
Abstract
Background:
Acceptability is crucial for treatment efficacy, and the World Health Organization emphasizes its impact on patient compliance. Taste plays a significant role in acceptability, with bitter taste often leading to treatment discontinuation. Clozapine, an effective drug for treatment-resistant schizophrenia, faces acceptability challenges that have been connected to its poor taste.
Objectives:
The aim of this study was to conduct, for the first time, a human taste assessment of clozapine to directly measure its level of aversiveness.
Design:
Human volunteer study.
Methods:
Employing a “swirl and spit” method, 23 young healthy adults rated the taste of four clozapine solutions (0.0011–0.018 mg/mL) on a visual analog scale (VAS) ranging from 0 (not aversive) to 100 mm (extremely aversive).
Results:
Clozapine was not aversive at any concentrations, even at saturation: mean VAS scores ranged from 5.6 to 10.3/100 (median scores ranged between 2 and 4).
Conclusion:
Reported barriers to compliance linked to taste aversiveness of marketed or extemporaneous dosage forms of clozapine may be linked to factors such as the dosage form itself, other negative formulation or excipients’ organoleptic characteristics, packaging, and user instructions linked to dosing frequency and duration, and of course, patient and disease-related factors, which require further investigations.
Plain language summary
Clozapine is an antipsychotic used for people who do not respond to other antipsychotics. It is usually taken in tablet form but sometimes patients are given liquid forms of clozapine so that carers can be sure that clozapine has been taken as prescribed. Patients often find the taste of liquid clozapine to be unpleasant, and this aversive taste may make people want to stop taking clozapine. We tested different concentrations of clozapine in volunteers. The taste of clozapine itself was not reported to be unpleasant and most people could taste nothing. We conclude that liquid clozapine has an unpleasant taste because of other chemicals (called excipients) used in making liquid formulations. Clozapine itself appears to be tasteless.
Introduction
Palatability in the context of medicine refers to the overall sensory appreciation of a medicinal product encompassing its taste, smell, aftertaste, and mouthfeel. 1 Therefore, taste can play a critical role in medication acceptability, and aversive taste often results in patient avoidance of medication itself. 2 It is well-known that taste perception depends on factors such as genetics, age, gender, presence of food, and medical condition. 3 Taste perception is also influenced by patient personality, social and psychological variables, which play a role in taste perception.
Medication acceptability is a key determinant of adherence in both adult and pediatric populations. In schizophrenia, and particularly in treatment-resistant schizophrenia (TRS), adherence to antipsychotic treatment is critical to prevent relapse and improve long-term outcomes. This is especially relevant in the context of emerging formulations, including long-acting oral antipsychotics, which aim to improve adherence through optimized pharmacokinetic and acceptability profiles. 4
Clozapine is the only effective drug for TRS. Liquid oral preparations and orally disintegrating tablets have been developed to assure adherence during supervised administration. Clozapine is a poorly water-soluble drug with a saturation solubility limit of 0.05 mM. 5 Saturation solubility is thought to represent the highest quantity of the drug that could be solubilized in the mouth, capable of interacting with taste receptors. Yet poorly soluble drugs can exhibit a bitter taste. For example, prednisolone and midazolam are among the active pharmaceutical ingredients (APIs) with the largest frequency of reports for poor taste. 6 Clozapine is a lipophilic weak base with limited aqueous solubility, characteristics that may influence its interaction with taste receptors. Additionally, excipients commonly used in clozapine formulations, including surfactants, preservatives, and buffering agents, may contribute significantly to the overall taste perception.
Aversive taste may affect adherence to clozapine. It has been suggested that clozapine has a bitter taste. 7 Also, Ramuth et al., in 1996, 8 reported that clozapine in the liquid form is unpalatable. Patient information leaflets of some of clozapine’s marketed dosage forms mention “bitterness” as a side effect. Several publications8 –10 refer to clozapine as having an aversive taste; however, the available evidence is limited and often relates to formulated products rather than the API itself. In many cases, reports of “bad taste” are anecdotal or confounded by the presence of excipients and dosage form characteristics. To date, no study has directly and quantitatively assessed the intrinsic taste of clozapine in humans.
While managing patients affected by TRS in clinical practice, clozapine dosage forms are often crushed to be administered to patients with swallowing difficulties. Tablet crushing could cause a bad taste perception by exposing the oral cavity to the chemical drug itself and other excipients, further affecting the medication discontinuation rate. 11
In addition, in several European countries, alternative routes of administration for clozapine remain limited. As a result, tablet crushing is often the only viable option for patients with swallowing difficulties, including individuals with schizophrenia or Parkinson’s disease psychosis. This practice may further impact palatability and patient acceptability.12,13
Taste-related challenges are not unique to clozapine. Several antipsychotics, including asenapine, risperidone, and haloperidol, have been reported to exhibit a bitter taste, which may negatively affect patient acceptance and adherence.14,15 These findings highlight the importance of understanding the intrinsic and formulation-related sensory properties of antipsychotic drugs.
In the present work, we aimed to investigate whether clozapine taste could affect palatability. As the human sensory analysis of clozapine taste has never been conducted before, a healthy adult panel evaluation of the taste of this drug was undertaken.
Materials and methods
Materials
Clozapine Pharma grade was procured from Fagron (Newcastle, Tyne & Wear, UK). Transparent 30 mL polypropylene universal tubes were purchased from Wheaton (Rochdale, Lancashire, UK).
Human taste assessment study design and methodology
This study was a single-blinded, randomized sensory evaluation (taste) of extemporaneously prepared aqueous solutions of clozapine.
Sample preparation
Samples were extemporaneously prepared under the supervision of General Pharmaceutical Council (GPhC; the independent regulator for pharmacists in Great Britain) registered pharmacists, under strict quality measures, and according to an internal standard operating procedure (SOP).
A stock solution of clozapine 0.018 ± 0.0008 mg/mL was prepared by fully dissolving 36 mg of clozapine in 2 L of deionized water and then filtered through a 0.45 mm Millex-GP filter (Merck Millipore, Livingston, West Lothian, UK). The concentration of clozapine was checked spectrophotometrically at 257 nm. The stock solution was accurately diluted to prepare clozapine solutions at 0.012, 0.0022, and 0.0011 mg/mL, respectively. The selected concentration range was designed to span from sub-threshold levels to the estimated saturation solubility of clozapine in aqueous media, representing the maximum concentration likely to be encountered in the oral cavity during administration of liquid or dispersed formulations.
Participant selection
Twenty-three participants were recruited from the university community (students and staff) at University College London as per the inclusion and exclusion criteria, detailed in Table 1. They signed an informed consent form to participate.
Inclusion and exclusion criteria for participant recruitment (UCL REC 4612/024).
“Swirl and spit” taste assessment protocol
Participants were instructed to swirl evenly in their mouth a 10 mL sample of the test solution for 10 s. After spitting out the sample, the intensity of test stimuli was rated using a continuous Visual Analog Scale (VAS) anchored from 0 “not aversive” to 100 “extremely aversive.” Participants were also prompted to record open-ended comments (Figure 1). Samples were rated using an electronic data collection tool (Qualtrics, Provo, UT, USA). Each participant evaluated all the samples three times, for a total of 12 blinded (coded) samples presented in a randomized order. Before and after the assessment of each sample, participants were instructed to rinse their mouth with bottled water (Buxton® Natural Mineral, Buxton, Derbyshire, UK) and eat plain unsalted-wheat crackers (Rakusen®, Traditional Matzos, Leeds, West Yorkshire, UK) to neutralize their palate. An interval of 7.5 min was maintained between samples to ensure the taste of the previous sample was no longer perceived. The 7.5-min interval between samples was selected based on established sensory analysis practices to minimize carryover effects and allow full recovery of taste perception between stimuli. Each session lasted up to 1.5 h.
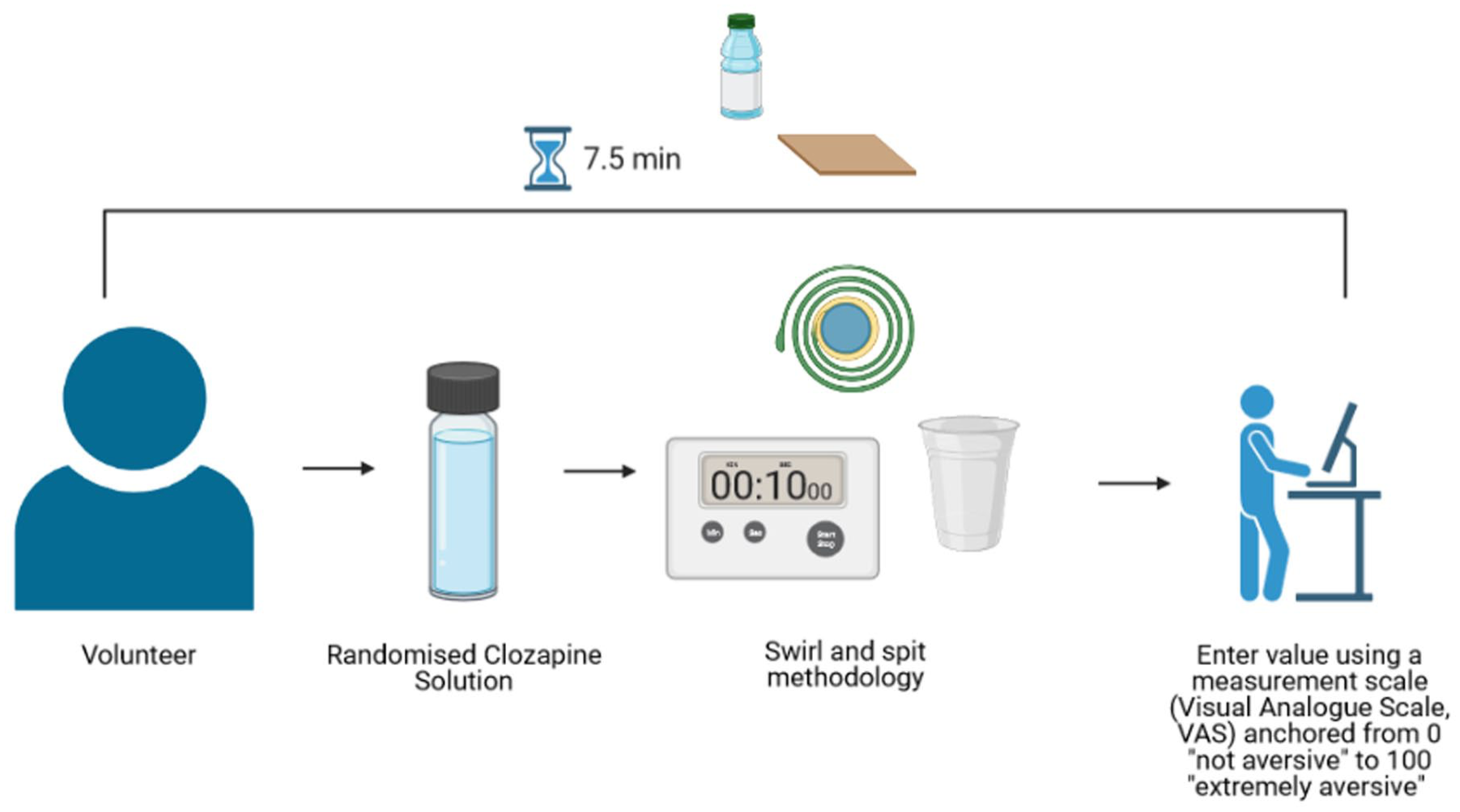
Schematic diagram of the human taste panel and swirl & spit methodology.
Human taste assessment: Data treatment and analysis
Data normality was checked with a Shapiro-Wilk test, and Gao’s post hoc analysis and the Kruskal-Wallis test were performed to check if there were significant differences in the rating of positive control between different sessions and between volunteers. All statistical analyses, boxplots generation and some graphs were done with R (version 3.0.1). Microsoft Office Excel 2016 (Reading, Berkshire, UK) was also used to produce figures.
Reporting guidelines
Strengthening the Reporting of Observational Studies in Epidemiology checklist for cohort studies was consulted in preparing this manuscript (Supplemental Material). 16
Sample size calculation
As an exploratory study, sample size was determined by convenience.
Results
Clozapine taste assessment
Twenty-three participants completed the sensory evaluation and did not report any discomfort. Results (Figure 2) showed an aversiveness rating of 5.7 ± 9.3%, 10.3 ± 15.8%, 5.5 ± 11.3% and 6.8 ± 9.6% for clozapine 0.018, 0.012, 0.0022, and 0.0011 mg/mL respectively. Shapiro-Wilk test of normality revealed the data were not normally distributed (p < 2.2e-16); therefore, non-parametric statistical tests were used for comparisons. Gao's post hoc analysis was used to look at the differences between concentrations. There was only one significant difference in mean score: aversiveness was lower for 0.0022 than for 0.0011 mg/mL (p = 0.034).
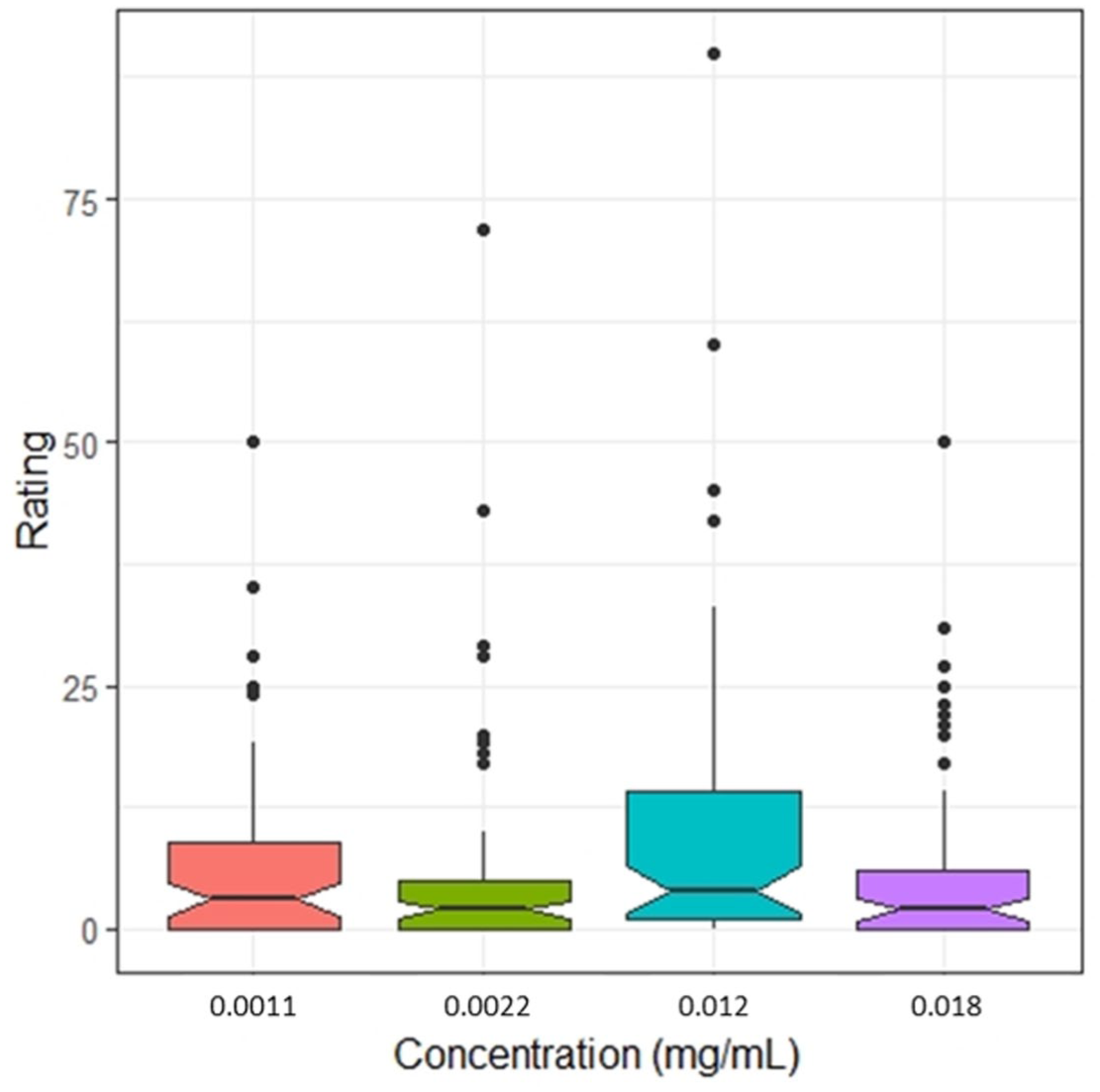
Aversiveness ratings (0 “not aversive” to 100 mm “extremely aversive”) as a function of clozapine concentration (mg/mL).
An effort was made to try to recruit a balanced number of male and female (taste naïve participants to consider the effect of sex on taste, but more females (14) participated versus males (9). Gender differences in the perception of clozapine taste were further explored (Figure 3) Aversiveness rating of 3.8 ± 4.8% (male) and 8.4 ± 12.1% (female), 11.7 ± 10.6% (male) and 11 ± 18.8% (female), 5.40 ± 11.3% (male) and 5.76 ± 12.59% (female), and 7.7 ± 9.5% (male) and 6.2 ± 9.8% (female), were measured for clozapine concentrations of 0.018, 0.012, 0.0022, and 0.0011 mg/mL respectively. There were no significant differences between male and female clozapine taste perception for the three lowest concentrations (Figure 3), but the highest concentration (0.018 mg/mL) females were significantly more sensitive. Overall, no significant differences were observed between males and females at all concentrations (Kruskal-Wallis’ test, all p values >0.05).
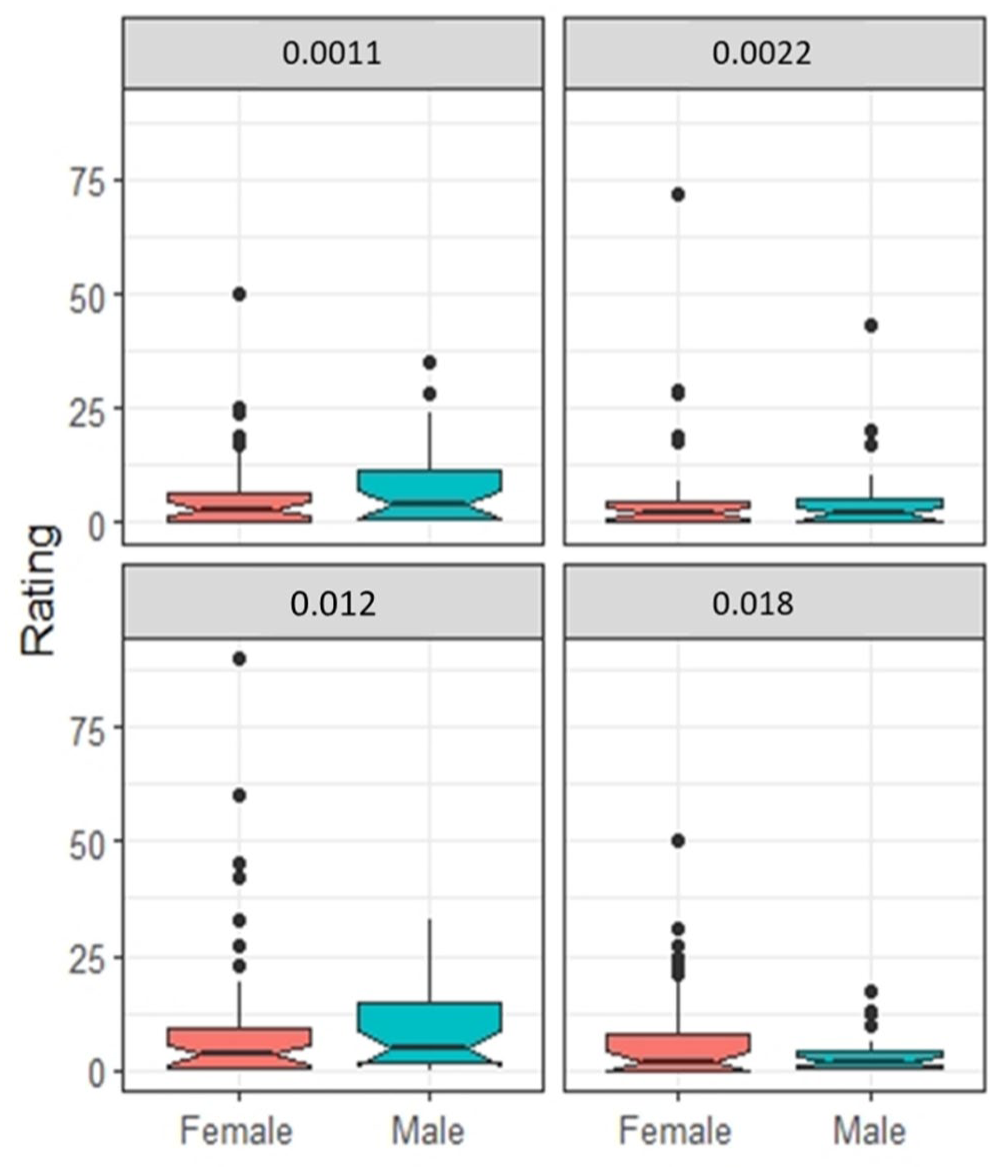
Comparison of male and female aversiveness ratings (0 “not aversive” to 100 mm “extremely aversive”) for each clozapine concentration (mg/mL).
Candidates did not perceive any taste from the solution compared with “plain water” available to neutralize the palate between each sample. The taste was described as “not aversive” or “like water” by almost all volunteers. Only one participant has stated an 'unpleasant feeling' for 0.018 mg/mL, while for concentration 0.012 mg/mL, two identified a “slight aversive after taste.” However, most of the comments for all solutions reported a watery taste, not aversive and acceptable, confirming the scores collected. Perceptions are summarized in Figure 4.
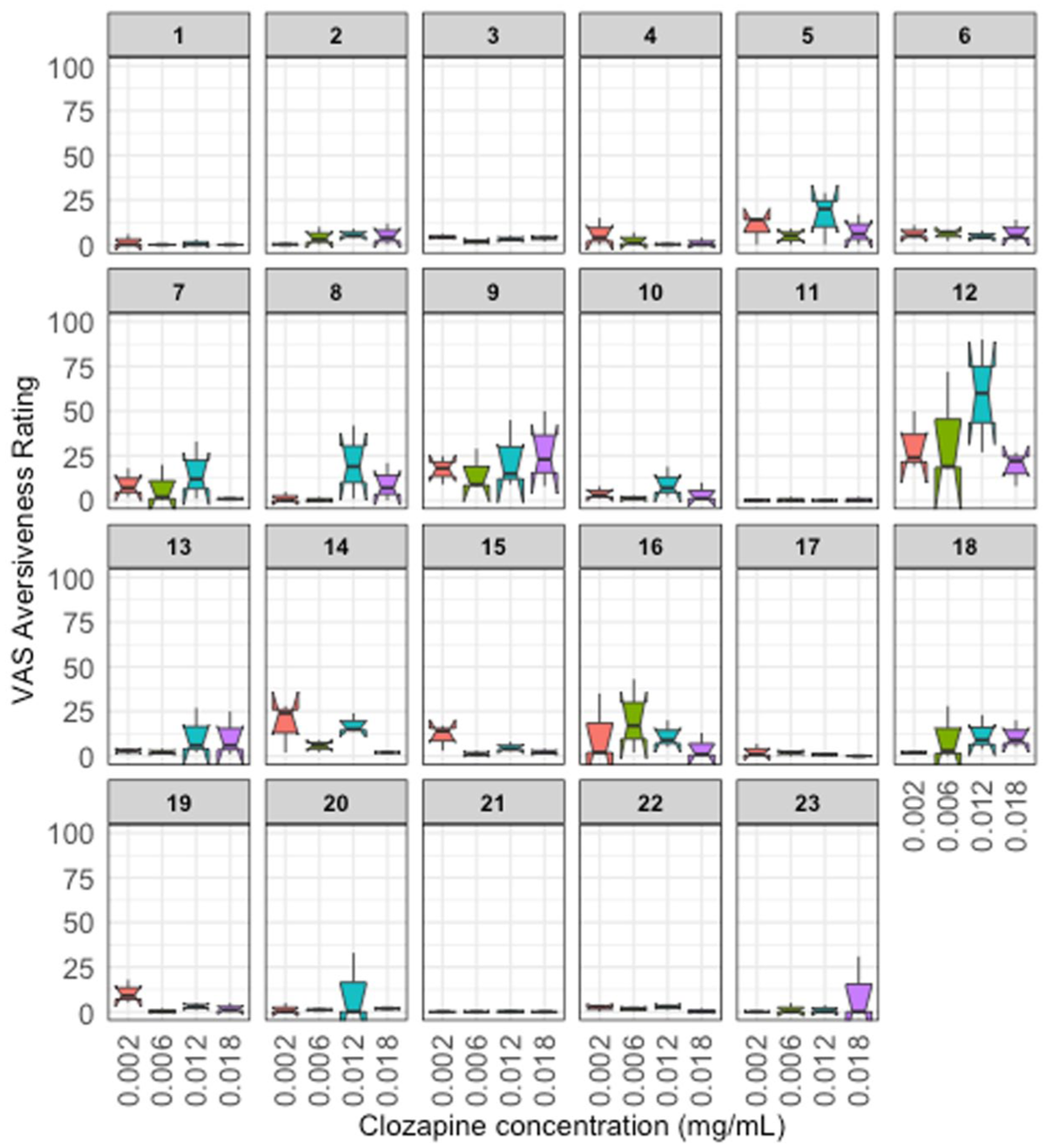
Individual aversiveness ratings (0 “not aversive” to 100 mm “extremely aversive”) as a function of clozapine concentration (mg/mL).
Discussion
The present findings provide an important clarification in the context of existing assumptions regarding clozapine palatability. While clozapine is often described as having an unpleasant taste, our results suggest that the API itself is not intrinsically aversive. This supports the hypothesis that the negative sensory experiences reported in clinical practice are more likely attributable to formulation-related factors, particularly excipients and dosage form characteristics.
In the present study, we quantitatively assessed clozapine taste through a human taste assessment study based on the “swirl and spit” method, which is designed to reduce bias and variability in the volunteers’ responses. 17 No trend was detected while increasing the drug concentration, even though clozapine permeability and chemical structure do suggest that the drug is able to bind G-proteins (typical of the T2R family), and therefore generating taste perception. 18
Due to clozapine’s low water solubility, saturation solubility (0.018 mg/mL) represents the highest quantity of the drug available in the mouth that can interact with taste receptors. 19 It could be that the taste threshold was not reached at the concentrations tested. Taste perception is influenced by multiple individual factors, including sex, hormonal status, genetic variability, smoking habits, and personal preferences. Although no major sex-related differences were observed in this study, these variables may contribute to inter-individual variability.
The World Health Organization (WHO) establishes that medication acceptability has an influence on patient compliance, thus on treatment efficacy and safety. 20 Medication acceptability pertains to the carer and patient’s ability but also willingness to use a pharmaceutical product as intended. 20 This encompasses aspects such as dosage form swallowability (dose size or volume) and palatability (smell, taste, mouthfeel, after taste), formulation (composition, appearance including tablet size, shape, color), ease of use/manipulation required, dosing frequency, packaging, medical/dosing devices, container closure systems, and accompanying user instructions (product label and package leaflet), ease transport and storage.20,21 Previous research has highlighted the complexity of bitter taste perception and its impact on medicine acceptability, emphasizing the role of both molecular interactions with taste receptors and formulation characteristics in shaping patient experience. 19 If tablets are crushed, they will be chalky, pasty to ingest, and might have a detrimental effect on palatability, more so than the taste of clozapine itself. Liquids can have an undesirable viscous mouthfeel; they contain excipients in larger quantities, whose taste might be more challenging.
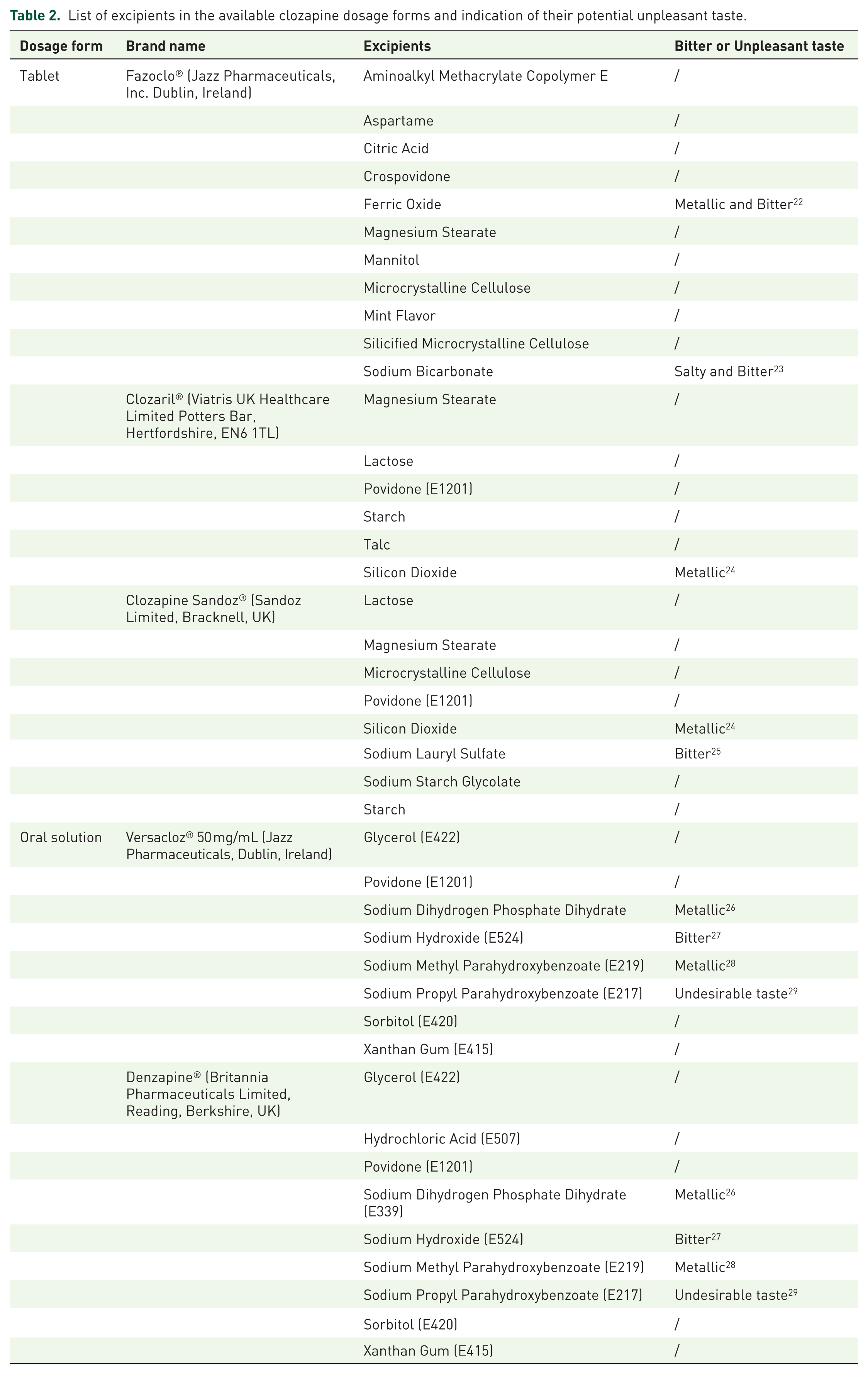
Excipients are major components of medicines, and understanding excipient sensory characteristics that may ultimately impact the palatability of the final formulation could provide some explanation. As dosage forms are often crushed to overcome swallowability issues, the excipients formulated in the marketed dosage forms of clozapine were reviewed to provide insights on those that could affect taste perception and overall palatability, as they could be responsible for a negative mouthfeel. Table 2 reports that each formulation contains at least one excipient that could be unpalatable.
List of excipients in the available clozapine dosage forms and indication of their potential unpleasant taste.
Limitations
This study presents several limitations that should be considered when interpreting the findings. First, the sample size was relatively small (n = 23) and determined by convenience, which may limit the statistical power and the generalizability of the results. Although this number is consistent with exploratory sensory studies, larger cohorts would be needed to confirm these findings. Second, taste perception is inherently subjective and can be influenced by individual variability, including genetic, psychological, and environmental factors. Although the use of a VAS provides a quantitative measure, it still relies on self-reported perception and may introduce variability. Third, the study assessed clozapine in its unformulated state. Therefore, the findings may not fully reflect the sensory experience of marketed formulations, where excipients and dosage form characteristics play a significant role in palatability. Fourth, Potential confounding factors such as smoking status, hunger state, or recent upper respiratory conditions were not systematically controlled, which may have influenced individual taste perception.
Conclusion
This study demonstrates that clozapine, as an active pharmaceutical ingredient, does not exhibit intrinsic taste aversiveness. These findings highlight the potential role of formulation components, particularly excipients, in shaping the overall palatability of clozapine-containing products. Optimizing excipient selection represents a key opportunity to improve medication acceptability and, consequently, treatment adherence, not only in pediatric populations but also in adults requiring long-term therapy.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261458524 – Supplemental material for Assessment of clozapine taste in healthy volunteers: evidence for non-aversive sensory profile
Supplemental material, sj-docx-1-tpp-10.1177_20451253261458524 for Assessment of clozapine taste in healthy volunteers: evidence for non-aversive sensory profile by Laura Modica de Mohac, Alex Keeley, David Taylor and Catherine Tuleu in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.