
Abstract
Background
For the large population of elderly patients with cardiovascular disease, it is crucial to identify clinically relevant measures of biological age and their contribution to risk. Frailty is denoting decreased physiological reserves and increased vulnerability. We analysed the manner in which the variable frailty is associated with 1-year outcomes for elderly non-ST-segment elevation myocardial infarction (NSTEMI) patients.
Methods and Results
Patients aged 75 years or older, with diagnosed NSTEMI were included at three centres, and clinical data including judgment of frailty were collected prospectively. Frailty was defined according to the Canadian Study of Health and Aging Clinical Frailty Scale. Of 307 patients, 149 (48.5%) were considered frail. By Cox regression analyses, frailty was found to be independently associated with 1-year mortality after adjusting for cardiovascular risk and comorbid conditions (hazard ratio 4.3, 95% CI 2.4–7.8). The time to the first event was significantly shorter for frail patients than for nonfrail (34 days, 95% CI 10–58, p = 0.005).
Conclusions
Frailty is strongly and independently associated with 1-year mortality. The combined use of frailty and comorbidity may constitute an important risk prediction concept in regard to cardiovascular patients with complex needs.
Introduction
The most common diagnostic category for frail elderly patients with complex needs for healthcare is cardiovascular disease.1,2 According to a scientific statement from the American Heart Association Council, the evaluation of comorbidity, frailty, and functional status is crucial when elderly patients with non-ST-segment elevation myocardial infarction (NSTEMI) are treated. 3
Many randomized controlled trials (RCTs)4,5 exclude elderly patients with specified severe comorbidities, which limits the generalizability of the results to patients in routine practice.3,6–9 In particular there is a lack of data regarding the long-term outcomes for these patients. 10 The present guidelines are based primarily on RCTs and systematic reviews, with focus on the treatment of defined organ-specific diagnoses (e.g. NSTEMI). This makes them difficult to apply to individual patients with multiple or severe comorbid conditions. The benefit of interventions can increase for elderly patients due to the increasing age-related cardiovascular risk. On the other hand, these patients are at higher risk of complications (e.g. bleedings).11,12 Adhering to guidelines in caring for elderly patients with many comorbid conditions has been stated to have potentially undesirable consequences, such as side effects from multiple drug regimens. 13
It has been emphasized that clinical priorities vary with life expectancy, since the benefits of preventive interventions accumulate over time whereas the harmful effects of many interventions are immediate. In discussing prognosis with the very elderly, clinicians could use prognostic indexes and take into account individual clinical factors rather than merely population-based averages. 14 Similarly, the Swedish national guidelines for heart disease point out that the patient’s biological age, i.e. biological status and expected length of life rather than the patient’s chronological age, is crucial for decision making. 15 However, there is very limited guidance in regard to how biological age should be estimated and how it influences the benefit-risk ratio of interventions.
Frailty denotes a multidimensional syndrome characterized by decreased physiological reserves and increased vulnerability.16,19–22 Frailty stratification predicts a patient’s need for institutional care and risk of death.17,18 There is not a single accepted operational definition. Frailty instruments have thus far been used and validated mainly in a geriatric context. However, they have also been identified as being potentially relevant for cardiac patients in regard to risk stratification for elderly patients with cardiovascular disease.23–28 In a recent study we found frailty, as well as comorbid conditions quantified by the coronary artery disease (CAD)-specific index, 29 to be independently associated with short-term outcomes for elderly patients with NSTEMI. 30
Our aim in this study is to describe patients aged 75 years or older with NSTEMI, especially in regard to the variables cardiovascular risk, comorbidity, and frailty, and to analyse the manner in which frailty is associated with survival rate and 1-year outcomes for these patients.
Methods
Study sample
Between October 2009 and June 2010, we included evaluable patients aged 75 years or older with diagnosed NSTEMI treated at Linköping University Hospital and the county hospitals in Trollhättan (NÄL-Uddevalla) and Jönköping (Ryhov). The patients received care in one or more of the following hospital departments: cardiology, acute medicine, geriatrics, and other areas of internal medicine.
This is an observational study focusing on a study instrument (Clinical Frailty Scale) that has not been used previously to predict risk of outcomes for NSTEMI patients. It was therefore difficult to perform a power analysis regarding outcomes for frail vs. nonfrail elderly patients. However, before the study we tried to estimate the expected percentages of outcome events (1 month 30 ) for frail and nonfrail NSTEMI patients aged 75 years or older. We approximated these two groups of patients with the percentages of outcome events of the GRACE (30%) and VIGOUR (15%) populations, aged 75 years or older, respectively. 3 Given this rough estimation, and a chosen level of significance of 5% and a power of 80%, approximately 260 patients should be included.
Data collection and variable selection
Patients aged 75 years or older with diagnosed NSTEMI according to their attending physicians were consecutively included.
The Canadian Study of Health and Aging (CSHA) Clinical Frailty Scale (CFS)
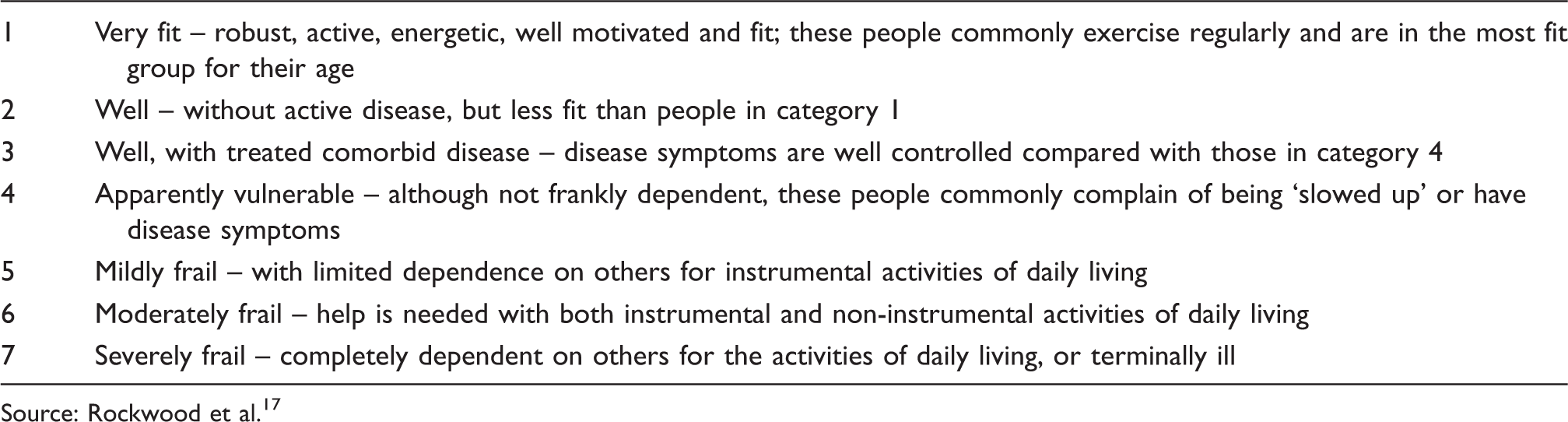
Source: Rockwood et al. 17
If the inclusion criteria were fulfilled and the patient had given informed consent, evaluation of the patient’s degree of frailty was based on bedside judgment regarding frailty and other clinical information, including the records in the patient file. If a patient was unable to give informed consent (without manifesting unwillingness to participate), but there was sufficient clinical information including the records in the patient file, evaluation of the patient’s degree of frailty was based on this information only (i.e. without bedside judgment). A few patients who fulfilled the inclusion criteria while evidently not fulfilling any of the exclusion criteria were for some reason not evaluated during the hospital care episode. For these cases the evaluation of frailty was based on the records in the patient file and/or information obtained via a telephone call to the patient, after the patient had provided written consent via a letter. After permission from the hospital board was received, a computer-based screening of the hospital’s diagnosis register was performed intermittently to detect potentially eligible but already discharged NSTEMI patients.
There were two exclusion criteria: (1) if the patient manifested unwillingness to participate or (2) if the patient was not evaluable because of communication problems and insufficient clinical information to enable a judgment of frailty.
The CAD-specific index
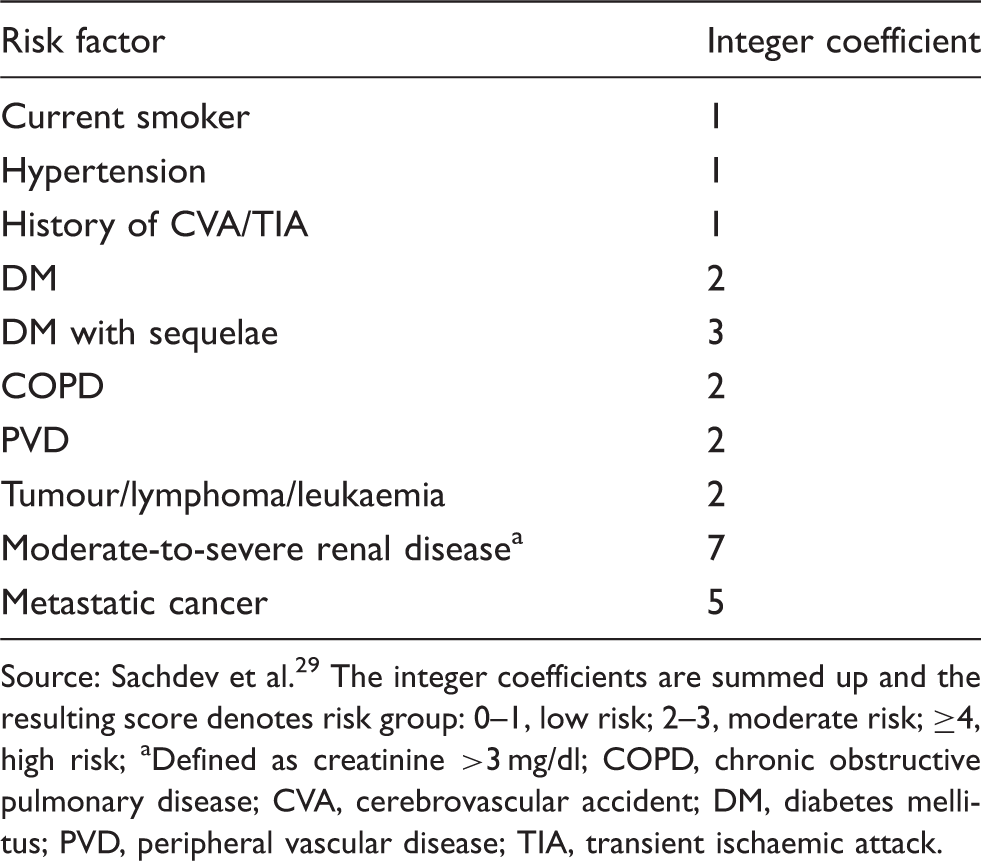
Source: Sachdev et al. 29 The integer coefficients are summed up and the resulting score denotes risk group: 0–1, low risk; 2–3, moderate risk; ≥4, high risk
Defined as creatinine >3 mg/dl
COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; DM, diabetes mellitus; PVD, peripheral vascular disease; TIA, transient ischaemic attack.
Follow up was done 1 month (first follow up) and 1 year (second follow up) after the time of inclusion via the patient files and the Causes of Death Register. The Linköping Academic Research Center (LARC) group at Linköping University Hospital performed study monitoring four times from study start until the second follow up.
Clinical outcomes
The primary outcome in this study was 1-year mortality. The 1-year composite outcome was the composite of death from any cause, myocardial reinfarction, revascularization due to ischaemia, hospitalization for any cause, major bleeding, stroke/transient ischaemic attack, and need for dialysis up to 1 year after inclusion. We studied time to first event according to the 1-year composite outcome.
A bleeding was defined as major if one of the following was present: intracranial bleeding, retroperitoneal bleeding, blood transfusion, haemoglobin decrease >3 g/dl with overt cause, or haemoglobin decrease >4 g/dl without overt source. 34 Stroke and transient ischaemic attack were defined according to a consensus statement. 35
Myocardial infarction (MI), including periprocedural MI, was classified according to the Joint European Society of Cardiology, American College of Cardiology Foundation, American Heart Association, and World Heart Federation Task Force consensus statement. 36 The events were recorded by the study nurses and reviewed by the study investigators.
Statistical analysis
Statistical analysis was performed via SPSS version 19.0 and SAS version 9.1.3. Categorical data were analysed by use of the Fisher Exact test or the chi-squared test, and continuous data were compared with the Student t-test. The association of frailty with the primary composite outcome was examined by Cox regression models 37 adjusted for relevant prognostic variables [age, sex, previous myocardial infarction, ejection fraction, presence or absence of diabetes mellitus, cardiovascular risk, classification of myocardial infarction, and comorbidities (i.e. the score according to the CAD index)].
All two-way interactions between frailty and the other independent variables were tested to validate the findings of the regression model. The regression model including possible statistically significant interactions was evaluated with a likelihood ratio test. All independent variables included in the models were analysed for possible collinearity with a variance inflation factor test. Variance inflation factor values of >2.5 were considered to indicate collinearity. 38
We studied the time between entry into the study and a subsequent event by the use of survival analysis. To describe the survival times and the event-free times of the patients we used Kaplan–Meier curves.
Ethics
The study was conducted in accordance with the Declaration of Helsinki and the latest version of the Good Clinical Practice Guidelines. The study was undertaken after the protocol and its appendices had received full approval from the Independent Ethical Review Board in Linköping. The main ethical issue was how to get a proper informed consent from these elderly patients.
Results
Baseline characteristics
Between October 2009 and June 2010, we included 307 evaluable patients aged 75 years or older with diagnosed NSTEMI. Of these 307 patients, 149 (48.5%) were considered frail according to the study instrument (5–7 on the scale), and 75 (24.1%) were considered moderately or severely frail (6–7 on the scale).
Baseline patient characteristics
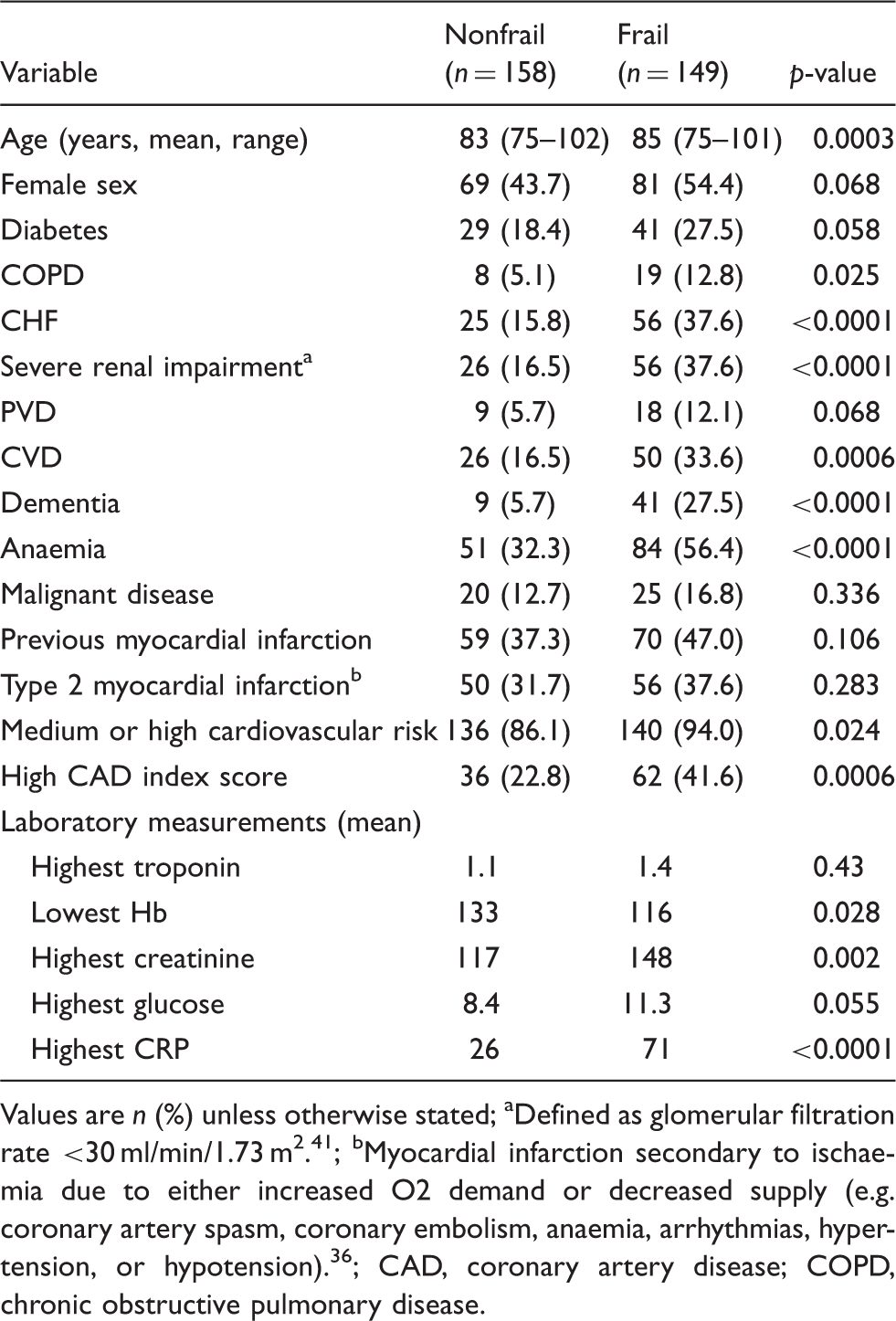
Values are n (%) unless otherwise stated
Defined as glomerular filtration rate <30 ml/min/1.73 m2. 41
Myocardial infarction secondary to ischaemia due to either increased O2 demand or decreased supply (e.g. coronary artery spasm, coronary embolism, anaemia, arrhythmias, hypertension, or hypotension). 36
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease.
Outcomes
Unadjusted 1-year outcomes
Of 307 patients, 231 manifested one or more event (Table 4). Of these 231 patients, 198 (86%) manifested rehospitalization as the first event. Of these 198 rehospitalizations, 99 were due to a cardiovascular cause and 99 were due to a noncardiovascular cause. Among frail patients, mortality was more prevalent than among nonfrail patients (p < 0.0001; Table 4). A survival analysis is reported in Figure 1.
Unadjusted survival analysis. Unadjusted outcomes at 1 year Values are n (%). One-year composite outcome denotes the composite of death from any cause, myocardial reinfarction, revascularization due to ischaemia, hospitalization for any cause, major bleeding, stroke/TIA, and need for dialysis up to one 1 after inclusion TIA, transient ischaemic attack.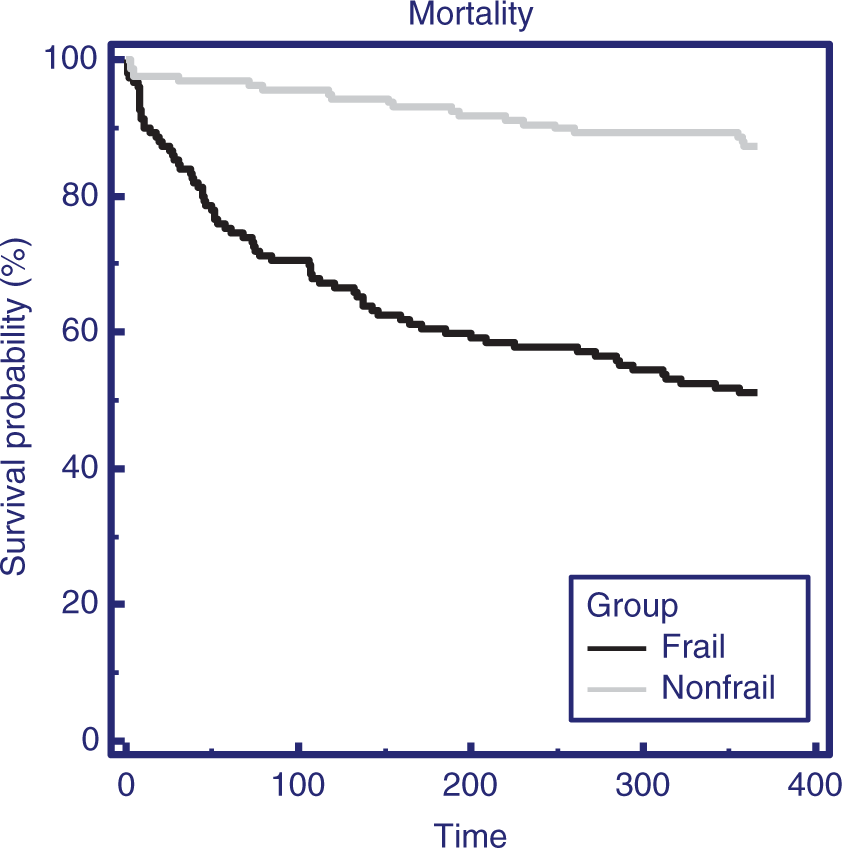
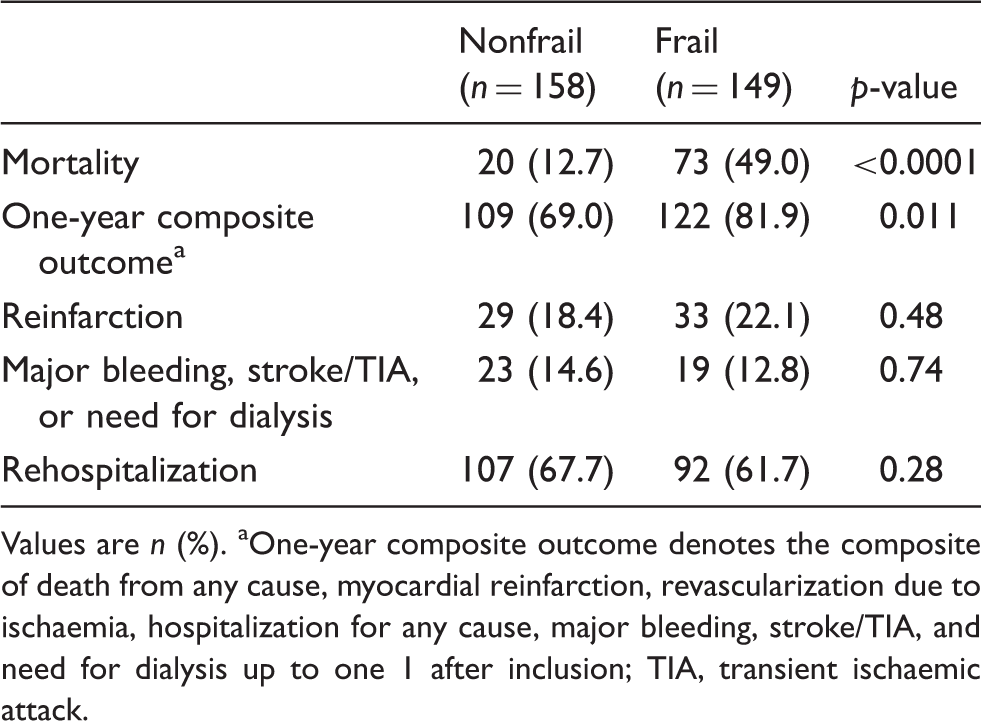
Frailty was significantly associated with increased fulfilment of the 1-year composite outcome (nonfrail n = 109, 69.0%; frail n = 122, 81.9%; p = 0.01). The main driver of the higher event rate among the frail patients was the higher mortality rate (frail 73, 49.0%; nonfrail 20, 12.7%; p < 0.0001). Of the frail patients, 49 were judged to have died from a cardiovascular cause, 16 died from a noncardiovascular cause, and in eight cases the cause of death was uncertain. Of the nonfrail patients, 18 were judged to have died from a cardiovascular cause and two patients died from a noncardiovascular cause.
Frail patients were less likely to be treated in intensive cardiac care units than nonfrail patients (nonfrail n = 85, 53.8%; frail n = 52, 34.9%; p < 0.001) during the index episode of care. Furthermore, frail patients were less likely to undergo coronary angiography than nonfrail patients (nonfrail n = 73, 46.2%; frail n = 23, 15.4%; p < 0.0001). Ninety-six of 307 patients underwent coronary angiography. Of these patients, four were moderately or severely frail, 19 were mildly frail, and 73 were nonfrail (Figure 2). Patients with severe comorbidity were less likely to undergo coronary angiography, whereas neither the cardiovascular risk score nor the CAD-specific index predicted the performance of coronary angiography.
The proportion of patients in each frailty stage not undergoing coronary angiography during the index episode of care.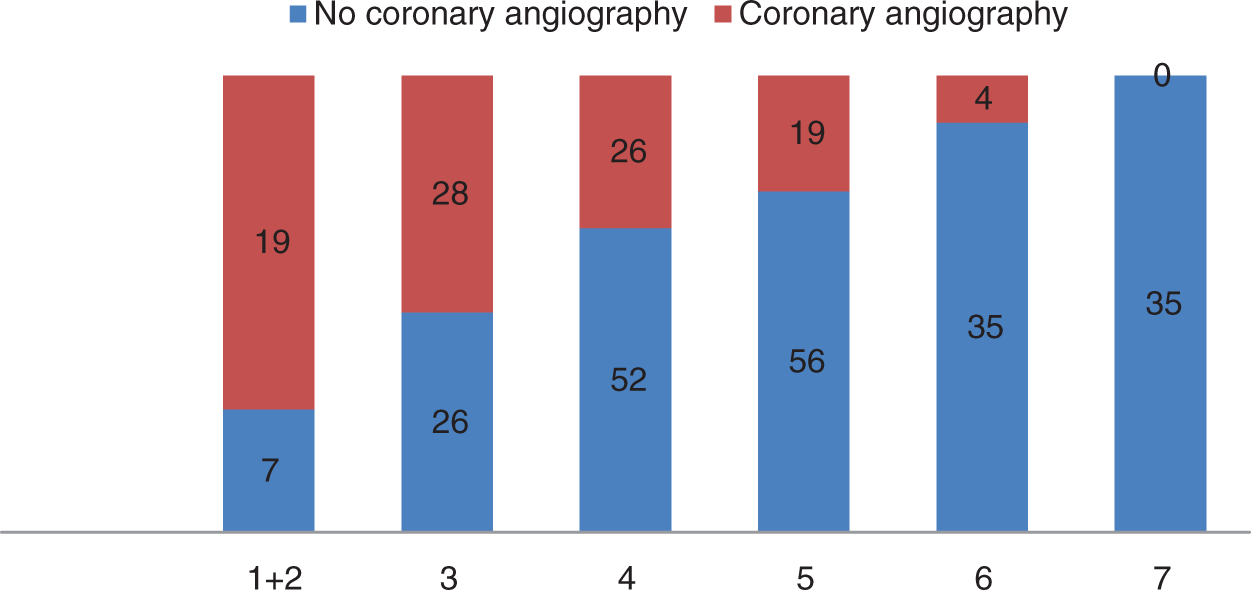
Adjusted 1-year outcomes
Adjusted mortality
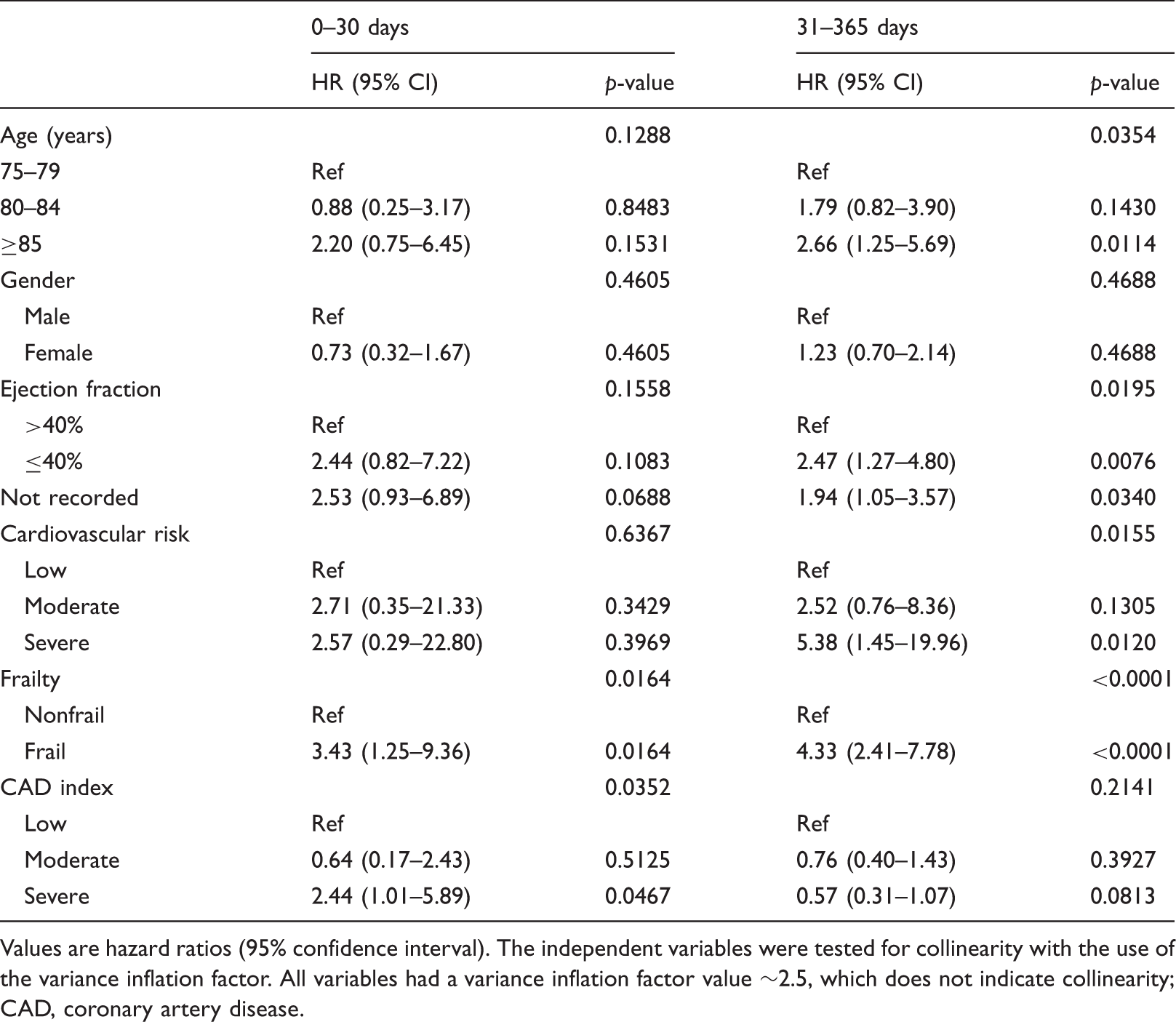
Values are hazard ratios (95% confidence interval). The independent variables were tested for collinearity with the use of the variance inflation factor. All variables had a variance inflation factor value ∼2.5, which does not indicate collinearity
CAD, coronary artery disease.
The CAD index score was not associated with 1-year mortality. No collinearity was indicated between the independent variables, and there was no interaction that influenced the results. No variable was independently associated with the 1-year composite outcome using Cox regression analyses (hazard ratio 1.3, 95% CI 0.87–1.8; p = 0.22). The time to the first event was significantly shorter for frail patients than for nonfrail (34 days, 95% CI 10–58; p = 0.005).
Discussion
Our study demonstrates frailty to be independently and strongly associated with 1-year mortality for elderly NSTEMI patients. In this study, nearly half of the population was frail. Frail patients were slightly older than nonfrail patients, and they manifested an increased burden of disease. Other variables that were independently associated with 1-year mortality were age, cardiovascular risk and ejection fraction. Time to the first event was significantly shorter for frail patients than for nonfrail patients.
Our study is a multicentre, prospective observational trial with very few exclusion criteria. Since our aim was to describe a representative sample of elderly NSTEMI patients treated in clinical practice, including patients not treated in coronary care units and patients with secondary coronary ischaemia 36 (i.e. not only coronary care unit patients), the study design seems appropriate. In an earlier publication, frailty was reported to be independently associated with short-term clinical outcomes for elderly NSTEMI patients, including 1-month mortality. 30 To our knowledge, this is the first study to demonstrate frailty as strongly and independently associated with 1-year mortality as well. We did this using an easily applied clinical measure of frailty, which was evaluated before the start of the study and was shown to have very good interrater reliability. The study was carefully monitored at four time points.
The trial did not have enough statistical power to properly analyse the manner in which frailty influences the benefit of coronary angiography and the possible invasive treatment that can follow. Because follow up was done with the use of patient files and the Causes of Death Register, quality of life and burden of symptoms were not measured explicitly. However, rehospitalization for cardiovascular causes indirectly indicates the burden of symptoms.
In most frailty studies, a geriatric patient cohort has been studied rather than acute heart patients. In these studies, frailty has been reported to be associated with long-term mortality, hospitalization, and institutionalization for geriatric patients.18,19 In the 1-month follow up of this study, it was indicated that frailty is independently associated with short-term outcomes for elderly NSTEMI patients. 30 Our present study including the 1-year follow up shows that frailty is independently and strongly associated with 1-year mortality. Furthermore, no other independent variable, with the exception of ejection fraction, cardiovascular risk and age, was associated with 1-year mortality in adjusted analysis with the use of Cox regression analysis, which emphasizes the predictive strength of frailty.
No variable was significantly and independently associated with the 1-year composite outcome, which may be an expected finding since as many as 231 of 307 patients had at least one event. However, the time to first event was significantly shorter for frail patients than for nonfrail patients. Rehospitalization was by far the most common event.
The Canadian Study of Health and Aging Clinical Frailty Scale is based on clinical judgment and is relatively easily applied in a clinical context. There may be other measures of frailty that are more sensitive, but that are also more time consuming and costly to administer. In our study, almost half of the population was frail. Thirty per cent of a community-dwelling population of octogenarians has been estimated to be frail. More relevant in comparison with our study, the prevalence of frailty in an elderly population requiring cardiac care ranges from 27 to 63%, depending on the classification scheme. 39
Despite overlap between frailty and comorbidity, the distinction between the concepts has been stressed in other studies.23,40 In earlier studies including patients with CAD and using the same CAD-specific index, 16 and 24% of the patients, respectively, presented with high scores.10,24 In regard to the burden of comorbidity in our study, 32% of the patients presented with high CAD-specific index scores, which is not surprising because our study included older patients than in earlier studies. This may be one of the causes of the finding that the CAD-specific index score was not associated with 1-year mortality.
Frail patients were less likely to be treated in intensive cardiac care units during the index episode of care than nonfrail patients, and, similarly, they were less likely to undergo coronary angiography. Frailty and severe comorbidity were strong negative predictors for performance of coronary angiography, whereas degree of cardiovascular risk did not influence the use of this measure. Clinical decision making for elderly NSTEMI patients seems to be based on factors other than the estimation of cardiovascular risk. This observation could be compared with recommendations in Swedish, European, and American heart guidelines, which rely primarily on cardiovascular risk. There are possible alternative interpretations of this finding. One could argue that if frail patients indeed benefit from interventions, more of these patients should undergo coronary angiography to improve outcomes. On the contrary, one could argue that frail NSTEMI patients should be treated in coronary care units to a lesser extent than today because they are not judged to benefit from specific coronary care. In fact, as many as 78.5% of the frail patients manifested one or more severe comorbid conditions (e.g. acute bleeding, severe renal insufficiency, severe anaemia, or severe dementia). Many of these conditions could be considered potential contraindications to invasive procedures. Clearly, this matter needs further evaluation. However, it would probably be questionable from an ethical viewpoint to perform an interventional study on the frailest patients.
Clinical priorities vary with life expectancy, since the benefits of preventive interventions accumulate over time whereas the harmful effects of many interventions are immediate. For very elderly patients with cardiovascular disease, it is therefore important to identify clinically and individually relevant measures of biological age and their contribution to risk and life expectancy. The use of frailty may constitute an important and robust risk prediction concept in regard to cardiovascular patients with complex needs.
In conclusion, our study indicates that frailty is independently and strongly associated with 1-year mortality for elderly NSTEMI patients. In the 1-month follow up frailty was also independently associated with short-term outcomes including 1-month mortality, which emphasizes the concept’s potential robustness in predicting adverse events. Other studies (e.g. Singh et al. 26 ) have pointed in the same direction.
We suggest that frailty should be considered in clinical decision making as well as in registers, clinical studies, and policy documents. Furthermore, there is a need for prospective studies with few exclusion criteria (RCTs, if possible from an ethical viewpoint) to study the benefit of interventions for frail cardiovascular patients. We believe that registries should be adapted for elderly NSTEMI patients including relevant measures (i.e. frailty) and relevant comorbidities (i.e. dementia). In clinical practice, individual clinical judgment and careful evaluation of initiated interventions are of great importance for these patients.
Footnotes
Funding
This study was supported by the Medical Research Council of southeast Sweden.
Conflict of interest
The authors declare that there is no conflict of interest.
Clinical trial registration
Unique identifier: NCT01049997.
Acknowledgements
We wish to thank Elisabeth Logander, Annica Koch, Niclas Jovander, and Maria Skön for their valuable contributions. We would like to acknowledge Lena Hector for her administrative assistance and LARC for monitoring the data.