
Abstract
There is a growing population of veteran endurance athletes, regularly participating in training and competition. Although the graded benefit of exercise on cardiovascular health and mortality is well established, recent studies have raised concern that prolonged and strenuous endurance exercise may predispose to atrial and ventricular arrhythmias. Atrial fibrillation (AF) and atrial flutter are facilitated by atrial remodelling, atrial ectopy, and an imbalance of the autonomic nervous system. Endurance sports practice has an impact on all of these factors and may therefore act as a promoter of these arrhythmias. In an animal model, long-term intensive exercise training induced fibrosis in both atria and increased susceptibility to AF. While the prevalence of AF is low in young competitive athletes, it increases substantially in the aging athlete, which is possibly associated with an accumulation of lifetime training hours and participation in competitions. A recent meta-analysis revealed a 5-fold increased risk of AF in middle-aged endurance athletes with a striking male predominance. Beside physical activity, height and absolute left atrial size are independent risk factors for lone AF and the stature of men per se may explain part of their higher risk of AF. Furthermore, for a comparable amount of training volume and performance, male non-elite athletes exhibit a higher blood pressure at rest and peak exercise, a more concentric type of left ventricular remodelling, and an altered diastolic function, possibly contributing to a more pronounced atrial remodelling. The sports cardiologist should be aware of the distinctive features of AF in athletes. Therapeutic recommendations should be given in close cooperation with an electrophysiologist. Reduction of training volume is often not desired and drug therapy not well tolerated. An early ablation strategy may be appropriate for some athletes with an impaired physical performance, especially when continuation of competitive activity is intended. This review focuses on the prevalence, risk factors, and mechanisms of AF in endurance athletes, and possible therapeutic options.
Introduction
The graded benefit of exercise on cardiovascular health and mortality has been demonstrated in several observational and cohort studies. 1 However, there remains considerable uncertainty about the consequences of prolonged high-intensity endurance exercise for overall health. This uncertainty existed long before Spiridon Louis, a Greek postal worker, won the first Marathon during the Olympic games in 1896 in Greece, as reflected in the ancient story of Pheidipides. Based more on fiction than on historic evidence, the story tells about an Athenian messenger who died after running more than 280 miles from Athens via Sparta to Marathon and back, reporting the end of the Persian War. 2
Although sudden cardiac arrests are rare events in long-distance races and are most commonly associated with an underlying heart disease, 3 recent studies have raised concern that prolonged and strenuous endurance exercise may predispose to atrial and ventricular arrhythmias.4–8 Postexertional increase in cardiac biomarkers and a transient cardiac dysfunction in marathon runners raised the question whether endurance sports may alter the cardiac substrate and serve as promoter rather than a trigger of arrhythmias.9,10 Much research has focused on the left ventricle (LV), but long-term follow up of Olympic athletes revealed neither deterioration in LV function, nor significant changes in LV morphology, nor occurrence of cardiovascular events. 11
However, the right ventricle and the atria are cavities with substantially thinner walls, which are more prone to exercise-induced remodelling due to repetitive episodes of volume overload during training and competition. Karjalainen et al. 12 were the first to report an association of vigorous exercise and atrial fibrillation (AF) in a longitudinal case–control study in top-level veteran orienteers. In an animal model, long-term intensive exercise training induced fibrosis in both atria and the right ventricle, and increased susceptibility to AF and right ventricular arrhythmias.13,14 A recent meta-analysis revealed a 5-fold increased risk of AF in endurance athletes. 15 However, there remains a controversy regarding the association of physical activity in general and the increased risk for AF.16,17
Since long-distance running has become very popular, especially in non-elite middle-aged athletes, 3 the topic is of clinical relevance, not only for the sports cardiologist.
Prevalence and risk of AF in athletes
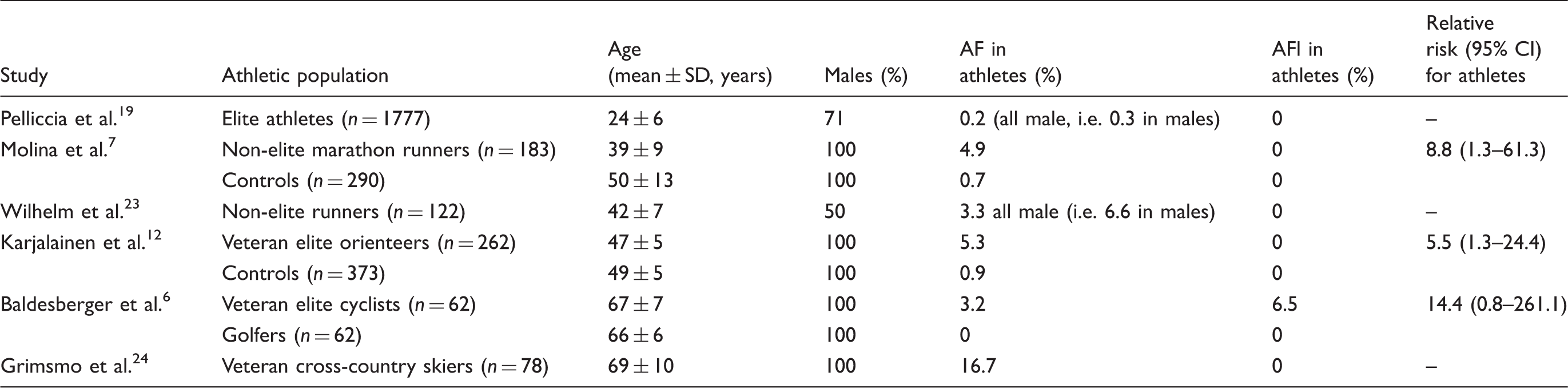
In general population studies, the average prevalence of paroxysmal or persistent AF is 0.5% in subjects aged 45–54 years, about 1% at 54–64 years, and 4% at 65–74 years. 18 Pelliccia et al. 19 reported a lower prevalence of AF (0.2%) in young competitive athletes. AF accounted for only 36% of all supraventricular arrhythmias and was not associated with atrial remodelling. In former elite athletes, who continued recreational sports activities after the end of their competitive careers, no AF could be demonstrated with Holter monitoring at 15 years’ follow up, when the athletes had an age of about 40 years. 20 In a study by Furlanello et al., 21 38% of young elite athletes with AF had an underlying substrate like Wolff–Parkinson–White syndrome, arrhythmogenic right ventricular cardiomyopathy or healed myocarditis. Karjalainen et al. 12 performed a longitudinal case–control study in top-level veteran orienteers. Compared with controls, orienteers had a higher prevalence of AF (5.3 vs. 0.9%) despite fewer risk factors for AF and a lower overall mortality (1.7 vs. 8.5%). The risk for developing AF was increased 5.5-fold in orienteers. 12
The higher risk of AF associated with endurance sports had subsequently been confirmed in different populations. Several studies analysed the proportion of athletes in a cohort of patients with arrhythmias. In a retrospective study, Mont et al. 4 reviewed 1160 records from an arrhythmia outpatient clinic and identified 70 patients younger than 65 years with lone AF. The proportion of sportsmen (endurance sports >3 hours per week) among patients with lone AF was higher than that reported in the general population of the area (63 vs. 15%). 4 The same population was analysed in an age-matched case–control study. Current endurance sport practice and more than 1500 accumulated hours of endurance training increase the risk of lone AF 2.9-fold, and the risk of vagal AF 5.1-fold. 5 Heidbuchel et al. 22 evaluated 137 patients (mean age 58 ± 10 years) after an ablation procedure for atrial flutter. 23% of patients had been regularly engaged in endurance sports (cycling, running, or swimming for >3 hours per week and for >3 years preablation). During a follow up of 2.5 years, endurance sport practice was a risk factor for post-ablation AF with a multivariate hazard ratio of 1.81 (range 1.10–2.98). 22
The prevalence and risk of atrial fibrillation (AF) and atrial flutter (AFl) in different athletic populations and age groups
Risk factors for AF and atrial flutter in athletes
AF and atrial flutter are facilitated by atrial remodelling, atrial ectopy, and an imbalance of the autonomic nervous system (see Figure 1 for an overview).25–28 Endurance sports practice has an impact on all of these factors and may therefore act as a promoter of these arrhythmias. Moreover, arterial hypertension is the most common cardiovascular risk factor in athletes
29
and is an independent risk factor for AF.
30
While moderate activity is effective in both systolic and diastolic blood pressure reduction, the effect of high-intensity activities on the blood pressure profile are inconsistent.
31
Compared to recreationally active control subjects, age-matched marathon runners exhibited a higher systolic blood pressure and arterial stiffness, possibly contributing to LV hypertrophy, diastolic dysfunction, and atrial remodelling in the long term.
32
Synopsis of factors influencing the development of atrial fibrillation in athletes.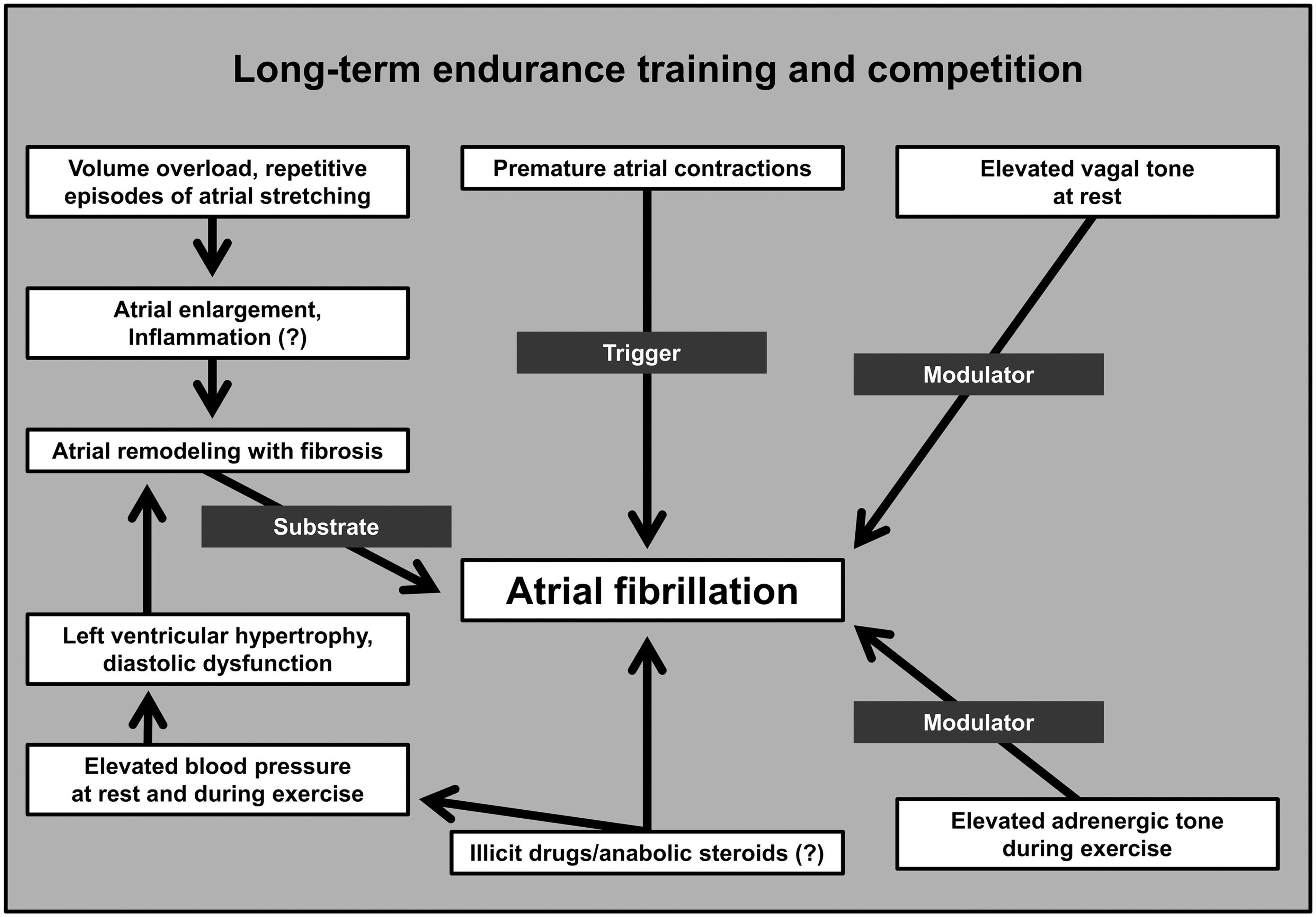
Although the arrhythmic mechanisms of illicit drugs like anabolic steroids remain unresolved, these substances have also been associated with hypertension, LV hypertrophy, and LV dysfunction and may contribute to atrial arrhythmias in athletes. Moreover, anabolic steroids may exhibit direct negative effects on the atrial myocardium.33,34
Noteworthy, structural heart disease, thyroid dysfunction, and alcohol abuse are factors that can cause AF independent from endurance sports practice. 35
The substrate: atrial remodelling in athletes
Left atrial size is an independent predictor of AF in healthy middle-aged individuals. 36 An enlarged left atrial volume was associated with a higher risk of AF in marathon runners. 7 In contrast, 20% of young competitive athletes exhibited left atrial enlargement without a greater risk of AF. 19
In general, endurance training leads to a harmonic enlargement of all four cardiac cavities as an adaptation to exercise conditioning. 37 However, according to the Law of Laplace, wall thickness and cavity radius contribute to wall tension. 38 Since the atrial walls are much thinner than the ventricular walls, atrial wall stress is higher during episodes of training-related volume overload and may contribute to progressive enlargement and remodelling. In Olympic athletes, extreme and uninterrupted endurance training over a period of up to 17 years was associated with an increase in left atrial size, while LV cavity size remained stable. 11
An age-dependent increase in left atrial volume had been demonstrated in professional soccer players. 39 In a cross-sectional study on middle-aged non-elite runners (mean age 42 ± 7 years), left atrial size increased gradually with lifetime training hours. Over 80% of athletes with more than 4500 lifetime training hours showed left atrial enlargement. 40
Besides exercise training duration, exercise quality (e.g. participation in strenuous competitions like long-distance running) makes an important contribution to atrial remodelling. Non-elite marathon runners had larger left and right atria compared to non-marathon runners. The number of marathon participations was an independent predictor for left and right atrial cavity enlargement but was not associated with ventricular cavity enlargement. 41 Increased atrial wall stress in these athletes was reflected by levels of pro-atrial natriuretic peptide (proANP), prior and post a long-distance race. 42 Since marathon runners exhibited larger atrial volumes, baseline and peak exercise levels of proANP were higher compared to non-marathon runners. 42 Interestingly, pro-ANP levels correlated only with right atrial volume, indicating the importance of volume overload of the right heart during strenuous activities. Acute dilatation of the right atrium, but not of the left atrium, has been demonstrated in runners immediately after a marathon race. 43 However, in the long term, a homogeneous enlargement of both atrial cavities has been demonstrated 41 and may be an explanation for the often simultaneous occurrence of AF and common atrial flutter.6,12,44 Claessen et al. 45 performed a case–control study in consecutive patients with atrial flutter. The proportion of sportsmen engaged in long-term endurance sports (>3 hours per week) was significantly higher in lone atrial flutter patients than in controls (31 vs. 8%). 45
Repetitive episodes of atrial stretching and an elevated wall stress may stimulate atrial fibrosis. Moreover, excessive endurance training has been associated with chronic inflammation, which may be a contributing factor for atrial fibrosis and AF.46,47 After a strenuous mountain marathon, runners exhibited a transient conduction delay in the atria, together with increased markers of inflammation and atrial wall tension. This may reflect exercise-induced atrial myocardial oedema, contributing to atrial remodelling over time. 48 In an animal model, prolonged exercise training over 16 weeks induced atrial fibrosis as a substrate for atrial arrhythmias. 14 Veteran athletes showed biochemical evidence of disruption of the collagen equilibrium favouring fibrosis. Compared to sedentary controls, markers of collagen synthesis, degradation and inhibition of degradation were elevated in the cohort of athletes. 49
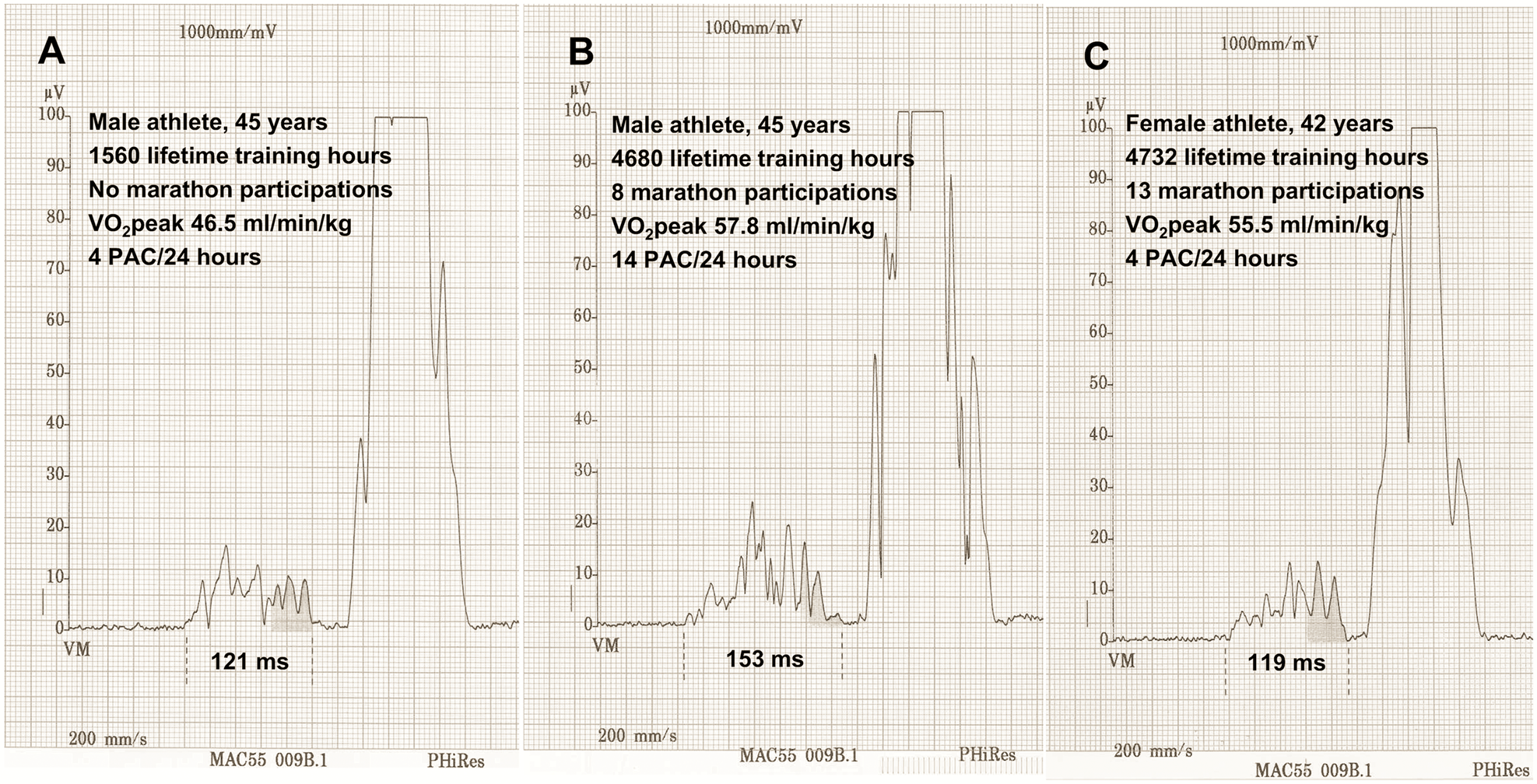
Signal-averaged P wave analysis can detect intra-atrial conduction delay as a surrogate for atrial fibrosis. It has been used in patients with and without structural heart disease to predict risk of AF.50,51 Non-elite male runners with more than 4500 lifetime training hours exhibited a prolonged signal-averaged P wave duration compared to runners with lesser training hours (Figure 2A and B).
40
Taken together, atrial enlargement is common in young endurance athletes and most probably reflects cardiac adaptation to exercise conditioning. However, it may be accompanied by atrial fibrosis in the aging athlete, thus create a substrate for AF and atrial flutter.
Modulators: the autonomic nervous system
The autonomic nervous system plays an important role in both the initiation and the maintenance of AF and atrial flutter. In patients with paroxysmal AF and pulmonary vein ectopy, adrenergic activation followed by an abrupt shift towards vagal predominance is often observed prior to AF initiation. 52 For example, vagal AF may occur during the recovery phase of an interval training, or in cycling after climbing a hill in the descent that follows, when the exercise intensity decreases sharply.
Moreover, endurance sport practice itself is associated with a high parasympathetic activity.
53
In middle-aged non-elite runners, markers of vagal tone increased with lifetime training hours (Figure 3A and B).
40
An increased vagal tone shortens the atrial refractory period facilitating macro re-entries of the left and right atrium, also in the absence of an altered atrial substrate. In sportsmen with atrial arrhythmias, 25% of orienteers, 67% of former cyclists, and 10% of non-elite endurance athletes presented with atrial flutter in addition to AF.6,12,44 Vagally mediated AF generally occurs at rest, during the night, or in the postprandial state.
25
In the general population, vagally mediated AF was more common in sportsmen (regular endurance training >3 hours per week) compared to sedentary individuals.
4
Endurance training and modulation of the autonomic nervous system. Power spectral analysis of short segments of heart rate variability (recorded at 6 a.m.) from representative athletes of studies by Wilhelm et al.:23,40 male leisure-time athlete (A); male competitive, non-elite athlete (B); and female competitive, non-elite athlete (C).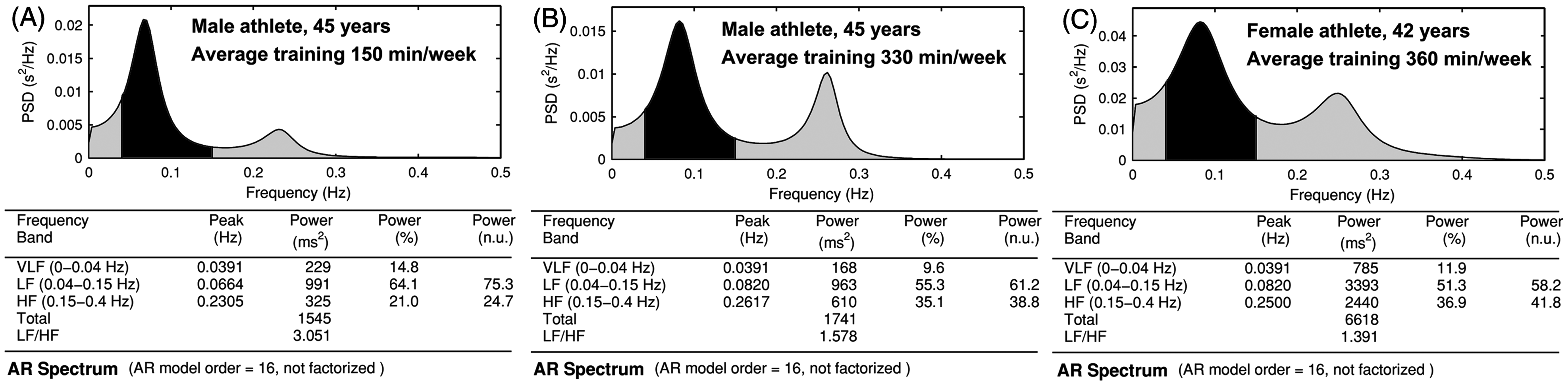
A conversion from vagal to adrenergic predominance has been demonstrated in highly trained athletes prior to competitions. 54 Adrenergic predominance favours automaticity and micro re-entries, especially in structurally remodelled atria. 25 However, in middle-aged endurance athletes (mean age 48 ± 8 years) with AF, both vagally and adrenergic-mediated forms of AF occurred (33 vs. 23%). Over a follow up of 9 years, two patients (20%) with vagally induced AF progressed to permanent AF, compared to no patient with adrenergic-induced AF, suggesting the absence of a severe atrial remodelling in this group. 44
Triggers: premature atrial contractions
Pulmonary vein ectopy is the major trigger for paroxysmal AF. 28 In general, atrial ectopy is only modestly increased in endurance athletes. Former professional cyclists (mean age 66 ± 7 years) did not differ in regard to premature atrial complexes with age-matched golfers 6 . In contrast, in non-elite runners (mean age 42 ± 7 years), premature atrial complexes increased with lifetime training hours 40 and the number of marathon participations. 42 In young individuals (mean age 24 years), premature atrial complexes during 24-hour Holter monitoring were also scarce but most frequent in top athletes, followed by athletic students and sedentary controls (2.0, 1.0, 0.7 beats/h, respectively). 55
Gender differences of AF in athletes
Observational studies suggest a striking male predominance of AF in athletes.4,21–23 In a prospective case–control study on middle-aged individuals, physical activity, height, and absolute left atrial size were independent risk factors for lone AF. Since height, body surface area, and atrial size are closely correlated, the taller stature of men per se may explain part of their higher risk for AF. 36 Furthermore, a study on middle-aged female and male non-elite runners suggested a more pronounced atrial remodelling in male runners. For a comparable amount of training and performance, male athletes exhibited a higher systolic blood pressure at rest and peak exercise together with a more concentric type of LV hypertrophy, an altered diastolic function, and a longer signal-averaged P wave duration (Figure 2B and C). Left atrial volume and right atrial volume index were larger in male athletes, while left atrial volume index showed no gender differences. Atrial ectopy was low and equally distributed between female and male athletes. Sympathetic activity was higher in male athletes (Figure 3B and C), favouring adrenergic-mediated AF, especially in the presence of an altered atrial substrate. Thus, the prevalence of paroxysmal AF was 6.7% in male runners, compared to 0% in female runners. 23 In conclusion, beside possible differences in training intensities between male and female athletes, the taller stature and higher blood pressure in men may play a pivotal role in arrhythmogenesis.
Diagnostic evaluation
AF is the most frequent cause of palpitations in athletes. 56 It is essential to obtain a thorough history, including frequency and duration of episodes and their association with sports activities, as well as the use of performance-enhancing or other drugs. 57
The initial evaluation includes a physical examination and a 12-lead electrocardiogram (ECG). Prolonged ECG monitoring is recommended for suspected but not documented episodes of AF. It has been estimated that 7-day Holter ECG recording may document the arrhythmia in approximately 70% of patients. 35
Ergometry may reveal exercise-associated AF and atrial flutter, and ECG registration should be continued at least 5 minutes during the recovery period. Echocardiography and laboratory tests should be performed to exclude common causes of AF like structural heart disease or thyroid dysfunction. 35
Signal-averaged analysis of the P wave is an accepted non-invasive marker for atrial electrical remodelling (Figure 2), but rarely used in clinical practice. 58 A signal-averaged P wave duration of more than 145 ms successfully predicts the transition from paroxysmal to persistent AF. 59 In athletes, the signal-averaged P wave duration may help to differentiate vagal AF from AF secondary to atrial remodelling.
Therapeutic options for athletes with AF
Given the importance of an elevated vagal tone for the initiation and maintenance of sports-related AF and atrial flutter, a reduction of exercise volume would shift the autonomic balance towards a higher adrenergic tone and reduce the burden of vagally mediated AF. In a small series of elite athletes with AF, sport abstinence resulted in a disappearance of the arrhythmia. 21 Moreover, also atrial remodelling is related to training volume.5,40 In the Physicians Health Study, the relative risk of AF increased in joggers practising more than 3 or 4 days a week. 60 Thus, limiting endurance training is the most important recommendation in athletes with AF.
The psychological consequences of limiting sports practice have to be discussed with the athlete, and probably strong psychological support is needed in some patients in whom endurance training is the centre of their lives. However, reducing endurance training volume may not be sufficient to prevent AF recurrence in all patients. Moreover, veteran athletes are often addicted to their sporting life and prefer alternative therapeutic options.
In the presence of an elevated blood pressure with or without structural heart disease, angiotensin II receptor blockers are beneficial in reducing the AF burden.61,62 A reduction of AF upon angiotensin II receptor blockers has not been observed in normotensive patients without structural heart disease, 63 and there are virtually no studies in athletes. Antiarrhythmic therapy should follow current guidelines.35,57 Sodium channel-blocking drugs like flecainide are often successful especially in vagally mediated AF. Medication may be administered as a ‘pill-in-the-pocket’ approach or on a regular basis. Therapy should be combined with a calcium antagonist like verapamil or diltiazem to prevent 1:1 atrial flutter. Amiodarone, although the most potent antiarrhythmic drug, is often not well tolerated, especially due to side effects like photosensitivity in outdoor sports. 64 The anticoagulation regime is based on the CHA2DS2-VASc score, as in non-athletes. 35 It must be reminded that an anticoagulation regime may limit the practice of sports with body collision risk, like soccer, ice hockey, or sometimes cycling. 57
An early ablation strategy may be appropriate for athletes with an impaired physical performance, especially when continuation of competitive activity is intended.35,57 Furlanello et al. 65 reported of radiofrequency catheter ablation for AF in 20 competitive athletes with disabling symptoms. Success rate after a mean of two ablations was 90% without major complications. 65 Calvo et al. 66 analysed a series of AF ablations in 182 consecutive patients, 59% with lone AF, and 39% of those were classified as endurance athletes (endurance sport activity >3 hours per week for at least 10 years). A second ablation was necessary in 37% of patients to achieve a 72% overall probability of freedom of AF at 1 year. Circumferential pulmonary vein ablation was as effective in AF secondary to endurance sport practice as in other aetiologies of AF. 66 Koopman et al. 67 compared the procedural outcome of 94 athletes (>3 hours training per week for >10 years or more than 1500 lifetime training hours, 63% endurance athletes) with 41 controls. Final outcome after a mean of 1.2 ± 0.5 ablations was similar for endurance athletes, non-endurance athletes, and controls (87 vs. 84 vs. 85% after 3 years of follow up, respectively). 67 Despite these encouraging results it has to be kept in mind that these ablation studies did not include high-level endurance athletes who may exhibit a more pronounced atrial remodelling, predisposing to a lower procedural success. 68
Conclusions
What should we recommend to the followers of Spiridon Louis? Should we encourage them to continue high-intensity and prolonged endurance activities even in their fifties? Although the aging endurance athlete has an increased risk of developing atrial arrhythmias, the benefits of regular exercise and an athletic lifestyle far outweighs the negative consequences. In the initial study of Karjalainen et al., 12 compared to controls, veteran orienteers had a lower overall mortality despite their higher risk of AF. However, male veteran athletes especially should be aware of additional risk factors for AF. Arterial hypertension is the most prevalent diagnosed disease in athletes over 35 years old. 29 Since athletes are already likely to lead a healthy lifestyle, early drug treatment for arterial hypertension, preferably with an angiotensin II receptor blocker, is to be recommended. 35 Athletes with episodes of AF should reduce training volume and intensity, and class I and III antiarrhythmic drugs can be prescribed. Circumferential pulmonary vein ablation is an option for athletes with severe symptoms. A first-line approach can be discussed, especially when the left atrium is not substantially enlarged. 35
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None.
Acknowledgements
The author likes to thank Prisca Eser, PhD for carefully reviewing the manuscript.