
Abstract
Background:
The association of insulin resistance (IR) with other cardiometabolic risk (CMR) factors in sub-Saharan Africans is poorly documented. This study examined the links between IR and the evolution of blood pressure (BP), glycaemia, serum lipids and abdominal obesity in the population of Benin.
Design:
Population-based longitudinal study.
Methods:
This study initially included 541 apparently healthy Beninese adults (50% women) aged 25–60 years who were randomly selected in a large city, a small town and a rural area. After a baseline survey, our subjects were followed up after 2 years, and again at 4 years. IR based on homeostasis model assessment (HOMA), blood glucose, BP, waist circumference (WC), triglycerides, total cholesterol and HDL-cholesterol were measured. Complete data at the end of the follow-up periods was available for 416 subjects.
Results:
IR was more prevalent in women than in men (33.2% versus 17.8%) and it was generally associated with more adverse values of CMR factors, excepting BP. In controlling for baseline age, sex, WC, diet, lifestyle variables and WC changes; the relative risk (RR) of hyperglycemia over 4 years was as least 3-fold in IR subjects, compared to normal subjects. The RR of abdominal obesity was 5.3 (1.04–26.93) in IR women, compared to non-IR. The association of IR with the evolution of dyslipidemia was inconsistent, but IR tended to exacerbate low HDL-cholesterol.
Conclusion:
Over 4 years, IR exacerbated hyperglycemia in both men and women, and abdominal obesity in women, but IR did not affect blood pressure. Further research on the link found between IR and dyslipidemia, particularly low HDL-C, is needed in sub-Saharan Africa.
Keywords
Introduction
Insulin resistance (IR) is a potent risk factor for cardiovascular disease (CVD) and type 2 diabetes.1,2 More than 346 million people worldwide currently have diabetes; and by 2030, their numbers will more than double without intervention. 3 Additionally, between 2005 and 2030, mortality from CVD is expected to double. 4 The largest share of mortality due to non-communicable diseases is borne by developing countries. 5 Cardiometabolic risk (CMR) factors including hyperglycemia, hypertension and dyslipidemia; their contributions to all-cause mortality 6 are considered largely preventable, so a better understanding of their determinants and evolution may help to tackle the current epidemic. The Benin Study was designed to document CMR factors in this African country. Previous papers reported on the relationship of CMR with urbanization, socioeconomic status, diet and lifestyle, as the result of the initial cross-sectional survey.7–9 The first paper on the longitudinal component of the Benin Study focuses on the impact of initial obesity on CMR: Abdominal or overall obesity was associated with an adverse evolution of cholesterolemia only. 10 We found there is only a trend for increased incidence of IR in obese subjects, in Benin. In this related study, we examine the relationship of IR with high blood pressure (HBP), high fasting glucose, dyslipidemia and abdominal obesity in the same Benin adults. We know that in African Americans, the relationship of IR with hypertension and dyslipidemia appears weaker than in Caucasians, in spite of a higher prevalence of diabetes and CVD; 11 however, the findings in African-Americans may not apply to sub-Saharan Africans. We hypothesized that IR would exacerbate other CMR factors in subjects within Benin.
Methods
Subjects and study design
This longitudinal and observational study included at the onset 541 subjects aged 25–60 years (50% women) randomly selected by a 3-stage sampling method in: a large city (n = 200), a small town (n = 171) and a rural area (n = 170) of Southern Benin, which is a West African country. Subjects with a prior diagnosis of hypertension, diabetes or a cardiac condition were excluded. In the main city, 10 out of the 140 neighbourhoods were randomly selected, after which 20 households were selected per neighbourhood, based on a household list. In each household, only one eligible adult was picked at random, alternating between men and women. In the town of Ouidah, we selected five out of the 22 neighbourhoods and five out of the 38 villages in the surrounding rural areas. Compounds and households within the compounds were given numbers, as there was no household census. In each selected neighbourhood or village, 34 households were randomly selected to have one adult per each household represented.
Following our cross-sectional baseline study (T0), subjects were then followed up, at 2 years (T1) and 4 years (T2) later. Of note, any subjects diagnosed for high blood pressure or diabetes during the initial study or at follow-up remained in the study cohort. Follow-up anthropometric, clinical and biochemical data on CMR factors was available for 416 subjects (77.0%). For sample size calculation, we used blood pressure as the main dependent variable, since hypertension is highly prevalent in this study population. 8 A final sample of 180 subjects was deemed sufficient to achieve 80% statistical power with a significance level (alpha) of 0.05, using repeated measure ANOVA to detect small effect size on blood pressure.
Data collection procedure
Our study was carried out from 2005–2010. Venous blood samples were drawn after a 12-hour overnight fast. Blood samples were kept on ice and centrifuged within 2 hours. Plasma or serum was stored at -30℃ until analysed. Self-help groups were formed with the initial participants (at T1), to facilitate follow-up and then active prevention support once the follow-up study ended. One self-help group was formed per study cluster (selected neighbourhood or village).
Study variables
Anthropometric parameters
We measured height, weight, and waist circumference (WC) with the subjects in the standing position. The average of two separate measures of WC was used in the analyses. Body mass index (BMI) status was categorised as follows: underweight <18.5; normal 18.5–24.9; overweight 25–29.9; obese ≥30. Generic cut-off values of WC for abdominal obesity were 80 cm and 94 cm, respectively, for women and men. 12
Blood pressure
BP was measured using a mercury sphygmomanometer. Systolic and diastolic BP was measured on the right arm of seated subjects after a 10-minute rest. Two readings of systolic and diastolic BP were taken and the mean was used in the analyses. The interval of time between the first and the second reading was at least 20 minutes. HBP was defined as systolic blood pressure (SBP) ≥130 mmHg, diastolic blood pressure (DBP) of ≥85 mmHg 12 or treatment for hypertension.
Biochemical parameters
Using appropriate kits (Elitechgroup, Sées, France) and standard colorimetric enzymatic laboratory methods, we determined fasting glucose, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG). The ratio of TC/HDL-C was computed. Abnormal values were defined as: high fasting glucose (HFG) (≥5.6 mmol/L) or treatment of diabetes; high triglycerides (>1.70 mmol/L); and low HDL-cholesterol (≤1.29 mmol/L in women and ≤1.03 mmol/L in men). The selected cut-offs for high TC/HDL-C were set at 5.0 for men and 4.0 for women. 13 Fasting serum insulin concentrations were determined using a solid phase enzyme-linked immunosorbent assay (ELISA) based on the sandwich principle (IBL, Hamburg, Germany). 14 The analytical sensitivity was 1.76 μIU/ml, with inter-assay and intra-assay coefficient of variation ranges, respectively, of 2.88–5.99% and 1.79–2.6%. The assay was free of pro-insulin cross-reactivity.
Homeostasis Model Assessment (HOMA) for insulin resistance
The HOMA for IR was computed as follows, in equation (1):
The IR cut-off was the 75th percentile of HOMA values in the whole sample of subjects. 15 Diabetic subjects, whether they were treated or not, were considered as insulin resistant, regardless of their HOMA value.
Metabolic syndrome
We used the harmonized definition of the metabolic syndrome (MetS), proposed in a joint interim statement in 2009. 12 Any three of the following five CMR risk factors must be present: abdominal obesity, elevated serum triglycerides, low serum HDL cholesterol, high blood pressure (or treatment for hypertension) and either HFG or diabetes.
Dietary quality
Dietary intake was computed at baseline on the basis of 2–3 non-consecutive 24-hour food recalls. Diet quality was appraised using several scores. In the baseline study, we found that only the micronutrient adequacy score is significantly associated with CMR;. 7 therefore, we used it in the present analyses. The micronutrient score (maximum 14) was based on adequacy of intake of 14 micronutrients, according to World Health Organization/Food and Agriculture Organization (WHO/FAO) recommended dietary intakes for age and sex. 16
Lifestyle variables
Subjects were asked about their habitual drinking patterns based on the STEPwise questionnaire, developed by WHO. 17 The amount of pure alcohol (in gr/day) was computed for use in the analyses. Baseline physical activity was assessed through 2–3 non-consecutive 24-hour recalls. According to the energy expenditure for each activity, estimated in metabolic equivalents (METs), we ranked activities as vigorous, moderate or light. Daily physical activity was computed as total time (min) devoted to vigorous and moderate activities (≥3 METs). We assessed smoking status in interviews, grouping the ex-smokers with smokers.
Statistical analyses
Data were analysed using SPSS, version 16.0 (SPSS Inc., Chicago, IL). HOMA values were log-transformed because of skewing. The relative risk (RR) of developing one or the other CMR factor during the course of the follow-up, according to IR status, was assessed using multiple logistic regression models while controlling for baseline age, diet (micronutrient intake adequacy score), and lifestyle (alcohol consumption and physical activity), as well as WC change between T0 and T2, and participation in the self-help group meetings (a percentage of total meetings attended by an individual). We used a linear mixed model for repeated measures, to compare changes in CMR variables according to IR status during the 4-year period. Subjects under treatment for high blood pressure or for diabetes were excluded when analyses were performed with continuous values of CMR factors. All p values were two-sided, and the significance level was set at p < 0.05.
Ethical considerations
This study was approved by the Ethics Committee of the Faculty of Medicine, University of Montreal and by the Ministry of Health in Benin. Written informed consent was obtained from each participant before enrolment. Participants with abnormal values were referred to a physician for diagnosis and treatment. The first medical consultation and prescription was paid by the research project.
Results
Study subjects
Data on the 416 subjects (out of 541 selected) who completed the last follow-up are presented in this report.
Baseline insulin resistance status and other cardiometabolic risk factors
Cardiometabolic risk factors and insulin resistance status at the Benin Study baseline (n = 416)
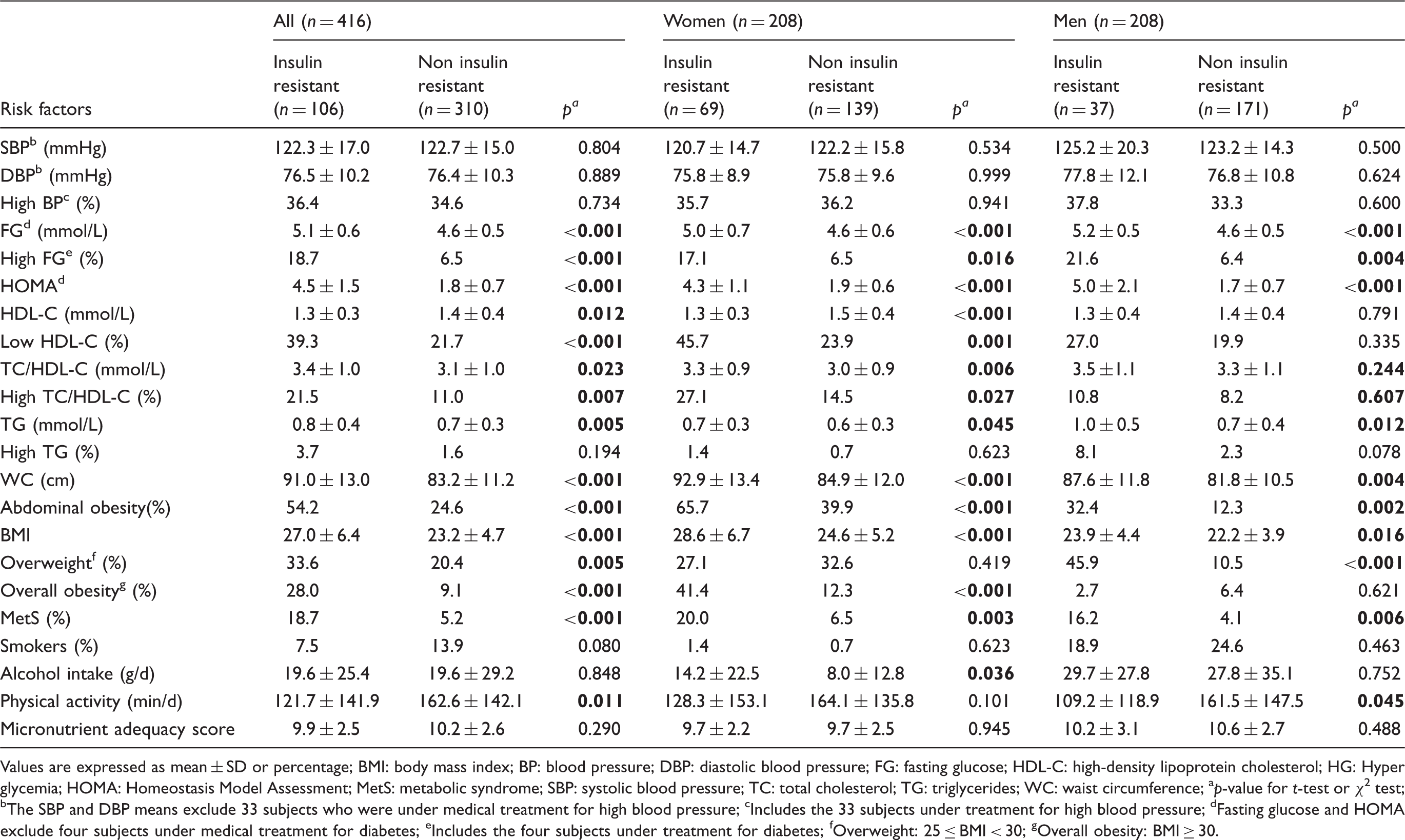
Values are expressed as mean ± SD or percentage
BMI: body mass index; BP: blood pressure; DBP: diastolic blood pressure; FG: fasting glucose; HDL-C: high-density lipoprotein cholesterol; HG: Hyper glycemia; HOMA: Homeostasis Model Assessment; MetS: metabolic syndrome; SBP: systolic blood pressure; TC: total cholesterol; TG: triglycerides; WC: waist circumference
p-value for t-test or χ 2 test
The SBP and DBP means exclude 33 subjects who were under medical treatment for high blood pressure
Includes the 33 subjects under treatment for high blood pressure
Fasting glucose and HOMA exclude four subjects under medical treatment for diabetes
Includes the four subjects under treatment for diabetes
Overweight: 25 ≤ BMI < 30
Overall obesity: BMI ≥ 30.
Four-year changes in cardiometabolic risk factors according to insulin resistance status
Association of insulin resistance (HOMA) with other cardiometabolic risk factors (n = 416)
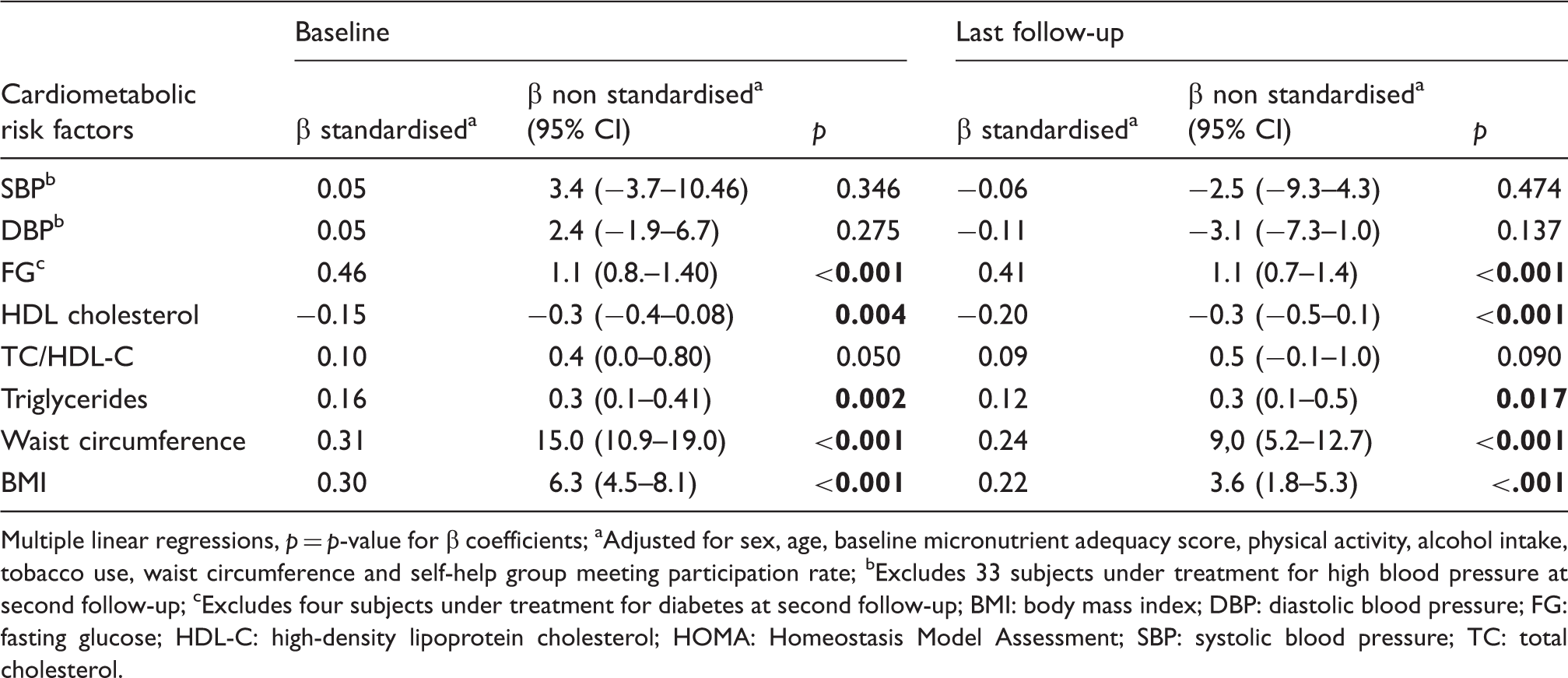
Multiple linear regressions, p = p-value for β coefficients
Adjusted for sex, age, baseline micronutrient adequacy score, physical activity, alcohol intake, tobacco use, waist circumference and self-help group meeting participation rate
Excludes 33 subjects under treatment for high blood pressure at second follow-up
Excludes four subjects under treatment for diabetes at second follow-up
BMI: body mass index; DBP: diastolic blood pressure; FG: fasting glucose; HDL-C: high-density lipoprotein cholesterol; HOMA: Homeostasis Model Assessment; SBP: systolic blood pressure; TC: total cholesterol.
In order to assess the changes in CMR profile during the follow-up period according to IR, we classified subjects into two groups. A ‘favourable’ change in CMR profile meant that there was no CMR factor at either the onset or follow-up, or that the number of CMR factors (other than IR) had declined. An ‘unfavourable’ change refers to either a sustained or increased number of CMR factors. Compared with non-IR subjects, unfavourable changes occurred in a significantly higher proportion in labile IR subjects (81.6% versus 14.4%) and in IR subjects (73.5% versus 26.5%) (data not shown). During this study, 13 new diabetes cases were detected (five cases at the first follow-up and eight at the last follow-up). In the untreated diabetes cases (n = 11), the HOMA mean increased significantly from 2.5 ± 1.1 to 4.9 ± 2.4 (p = 0.004).
Risk of onset of cardiometabolic risk factors over the follow-up period (n = 416)
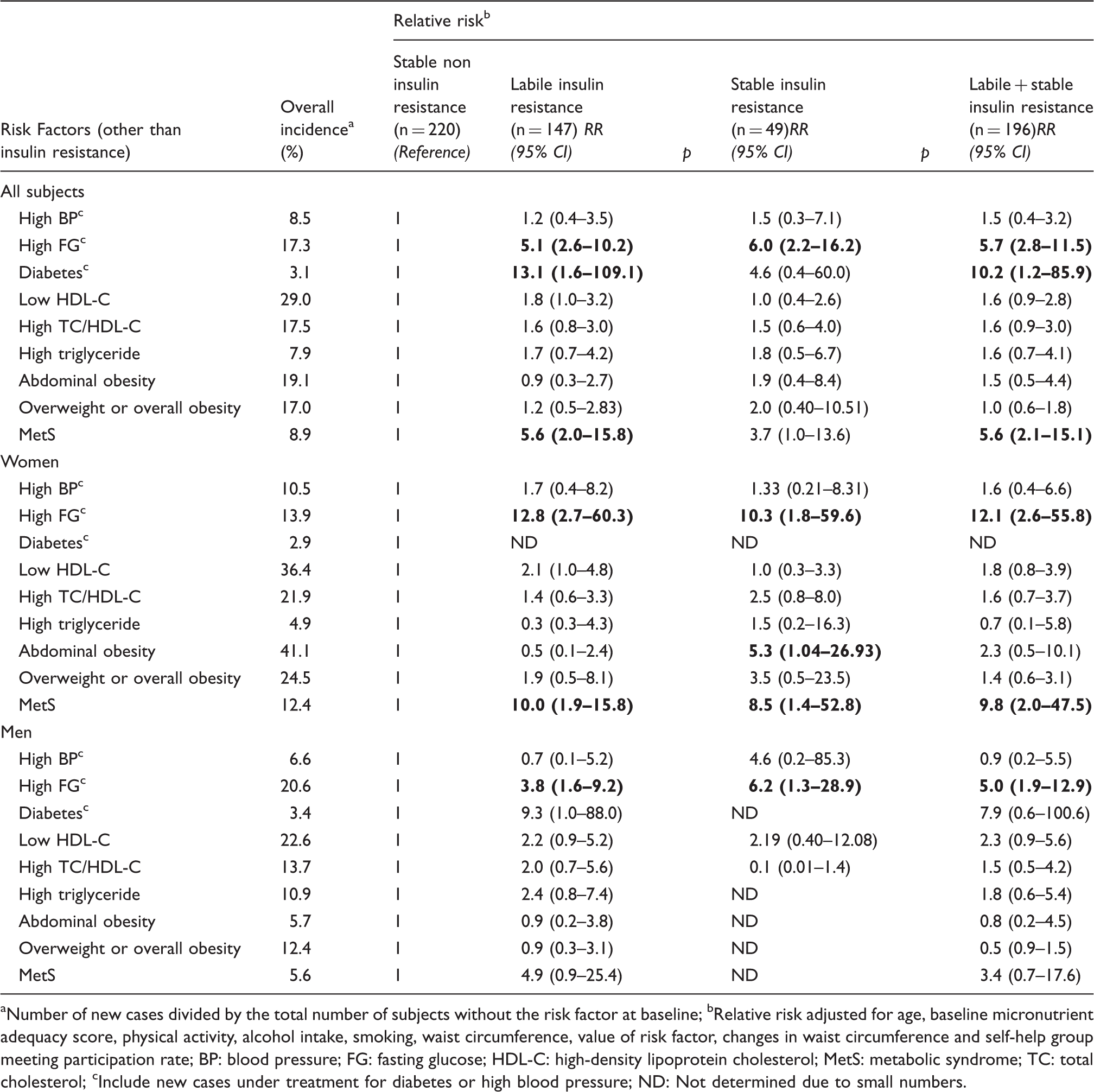
Number of new cases divided by the total number of subjects without the risk factor at baseline
Relative risk adjusted for age, baseline micronutrient adequacy score, physical activity, alcohol intake, smoking, waist circumference, value of risk factor, changes in waist circumference and self-help group meeting participation rate
BP: blood pressure; FG: fasting glucose; HDL-C: high-density lipoprotein cholesterol; MetS: metabolic syndrome; TC: total cholesterol
Include new cases under treatment for diabetes or high blood pressure
ND: Not determined due to small numbers.
Changes in cardiometabolic risk factor means during the follow-up, according to insulin resistance status (n = 416)
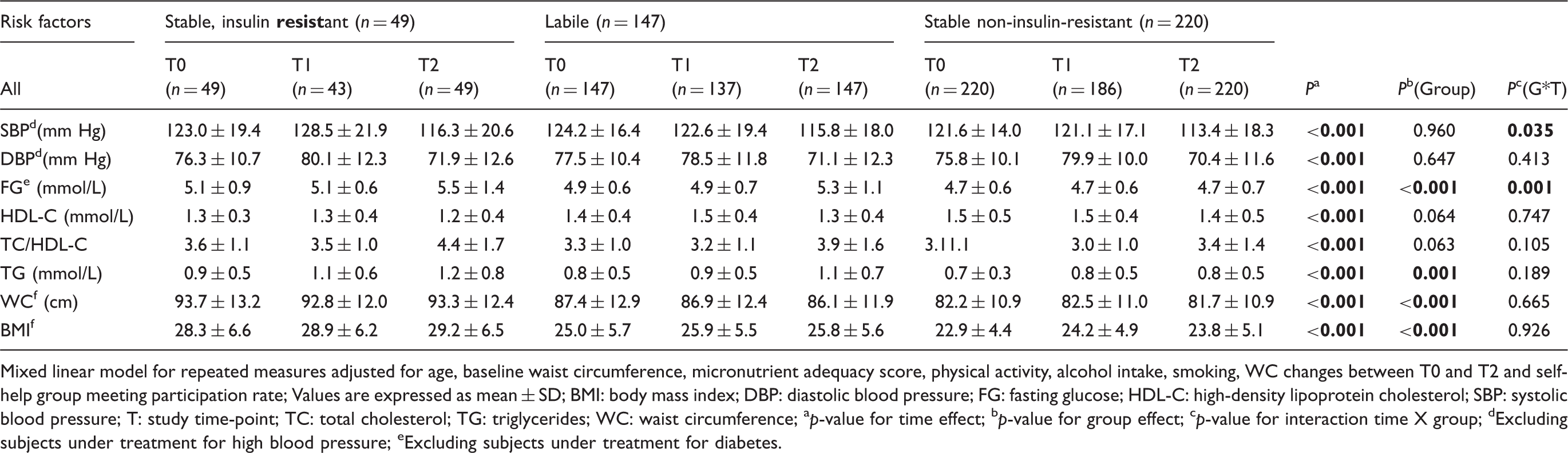
Mixed linear model for repeated measures adjusted for age, baseline waist circumference, micronutrient adequacy score, physical activity, alcohol intake, smoking, WC changes between T0 and T2 and self-help group meeting participation rate
Values are expressed as mean ± SD
BMI: body mass index; DBP: diastolic blood pressure; FG: fasting glucose; HDL-C: high-density lipoprotein cholesterol; SBP: systolic blood pressure; T: study time-point; TC: total cholesterol; TG: triglycerides; WC: waist circumference
p-value for time effect
p-value for group effect
p-value for interaction time X group
Excluding subjects under treatment for high blood pressure
Excluding subjects under treatment for diabetes.
HDL-C means tended to be lower and TC/HDL-C higher, in the IR subjects as compared to non-IR subjects. There was a significant interaction effect (group [IR, labile IR or non-IR] x time) for changes in fasting glucose. There was also a significant interaction of group (the IR status) by time for SBP, which showed a general downward trend, except between T0 and T1 in stable IR subjects. In a gender-separate analysis (data not shown), we found a significant interaction effect of group (IR status) by time, for changes in triglyceride concentrations in men (it was only a trend in women).
Discussion
To our knowledge, this is the first longitudinal cohort study on IR and other CMR factors in sub-Saharan Africa. The study confirmed that IR was more prevalent in women and was associated with a more adverse CMR profile, except for BP. IR was associated with a much higher RR of hyperglycemia, diabetes and MetS. IR tended to exacerbate low HDL-C.
In several cases, the IR status was inconsistent during follow-up. This is why a ‘labile’ IR group was formed. Only 49 subjects (11.8%) were IR at the onset of the study and remained so at the last follow-up.
Baseline IR was associated with higher CMR, as compared with non-IR status, and remained so during the follow-up period, in accordance with previous studies; 1 however, even in women without IR, the proportion of the abdominally obese was high (39.9%). This raises again the issue of the absence of specific WC cut-offs for Africans. 18
In agreement with the results of Osei et al., 19 but in contrast with others, 20 we did not find any statistically significant association between HOMA and BP, but our IR subjects had higher BP by at least 5 mm Hg, as compared to non-IR at T1 only. This explained the significant interaction effect observed. The suggested mechanism linking IR and hypertension appears to be the activation of the renin-angiotensin-aldosterone system, which is mediated by adipocyte hormones. 21 Because Blacks have less visceral fat, 22 this relationship may be weaker than in Caucasians.
Regarding the downward trend of BP that was observed at the end of the follow-up period in our study, we believe it cannot be ascribed to the influence of subjects under treatment for hypertension, because they were excluded. Behavioural changes resulting from sensitization in self-help groups cannot be totally ruled out as a possible explanation: Individual participation rates in self-help group meetings varied from 0% to 100%. We found that sex, age and location did not influence participation; however, subjects with at least one CMR factor showed a higher participation rate in meetings (57.5%) than subjects with no CMR (44.8%), p = 0.003. When controlling for participation in group meetings, the results were unchanged, but this does not exclude that our subjects adopted a more preventive diet and lifestyle, which cannot be verified. In a recent review, Reaven et al. 21 reported that approximately 50% of individuals with essential hypertension are not insulin resistant. In our study, only 26.7% of subjects with high BP were insulin-resistant at baseline (prior to self-help group formation). The weak association of HOMA with BP also suggests that hypertension is a multifactorial and complex problem.
Our study confirms the well-established association of IR with high fasting glucose and abdominal obesity. 23 The increased triglyceride concentration seen in men was associated with the labile IR status (according to the mixed model utilized, but not the regression model), which is in agreement with McLaughlin et al., 24 but at variance with others. 25 Although several studies have reported low or normal triglyceride concentrations among Blacks, 26 some studies have observed an association between high triglycerides and IR: 27 For example, in non-diabetic, overweight East-Africans, high triglyceride concentrations predict IR, 28 although the association is weaker than in non-African individuals. In any case, high triglyceride concentrations are not common in Africans, which our study confirmed. In contrast, low HDL-C is a frequent MetS feature in Africans. 29 We found that low HDL-C was highly prevalent in Southern Benin and it increased over time, in women. This may be associated with the high prevalence of abdominal obesity in women in Benin. The likelihood of onset of low HDL tended to be higher in the labile IR subject group compared to normal subjects, particularly in women. An involvement of higher plasma lipoprotein lipase (LPL) activity in blacks is proposed to explain the cardioprotective plasma lipoprotein profile that is found in blacks, as compared to whites, 22 but the ongoing nutritional transition characterized by changes in diets and lifestyles may be contributing to the higher prevalence of low HDL that we observed in the study population.
IR based on the hyperinsulinemic-euglycemic clamp method, is found to be highly prevalent in African-Americans. 30 Because we chose to use HOMA, and not the gold-standard clamp method, we cannot claim that IR is highly prevalent in our study population; however, like in Afro-Americans, 11 we found that in our study population, there was a weak relationship between IR and high blood pressure, high triglycerides or low HDL-C; although IR is considered as a central element of MetS. 31 These ethnic specificities may largely explain why Blacks have a lower-than-expected prevalence of MetS. 26 Ethnicity-specific formulation of criteria for MetS may lead to better identification of Afro-Americans or sub-Saharan Africans who are at high risk of diabetes and cardiovascular disease.
There are limitations in this study. Subjects who were available for the last follow-up (n = 416) were somewhat different from those missing this last follow-up (n = 125), as we had a significantly higher proportion of missing subjects in the larger city, and significantly higher BMI and WC in the subjects we retained. However, there were no differences in socio-economic nor behavioural parameters. Furthermore, the study was only conducted in Southern Benin, a caveat to extrapolation of our findings to the other population groups in Benin. The small number of subjects who were IR at baseline and remained so during follow-up, plus a lack of data on inflammatory status, were also a limitation. Finally, as already stated, we used HOMA and not the gold standard technique for the measurement of IR.
Conclusion
This study showed that over a 4-year follow-up period, IR exacerbated hyperglycemia in men and women, as well as abdominal obesity in women. We found that IR was not associated with a deterioration of BP. The association of IR with a more adverse evolution of dyslipidemia was inconsistent, although low HDL-C tended to become aggravated by IR. Further research on the link between IR and dyslipidemia, particularly low HDL-C, is needed in sub-Saharan Africa.
Footnotes
Acknowledgements
We thank A Sanni from the Applied Biomedical Sciences Institute for performing laboratory analyses, our field workers and the participants in our study.
Funding
This work was supported by the Canadian International Development Agency (grant number SO64359).
Conflict of interest
The authors declare no competing interests.