
Abstract
Aims:
We prospectively examined the association of TV viewing, computer use, and total screen time in adolescence, and change in these behaviours, with cardiovascular disease (CVD) risk factors in young adulthood.
Methods and results:
This was a prospective cohort study among Danish men and women (n = 435) followed for up to 12 years. Adiposity, blood pressure (BP), triglycerides, high-density lipoprotein (HDL), glucose, insulin, and self-reported TV viewing and computer use were obtained in adolescence and in young adulthood. A continuous metabolic syndrome z-score was calculated as the sum of standardized values of each risk factor (inverse of HDL). In multivariable-adjusted analyses, TV viewing and total screen time in adolescence were positively associated with adiposity, triglycerides, and metabolic syndrome z-score in young adulthood (p < 0.05). Individuals who increased their TV viewing, computer use, or total screen time with more than 2 hours/day from adolescence to young adulthood had 0.90 (95% CI 0.12 to 1.69), 0.95 (95% CI 0.01 to 1.88), and 1.40 (95% CI 0.28 to 2.51) kg/m2 higher body mass index, respectively, in young adulthood compared with individuals who remained stable or decreased their viewing time. Insulin and metabolic syndrome z-scores were also higher among individuals who increased their TV viewing, computer use, or total screen time more than 2 hours/day compared with individuals who remained stable or decreased their viewing time (p < 0.05).
Conclusions:
Prolonged TV viewing and total screen time during leisure time in adolescence, and increases in these behaviours, are associated with unfavourable levels of several cardiovascular risk factors in young adulthood.
Introduction
TV viewing and computer use are common daily activities during leisure time among children, adolescents, and adults in Western countries.1,2 Among adults, prolonged TV viewing and unspecified screen-viewing time have been consistently associated with greater risk of chronic diseases, premature death, and raised levels of cardiovascular risk factors independent of moderate and vigorous physical activity level (MVPA).3–6 More recently, organizational and national recommendations for sedentary behaviours including screen time for children and adolescents have emerged.7–9 Some of these recommendations state that children and adolescents should limit their recreational screen time to no more than 2 hours/day to minimize health risks.7,8,10 The evidence from prospective studies to support these specific time limits is weak, and it is unknown if time spent on TV viewing and computer use each are independently associated with cardiovascular outcomes. Furthermore, the evidence that childhood or youth screen-viewing time are associated with adult cardiovascular health is scarce.10–12 To extend the evidence that screen-viewing time during youth have health effects later in life, we aimed to examine the association of TV viewing, computer use, and total leisure screen-viewing time in adolescence with cardiovascular risk factors in young adulthood among Danish men and women participating in the European Youth Heart Study (EYHS) with up to 12 years of follow up. We also examined the influence of changes in viewing time on cardiovascular risk in young adulthood.
Methods
Design
The EYHS is an international population-based multicentre study that addresses cardiovascular disease (CVD) risk factors in children and adolescents. 13 The current study is based on the Danish cohort. In this study, a random sample of 658 15-year-old adolescents were invited to participate in 1997–98, of whom 429 (65%) agreed to take part in the study. In 2003–04, another random sample of 771 15-year-old adolescents was invited of whom 444 (58%) agreed to take part. In 2009–10, a 6- or 12-year follow up was conducted where all originally invited participants from 1997–98 and 2003–04 were invited again. The eligible cohort for the current analyses was 435 individuals who had complete data on exposures and outcomes (244 individuals with 6-year follow up and 191 individuals with 12-year follow up). The study was approved by the local scientific ethics committee and all participants gave informed consent to participate.
Television viewing, computer use, and total screen time
At baseline and follow up, TV viewing and computer use time during leisure was obtained by self-report. In both instances, this was done using a computer-based questionnaire. 13 At baseline, two questions were asked about the amount of time viewing TV (before and after school). 14 From these two questions, a summary variable of daily TV viewing time variable in adolescence was constructed (hours/day). Frequency of eating while viewing TV (5-point scale) was also asked. Daily time spent using computer in adolescence was asked in one question. At follow up the participants were asked to report their TV viewing time (hours and minutes) in the morning, afternoon, and evening. Again, a summary variable for daily TV viewing (hours/day) in young adulthood was constructed. Participants were asked about their time spent using a computer during leisure time (hours/day and min/day) separately for surfing the internet, playing games, and other tasks (i.e. word processing). From response to these questions, a summary variable for daily computer use was constructed (hours/day). A total screen time variable (hours/day) was created by summarizing TV viewing and computer use in adolescence and young adulthood, respectively.
Other covariates
Monthly frequency of soft drinks, fruit, and vegetable intake were obtained by self-report in adolescence. Family history of CVD (paternal or maternal, yes/no) and parental educational level were obtained by parental self-report. Parental educational status was defined according to the International Standard Classification of Education (ISCED) (UNESCO 1997). However, as the details obtained of the description of education was insufficient, the ISCED 7-point scale was combined into three new groups (1 = level 1–2; 2 = level 3–4; and 3 = level 5–7). Current smoking status (yes/no) was obtained in young adulthood. MVPA and sedentary time in adolescence was assessed using accelerometry with data reduction as described previously. 15 An output >2000 counts/min (equivalent to walking about 4 km/h) was defined as MVPA and an output <100 count/min was defined as sedentary. MVPA and sedentary time were expressed as continuous variables as percentage of total registered time.
Cardiovascular risk factors
Height, weight, and waist circumference (WC) were measured using standard anthropometric procedures. Fasting blood samples (overnight) were taken in the morning from the antecubital vein. Samples were aliquoted and separated within 30 min, and then stored at −80℃ until they were transported to a WHO-certified laboratory in Bristol and Cambridge (UK) for analysis at baseline and in Cambridge at follow up. Samples were analysed for serum glucose, insulin, HDL cholesterol, and triglyceride. Triglyceride was analysed using the lipase/glycerol kinase/glycerol phosphate oxidase enzymatic method. HDL was analysed using the homogeneous polyanion/cholesterol esterase/oxidase enzymic method. Glucose was analysed using the hexokinase method. Blood lipids and glucose were measured on an Olympus AU600 autoanalyser (Olympus Diagnostica, Germany) at baseline and on a Dade Behring Dimension RxL autonalyser (Siemens Healthcare, UK) at follow up. Insulin was analysed using enzyme immunoassay (microtitre plate format; Dako Diagnostics, http://www.dako.co.uk, at baseline; and 1235 AutoDELFIA automatic immunoassay, Wallac Oy, Finland at follow up). Between-laboratory correlations in lipids, glucose, and insulin for 30 randomly selected samples analysed at both laboratories were 0.94–0.98 at baseline. 14
Resting BP was measured with a Dinamap paediatric and adult neonatal vital signs monitor (model XL; Critikron, Tampa, FL, USA) using an appropriate cuff size. Five measurements were taken at 2-min intervals with the mean of the final three measurements used in all analyses. Prior to measurements individuals were resting for 5 min while seated.
We calculated a continuous metabolic syndrome z-score to preserve statistical power and because the number of incident cases of metabolic syndrome according to the American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI) definition 16 in young adulthood was low (n = 17). The z-score was based on the AHA/NHLBI definition with additional inclusion of fasting insulin. Thus, WC, the mean of diastolic and systolic BP, triglycerides, HDL (inverted), fasting glucose, and fasting insulin were standardized and subsequently summed to create a continuous metabolic syndrome z-score. Standardization in young adulthood (follow up) was done according to the baseline distribution (mean ± SD) of each risk factor.
Statistics
Associations of screen time use in adolescence with cardiovascular risk factors in young adulthood were analysed using multiple linear regression with baseline levels of respective risk factors included as a covariate. In multivariable analyses, we adjusted for parental educational level, current smoking, family history of CVD, frequency of intake of soft drinks, intake of fruit and vegetables, and MVPA. Because we observed no gender- or cohort-dependent associations for any outcomes we present all analysis for men, women, and follow-up time (cohort) combined. Standard linear regression diagnostics were performed, including examining linearity and normality of residuals. Since we and others previously have shown that the association of prolonged TV viewing with metabolic risk may be mediated by adiposity,14,17 we also analysed the association of screen-viewing time with metabolic syndrome z-score without adiposity included but with adjustment for WC in adolescence. Furthermore, we included both computer use and TV viewing in the same model to examine the independent role of each type of behaviour. The association of adolescence TV viewing with each outcome was also analysed with additional adjustment for eating while viewing TV and with adjustment for percentage time spent on sedentary behaviour. Because adiposity also have been shown to predict sedentary time, 18 we also analysed if BMI and WC in adolescence was associated with screen-viewing time in young adulthood.
We then examined the association of change in viewing time with each respective cardiovascular risk factor in young adulthood. We used the difference in young adult and adolescence viewing time as a continuous variable adjusting for adolescence viewing time, and we also analysed change in TV viewing and total screen time as categorical variables using the following categories: stable or decrease (≤0 hours/day), modest increase (>0–2 hours/day), and large increase (>2 hours/day). A test for linear trend across groups of change in the categorical analysis was done by treating the ‘change variable’ as ordinal in the models.
As information on accelerometry measured MVPA and sedentary behaviour at baseline was missing among 161 individuals (37%), we imputed missing values using a multiple univariate linear regression imputation approach (‘mi impute’ in STATA) including all covariates. Beta coefficients and SEs were obtained based on 20 imputed datasets while the variability between imputations is adjusted for. 19 We did not observe appreciable differences in magnitude of effect estimates from complete case analyses compared with analyses on imputed dataset, although the CI’s were wider in complete case analyses.
All statistical analyses were performed in STATA 11.2 with alpha = 0.05 (two-sided). As the study is observational and the nature of the present analysis is exploratory rather than a confirmatory analysis of a clinical trial, no adjustments for multiple testing were carried out.
Results
Baseline characteristics by television viewing time in adolescence
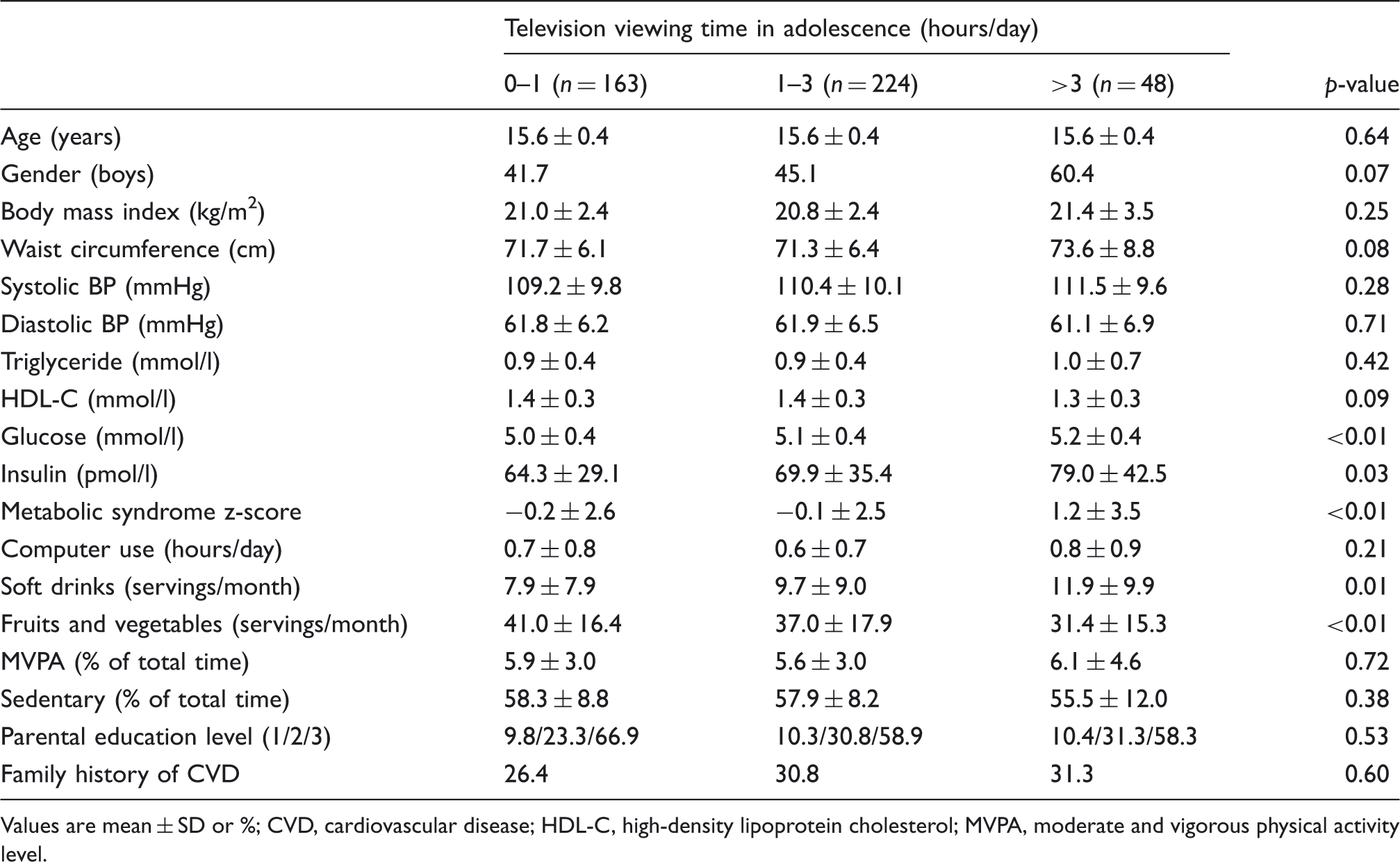
Values are mean ± SD or %
CVD, cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; MVPA, moderate and vigorous physical activity level.
TV viewing, computer use, and total screen time increased noticeably from 1.6 hours/day of TV viewing, 0.6 hours/day of computer use, and 2.2 hours/day of total screen time in adolescence to 3.2 hours/day of TV viewing, 2.9 hours/day of computer use, and 6.1 hours/day of total screen time in young adulthood (Figure 1). Changes were fairly similar in men and women and between cohorts (p > 0.1 for interaction). TV viewing, computer use, and total screen time tracked with stability coefficients (partial correlation coefficients) of 0.36 (95% CI 0.27 to 0.45), 0.15 (95% CI 0.05 to 0.25), and 0.30 (95% CI 0.20 to 0.39) from adolescence to young adulthood (age-, gender-, and cohort-adjusted) indicating moderate tracking of TV viewing and total screen time and low tracking of computer use.
Age-, gender-, and cohort-adjusted estimates (with 95% CI) of TV viewing, computer use, and total screen time during leisure from adolescence to young adulthood (n = 435).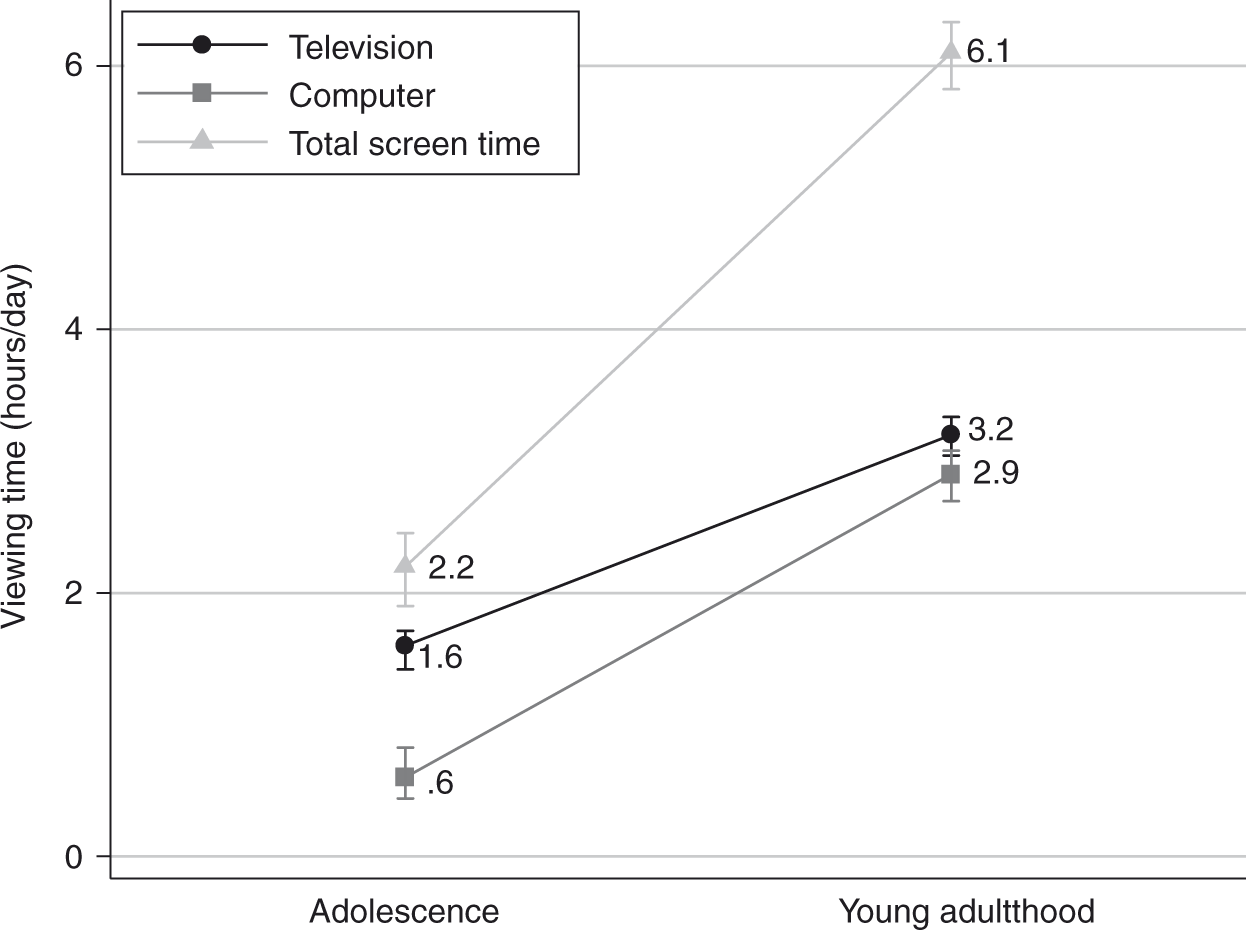
Television viewing, computer use, and total screen time in adolescence and cardiovascular risk factors in young adulthood
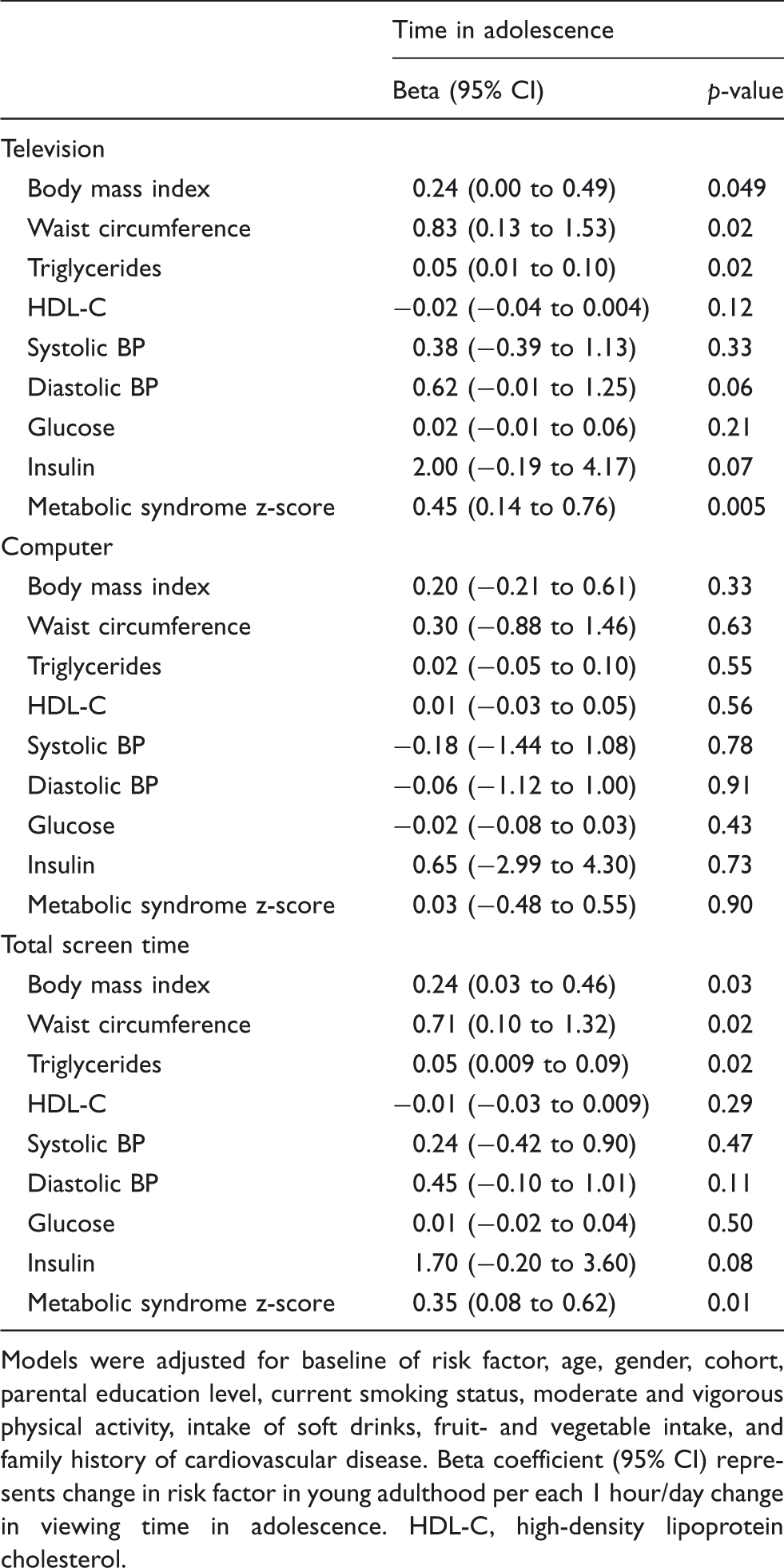
Models were adjusted for baseline of risk factor, age, gender, cohort, parental education level, current smoking status, moderate and vigorous physical activity, intake of soft drinks, fruit- and vegetable intake, and family history of cardiovascular disease. Beta coefficient (95% CI) represents change in risk factor in young adulthood per each 1 hour/day change in viewing time in adolescence. HDL-C, high-density lipoprotein cholesterol.
Change in TV viewing, computer use, and total screen time from adolescence to young adulthood and cardiovascular risk factors in young adulthood
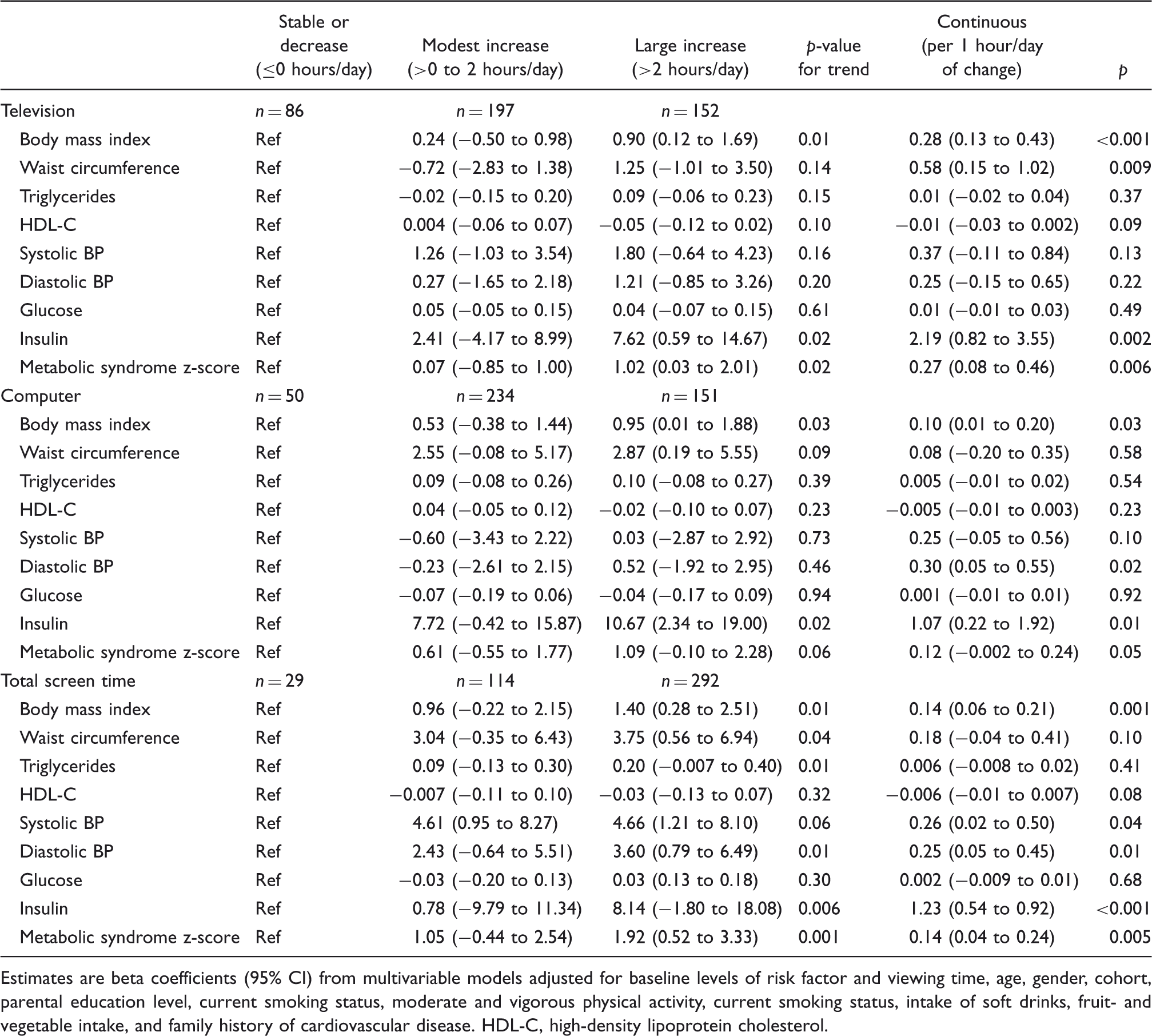
Estimates are beta coefficients (95% CI) from multivariable models adjusted for baseline levels of risk factor and viewing time, age, gender, cohort, parental education level, current smoking status, moderate and vigorous physical activity, current smoking status, intake of soft drinks, fruit- and vegetable intake, and family history of cardiovascular disease. HDL-C, high-density lipoprotein cholesterol.
Discussion
In this population-based prospective study, prolonged TV viewing and total screen time in adolescence, and increases in screen time through young adulthood, were consistently associated with greater adiposity and clustered CVD risk in young adulthood. The associations were independent of various confounding factors, including objectively measured MVPA and showed evidence of dose–response relationships. Associations were generally attenuated after adjustment for viewing time in young adulthood, which suggest that prolonged viewers in adolescence are likely to be prolonged viewers in young adulthood as indicated by the moderate stability coefficients of TV viewing and total screen time. Whereas adolescent computer use was not associated with any of the cardiovascular outcomes in young adulthood, increases in computer use during leisure time from adolescence to young adulthood was associated with higher levels of BMI and insulin in young adulthood independent of changes in TV viewing. Collectively, these findings provide support for recommending limiting screen-viewing time among youth.
Our findings on TV viewing are consistent with a previous study among New Zealanders followed from childhood to young adulthood; in this study, prolonged TV viewing in childhood and adolescence was associated with greater BMI, lower cardiorespiratory fitness, and raised cholesterol in young adulthood independent of physical activity level. 11 Another study from the USA among 13-year-olds followed over 5 years found that TV viewing was positivity associated with the risk of high systolic BP. 20 We extend these findings by showing that both TV viewing and total screen time in adolescence, and change in TV viewing and computer use, are independently associated with unfavourable levels of several cardiovascular risk factors in young adulthood.
Because previous studies among children, adolescents, and adults on the associations of objectively measured sedentary behaviour with cardiovascular risk factors have been equivocal18,21,22 it is unclear if sedentariness per se is the principle cause of the harmful cardiovascular effect of prolonged screen-viewing time. It is possible that especially TV viewing are accompanied by other unhealthy lifestyle, such as eating more unhealthy food and increasing or initiating alcohol drinking or smoking during and beyond TV viewing time,23–25 may exert effects on cardiovascular risk factors beyond what originates from sedentariness. When we adjusted for eating while viewing TV, no change in the estimates was observed; nevertheless, because we observed weaker associations of computer use with cardiovascular risk, it is likely that the influence of prolonged TV viewing at least partly is mediated by these exposures and not only by sedentariness. Possible explanations to why computer use in youth was unrelated to CVD risk factors in young adulthood could be that youth in the present study on average spent little time using a computer, that computer use is less sedentary compared with TV viewing, or that exposure to factors such as food advertisements are more intense for TV viewing compared with computer use. We also found that the association of TV viewing with clustered cardiovascular risk was only partly mediated by adiposity. This is in accordance with studies among adults having incident CVD or type 2 diabetes as outcomes,3,6 but in opposite to our previous cross-sectional analysis among children and adolescents 14 and a previous study among adults. 26
Limited amount of evidence from randomized trials on restricting TV viewing or screen-viewing time exists. However, the few studies that have been carried out provide some support of the associations observed here. Two randomized trials among children have shown that reducing TV viewing time can lead to favourable changes in adiposity status.27,28 Another small-scale randomized trial among overweight or obese adults did not find a statistically significant change in adiposity status from restricting TV viewing time during a period of 3 weeks, but did see an increase in energy expenditure. 29
There are a number of limitations to this study. All screen time measures were self-reported and measurement errors are therefore inevitable. Loss to follow up and missing data can lead to bias if the associations are different in these individuals. We found differences in some baseline characteristics among individuals lost to follow up or with missing data compared with the individuals with complete data. However, associations between TV viewing and outcomes were fairly similar by parental educational level (data not shown), which gives us some confidence that the associations are unaffected by selection bias. In addition, our study was not adequately powered to consistently do stratified analyses by cohort, which could provide valuable information about the timing of interventions to prevent the large increase in viewing time. Other limitations of this study include the possibility of unknown and residual confounding, although we adjusted for important confounding factors including objectively measured MVPA. Because the magnitudes of the multivariable-adjusted estimates were substantial for many of the outcomes, it is unlikely that residual or unknown confounding fully accounts for these associations. Finally, some of the statistically significant findings may arise from multiple testing since we tested several CVD risk factors.
In conclusion, our findings suggest that prolonged TV viewing and total screen-viewing time during leisure time in adolescence, and increases in these behaviours, are associated with unfavourable levels of several cardiovascular risk factors in young adulthood. These findings indicate that efforts to reduce these viewing behaviours in youth would be important to prevent adverse cardiovascular effects in adulthood, and provide support for recommending limits in TV viewing and total screen-viewing time among youth.
Footnotes
Acknowledgements
The authors are grateful to the participants and their families who gave their time to the study.
Funding
This work was supported by the Danish Council for Strategic Research [grant number 2101-08-0058], the Danish Heart Foundation, the Danish Health Fund (Sygekassernes Helsefond), and the Trygfoundation (Trygfonden).
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.