
Abstract
Background
Type D personality may be a risk factor for poor outcome in patients with cardiovascular disease. The biological mechanisms underlying this association are poorly understood. The objective of the study was to test the hypotheses that Type D personality is associated with biological markers for sympathetic dysregulation.
Design
Cross-sectional community-based study.
Methods
Type D personality was evaluated by DS-14 in 450 persons (46% men), aged between 30 and 65 years. From a Holter-recording, (mean length 18.3 hours), long-term heart rate, ventricular arrhythmias, and heart rate variability (HRV) were registered as markers of sympathetic dysregulation. Traditional cardiovascular risk factors, apnoea–hypopnoea index, medication, and anxiety symptoms were adjusted for.
Results
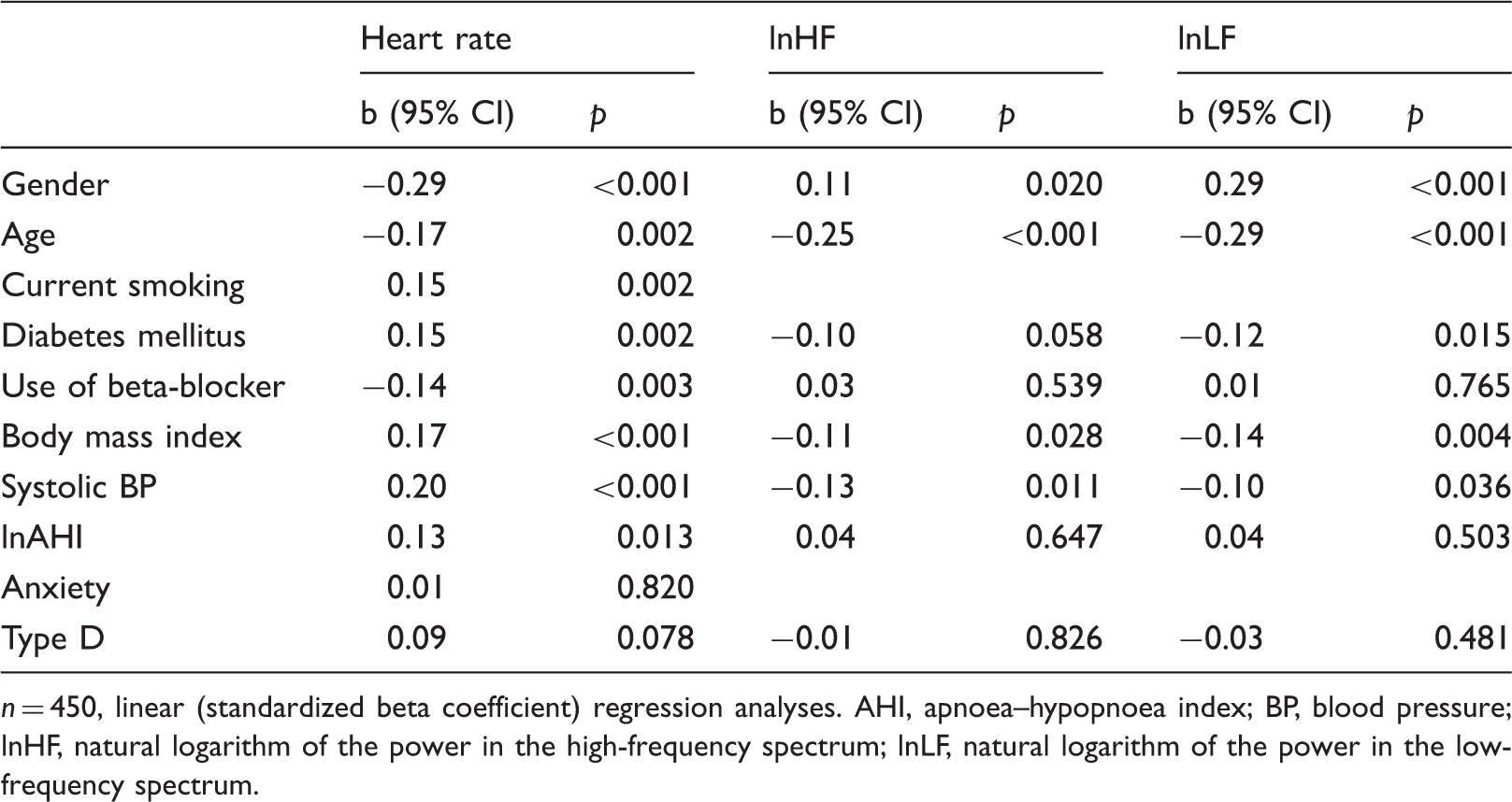
Type D persons had higher long-term averaged heart rate (74 vs. 71 beats/min, p = 0.003), but this difference was attenuated and not significant in the multivariate model (p = 0.078)). There was an increased prevalence of complex ventricular ectopy (bigeminy, trigeminy, or non-sustained ventricular tachycardia; 14 vs. 6%, p = 0.005 in multivariate model). HRV indices did not differ significantly between those with or without Type D personality. Anxiety symptoms did not confound these associations.
Conclusions
Type D personality is independently associated with a higher likelihood of ventricular arrhythmias, which may be implicated in the increased cardiovascular risk observed in persons with Type D personality.
Introduction
Type D personality is defined by having a stable trait of both negative affectivity and social inhibition 1 and is a common psychological feature with an estimated prevalence ranging from 21–32% among population-based samples in Western Europe.2–5 Current documentation suggests that this combination of personality traits may be an independent risk factor for recurrent cardiovascular events and indicative of poor somatic and psychological health among patients with established coronary heart disease (CHD).6–8 However, the mechanisms connecting Type D personality and poor cardiovascular outcome are yet uncertain. 8
Systemic inflammation, dysfunction in the hypothalamo–pituitary–adrenal (HPA) axis, and altered autonomic regulation are mechanisms hypothesized to be associated with Type D personality in patients with established CHD. 8 Alterations in catecholamine levels or sympathetic activity may be manifested as ventricular arrhythmias. 9 Furthermore, asymptomatic ventricular arrhythmias and faster resting heart rate may also have clinical significance, as it is associated with increased mortality and a heightened incidence of CHD in community-based samples.10,11
Previous studies investigating indices of dysfunctions in HPA axis and autonomic regulation in Type D persons have reported increased cortisol awakening response and reduced heart rate recovery.12,13 Also, presence of Type D personality has been associated with life-threatening arrhythmias among patients with implantable cardioverter-defibrillators. 14 In CHD-free populations, increased reactivity to stress and altered heart rate variability (HRV) have been reported in Type D persons.15–17 Our group has previously noted an increased resting heart rate in Type D persons. 18
However, to our knowledge, no study has previously examined the association between Type D personality and long-term averaged heart rate or the rates of ventricular arrhythmias in community-residing persons with Type D personality.
Critic has been levelled against the concept of Type D personality as a risk factor beyond other episodic psychological risk factors such as depression and anxiety. 19 Denollet et al. advocated viewing psychosocial factors in relation to each other when investigating their potential role for somatic health. 20 In another cohort of patients with implantable cardioverter-defibrillators, only Type D patients with concurrent anxiety had increased incidence of severe arrhythmias. 21
Thus, in this community-based study we tested the hypotheses that Type D personality is associated with faster long-term average heart rate, increased prevalence of ventricular arrhythmias, and impaired HRV, indicative of increased sympathico-vagal balance, in persons without established CHD. Furthermore, we explored the influence of concurrent anxiety on these associations.
Methods
Design and participants
The Akershus Sleep Apnea Project is a cross-sectional study in the South-East of Norway. Among 29,258 persons aged 30–65 years randomly drawn from the Norwegian Population Register and receiving the study invitation, 16,302 (55.7%) were willing to participate. Participants responded to a questionnaire designed to evaluate risk for obstructive sleep apnea, the Berlin Questionnaire. 22 A second random selection consisted of 1350 responders who were contacted and invited to the clinical phase of the study. The selection was stratified to meet pre-defined criteria of equal distributions of gender and 5-year age cohorts, as well as a two-thirds proportion of persons at high risk for obstructive sleep apnoea. Of the total contacted, 202 did not reply, 585 declined participation, and 28 were excluded, thus a total of 535 (46.7% of contacted) were examined between 2005 and 2007. More details of the recruitment process have been published previously.18,23
Data collection
All data were collected during an overnight stay at Akershus University Hospital, Stensby.
Type D personality
The presence of Type D personality was evaluated by the 14-item self-report questionnaire DS-14. 3 There are two subscales, each consisting of seven items scaled 0–3, denoting social inhibition and negative affectivity respectively. A total score of ≥10 on each subscale is regarded positive, if both subscales are positive the persons is classified as having Type D personality. The Norwegian translation of DS-14 has been validated in another community-based study. 24
Cardiac arrhythmias and heart rate variability
A 5-channel Holter recording (MedilogAR12, Oxford Instruments Medical, Surrey, UK) was performed during the overnight stay, with a recording length of (mean ± SD) 18.3 ± 2.1 hours. The digital recordings were interpreted by an automatic engine (Medilog Darwin; ScanMed Medical, Gloucestershire, UK) and manually reviewed by two researchers blinded to other participant data. A third reviewer was consulted for discrepant interpretations (<5% of recordings). Mean heart rate was calculated based on the whole recording. A ventricular complex was defined premature (PVC) when the RR-interval was >30% shorter than the average of the three previous RR-intervals. Bigeminies and trigeminies were defined as ≥3 V-N or V-N-N couples, respectively. Ventricular tachycardia was defined as three or more consecutive ventricular beats >110 beats/min, non-sustained if shorter than 30 seconds. All arrhythmias were coded as dichotomous outcomes (present or absent) according to previously used cut offs. 11 The RR-interval was linearly detrended and a Fast Fourier Transformation was used for the frequency-domain analyses of HRV (natural logarithm of the total power in the high- and low-frequency spectra (lnHF and lnLF, respectively)).
Clinical and demographical data
Clinical and demographic characteristics registered in the study include history of CHD (self-reported myocardial infarction, percutaneous coronary intervention, or coronary artery bypass grafting), diabetes mellitus, current smoking, arterial blood pressure, body mass index, blood lipid levels, and apnoea–hypopnoea index as measured by polysomnography. 25 The mean sleep duration registered in the polysomnography was 6.9 ± 1.4 hours. Anxiety symptoms were semi-quantified by seven items (scored 0–3) on the self-report questionnaire Hospital Anxiety and Depression Scale (HADS). 26 The sum-score of the seven items was dichotomized, where ≥8 was considered likely to denote a person with clinical relevant anxiety symptoms. 27
Statistical analysis
For the purpose of this study, 54 participants with established CHD were excluded. Furthermore, persons without complete DS-14 (n = 10), missing Holter-recording (n = 7), short Holter recording ( < 10 hours, n = 5), or a high level of artifacts (>15%, n = 9) were excluded from the analyses, resulting in a study sample of 450 persons. The 31 persons excluded due to missing data did not deviate from the included persons regarding clinical and demographic data.
Continuous data were assessed for normality by histograms and normal Q-Q plots. Parameters without normal distribution were logarithmically transformed, and re-checked for normality. Differences between groups were compared by the Student’s t test, Mann–Whitney U test or chi-squared test as appropriate. The associations between arrhythmias, HRV, and Type D personality were further assessed by univariate and multivariate linear and logistic regression models as appropriate. Five of more PVC per hour, complex ventricular ectopy (presence of bigeminy, trigeminy, or non-sustained ventricular tachycardia), average heart rate, and lnHF and lnLF were dependent variables. Covariates included age, gender, current smoking, diabetes mellitus, systolic blood pressure, body mass index, apnoea–hypopnoea index, and HADS anxiety. These were tested in univariate models and added to the multivariate models if p < 0.20. Finally, to evaluate the effect of any cluster of psychological distress, the product of Type D x dichotomized HADS anxiety was added in a second step to all multivariate models. The interaction terms were retained in the models if statistical significant. Analyses were performed with SPSS for Windows version 17.0 (SPSS, Chicago, IL, USA), and the significance level was set to p < 0.05.
Results
Comparisons of baseline parameters, average heart rate, and heart rate variability between Type D and non-Type D persons
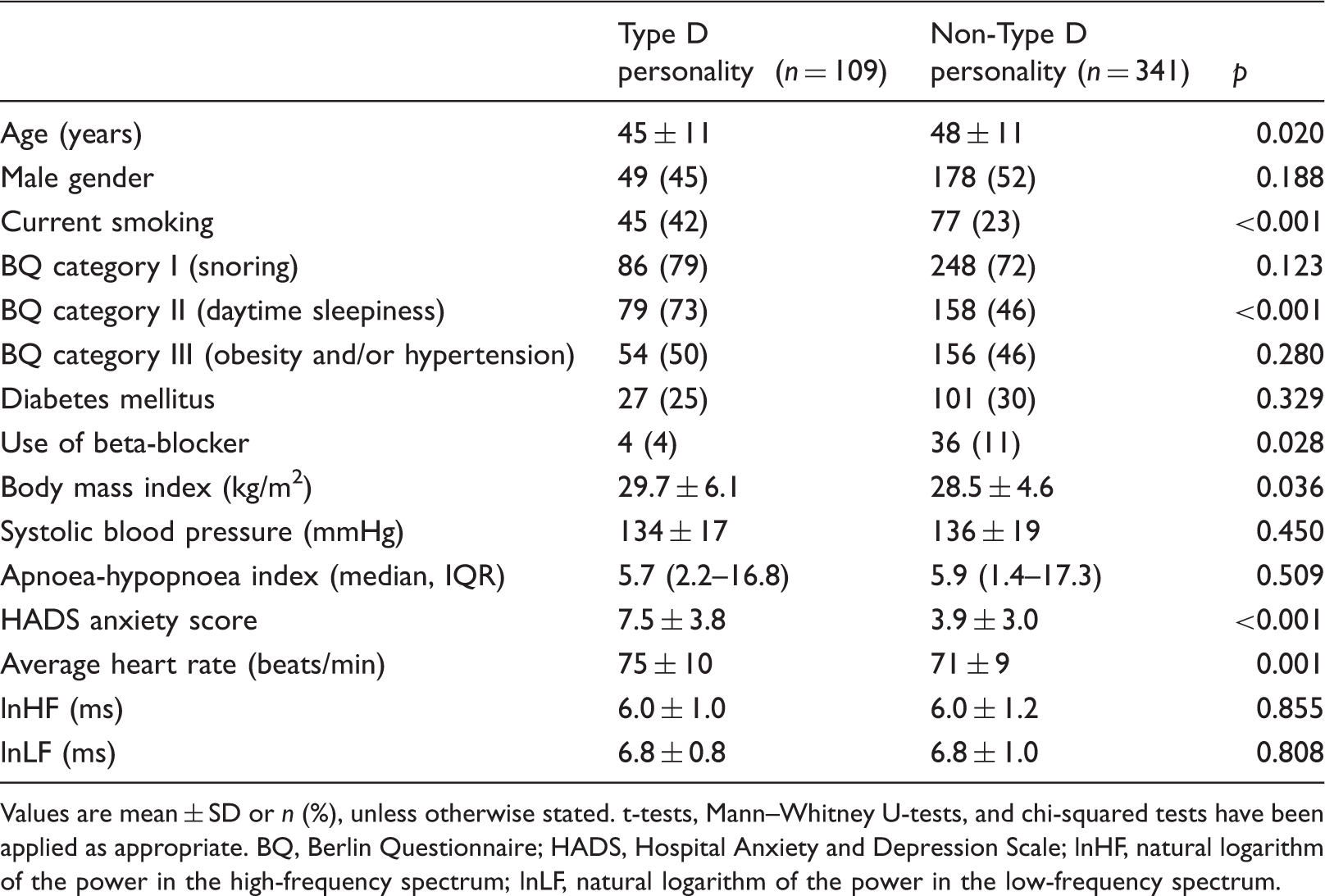
Values are mean ± SD or n (%), unless otherwise stated. t-tests, Mann–Whitney U-tests, and chi-squared tests have been applied as appropriate. BQ, Berlin Questionnaire; HADS, Hospital Anxiety and Depression Scale; lnHF, natural logarithm of the power in the high-frequency spectrum; lnLF, natural logarithm of the power in the low-frequency spectrum.
Long-term heart rate and ventricular arrhythmias
Univariate associations between demographic, clinical, and psychological variables and ventricular arrhythmias
n = 450, logistic regression analyses. AHI, apnoea–hypopnoea index; BP, blood pressure; PVC, premature ventricular complex.
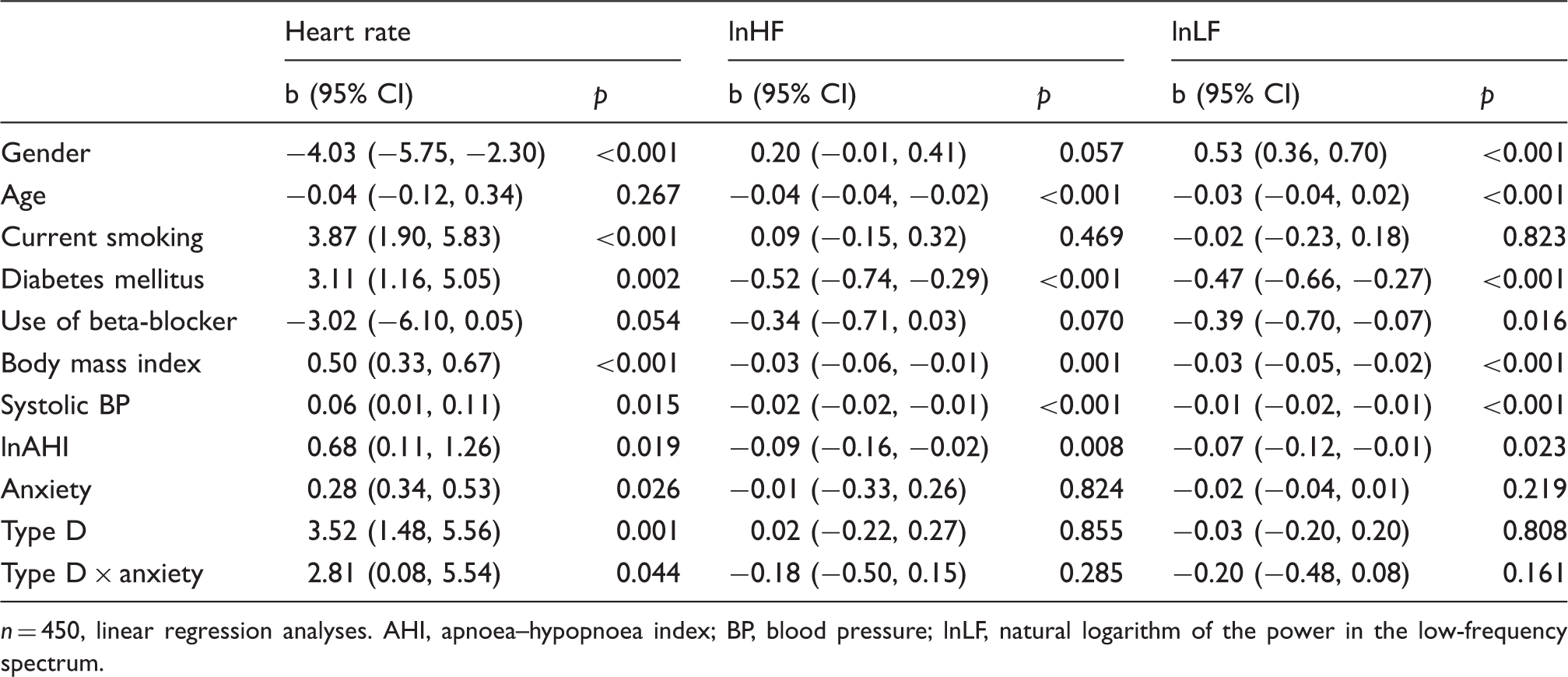
Univariate associations between demographic, clinical, and psychological variables and long-term average heart rate and heart rate variability
n = 450, linear regression analyses. AHI, apnoea–hypopnoea index; BP, blood pressure; lnLF, natural logarithm of the power in the low-frequency spectrum.
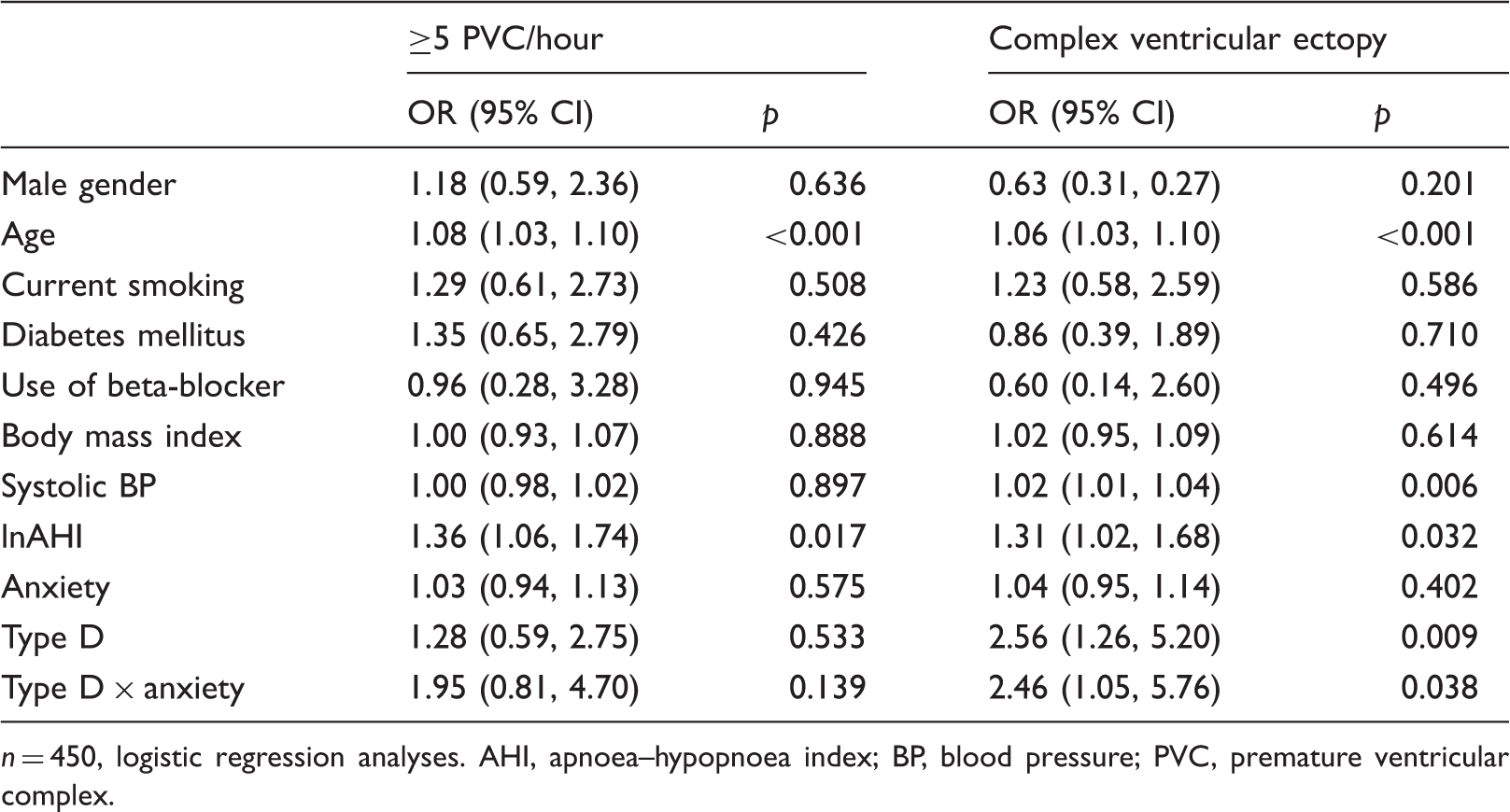
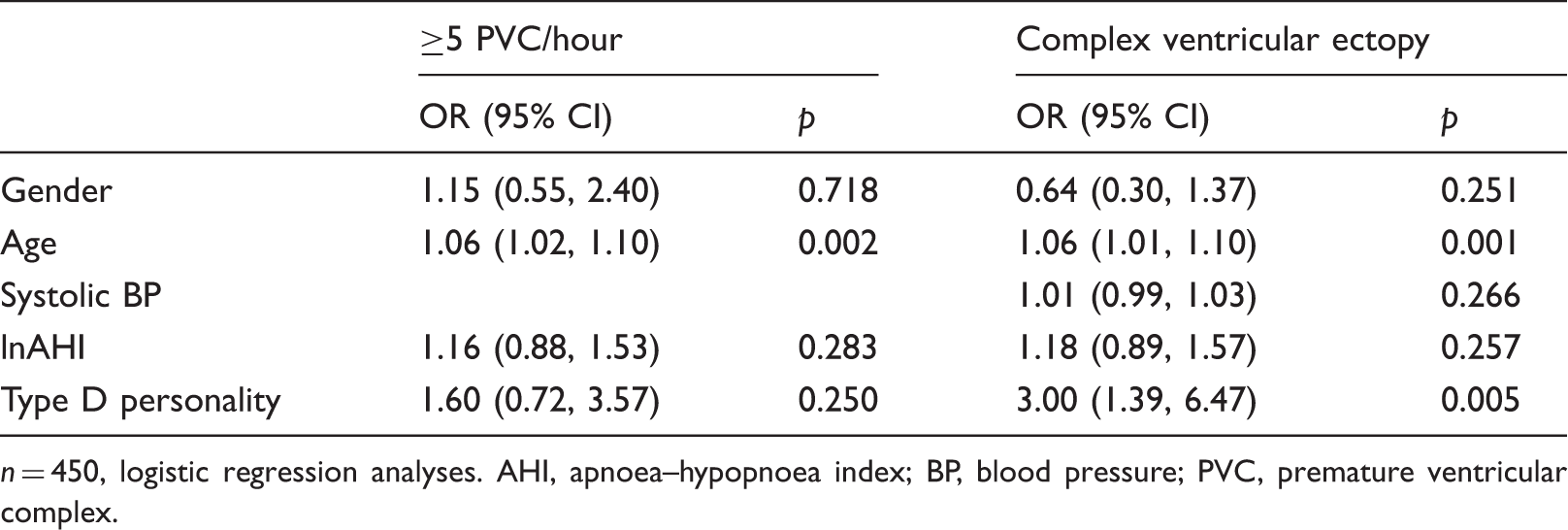
Multivariable predictors of ventricular arrhythmias
n = 450, logistic regression analyses. AHI, apnoea–hypopnoea index; BP, blood pressure; PVC, premature ventricular complex.
Multivariable predictors of long-term average heart rate and heart rate variability
n = 450, linear (standardized beta coefficient) regression analyses. AHI, apnoea–hypopnoea index; BP, blood pressure; lnHF, natural logarithm of the power in the high-frequency spectrum; lnLF, natural logarithm of the power in the low-frequency spectrum.
No runs of sustained ventricular tachycardia or other symptomatic ventricular arrhythmias were observed. The prevalences of asymptomatic ventricular arrhythmias are given in Figure 1. There was significantly increased prevalence of trigeminies in Type D persons compared to non-Type D persons (7.3 vs. 2.9%, p = 0.041). However, this association was not tested in multivariate analyses due to the low prevalence. Any occurrence of a complex ventricular ectopy was significantly more prevalent in persons with Type D personality than in those without (13.9 vs. 5.9%, p = 0.007) (Figure 1).
Comparisons of prevalences of ventricular arrhythmias between Type D and non-Type personality persons during Holter recording.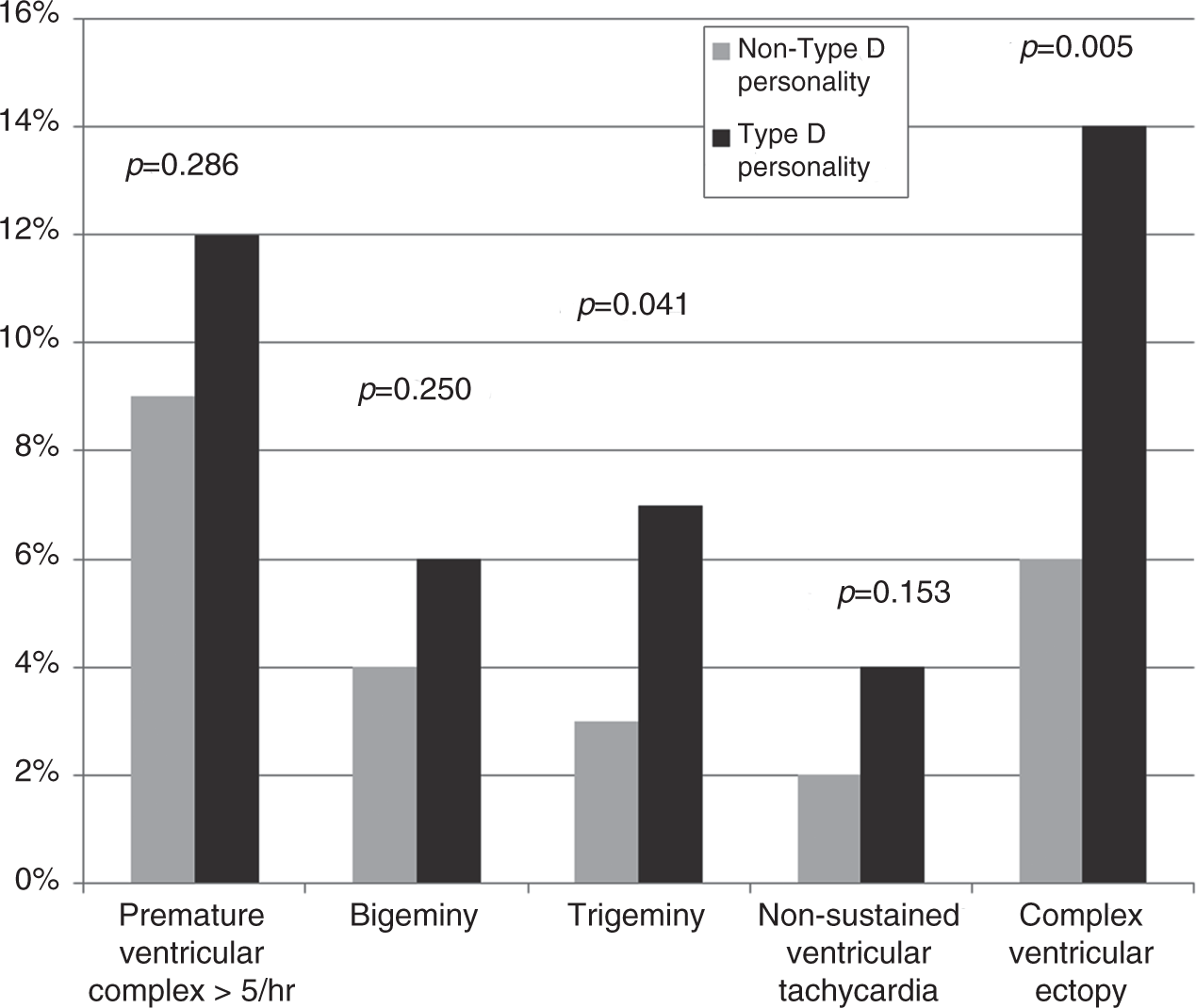
The covariates age and systolic blood pressure were also positively associated with the prevalence of complex ventricular ectopy (Table 3). Thus, as Type D persons were younger and with lower systolic blood pressure than non-Type D persons, the association between Type D personality and complex ventricular ectopy was strengthened in the multivariate model, yielding an adjusted odds ratio of 3.0 (95% CI 1.4–6.5, p = 0.005) (Table 5). Use of beta-blockers was not included in the multivariate model, as it was not associated with prevalence of complex ventricular ectopy by univariate analyses. Due to the difference in usage of beta-blockers between Type D and non-Type D persons, additional analyses were performed to evaluate its potential confounding role. Entering beta-blocker use in the model shown in Table 5 changed the OR (95% CI) and p for the association between Type D personality and complex ventricular ectopy to 2.8 (95% CI 1.3–6.1, p = 0.009). There was no univariate or multivariate association between Type D personality and the occurrence of >5 PVC/h.
Heart rate variability
There were no differences between Type D and non-Type D persons regarding lnHF or lnLF. Female gender, higher age, and traditional cardiovascular risk factors were associated with lower HRV, but adjustment for these factors did not substantially alter the relation between Type D and HRV (Tables 1, 2 and 4).
Influence of anxiety symptoms
The severity of self-reported anxiety symptoms as measured by HADS anxiety was associated with faster average long-term heart rate (p = 0.026 in univariate analyses), but not with the prevalence of ventricular arrhythmias or HRV. When adjusted for in a multivariate model, the association between anxiety and heart rate was attenuated and not significant. The clustering of Type D personality and anxiety did not contribute with significant explanation in any of the multivariate models.
Discussion
The main finding in this study is that Type D personality is associated with an increased prevalence of complex ventricular ectopy. The elevation of heart rate in Type D persons may be mediated by traditional cardiovascular risk factors, while there was no significant association between Type D personality and HRV. Concurrent anxiety did not have an effect on the relations between Type D personality and heart rate, ventricular arrhythmias and HRV.
Average heart rate and ventricular arrhythmias
Type D personality is considered to be a stable construct over time probably involving genetic factors predisposing persons to chronic distress when exposed to physical and psychological challenges. 28 Given the activation of the autonomic nervous system and HPA axis during acute stress, 29 the possibility that Type D personality is accompanied by chronic dysfunction of these systems constitute an intriguing hypothesis. In the present study, heart rate, arrhythmias, and HRV were studied as markers of such dysfunction.
Elevations of resting heart rate is emerging as an increasingly important independent predictor of cardiovascular risk,30,31 and we have previously reported that Type D personality is associated with increased heart rate. 18 However, this was a post-hoc finding based on a single measurement of heart rate, which is susceptible to influence by the white-coat effect, as well as environmental conditions, both of which may have conceivably greater effects in Type D personalities. Thus, a novel approach in this study was to evaluate continuous heart rate monitoring over 18 hours, providing a more physiological measure. We found faster average heart rate among Type D persons throughout the day and night, even in standardized laboratory condition. However, it seems that somatic comorbidity and medication mediate this association. Notably, Type D participants used less frequent beta-blockers. This could be explained by them being younger and having lower systolic blood pressure, however previous literature have pointed to Type D persons as attending regular medical examination less frequently and having lower compliance for medical treatment.32,33
Furthermore, we report increased occurrence of any ventricular ectopy including bigeminy, trigeminy, and non-sustained ventricular tachycardia. These data extend previous reports showing that Type D personality might influence the risk for symptomatic ventricular arrhythmias in patients with an implantable cardioverter defibrillator.14,21 Importantly, the present results are reported in a sample without established CHD, which increases the probability for this being an effect of Type D personality per se, and not simply the effect of comorbid somatic conditions. In the present study, several traditional cardiovascular risk factors were indeed lower in Type D persons, including age and systolic blood pressure.
Heart rate variability
HRV is a non-invasive marker of autonomic activity, in which lnHF is considered to reflect parasympathetic activity, while lnLF is among the measures representing sympathetic activity. 34 Low HRV has recently been associated with depression. 35 Experimental data suggests similar findings among young adults with Type D personality. 15 In the present study, we found no significant association between HRV parameters and Type D personality. However, there were negative associations between traditional cardiovascular risk factors and HRV, counting against that sympathico-vagal disturbance was the cause of arrhythmias in our sample.
Concurrent anxiety
In the present study, Type D persons reported significantly more anxiety symptoms than non-Type D persons, in line with previous literature. 36 However, the univariate analyses show that Type D personality is more closely related to the dependent variables than anxiety in this sample. Consequently, adjusting for anxiety did not alter the relation between Type D and arrhythmias or heart rate. Neither was there a significant interaction by the cluster of Type D and anxiety as measured by HADS ≥8.
While this study cannot further differentiate the discussion of the psychological validity of Type D personality versus other psychological factors, it is evident that DS-14 more accurately than other psychological instruments select persons at risk for cardiovascular risk or risk markers. 37
Although this study is community based, the generalizability to the general population is reduced by the inclusion procedure, which included deliberate oversampling of persons at high risk for obstructive sleep apnoea in part of the study group. However, Type D persons did not differ from non-Type D persons regarding snoring, obesity, or hypertension, and the presence of obstructive sleep apnoea was adjusted for in the multivariate model. The markers of sympathetic activity are influenced by factors not accounted for in this study, such as physical activity, respiratory rate, and sleep duration. However, an important and unique strength of our study is the objective and subjective sleep registration, excluding the potential effect of sleep apnoeas. Moreover, the self-reported increase in daytime sleepiness among Type D persons, in line with previous literature pointing to Type D personality as a determinant of poor health, 36 may be worth further studies. The lack of objective measurements of myocardial function is a limitation of this study, and future studies should rectify this. In mitigation, the expected prevalence of structural cardiac disease in this community-based sample is likely to be low. The clinical significance of asymptomatic ventricular arrhythmias may be questioned. However, ventricular ectopy is associated with the risk of future fatal arrhythmias. 11
Conclusion
Type D personality is associated with increased rate of asymptomatic complex ventricular ectopy, as well as a tendency towards higher day- and night-time heart rate in persons derived from a community sample. No association between Type D personality and HRV was evident.
To determine the clinical relevance of arrhythmias among Type D persons, our data speak to the need for evaluation of these associations in samples with higher prevalence of arrhythmias, including symptomatic arrhythmias. Identification of likely mechanisms would help guide whether future interventions should target biological pathways, personality, or both.
Footnotes
Funding
This work was supported by the South-Eastern Norway Regional Health Authority (grant number 2004219).
Conflic of interest
None declared.