
Abstract
Background:
Ensuring participants understand informed consent forms (ICFs) is a core ethical requirement of clinical research, particularly in psychiatry, where cognitive and affective symptoms can compromise decisional capacity. As ketamine-based interventions are increasingly studied for mental health conditions, the readability of consent materials in these trials warrants systematic evaluation.
Objectives:
To assess the readability and linguistic complexity of ICFs from ClinicalTrials.gov used in ketamine clinical trials for mental health conditions.
Design:
Cross-sectional analysis.
Methods:
We conducted a cross-sectional analysis of English-language ICFs posted on ClinicalTrials.gov for interventional ketamine clinical trials involving mental health conditions. All documents were converted to plain text and standardised for text-based analysis. Readability and linguistic complexity were assessed using established indices, including the Flesch–Kincaid Grade Level, Gunning Fog Index, Flesch Reading Ease Score, and Fry Readability Graph. Document length and estimated silent reading time were also calculated. Descriptive statistics summarised the findings.
Results:
Fourteen ketamine clinical trials met the inclusion criteria. ICFs ranged from 1681 to 8637 words (mean: 5031; median: 4622), with sentence counts from 129 to 503. Estimated silent reading times ranged from 7.0 to 36.0 min (mean: 21.4; median: 19.5). Flesch–Kincaid Grade Level scores ranged from 5.7 to 11.5 (mean: 9.8), with 13 of 14 documents above grade 8. Gunning Fog Index values ranged from 7.7 to 13.8 (mean: 11.7). Flesch Reading Ease Scores ranged from 41.3 to 73.9 (mean: 52.8). Fry Readability scores ranged from grade 6 to grade 13.
Conclusion:
Thirteen of fourteen ketamine mental health trial consent forms on ClinicalTrials.gov exceeded recommended readability thresholds. Sponsors and ethics committees should require consent materials to meet an eighth-grade reading level, verified by a documented readability assessment before approval, to support informed participation in psychiatric research.
Plain language summary
People who participate in clinical trials must receive clear and understandable information before deciding whether to take part. This information is usually provided in an informed consent form. In mental health research, this is especially important because symptoms such as low concentration, low mood, or anxiety can make it harder to process complex written information. Ketamine is increasingly studied as a treatment for mental health conditions such as depression, post-traumatic stress disorder, and substance use disorders. In this study, we examined how easy it is to read the informed consent forms used in ketamine clinical trials. We analysed informed consent forms posted on the ClinicalTrials.gov website. Only English-language forms from interventional ketamine trials for mental health conditions were included. In total, 14 consent forms met the inclusion criteria. We measured basic features of the text, such as length and estimated reading time, and applied several widely used readability formulas. These formulas estimate the level of education a reader may need to understand the text. The consent forms varied greatly in length, ranging from about 1,700 to more than 8,600 words. On average, a person would need more than 20 minutes to read a single consent form. Most forms required a reading level above what is usually recommended for health information. Thirteen of the fourteen consent forms exceeded at least one commonly recommended readability threshold. These findings suggest that many consent forms used in ketamine mental health trials may be difficult to read for people with lower reading skills or for patients experiencing mental health symptoms. Using simpler language and clearer sentence structures may help future participants better understand trial information and make more informed decisions about participation.
Keywords
Introduction
According to Good Clinical Practice (ICH E6 R3), information given to potential trial participants during informed consent must be clear, concise and easy to understand – written in simple language, free from unnecessary complexity, yet sufficient to support a fully informed decision. This is a fundamental patient right. 1 Food and Drug Administration (FDA) reinforced the same approach, emphasising the need to use understandable language in the guideline published in 2024. 2 King-Kallimanis recently confirmed that patients may feel overwhelmed by the Informed Consent Form (ICF) content, both in terms of the amount of information provided and its poor readability. 3 Since mental health patients are particularly vulnerable, great effort is needed to minimise the health disparities, inter alia, ensuring access to clinical trials that may improve prognosis and quality of life.4,5 Moreover, the informed consent process can be particularly demanding for patients with mental health disorders, especially severe mood and psychotic disorders, as these may impair decisional capacity and require additional effort from investigators and Ethics Committees. 6
Ketamine has recently gained special attention in psychiatry as a treatment option for patients with Treatment-Resistant Depression (TRD). 7 Esketamine, the enantiomer of ketamine, has been approved by the FDA for TRD and Major Depressive Disorder (MDD) with Acute Suicidal Ideation or Behaviour. In contrast, the European Medicines Agency (EMA) approval is not limited to TRD but also includes an indication for the short-term treatment of severe MDD, targeting the rapid reduction of depressive symptoms.8,9 Given ketamine’s dissociative effects, which are not essential for its antidepressant action, its use in vulnerable patients with severe mood disorders requires particular caution. Furthermore, because of its off-label status in psychiatry, providing clear and accessible patient information is essential. 10 Hence, every effort needs to be made to fulfil this need.
Readability refers to the use of systematic formulas to estimate the level of reading comprehension required to understand a written text. 11 Readability is a key factor in determining how much cognitive effort is needed to process written health information. Complex language increases the effort needed to understand and retain key trial information, especially in patients with severe mood or psychotic disorders whose decisional capacity may be impaired. Evidence shows that this capacity depends on both the nature of the disorder and the way information is presented. 12 In particular, Morena et al. emphasised that the capacity to provide informed consent should be carefully assessed and considered at every stage of the illness, whether the patient is in an acute episode or in remission. 13
Health literacy models show that people’s ability to understand and integrate information from health care providers is a key mechanism linking health literacy to decision-making and health outcomes. 14 Mantell et al. demonstrated that health literacy among patients with mental disorders is lower than in the general population; importantly for our work, an increase in depressive symptoms correlates with lower health literacy. 15 Boutemen and Miller confirm that, despite numerous studies on the importance of health literacy among patients with mental disorders, the situation is not improving. Moreover, patient education materials remain linguistically and structurally inadequate. 16 Empirical research on informed consent has consistently shown that consent forms are often written above recommended reading levels, and this mismatch can undermine participants’ understanding of key trial features.17,18 Studies that deliberately simplified and restructured consent documents have shown measurable comprehension gains across both general and vulnerable populations, including parents of paediatric patients and older adults with psychotic disorders. Dunn et al. further demonstrated that comprehension can be improved through computerised consent presentations. 19
This study evaluates the readability and linguistic complexity of informed consent forms (ICFs) used in ketamine clinical trials, assessing whether they meet established standards for comprehensible consent, especially for psychiatric patients with cognitive or emotional challenges. Using the Flesch–Kincaid Grade Level, Gunning Fog Index, Flesch Reading Ease Score and other metrics, the study aims to identify barriers to informed participation and provide evidence-based recommendations for improving accessibility. We hypothesised in advance that most ICFs would exceed recommended readability thresholds and therefore be difficult for many potential participants.
Material and methods
This was a cross-sectional analysis of publicly available ICF documents retrieved from ClinicalTrials.gov. The reporting of this study conforms to the STROBE statement, and the completed checklist is provided as Supplemental Material 3. 20 To minimise selection bias, all records meeting the a priori eligibility criteria were included consecutively, with no discretionary selection or ranking. Two reviewers (DS, AK) applied the criteria independently, and discrepancies were resolved by the senior author (WJC).
A systematic search of ClinicalTrials.gov was conducted through 8 March 2025, to identify interventional ketamine trials for mental health conditions, including substance use disorders, with publicly available English-language ICFs. Studies were excluded if they addressed non-psychiatric indications, did not use ketamine as the core intervention, were non-interventional or lacked an accessible English-language ICF. ICFs were converted to plain text, with formatting and non-textual elements (headings, tables, figures, bullet points, logos and page furniture) removed to ensure a like-for-like comparison of the core running text. Therefore, the indices reported here quantify the linguistic complexity of the textual content rather than the functional readability of the consent document as experienced by participants, since layout and navigational features that may support real-world comprehension are not captured. Readability was assessed using the Flesch–Kincaid Grade Level, Gunning Fog Index, Flesch Reading Ease Score and Fry Readability Graph, along with word and sentence counts and estimated silent reading time. Descriptive statistics were calculated in JASP (v. 0.19.3). The full search strategy and analytical procedures are detailed in Supplemental Material 2.
Results
Trial selection
A total of 42 potentially relevant ClinicalTrials.gov records were identified through the predefined search strategy (Figure 1). All 42 records were screened, and the corresponding reports were assessed for eligibility; none were removed before screening, and no reports were unavailable for retrieval. After applying the predefined eligibility criteria, 14 trials were included in the final analysis. The 28 excluded trials primarily addressed conditions outside the scope of this review (e.g. anaesthesia, pain, or head and neck cancer) or involved interventions that did not meet the requirement for ketamine to be the core study intervention, as in NCT03980067 (Virtual Reality Game) and NCT04711005 ((2R,6R)-Hydroxynorketamine).
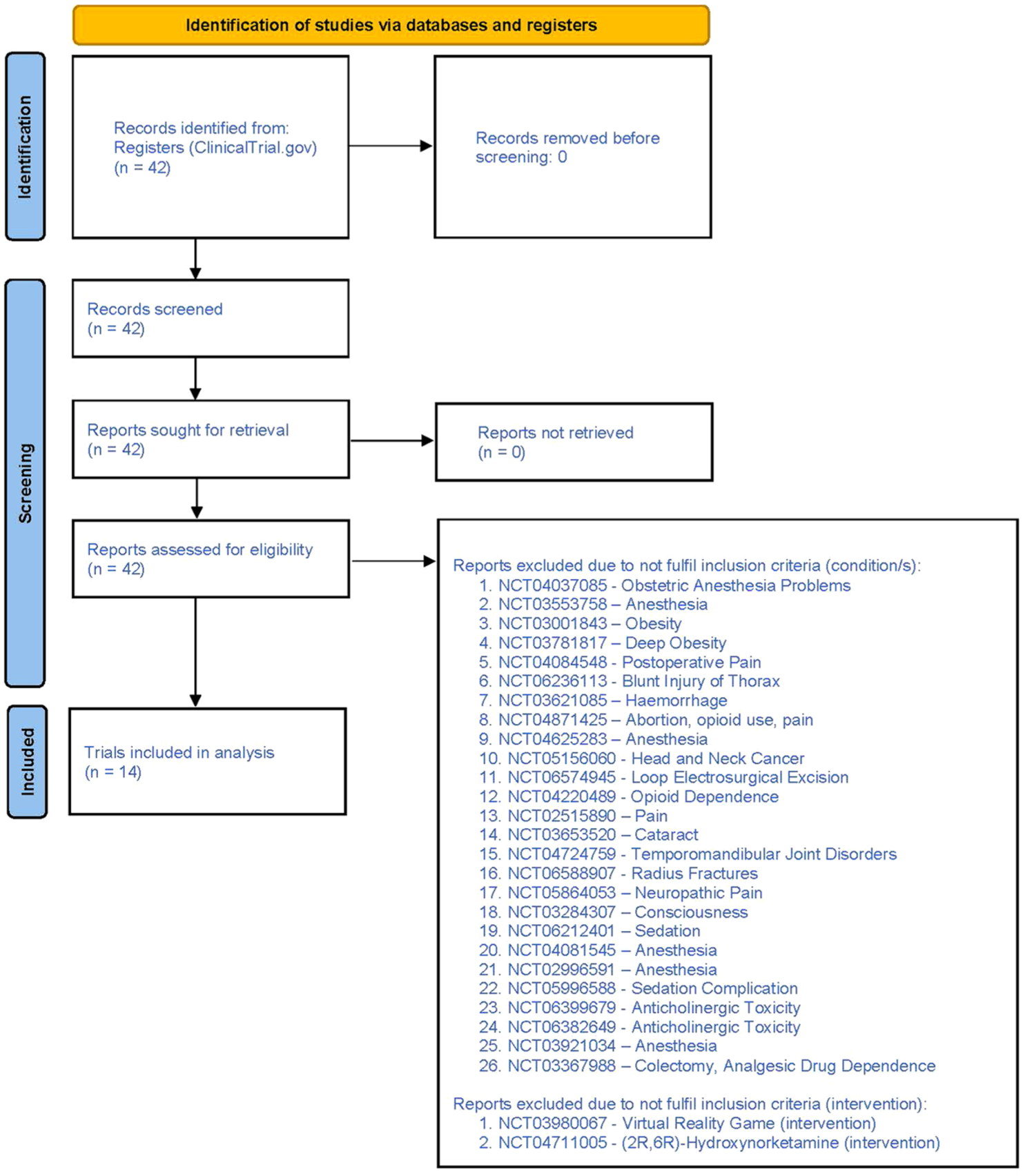
The trial selection process – flow diagram.
Characteristics of included trials
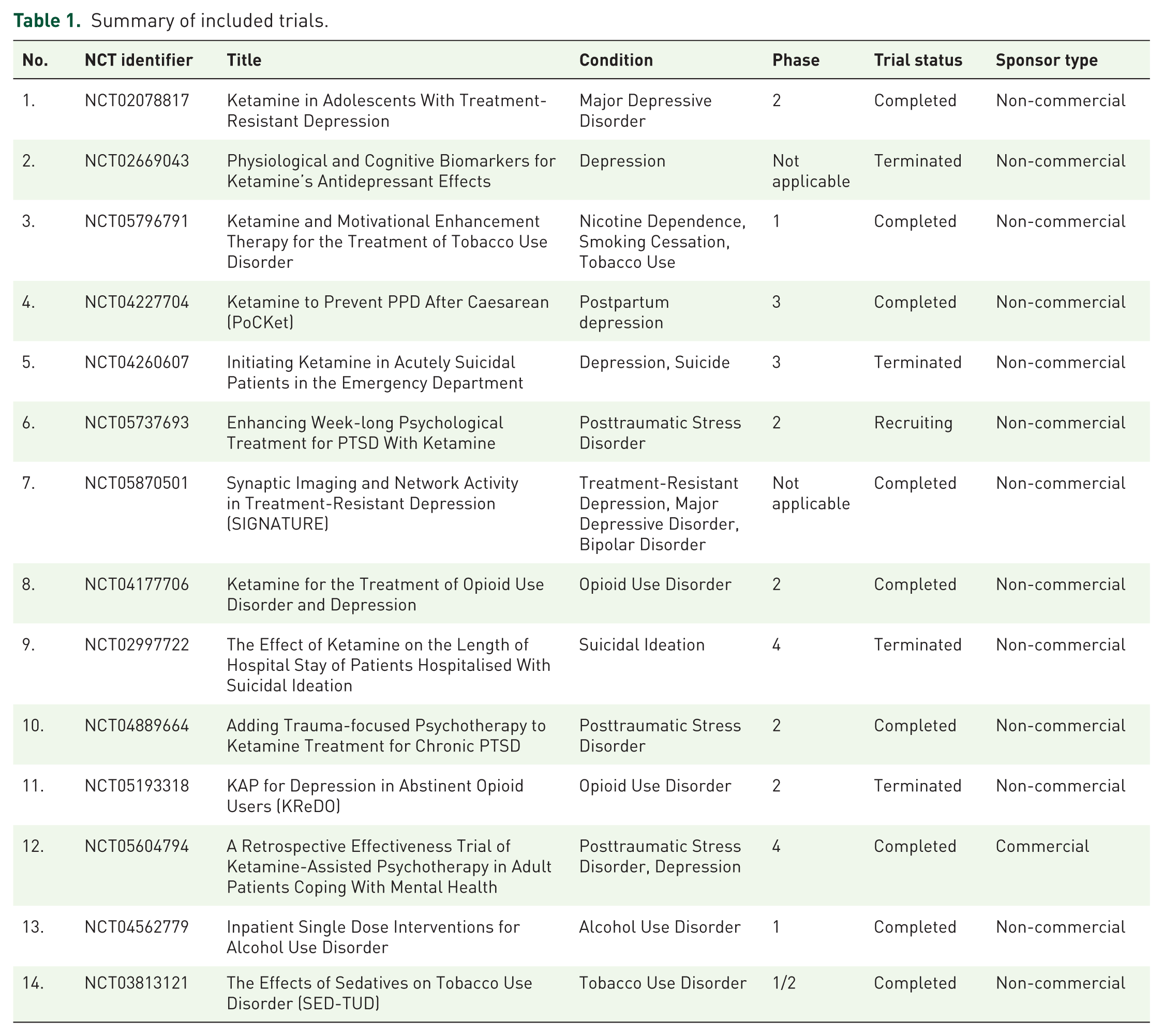
The included trials addressed MDD, TRD, opioid use disorder, nicotine dependence/tobacco use disorder, postpartum depression, posttraumatic stress disorder, suicidal ideation and alcohol use disorder. Three trials were in phase I or phase I/II, five were in phase II, two were in phase III, and two were in phase IV; two additional trials were listed on ClinicalTrials.gov as phase not applicable. Of the 14 included trials, nine were completed, one was recruiting, and four were terminated. Thirteen of the 14 trials were non-commercial. Table 1 summarises the included studies.
Summary of included trials.
Readability assessment of ICFs
Readability scores varied significantly across the 14 ICFs (Table 2). The word count for the ICFs ranged from 1681 to 8637 words, with a median of 4622 words (IQR: 3077–7123), a mean of 5,031 words (SD: 2360). Sentence count was also variable, ranging from 129 to 503 sentences. The median was 287 sentences per ICF (IQR: 234–414), with a mean of 311 (SD: 119). Silent reading time, at an average rate of 238 words per minute, ranged from 7.0 to 36.0 min. Median reading time was 19.5 min (IQR: 13.3–30.3), with a mean of 21.4 min (SD: 10.0). The Flesch–Kincaid Grade Level varied from 5.7 to 11.5, with a median of 10.0 (IQR: 9.1–10.7), a mean of 9.8 (SD: 1.5). Similarly, the Gunning Fog Index ranged from 7.7 to 13.8, with a median of 12.2 (IQR: 10.8–12.7), a mean of 11.7 (SD: 1.6). The Flesch Reading Ease Score (FRES) ranged from 41.3 to 73.9. The median FRES was 49.9 (IQR: 48.2–57.7), with a mean of 52.8 (SD: 8.2). Fry Readability scores ranged from 6 to 13, with a median of 11 (IQR: 9–11), a mean of 10. Trial-level results are shown in Table 2, and summary statistics are presented in Table 3.
ICFs’ readability – Findings.
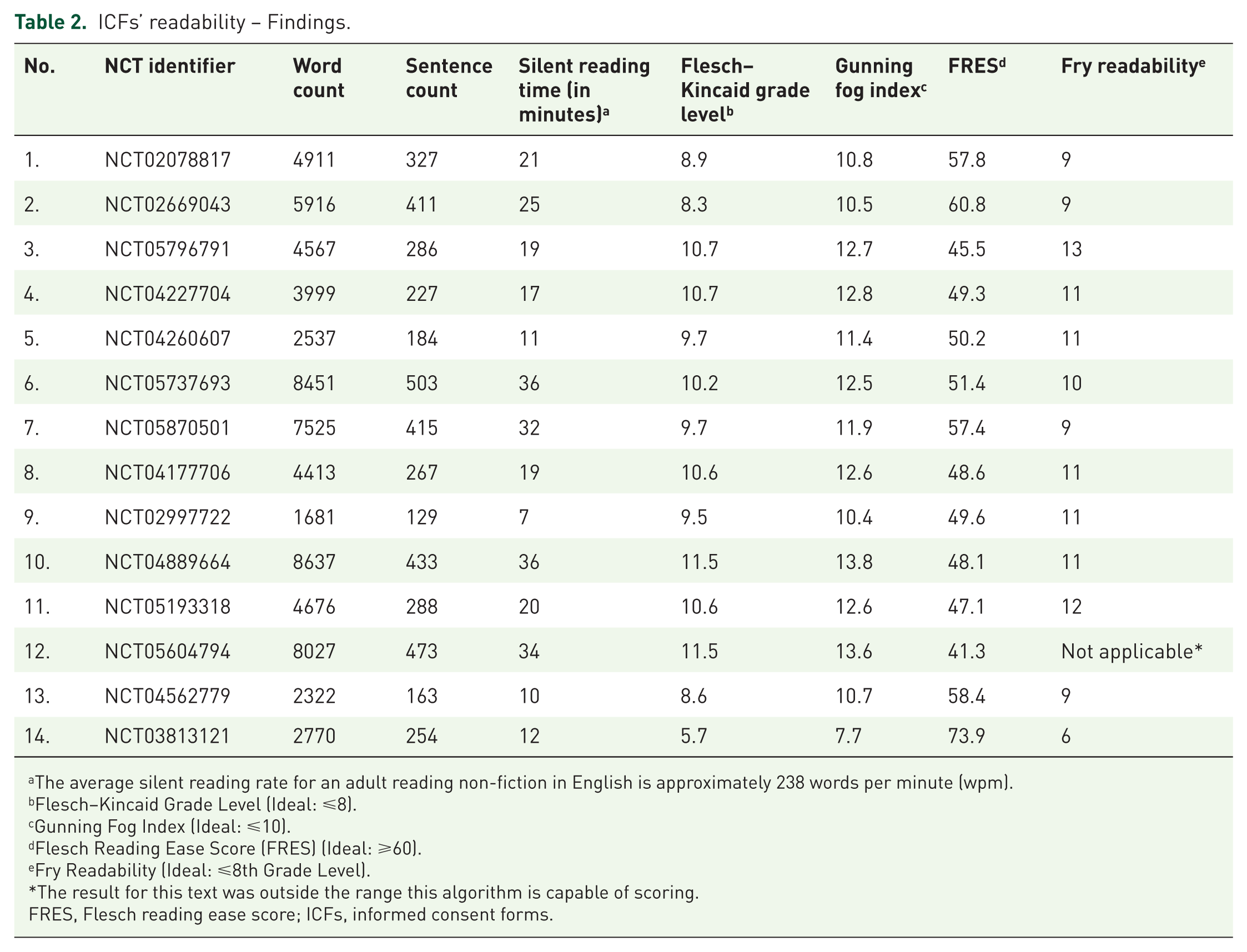
The average silent reading rate for an adult reading non-fiction in English is approximately 238 words per minute (wpm).
Flesch–Kincaid Grade Level (Ideal: ⩽8).
Gunning Fog Index (Ideal: ⩽10).
Flesch Reading Ease Score (FRES) (Ideal: ⩾60).
Fry Readability (Ideal: ⩽8th Grade Level).
The result for this text was outside the range this algorithm is capable of scoring.
FRES, Flesch reading ease score; ICFs, informed consent forms.
ICFs’ readability – summary.
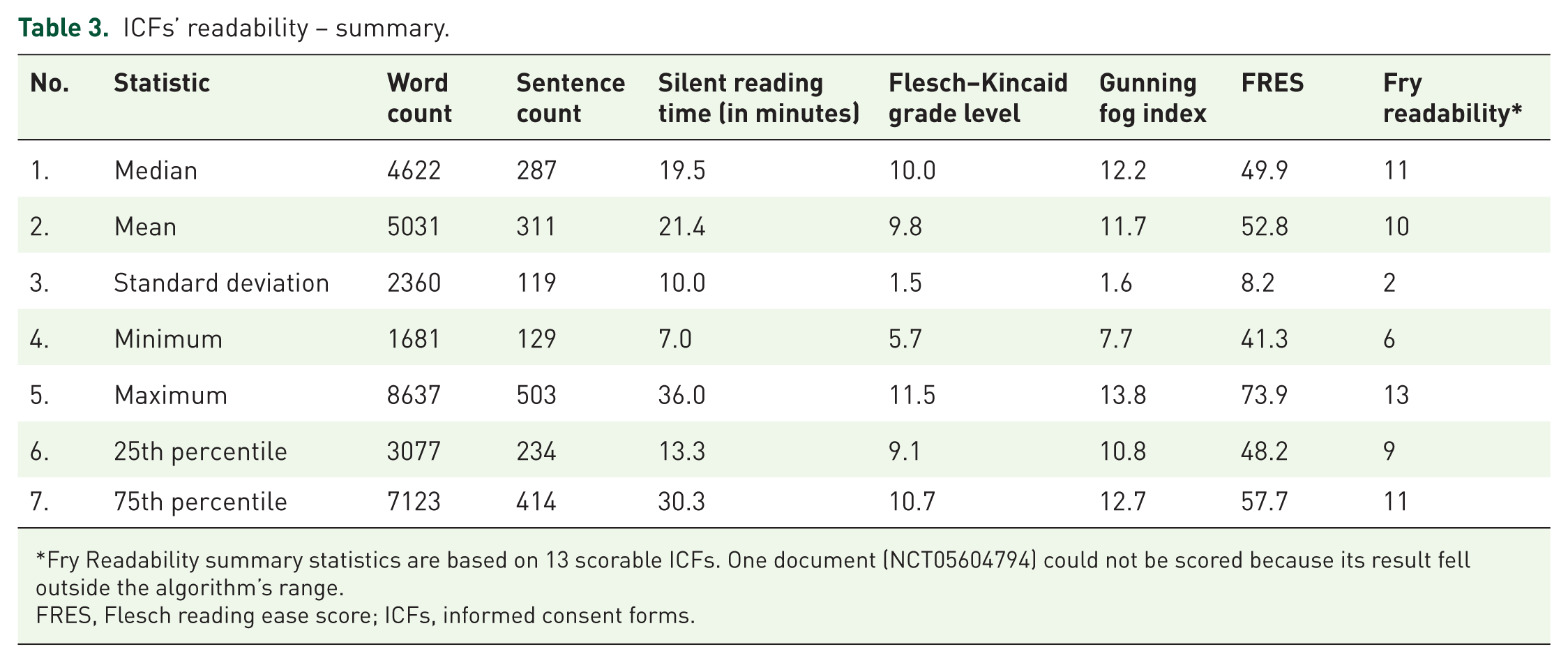
Fry Readability summary statistics are based on 13 scorable ICFs. One document (NCT05604794) could not be scored because its result fell outside the algorithm’s range.
FRES, Flesch reading ease score; ICFs, informed consent forms.
Variability in readability scores
NCT05604794 was the most linguistically demanding trial, with a Flesch–Kincaid Grade Level of 11.5, a Gunning Fog Index of 13.6, and a FRES of 41.3. Similarly, NCT04889664 showed comparable linguistic difficulty, with a Flesch–Kincaid Grade Level of 11.5, a Gunning Fog Index of 13.8, and a FRES of 48.1. In contrast, NCT03813121, identified as the least linguistically complex trial, had a Flesch–Kincaid Grade Level of 5.7, a Gunning Fog Index of 7.7 and a FRES of 73.9. Another relatively difficult trial was NCT04562779, with a Flesch–Kincaid Grade Level of 8.6, a Gunning Fog Index of 10.7, and a FRES of 58.4. Additional differences were observed in NCT02078817 and NCT05870501. NCT02078817 is 4911 words long, with a Flesch–Kincaid Grade Level of 8.9, a Gunning Fog Index of 10.8, and a FRES of 57.8. In contrast, NCT05796791 consisted of 4567 words, with a Flesch–Kincaid Grade Level of 10.7, a Gunning Fog Index of 12.7, and a FRES of 45.5. The cross-trial readability discrepancies in ICFs are summarised in Supplemental Material 1.
Discussion
Across all four indices, ICFs in ketamine mental health trials consistently exceeded recommended thresholds: the mean Flesch–Kincaid Grade Level was 9.8 (target ⩽ 8), the Gunning Fog Index was 11.7 (target ⩽ 10), the FRES was 52.8 (target ⩾ 60), and the mean Fry grade level was 10. The consistency across metrics reinforces the concern that these documents may be inaccessible to many potential participants.
These deficits carry direct ethical significance, especially in psychiatric research. Patients with MDD, TRD, psychotic disorders or substance use disorders (SUDs) often have impaired decisional capacity and overly complex consent materials increase this vulnerability by obscuring key information, raising the risk of therapeutic misconception, and compromising voluntary consent. The burden on investigators and ethics committees is therefore greater. Given ketamine’s rapid psychoactive effects, comprehension must be ensured before exposure. Our findings are consistent with broader trends in the literature: Samadi and Asghari, in their review of ICFs from 45 clinical trials in Iran, also found that most consent forms exceed the recommended grade 8 reading level. 21 Only one trial in our sample (NCT03813121) did not exceed grade 8 complexity. Fischer et al. reported similar results: analysing 75 ICFs from 35 studies conducted in South Africa, they found that these documents required high school-level literacy, with a median Flesch–Kincaid Grade Level of 10.2, comparable to 9.8 in our analysis. 22 Compared to ICFs in oncological trials, ketamine trial consent forms were harder to read: FRES scores were lower (52.8 vs 61.2) and grade levels were higher (9.8 vs 7.4). 23 ICFs in our sample were long – approximately 15 to 18 pages – and, although shorter than the 20-page median reported by Malik et al. in cancer trials, both exceed recommended standards for brevity. 24
Readability indices measure linguistic complexity in isolation; they do not account for the role of headings, white space, tables, summaries or visual aids in supporting comprehension in real-world consent documents. Therefore, scores should be interpreted as estimates of textual complexity, not as direct measures of a document’s actual readability. Moreover, discrepancies between indices highlight the inherent difficulty in quantifying text complexity. Flesch-based measures use global averages, which moderate the effect of difficult passages, while the Gunning Fog Index gives greater weight to polysyllabic words and tends to rate technical texts as more demanding. The Fry score reflects overall patterns of sentence length and syllable density. As a result, the same ICF may appear readable under one metric but challenging under another (e.g. NCT02078817, NCT05870501, NCT04562779, NCT02997722). All indices used here rely on proxies – sentence length and syllable count – and overlook semantic, contextual and layout factors; they measure linguistic complexity, not comprehension. A practical complement is to involve patients directly by soliciting qualitative feedback on ICF content. Meneguin and Ayres found that ICFs were often not read in full and that the term ‘placebo’ was frequently not understood – a finding that would not have been apparent from readability scores alone. 25 Bernardi et al. identified a gap between ICF content and participants’ perceptions, with a significant proportion believing that clinical trials guaranteed them the best available care. 26 Because informed consent is an ongoing, interactive process, readability cannot be separated from the quality of investigator–participant communication.
Prior research consistently supports this view: participant feedback on ICF content is valuable for improving readability and comprehension.27,28 Ethics Committees, as bodies responsible for approving clinical trials, should pay closer attention to the language of ICFs. At a more interventional level, Koonrungsesomboon et al. demonstrated that the Strategic Initiative for Developing Capacity in Ethical Review (SIDCER) methodology can meaningfully improve ICF quality, suggesting that a validated, step-by-step verification process may enhance overall patient comprehension.29,30 Geier et al. found that highly interactive digital consent forms significantly improved comprehension, while readability also increased but did not reach statistical significance. 31 Sponsors and investigators could adopt predefined readability thresholds and pilot test key ICF sections with target populations. Ethics committees, in turn, could incorporate readability review and its documentation into standard approval checklists, particularly for complex interventions such as ketamine-assisted psychotherapy.
While this study focused on readability rather than regulatory compliance, adherence to GCP remains essential for protecting patient rights. Nair and Ibrahim found that GCP compliance was significantly higher in industry-sponsored studies (79.5%) than in non-sponsored studies (55.8%), yet both figures fall below acceptable standards. 32 GCP compliance was not assessed in this study, which is a limitation and an area for future research. Beyond this, regulatory frameworks impose constraints on ICF language that investigators cannot fully overcome. Although guidelines such as ICH E6 R3 and FDA and European/UK regulations encourage plain language, mandatory legal elements – such as data protection, compensation and liability – are inherently difficult to simplify. This creates tension between readability expectations and regulatory requirements and likely contributes to the complexity observed in our sample.
At the same time, ICF complexity reflects not only investigators’ drafting choices but also jurisdiction-specific consent frameworks. In the European Union, the Recruitment and Informed Consent Procedure template – endorsed by the Clinical Trials Coordination and Advisory Group (CTAG) and included in the Part II application documents under the Clinical Trials Regulation (CTR), though not legally mandatory – requires sponsors to specify how participants will be approached, when and where consent will be obtained, how understanding will be assessed and what arrangements exist for non-native speakers. It also addresses withdrawal procedures and, where relevant, additional safeguards for incapacitated adults, individuals with fluctuating or borderline decision-making capacity, legal representative identification, witnessed consent and emergency enrolment. 33 European Commission guidance on the interplay between the CTR and GDPR clarifies that informed consent under the CTR serves as an ethical and procedural safeguard, not as a legal basis for processing personal data under the GDPR. Participants must also receive the information required under Article 13 of the GDPR. 34 In the United Kingdom, the Health Research Authority (HRA) relies on guidance and quality standards rather than a single mandatory template. Participant information should begin with a study-specific summary and clearly address participation, risks, benefits, withdrawal and contact details. The HRA provides sponsor wording to support data protection compliance and recommends a layered approach to information provision. 35 For clinical trials with investigational medicinal products (IMPs) involving adults who lack capacity, HRA guidance requires that legal representatives receive information in an understandable form, while participants receive information appropriate to their level of understanding. Ongoing consent must also be planned, including seeking the participant’s own consent if capacity is later regained.36,37 Within the NIH Intramural Research Programme, Office of Human Subjects Research Protections (OHSRP) consent templates require an opening ‘Key Information’ section and recommend using plain language at a sixth- to eighth-grade reading level. Specific safeguards are outlined for research involving adults who lack decision-making capacity, including NIH IRB approval and procedures involving legally authorised representatives.38,39 Taken together, these frameworks are not disease-specific, yet they share a set of cross-cutting features – plain-language or layered presentation, transparency about data use, procedures for addressing decision-making capacity, involvement of legal representatives and provisions for ongoing consent – that are particularly relevant to ketamine trials in mental health settings.
Evidence from research on ICF comprehension in other psychiatric populations, such as the postpartum cohort examined by Barrera et al., is encouraging, but these findings cannot be assumed to generalise to ketamine trials, given substantial demographic differences between postpartum depression and TRD populations. 40
Limitations
This analysis is based on a sample of 14 English-language ICFs from ClinicalTrials.gov. This set includes all documents identified under predefined criteria as of the search date, but the findings may not generalise to all ketamine trials, especially industry-sponsored or non-U.S. studies without publicly available consent documents. Thirteen of the 14 trials were non-commercial, so the observed readability patterns likely reflect academic or publicly funded research settings. Non-public ICFs from commercial sponsors were not systematically sought, as obtaining them would have required additional approvals and would have substantially altered the scope of this registry-based study. Future research could expand this work by including non-public ICFs, additional registries and non-English documents. The exclusive focus on English-language materials limits applicability to other linguistic and regulatory contexts, which is important because readability and comprehension challenges may differ in translated or non-English consent forms. We also did not systematically examine how different regulatory frameworks – FDA, EMA, MHRA, ICH – may influence ICF readability. Jurisdiction-specific requirements regarding wording, legal clauses or formatting can constrain simplification and may partly explain the complexity we observed. Country-level differences must therefore be considered when interpreting and extending these findings, as local ICFs have been shown to differ substantially from international templates in both length and guideline alignment. 41 Industry-sponsored trials may produce longer, more legally detailed ICFs due to corporate risk management practices, although these sponsors may also invest more in plain-language editing. Similarly, translated or locally drafted non-English consent forms may vary in readability depending on translation quality and local regulatory expectations. Layout features common in ICFs, such as headings, bullet lists, tables, visual aids and key information summaries, support navigation and comprehension but are not captured by readability indices. Because formatting and paratextual elements were removed during preprocessing, the reported scores reflect only the complexity of the running text and likely overestimate the document’s difficulty as experienced by a real participant. Moreover, the written document is only one component of the consent process, which also depends on dialogue, clarification and the opportunity to ask questions.
Further research
A natural extension of this work would be to assess ICF readability in clinical trials involving classic psychedelics. Marks et al. identified seven elements required in psychedelic consent forms, including perceptual disturbances, transformed metaphysical beliefs, and the potential for abuse and coercion. 42 These elements are essential for ensuring truly informed consent in psychedelic trials, yet communicating them in clear, accessible language remains a significant challenge. Further research on ICF readability in this area is therefore warranted. In practical terms, sponsors and investigators should set explicit readability targets, revise ICFs iteratively and pilot key sections with members of the target population. Ethics committees and IRBs could also require evidence of readability assessment and encourage layered consent formats with concise key information sections.
Conclusion
ICFs in ketamine mental health trials consistently exceed recommended readability levels, likely affecting comprehension among psychiatric patients. Three stakeholder-directed actions follow from these findings. Sponsors and investigators should set a prespecified readability target of eighth grade or below, revise ICFs iteratively using validated tools and pilot test key sections with members of the target population. Ethics committees and IRBs should require documented readability assessment as a standard part of protocol review and favour layered consent formats with an opening key information section. Regulators should reconcile mandatory legal language with plain-language principles, for example, by providing validated short-form templates for high-complexity clauses. Clearer, empirically tested consent materials are essential for truly informed and voluntary consent in psychiatric research.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261456385 – Supplemental material for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis
Supplemental material, sj-docx-1-tpp-10.1177_20451253261456385 for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis by Damian Swieczkowski, Aleksander Kwaśny and Wiesław Jerzy Cubała in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253261456385 – Supplemental material for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis
Supplemental material, sj-docx-2-tpp-10.1177_20451253261456385 for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis by Damian Swieczkowski, Aleksander Kwaśny and Wiesław Jerzy Cubała in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-3-tpp-10.1177_20451253261456385 – Supplemental material for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis
Supplemental material, sj-docx-3-tpp-10.1177_20451253261456385 for Readability of informed consent forms from ClinicalTrials.gov in ketamine clinical trials for mental health conditions: a cross-sectional analysis by Damian Swieczkowski, Aleksander Kwaśny and Wiesław Jerzy Cubała in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.