
Abstract
Background
Cardiovascular diseases (CVDs) are the main cause of death and disability in the western world. Women are known to be older at the time of first CVD event, but the main types of CVD events and their relative importance and differences compared with men are not well known. Our aim was to evaluate gender differences in the clinical presentation of incident major adverse cardiovascular events (MACE).
Design
A population-based study with prospective follow-up.
Methods
We used data from the population-based National FINRISK Surveys from years 1992, 1997, 2002 and 2007. People with prevalent cardiovascular disease were excluded. In total, 27,897 participants (53, 2% women) aged 25–74 years were included in the analyses.
Results
During the 292,316 person-years of follow-up, 2573 MACE were identified. MACE were more frequent in men than women (1318; 95% CI 1252–1388 in men vs. 736; 686–789 in women). Men had four times more fatal coronary heart disease (CHD) events (149; 126–174 vs. 39; 28–53) and three times more non-fatal CHD events (512; 471–555 vs. 164; 141–189) than women. Stroke incidence was higher in men than women (268; 238–301 vs. 169; 145–195). Heart failure (HF) incidence did not differ between genders. The relative proportions of MACE categories differed substantially between genders: HF was the most common type among women (50% vs. 30% in men), whereas the most common type among men was CHD (50% vs. 28% in women).
Conclusions
Incident MACE were more common in men than women. HF was the dominant type of MACE in women, whereas CHD dominated in men.
Introduction
Cardiovascular diseases (CVDs) are the main cause of mortality, morbidity and disability in both genders in the western world. In 2008, CVD accounted for 32.8% of all deaths in the USA, causing one of every three deaths. 1 In Europe, CVD accounted for 47% of all deaths; 52% of all women’s and 42% of all men’s deaths result from CVD. 2 Coronary heart disease (CHD) and stroke are the main forms of CVD. CHD is the single most common cause of death in both genders in people aged < 75 years. According to the 2012 European Cardiovascular disease statistics in Europe CHD accounted for 17% of deaths in women and stroke a further 11% and in men CHD caused 19% of deaths and stroke a further 6%. 2
In recent decades, age-adjusted CVD mortality and incidence rates have declined in most western countries.1,2 However, some age- and sex-dependent differences, unfavourable to young and middle-aged women, have been shown to exist in both CHD and stroke mortality and prevalence trends.3–6 National Health and Nutrition Examination Surveys (NHAHES) data from the USA have shown increasing stroke prevalence and myocardial infarction (MI) prevalence in middle-aged women.4,5 We have previously shown slower decline in MI incidence and mortality in middle-aged women in Finland. 6 At the same time heart failure (HF) prevalence has steadily increased. It has been estimated that one in every five middle-aged men and women will develop HF during their lifetime. 7 In the population aged > 65 years, HF is the leading cause of hospital admissions in the USA and the prevalence of HF increases with ageing. 1
Although, quite a lot is known about the gender differences in CVD incidence and mortality rates, there are few population-based follow-up studies on gender differences in clinical manifestations of the first CVD events. The aim of the present study was 1. to evaluate gender differences in the incident (=first) major cardiovascular event (MACE) rates, and 2. to evaluate whether there are gender differences in the clinical spectrum (acute non-fatal or fatal CHD events, stroke and HF) of incident MACE.
Materials and methods
We used data from the population-based FINRISK Surveys, which have collected data on cardiovascular risk factors in Finland. A survey has been conducted in 5-year intervals since 1972. During the years 1992, 1997, 2002 and 2007 five different areas in Finland were included: North Karelia and Kuopio Provinces in Eastern Finland, Turku-Loimaa in South-western Finland, Oulu Province in North-western Finland (participated since 1997) and Helsinki-Vantaa in Southern Finland. For each survey, an independent random sample of inhabitants aged 25–74 years, stratified by sex, 10-year age group and geographical region, were drawn from the Finnish Population Information System. Survey methodology has followed the WHO Monica project manual 8 and, since 2002, recommendations of the European Health Risk Monitoring Project. 9 To obtain the risk factor information a self-administered questionnaire, physical measurements and blood tests were performed. Full details on the methodology and the participation rates of the FINRISK Survey protocol have been described previously.10,11
Firstly, we identified subjects with prior history of MACE event from National Hospital Discharge Register (see ICD-codes below) backwards until the year 1969. These subjects with a history of MACE prior to the survey (n = 1388) were excluded from the analyses of incident MACE during the follow-up. Subjects were followed from the FINRISK examination date until the date of the first (=incident) event, or until 31 December 2010 when the follow-up time ended. If the subject died during the follow-up from a non-MACE event, the person was censored at the date of death. If more than one MACE event had been registered on the same date, acute CHD event was prioritized over stroke and stroke over HF. CHD event was considered in this analysis if ICD-codes (detailed below) for acute CHD event were met or the subject had a history of revascularization. Incident events leading to death were confirmed from the Causes of Death Register. An incident event was considered as fatal, if the event had occurred 0–28 days before the death, and the cause of death was any of those listed below.
Definitions for incident events
Incident events during the follow-up were identified using the national health care registers: the National Hospital Discharge Register, Causes-of-Death Register and the National Drug Reimbursement Register. These registers have been described in more detail in our recent publication. 12 In the Hospital Discharge Register and Causes-of-Death Register, diagnoses are recorded using the ICD-codes. ICD-8 was used between the years of 1968 and 1986. ICD-9 was used in Finland until the end of 1995 and ICD-10 after that. Cardiovascular diagnoses in Finnish health care registers, used as described below, have been validated previously.12–14 Acute non-fatal CHD events were identified with ICD-10 codes: I200, I21, I22 and corresponding ICD-8 and -9 codes 410 and 4110. For fatal CHD events, somewhat wider categories were used: I20–I25, I46, R96, R98 in ICD-10 and 410–414 and 798 (not 7980A) in ICD-8 and -9. CHD was also considered if the subject had prior revascularization in hospital records (percutaneous coronary intervention, coronary artery by-pass grafting). Stroke diagnoses in ICD-10 were: I60-I61, I63-I64, (not I636) and in ICD-8 and -9 430, 431 (not 43101, 43191), 433, 434 and 436. HF diagnoses included ICD-10 codes: I50, I110, I30, I132 and corresponding ICD-8 codes: 42700, 42710, 428 and ICD-9 codes: 4029B, 4148, 428. HF cases were also identified using the Drug Reimbursement Register of the Finnish Social Insurance Institution, if the participant was entitled to special reimbursements for the costs of HF medications, he/she was considered to have HF. Furthermore, if a participant had purchased furosemide prescribed by a doctor at least three times since 1995 to the end of the follow-up, he/she was considered as having HF, one time was sufficient if the subject had either the special reimbursement or had a hospital diagnosis of HF. HF includes subjects mainly from furosemide purchases. A detailed description of proportions of HF diagnoses from these different sources are shown in the web supplement.
Secondly, we separately analysed the potential aetiology of HF. We identified all subjects with diagnosed incident HF during the follow-up (n = 1195), from whom prior HF diagnosis, but not other CVD events (non-fatal CHD and stroke), had been excluded.
Statistical methods
We pooled data from all study areas and years 1992, 1997, 2002 and 2007. MACE event rates are expressed per 100,000 persons and age-standardized according to the direct method using 5-year age groups and the European standard population (http://seer.cancer.gov/stdpopulations, accessed July 2012). Incidence rates of MACE were determined by dividing the number of incident cases by the total number of person-years accumulated in the previously healthy study population. Male/female ratios (M/F ratios) were obtained by dividing incident event rates in men by event rates in women. M/F ratios were checked separately for the first and last survey years (1992 and 2007), and the results showed that the ratio remained approximately the same throughout the study period. To investigate the effect of age, we repeated all male/female comparisons separately for the younger (25–54 years) and the older (≥55) age groups. The 95% CI of age-adjusted rates and rate ratios were calculated using methods based on gamma- and F-distributions. 15 All tests were double-sided and we considered p < 0.05 to be statistically significant. All the statistical analyses were carried out using R-software, version 2.14 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Numbers, co-morbidities and mean age (±SD) of study participants with incident MACE. a
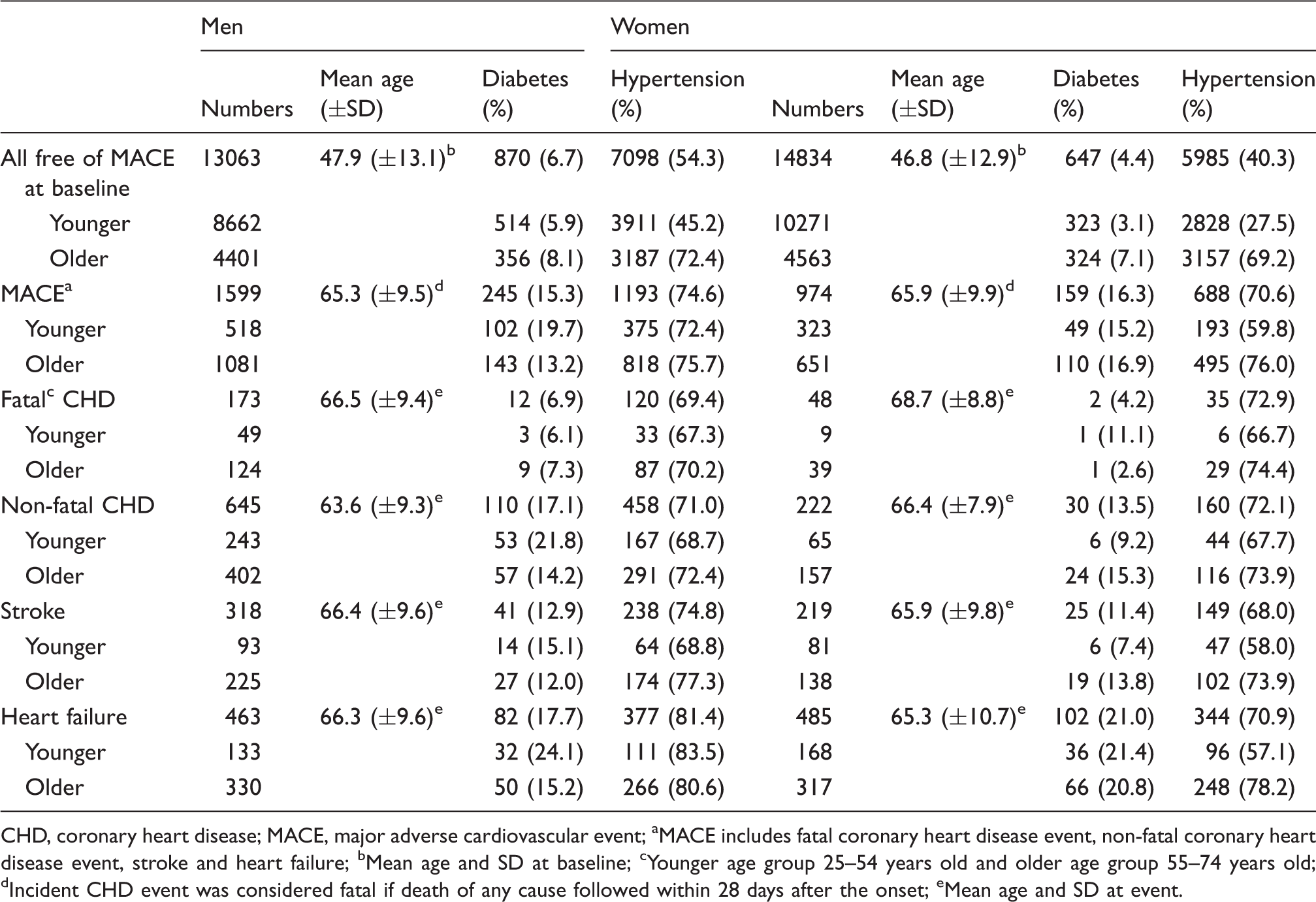
CHD, coronary heart disease; MACE, major adverse cardiovascular event
MACE includes fatal coronary heart disease event, non-fatal coronary heart disease event, stroke and heart failure
Mean age and SD at baseline
Younger age group 25–54 years old and older age group 55–74 years old
Incident CHD event was considered fatal if death of any cause followed within 28 days after the onset
Mean age and SD at event.
The incidences of MACE per 100,000 persons per year according to age group, gender and MACE subgroup are shown in Figure 1, and the male to female incidence rate ratios are shown with similar subgrouping in Table 2. The results show that the incidence of MACE in men was almost double among men compared to women, similarly in both age groups. Overall, men had significantly higher incident acute CHD event rates, especially fatal CHD events and stroke compared with women. On the other hand, HF incidence rates were equal in both genders in all studied age groups.
Incidence rates of MACE per 100,000 persons per year by gender and age group. The bars indicate 95% CI. (a) Persons aged 25–74 years. (b) Persons aged 25–54 years. (c) Persons aged 55–74 years. Male/female incidence rate ratios
a
and 95% CI of major cardiovascular events during the median follow-up of 8.9 (IQR 8.8) years in FINRISK 1992, 1997, 2002 and 2007 cohorts M/F ratios were obtained by diving incident event rates in men by event rates in women. Participants with a history of MACE at baseline are excluded MACE (major adverse cardiovascular event) include fatal coronary heart disease event, non-fatal coronary heart disease event, stroke and heart failure The event was considered fatal if it led to death within 28 days after the onset.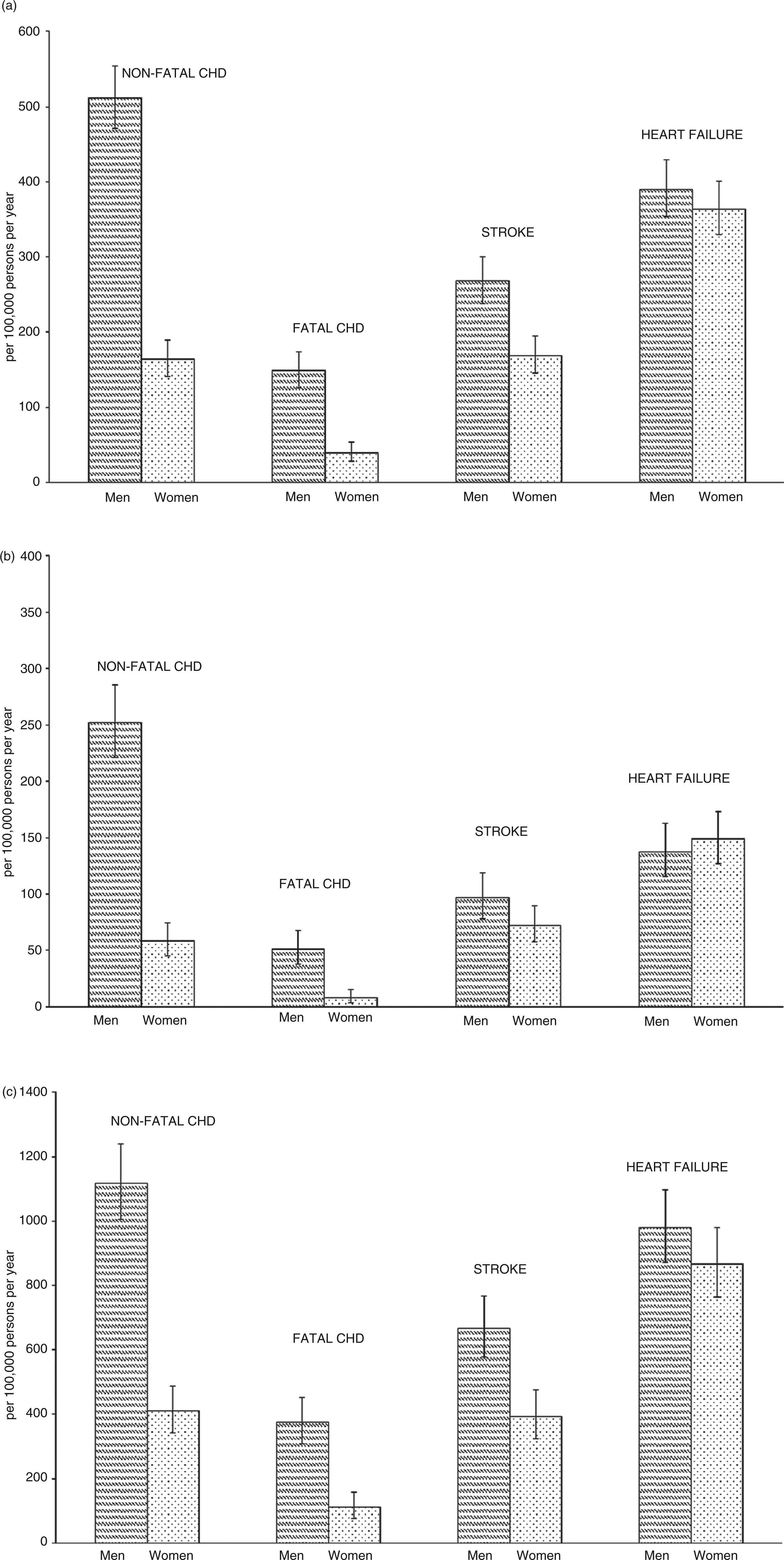
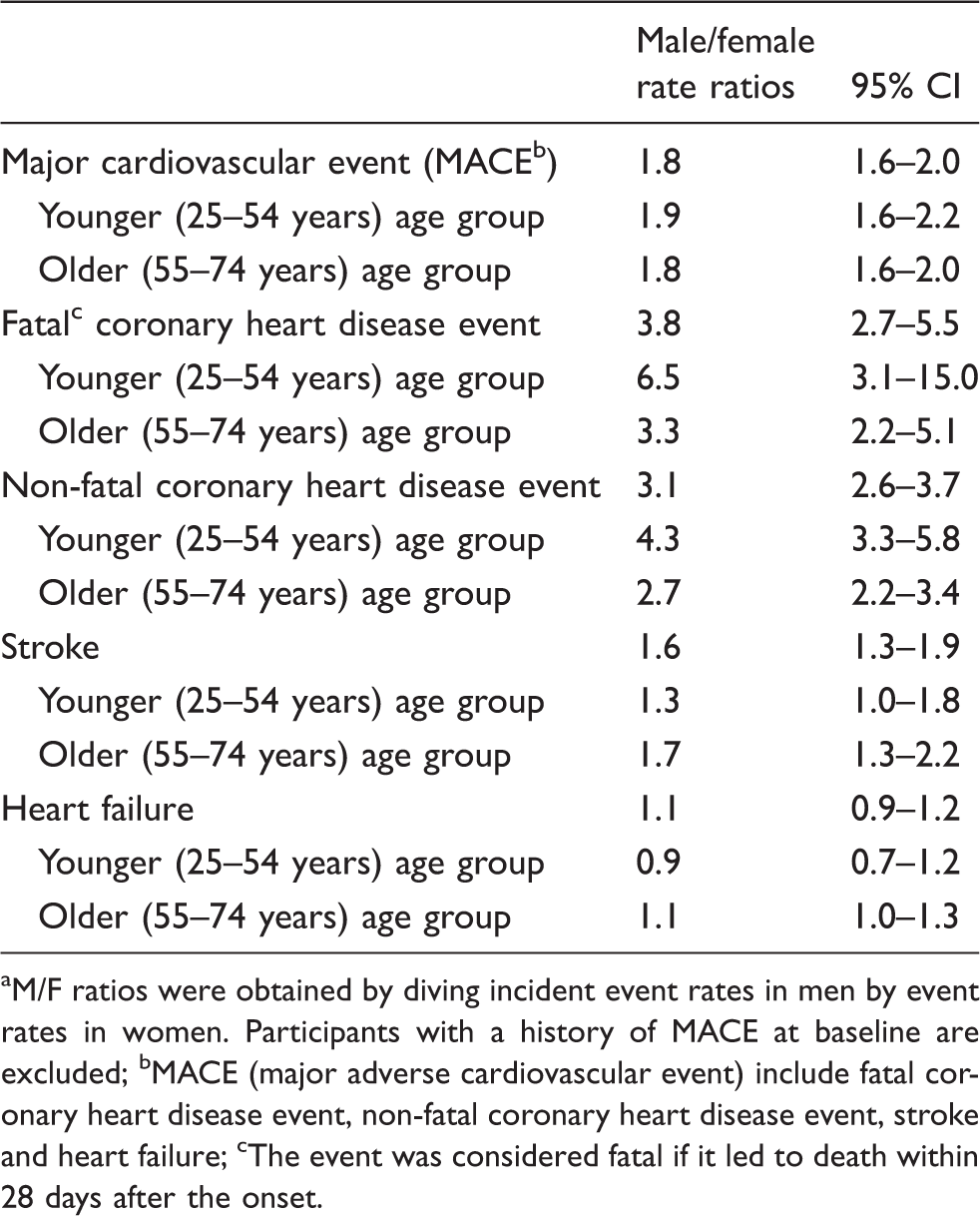
Figure 2 shows relative proportions of MACE categories in the age group of 25–74 years. The most common incident MACE in men was an acute non-fatal CHD event, and in women was HF. The relative proportions of MACE subgroups were similar in different age groups. In young men, 25–54 years old, the proportions were: acute non-fatal CHD event 46.9%, HF 25.6%, stroke 18.0% and fatal CHD event 9.5%, and in women: HF 51.8%, acute non-fatal CHD event 20.3%, stroke 25.1% and fatal CHD 2.8%. In the age group 55–74 years old, the proportions in men were: acute non-fatal CHD event 35.6%, HF 31.2%, stroke 21.3% and fatal CHD event 12.0%, and in women: HF 48.6%, acute non-fatal CHD event 23.0%, stroke 22.1% and fatal CHD event 6.3%.
Clinical spectrum of incident (=first) major adverse cardiovascular events in men and women aged 25–74 years during the median follow-up of 8.9 (IQR 8.8) years in FINRISK 1992, 1997, 2002 and 2007 cohorts.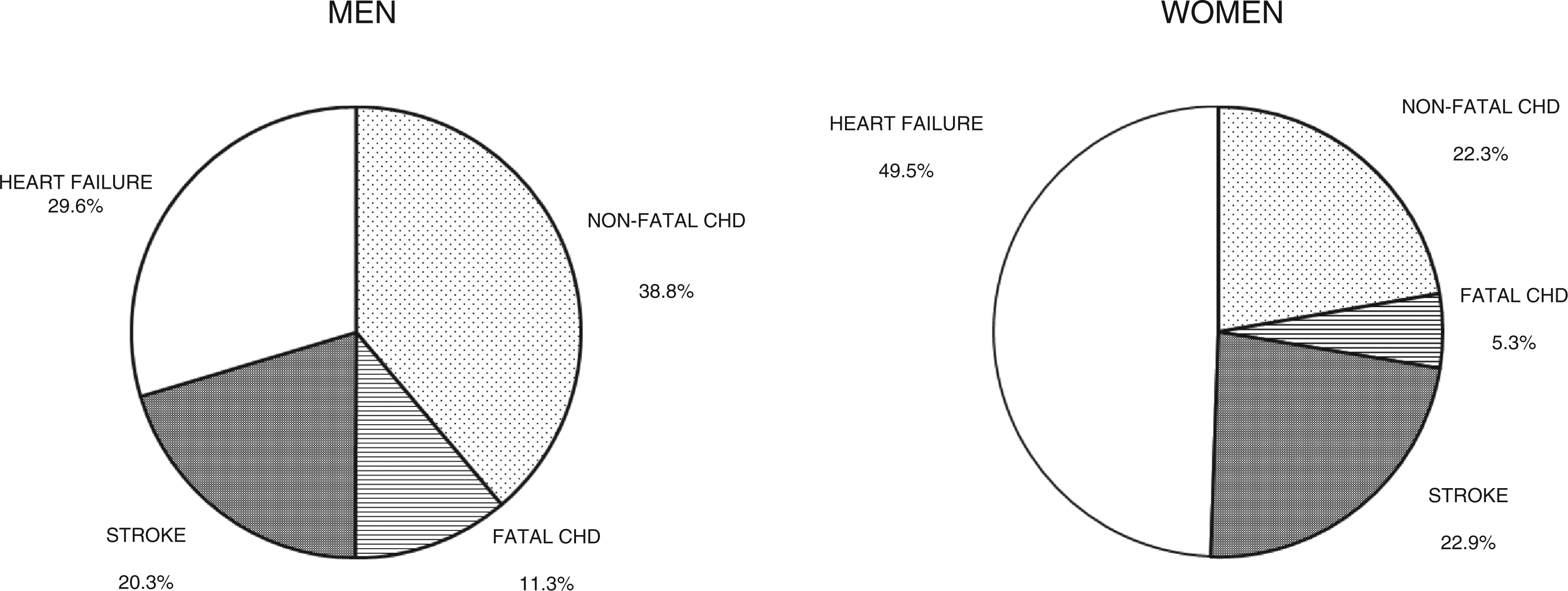
Secondly, we analyzed potential aetiological factors for subjects considered to have HF; for this analysis only prevalent HF was excluded. A total number of 1195 incident HF were identified during follow-up, 633 in men and 562 in women. Detailed proportions of HF diagnosis from different data sources are shown in the web supplement. Hypertension was the main factor preceding the HF; 83% of men and 76% of women had hypertension prior to HF. Prior ischemic heart disease was found in 42% of men and 24% of women. Diabetes was diagnosed in 28% of men and in 24% of women. In the younger age group, hypertension preceded the HF in 83% of men and 62% of women, CHD was found in 28% of men and in 12% of women, and diabetes in 27% of men and 21% of women. In the older age group, hypertension preceded the HF in 83% of men and 82% of women. CHD had been diagnosed in 46% of men and 29% of women. Diabetes preceded the HF in 28% of men and 26% of women.
Discussion
We followed up a large cohort of initially healthy men and women to detect gender differences in the clinical spectrum of incident (=first) MACE. As expected, the incidence of any MACE was significantly higher in men than in women. This was mainly as a result of the excess of acute CHD events, especially fatal CHD events, in men compared with women. The stroke incidence was also higher in men than in women but the difference was smaller than that of acute CHD events. Interestingly, the incidence of HF did not differ between the genders. When the relative proportions of different MACE types were compared, clear differences between the genders became evident. HF was by far the most common type of incident MACE in women, constituting half of all first events. The proportion of stroke was also slightly higher in women than in men. Acute CHD event was the dominant type of MACE in men with fatal and acute non-fatal CHD events combined contributing about half of all first events.
HF, like other major CVDs, is considered to be predominantly a men’s disease. Previously reported HF incidence rates, varying highly depending on the HF definition used and study population included, have been higher in men than in women in large population-based studies.16–19 However, in conflict with these, another population-based study from Worcester Hospitals in Massachusetts found a higher incidence rate of HF rate in women; 250/100,000/year in a cohort of first hospitalized HF vs. 194/100,000/year in men. 20 Compared with these incident event numbers obtained from hospitalized patients only, our study, collecting patients also from an outpatient setting, found considerably higher incidence rates (390/100,000/year in men and 364/100,000/year in women). Our event rates were, however, comparable with the rates published by a population-based study from the Olmsted County. Roger et al.16 reported HF rates of 378/100,000 in men and 289/100,000 in women. Despite the different HF case definitions, the lack of diagnostic procedures in women may cause a lower rate of HF diagnosis in spite of the HF symptoms. 21 Also, women are known to have more HF with preserved ejection fraction, which suffers from a lack of univocal clinical definition.21,22 Mosterd et al. showed an equal prevalence of HF between the genders in a general population in the Netherlands when comparing the prevalence of clinical HF. However, fewer women with clinical HF had decreased left ventricular function, that is had objective evidence of HF to confirm the diagnosis. 23
The aetiological factors of HF also have gender differences. CHD, hypertension, smoking, obesity and diabetes often precede HF development. Dunlay et al. have shown greatest risk for HF development with CHD and diabetes. 24 However, when taking the prevalence of a risk factor in the general population into consideration, population attributable risks (PAR) for HF were highest for CHD and hypertension. CHD was responsible for 23% of HF in men, and hypertension was most important in women with a PAR of 28%. 24 Similar to this, in our study acute CHD events more commonly preceded HF in men than women, and hypertension was common in both genders. However, the control of hypertension in FINRISK populations has been slightly better in women than in men. 25 As all the putative risk factors for HF were actually more common in men than women in our study, it is possible that women have had more undiagnosed and untreated (clinically silent or atypical) CHD than men, which later on contributed to their high incidence of HF. A higher incident rate of unrecognized MIs has been reported in women than men. 26 Women are often reported to have more atypical symptoms, for example dyspnoea during acute coronary syndrome, 27 and together with lower rate of diagnostic interventions in women, it may be possible that CHD remains undiagnosed, or symptoms are considered to be a result of HF. Women have been reported to have a higher rate of previously diagnosed HF during the time of acute coronary syndrome (ACS). 28
The differences observed in our study in the clinical spectrum of first CVD events may have potential implications for CVD prevention, as the occurrence of first CVD event increases the risk for subsequent CVD events. Patients with stroke or cervicocephalic arterial stenosis have a high rate of asymptomatic CHD, and vice versa.29,30 It is essential to recognize gender differences and differences according to age within gender in order to identify preventive actions and to target specific interventions to each gender. Some important differences in pharmacological prevention have already been shown to exist. Berger et al. have shown in their meta-analysis including over 51,000 women, that acetylsalicylic acid reduced the risk of stroke by 17% in women and had no effect on MI risk, and vice versa in men, in whom acetylsalicylic acid showed a reduction of 32% in MI, but no reduction in stroke events was seen in primary prevention. 31 It might be worth considering whether it would be beneficial to prioritize preventive therapies differently depending on the type of MACE that is most likely to occur first in a particular population group. As to women, for whom the first incident events were stroke and HF, more efforts should be focused on the hypertension because of its stronger association with stroke and HF in women.16,32
We acknowledge some limitations in this study. Firstly, Finland is known to be, according to the WHO MONICA Project, one of the high CVD incidence countries. So our incidence rates and other results may not be directly applicable to lower risk countries. Secondly, we did not differentiate between haemorrhagic and ischaemic stroke; however, our main aim was to assess the overall stroke burden compared with other CVD events. Some bias could be accounted for possible misclassification of incident MACE as a result of individual errors in diagnostic process; however, validation studies have proved good concordance between administrative registers and FINAMI, an MI register using standardized clinical event definition. 13 Moreover, we did not have echocardiography on subjects with HF, which would have given a more detailed overview of gender differences in different HF subtypes, but, again, our aim was to assess the overall HF burden. A validation study of our HF detection method has been published previously, and this reported 99.7% specificity and 48.5% sensitivity. 12 In our study, the mean age of women did not differ from that in men; however, this was a result of stratified sampling and the age limit of 74 years for subjects entering the follow-up.
In conclusion, men had a higher rate of incident MACE, except for HF events which were equal in both genders. Further studies are needed to understand the gender differences in relative burdens as a result of different vascular diseases and their risk factors. Understanding the gender differences in first CVD events may have implications for more focused CVD prevention strategies in different subgroups of patients.
Footnotes
Funding
Supported by grants from the Finnish Foundation for Cardiovascular Research to HRL and VS.
Conflict of interest
The authors declare that there are no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.