
Abstract
Aim:
To examine whether use of a standardized cardiovascular disease (CVD) risk assessment recommended by national guidelines is associated with appropriate initiation and maintenance of medication in a large primary care cohort.
Methods and design:
A total of 90,631 people aged 30−80 years were followed for up to 3 years after a formal CVD risk assessment was undertaken between January 2006 and October 2009, during routine primary care visits in New Zealand. Patients either had prior CVD or had their CVD risk estimated using a modified Framingham prediction equation for fatal or non-fatal CVD events. The individual risk profiles were anonymously linked to national dispensing data for blood-pressure-lowering and lipid-lowering medications in the 6-month period before and in consecutive 6-month blocks after the baseline CVD risk assessment.
Results:
At baseline, a combination of blood-pressure-lowering and lipid-lowering therapy was already being used by about two-thirds of patients with prior CVD, one-quarter with a 5-year CVD risk greater than 10% (approximately 20% 10-year risk), and one-tenth with CVD risk below this level. Among these previously treated patients, dispensing rates for blood-pressure-lowering, lipid-lowering, or both medications together declined by only 4⊟16% up to 3 years after baseline assessment, irrespective of risk category. Among patients untreated at baseline, combination therapy was initiated within 6 months for 21% with prior CVD, 16% with 5-year CVD risk greater than 15% (approximately 30% 10-year risk and the national drug-treatment threshold), 10% with 5-year CVD risk between 10 and 14% (approximately 20⊟29% 10-year risk), and 3% in the lowest risk category. Across the study population, patients with prior CVD had the highest dispensing rates for each category of medication, and incrementally higher dispensing rates were noted as CVD risk group increased.
Conclusions:
In this primary care cohort, most patients already using CVD medications at the time of the baseline CVD risk assessment maintained treatment over a maximum of 3 years follow up, irrespective of their estimated baseline risk. Among patients untreated at baseline, subsequent dispensing rates were strongly related to estimated CVD risk group. Around 15⊟20% of untreated patients meeting national drug-treatment criteria commenced combination pharmacotherapy within 6 months of CVD risk assessment.
Keywords
Introduction
New Zealand cardiovascular disease (CVD) risk management guidelines advocate systematic CVD risk assessment in middle-aged and older adults. Long-term treatment with aspirin, blood-pressure-lowering, and lipid-lowering medications is recommended for people with CVD or those without CVD who have a predicted 5-year risk of 15% or greater (approximately 30% or greater 10-year CVD risk). 1
Few studies have examined initiation of pharmacotherapy for CVD following cardiovascular risk assessment. Once pharmacotherapy for CVD is commenced, however, a common theme in the international literature is that maintenance of treatment declines markedly in the medium to long term.2–10 Nevertheless, some studies have noted more favourable rates of CVD medication maintenance. The Heart Protection Study randomized 20,536 UK adults aged 40–80 years with coronary heart disease, other occlusive arterial disease or diabetes to receive either 40 mg simvastatin or placebo daily. In the treatment arm, 80% or more of the scheduled doses were taken by 89% of participants at the end of the first year of follow up, and by 82% after 5 years. 11
We are able to link individual patient data from a comprehensive national medication dispensing database to a large cohort of patients who have had a computerized CVD risk assessment undertaken during routine visits to their general practitioners. This cohort currently includes about one-third of adults eligible for a CVD risk assessment in the Auckland and Northland regions of New Zealand, where about one-third of all New Zealanders live. This study examines initiation and maintenance of cardiovascular medication dispensing by CVD risk group within this large primary care cohort.
Methods and design
Study population
Study participants are automatically recruited when primary care practitioners use PREDICT, a web-based clinical decision support programme for assessing and managing a patient’s CVD risk that is integrated with electronic patient record systems. When a risk assessment is performed with PREDICT, standardized cardiovascular risk factor data for each patient are stored both in the patient record and on a remote server using a one-way encrypted personal identifier, generating a large and evolving patient cohort. PREDICT has been widely used in the Auckland and Northland regions of New Zealand since 2002, mainly opportunistically and principally in primary care. 12 Auckland is New Zealand’s most populous region with a population of about 1.5 million people, more than 90% of whom live in urban areas. By contrast, more than 50% of the 150,000 people living in Northland reside in rural areas. 13
Primary care patients were included in these analyses if they were first risk assessed using PREDICT between 1 January 2006 and 15 October 2009 and were aged 30–80 years. Patients with and without a history of CVD were included. Prior CVD was defined as a history of angina or myocardial infarction, stroke, transient ischaemic attack, peripheral vascular disease, percutaneous coronary intervention, or coronary artery bypass graft reported by the primary care practitioner at the time of the baseline risk assessment. No data regarding diagnostic investigations for ischaemia were available. People without prior CVD were stratified according to whether their 5-year New Zealand-adjusted Framingham CVD risk score 1 was 15% or greater (approximately 30% or greater 10-year Framingham CVD risk), 10 to 14% (approximately 20–29% 10-year risk), or less than 10% (approximately less than 20% 10-year risk).
Patients were excluded if the primary care practitioner did not report a history of CVD on the PREDICT template, but either a publicly funded CVD-related hospital admission had occurred between 7 January 1993 and the first PREDICT assessment, or anti-anginal medications were dispensed on at least one occasion between 15 February 2002 and the baseline risk assessment. Anti-anginal medications consisted of nitrates and perhexiline (note: molsidome is not currently available in New Zealand).
Linkage to medication dispensing data
Over 95% of New Zealand citizens have a National Health Index (NHI) number that uniquely identifies them in multiple New Zealand health system databases. 14 Cardiovascular medications dispensed to each patient in the cohort were identified by anonymously linking the PREDICT database to the Pharmaceutical Collection (PHARMS), using encrypted NHI numbers. PHARMS is a data warehouse that is jointly administered by the New Zealand Ministry of Health and the Pharmaceutical Management Agency of New Zealand, and collects data on government-subsidized medications dispensed by community pharmacies nationwide. 15 In 2006, 92% of dispensing episodes were reliably identifiable by NHI numbers, and by 2009 this had increased to 96%. (S Ross, personal communication, 2009). All medications relevant to these analyses are government subsidized.
Outcomes
The main outcome of interest was dispensing of blood-pressure-lowering medications and lipid-lowering medications at least once in each 6-month period of follow up from the date of first PREDICT assessment. Aspirin was not examined as it is available in New Zealand without prescription, and dispensing was not comprehensively captured in the PHARMS database during this period.
All classes of blood-pressure-lowering medications and lipid-lowering medications were considered (listed in supplementary material Appendix 1). Three categories of therapy were used: blood-pressure-lowering medications alone, lipid-lowering medications alone, and both classes of medications together.
Data collection was undertaken in 6-month periods because, although cardiovascular medications are usually prescribed every 3 months, people sometimes fill their prescriptions outside this time period. In each of the 6-month intervals, the proportion of people who were dispensed medications was calculated. The denominator for each 6-month interval was those participants with complete follow up for that period. Patients who died or had a CVD event during follow up were excluded from the denominator for the 6-month intervals of follow up after death or CVD event. Over the study period (1 January 2006 to 15 October 2009), the number of people in the cohort increased markedly, and the reported proportions of the cohort dispensed medications are cross-sectional estimates of dispensing for each 6-month interval up to 36 months following the baseline risk assessment.
Statistical analysis
Data was analysed using STATA 10.0 statistical software. Simple descriptive statistics and line graphs are presented, with results stratified according to a history of CVD at baseline risk assessment or by the calculated CVD risk score.
Ethical approval
The cohort study and research process was approved by the Northern Region Ethics Committee Y in 2003 (AKY/03/12/314) with subsequent annual approval by the National Multi Region Ethics Committee since 2007 (MEC/07/19/EXP).
Results
Baseline characteristics of the PREDICT cohort
Patients included within the PREDICT cohort were aged between 30–80 years and were risk assessed for the first time between 1 January 2006 and 15 October 2009 inclusive
Patients were categorized into ethnic groups based on ethnicities recorded in either the National Health Index or the PREDICT database. If more than one ethnic group was recorded, ethnicity was prioritized in the following order: Maori, Pacific Island, Indian, and Others
NZDep01 was used to approximate socioeconomic status. NZDep01 is a census-based measure of deprivation in small areas, based on nine variables from the 2001 Census
In people without prior CVD; 10-year Framingham CVD risk scores are approximately double the 5-year New Zealand-adjusted Framingham CVD risk scores
CVD, cardiovascular disease.
Figure 1 presents cross-sectional estimates of the proportion of people dispensed CVD medications during 6-month intervals following first PREDICT assessment. Further detail is presented in supplementary material Appendix 2 Table a. Dispensing rates were higher for blood-pressure-lowering medications than for lipid-lowering medications. Patients with prior CVD had the highest dispensing rates for each category of medication. Among people without CVD, incrementally higher dispensing rates were noted as CVD risk group increased. For example, in the 6 months following the baseline risk assessment, the proportion of people dispensed both blood-pressure-lowering and lipid-lowering medications was 70% of patients with prior CVD, 36% with 5-year CVD risk of 15% or greater, 29% in the 10–14% risk group, and 11% of people in the lowest risk category. Across all 6-month periods of follow up, the proportion of the study population fulfilling national criteria for combination therapy who received both blood-pressure-lowering and lipid-lowering medication ranged from 60–70% for patients with prior CVD, and 36–41% with an estimated 5-year CVD risk of 15% or greater.
Proportion of people followed up during specified 6-month periods after baseline CVD risk assessment who were dispensed CVD medications (cross-sectional analyses at 6-month intervals): (a) blood-pressure-lowering medication; (b) lipid-lowering medication; (c) both blood-pressure-lowering and lipid-lowering medications.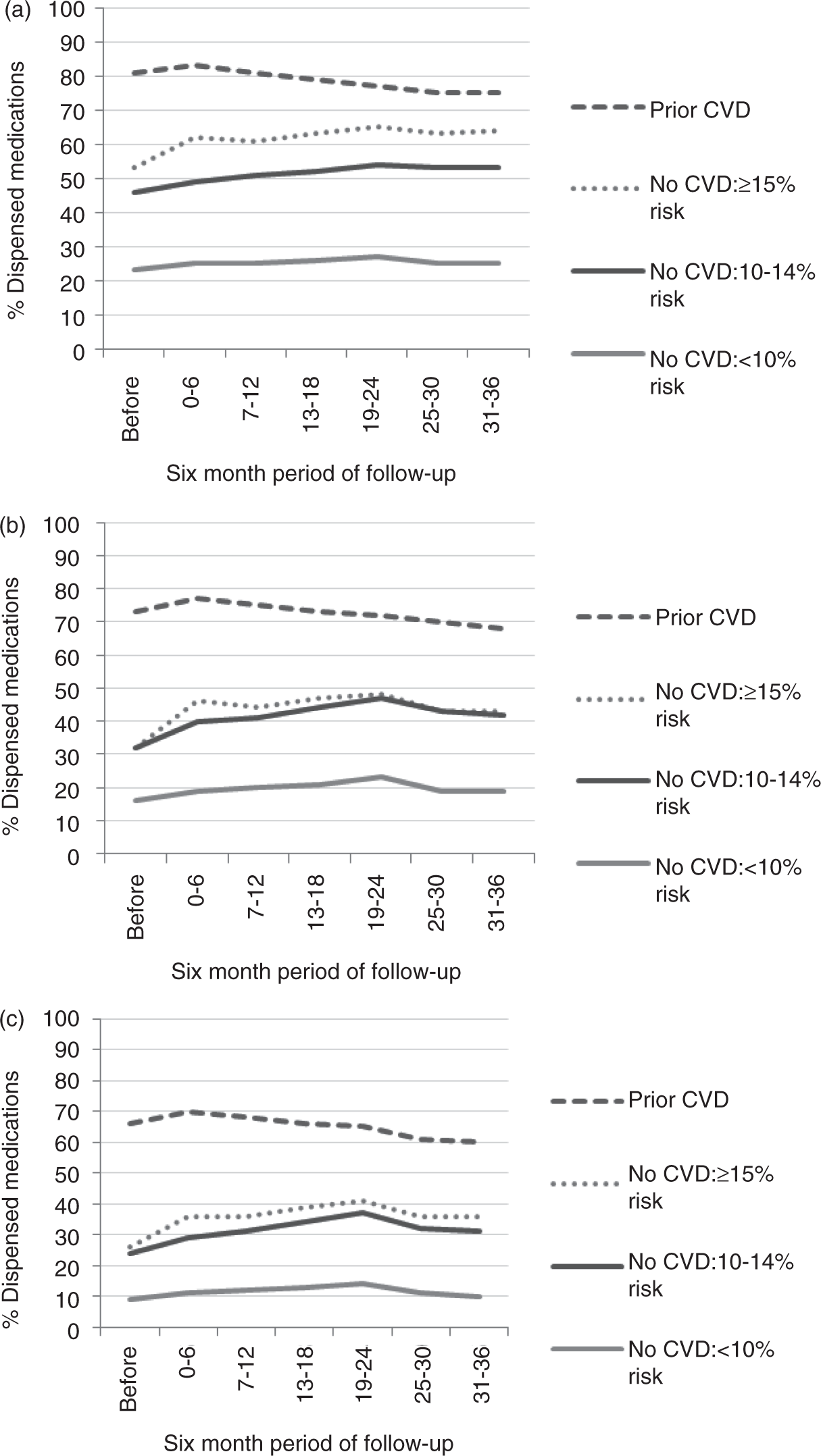
Figure 2 shows that, for people who were already being dispensed medications in the 6 months before the baseline assessment, dispensing rates declined minimally (4–16%) across the 6-month intervals of follow up irrespective of the category of medication, history of CVD, or CVD risk group. Further detail is presented in supplementary material Appendix 2 Table b.
Proportion of people dispensed medications prior to baseline CVD risk assessment and followed up during specified 6-month periods who continued to be dispensed CVD medications (cross-sectional analyses at 6-month intervals): (a) blood-pressure-lowering medication; (b) lipid-lowering medication; (c) both blood-pressure-lowering and lipid-lowering medications.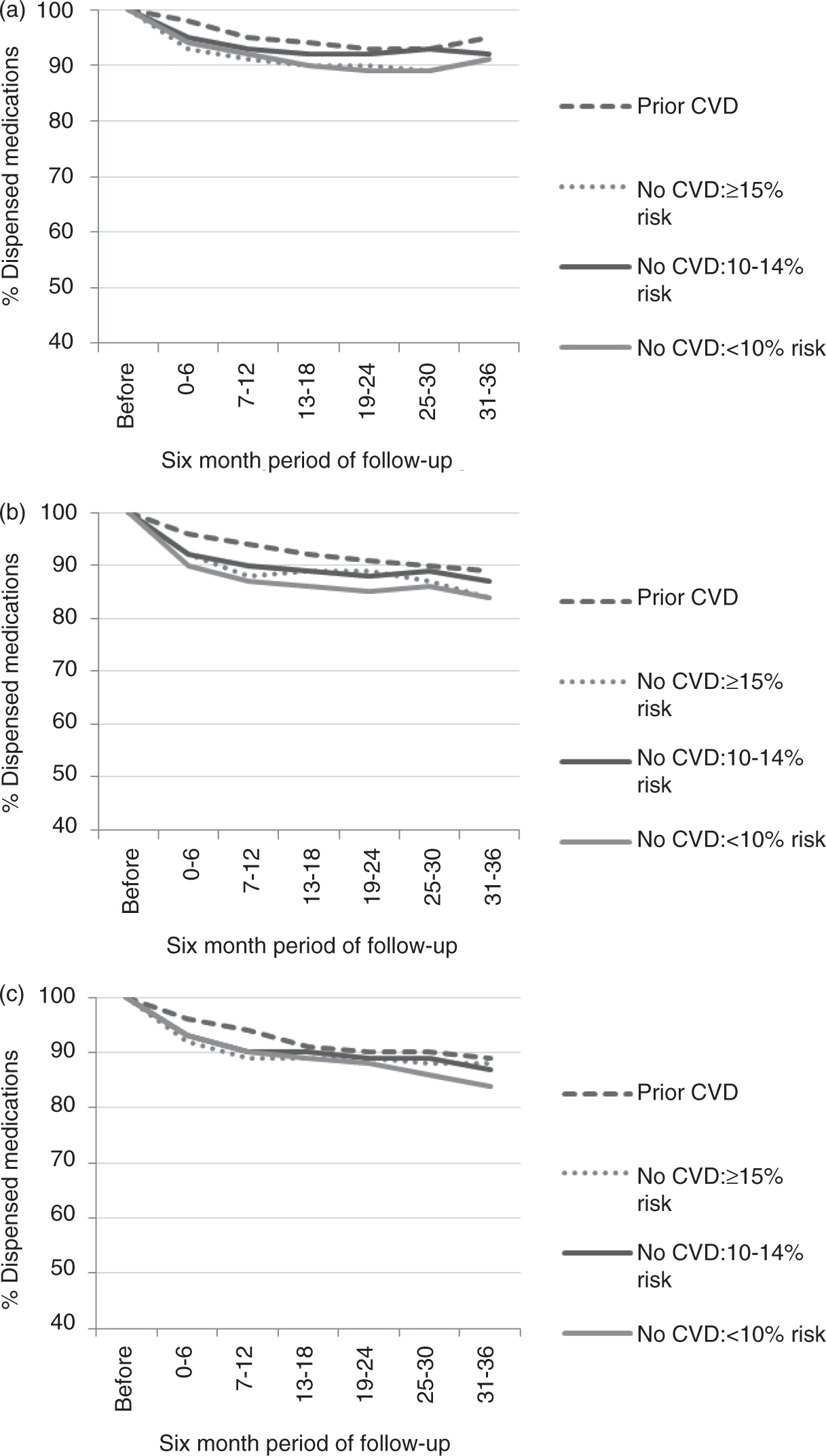
Figure 3 presents dispensing rates among people who were not on CVD medications during the 6 months before the baseline assessment. Across all three medication categories, dispensing rose most sharply in the 6-month interval after baseline and commencement of medications differed by level of CVD risk. Among high-risk patients, who met national criteria for treatment with both blood-pressure-lowering and lipid-lowering medications, combination therapy was initiated within 6 months of risk assessment by 21% of those with prior CVD and 16% of patients with a 5-year CVD risk of 15% or greater. However, blood-pressure-lowering medications, lipid-lowering medications, and both medications together were also commenced by 12%, 15%, and 9%, respectively, of people with a 5-year CVD risk of 10–14%, and by 4%, 6%, and 3%, respectively, of patients in the lowest risk category. Further detail is presented in supplementary material Appendix 2 Table c.
Proportion of people not dispensed medications prior to baseline CVD risk assessment and followed up during specified 6-month periods who were dispensed CVD medications (cross-sectional analyses at 6-month intervals): (a) blood-pressure-lowering medication; (b) lipid-lowering medication; (c) both blood-pressure-lowering and lipid-lowering medications.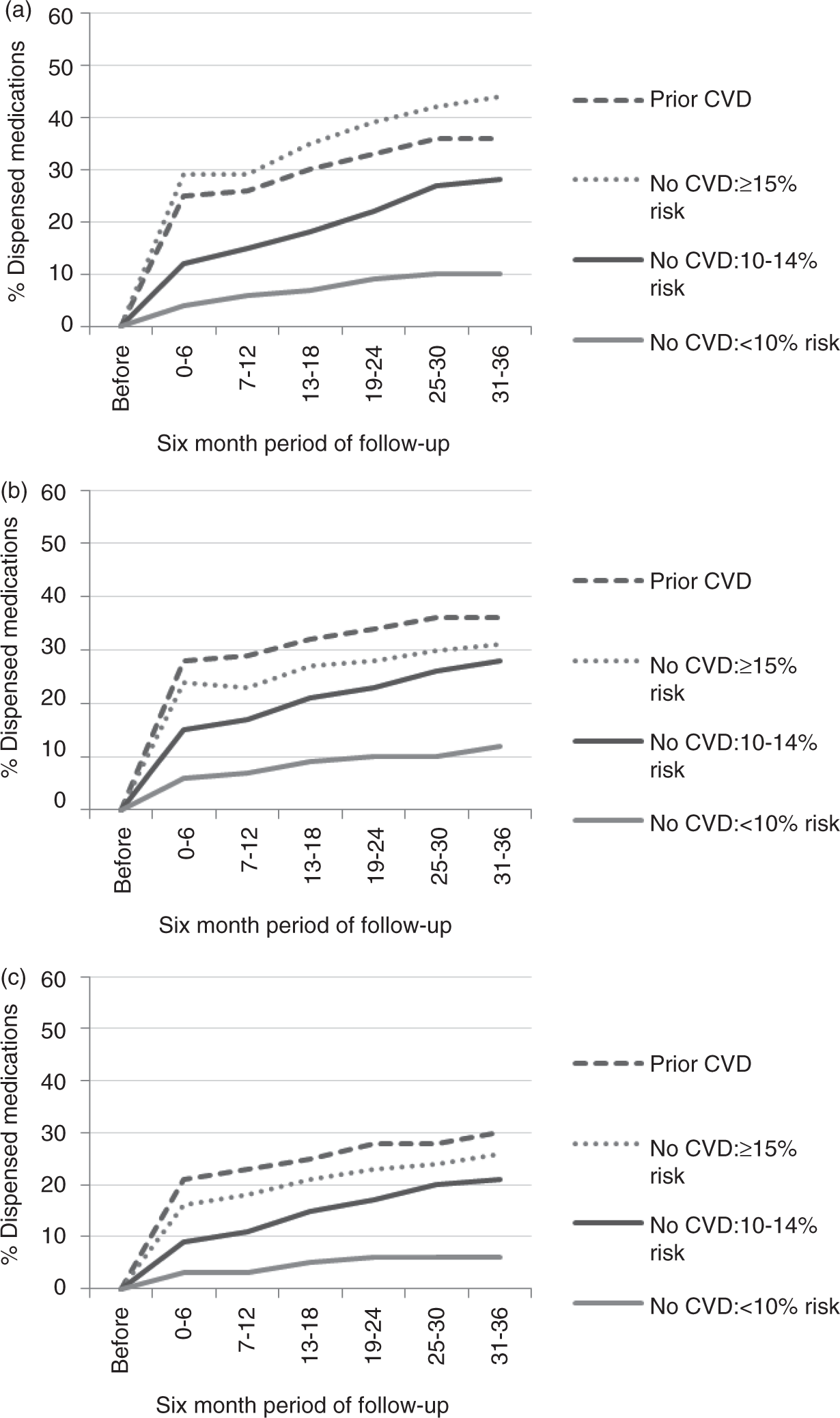
Discussion
In this primary care cohort, we examined dispensing rates of blood-pressure-lowering and lipid-lowering medications cross-sectionally for each 6-month period over a maximum of 3 years follow up after a baseline CVD risk assessment. The vast majority of patients on pharmacotherapy for CVD risk management at the baseline assessment maintained treatment during follow up irrespective of their estimated CVD risk. Among patients untreated during the 6 months before the baseline assessment, a substantial increase in treatment of high-risk groups was observed within 6 months of risk assessment. Overall dispensing rates of CVD medications were higher but, nevertheless, suboptimal among high-risk groups. Across all 6-month periods of follow up, the proportion of the study population fulfilling national criteria for combination therapy who received both blood-pressure-lowering and lipid-lowering medication ranged from 60–70% for patients with prior CVD, and 36–41% of people with an estimated 5-year CVD risk of 15% or greater (approximately 30% or greater 10-year risk).
This study is one of the largest single cohorts of patients prospectively assessed for risk of CVD in primary care worldwide. The demographic and drug dispensing data for the sample were generated through routine clinical interactions, which aids the generalizability of the findings to the wider primary care setting. We minimized the potential for misclassification error based on patient self-report or incomplete health provider records of pharmacotherapy by abstracting data regarding dispensed medications from a comprehensive nationwide database recording government-subsidized dispensing episodes. Preliminary analyses (Figure 4 and supplementary material Appendix 2 Table d) to determine if any bias was introduced by differing lengths of follow up do not suggest that this was a problem. When the cohort has been followed for several more years, we plan to repeat the analyses for participants with at least 3 years follow up after baseline risk assessment. We also intend to examine the proportion of follow-up time in which medications were dispensed among defined groups of individuals, including patients with CVD stratified according to the clinical significance of their diagnoses.
Proportion of people followed up during specified 6-month periods after baseline CVD risk assessment with at least two years of follow-up who were dispensed CVD medications (cross-sectional analyses at 6-month intervals): (a) blood-pressure-lowering medication; (b) lipid-lowering medication; (c) both blood-pressure-lowering and lipid-lowering medications.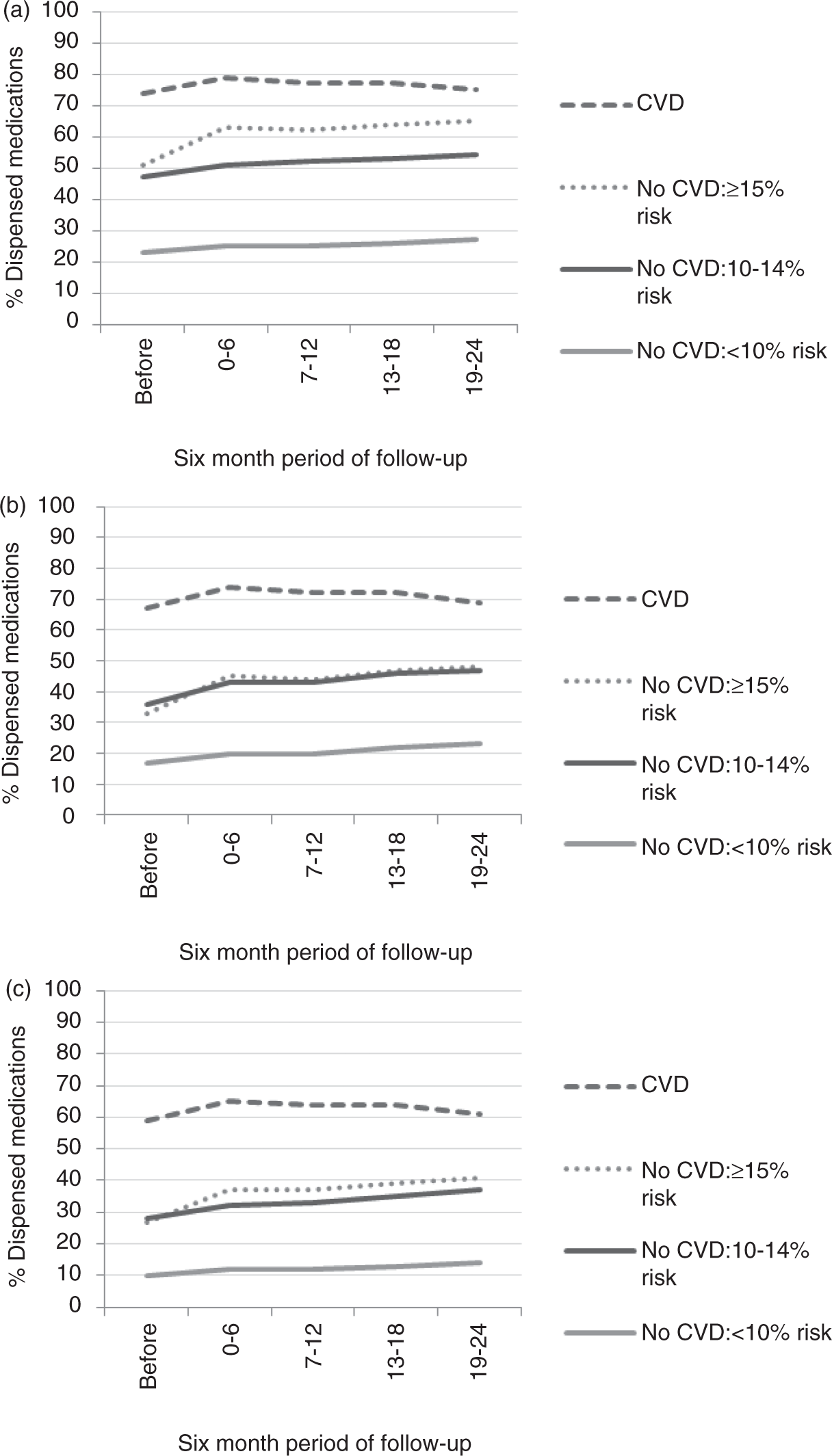
The main limitation of these analyses is the possibility of recruitment bias. Study participants potentially encompassed a better-treated patient group whose primary care was provided by the most motivated practitioners. While all general practices in the study region are provided with the PREDICT system and national performance-based funding has encouraged its use, early adopters and frequent users of PREDICT will be over-represented. Participants also had to visit a general practitioner to enter the study population, and non-regular patients are less likely to have been risk assessed with PREDICT. Our findings, therefore, probably represent the best case scenario in terms of treatment initiation and maintenance.
As expected, there were greater proportions of males, Maori and Pacific peoples, and those living in the most deprived areas within the cohort than in the total New Zealand population.17,18 This reflects the national CVD risk management guideline recommendations to prioritize the highest risk patients for CVD risk assessment. Men are screened 10 years earlier than women and Maori, Pacific, and South Asian patients are risk assessed 10 years before other ethnic groups. In addition, the disproportionate number of people at high risk of CVD events within these populations may have influenced the rates of medication dispensing noted in our study. Of these particular demographic groups, Maori and Pacific peoples and those living in deprived neighbourhoods also face the greatest barriers to access and utilization of health services, such as dispensing of pharmacotherapy which attracts a co-payment for some medications within New Zealand.
We were not able to determine the proportion of each 6-month period of follow up that medications were dispensed. Also, due to the cross-sectional nature of our analyses, the actual people dispensed medications in different 6-month intervals may have changed even if the proportion of the population dispensed medications remained identical for two given periods. As data regarding diagnostic investigations for ischaemia were unavailable, we were also unable to differentiate patients diagnosed clinically with CVD from those confirmed by tests for ischaemia. Furthermore, our study did not consider the influence of medication intolerance and side-effects on dispensing rates, and we could not determine whether dispensed medications were actually taken by patients.
Our previous research has demonstrated a major increase in appropriate risk assessment after introduction of electronic decision support. 19 These new findings suggest that a formal CVD risk assessment also has a positive influence on management: among the subgroup of participants who were untreated at the baseline risk assessment, a sizeable improvement in appropriate dispensing occurred within 6 months. As this is an observational study, with no control group of patients who received usual care, we cannot categorically link initiation of pharmacotherapy with the risk assessment process. However, the greatest increase in commencement of pharmacotherapy occurred immediately following the baseline assessment, and no changes in national treatment guidelines or availability of medications occurred during the study period.
The limited literature examining initiation of pharmacotherapy following cardiovascular risk assessment is also consistent with our findings, though publication bias is possible. Grover et al. 20 randomized 3053 Canadian patients aged 30–70 years to receive either electronic cardiovascular risk assessments every 3 months or usual care. Of the 2631 participants who completed 12 months of follow up, 31% of those risk profiled initiated blood-pressure-lowering medications compared to 24% receiving usual care (odds ratio of initiating therapy among those who were risk assessed 1.78, 95% confidence interval 1.06–3.00, after adjusting for inter-physician differences and confounders). Unlike our study, however, Grover et al. did not examine commencement of pharmacotherapy according to CVD risk.
Once treatment is initiated, the international literature does not present a consistent picture of CVD medication maintenance. A number of longitudinal studies examining dispensing patterns among patients commenced on CVD medications at a similar time noted a sharp initial decline in treatment rates followed by more gradual waning in medication dispensing,2–4,6,8 while some studies found that pharmacotherapy for CVD was maintained steadily. 11 The latter pattern was observed within our study population, where rates of medication dispensing increased across follow up intervals among patients who commenced medications following PREDICT assessment.
The patterns of pharmacotherapy for primary prevention noted in our analyses, which considered medication dispensing according to absolute CVD risk scores, could not be directly compared with the EUROASPIRE (European Action on Secondary and Primary Prevention through Intervention to Reduce Events) III study which examined treatment for individual CVD risk factors. Both our study and the EUROASPIRE surveys, however, examined drug therapy among patients with prior CVD. Three cross-sectional surveys were carried out by the European Society of Cardiology in multiple countries across Europe beginning in 1995/1996 to determine whether Joint European Guidelines on management for CVD were followed in daily clinical practice.21–24 A total of 8966 patients with coronary heart disease from 22 European countries were interviewed between 2006 and 2007 for EUROASPIRE III, an average of 1.24 years following their coronary event. 23 Pharmacotherapy for secondary prevention of CVD occurred at similar levels to those noted within our cohort; 80% of patients were taking beta-blockers, 71% used angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers (all of which were classed as blood-pressure-lowering medications in our study), while 78% were on statin therapy.
The EUROASPIRE studies also showed that use of cardioprotective medications did not translate to adequate risk factor control. Across the eight countries that participated in all three EUROASPIRE surveys, blood pressure control remained unchanged among patients with coronary heart disease, with nearly three-fifths failing to achieve the blood pressure goal (>140/90 mmHg for non-diabetics and >130/80 mmHg in patients with diabetes) in the third survey. 25 Similarly, EUROASPIRE III indicated that of the 4366 patients without a history of CVD from 66 general practices across 12 European countries, only about a quarter of people using antihypertensive medication achieved the blood pressure goal, and about 30% of patients on lipid-lowering medication had total cholesterol ≥5.0 mmol/l (or ≥4.5 mmol/l among people with diabetes). 22 We were unable to determine the adequacy of risk factor control among our cohort as we have incomplete follow-up data regarding risk factor levels.
Dispensing rates in our study were higher with increasing estimated risk of cardiovascular morbidity and mortality. In addition, the greatest increases in medication dispensing after patients were risk assessed occurred among those groups of patients with highest estimated risk. It appears that a shift to targeting treatment by predicted CVD risk, in line with guideline recommendations, is occurring among local primary care practitioners, and utilization of risk assessment programmes such as the PREDICT tool (which provides numerical, descriptive, and dynamic pictorial functions 26 to support risk communication) aids this process.
Treatment of individual risk factors rather than treatment based on the estimated CVD risk may partially account for the treatment gap observed for people with established CVD and those with a 5-year CVD risk score of 15% or greater (approximately 30% or greater 10-year risk). Despite their high CVD risk, many of these patients will have a blood pressure or lipid level in the ‘normal’ range and some clinicians may still follow the traditional approach of treating individual risk factors when they are significantly raised. Medication intolerance or other patient-related factors, such as financial constraints (particularly when patient co-payments are required) and transport difficulties,27–29 may also explain why some high-risk patients do not receive CVD medications. Separate analyses of demographic differences in dispensing patterns within the PREDICT cohort during follow up (not shown) indicate that the treatment gap does not differ across gender, ethnicity, or socioeconomic status, but under-utilization of pharmacotherapy for CVD is a particular issue for younger people.
In conclusion, these findings are based on a patient population who were opportunistically risk-assessed in routine primary care practice and included approximately one-third of the population eligible for a CVD risk assessment in the Auckland and Northland regions of New Zealand. About 85–95% of people dispensed cardiovascular medications before the baseline risk assessment maintained treatment for up to 3 years, indicating that it is possible to maintain high levels of treatment with blood-pressure-lowering and lipid-lowering medications. Among people who were not dispensed CVD medications before baseline, a substantial and rapid change in treatment occurred following quantitative CVD risk assessment using a standardized web-based decision support system. Both initiation and maintenance of treatment were greatest among those groups of patients at highest estimated CVD risk, who have the most to gain. However, there is still a substantial treatment gap, with only 60–70% for patients with prior CVD and 35–40% with an estimated 5-year CVD risk of 15% or greater receiving combination pharmacotherapy as recommended by national guidelines for high-risk groups.
Footnotes
Acknowledgements
The authors would like Dr Scott Metcalfe (Pharmaceutical Management Agency of New Zealand) for reviewing the draft manuscript.
The authors would also like to thank members of the PREDICT Maori Advisory Group and the PREDICT Pacific Advisory Group, as well as affiliated general practitioners, practice nurses and patients belonging to the following primary health organizations (PHOs): ProCare Network North, ProCare Network Auckland, ProCare Network Manukau, Auckland PHO Ltd, Tamaki Healthcare, HealthWest, East Health Services, TaPasefika, Te Kupenga o Hoturoa, Total Healthcare Otara, Te Tai Tokerau, Manaia, Kaipara Care, Tihewa Mauriora, and Whangaroa PHOs.
PREDICT was developed by a collaboration of clinical epidemiologists at the University of Auckland, IT specialists at Enigma Publishing (a private provider of online health knowledge systems), primary health care organizations, non-governmental organizations (New Zealand Guidelines Group, National Heart Foundation, Diabetes New Zealand, Diabetes Auckland), several district health boards, and the Ministry of Health. The PREDICT software platform is owned by Enigma Publishing (PREDICT is a trademark of Enigma Publishing).
Funding
The PREDICT research project is supported by the Health Research Council (grants 03/183 and 08/121). SW and TR are recipients of Heart Foundation (New Zealand) Fellowships. CG is the recipient of a New Zealand Health Research Council/New Zealand Ministry of Health Pacific Research Fellowship. ST is the recipient of a New Zealand Health Research Council Clinical Training Fellowship.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.