
Abstract
Background:
Resistance training has become a mainstay of exercise training in type 2 diabetes mellitus (T2DM). However, it remains controversial whether hypertrophy resistance training (HRT) is superior to endurance resistance training (ERT) with regard to its effects on glycaemic control, muscle mass and strength.
Methods:
Thirty-two patients with T2DM (13 men and 19 women; 64.8 ± 7.8 years) were randomly assigned to either eight weeks of HRT (n = 16; 2 sets, 10–12 repetitions, 70% of the one-repetition maximum (1-RM)) or ERT (n = 16; 2 sets, 25–30 repetitions, 40% 1-RM). In addition, all patients participated in aerobic exercise training (AET; 1 hour/day on 2 non-consecutive days/week; cycle ergometer; 70% of heart rate reserve).
Results:
After eight weeks of intervention, there were time but not group effects for reduced glucose and fructosamine levels, weight, BMI, waist circumference, subcutaneous abdominal fat, resting heart rate, systolic and diastolic blood pressure; muscle mass of the arms and physical exercise capacity increased significantly. Significant time and group effects were documented for maximum strength of the chest, with a greater increase for HRT than ERT (p = 0.01).
Conclusions:
Specific maximal resistance training of the chest muscles led to superior gain in strength as compared to endurance resistance training. This, however, did not translate into superior values of glycaemic control, weight, waist circumference, muscle mass and physical work capacity, which all improved significantly by a similar magnitude in both groups. Since overall effects of both protocols were comparable, both may be offered to patients according to their personal preference.
Keywords
Introduction
Aerobic exercise training (AET) has become a mainstay in secondary prevention of type 2 diabetes mellitus (T2DM).1–3 Resistance training, however, has received little attention despite the fact that skeletal muscle accounts for up to 40% of total body weight and is responsible for approximately 75% of whole body insulin-stimulated glucose uptake. This is unjustified, since combination of aerobic and resistance training produces superior results on glycaemic control as compared to aerobic or resistance training alone.4,5 Furthermore, resistance training has been shown to improve insulin-stimulated glucose uptake in patients with T2DM, and likewise to improve muscle strength in elderly subjects with or without T2DM. 6 Furthermore, muscle strength but not muscle mass is independently associated with physical performance 7 and mortality. 8 It still remains unclear, however, which is the more effective kind of resistance training for T2DM.
Hypertrophy resistance training (HRT) has been shown to induce muscle fibre hypertrophy and subsequently muscle mass and strength,9,10 and these effects are more pronounced if heavy weights are chosen, which only allow a few repetitions until fatigue is reached. Among other beneficial changes, blood glucose levels5,11 and insulin sensitivity12,13 improve. As a consequence, professional societies recommend HRT in their current guidelines.14–16 Unfortunately, not all patients are able to lift heavy loads due to orthopaedic problems or because they prefer lighter weights. Even though endurance resistance training (ERT) is a common mode of exercise training in athletes,17,18 it has received very little attention in rehabilitation programmes. This is surprising since cycle ergometer training – a type of endurance resistance training – has been shown to exert an array of beneficial effects leading to a decrease in fasting blood glucose levels, HbA1c, weight and waist circumference, and an increase in oxidative enzyme activity and capacity of skeletal muscle, 19 a gain in muscle mass and strength, and a concomitant reshift to type I fibres.5,20–28 Furthermore, in patients with T2DM we found improved mRNA expression of diabetes candidate genes in skeletal muscle, with mRNA expression of AdipoR1, AdipoR2, Glut4, IL-6, eNOS, PGC-1α showing a linear increase during the course of the study, whereas oxidative stress-related genes p22, gp91, haem oxygenase, PPARα, and PPARγ showed a transient increase during the first 4 weeks, but were normalized during a further 5 months of training. 21 Stimulated by these and other findings, we initiated this study in order to assess whether combined AET and HRT or ERT of the upper body induces comparable effects on body composition, glycaemic control, and muscle mass and strength.
Methods
Study population
In our study, 32 patients (mean age 64.8 ± 7.8 years; 13 men and 19 women) with T2DM were randomized between two supervised groups of either HRT or ERT, which were both performed in combination with AET.
Inclusion criteria were T2DM diagnosed at least 6 months prior to screening, and the ability to perform physical exercises. Exclusion criteria were myocardial infarction within the previous 6 months, unstable angina pectoris or left ventricular ejection fraction of less than 40%. Medication remained unchanged throughout the course of the study.
The study protocol was approved by the ethics committee of the State of Salzburg, Austria, and written informed consent was obtained from all patients prior to enrolment.
Body composition
Body height, weight and waist circumference were measured. Waist circumference was measured using a measuring tape with a spring handle in the standing position, midway between the lowest rib and the iliac crest (highest point of the ilium). 29
Whole body fat mass and muscle mass were determined by DEXA-scan. Calculations were performed using software version 12.4.2 for whole body measurements (QDR 4500 W Hologic, Inc, Bedford, MA, USA). Pre- and post-scans for all patients were analysed by the same technician who was blinded to their origin. Daily quality assurance for body composition measurements was performed according to the manufacturer’s guidelines.
Quantitative computer tomography was performed for the assessment of abdominal fat distribution in all patients with a 4-slice multi-detection computer tomograph (Somatom volume zone, Siemens) before and after 8 weeks of training. To limit radiation, a single computer tomography scan was obtained at the level of L3 to L4 of the lumbar vertebrae during each examination. From these single sections, quantitative assessment of body fat distribution was performed on a workstation (Extended Brilliance Workspace, Philips). Fat was defined visually and by measurement of Hounsfield Units (HU) ranging from −50 to −250. Quantitative assessment of body fat was performed manually on 2D images by outlining boundaries using a spline region of interest (ROI). The area between the body periphery and the muscular abdominal wall was defined as subcutaneous fat area. The intra-abdominal fat area was outlined manually by excluding bones, the muscular abdominal wall, retroperitoneal muscles, bowels and large vessels within the abdominal cavity. Subcutaneous and intra-abdominal fat areas were assessed separately and their sum was defined as the total fat area.
Haematology and blood chemistry
Samples of venous blood (50 ml) (BD Vacutainer®, Heidelberg, Germany) were drawn after a 10-hour overnight fast and at least 16 hours after training sessions. Routine laboratory blood analyses included HbA1c, fasting glucose, fructosamine, and lipid profile (trigylcerides, total cholesterol, HDL and LDL). Blood samples were analysed at the University Institute of Laboratory Medicine, Paracelsus Medical University Salzburg, Austria (Roche/Hitachi Systems, Roche Diagnostics® GmbH, Mannheim, Germany).
Physical work capacity
Cycle ergometry was performed on an electronically braked ergometer (Ergoline® ergoselect 200) with blood pressure measurements during progressive incremental work rates. Ergometry started at 25 W with a pedaling rate of 60–70 rotations per minute (rpm), followed by 2-minute progressive incremental work rate increases of 25 W until exhaustion. Patients’ state of exhaustion was estimated according to Borg. 30 Furthermore, maximal heart rates of each patient at baseline and after 8 weeks of exercise were compared.
Maximum strength test
Prior to training intervention, the intensity for both resistance-training protocols (HRT and ERT) was determined by using a maximal dynamic strength test (Concept2® dyno) for two muscle groups – pectoral and latissimus muscles. The Concept2® dyno is a dynamometer that creates resistance by a flywheel that is specifically designed to produce a resistance range from 0 to 500 kg. A maximum of three tests was performed in order to avoid muscle fatigue. All patients did a 5-minute warm-up prior to testing maximal strength. The handlebar was adjusted to the level of the patients’ sternum; three warm-up lifts were done before the monitor asked patients to perform three maximum lifts with exactly 3 s of recovery between efforts.
Exercise training intervention
In order to compare two standard protocols of resistance training, patients were randomized between two supervised HRT or ERT programmes, which were both performed in addition to 8 weeks of AET. Resistance training, which was not aimed to be isocaloric, was nevertheless carried out at comparable energy costs of 186 MET/min in HRT and 162 MET/min in ERT.
Aerobic exercise training (AET)
All patients performed supervised AET for 8 weeks on cycle ergometers (Daum® fitness 3, Fürth, Germany) on 2 non-consecutive days per week. Sessions consisted of 5 minutes warm up, 60 minutes cycling and 5 minutes cool down. Exercise intensity and training heart rate reserve (HRR) were derived from the Karvonen-Formula. 31
Resistance training
Strength training of the upper body was performed on a multi weight-lifting machine (Nautilus® NS200, Köln, Germany) for 50 minutes per session. Exercises included chest press, back pull, latissimus pull down, biceps curl, seated rowing and upright rowing. HRT consisted of two sets of 10–12 repetitions for each muscle group with 3–5 minutes rest between sets. Weights for each exercise were set at 70% of the patient’s one-repetition maximum. Whenever patients were able to perform ≥12 repetitions, weights were increased. ERT consisted of identical exercises as HRT, but with 40% of the one-repetition maximum as training load for two sets of 20–30 repetitions with 3–5 minutes breaks between sets. Weight was increased whenever patients were able to perform ≥30 repetitions. Sessions were concluded with 5 minutes of stretching exercises.
Statistical analyses
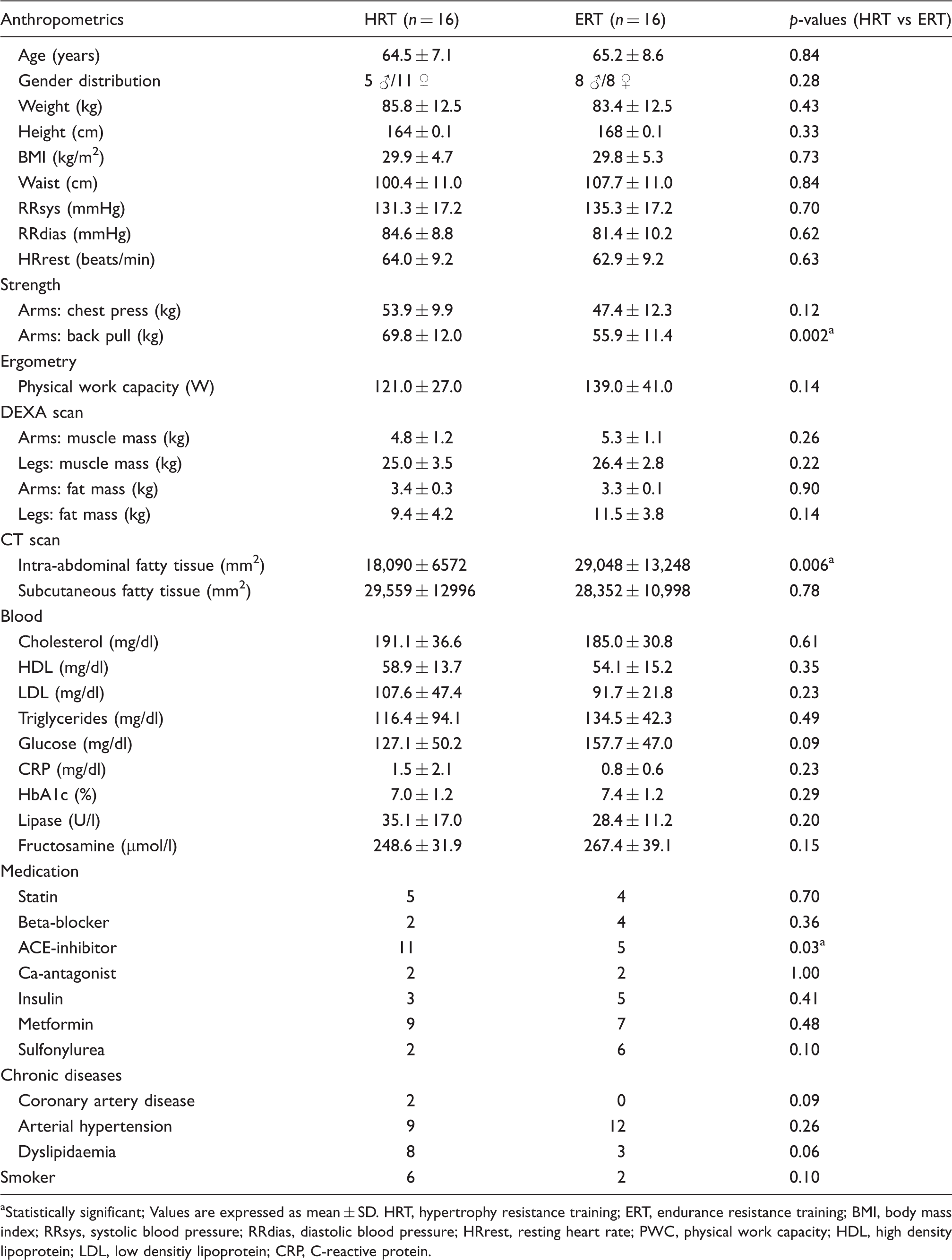
We performed a power analysis, revealing that significant results for the primary endpoints weight, waist circumference and BMI were to be expected from twenty-four patients upwards. As a consequence, we randomized all 33 patients that met the inclusion criteria into two groups (Figure 1). All other parameters were considered secondary outcome measures (Table 1). Groups were not matched with respect to target variables.
Flow chart of patients’ enrolment. Baseline characteristics aStatistically significant; Values are expressed as mean ± SD. HRT, hypertrophy resistance training; ERT, endurance resistance training; BMI, body mass index; RRsys, systolic blood pressure; RRdias, diastolic blood pressure; HRrest, resting heart rate; PWC, physical work capacity; HDL, high density lipoprotein; LDL, low densitiy lipoprotein; CRP, C-reactive protein.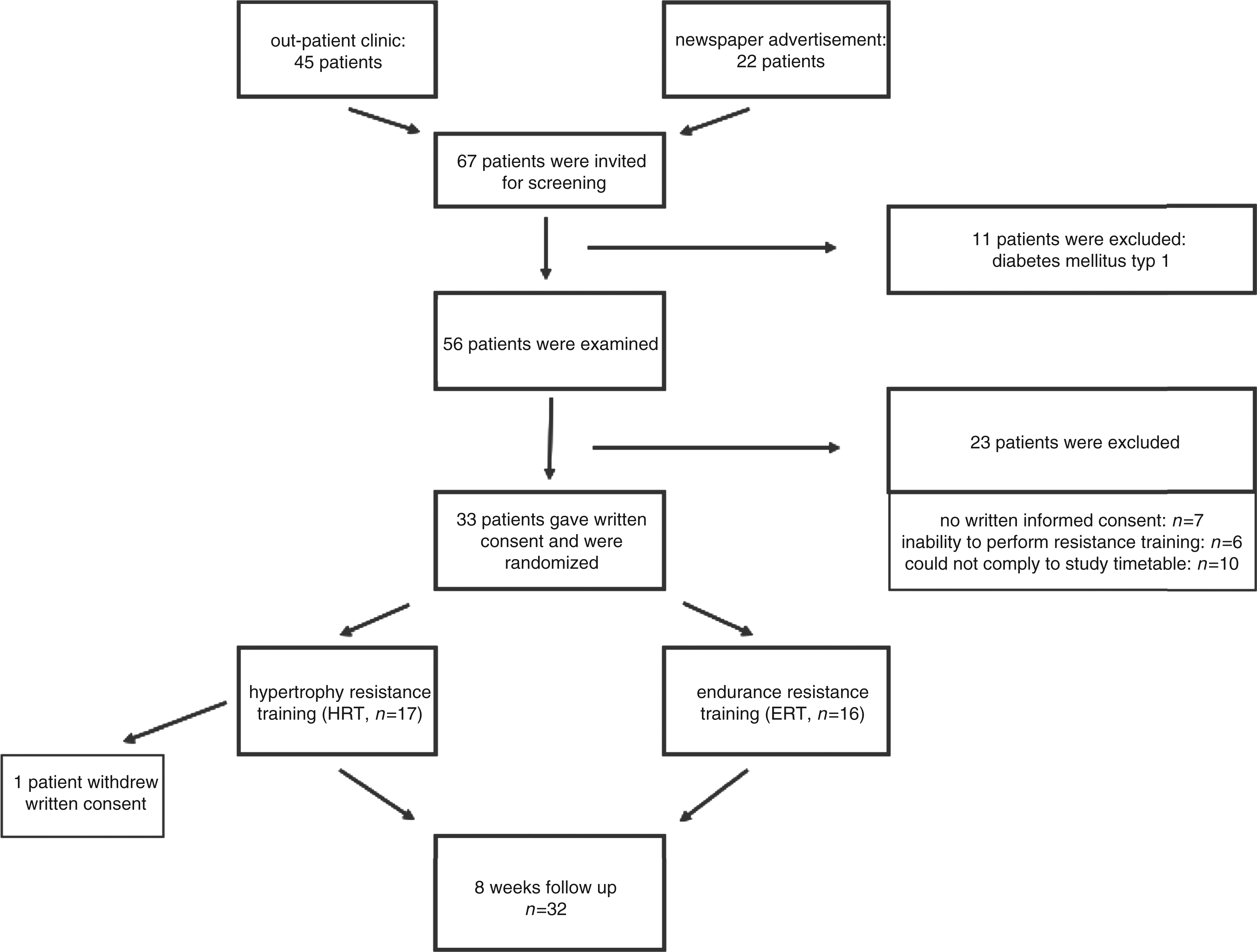
Measurements at baseline and after 8 weeks of study
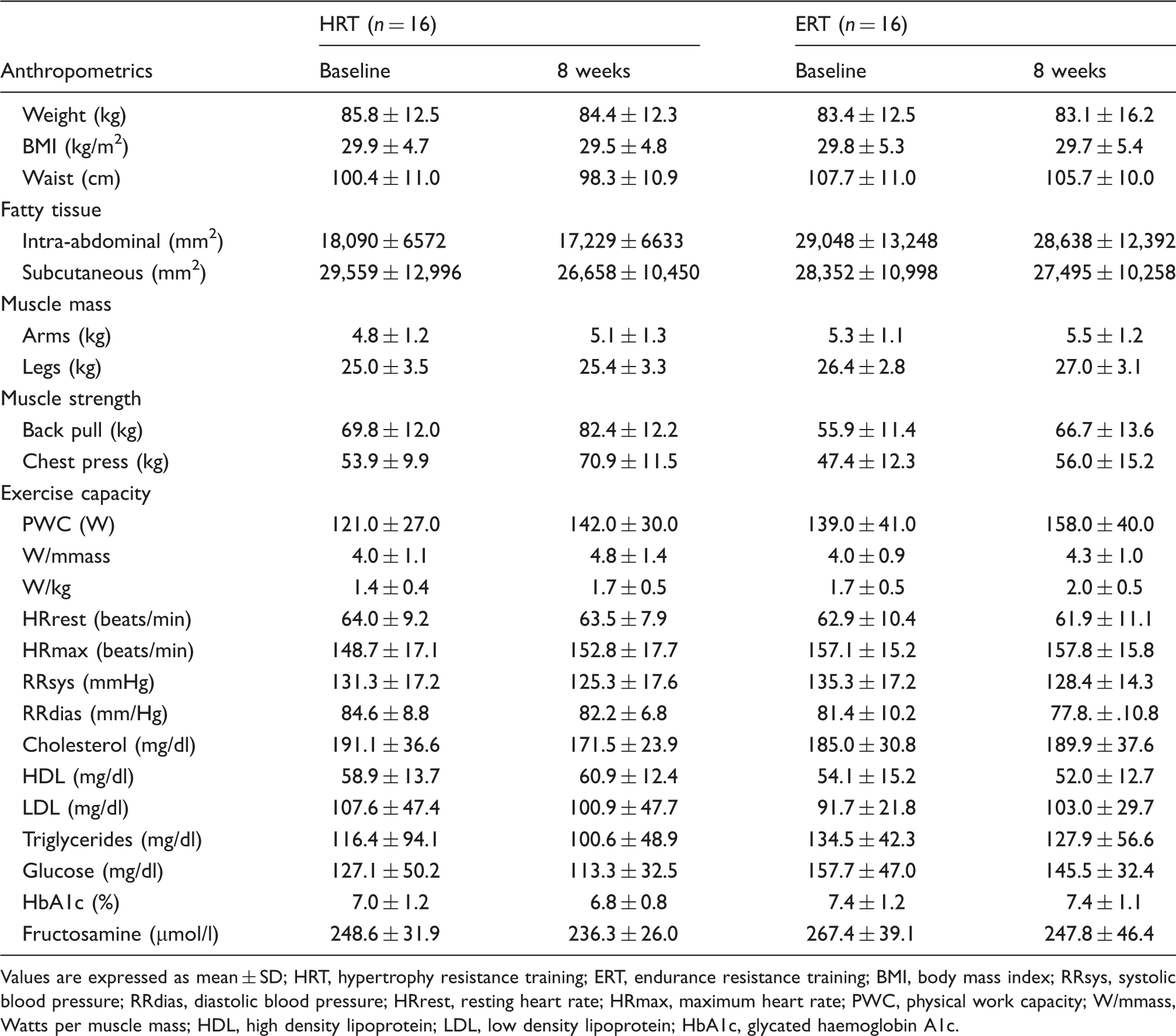
Values are expressed as mean ± SD; HRT, hypertrophy resistance training; ERT, endurance resistance training
BMI, body mass index; RRsys, systolic blood pressure; RRdias, diastolic blood pressure; HRrest, resting heart rate
HRmax, maximum heart rate; PWC, physical work capacity; W/mmass, Watts per muscle mass; HDL, high density lipoprotein
LDL, low density lipoprotein; HbA1c, glycated haemoglobin A1c.
Furthermore, a two-way-analysis of variance (ANOVA) with repeated measures was calculated with the factors group (two steps) and time (two steps). The main focus was attached to the interaction of time and group to assess intervention-induced effects. Greenhouse-Geisser corrected values are reported.
Differences of medication use, gender and chronic diseases were assessed by Chi2 tests where Fisher’s exact test results are reported.
For all calculations, a statistical probability of p < 0.05 was considered significant.
Results
Baseline characteristics
Thirty-three patients gave written content and were randomized; all but one completed the study (Figure 1). No exercise-related injuries occurred during the study. At baseline, there were no significant differences between groups, with the exception of intra-abdominal fatty tissue (p = 0.006) and arm strength in back pull (p = 0.002; all values are depicted in Table 1).
Body composition, glycaemic control and dyslipidaemia
Both interventions were accompanied by a significant reduction in waist circumference (p < 0.001), weight loss (p = 0.01), and BMI (p = 0.03). Furthermore, after 8 weeks of training there were significant reductions in fasting glucose (p < 0.01) and fructosamine (p < 0.01) in both groups over time, but without significant effects on interaction in time and group.
HbA1c remained essentially unchanged but with a trend towards significant reduction over study time in both groups (p = 0.08). There were no significant differences between groups except for glucose, where values were lower in HRT than ERT (p = 0.03).
Total cholesterol remained unchanged with regard to the factor time but showed a significant interaction in time and group (F(1,30) = 5.82, p = 0.02, η2 = 0.16). Data showed a significant decrease in HRT and a small increase in ERT with no significant effects over time and between groups. Between-group comparisons of lipid parameters revealed no statistical differences.
Results of two-way-ANOVAs with repeated measures for selected anthropometric, metabolic and exercise parameters
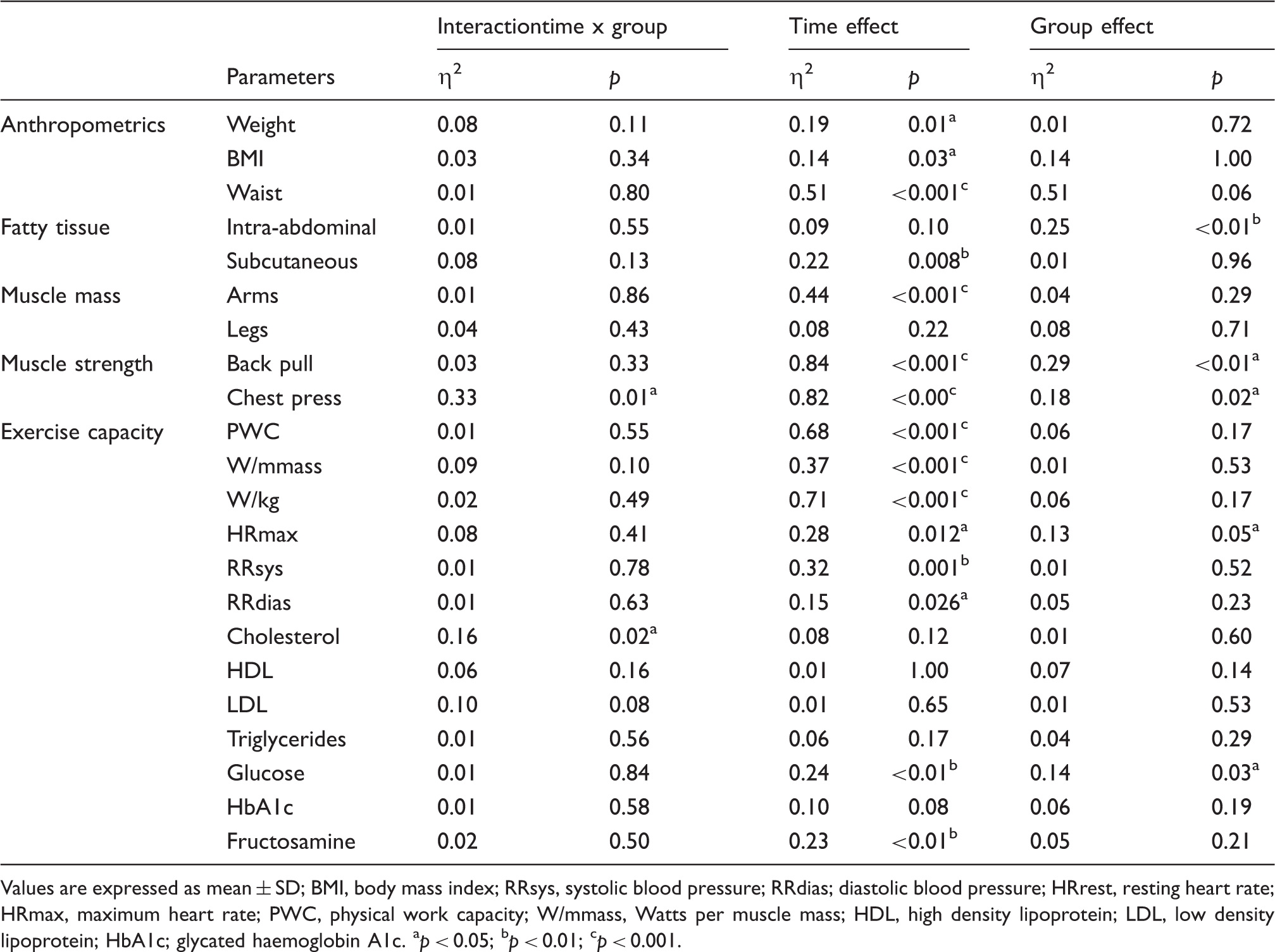
Values are expressed as mean ± SD; BMI, body mass index; RRsys, systolic blood pressure; RRdias
diastolic blood pressure; HRrest, resting heart rate; HRmax, maximum heart rate; PWC, physical work capacity
W/mmass, Watts per muscle mass; HDL, high density lipoprotein; LDL, low density lipoprotein; HbA1c
glycated haemoglobin A1c. ap < 0.05; bp < 0.01; cp < 0.001.
Intra-abdominal and subcutaneous fat
While neither intervention led to any statistically significant change in intra-abdominal fat except for a group effect (p < 0.01), subcutaneous fat was significantly reduced in both groups (p = 0.008), without showing superior results for one of the interventions. Both body weight (p = 0.01) and subcutaneous fat (p = 0.008) were reduced over time, whereas muscle mass in the arms was significantly increased over the study period (p < 0.001). Changes were of comparable magnitude in both groups without significant differences between groups (all p = NS).
Physical work capacity
After 8 weeks of study, there was a significant improvement in physical work capacity of 17% in the HRT and 14% in the ERT group (p < 0.001) (Figure 1), while no significant difference between groups (p = 0.17) and no significant interaction of time and group (p = 0.55) was observed (Table 3).
Muscle mass and strength
A significant increase in upper arm muscle mass was observed in both groups after 8 weeks of intervention (p = 0.01), while no significant differences were observed between groups. Leg muscle mass remained essentially unchanged. Significant improvement over time was observed in muscle strength during chest press (p < 0.001) and back pull (p < 0.001) in both groups. Between-group comparison showed significant differences in muscle strength during back pull (p < 0.01) and during chest press (p = 0.02). Analysis of interaction in time and group demonstrated a significant increase in muscle strength during chest press in HRT (p < 0.001) (Figure 2).
Change in chest press strength before and after 8 weeks of intervention (n = 32). A significant improvement over time was observed in muscle strength during chest press (p < 0.001) in both groups. Between-group comparison showed significant differences in muscle strength during chest press (p = 0.02). Analysis of interaction in time and group demonstrated a significant increase in muscle strength during chest press in HRT (p < 0.001).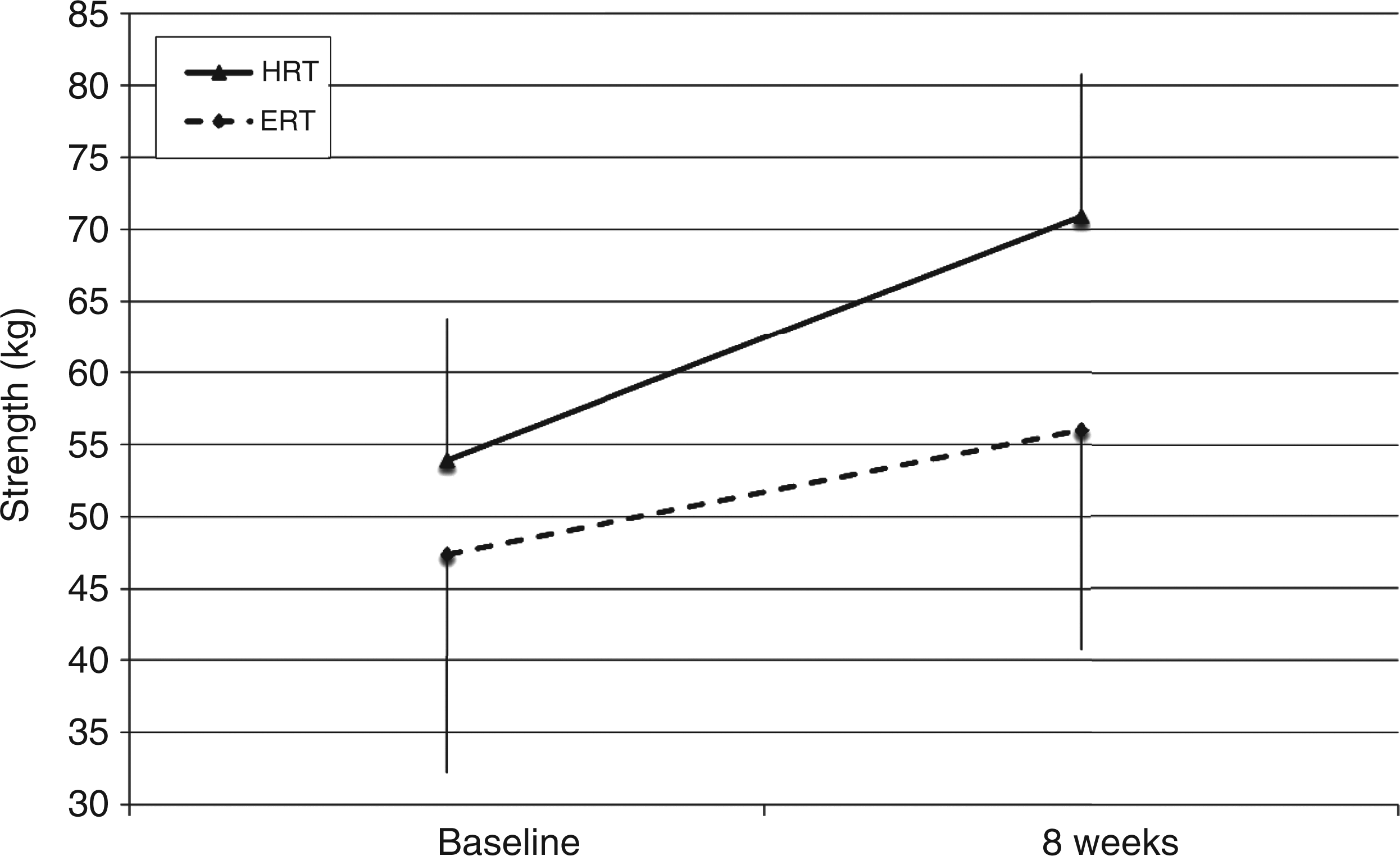
Discussion
The main findings of this study are: (1) Eight weeks of combined AET with either HRT or ERT induce comparable beneficial effects on glycaemic control, body composition, physical work capacity and muscle mass; and (2) Both resistance training protocols prove largely equipotent and safe, and can thus be included into the exercise regime of patients with T2DM according to their personal preference.
Physical work capacity
While AET has become a mainstay of diabetes therapy,1,16,32,33 strength training has only recently received recognition, due to several studies demonstrating strikingly beneficial effects.24,34,35 In our study, 8 weeks of combined endurance and strength training induced a significant increase in physical work capacity both in the HRT and ERT groups, which was comparable with changes reported in the current literature, 23 and without one training modality being superior to the other.
Body composition, intra-abdominal and subcutaneous fat
Patients with T2DM are frequently obese and have abnormal amounts of intra-abdominal and subcutaneous fat. The accumulation of intra-abdominal fat especially increases the risk of developing metabolic and cardiovascular diseases. 36 Furthermore, a reduction of intra-abdominal fat has been shown to be of prognostic importance.36,37 In this study we assessed both intra-abdominal and subcutaneous fat. For intra-abdominal fatty tissue there was a group effect but not a time one. This indicates that it was not the intervention itself, but the group assignment, with significantly lower baseline values in the HRT group, leading to lower absolute values after 8 weeks of study as compared to ERT. For subcutaneous fatty tissue, there was a significant time effect but not a group one, indicating that both programmes led to a reduction in subcutaneous abdominal fat of similar magnitude.
We also observed in both groups a significant reduction in waist circumference, body weight and BMI over time, which is well in keeping even with programmes that ran for longer periods of time; 38 there was no group effect.
Metabolic parameters
There was a time and group effect found for glucose and a time effect for fructosamine, which compares well with prior studies.24,39 The finding that there was only a trend for a time effect in HbA1c can possibly be explained by the fact that post-intervention HbA1c levels in other studies were in the same range as baseline levels in our study, i.e. 7.0% in HRT and 7.4% in ERT,11,23 thus making it more likely to achieve improvement. Indeed, Cauza et al. 23 reported a decrease from 8.3 to 7.1% and Castaneda et al. 11 from 8.7 to 7.6%. Also, drug trials have frequently failed to reach lower targets, 40 and most recent data strongly argue whether such low levels should be reached at all since they have been associated with increased mortality.41
Lipid levels
For total cholesterol, we found an interaction in time and group (p = 0.02) in HRT but not ERT. Since resistance training has previously been reported not to be associated with changes in lipid levels, 5 and since our data analysis did not reveal a plausible cause, we believe this to be a chance finding.
Muscle mass and strength
Back pull showed both a time and group effect, implying that both training modalities were effective while changes in HRT were superior to ERT. However, since the improvement within groups was similar in absolute numbers, it was the group assignment, with its significant baseline differences that were maintained throughout the study, rather than the different training modalities that led to a group effect. In both groups, improvement in muscle strength was fully comparable with other studies.23,42,43
In conclusion, 8 weeks of a combined programme of AET with HRT or ERT in T2DM led to a significant reduction of body weight, glucose, fructosamine and subcutaneous fatty tissue, as well as a significant increase in physical work capacity, muscle mass and muscle strength. Since differences between the two resistance training programmes were rather modest, and preferences of patients regarding training modalities and tolerability of heavy weights vary substantially, it appears warranted that training modalities should be left to the patients’ discretion in order to provide a more individualized and thus more attractive exercise training programme, which might lead to improved long-term compliance.
Footnotes
Acknowledgments
Clinical trials number: NCT0121825.
Funding
This study was supported in part by SportUnion Österreich and Fond Gesundes Österreich.
Conflict of interest
The authors declare that there is no conflict of interest associated with this manuscript.