
Abstract
Background:
Amisulpride is an important antipsychotic used in the treatment of schizophrenia, yet its exposure shows inter-individual variability. Although therapeutic drug monitoring (TDM) is recommended, supratherapeutic concentrations (>600 ng/mL) still occur in routine practice and may increase the risk of adverse effects. However, practical risk prediction studies of supratherapeutic amisulpride exposure based on routine clinical variables remain limited.
Objectives:
To identify patients at increased risk of supratherapeutic amisulpride exposure in routine psychiatric care and to develop a clinically interpretable risk prediction approach based on routinely available clinical variables.
Design:
This was a retrospective observational study using real-world TDM data from psychiatric inpatients.
Methods:
Therapeutic drug monitoring data were retrospectively analyzed. Patients were split at the patient level into training (70%) and validation (30%) cohorts. To identify the optimal representation of renal function and drug elimination, predictors were organized into three candidate pools: (i) apparent clearance (CL/F) calculated from the final covariate equation of a previously published population pharmacokinetic model, (ii) estimated creatinine clearance (eCLcr), and (iii) the original clinical variables used to calculate eCLcr. Within each candidate predictor pool, predictors were screened using LASSO-penalized logistic regression and then entered into multivariable logistic regression. The most clinically practical model was selected for nomogram construction. Model performance was assessed by discrimination, calibration, and decision curve analysis.
Results:
A total of 413 steady-state trough samples from 299 patients were analyzed, of which 19.6% exceeded a steady-state trough plasma concentration of 600 ng/mL. Reduced renal function and higher daily doses were consistently associated with an increased risk of supratherapeutic exposure. Among the three candidate strategies, the Key Covariate-based strategy achieved acceptable discrimination in both the training (area under the receiver operating characteristic curve (AUC) 0.738) and validation (AUC 0.720) cohorts, with good calibration. Decision curve analysis suggested potential clinical utility across a range of lower to moderate threshold probabilities.
Conclusion:
A simple risk stratification approach based on eCLcr and daily dose may offer a reference for individualized risk assessment. This model may provide preliminary support for identifying patients at risk of supratherapeutic exposure in routine psychiatric practice.
Plain language summary
Background Amisulpride is a common medication used to treat schizophrenia. While it is effective, having too much of the drug in the blood, known as “supratherapeutic exposure,” can increase the risk of side effects. It would be helpful to predict who is at risk before a high level occurs. Why was this study done? The researchers wanted to create a simple, easy-to-use tool for doctors to identify patients at risk of having excessively high drug levels. While complex computer models exist to predict drug behavior, they may require specialized expertise and software, which can limit their use in routine clinical practice. What did the researchers do? The team looked at data from 299 patients at the Xi'an Mental Health Center. They compared three different methods to predict high drug levels based on factors like age, weight, dose, and kidney function. They then developed a “nomogram,” a simple chart that allows a doctor to quickly calculate a patient's risk. What were the results? The study identified that a patient’s kidney function (measured by estimated creatinine clearance) and daily dose were the main predictors associated with a higher risk of excessive drug levels. The newly developed chart demonstrated satisfactory predictive accuracy in identifying patients at risk of exceeding the safety threshold. In this study, approximately 20% of the blood samples analyzed were found to be above the predefined upper concentration threshold of 600 ng/mL. How will this help patients? This tool allows doctors to identify high-risk patients early using routinely available clinical information, including kidney function and daily dose. By knowing which patients are likely to have high drug levels, doctors can consider earlier blood-level monitoring, closer follow-up, or more cautious dose titration to ensure their treatment is both safe and effective.
Introduction
Schizophrenia is a severe and chronic mental disorder associated with a substantial disease burden and long-term management challenges. 1 Amisulpride, a substituted benzamide antipsychotic with high affinity for dopamine D2 and D3 receptors, is widely used in the treatment of schizophrenia. Owing to its dose-dependent pharmacodynamic profile, amisulpride is prescribed across a broad dose range in routine clinical practice. Although not FDA-approved for the treatment of schizophrenia in the United States, amisulpride is included as a recommended antipsychotic option in schizophrenia treatment guidelines and remains widely used for the treatment of schizophrenia in more than 50 countries worldwide.2–4
Amisulpride is characterized by rapid absorption and a biphasic plasma profile with peaks appearing at approximately 1.5 and 3 to 4 h post-dose. Its absolute bioavailability is approximately 48%, and it exhibits low plasma protein binding. 5 Amisulpride is predominantly eliminated unchanged via the renal route, with an elimination half-life of approximately 12 h that typically requires twice-daily dosing to maintain steady-state concentrations.6,7
Regarding therapeutic drug monitoring (TDM), the Arbeitsgemeinschaft für Neuropsychopharmakologie und Pharmakopsychiatrie (AGNP) Consensus Guidelines recommend a therapeutic reference range of 100–320 ng/mL for amisulpride.8,9 However, real-world data from Chinese populations suggest that this range may not fully reflect routine clinical practice in China, as more than 57% of Chinese patients receiving amisulpride have plasma concentrations above 320 ng/mL.10–12 In addition, a Chinese study found that when amisulpride concentrations were 100–600 ng/mL, adverse reaction rates ranged from 53% to 85%. 13 Based on these findings, the Expert Consensus on Clinical Application of Psychiatric Therapeutic Drug Monitoring in China defines 600 ng/mL as the upper therapeutic reference concentration for amisulpride in Chinese patients. 14 Accordingly, in the present study, we used 600 ng/mL as the predefined threshold for high exposure and aimed to identify patients at risk of exceeding this threshold in routine psychiatric practice.
Although our previous PopPK study identified estimated creatinine clearance (eCLcr) as a key determinant of amisulpride clearance and provided a covariate equation–based representation of apparent clearance (CL/F), the clinical accessibility of such derived predictors differs from that of routinely available raw data. 10 To determine the optimal predictive strategy, we established three distinct candidate pools, each containing daily dose and other routinely available clinical variables but differing in how renal function and drug elimination were represented: one including CL/F calculated from the final covariate equation of the previously published PopPK model, one including the key covariate eCLcr, and one consisting of the raw clinical variables used to calculate eCLcr.
Consequently, the primary objective of this study was to evaluate and compare the predictive performance of these three modeling strategies. We aimed to develop and validate a clinically interpretable risk stratification approach by comparing different clinically available representations of predictors relevant to amisulpride exposure. Ultimately, this approach is intended to support clinicians in the early identification of patients at increased risk of supratherapeutic exposure (>600 ng/mL) and to inform closer monitoring or more cautious dose titration in routine psychiatric practice.
Methods
Patient population
This retrospective study was conducted at Xi’an Mental Health Center. Clinical data were collected from inpatients treated with amisulpride between June 1, 2023, and May 30, 2025. The study protocol was approved by the Ethics Committee of Xi’an Mental Health Center. The study was conducted in accordance with the Declaration of Helsinki. The inclusion criteria were as follows: (1) age ⩾18 years; (2) receiving oral amisulpride therapy for at least 5 days to ensure steady-state concentrations; and (3) having at least one valid steady-state trough plasma concentration measurement. Patients were excluded if they: (1) were pregnant or lactating; or (2) had significant missing data for key covariates.
Data collection
Demographic and clinical data were retrospectively extracted from the electronic medical records (EMR). Collected variables included age, sex, body weight, body mass index (BMI), daily dose of amisulpride, and concomitant medications. Routine laboratory indices, including serum creatinine, alanine aminotransferase (ALT), and aspartate aminotransferase (AST), were also recorded. Serum amisulpride concentrations were quantified using a validated liquid chromatography–tandem mass spectrometry (LC–MS/MS) assay with a linear calibration range of 20–2000 ng/mL, as previously described. 10 The primary outcome was supratherapeutic exposure, defined as a steady-state trough plasma concentration exceeding 600 ng/mL, corresponding to the upper therapeutic reference concentration recommended by the Chinese expert consensus on psychiatric therapeutic drug monitoring (2022 edition). 14
Key pharmacokinetic covariates were calculated for model development. eCLcr was calculated using the Cockcroft–Gault equation based on serum creatinine, age, body weight, and sex.15,16 Individual apparent clearance (CL/F) was calculated by entering each patient’s clinical covariates into the final covariate equation from our previously published PopPK model. In that model, amisulpride pharmacokinetics were described by a one-compartment model with first-order absorption and elimination, and eCLcr was identified as a covariate on CL/F. The final covariate equation was as follows: 10

Statistical analysis and model development
All statistical analyses were performed using R software (version 4.1.0; R Foundation for Statistical Computing, Vienna, Austria). Missing data were processed prior to analysis: variables with a missing rate exceeding 20% were excluded. For the remaining variables, missing values in continuous features were imputed using the median value. The dataset was randomly split into a training set (70%) and a validation set (30%). Notably, this partition was performed at the patient level (grouped by patient ID) to prevent data leakage and ensure that all samples from the same patient remained in the same cohort. Continuous variables were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate, and compared using Student’s t-test or the Mann–Whitney U test. Categorical variables were expressed as counts (percentages) and compared using the chi-square test or Fisher’s exact test. All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
To compare predictive performance across different approaches, three candidate predictor pools were evaluated. Across all three pools, daily dose and a common set of baseline clinical variables, including demographic characteristics, laboratory biochemical parameters, and concomitant medications, were consistently considered. The key difference among the three pools lay in how renal function and drug elimination capacity were represented. The first pool incorporated PopPK-derived apparent clearance (CL/F), calculated using the final covariate equation from our previously published PopPK model. 10 The second pool focused on eCLcr, a key determinant of amisulpride clearance identified in our previous PopPK analysis. 10 The third pool directly incorporated the individual clinical variables used to calculate eCLcr.
Feature selection was performed using logistic regression with a Least Absolute Shrinkage and Selection Operator (LASSO) penalty and 10-fold cross-validation to reduce dimensionality and prevent overfitting. The optimal penalty parameter (λ) was selected based on the minimum cross-validated binomial deviance (λmin). Variables with non-zero coefficients at the selected λ were retained and subsequently entered into multivariable logistic regression models to construct candidate prediction models.
The predictive performance of the three modeling strategies was compared using the area under the receiver operating characteristic curve (AUC). Considering both discrimination performance and clinical accessibility, one model was selected for subsequent nomogram construction. The final nomogram was developed based on the selected model using the rms framework. The performance of the nomogram was evaluated in both the training and validation datasets. Discrimination was assessed using the concordance index (C-index) and AUC. In the training set, calibration was assessed using bootstrap-resampled calibration curves with 500 iterations for internal validation and correction of potential optimism. In the validation set, calibration was assessed by comparing predicted probabilities from the final model developed in the training set with observed event frequencies. The mean absolute error was additionally reported as a descriptive summary of the deviation between predicted and observed probabilities in the calibration plots. Clinical utility was evaluated using decision curve analysis (DCA), in which the net benefit of using the nomogram for risk stratification was assessed across a range of threshold probabilities and compared with the treat-all and treat-none strategies.
To further assess the potential influence of within-patient correlation due to repeated measurements, we performed a one-patient-one-record sensitivity analysis. In this analysis, each patient contributed only one observation: for patients with multiple TDM measurements, only the first eligible steady-state trough sample was retained. The resulting patient-level dataset was then analyzed using the same workflow as in the primary analysis, including LASSO-based variable selection, multivariable logistic regression, and comparative evaluation of the three predefined modeling strategies.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement, and the completed STROBE checklist is provided as Supplemental Material. 17
Results
Demographic and clinical characteristics
A total of 299 patients (413 steady-state serum samples) were included in this study. The study population consisted of 154 males (51.5%) and 145 females (48.5%), with a mean age of 34.17 ± 10.81 years and a mean body weight of 69.03 ± 15.58 kg. The daily dose of amisulpride ranged from 100 to 1200 mg (mean: 467.39 ± 220.77 mg), and the corresponding steady-state trough concentrations varied widely from 33.9 to 1636.7 ng/mL, with a mean value of 416.30 ± 260.26 ng/mL. Notably, 81 samples (19.6%) exhibited concentrations exceeding the safety threshold of 600 ng/mL. The patients were randomly allocated into a training cohort (n = 209, 70%) and a validation cohort (n = 90, 30%). As summarized in Table 1, there were no statistically significant differences in demographic characteristics between the two cohorts (all p > 0.05). This balanced distribution confirms the comparability of the training and validation sets for subsequent model development and evaluation. Missing data were present for several candidate covariates but did not exceed the prespecified 20% exclusion threshold, with the highest missing rate observed for CK (62/413, 15.0%); remaining missing values were handled by median imputation before model development.
Demographic and clinical characteristics of patients in the training and validation cohorts.
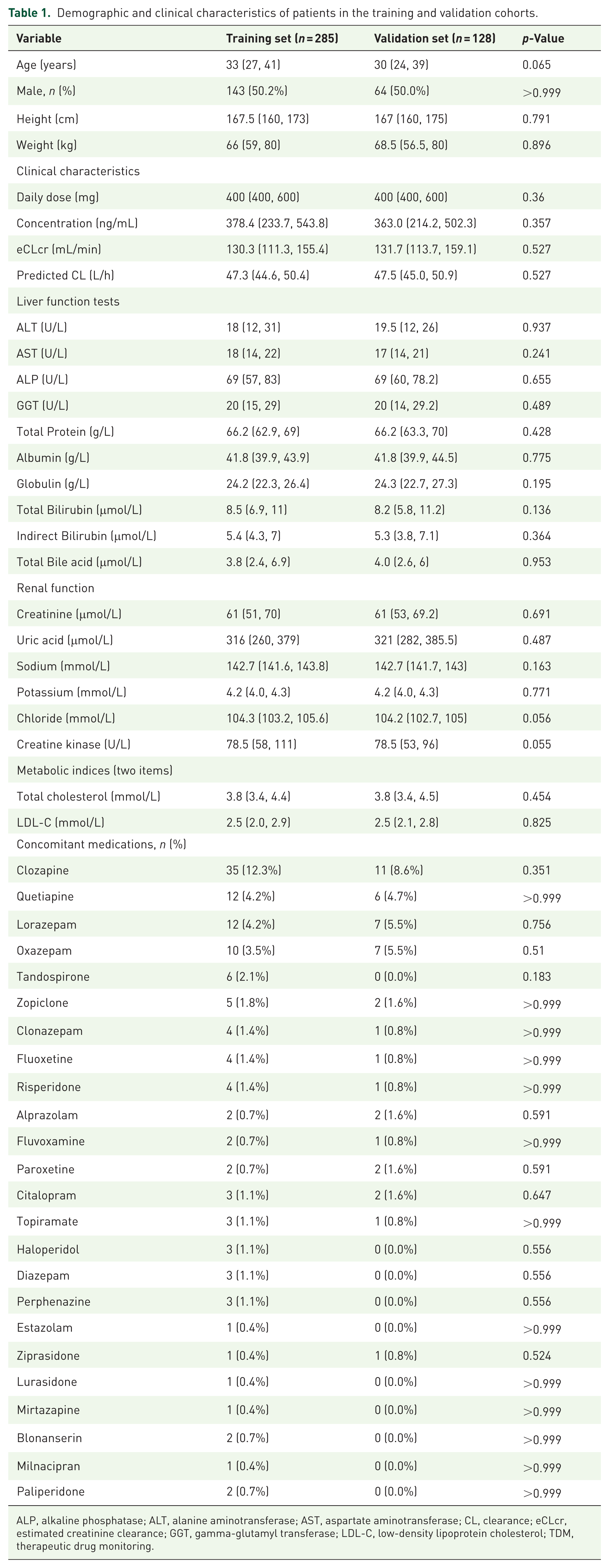
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CL, clearance; eCLcr, estimated creatinine clearance; GGT, gamma-glutamyl transferase; LDL-C, low-density lipoprotein cholesterol; TDM, therapeutic drug monitoring.
Variable selection and model development
For each of the three predefined modeling strategies, LASSO regression yielded parsimonious subsets of predictors with non-zero coefficients (Supplemental Figures S1–S3). These retained variables were then entered into multivariable logistic regression models, and the detailed regression results are summarized in Table 2.
Model 1 (PopPK-derived strategy): Apparent clearance and daily dose were retained. In the multivariable analysis, higher apparent clearance predicted a lower probability of supratherapeutic exposure (>600 ng/mL), whereas a higher daily dose significantly elevated this risk.
Model 2 (Key Covariate-based strategy): eCLcr and daily dose were retained. In the multivariable analysis, higher eCLcr predicted a lower probability of supratherapeutic exposure, whereas a higher daily dose significantly elevated this risk.
Model 3 (Raw clinical data strategy): Age, serum creatinine, and daily dose were retained. In the multivariable analysis, older age and higher serum creatinine predicted a greater probability of supratherapeutic exposure, whereas a higher daily dose significantly elevated this risk.
Parameter estimates of the three logistic regression models for predicting supratherapeutic amisulpride exposure.
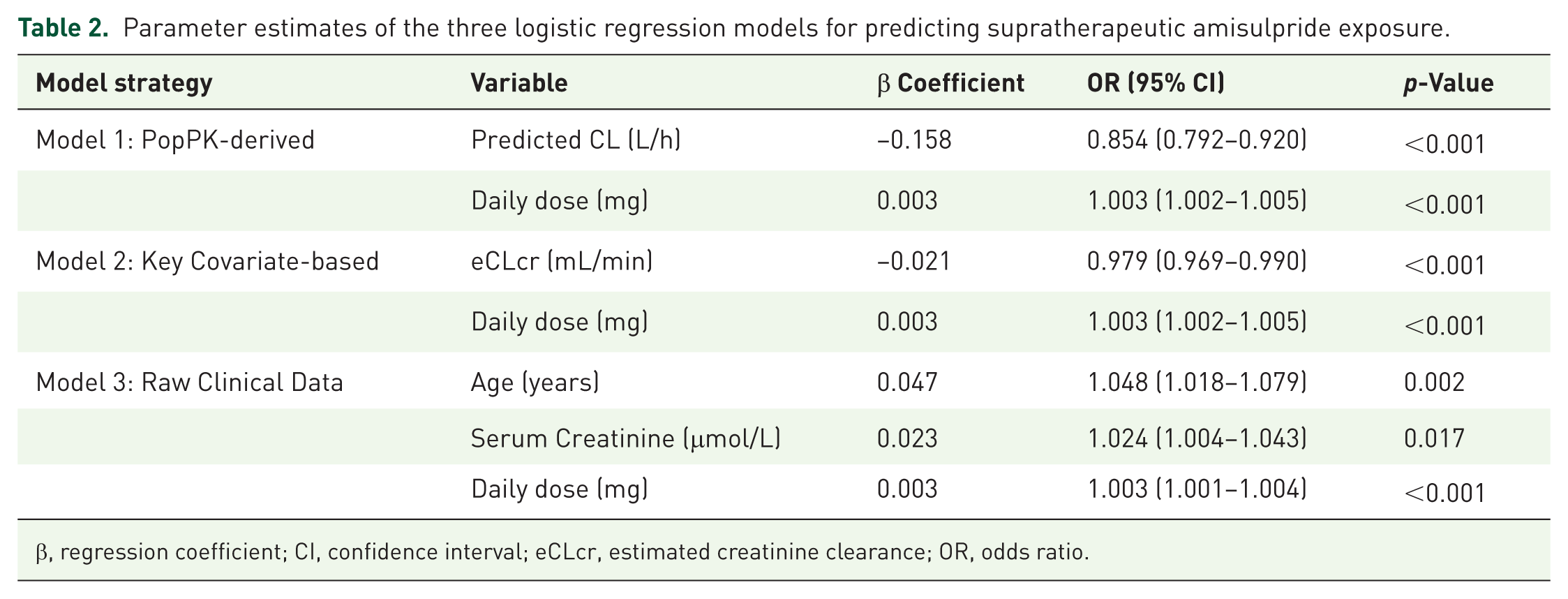
β, regression coefficient; CI, confidence interval; eCLcr, estimated creatinine clearance; OR, odds ratio.
Model comparison and nomogram construction
The predictive performance of the three candidate strategies was evaluated using receiver operating characteristic (ROC) analysis. As summarized in Table 3 and Figure 1, the eCLcr-based model and the PopPK-derived model demonstrated similar discrimination performance in both the training and validation datasets. The eCLcr-based model achieved an AUC of 0.738 in the training set and 0.720 in the validation set, which was numerically comparable to that of the PopPK-derived model (AUC 0.740 and 0.718, respectively). Both models exhibited higher discrimination than the model based on raw clinical variables (AUC 0.716 and 0.708 in the training and validation sets, respectively).
Comparison of predictive performance among the three modeling strategies in the training and validation sets.
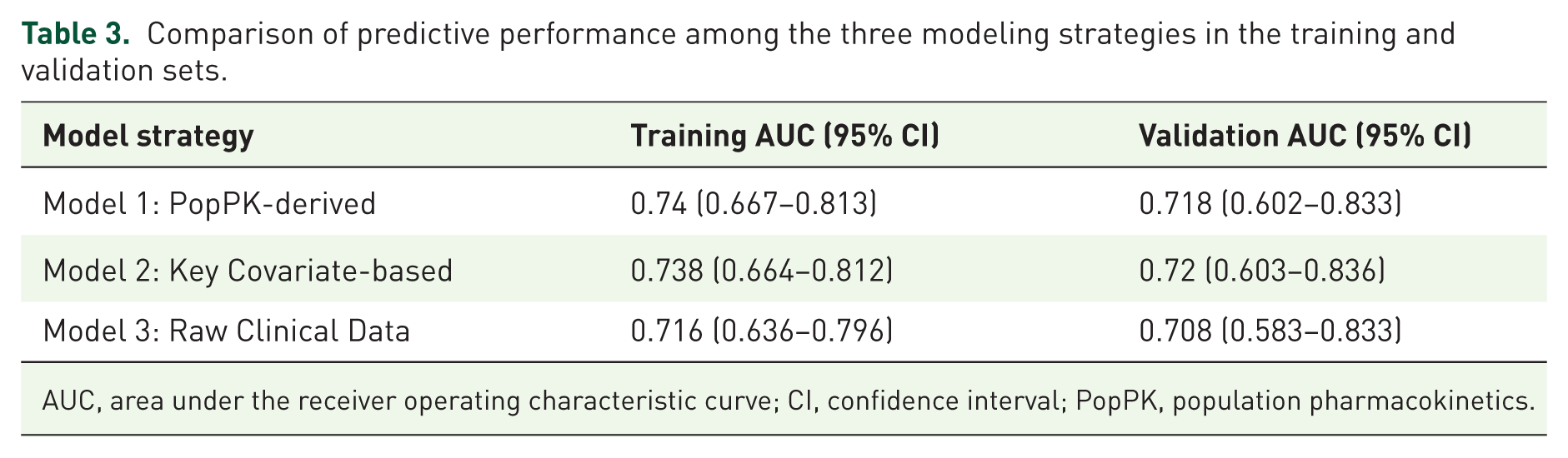
AUC, area under the receiver operating characteristic curve; CI, confidence interval; PopPK, population pharmacokinetics.
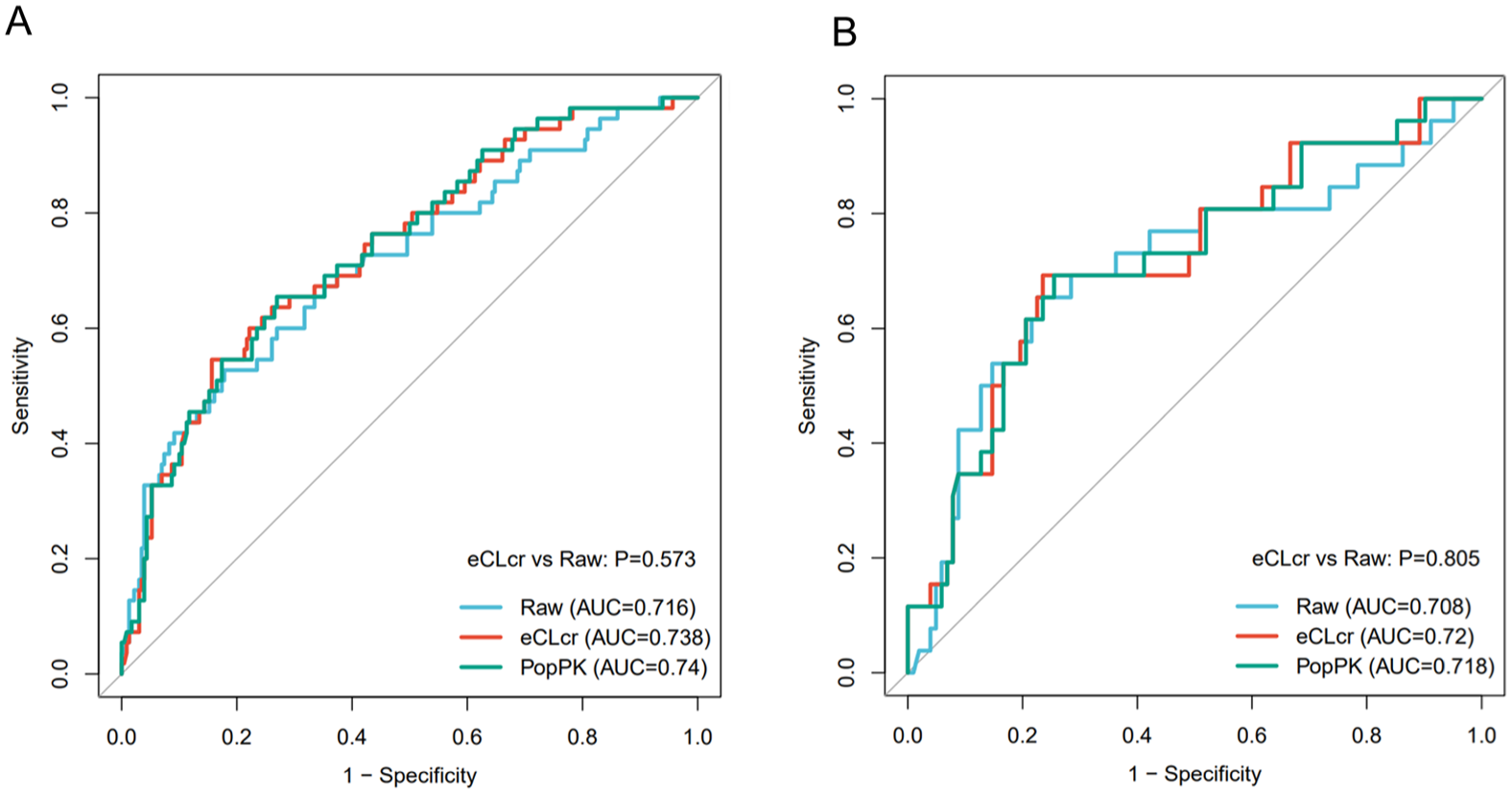
Comparison of performance among three modeling strategies. ROC curves illustrating model discrimination in the (a) training set and (b) validation set.
Given the comparable predictive performance of the eCLcr-based and PopPK-derived models, the eCLcr-based model was selected for final nomogram construction because it relies on routinely available clinical variables, thereby offering clinical accessibility. This model relies on routinely available clinical parameters, including estimated creatinine clearance and daily dose, without the need for complex pharmacokinetic modeling procedures.
Based on the multivariable logistic regression analysis of the eCLcr-based model, a nomogram was constructed to estimate the probability of amisulpride supratherapeutic exposure (Figure 2). The nomogram integrates estimated creatinine clearance and daily dose to provide an individualized risk estimate for steady-state trough plasma concentrations exceeding 600 ng/mL.
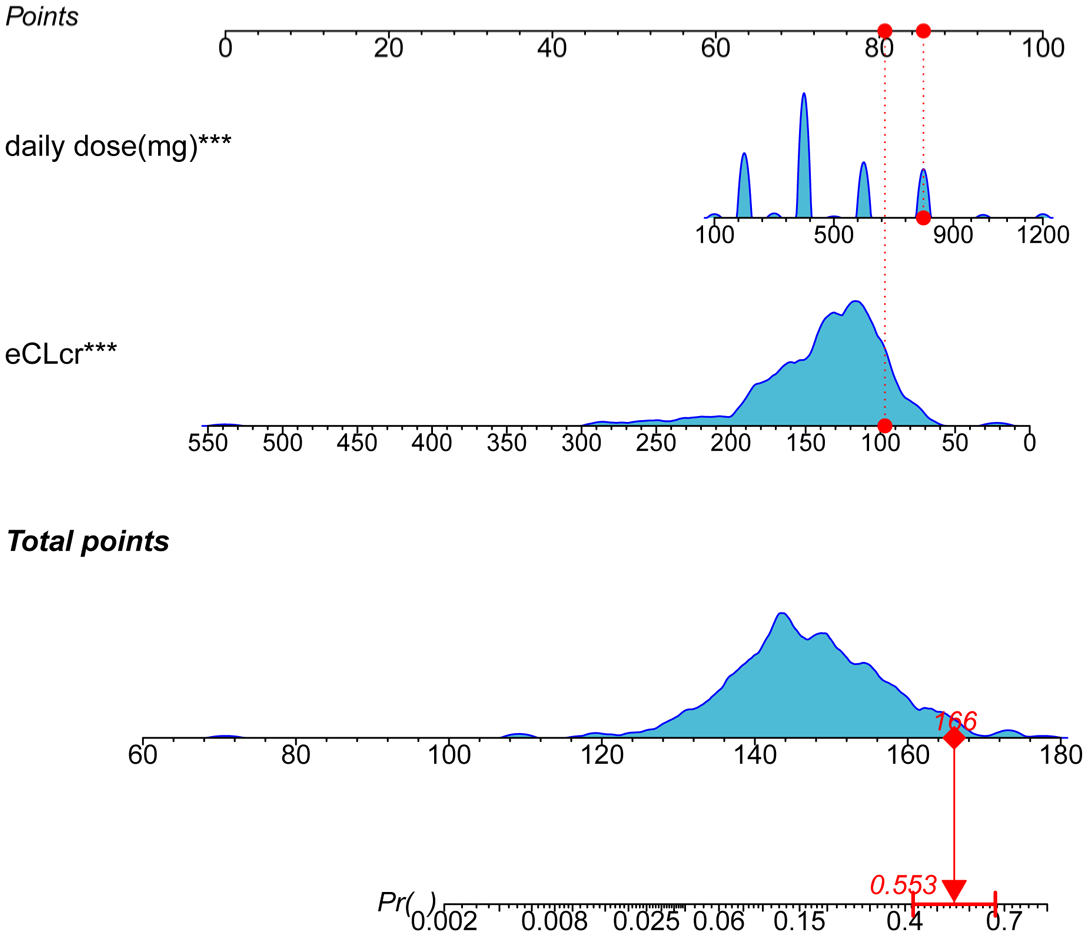
Nomogram for predicting supratherapeutic amisulpride exposure.
An example of clinical application is illustrated in Figure 2 (red dashed line). Consider a representative patient with an eCLcr of 97 mL/min receiving a daily amisulpride dose of 800 mg. By locating these values on the respective axes, the patient obtains a total score of approximately 166 points, corresponding to an estimated probability of approximately 55.3% for supratherapeutic exposure. This visualization facilitates rapid risk stratification and individualized dose optimization.
Validation of the nomogram
The predictive accuracy and robustness of the final nomogram (based on the Key Covariate-based Model) were comprehensively evaluated in both the training and validation cohorts.
In terms of discrimination, the nomogram demonstrated satisfactory performance, yielding a C-index of 0.738 in the training set and 0.720 in the validation set. The calibration curves are shown in Figure 3. In the training set, the bootstrap-resampled calibration curve showed good agreement between predicted probabilities and observed outcomes, with a mean absolute error of 0.016. In the validation set, the calibration curve showed acceptable overall agreement with the ideal reference line, with a mean absolute error of 0.092.
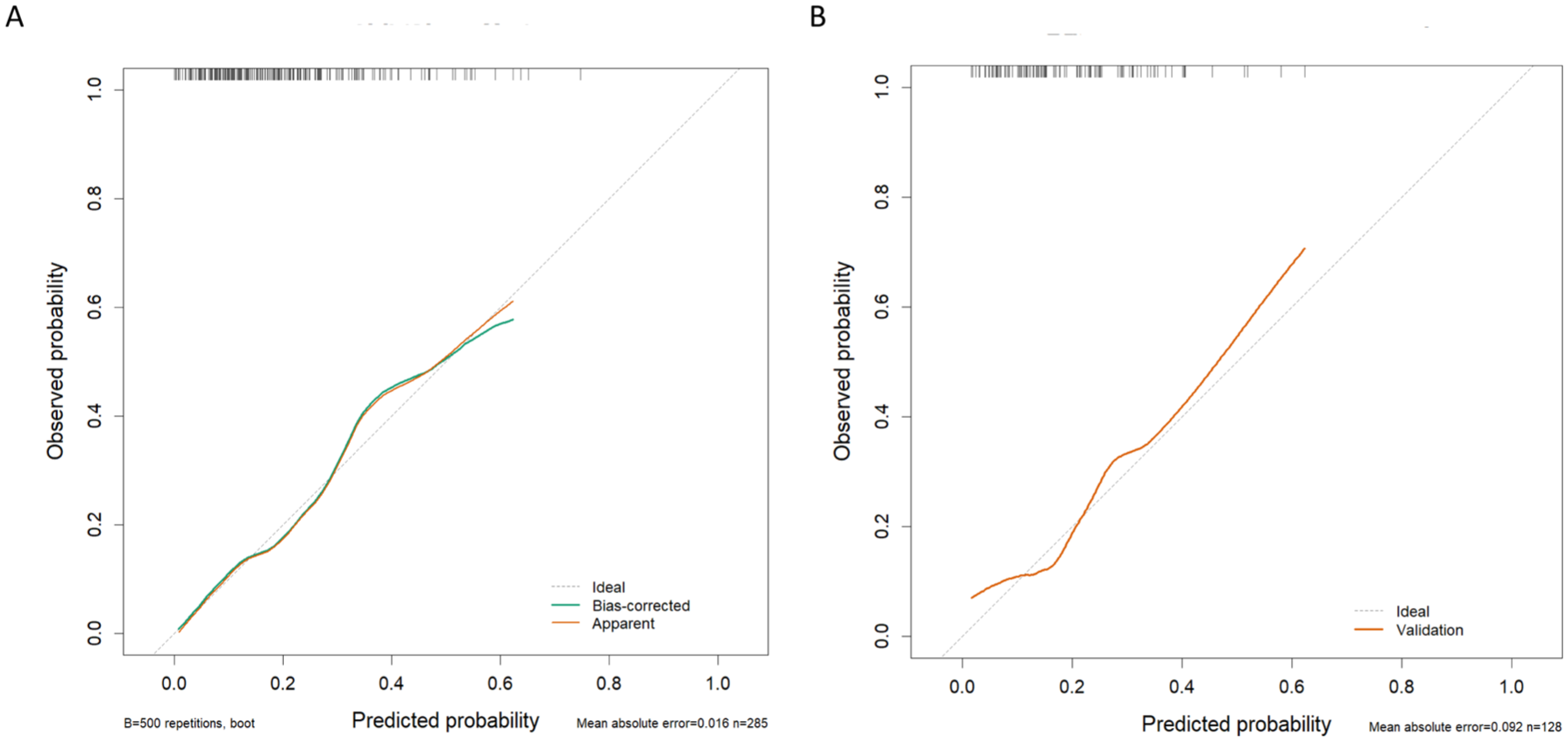
Calibration curves of the nomogram. The plots show calibration in the (a) training set and (b) validation set. The dashed diagonal line indicates the ideal reference. In panel (a), the green and orange solid lines represent the bias-corrected and apparent calibration curves, respectively; in panel (b), the orange solid line represents the validation calibration curve. Rug plots along the top indicate the distribution of predicted probabilities. Mean absolute error denotes the average absolute difference between predicted probabilities and observed event frequencies.
DCA showed that the nomogram achieved a higher net benefit than the treat-all and treat-none strategies across a range of lower to moderate threshold probabilities, as shown in Figure 4. The main advantageous threshold range was approximately 0.05–0.48 in the training set and 0.12–0.49 in the validation set. At higher threshold probabilities, the net benefit advantage of the nomogram became less evident.
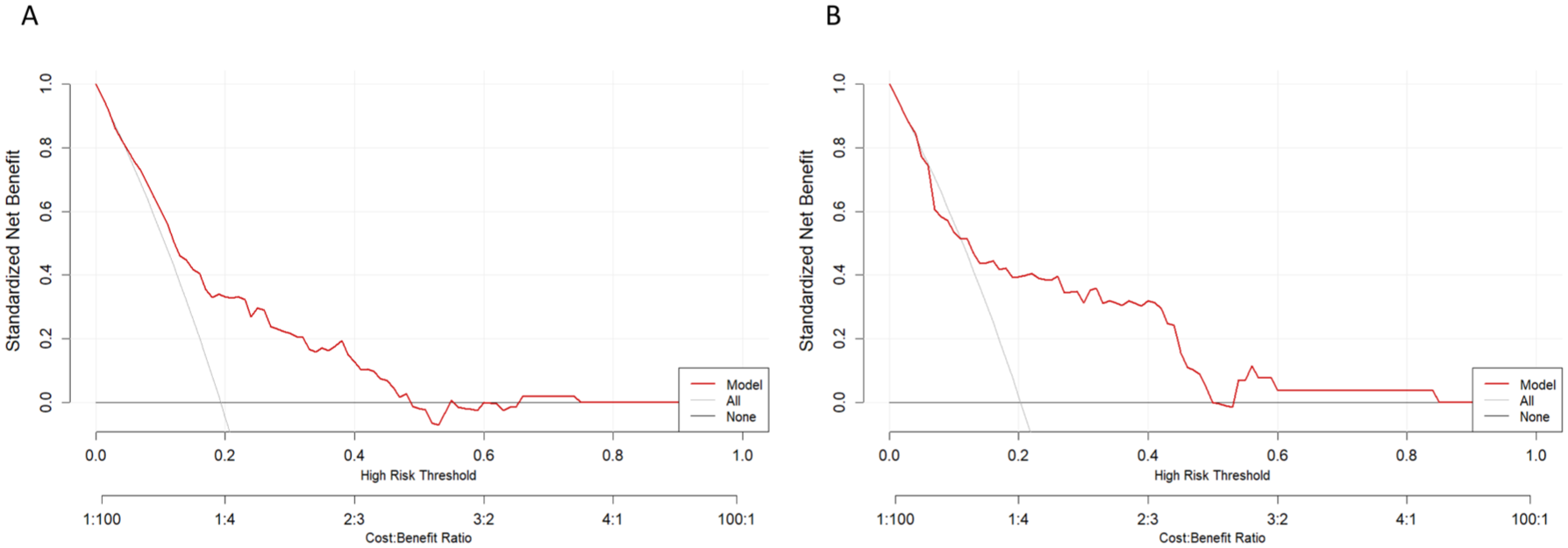
DCA. The curves evaluate clinical utility in the (a) training set and (b) validation set. The red line represents the nomogram. The gray line represents the assumption that all patients are at high risk (“treat-all”), and the horizontal black line represents the assumption that no patients are at high risk (“treat-none”).
Sensitivity analysis for repeated measurements
In the one-patient-one-record sensitivity analysis, the key predictors in the Key Covariate-based and PopPK-derived strategies were unchanged from the primary analysis, whereas in the Raw Clinical Data strategy, only the daily dose was retained after penalized selection (Supplemental Table S1). The training AUCs of the Key Covariate-based, PopPK-derived, and Raw Clinical Data strategies were 0.716, 0.721, and 0.643, respectively, and the corresponding validation AUCs were 0.683, 0.684, and 0.653. The Key Covariate-based strategy was selected as the final model in both the primary and sensitivity analyses.
Discussion
In the present study, we developed and validated a clinically interpretable risk stratification tool for predicting supratherapeutic amisulpride exposure using real-world, routinely available clinical data. We focused on three distinct modeling strategies, namely a PopPK-derived CL/F representation, a key covariate-based approach using eCLcr, and raw clinical variables. This comparison allowed us to assess the relative value of these different representations of renal function and drug elimination for risk stratification in routine psychiatric practice. Ultimately, the eCLcr-based strategy was selected for final nomogram development because it combined predictive performance comparable to that of the PopPK-derived strategy with greater clinical accessibility in routine psychiatric practice. These findings suggest that eCLcr and daily dose may serve as two applicable clinical risk indicators, providing a practical basis for individualized risk stratification in routine practice.
The present study adopted a logistic regression framework to develop a clinically interpretable nomogram for a binary outcome, namely whether the steady-state trough concentration exceeded 600 ng/mL, using predictors that are readily obtainable in routine clinical practice. Within this framework, we were particularly interested in whether a PopPK-derived CL/F representation, calculated from the final covariate equation of our previously published model and retaining the structured relationship between renal function and drug elimination embedded in that model, might perform better than direct use of eCLcr or clinical variables considered separately. 10 This design allowed a direct comparison among a model-derived clearance metric, an integrated physiological index, and raw clinical variables within the same risk stratification framework.
The PopPK-derived and eCLcr-based strategies showed similar performance. This may be explained, at least in part, by the close relationship between the two representations in our modeling framework. In our previously published PopPK model, eCLcr was a key determinant of CL/F, and the PopPK-derived CL/F used here was calculated directly from that final covariate equation. 10 The PopPK-derived metric therefore did not function as an independent predictor, but rather as a model-derived transformation that retained structured information related to renal function and drug elimination. In addition, the relatively narrow distribution of renal function observed in the current dataset may have further limited the extent to which any incremental predictive advantage of the PopPK-derived metric could be distinguished.
As expected from both routine prescribing practice and the pharmacokinetic characteristics of amisulpride, the daily dose emerged as an important determinant of exposure in the present study. Previous studies have also shown that the amisulpride dose is generally associated with plasma concentration. Sparshatt et al. 9 reviewed 10 studies and reported an overall correlation between dose and plasma amisulpride concentration. However, these data also indicate that dose alone cannot fully explain the marked between-patient variability in exposure. For example, Bowskill et al. 18 found that dose explained only 42% of the observed variation in plasma amisulpride concentration after log transformation of both variables. Taken together, the daily dose may be understood as a readily available indicator of drug input, but the remaining variation in exposure requires consideration of individual elimination capacity.
In this context, the clinical relevance of eCLcr as a predictor is supported by the known pharmacokinetic properties of amisulpride.10,12 Unlike many antipsychotics that undergo extensive hepatic metabolism (e.g., clozapine or olanzapine), amisulpride is eliminated from the systemic circulation primarily by renal excretion as an unchanged drug, with limited metabolic transformation. 19 Consequently, its systemic clearance is largely dependent on glomerular filtration capacity. While serum creatinine is commonly used as a renal marker, it is imperfect when used in isolation because its generation rate depends on muscle mass, which varies significantly with age, weight, and gender. 20 As a composite physiological index, estimated creatinine clearance calculated using the Cockcroft–Gault equation integrates demographic variables into a functional estimate of renal elimination capacity. It therefore serves as a more robust surrogate of renal elimination capacity than any single laboratory measure. This framework explains why patients with age-related or pathological reductions in renal function exhibit decreased drug clearance and a correspondingly higher risk of supratherapeutic exposure, consistent with findings from our previous PopPK analysis.
The difference between the eCLcr-based strategy and the raw clinical data strategy can be better understood by considering how the predictors are represented in the two approaches. In the raw-variable model, age and creatinine were retained as separate predictors and entered the model as linear additive terms. By contrast, eCLcr is a predefined physiological measure derived from the Cockcroft–Gault equation, which combines age, body weight, sex, and serum creatinine into a single index of renal elimination capacity through a structured functional form.15,16 Thus, the eCLcr-based model does not simply replace several raw variables with a single summary term; rather, it incorporates these related variables into a unified physiological index of renal elimination capacity, while also better preserving aspects of their potentially non-linear contribution to amisulpride elimination. In this way, the model no longer needs to determine the role of each component separately from the current dataset. This may partly explain the improved discrimination observed with the eCLcr-based approach. More broadly, these findings suggest that, in clinically oriented risk stratification, physiologically informed composite measures may offer advantages over relying solely on separate raw clinical variables selected from the data.
The calibration curves and DCA showed broadly similar trends. The calibration curves indicated that most predicted probabilities were below approximately 0.6, with relatively few observations beyond this range. Consistently, the DCA suggested that the model’s clinical utility was concentrated mainly at lower to moderate threshold probabilities. In our dataset, extremely high-risk profiles were uncommon, particularly cases involving both higher daily doses and marked renal impairment, suggesting that such scenarios may be relatively infrequent in routine clinical practice.
Crucially, the probabilities generated by this nomogram are intended to gauge individual risk, not to serve as rigid cutoffs for dose adjustment. These probabilities should therefore be interpreted as relative estimates of patient risk within the current clinical setting, rather than as absolute predictions for individual patients. To illustrate, a predicted risk of 40%–50% should not automatically trigger a dose reduction but rather signal the need for heightened vigilance, such as prioritizing early TDM or slowing down dose titration. Ultimately, the nomogram should be regarded as an adjunct to individualized clinical judgment.
In the present study, the threshold probability represents the level of predicted risk at which a clinician would consider it worthwhile to modify management for a patient receiving amisulpride, for example by arranging earlier TDM, increasing monitoring intensity, or adopting a more cautious titration strategy. Net benefit reflects the clinical value of using the nomogram to support such additional vigilance after balancing the benefit of correctly identifying patients at increased risk of supratherapeutic amisulpride exposure (>600 ng/mL) against the burden of unnecessary intensified monitoring in lower-risk patients. In our clinical context, the treat-all strategy would correspond to applying the same heightened vigilance to all patients receiving amisulpride, such as routinely prioritizing early TDM or adopting a more cautious dosing approach regardless of individual risk. Although this strategy may reduce the chance of missing high-risk patients, it would also increase unnecessary monitoring in many patients who are actually at lower risk. Conversely, the treat-none strategy would correspond to relying entirely on routine practice without using the model to trigger any additional vigilance, thereby avoiding extra monitoring but also missing opportunities to identify patients at increased risk of supratherapeutic exposure. The nomogram showed a higher net benefit than both reference strategies across a range of lower to moderate threshold probabilities. This suggests that the model may provide a useful reference for identifying patients with reduced eCLcr or higher daily doses at increased risk of supratherapeutic exposure in routine psychiatric practice.
The one-patient-one-record sensitivity analysis provided additional insight into the effect of repeated measurements in the present study. Under this patient-level analysis, model performance decreased across all three strategies. This decrease in performance was likely related, at least in part, to the reduced dataset size and the loss of trough concentration information in the patient-level analysis, rather than necessarily indicating that the primary analysis overestimated model performance. Furthermore, in the patient-level analysis, the Raw Clinical Data strategy retained only the daily dose, whereas age and serum creatinine were no longer selected. These findings suggest that, when renal function is represented by separate raw variables, the model must estimate the contribution of each component from the data itself, a process that may become less stable when fewer observations are available. Taken together, these findings suggest that although the handling of repeated observations influenced model performance estimates and variable selection, it did not materially alter the main comparative conclusion of the study. The Key Covariate-based strategy remained the most practical final model, with performance comparable to that of the PopPK-derived strategy.
Limitations
This study has several limitations. First, due to its retrospective design, potential selection bias cannot be entirely excluded, although strict inclusion criteria were applied to ensure data quality. Therefore, the generalizability of the findings requires further validation in fully independent external cohorts. Second, a formal a priori sample size calculation or power analysis was not performed because this was a retrospective study, and the sample size was determined by the number of eligible patients available during the study period. This may have reduced the ability to detect weaker associations for some clinical variables. Third, the high-risk outcome was defined using a steady-state trough plasma concentration threshold rather than direct clinical adverse events. Although this concentration threshold is widely used in clinical practice as a surrogate marker of increased exposure risk, it does not capture inter-individual pharmacodynamic variability. As a result, the relationship between supratherapeutic concentrations and clinical manifestations may differ across patients. Fourth, because some patients contributed more than one observation, the primary analysis using standard logistic regression did not explicitly model within-patient correlation. Although we performed a one-patient-one-record sensitivity analysis and the main comparative conclusions were unchanged, this approach should be regarded as a robustness check rather than a formal method for modeling correlated data. Future studies may further examine these findings using approaches such as mixed-effects logistic regression or generalized estimating equations. Fifth, the PopPK-derived CL/F representation used in this study was calculated from a fixed covariate equation rather than obtained through maximum a posteriori (MAP) Bayesian estimation based on observed concentrations. Therefore, it should be interpreted as a simplified model-based representation of expected clearance. Future studies may examine whether incorporating individualized pharmacometric feedback provides additional value for early risk stratification.
Conclusion
In this study, we developed a nomogram to predict the risk of supratherapeutic amisulpride exposure based on estimated creatinine clearance and daily dose. By comparing multiple modeling strategies, we demonstrated that the Key Covariate-based strategy achieved discrimination performance comparable to that of the PopPK-derived strategy while offering greater clinical accessibility. This nomogram may assist clinicians in identifying patients at increased risk of supratherapeutic exposure and support individualized risk assessment in routine practice.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-docx-1-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-docx-2-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-xlsx-1-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-xlsx-1-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-tif-1-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-tif-1-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-tif-2-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-tif-2-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-tif-3-tpp-10.1177_20451253261460142 – Supplemental material for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study
Supplemental material, sj-tif-3-tpp-10.1177_20451253261460142 for Identifying patients at risk of supratherapeutic amisulpride exposure in routine psychiatric practice: a real-world therapeutic drug monitoring study by Keyu Yan, Gehang Ju, Aowei Li, Ruomei Gao, Na Wang and Qing Shao in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.