and its association with intussusception. 45 The increasing use and routine practice of sequential analysis in vaccine surveillance are largely facilitated by the inherent nature of vaccines, which typically involve well-defined, transient exposures and acute-onset outcomes in largely healthy populations. 42 By comparison, therapeutic drug use is more complex: exposures are often prolonged, heterogeneous, and dynamic; and adverse outcomes may be delayed or influenced by underlying disease severity. 46 These features amplify challenges related to confounding by indication, and other time-varying factors, thereby complicating both the design and statistical properties of sequential monitoring in observational settings.
Despite these challenges, drug safety surveillance plays a central role in preventing ADEs, which remain a major and often preventable cause of hospitalization and healthcare burden in routine clinical practice. Early identification of safety signals in the post-marketing phase is critical, as pre-marketing clinical trials are inherently limited in their capacity to identify rare, delayed, or population-specific adverse effects. In this context, sequential analysis offers important clinical value by enabling continuous and near real-time evaluation of accumulating safety data, rather than relying on delayed end-of-study assessments. Such timeliness is particularly relevant for clinical decision-making and regulatory action, where even modest reductions in detection latency may translate into reduced patient exposure to harmful therapies and more rapid implementation of risk mitigation strategies. Therefore, sequential methods can be viewed not only as statistical tools, but also as operational frameworks that support earlier clinical awareness and more responsive pharmacovigilance systems.
Our synthesis identified two predominant paradigms of sequential analysis implemented in drug safety surveillance: sequential testing and sequential risk estimation. The first paradigm is adapted from classical sequential frameworks originally developed for clinical trials, which rely on formal hypothesis testing and pre-specified signaling threshold. The threshold is usually achieved through α-spending plans designed to preserve the overall chance of type I error (e.g., false positive) below 0.05 across the total number of sequential tests conducted. 42 Such approaches provide statistical rigor and clear signaling rules. Regarding specific methods, MaxSPRT was the most common in empirical studies, consistent with observations in the field of vaccine safety surveillance. 20 It remains uncertain whether continuous or group sequential methods are preferable in the context of post-marketing surveillance. Group sequential methods are generally considered more appropriate when data updates occur less frequent. 47 However, methodological comparisons (simulation study) suggest that continuous sequential approaches may offer superior performance when frequent data evaluation is feasible. 41 Additionally, recent work has introduced Bayesian sequential approaches that offer greater flexibility and have demonstrated advantages compared to existing frequentist frameworks.48–50 However, these promising approaches are still at the development stage and have not yet been applied in empirical studies.
The second paradigm, inspired by traditional pharmacoepidemiological risk measures, relies on the periodic estimation of effect sizes (e.g., HRs) as data accrue rather than awaiting a single final analysis delayed by several years.38,51 This estimation-based approach appears more prevalent in recent drug surveillance studies, likely because such methods grounded in familiar concepts are perceived as more accessible to stakeholders than sophisticated hypothesis-testing frameworks. 19 Distinct from clinical trials, where sequential analyses utilize interim looks to trigger early stopping, this approach prioritizes the continuous characterization of evolving risk. 36 In this post-marketing setting, sequential analysis serves less as a direct signaling decision rule and more as a mechanism for regular evidence updating, facilitating near real-time information sharing with clinicians and regulators. Nevertheless, the absence of formal multiplicity adjustments raises concerns regarding inflated false-positive findings, particularly during early monitoring phases when event counts are sparse and estimates remain unstable.24,42 Consequently, balancing statistical validity with operational simplicity remains a critical unresolved tension in the design of sequential drug safety surveillance systems.
Beyond methodological heterogeneity, our review also identified important challenges regarding the practical implementation and reliability of sequential drug safety surveillance. A primary concern is the limited control of potential confounding, both in the strategies employed and, in the factors, adjusted for. We observed that most empirical studies relied on design-based strategies, such as matching or stratification. Recent methodological research has advocated for more rigorous approaches to confounding adjustment, particularly at the analysis stage, such as integrating generalized estimating equations or inverse probability weighting within sequential frameworks. 52 But their practical performance in prospective drug safety monitoring remains largely unexamined. Meanwhile, it is important to recognize that sequential surveillance is primarily intended for early signal detection rather than definitive causal inference. An end-of-surveillance epidemiologic study with more comprehensive confounding control is often warranted to further confirm the findings from sequential analysis. Furthermore, the utility of these methods depends heavily on data timeliness. Near real-time data availability does not ensure data completeness. Data-accrual lags, defined as the interval between the occurrence of exposure or safety outcomes and their recording in the database with sufficient quality, may introduce bias into sequential analysis. 53 One way to address this issue is to delay the analysis until the data have stabilized.37,54,55 A more timely approach is to know how long it takes for data to accrue and then use the pattern into modeling adjustments. 54 However, our review suggests that explicit consideration of data-accrual lags remains limited in practice. Lastly, several challenges arise from the real-world settings, including outcomes misclassification, rare events, and unpredictable changes in exposure patterns (e.g., variable uptake rates and composition of the population adopting a new product).56–58 Further methodological work is needed to better characterize these challenges and to establish more rigorous and standardized approaches to overcome them.
We propose three critical directions for future research. First, methodological guidance is needed to standardize sequential analysis in observational settings. Such guidance should specify key design and operational parameters, including the choice of surveillance design and comparator, the sequential framework and approaches, analysis frequency and stopping rules, and principled approaches to confounding and time-varying biases. Second, progress will depend on wider access to continuously updated and harmonized data infrastructures, particularly in low- and middle-income countries. The expansion of Common Data Models, distributed data networks, and reusable analytic pipelines creates opportunities to scale sequential monitoring across multiple sites. 59 Carefully validated analytical automation, including machine learning and artificial intelligence approaches, may further improve the timeliness and accuracy of signal detection. 60 Third, sequential monitoring should be embedded within the broader signal management and regulatory ecosystem rather than viewed as a standalone statistical exercise. Clear governance frameworks, predefined action plans for signal evaluation and confirmation, and structured communication pathways between data partners and regulators are necessary to ensure that early detected signals translate into timely regulatory and clinical responses.
Limitations
By synthesizing both empirical applications and methodological developments, this review provides a structured overview of the current state of the field and identifies priorities for future research, implementation, and regulatory use. However, several limitations of this review must be acknowledged. As this was a scoping review, we did not conduct a formal risk-of-bias assessment of the included studies. However, given the absence of a validated quality assessment tool for these types of research, rigorous assessment would have been challenging. Second, although we employed a comprehensive search strategy, relevant studies may have been missing, particularly unpublished methodological work or recently developed approaches not yet widely applied in empirical studies. Finally, publication bias is an inherent concern, as studies with negative or null results may be less likely to be published.
Conclusion
Over the past decade, post-marketing drug safety surveillance has undergone a substantial transformation from passive monitoring toward more active and systematic approaches, driven by the expanding availability of real-world data and advances in analytic methods. Sequential analysis provides a principled framework for near real-time safety assessment using continuously updated data. This scoping review demonstrates that, despite increasing interest and methodological progress, the empirical application of sequential analysis in post-marketing drug safety surveillance remains limited and is still largely concentrated in pilot implementations in high-income countries. Careful consideration is required at both the sequential design and implementation phases, as many methodological and practical challenges arise in observational settings including confounding control and data-accrual lags. Future work should prioritize stronger approaches, clearer implementation standards, and better integration of sequential monitoring into the broader signal management process. With the increasing availability of real-world data and continued advances in analytical automation, sequential analysis is likely to play a growing role for near real-time active surveillance to complement traditional pharmacovigilance.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261454206 – Supplemental material for Sequential analysis for post-marketing drug safety surveillance using routinely collected electronic healthcare data: a scoping review
Supplemental material, sj-docx-1-taw-10.1177_20420986261454206 for Sequential analysis for post-marketing drug safety surveillance using routinely collected electronic healthcare data: a scoping review by Yixin Sun, Qian Ding, Hongting Nie and Peng Guo in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.