
Abstract
Treatment-resistant depression (TRD) and bipolar depression (TRBD) are severe, heterogeneous mood disorders associated with substantial functional impairment, elevated suicide risk and persistent unmet treatment needs. While pharmacological and psychological interventions continue to advance, many patients experience delayed, partial or unsustained benefit, underscoring the need for therapies with novel mechanisms and rapid onset of action. Ketamine and esketamine have emerged as distinctive treatments in this context, demonstrating rapid antidepressant and anti-suicidal effects, yet differing fundamentally from conventional antidepressants in their acute subjective effects, physiological profile, delivery models and misuse potential. This narrative review synthesizes evidence from regulatory guidance, clinical trials, observational studies and qualitative research to identify key patient information needs and propose practical psychoeducational strategies. Core elements include explanations of indications, mechanisms and treatment algorithms; guidance on visit preparation, scheduling and monitoring; management of acute adverse effects; counselling on suicidality and substance misuse; and tailored considerations for special populations, including older adults, women of reproductive potential and medically complex patients. Drawing on this synthesis, the review proposes a patient-centred framework for ketamine and esketamine psychoeducation, outlining key informational domains and practical tools that can be embedded within clinical services, and identifies priorities for future research aimed at optimizing patient experience and supporting the responsible integration of ketamine-based therapies into mood disorder care.
Keywords
Introduction
Treatment-resistant depression (TRD) and bipolar depression (TRBD) are severe and disabling conditions associated with marked functional impairment, reduced quality of life, elevated suicide risk and substantial health-care utilization. 1 Conventional antidepressants and mood stabilizers often provide incomplete or delayed benefit, leaving many individuals exposed to prolonged depressive morbidity and recurrent suicidal ideation. 2 These limitations underscore the urgent need for effective treatments with more rapid and robust antidepressant effects. 3
Ketamine, initially developed as a dissociative anaesthetic, and its S-enantiomer esketamine, have demonstrated rapid antidepressant and anti-suicidal effects in patients with TRD and major depression with acute suicidal ideation or behaviour. 4 Intranasal esketamine has been approved by regulators in several jurisdictions as an add-on treatment for TRD and, in some regions, for depression with acute suicidal ideation or behaviour, with a clinic-based, monitored administration model. 5 A recent double‑blind, randomized clinical trial demonstrated that esketamine monotherapy is effective for TRD, supporting its use as a stand‑alone option. 6 Intravenous (IV), intramuscular, subcutaneous, oral and sublingual ketamine are widely used off-label in specialist settings – delivered either as a medically monitored administration or, in some services, integrated with structured psychotherapy (ketamine-assisted psychotherapy (KAP) or ketamine combined with psychotherapy (KCP)) – with psychoeducational needs differing accordingly. These treatments are characterized by:
Rapid onset of action 7 ;
A distinctive profile of acute perceptual and dissociative effects 5 ;
Transient haemodynamic changes 5 ;
The need for specialized settings and staff 8 ; and
A non-trivial potential for misuse. 8
While TRD constitutes the majority of the available evidence base, TRBD and schizoaffective treatment-resistant depression represent clinically important contexts in which ketamine is increasingly considered, often with distinct safety and tolerability implications. 9 Despite this clinical momentum, no consolidated patient-centred psychoeducational framework currently exists for ketamine-based care in mood disorders, and existing safety-monitoring tools such as the Ketamine Side Effect Tool address adverse-event capture but not the broader educational needs of patients. 10 Drawing on regulatory documents, clinical trials, observational studies and qualitative research, this narrative review uniquely synthesizes patient-relevant evidence into a practical psychoeducational framework (informational domains and tools) that clinicians can embed in routine ketamine/esketamine care pathways. Finally, it highlights gaps in the evidence base and outlines priorities for future research on psychoeducational interventions in ketamine-based treatment pathways.
Methods
A selective narrative review methodology was adopted to allow integrative synthesis and critical interpretation of heterogeneous evidence spanning regulatory, clinical and experiential domains, in accordance with established guidance for narrative reviews. The conduct and reporting of the review were informed by the Scale for the Assessment of Narrative Review Articles (SANRA) framework to enhance transparency, structure and interpretability. 11 A completed SANRA checklist is available as Supplemental File 1.
A targeted literature search was conducted in MEDLINE (via PubMed) and Scopus in December 2025. Search terms were iteratively developed to capture evidence on therapeutic ketamine and intranasal esketamine across mood disorders and included combinations of the following keywords: (ketamine OR esketamine) AND (depression OR ‘treatment resistant depression’ OR ‘TRD’ OR ‘bipolar depression’ OR ‘bipolar disorder’ OR ‘TRBD’)
Eligible sources included:
Regulatory documents and health technology appraisals related to intranasal esketamine;
Pivotal, extension, and long-term safety trials of intranasal esketamine;
Observational, open-label, and naturalistic studies of ketamine in TRD and TRBD;
Qualitative and mixed-methods studies reporting patient experiences, perspectives, or preferences;
Narrative and systematic reviews addressing integrative, psychotherapy-enhanced, or service-delivery models of ketamine treatment;
Recent literature on ketamine misuse, diversion and ketamine use disorder.
Studies were excluded if they:
Focused exclusively on recreational or non-therapeutic ketamine use without relevance to antidepressant treatment;
Reported only quantitative symptom outcomes without broader clinical, experiential or safety implications;
Presented clinician or policy perspectives without linkage to patient-relevant outcomes.
Rationale for patient-centred education in ketamine-based treatment
While the Ketamine Side Effect Tool (KSET) provides a rigorously developed, four-form instrument for systematic capture of acute and longer-term adverse events, it is limited to safety monitoring and does not address the broader educational needs of patients, such as treatment expectations, preparation procedures, substance-misuse counselling or family-involvement strategies that are essential for safe and effective ketamine/esketamine care. 10
Unique features of ketamine and esketamine
Unlike traditional antidepressants, ketamine and esketamine can improve depressive symptoms within hours to days, but their acute psychoactive effects – dissociation, depersonalization, alterations in time and space and somatic sensation 10 – may be unfamiliar or frightening to patients without prior preparation. Intranasal esketamine requires monitored clinic visits, fasting or reduced intake prior to dosing, and abstinence from driving or operating machinery for the rest of the day. 12
Patients increasingly encounter information (and misinformation) about ‘ketamine therapy’ via media, social networks and direct-to-consumer clinic advertising. 13 Clear, evidence-based psychoeducation is therefore essential to:
Correct inaccurate beliefs and unrealistic expectations;
Contextualize ketamine as one component of a broader treatment plan;
Enhance informed consent and shared decision-making; and
Reduce anxiety related to acute drug effects and medical monitoring.
Patient perspectives and expectations
Qualitative studies of individuals receiving ketamine for TRD reveal that patients often approach treatment with a mixture of hope and apprehension. Many regard ketamine as a ‘last resort’ and may overestimate its likelihood of producing complete, sustained remission.14,15 Patients value 16 :
Clear explanations of what to expect during and after dosing;
Continuity of staff and consistent routines;
Opportunities to discuss the meaning and integration of the ketamine experience; and
Guidance for family members or carers.
These findings strongly support the development of structured educational protocols that accompany clinical dosing regimens.
Core content of psychoeducation
Indications, mechanisms and role in treatment algorithms
Psychoeducation should begin with a concise explanation of:
Indications: TRD, defined as inadequate response to at least two adequate antidepressant trials, and, in some jurisdictions, major depressive disorder with acute suicidal ideation or behaviour 17 ; with more limited and emerging evidence in TRBD and schizoaffective treatment-resistant depression. 9
Formulations: distinction between FDA/EMA-approved intranasal esketamine and off-label racemic ketamine (IV, IM, SC, oral, sublingual). 5
Mechanism (in accessible language): rapid modulation of glutamatergic neurotransmission and downstream synaptic plasticity, distinct from monoaminergic antidepressants.
Position in treatment algorithm: usually as an adjunct to ongoing pharmacotherapy and psychotherapy, often after failure of multiple prior treatments; in some settings, as an alternative or bridge to electroconvulsive therapy (ECT). 2
Patients should be informed that (es)ketamine is not a stand-alone cure and that response is variable; some individuals experience robust and sustained benefit, others partial or transient improvement, and a subgroup does not respond.
Visit scheduling and treatment course
Education about the treatment course should cover:
Induction and maintenance for esketamine: typically twice weekly for 4 weeks, weekly for 4 weeks, then individualized weekly or fortnightly maintenance at the lowest frequency that maintains benefit. 12
Off-label ketamine regimens: for example serial IV infusions over 2–4 weeks with possible maintenance sessions; emphasize clinic-specific protocols and ongoing evaluation of need. 18
Session duration: explain that each visit generally lasts around 3 h, including pre-dose assessment, dosing, and 1.5–2 h of observation until clinical stabilization.
Patients should be actively involved in scheduling to accommodate work, caregiving responsibilities and transport, which improves adherence and reduces missed appointments.
Preparation for the visit and treatment setting
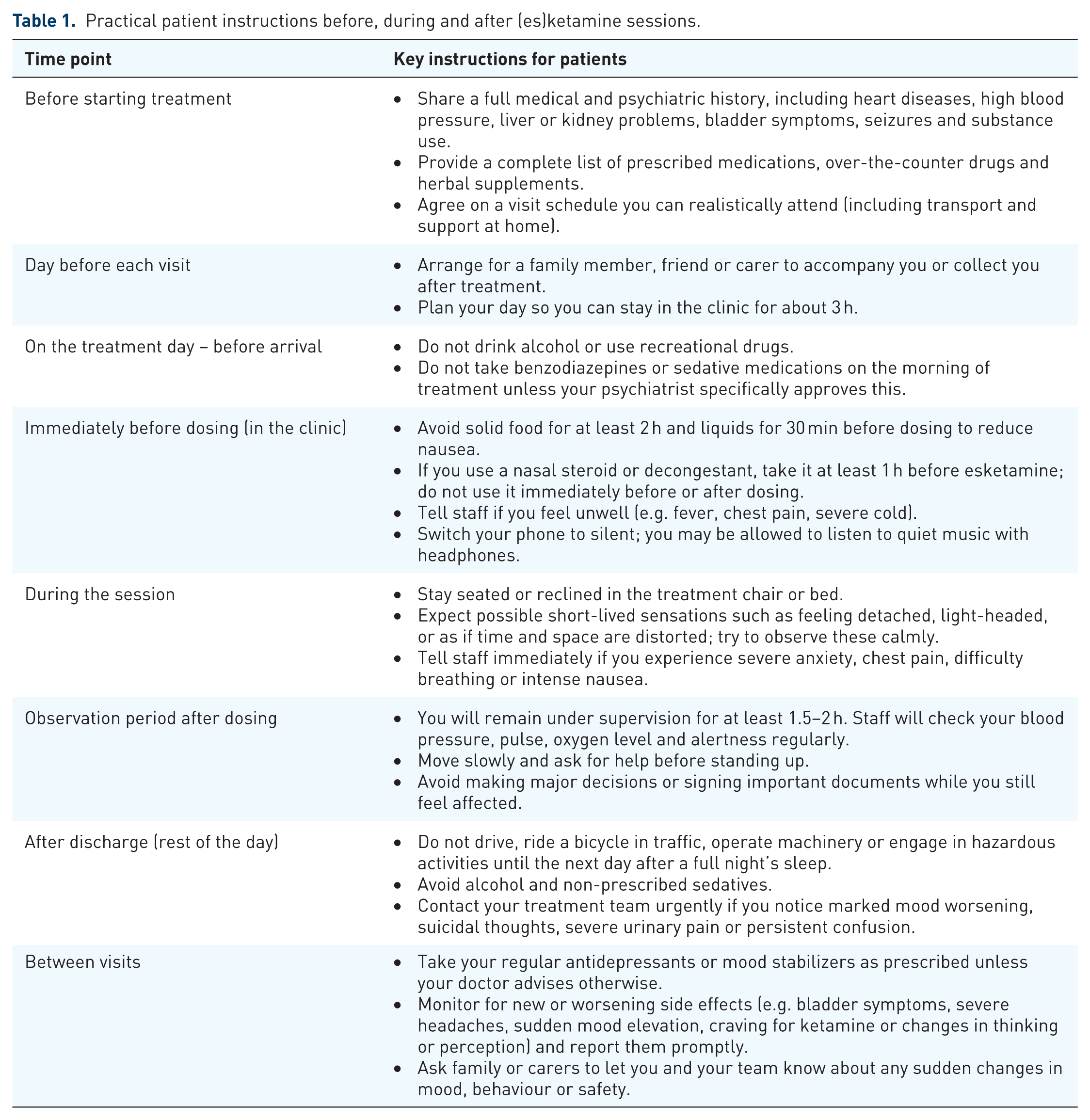
While the core preparatory instructions outlined below apply across delivery models, the framing and emphasis of pre-session education differ meaningfully between medically monitored infusion settings and psychotherapy-integrated approaches (KAP or KCP). In the latter, preparation additionally encompasses intention-setting, a discussion of how to relate to emerging emotional or perceptual material, and clarification of the therapist’s role during the dosing session; these elements are addressed further in ‘Educational models and therapeutic context’ Section. Key preparatory instructions can be summarized for patients (Table 1).
Practical patient instructions before, during and after (es)ketamine sessions.
The physical setting should be a low-stimulation environment: dim lighting, minimal noise and limited interruptions. 19 Complete sensory deprivation is not recommended, as it can intensify dissociation; a balanced, calming environment is preferable.
Adverse events: Explaining what to expect
Education about adverse events (AEs) should emphasize that most reactions are predictable, mild to moderate and resolve on the day of dosing. 20 Common AEs include dizziness, dissociation, nausea, vomiting, headache, somnolence, dysgeusia, hypoesthesia, anxiety and transient increases in blood pressure and heart rate. 20
Key messages for patients about acute AEs
Most side effects are mild to moderate and short-lived.
Cardiovascular symptoms typically start within 30–40 min, peak around 40 min, and resolve within about 1–2 h after dosing 21
You will be continuously monitored (blood pressure, pulse, oxygen level, mental state) and staff are close by throughout the session.
Dissociation (feeling detached from your body or surroundings, changes in how you see time, size or colours) is a temporary drug effect; it does not mean ‘going crazy’ or losing control.
Trying to ‘fight’ dissociation can increase distress; instead, you are encouraged to accept it as a temporary experience that will fade. In psychotherapy-integrated models (KAP or KCP), patients are additionally prepared to engage actively with dissociative or emotionally charged states as part of a structured therapeutic process; the appropriate framing of these experiences should therefore be discussed with patients in the context of the specific service model they are receiving.
Experiencing little or no dissociation does not mean the treatment is ineffective. Studies do not show a clear link between dissociation and antidepressant response.
Serious complications are rare; if they do occur (e.g. very high blood pressure, chest pain, severe agitation), the clinical team will provide immediate care and may keep you longer for observation.
For IV and subcutaneous ketamine, patients should also be informed about mild local injection-site reactions (erythema, discomfort, bruising) 22 and reassured that these typically do not require specific intervention.
Between-visit monitoring, suicidality and substance misuse
Psychoeducation should clearly state that some symptoms may emerge or change between visits, including10,12:
Transient memory or concentration difficulties;
Sleep disturbances (insomnia, vivid dreams, nightmares);
Fluctuations in mood and anxiety, including possible hypomanic or mixed symptoms in vulnerable individuals;
Urinary symptoms (frequency, urgency, dysuria);
Skin rashes or other unusual physical symptoms.
Patients must be counselled that suicidal ideation can still occur – or, in rare cases, emerge – during treatment and that any such thoughts or behaviours require immediate contact with the treatment team or emergency services, despite ketamine’s overall anti-suicidal effects.
Given the abuse liability of ketamine, education about substance misuse is critical 23 :
Clarify that intranasal esketamine and most clinic-based IV ketamine are administered under supervision only and are not dispensed for home use;
Explain the difference between controlled clinical dosing and unsupervised recreational use;
Encourage disclosure of craving, urges to obtain ketamine outside the clinic, or changes in other substance use;
Involve family or carers (with consent) in monitoring for behavioural signs of misuse or intoxication.
Pregnancy, breastfeeding and special populations
Women of reproductive potential should be informed that data on esketamine use in pregnancy are limited and that regulators generally advise against use during pregnancy and breastfeeding unless potential benefits clearly outweigh risks. 24 Contraception during treatment should be discussed, as well as the need to notify clinicians immediately if pregnancy occurs.
The elderly population appears to derive less benefit from ketamine treatment. In the primary efficacy analysis, the difference between esketamine + antidepressant and antidepressant + placebo after 4 weeks of therapy for TRD was not statistically significant. However, subgroup analyses indicated that participants aged 65–74 years, those classified as ‘younger-elderly’, and individuals whose depressive episode began before age 55 showed greater improvement with esketamine + antidepressant. 25
Because older adults often have comorbid cardiovascular, metabolic, or neurological conditions, psychoeducation for this group should:
Emphasize the need for baseline assessment and careful monitoring;
Explain why blood pressure and heart rate are checked repeatedly;
Clarify any contraindications (e.g. recent intracerebral haemorrhage, unstable cardiovascular disease).
Preliminary evidence suggests that individuals <18 years old may experience a smaller antidepressant response to ketamine than adults, and the existing data are insufficient to confirm a robust therapeutic benefit in this age group; consequently, the present narrative review excludes children and adolescents from its analysis. 26
Patients should be reassured that long-term extension studies and real-world data suggest that esketamine can be used safely in many such populations with appropriate precautions.
How to deliver patient education: Modalities and models
Psychoeducation in ketamine- and esketamine-based treatment should be conceptualized as an ongoing, structured process rather than a single pre-treatment consent discussion. Given the rapid onset of effects, the distinctive subjective experiences and the clinic-based delivery model, effective education requires repetition, multimodal reinforcement and adaptation to patient characteristics and service context
Educational modalities
Effective psychoeducation typically combines several complementary modalities:
Structured verbal counselling before induction, at each dose adjustment, and when new AEs arise.
Written materials (patient leaflets, checklists, visit-day reminders) tailored to health literacy and local language, such as those developed by NHS services and regulatory bodies.
Visual aids and diagrams illustrating the treatment timeline, potential symptom trajectory and observation periods.
Digital tools, including patient portals, SMS reminders, or secure apps, to reinforce dosing schedules, fasting instructions and safety warnings.
Family- or carer-inclusive sessions, where core messages and monitoring responsibilities are discussed explicitly.
Integration with psychotherapy or structured psychological support, particularly in KAP models, where meaning-making and behavioural change are explicitly addressed. 27
These approaches can be adapted to setting (academic centre vs community clinic), formulation (intranasal vs IV), and patient characteristics (e.g. cognitive impairment, anxiety about medical procedures).
Educational models and therapeutic context
Beyond modality, the content and framing of psychoeducation shape patient expectations, therapeutic alliance and the subjective treatment experience. 28 Psychoeducation establishes a shared understanding of the treatment rationale and promotes realistic expectations, which represent important non-pharmacological influences on outcome. Models grounded in predictive processing and Bayesian frameworks suggest that expectations function as high-level priors that influence perception and interpretation during ketamine’s period of enhanced neuroplasticity. 29 When patients understand that dissociation is a transient and non-pathological drug effect, and not a biomarker of efficacy, they may be less likely to interpret challenging experiences as treatment failure. 30
The concept of set and setting, encompassing the patient’s mindset, the physical and interpersonal environment, and prior contextual exposures, further illustrates how non-pharmacological factors modulate the intensity and meaning of acute effects. 31 Psychoeducation can therefore contribute to optimizing these contextual variables by preparing patients for altered states of consciousness, encouraging acceptance of emerging emotional material, and linking acute experiences to broader therapeutic goals. 28
In KAP models, psychoeducation explicitly prepares patients to engage therapeutically with dissociative or psycholytic effects, supporting real-time experiential processing during the acute ketamine session. These models emphasize intention-setting, guided emotional exploration and meaning-making that occur in parallel with the pharmacological effects, using the session itself as a psychotherapeutic intervention. 27 By contrast, KCP models pair ketamine’s neuroplastic and mood-enhancing effects with established, manualized psychotherapy delivered independently of the acute drug session. In KCP, the psychoeducational focus is typically on preparation for dosing, safety, and reinforcement of between-session behavioural or cognitive strategies, with integration occurring primarily through structured therapy sessions rather than in-the-moment engagement with altered states. Clarifying which model is offered within a given service helps align patient expectations, guides the focus of preparatory discussions, and supports informed decision-making. 27
The therapeutic alliance, developed through consistent, empathic and transparent communication across educational encounters, functions as a common factor that may enhance tolerability and engagement. 29 Integration, understood as the process of reflecting upon and applying insights or emotional shifts following dosing sessions, should be introduced early as a structured component of care. 32 Psychological frameworks, such as Acceptance and Commitment Therapy or related value-oriented models, may provide practical tools for translating acute experiences into sustained behavioural change. 33
Taken together, psychoeducation extends beyond the provision of procedural information. By shaping expectations, fostering alliance and supporting integration, it may influence whether ketamine’s pharmacological effects are translated into clinically meaningful and sustained benefit.
Implementation and service-level considerations
From a service perspective, embedding patient education into ketamine pathways requires:
Standard operating procedures that specify when and how education is delivered (e.g. pre-treatment orientation visit, pre-dose briefing, post-dose debriefing).
Training for clinicians and nurses in explaining dissociation, risk communication and responding to patient anxiety during sessions.
Documentation templates in the medical record for informed consent, education content delivered and safety planning.
Quality indicators, such as rates of unplanned hospital presentation after treatment, missed appointments and patient-reported understanding of treatment.
Continuous feedback mechanisms, including patient satisfaction surveys and qualitative feedback, to refine educational materials.
Staffing models typically rely on psychiatrists or other physicians experienced in ketamine treatment, supported by psychiatric nurses or other trained HCPs. Current safety data suggest that, in medically stable patients receiving sub-anaesthetic doses, routine involvement of an anaesthesiologist is not necessary if appropriate monitoring and emergency protocols are in place. Services offering psychotherapy-integrated models (KAP or KCP) in addition require staff trained in psychotherapeutic facilitation of altered states, including preparation, in-session support and structured post-session integration – competencies that extend beyond the medical and nursing training sufficient for monitored infusion settings.
Future directions
Key research gaps include:
Development and testing of standardized psychoeducational interventions (e.g. manuals, decision aids) tailored to ketamine/esketamine;
Randomized or pragmatic studies evaluating whether enhanced patient education improves adherence, tolerability and long-term outcomes;
Exploration of digital and remote support tools in maintenance phases;
Further characterization of patient preferences and experiences in diverse populations, including treatment-resistant bipolar depression, and schizoaffective TRD, adolescents, and individuals with comorbid substance use disorders;
Evaluation of how best to integrate ketamine treatment with psychotherapy and rehabilitation, and how education can bridge biological and psychological models of care.
More broadly, the field is increasingly moving toward precision psychiatry approaches, in which clinical, phenotypic and emerging biological markers may help identify which patients are most likely to benefit from ketamine-based therapies, although such approaches remain at an early stage of development. 34
Discussion
This narrative review synthesizes evidence from regulatory documents, clinical trials, observational studies and qualitative research to propose a patient-centred psychoeducational framework for (es)ketamine-based treatment in mood disorders. The central finding is that psychoeducation is not a peripheral or optional component of care but a core clinical responsibility, one that is structurally underprovided in current service models. While existing instruments such as the KSET address adverse-event surveillance, 11 no consolidated framework has previously defined the broader informational and relational needs of patients receiving these treatments – including expectation management, visit preparation, misuse risk counselling and tailored guidance for special populations.
What patients know, expect and are prepared for before and during treatment emerges as a consistent determinant of acceptability, engagement and perceived benefit. The acute dissociative and perceptual effects that accompany ketamine administration are not merely side effects to be monitored, but experiences that require contextualization and preparation. 20 When inadequately explained, these effects may provoke anxiety, loss of trust or premature discontinuation; when anticipated and normalized, they are more likely to be tolerated and integrated into the overall treatment process. 35 This reframes psychoeducation as a core clinical responsibility sitting at the intersection of prescribing practice and psychological care – yet one that current regulatory frameworks leave structurally under-specified. Prescribing authority is typically embedded within structures that emphasize medical oversight, safety monitoring, and risk mitigation, 5 with little guidance on preparation for acute psychoactive effects, management of distress during sessions or post-session integration. Where formal psychotherapeutic support is absent, the prescriber’s role consequently expands, often implicitly, beyond traditional biomedical boundaries. 27
Three mutually reinforcing mechanisms explain how psychoeducation may determine whether ketamine’s rapid pharmacological effects translate into sustained, acceptable clinical benefit. First, drawing on predictive-processing frameworks, psychoeducation recalibrates patients’ prior expectations about the likely time-course and variability of response and the meaning of acute dissociative experiences, reducing the likelihood that expected, time-limited drug effects are misinterpreted as danger or treatment failure. 29 Second, consistent with the concept of set and setting, psychoeducation optimizes the treatment context by making the monitoring environment and session structure predictable, thereby reducing uncertainty during periods when dissociation and haemodynamic effects are most prominent. 31 Third, because ketamine and esketamine are delivered through repeated, supervised sessions, psychoeducation functions as a longitudinal relationship-building process that supports the therapeutic alliance, sustaining engagement and continuity across visits rather than operating as a one-time consent event. 30 Through these mutually reinforcing mechanisms, psychoeducation may determine whether pharmacological effects translate into sustained and clinically meaningful benefit. 32
Importantly, existing safety-focused instruments such as the KSET provide robust frameworks for adverse-event monitoring 11 but do not address broader psychoeducational domains, including expectation management, visit preparation, family involvement or substance misuse counselling. 23 The present review suggests that this gap reflects a broader structural divide between regulatory priorities, often centred on pharmacovigilance and controlled access, and the lived realities of patient care, which require a more relational and context-sensitive approach. Bridging this divide may require clearer delineation of roles within interdisciplinary teams, including how responsibilities for psychological safety and patient education are distributed between prescribers, nurses and mental health professionals. 27
Qualitative studies consistently demonstrate that patients approach ketamine treatment with a complex mixture of hope, desperation and apprehension, frequently framing it as a ‘last resort’ intervention.9,16 Media portrayals and direct-to-consumer messaging further shape expectations, often emphasizing dramatic benefits while minimizing uncertainty or limitations. 13 In this context, psychoeducation serves several critical functions: correcting unrealistic beliefs, contextualizing ketamine within broader treatment pathways, normalizing transient dissociative experiences and supporting informed consent and shared decision-making. Studies exploring patient experiences with intranasal and oral esketamine suggest that clarity, continuity of care and a predictable treatment environment enhance perceived safety and acceptability. 19
The structured educational framework proposed in this review aligns with principles of shared decision-making and informed consent, while also acknowledging the practical realities of clinic-based ketamine delivery. 5 Embedding psychoeducation into standard operating procedures, staff training and service-level quality indicators may reduce preventable adverse experiences, improve adherence and support more sustainable treatment engagement. 9 At the same time, integrating education with psychotherapy or psychological support may help bridge biological and experiential models of care, particularly in patients who seek meaning-making around their ketamine experiences. Future models of care may benefit from more explicitly defined interdisciplinary structures in which prescribing authority, psychological support and patient education are coordinated rather than siloed, thereby enhancing both safety and therapeutic coherence. 27
Limitations
This review has several limitations. First, as a narrative rather than a systematic review, it does not aim to provide exhaustive coverage of all ketamine-related literature, and study selection was necessarily selective and interpretive. Second, much of the evidence informing patient education, particularly qualitative studies and service descriptions, is heterogeneous in methodology and variable in quality, limiting the ability to draw definitive conclusions about best practices. Third, there is a relative paucity of empirical studies directly evaluating psychoeducational interventions in ketamine treatment, meaning that many recommendations are extrapolated from adjacent fields or derived from clinical consensus rather than randomized evidence. Importantly, many of the psychoeducational practices described here reflect emerging professional norms and service-level innovations rather than uniformly mandated regulatory requirements, highlighting both the flexibility and variability of current ketamine care models. Finally, this review focuses on adult populations and specialist treatment settings; the generalizability of its recommendations to adolescents, older adults with significant cognitive impairment or low-resource settings remains uncertain.
Conclusions
Ketamine and esketamine represent important additions to the therapeutic armamentarium for mood disorders, particularly for individuals with TRD. Their safe, ethical and effective use, however, depends not only on pharmacological efficacy but also on the quality of patient education that accompanies treatment delivery.
This narrative review synthesizes current evidence to outline a structured, patient-centred approach to psychoeducation in ketamine-based care, encompassing expectation setting, practical preparation, adverse-event management, substance misuse risk and tailored counselling for special populations. Key elements include a clear explanation of indications and treatment goals, practical guidance on visit scheduling and preparation, a detailed discussion of common AEs and how to cope with them, explicit attention to substance misuse risk and suicidality, and tailored counselling for pregnancy, breastfeeding and comorbid medical conditions.
Beyond identifying gaps, the findings support several practical recommendations. Policymakers and professional bodies should consider defining minimum psychoeducation standards for ketamine services, incorporating core informational domains into routine care. Training frameworks should include not only medical management but also communication about psychoactive effects and management of psychological distress. Clearer delineation of interdisciplinary roles is needed to ensure responsibility for both medical and psychological safety. In addition, more standardized service models or accreditation pathways may help reduce variability in care delivery.
Standardizing these educational components and embedding them into service protocols can help clinicians deliver ketamine/esketamine therapy that is safer, more acceptable to patients and more likely to result in sustained benefit.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261456405 – Supplemental material for Patient-centred education for ketamine and esketamine therapies in mood disorders
Supplemental material, sj-docx-1-tpp-10.1177_20451253261456405 for Patient-centred education for ketamine and esketamine therapies in mood disorders by Zofia Kachlik, Wiesław Jerzy Cubała and Michał Walaszek in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.