
Abstract
Objective:
The implementation of evidence-based secondary medical prevention in peripheral arterial disease (PAD) patients has received increasing attention in recent years, but population-based data are sparse. This study examined the use of secondary medical prophylaxis in unselected symptomatic PAD patients in Denmark.
Design:
A nationwide follow-up study based on individual-level record linkages of population-based healthcare registers was performed.
Participants:
All patients who underwent primary vascular reconstruction in Denmark between 1996 and 2006 with a minimum of 6 months of follow-up were included (n = 16,492).
Methods:
Data were obtained from prescriptions that were filled six months after primary vascular reconstruction (±90 days). The use of secondary medical prevention was examined according to calendar year and place of residence.
Results:
The use of lipid-lowering drugs increased from 32.2% in 1996 to 76.1% in 2006 (adjusted relative risk (RR) 1.95, 95% CI 1.81–2.10). The overall use of antihypertensive therapy was unchanged during the study period, but treatment shifted from diuretics/calcium antagonists towards angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists. The use of combination therapy (concomitant lipid-lowering, antiplatelet and any antihypertensive therapies) increased from 29.1% in 1996 to 67.6% in 2006 (adjusted RR 1.95, 95% CI 1.80–2.12). This shift in the use of secondary medical prevention was independent of sociodemographic and clinical factors. No substantial differences in pharmacological use based on place of residence were observed.
Conclusion:
The use of evidence-based secondary medical prevention, especially lipid-lowering drugs, increased substantially among symptomatic PAD patients in Denmark from 1996 to 2006. However, recommendations in current clinical guidelines suggest that room for improvement remains.
Keywords
Introduction
Peripheral arterial disease (PAD) is a common manifestation of systemic arthrosclerosis and is associated with significant morbidity and mortality. PAD is effectively treated as a systemic disease because symptomatic PAD patients have the same risk of cardiovascular events as patients with ischaemic heart disease or stroke.1–4 Current national and international guidelines recommend lipid-lowering and antiplatelet therapy supplemented with aggressive antihypertensive treatment for all patients with symptomatic and asymptomatic PAD, regardless of age and sex.5–8 However, the use of secondary medical prevention is generally insufficient for patients with PAD.9–14 Furthermore, substantial geographic international and national variations in the use of secondary medical prevention have been reported, and this variation reflects the problem of treatment implementation.14,15 Recent attention has focused on the implementation of evidence-based secondary medical prevention. However, the effects of these efforts remain uncertain because population-based data of the changes over time in routine clinical practice with unselected patients are sparse. Therefore, this study examined alterations in the use of secondary medical prevention in all Danish patients who underwent primary vascular reconstruction between 1996 and 2006.
Materials and methods
The entire Danish population (n ≈ 5.5 million) receives tax-supported health care from the Danish National Health Service, which provides free access to hospital care and general practitioners and reimburses individuals for expenses on a wide range of prescription drugs. Each Danish citizen receives a unique civil registration number at birth or immigration that encodes the citizen’s sex and date of birth. The civil registration number enables an unambiguous individual link between population-based administrative and health care registries.
Denmark was divided into 14 counties in January 1st 2007. Four of these counties (Copenhagen, Funen, Aarhus and North Jutland) have the largest populations and university hospitals with departments of vascular surgery. Viborg, Vejle and West Zealand also have departments of vascular surgery.
Study population
The study population included all Danish patients who underwent primary vascular surgical reconstruction as a result of atherosclerotic disorders between 1996 and 2006. Only patients who underwent primary vascular reconstruction as a result of moderate intermittent claudication, ischaemic pain at rest, ulceration or gangrene were included. Patients who died within 30 days after discharge, patients who were < 40 years old and patients without six months of follow up after primary vascular reconstruction were excluded. A final total of 16,492 patients were analysed (Figure 1).
Flow diagram of the study population.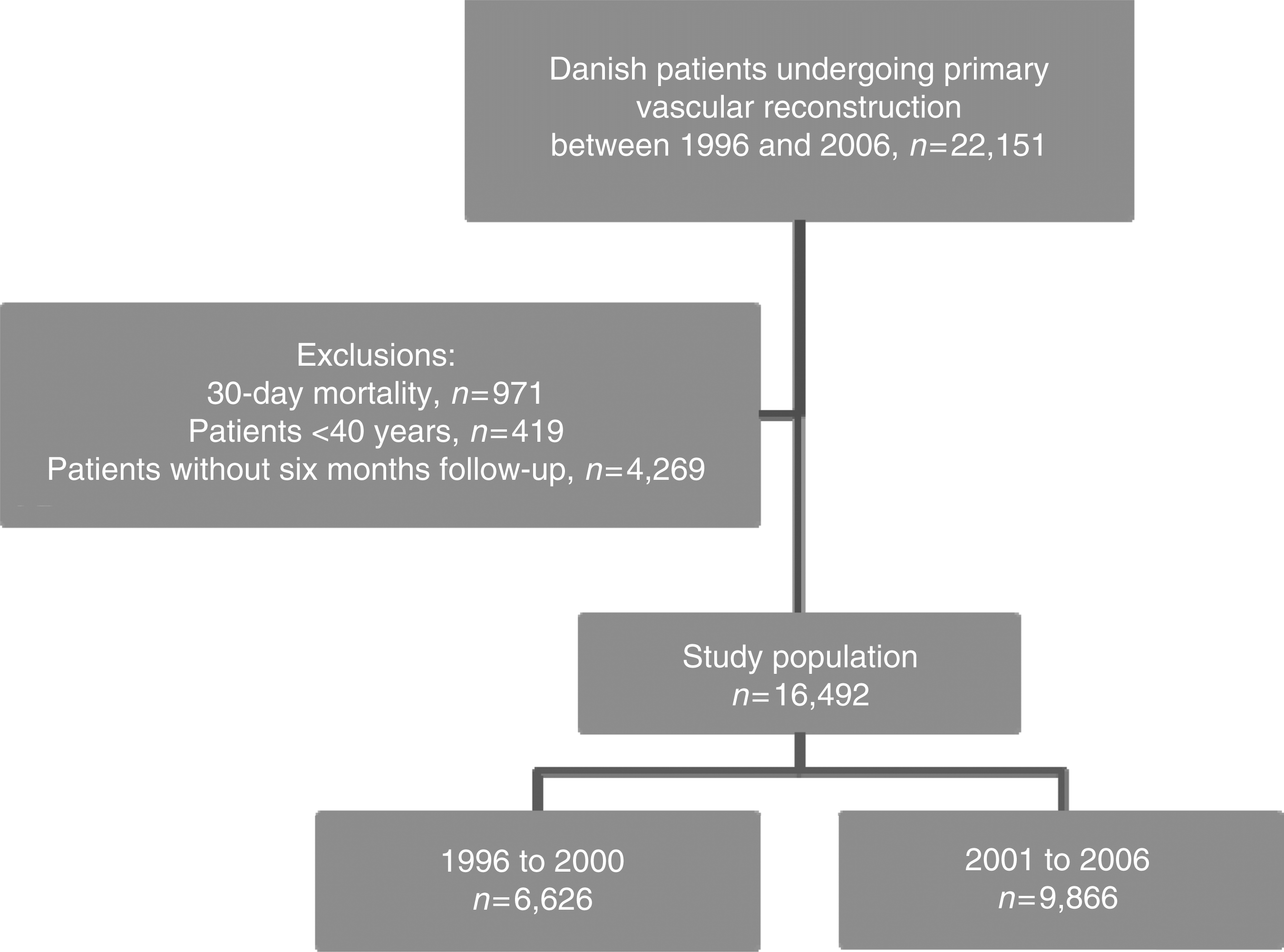
Patients were identified in the Danish Vascular Registry, which contains prospectively collected information on all vascular procedures that have been performed in Denmark since 1996. The primary objectives of the registry are surveillance and quality improvement. The registry contains 65 variables, including surgery indication and timing (acute/elective), patient characteristics, types of intervention, vascular patency at discharge, discharge destination and post-operative complications. 16 Reporting is mandatory for all vascular surgery departments (n = 9) and the registry covers 99.2% of all vascular procedures that were performed at Danish hospitals (Årsrapport, 2009: annual reports are found at www.karbase.dk). Data from a random national sample of 200 medical records were compared with data from the Danish Vascular Registry to assess the validity of the data in the registry. The discrepancy between operation-related and vascular patency at discharge data was less than 1%, and the discrepancy between these data for surgery type was less than 3%.
Information on vital status of patients during follow-up was obtained via linkage with the Danish Civil Registration System. This system maintains electronic records of changes in the vital status of all citizens since 1968. 17
Secondary medical prevention
Data on all filled prescriptions in the study population after discharge were obtained from the Medical Register of the Danish Medicines Agency, which was established in 1995 and includes all prescriptions that have been filled at all Danish pharmacies. The data include the type of drug according to the Anatomical Therapeutically Chemical (ATC) classification system 18 and the date that it was dispensed. All cardiovascular drugs except low-dose aspirin require a prescription. However, low-dose aspirin is available with a refundable prescription for patients with chronic diseases and pensioners. All prescriptions that were filled within six months (± 90 days) of surgery, including prescriptions for antihypertensive drugs (angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists (ACEs/ATIIs)), beta-adrenoceptor blocking agents (beta blockers), calcium antagonists, diuretics, antiplatelet drugs (including low-dose aspirin, dipyridamole and clopidogrel) and lipid-lowering drugs, were identified.
Covariates
Data on covariates were obtained from the Danish National Patient Registry (comorbidity), the Integrated Database for Labor Market Research (socioeconomic variables) and the Danish Vascular Registry (clinical variables).
The Danish National Patient Registry retains information on all discharges from somatic hospitals from 1977, and this information is coded according to the International Classification of Diseases (8th revision until 1993 and 10th revision thereafter). 19 A history of hospital admissions of all patients beginning in 1977 was constructed. Based on the history, a comorbidity index score (at the time of surgery) was computed based on patient history, as described previously by Charlson et al. 20 The Charlson comorbidity index covers 19 major disease categories, including myocardial infarction, heart failure, cerebrovascular diseases, diabetes and cancer which are weighted according to their prognostic impact on patient survival. This index was previously adapted and validated for use with our hospital discharge registry data. 21 Three levels were defined: ‘no comorbidity' (score 0); ‘low comorbidity' (scores 1–2); and ‘high comorbidity' (scores >2).
The Integrated Database for Labor Market Research retains yearly updated information on socioeconomic status for the entire Danish population. Patients were classified according to employment (employed, pensioner or other), marital status (single, married, widowed or divorced), gross income in quartiles and educational level (primary and lower secondary school, upper secondary school and vocational education or higher education).
The Danish Vascular Registry provided information on the following variables: acute/elective surgery, surgery region (central arteries (aorta and arteria iliaca communis), groin arteries, or peripheral arteries), indication for primary vascular reconstruction, vascular patency at discharge, discharge destination and smoking habits at the time of surgery.
Statistical analysis
Prescribed medication use was assessed annually between 1996 and 2006 and was defined as the filling of at least one prescription six months after primary vascular surgery reconstruction (± 90 days) because prescriptions for secondary medical prevention are usually issued for a three-month period in Denmark.
Time periods were defined as early (1996 to 2000, n = 6,626) and late (2001 to 2006, n = 9,866). The year 2000 was used as the cut-off point because the first international guidelines on PAD management were published in 2000 22 and therefore reflect clinical practice before and after the availability of official evidence-based recommendations.
A Poisson analysis with robust error estimates was used to perform crude and adjusted comparisons of prescription medication use across the time period and between 1996, 2000 and 2006. Poisson regression rather than logistic regression was performed because of the high prevalence of drug use and the need to adjust for a range of covariates, which may cause convergence problems in a log-binomial model.23,24 Data were also sub-grouped into 14 counties according to the patients’ place of residence. Crude and adjusted comparisons across these counties were performed using the capital area as a reference.
The adjusted analyses included comorbidity index scores and socioeconomic status (gross income, education level, marital status and employment) that were assessed as covariates six months after surgery. In addition, surgery timing (acute/elective), discharge destination, vascular patency at discharge, smoking habits, indications for primary vascular reconstruction and surgery region were assessed at the time of surgery. These factors were included in the analyses as covariates. Data were analysed using STATA version 11.0 (StataCorp).
Results
Patient characteristics six months after primary vascular reconstruction stratified according to time period (early: 1996–2000 or late: 2001–2006)

COLD: chronic obstructive lung disease.
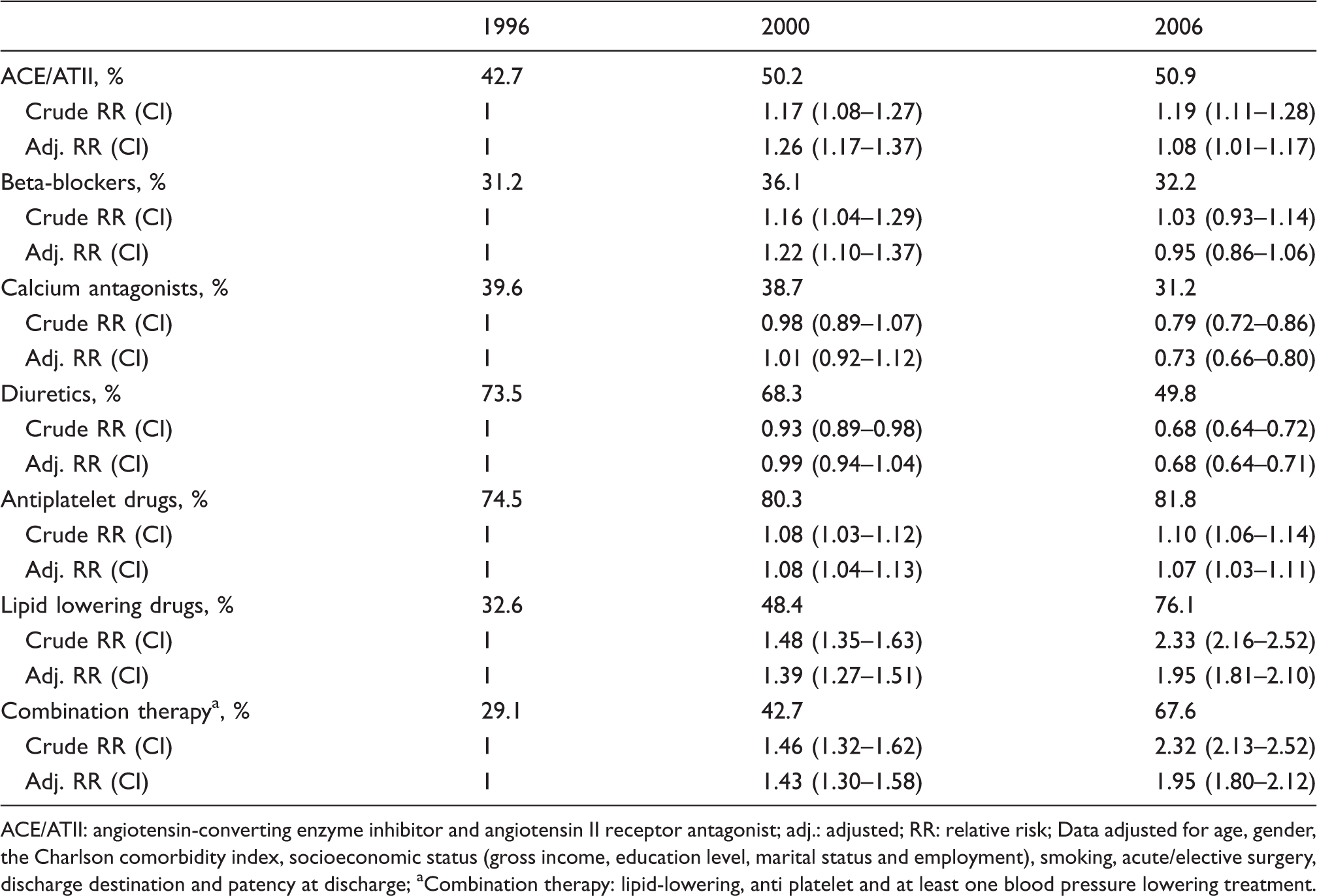
Figure 2 illustrates the proportions of patients who filled prescriptions for secondary medical prevention between 1996 and 2006, and Table 2 displays the corresponding adjusted relative risk (RR) with 95% confidence intervals (CIs). Major changes in the use of lipid-lowering drugs (33.7% in 1996 versus 77.4% in 2006; adjusted RR 1.95, 95% CI 1.81–2.10) and diuretics (74.4% in 1996 versus 49.9% in 2006; adjusted RR 0.68, 95% CI 0.64–0.71) were observed. A smaller increase in antithrombotic drug use was also observed (75.0% in 1996 versus 83.3% in 2006; adjusted RR 1.07, 95% CI 1.03–1.11). The overall use of antihypertensive treatment was not altered but treatment shifted from diuretics and calcium antagonists towards an increased use of ACEs/ATIIs. The use of combination therapy (concomitant lipid-lowering, antiplatelet and any antihypertensive therapy) increased from 29.1% in 1996 to 67.6% in 2006 (adjusted RR 1.95, 95% CI 1.80–2.12).
Proportions of Danish patients with symptomatic peripheral arterial disease (PAD) who filled specific prescriptions for secondary medical prevention between 1996 and 2006. ACE/ATII: angiotensin-converting enzyme inhibitor and angiotensin II receptor antagonist. Adjusted relative risk for the prescription rate of secondary medical prevention six months after primary vascular reconstruction ACE/ATII: angiotensin-converting enzyme inhibitor and angiotensin II receptor antagonist; adj.: adjusted; RR: relative risk Data adjusted for age, gender, the Charlson comorbidity index, socioeconomic status (gross income, education level, marital status and employment), smoking, acute/elective surgery, discharge destination and patency at discharge Combination therapy: lipid-lowering, anti platelet and at least one blood pressure lowering treatment.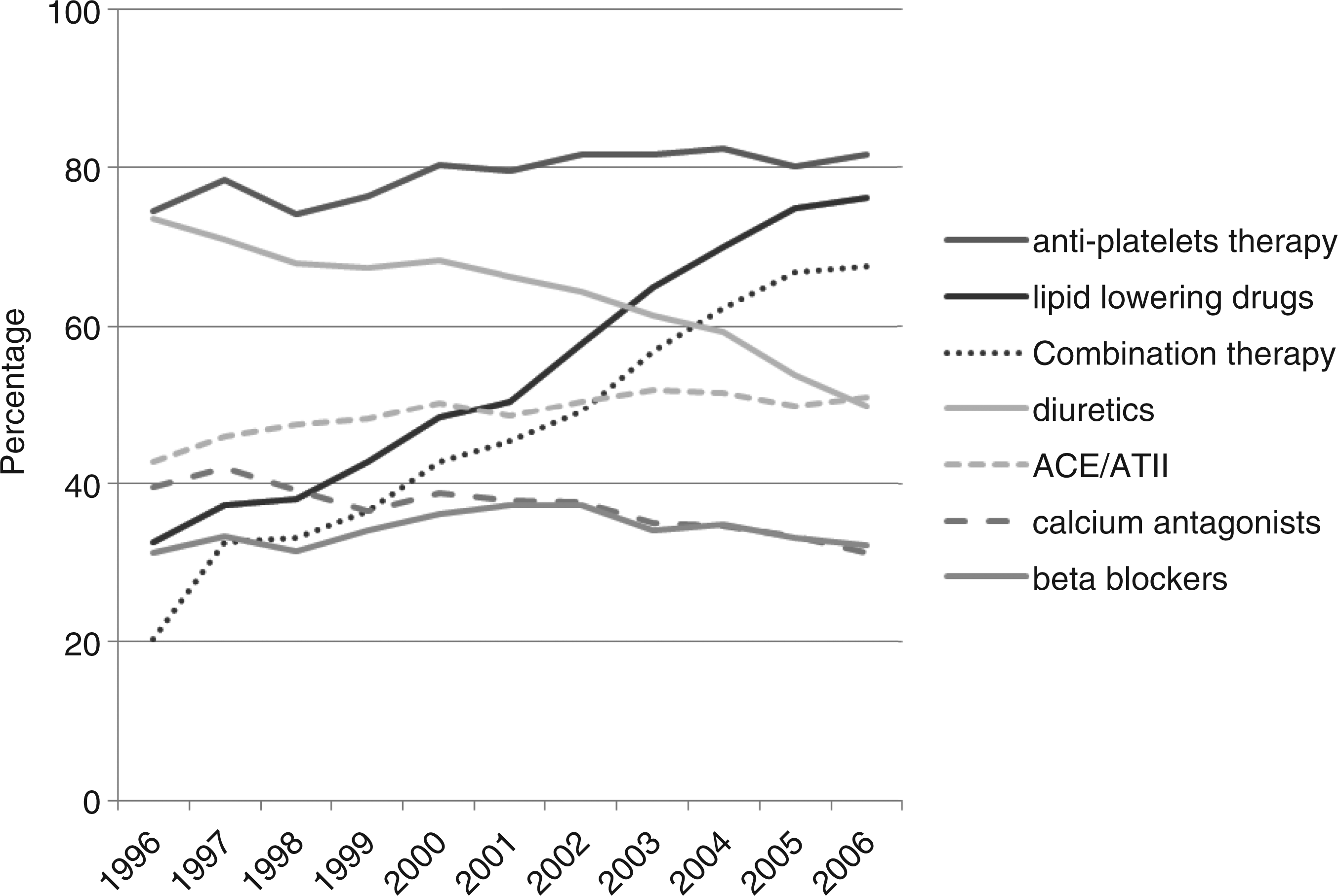
In the early time period (1996–2000) before the publication of guideline recommendations, 2.8% of the patients did not did not receive any prescriptions for secondary medical prevention. This proportion was reduced to 1.4% in the late period (data not shown).
The same pattern from the overall analyses remained when the analyses were stratified according to the county of residence. No major differences in the use of secondary medical prevention were observed across counties (data not shown).
Discussion
We found a substantial increase in the use of lipid-lowering drugs and combination therapy (concomitant filling of prescriptions for lipid-lowering, antiplatelets and at least one antihypertensive drug) in Danish PAD patients who underwent primary vascular reconstruction between 1996 and 2006. This increase was not explained by changes in sociodemographic and clinical factors. In contrast, the overall use of antihypertensive therapy was unchanged over the observed period, but the treatment shifted from diuretics/calcium antagonists towards ACEs/ATIIs.
Our study covered a decade in which the evidence for and attitudes towards the use of secondary medical prevention in PAD patients have changed markedly. The first Trans-Atlantic Inter-Society Consensus (TASC I) 22 recommended aspirin and statins to all PAD patients in 2000. The recommendations for the use of heart rate- and blood pressure-lowering agents were added in 2007 (TASC II). 5 Specific Danish guidelines were first published in 2005. 8 Previous studies confirm that guideline implementation in daily practice is a challenge both in symptomatic as well as asymptomatic patients at high cardiovascular risk. The publication of clinical guidelines does not necessarily lead to improvements in medical care but improvements may be achieved when guidelines are introduced in the context of rigorous evaluations. 25
Recently, the use of secondary medical prevention has received increasing attention in Denmark, especially for high-risk individuals such as PAD patients. However, the use of secondary medical prevention was not systematically monitored during the study period. These gaps may explain the increased use of secondary medical prevention in Denmark following the publication of the international guidelines in 2000. However, the proportion of patients treated remain lower than the guideline recommendations years after their publication.5–8 Another factor of importance may be the organisation of care. Traditionally, the medical treatment of PAD patients has in most health care systems not belonged to a well-defined dedicated speciality as patients with ischemic stroke and acute coronary syndrome. The vascular surgeon takes care of the peri-operative pharmacologic treatment whereas the general practitioner undertakes the recurrent secondary medical prevention after discharge.
Central components in ensuring optimal adherence to guideline-based secondary medical prevention are therefore likely to be close monitoring and auditing of the use of secondary medical prevention combined with comprehensive multidisciplinary cooperation between the general practitioner and the vascular surgeon.
Strengths and limitations of this study
The strengths of our study included the population-based design, the availability of detailed individual-level data and complete follow-up. The validity of our estimates depends on the accuracy of the data sources, and the accuracy of the Danish Vascular Registry is high. 16 Our study confirmed this accuracy because the data from the Danish Vascular Registry were in good agreement with information from the patient medical records. The validity of the Danish Patient Registry is also high for a range of diagnoses, including myocardial infarction, cancer and diabetes. 26 However, potential residual or unaccounted confounding factors can never be totally excluded despite the adjustment for a wide range of covariates (e.g. data on the possible contraindications to secondary medical prevention were missing).
Furthermore, filled prescriptions were used as a proxy for actual drug use. Therefore, patient ingestion of prescriptions could not be guaranteed, but the out-of-pocket payments for prescriptions were likely to reflect actual drug use. Whether any lack of drug use reflected the absence of a physician prescription or the failure of the patient to fill the prescription could not be ascertained.
The lack of any major variation in the use of secondary medical prevention across counties may not reflect an absence of geographic variation at a more local level. Nevertheless, our findings indicate that the overall population was offered similar healthcare service regardless of their administrative area of residence.
Conclusions
A substantial increase in the use of lipid-lowering drugs and combination therapy and no major geographic variation were observed in PAD patients who underwent primary vascular reconstruction from 1996 to 2006. However, the use of secondary medical prevention remained lower than current national and international clinical guideline recommendations. Continuous efforts are warranted to ensure the full implementation of evidence-based recommendations on the use of secondary medical prevention in PAD patients.
Footnotes
Acknowledgments
The authors would like to thank the Danish Vascular Registry for data access.
Funding
The authors thank the Danish Heart Foundation and the Health Department of Viborg County for their financial support.
Conflicts of interest
The authors declare that there are no conflicts of interest.