
Abstract
Background:
Polypharmacy is common in people with dementia but may be insufficiently tailored to personal preferences and goals, particularly in the presence of a life-limiting condition.
Objectives:
To evaluate the effectiveness of pharmacists working with general practitioners (GPs) to optimise medicine regimens and health outcomes of people with dementia by applying the Medication Appropriateness Tool for Comorbid Health Conditions During Dementia (MATCH-D) as part of a structured Team Approach to Polypharmacy Evaluation and Reduction (AusTAPER).
Design:
Randomised controlled trial.
Methods:
This study was conducted in Perth, Western Australia, with 12month follow‑up. The intervention was a collaborative medicine review that included a medicines history, interview by a research pharmacist, and a case conference with the participant’s GP. Outcomes included medicines regimen, emergency department presentation, hospitalisations, and health outcomes at 12 months.
Results:
Overall, 19 GPs and 31 participants were recruited (five directly; 26 through GP practices). The pharmacist spent an additional mean of 5.5 hours with intervention participants. At baseline, the median number of regular medicines was 8.5 (IQR 3) in the control group and 10 (IQR 7) in the intervention group, and at 12 months, 11 (IQR 4) and 9.5 (IQR 5), respectively. Emergency department presentations were observed for 9/16 (56%) control and 10/15 (66%) intervention participants, with a median of 1 (IQR 1.5) versus 1 (IQR 4) presentations (z = 1.18, p = 0.25). Eight participants in each group had at least one day of unplanned hospital admission with a similar length of stay (0.5 (IQR 5) versus 1 (IQR 9) days; z = 0.44, p = 0.67). Quality of life, physical function, cognition, frailty, and falls were similar between groups.
Conclusion:
Over 12 months, participants in both groups had similar medicine use, outcomes and quality of life. It was feasible to recruit people with dementia, and their doctors, to a medicine review intervention.
Trial registration:
This study was prospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTR; ACTRN12619000453189) on 19 March 2019.
Plain language summary
People living with dementia often take multiple medicines, which may not always align with their personal goals or health needs. This study explored whether a structured medicine review involving pharmacists and general practitioners (GPs) could improve medication use and health outcomes. A randomised controlled trial was conducted in Perth, Western Australia. People with dementia living in the community were recruited through GP practices. Participants were assigned to either usual care or an intervention where a pharmacist reviewed their medicines, interviewed them, and held a case conference with their GP. We tracked medication use, hospital visits, and health outcomes over 12 months. Thirty-one participants and 19 GPs took part. The pharmacist spent extra time with those in the intervention group, but after 12 months, both groups had similar numbers of medicines, hospital visits, and quality of life. It was feasible to involve people with dementia and their doctors in a structured medicine review. However, in this small study, the approach did not lead to major changes in health outcomes or medicine use. Larger studies are needed to understand its potential benefits.
Introduction
Dementia is the second leading cause of death and the leading cause of disability burden in adults aged 65 years and older in Australia. 1 People living with dementia typically have coexisting health conditions or comorbidities and are frequently exposed to polypharmacy. 2 The medical management of people with multiple comorbidities is complex 3 and becomes even more complex in people living with dementia.4,5 Suboptimal pharmacological management can exacerbate the rate of functional decline and increase the risk of adverse drug events in people living with dementia. 6 The life-limiting nature of dementia may also mean that the benefits of some preventive treatments are unlikely to be realised.7,8 Additionally, care goals may change over time, meaning optimal medicines management in the early phases of dementia is often not the same in the later stages. Consequently, medicines management becomes more challenging as dementia progresses. 9 Limited evidence exists to inform practice as clinical trials frequently exclude people with dementia directly, or indirectly by imposing a maximum age limit, and by excluding comorbidities or concurrent treatments. 10
Engaging people with dementia and their advocates in research to optimise medicines use is important but under-explored. 11 Despite the increasing understanding of the importance of including people with dementia in research to ensure the relevance and applicability of the findings, 12 limited research has effectively recruited and engaged people with dementia and their advocates to studies aimed at optimising medicines regimens. 13 Strategies have been explored to increase participation and improve recruitment 14 ; however, there are few randomised controlled trials (RCTs) designed to test interventions to improve medicines management involving people with dementia and their advocates.15,16
It remains unclear to what extent people with dementia and their advocates can be successfully engaged, recruited and followed up in Randomised Control Trials (RCTs). Further, it is unclear if the negative effects on health associated with polypharmacy in people with dementia are reversible or whether improving medicines use will enhance clinical outcomes and wellbeing. Consensus-based guidance for clinicians who manage comorbid health conditions in people with dementia has been developed (Medication Appropriateness Tool for Comorbid Health Conditions During Dementia; MATCH-D). 17 We aimed to evaluate the effectiveness of pharmacists working with general practitioners (GPs) to optimise the medicine regimens and health outcomes of people with dementia by applying the Medication Appropriateness Tool for Comorbid Health Conditions During Dementia (MATCH-D) as part of a structured Team Approach to Polypharmacy Evaluation and Reduction (AusTAPER).
Methods
Ethics
The Team Approach to Polypharmacy Evaluation and Reduction for General Practice Patients with Dementia: (the AusTAPERdem) Study was approved by The University of Western Australia’s Human Research Ethics Committee (Ref RA/4/20/4354) and prospectively registered with the ANZCTR (ACTRN12619000453189).
Study design and randomisation
This study was a prospective single-blinded parallel group study in one Australian capital city. General practices were randomised using computer-generated randomisation tables to one of two groups, either the control group (continued usual care) or the intervention group (intervention using MATCH-D in the AusTAPER app). The chief investigators were blinded to study allocation, and data analysis was undertaken blinded. The Consolidated Standards of Reporting Trials (CONSORT) checklist was followed in preparing this manuscript and the completed checklist is provided as Supplemental Material. 18
Participant eligibility
Eligible participants were people living with dementia (defined as a documented diagnosis of dementia by the GP, which could be mild, moderate or severe), taking five or more medicines and living in the community. Participants were excluded if they were not community dwelling, or remained community dwelling but had inadequate language skills to participate, were in the terminal phase of life, or had a comprehensive community pharmacist medicine review (‘MedsCheck’) or GP-led home medicine review within the preceding 12 months. Carers were not participants per se (i.e. we did not recruit research dyads), but we engaged with participants’ carers at all stages of the research to support successful participation of people living with dementia.
Recruitment
General practice recruitment
Initial recruitment was through GP practices. A hardcopy mail-out was sent to 469 general practice providers in the Perth, Western Australia metropolitan area in May 2019. The study was also promoted with an invitation to participate via the Australian Medical Association (AMA) emailing list to members and non-members. Promotion with an invitation to participate was also sent to around 350–400 GP practices through the WA Primary Health Alliance (WAPHA) Connect Newsletter (September 2019 and May 2020). Practice managers and GPs were invited to be part of the study by providing them with written information about the study, including participant information sheets, questionnaires, details on the AusTAPER web-based application and consent forms. Potentially interested GPs and GP practices were invited to have discussions with the study team to provide more information about the study to the GPs, practice managers and practice nurses. Participating general practices systematically screened practice records to identify potentially eligible participants. Potentially eligible patients were sent a letter with information about the study and an invitation to consent to a 15-min telephone screening interview. Where recruited through the GP practice, potentially eligible participants also had to be a regular patient at the participating GP practice.
Direct recruitment
Additionally, we advertised the opportunity to participate in the study directly to consumers on the StepUp for Dementia Research (https://www.stepupfordementiaresearch.org.au/) and social media platforms. After screening and consenting these potential participants, their regular GPs were provided with information about the study and approached for their agreement for their patient to participate in the study. When recruited directly, the participant’s regular GP was required to agree to their participation.
COVID-19 pandemic impacts on recruitment
Recruitment was substantially affected by the COVID-19 pandemic and was extended on several occasions in an attempt to achieve the target sample size. Protocol amendments subsequently enabled additional recruitment strategies, including telephone follow-up, direct contact via professional networks and dementia-related organisations (e.g. StepUp for Dementia Research), and expansion to virtual recruitment channels. Newspaper and classified advertisements were also ethically approved but were not ultimately implemented due to feasibility constraints. General practices were heavily impacted by the COVID-19 pandemic, with clinical care demands and vaccination roll-out prioritised, limiting capacity to engage in research. Recruitment continued with multiple extensions (first participant enrolled September 2019; final participant November 2022), including re-contacting previously interested practices in August 2022; however, no additional participants were recruited. Achieving the original recruitment target of 750 participants became almost impossible once it became apparent the Perth metropolitan region (postcodes 6000 to 6164) would be the only Australian location running the study.
Sample size
The intended sample size was 750 participants recruited across 48 GP practices at multiple sites. The a priori sample size calculation was based on 80% power to detect an absolute reduction of 8.5% (equivalent to a 34% relative reduction) in emergency presentations and/or unplanned hospital admissions at the 12month follow-up. This effect size was informed by previous similar interventions. However, the planned multi-site recruitment was not achieved, and the final sample size was considerably smaller than originally intended as described above.
Intervention
The AusTAPER web-based application (available at https://meds.tapermd.org/), designed for collaborative medicine review, was used to facilitate the application of MATCH-D by pharmacists and doctors. AusTAPER is an Australian adaptation of the Canadian TAPER intervention, 19 initially piloted in Australian general practice settings, 20 and had been implemented in older hospital inpatients. 21 AusTAPER performs a ‘machine screen’ comprising (i) interaction checker; and (ii) listing of potentially inappropriate medicines (including anticholinergic and serotonergic burden, and QT-prolonging drugs) linked to existing evidence-based tools providing Numbers Needed to Treat/Harm, and patient decision aids. The intention was to maintain essential drugs while supporting reduction in medicines known to be associated with adverse reactions, and those where risk frequently outweighs benefit (e.g. anticholinergics, sedatives, opiates, proton pump inhibitors).
Study pharmacist/participant interview: The person with dementia (and their advocate/carer) was engaged in a medicines-focused interview with the study pharmacist within 2 weeks of baseline data collection. This interview was usually conducted at the person’s home as this is where people feel most comfortable, and the most accurate medicines histories are obtained. 22 The medication history collected at baseline, indications for medicines and other medication-related information if available (such as blood pressure creatinine, falls history), prioritised functional and symptom goals for medical treatment, preferences for care, and perceived medicine problems or side effects were compiled, entered into the AusTAPER app, and reviewed. Through the application of automated filters within the AusTAPER App, potentially inappropriate medicines (including automated application of the MATCH-D criteria), medicine interactions and warnings were identified, and medicines that were candidates for discontinuation or dose reduction were flagged.
Informed by this list with automated flags, reported medicines-related adverse effects from the participant, and after reviewing the participant’s goals for treatment, the study pharmacist carried out a comprehensive medicine review focused on medicines suitable for discontinuation or dose reduction. In addition to the integration of MATCH-D criteria into the AusTAPER App to apply automated flags, the pharmacist was asked to consider the MATCH-D criteria in their reviews of the medication regimens. Recommendations were made and added to the AusTAPER clinical pathway. This information, including all the supporting information and the machine screen dashboard data was available to the clinic GP for review at their consultation, and was also cut and pasted using the AusTAPER Snapshot format into the community pharmacist’s record, to avoid double data entry and fragmentation of care.
GP consultation: Approximately 1 week (and ⩽ 2 weeks) after the study pharmacist/participant meeting, the participant had an extended face-to-face appointment with their GP to discuss medicines that may be suitable for a ‘pause and monitor’ trial of discontinuation or dose reduction. The GP had available the pharmacist-generated accurate medicine list with flagged recommendations, and evidence and tools to support deprescribing linked in the AusTAPER App. The GP could modify or add information to the tool if necessary. The GP discussed the participant’s priorities and preferences for care, which informed a prioritised plan for appropriate discontinuations and a template for monitoring frequency, duration and criteria for medicine recommencement. If a specialist had prescribed medicines, the GP/study pharmacist followed their usual clinical process for seeking specialist advice if appropriate.
Community pharmacy engagement: The research pharmacist gave a report to the participant and regular dispensing community pharmacy (or pharmacies). If changes to medicines were recommended, it also included a copy of the agreed discontinuation and monitoring plan. This information was also provided to the GP. The GP wrote prescriptions required for any tapering plan until the medicine was ceased. These prescriptions were dispensed as usual by the participant’s regular dispensing community pharmacy/ies following usual care processes.
Monitoring: Six- and 12month follow-up appointments were made as the GP and/ or pharmacist agreed was required for each individual participant. These generally occurred approximately 2 weeks after any medicines were changed. If no changes were made to a person’s medicines, the GP and participant determined the timing of monitoring visits. At each monitoring visit, participants had a brief GP consultation to review progress with the MATCH-D AusTAPER plan and address any concerns (such as perceived Adverse Drug Withdrawal Events) as clinically appropriate.
Comparison (usual care)
The control group continued to receive the usual care from their regular practitioners, including their general practitioner, other practice staff and their community pharmacy.
Outcomes
The primary outcomes were emergency department presentations and unplanned admission to hospital, measured through self (or proxy report) and audit of health records at 6 and 12 months.
Secondary outcome measures included, at 6 and 12 months follow-up:
Change in number of regular medicines (assessed by direct interview of the participant by research staff, pharmacy dispensing records and prescribing records) and Drug Burden Index score 23 from baseline.
Number of falls, falls with injury without fracture and falls resulting in fracture, collected by solicited enquiry, records audit as well as use of a diary.
Change in frailty, measured using the FRAIL scale. 24
Physical function measured using the Self-Rating Barthel Index (MBI). 25
Cognition measured using the Telephone Interview for Cognitive Status (TICS). 26
Quality of Life, measured using the EQ-5D-5L. 27
Data collection
Baseline data collection
Baseline data were gathered by trained research staff from medical records and participant interviews. Baseline data included demographic details, and cognition assessed using the Telephone Interview for Cognitive Status (TICS) 26 ; self-reported physical function was measured by the Self-Rating Barthel Index 25 ; blood pressure; Charlson Comorbidity index 28 and Frailty screened using the FRAIL score. 24
A comprehensive medicine history was compiled using GP practice records, community pharmacy dispensing records and participant interview from either the participant or carer. This included all prescribed medicines, over-the-counter and alternative remedies, and herbal and mineral supplements (and all formulations). The generic name, indication, dosage and frequency of all medicines were collected.
Follow-up data collection
Clinical records held by the GP and GP practice, specialists, community pharmacy and hospital records were sought. Research staff reconciled medicine changes using the practice records, dispensing records from community pharmacies and the participant interview. A 5- to 10-min telephone follow-up call was made to all participants in both groups at 1 week and 3 months post-baseline. The call reminded the participant to complete the participant diary, and to aid recall, particularly of any medicines-related Adverse Events (AEs) or Adverse Drug Withdrawal Events (ADWEs) during the initial discontinuation phase. The research pharmacist recorded time spent on the intervention in field journals.
Statistical analyses
Quantitative data were analysed using a blinded intention-to-treat basis using STATA v18. Group characteristics were analysed and reported descriptively (i.e. count data, proportions, median and interquartile range as appropriate). Significance testing was undertaken using Wilcoxon rank sum and χ2 tests as appropriate. Pre-specified recruitment targets aiming to power the study for clinical endpoints were not achieved in the context of the effects of the pandemic, and the study instead predominantly focused on feasibility of the intervention.
Results
A total of 181 individuals were initially identified from multiple sources (GP/GP practice n = 138; Direct recruitment n = 43) and assessed for eligibility. Of these, 27 individuals (15%) were excluded prior to patient contact, including instances where GPs opted not to approach eligible patients or did not permit delegation of contact to the research team. In addition, 60 (33%) were excluded following screening as ineligible. The reasons for ineligibility were shown in Figure 1. Among the remaining individuals, 61 (34%) declined participation or did not respond to contact attempts. Reasons for non-participation included lack of interest, time constraints, and perceived lack of benefit, as well as perceived complexity or burden related to psychosocial factors, communication barriers, and overall frailty or health status. Practical barriers were also common, including competing health and social care demands, caregiver burden and logistical constraints. Two additional participants (1%) were excluded due to next-of-kin refusal and other reasons. This resulted in 31 participants (17%) being enrolled in the study. There were 17 GP practices that expressed interest in the study, of which 9 participated with a total of 19 individual GPs and 31 participants. Of these participants, five were enrolled through direct recruitment via the StepUp for Dementia Research register and social media advertising, and 26 through GP practices. Participants were distributed evenly between the two groups (i.e. 16 in group control and 15 in group intervention; Figure 1). The research pharmacist spent 20 min with the control group participants. The research pharmacist spent an additional 5.5 h with the participants in the intervention group (5 h 56 min), representing the time taken to deliver the intervention, which included a single comprehensive medication review, plan development, and GP contacts.
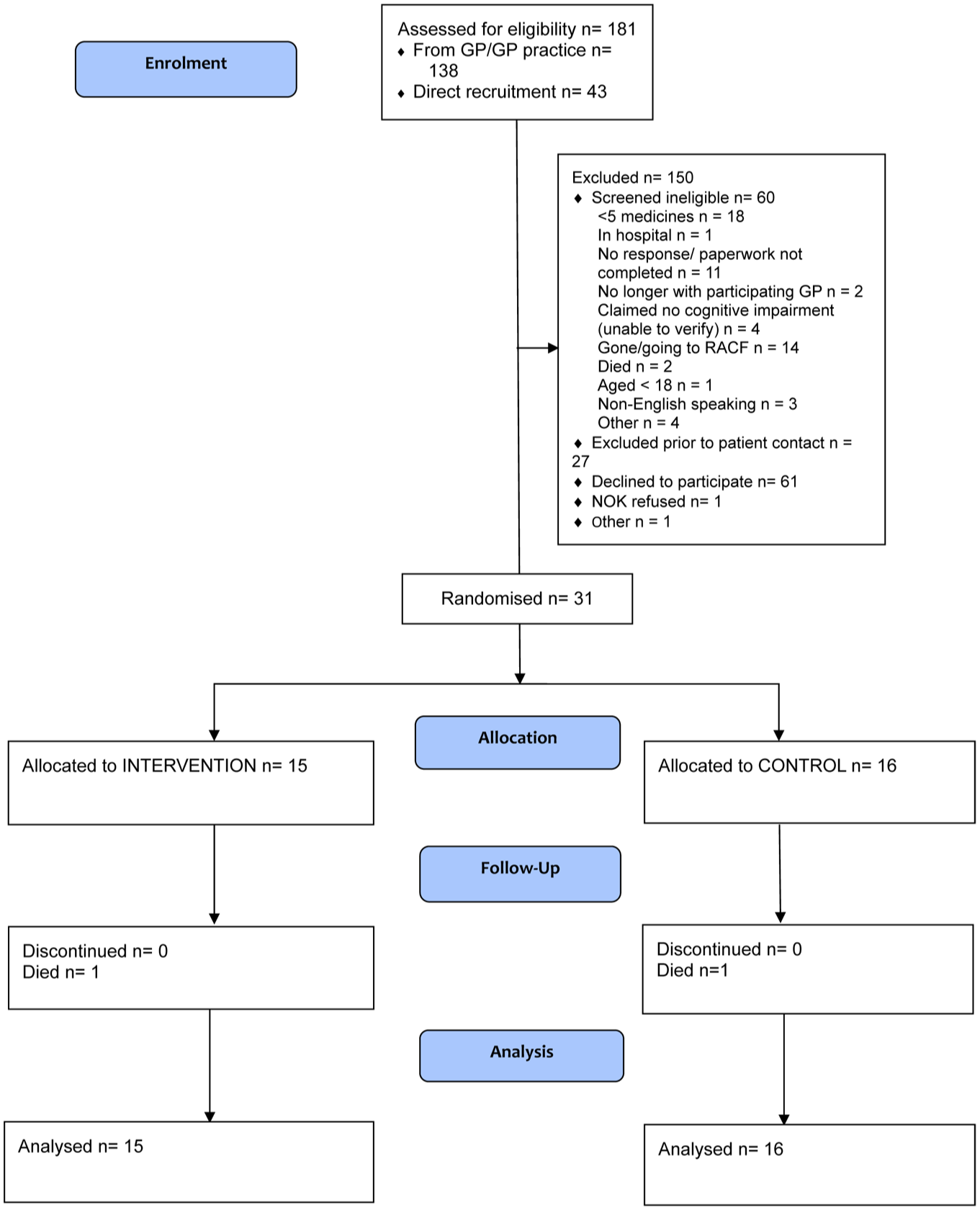
AusTAPER dem CONSORT flow diagram.
At baseline, cognitive impairment categories were determined using the interpretive ranges for the TICS total score (Table 1). Five participants in each group were classified as ambiguously impaired (score 26–32). Seven participants were classified as mildly impaired (score 21–25), including two in the intervention group and five in the control group. Thirteen participants were classified as moderately to severely impaired (score ⩽20), comprising eight in the intervention group and five in the control group. Cognitive data were missing for one control group participant as the TICS could not be completed.
Clinical characteristics at baseline and follow-up.
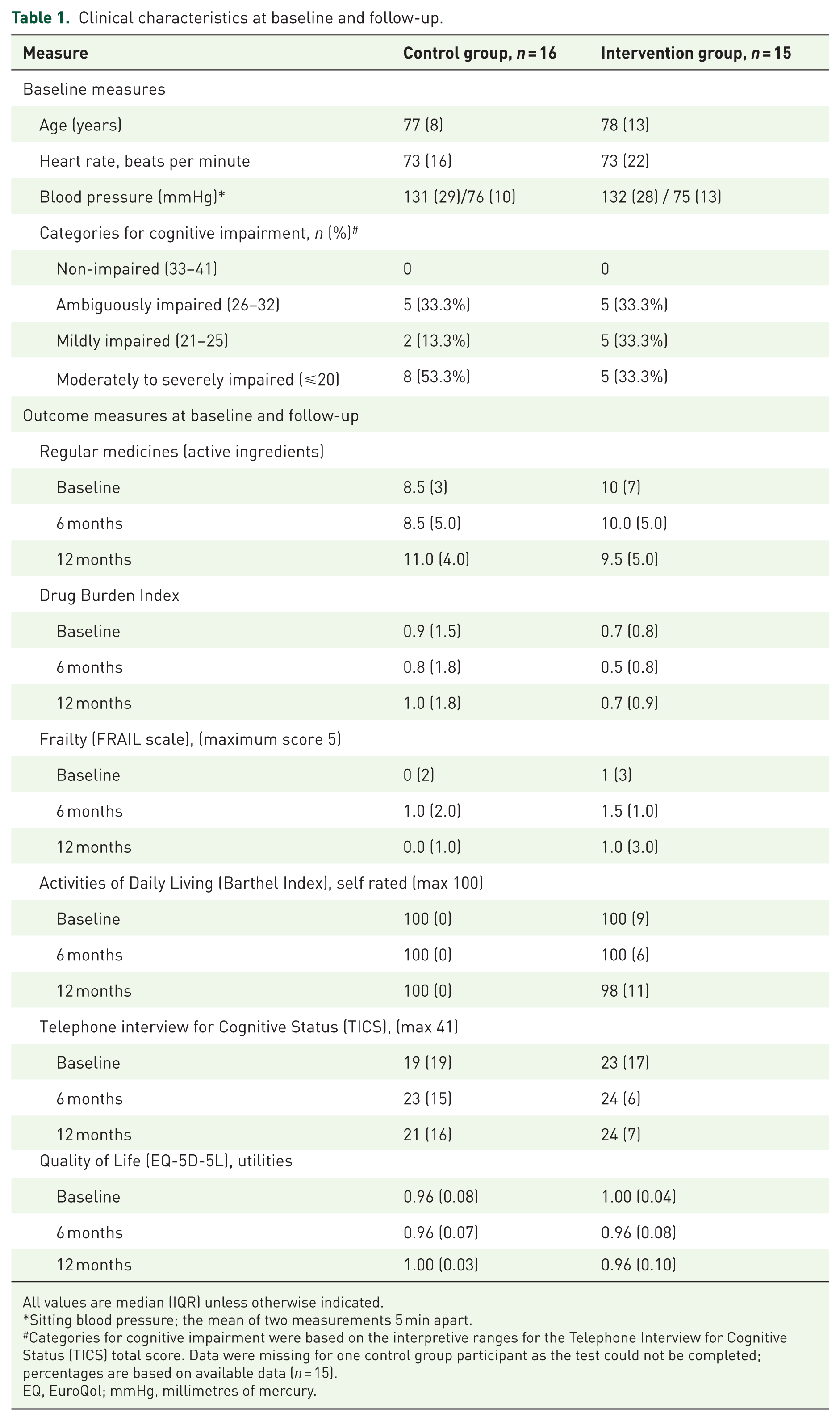
All values are median (IQR) unless otherwise indicated.
Sitting blood pressure; the mean of two measurements 5 min apart.
Categories for cognitive impairment were based on the interpretive ranges for the Telephone Interview for Cognitive Status (TICS) total score. Data were missing for one control group participant as the test could not be completed; percentages are based on available data (n = 15).
EQ, EuroQol; mmHg, millimetres of mercury.
Participants used a median + IQR of 8.5 + 3 (control group) vs 10 + 7 (intervention) regular active medicines at baseline. The baseline drug classes, categorised by Anatomical Therapeutic Chemical (ATC) classification, are available in the Supplemental Material. Regular medicines increased numerically in the control group and decreased slightly in the intervention group at 12 months (11 + 4 regular active medicines vs 9.5 + 5). At 12 months, there were 4/13 participants in the control group compared with 5/14 in the intervention who used at least one fewer medicine at 12 months compared to baseline (Table 2). No statistically significant differences were observed between the control and intervention groups at 12 months (Table 2). In the sensitivity analysis excluding over-the-counter and complementary and alternative medicines, the number of regular active medicines increased slightly in the control group and remained relatively stable in the intervention group over 12 months (Supplemental Material). Overall (combining regular and as-needed medicines), for the intervention group, the use of medicines in 14 classes increased over the 12-month period, and use of medicines in 16 classes decreased (Figure 2). In contrast, for the control group, the use of medicines in 10 classes increased over the 12-month period, and use of medicines in 21 classes decreased (Figure 3). However, there is an observed trend towards a reduction in the Drug Burden Index in the intervention group compared to baseline, especially at 6 months (0.7 ± 0.8 vs 0.5 ± 0.8), which indicates lower cumulative exposure to anticholinergic and sedative medications.
Medicines and health-related outcomes, self-reported utility and quality-adjusted life-years at 6 and 12 months (change from baseline).
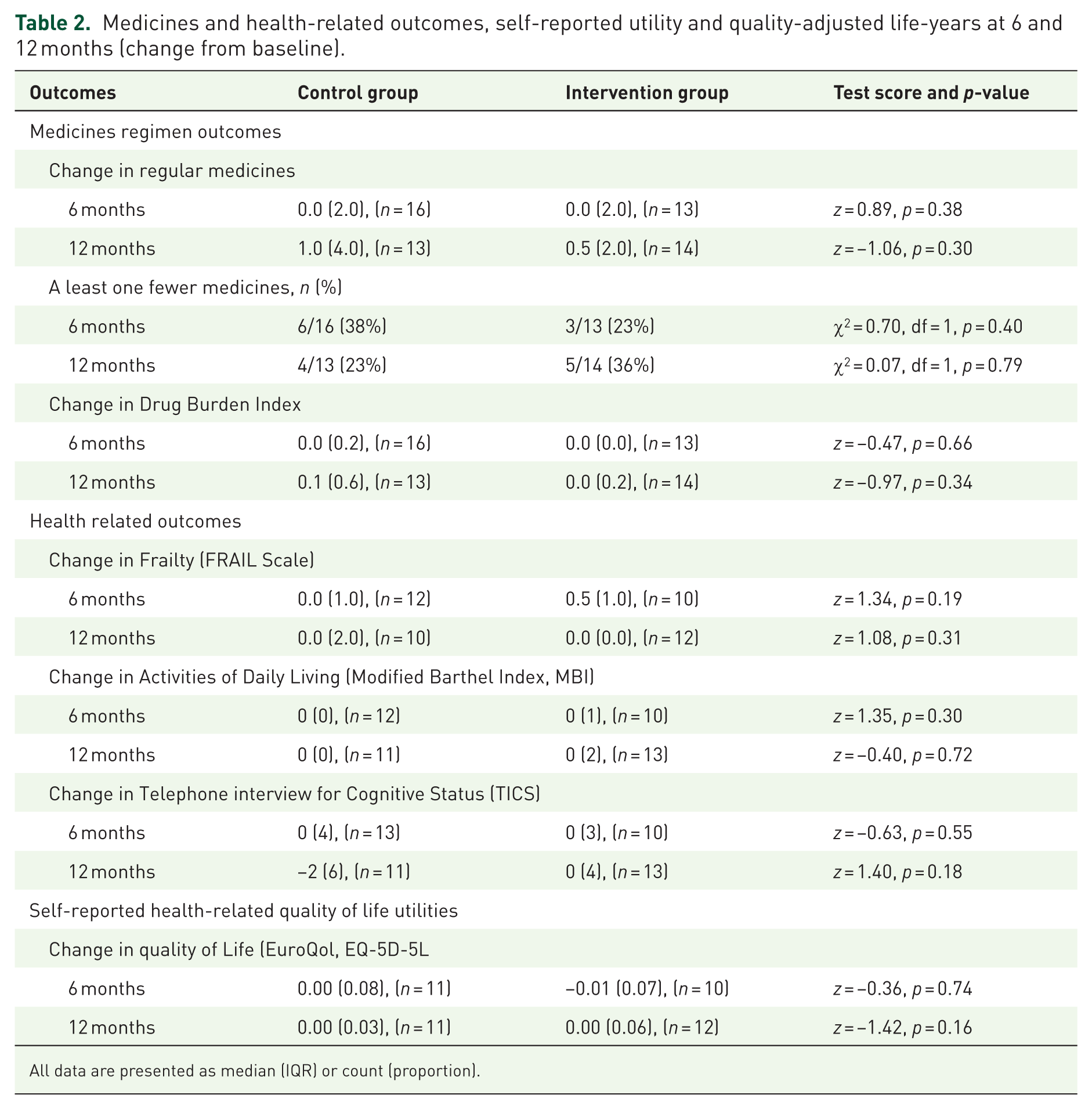
All data are presented as median (IQR) or count (proportion).
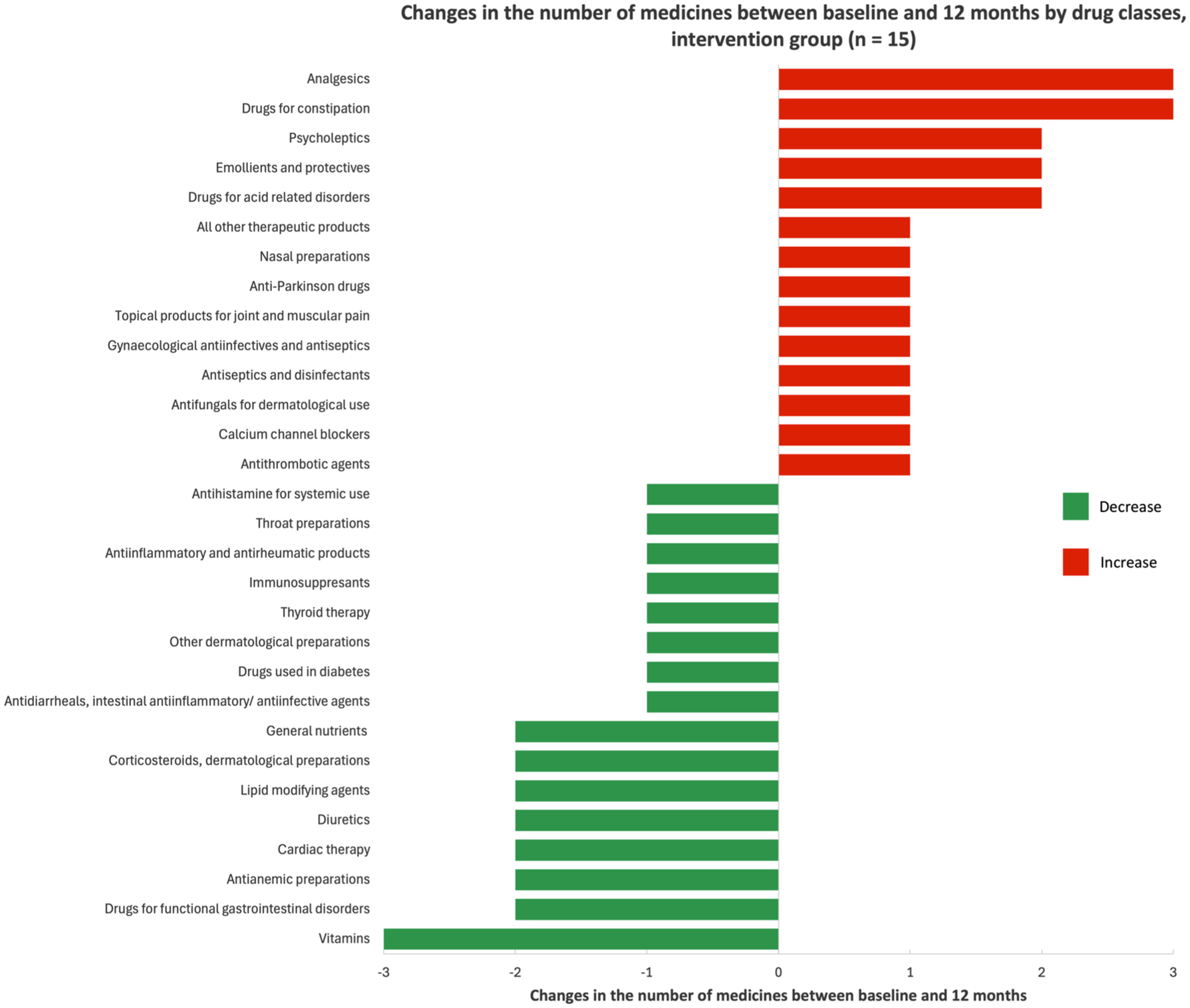
Changes in the number of medicines between baseline and 12 months by drug classes, intervention group (n = 15).
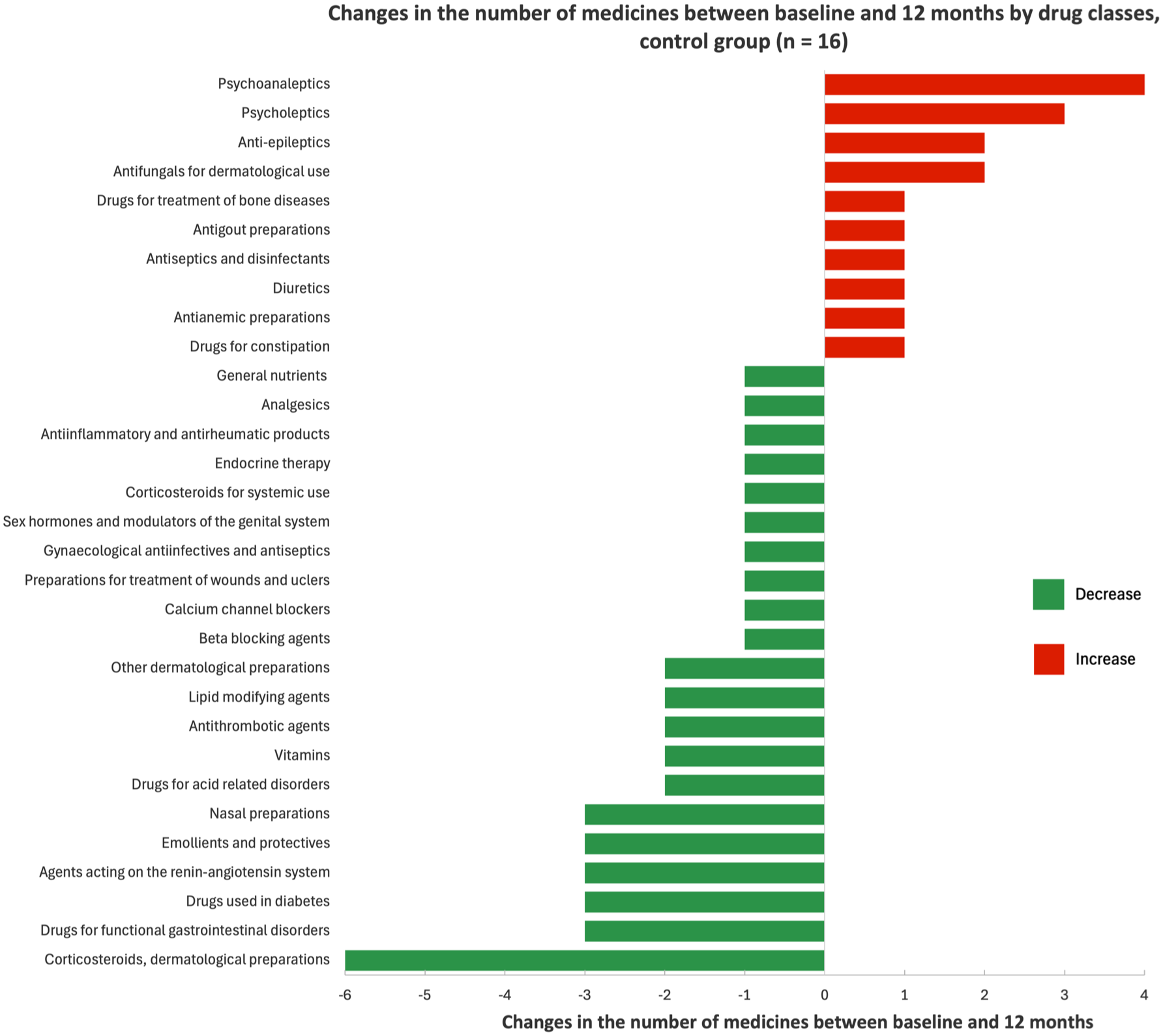
Changes in the number of medicines between baseline and 12 months by drug classes, control group (n = 16).
When examining the pattern of medication changes across drug classes in the intervention group, although total medication counts were similar between groups, the classes of medications that were started and deprescribed differed. In the intervention group, medicine increases were mostly seen in medicines commonly used ‘as required’ for symptomatic relief, such as analgesics, drugs for constipation and agents for acid‑related disorders. In parallel, decreases tended to occur in medicines commonly used long‑term for preventive or maintenance measures such as lipid‑modifying agents, some cardiovascular medicines (e.g. diuretics), vitamins and antidiabetic drugs. In comparison, increases in the control group were commonly observed in centrally acting medicines, including psychoanaleptics, psycholeptics and antiepileptics, which were commonly identified as potentially inappropriate medicines in older people. In parallel, reductions occurred across a broad range of cardiovascular, metabolic, dermatological and gastrointestinal drug classes.
Emergency department and unplanned hospital admissions
The number of emergency department presentations, resulting in either discharge or admission, and unplanned hospital admissions were statistically similar in both groups. There were a similar number of emergency department presentations (9/16 participants (56%) in the control group compared with 10/15 participants (66%) in the intervention group (1 + 1.5 vs 1 + 4, z = 1.18, p = 0.25). There were eight participants in both groups who had at least one night of unplanned hospital admissions with a statistically similar length of stay (0.5 + 5 days compared to 1 + 9 days, z = 0.44, p = 0.67). One hospital admission (in the intervention group) resulted in a new admission to residential aged care, whereas all the other people admitted to hospital were discharged to their original residence.
Health outcomes
Quality of life, independence, cognition, frailty and adverse events remained similar in both groups at each follow-up (Table 2). Falls resulting in injuries (including fracture) and health care utilisation were similar in both groups (Table 3).
Falls over the 12-month follow-up period.

All data are presented as count (proportion).
Discussion
We experienced substantial challenges in recruiting for the study, predominantly due to external factors (such as the COVID-19 pandemic) rather than challenges in engaging people with dementia and their advocates in the intervention per se, leading to a small sample size and resulting in limited power. The study did demonstrate it was feasible to engage people with dementia and their caregivers to participate in a randomised controlled trial of a medicines review intervention (although this was not a pre-specified outcome), suggesting that the intervention may be scalable. Medicines utilisation tended to increase in the control group but stayed stable in the intervention group. Allowing for the small number of participants, the number of emergency presentations, unplanned hospital admissions and health outcomes were similar in both groups across the study.
This study suggested there was a much greater length of time required for the research pharmacist to implement the intervention in this study (in the order of 5.5 h per participant) than has been identified in previous studies we have undertaken in other settings. In this study, the pharmacist performing the intervention undertook all of the activities that would normally be associated with the medicines review process, which included liaising with general practitioners and both the participant and their families.20,29 –31 Currently funded home medicines reviews can include up to two follow-up services. The intensity (5.5 h) is comparable to the time reported to be required to undertake a currently funded Home Medicines Review, including both the first and second follow-up visits that is 3.5–6.5 h.22,32 While most of this workload is undertaken by pharmacists, the time intensity may have implications for both pharmacist and GP workforce capacity as well as for the scalability within existing healthcare service models.
Although feasibility was not formally assessed in the present study, these findings suggest that elements of the intervention may be feasible within existing care structures. However, further research is needed to evaluate feasibility, acceptability and scalability in real-world settings. Given the substantial costs of medicine use, particularly for inappropriate medicines, these findings suggest that the intervention may have the potential to be cost-effective, 33 although both its economic and clinical effectiveness remain uncertain.
There was a trend, particularly in the control group, for the number of medicines to accumulate even as other medicines are withdrawn. Similar trends have been consistent across deprescribing studies,34,35 and are also observed when following older adults with multiple morbidities and dementia more generally.2,3,36 Deprescribing interventions appear to be able to reduce the trend towards increasing medicines, though may not fully abate the tendency for medicines to accumulate over time. This highlights the critical nature of regular, repeated medicines review, as opposed to time-limited specific interventions.
In the intervention group, the pattern of medication changes suggests closer alignment with geriatric pharmacotherapy principles compared with the changes in the control group, which prioritise symptom control, preservation of function and minimisation of treatment burden particularly with regard to exposure to anticholinergic and sedative medications. The increase in the number of medicines may also reflect the identification of undertreatment during structured medication reviews. These findings highlight the importance of evaluating broader prescribing appropriateness in future studies when assessing medicine optimisation interventions, particularly in a small sample which limits statistical power to detect statistically significant differences in outcomes.
Limitations
This research shows it is possible to engage people with dementia to participate in RCTs for optimising medicines regimens and successfully follow them up. However, the strategy of approaching general practices first and then identifying their patients was a major barrier to this research during the pandemic as the general practice environment was already stretched and overburdened. This resulted in no general practices being recruited in one of the originally proposed cities. Once general practices were engaged to participate in the research, it was possible to recruit people with dementia and their advocates to participate. This recruitment strategy may also introduce selection bias. Participating general practices were likely those with greater capacity or motivation to engage in medication optimisation initiatives. This may have shaped the characteristics of patients identified and invited to participate, potentially favouring those who were more engaged with their GPs or perceived by GPs as more suitable for research participation. Additionally, there was very low loss to follow-up; that is once people were recruited, they appeared to remain engaged in the research. The only losses to follow-up were due to mortality. While this supports the feasibility of the study procedures, there is a possibility that this group may differ substantially from the eligible individuals who declined participation, particularly in terms of health literacy, engagement with healthcare services, functional status, caregiver support and confidence in medicine management. Most participants were relatively physically well, functionally independent and actively engaged in daily and social activities, which could introduce volunteer bias. Furthermore, the absence of GP interviews and limited participant recall constrained our ability to evaluate shared decision-making processes and the role of caregivers in influencing medication changes. This limitation should be considered when interpreting findings related to patient involvement. Collectively, these sources of bias have implications for the generalisability of the findings. The feasibility observed in this study may potentially overestimate what could be achieved in the broader population of people with dementia. Caution is therefore required when extrapolating the findings to the broader populations, including those with lower engagement in healthcare.
Despite these limitations, this study shows that once people with dementia and their advocates are recruited, high levels of retention are achievable. However, engaging health services remains a major obstacle, particularly during times of staff shortages and low resourcing, such as during the pandemic. Known barriers to engaging people with dementia in research include limited awareness of research opportunities,12,14 which we worked to overcome through actively informing patients at participating general practices about the opportunity, use of the StepUp for Dementia Research register and social media advertising. Late in the study we added a third recruitment pathway via social media (given the limited recruitment through general practice and the StepUp for Dementia Research platform) but were unable to test this strategy for a prolonged period. Direct recruitment of people with dementia warrants further evaluation.
The low participant numbers mean that we cannot draw any reliable conclusions about the health outcomes from the study. Negative effects of the intervention on quality of life or functional state would not be expected and may be due to chance considering the small number of participants and large number of statistical tests. In addition, our participants had high functional status and quality of life, indicating a potential volunteer bias. Future interventions may need to consider strategies to address medicine appropriateness as a continual improvement approach rather than a point-in-time intervention.
Conclusion
Over 12 months, this small study observed no significant differences between groups in medicines use, clinical outcomes, or quality of life. Although the study shows feasibility in recruiting people with dementia and their doctors to a medicine review intervention, future research should consider other recruitment strategies that reduce selection bias to improve the broad representativeness and generalisability of findings.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261464335 – Supplemental material for Team approach to polypharmacy evaluation and reduction for general practice patients with dementia: the Australian TAPERDem study
Supplemental material, sj-docx-1-taw-10.1177_20420986261464335 for Team approach to polypharmacy evaluation and reduction for general practice patients with dementia: the Australian TAPERDem study by Christopher Etherton-Beer, Amy Theresa Page, Hui Wen Quek, Lynne Parkinson, Vasi Naganathan, Gillian Caughey, Julie Redfern, Rhonda Clifford, Sarah Hilmer and Dee Mangin in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
This study was supported by the National Health and Medical Research Council, Australia Project Grant GNT1139616. We gratefully acknowledge the contribution of Professor Elizabeth Geelhoed and the late Dr Kieran McCaul. JR is funded by an NHMRC Investigator Grant Level 2 (GNT2007946). GC is supported by an NHMRC Investigator Grant (GNT2026400).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.