
Abstract
Background
It is currently not known whether dairy food influences the risk of cardiovascular disease or diabetes. This study evaluates effects of changing dairy intake on cardio-metabolic risk factors.
Methods
180 healthy volunteers were randomised to increase, reduce or not change their dairy intake for 1 month in response to dietary advice. Body weight, waist circumference, blood pressure, fasting plasma lipids, insulin resistance and C-reactive protein (CRP) were measured at baseline and after 1 month and compared by dietary group.
Results
176 (98%) subjects completed the study. Average change in self-reported dairy fat intake for increased dairy food was +0.9 SD 1.1 g/day (+71%), no change was −2.1 SD 0.4 g/day (−15%) and decreased dairy food was −10.8 SD 1.2 g/day (−77%) respectively. There was no statistically significant change in LDL or HDL cholesterol, triglycerides, systolic or diastolic blood pressure, C-reactive protein, glucose or insulin with 95% CI standard mean differences <0.2 for all and CRP <0.3. There was a small increase in weight (+0.4 kg, SD 3.1) in those asked to increase dairy food.
Conclusions
In healthy volunteers, dietary advice to change dairy intake for 1 month did not have a clinically significant effect on cardio-metabolic risk factors. These observations suggest that dairy food can be included as part of a normal healthy diet without increasing cardio-metabolic risk.
Trial registration number: ACTRN12612000574842
Keywords
Background
The influence of dairy food on the risk of cardiovascular disease and diabetes is currently uncertain. For many years reduction in high-fat dairy food was recommended to decrease saturated fat intake, 1,2 but some more recent guidelines place less emphasis on the importance of a low-fat diet. 3,4 Clearer guidance is important, particularly given the high and increasing prevalence of cardiovascular disease and diabetes in most countries, and the increasing global consumption of dairy food. 5 Food pyramids recommend consumption of three to four servings of dairy food per day, 2,6 but other major guidelines 3,4,7,8 recommend substituting dairy food with non-animal sources of protein.
Most evidence on the relationship between dairy and cardio-metabolic risk comes from observational studies. 9 –13 A major concern has been that dairy is a source of both saturated fats and trans fats, which are thought to increase cardiovascular risk. 14 –16 However, dairy has not been shown to have adverse effects on lipids 17,18 and a number of studies suggest that it could have beneficial effects on blood pressure (BP), 10 –12,19,20 weight 10,13,20,21 and insulin resistance. 10,13,20 –22 Dairy is a complex food and an important source of protein, vitamin D, potassium, phosphorus, magnesium and calcium, 23 and could potentially improve cardio-metabolic risk by a number of mechanisms. Small experimental studies suggest that dietary calcium induces thermogenesis and weight loss, 24,25 magnesium reduces blood pressure 23 and vitamin D improves endothelial function. 26 There is evidence that the negative effects of saturated fats could be offset by the health benefits of conjugated linoleic acid. 27,28
Data from randomised clinical trials are currently limited to small (n < 100) narrowly focused studies, 18,29 –32 or larger studies which are confounded by multiple interventions. 23 More evidence on the effects of changing dairy food intake on overall cardio-metabolic risk from randomized trials in real world settings is needed to guide recommendations on dairy food consumption as part of a healthy diet. Evidence from previous studies show that effects on BP, 23 lipids 33,34 and weight 18 are apparent in the first month, and that compliance over long periods is difficult. We therefore undertook a randomized clinical trial comparing the effects of increasing, decreasing or not changing daily dairy food intake for 1 month on cardio-metabolic risk factors in 180 healthy volunteers.
Methods
Study population
Healthy volunteers living in Auckland, New Zealand regularly consuming dairy, and who were willing to modify dairy intake for 1 month, were recruited by advertisement from February 2011 to September 2011. Exclusion criteria included inability to tolerate dairy food, known diabetes, cardiovascular disease, inflammatory conditions, currently taking any lipid or glucose modifying medication and age ≤18 years. Ethics approval was obtained from the Northern X Ethics Committee and all participants provided written informed consent. One-hundred and eighty participants were randomised into the study.
Study procedures
After written consent was obtained, height, weight and waist circumference were measured, a 3-day food frequency questionnaire was completed and a fasting blood sample collected. Participants were then randomised by a computer-generated randomisation algorithm to one of three possible arms; increased dairy, reduced dairy or no change for 1 month. Participants then met with a study coordinator with experience in dietary advice for 15 minutes. Dietary sheets with advice on how to increase or decrease dairy were given to participants. Participants randomised to increase dairy were asked to consume an extra two to three servings per day, and to change to high-fat milk and dairy solids which are high in fat. Participants randomised to decreased dairy were asked to eliminate all possible sources of dairy. Alternatives such as rice milk or soya were suggested. A follow-up assessment was arranged for 1 month at which time the above assessments were repeated. Subjects were phoned after 2 weeks to encourage dietary compliance.
Sitting BP was measured in the right arm after sitting for 5 minutes. Waist and hip circumference were measured according to the International Standards for Anthropometric Assessment, with the subject in a relaxed standing position with arms folded across the chest. Waist circumference was measured at the halfway mark between the iliac crest and the bottom rib; hip circumference was measured at the level of the greater trochanter. Weight was measured on a calibrated digital scale.
Fasting blood tests were taken on all participants at baseline and after 1 month. For blood glucose and lipids, blood was taken in a heparin tube and analysed within 60 minutes using a standard Roche Modular analyser. The following methods were used: glucose: glucose oxidase; total cholesterol (TC): cholesterol oxidase; HDL-c: PEG-modified cholesterol esterase and oxidase, with dextran sulphate; lipoprotein lipase. Low density lipoprotein cholesterol (LDL-c) was calculated using the Friedwald equation. To measure insulin, blood was taken in a plain tube. Serum was separated in a 4° centrifuge and stored at −70℃ until analysis. Serum insulin was measured by chemiluminescence immunoassay using an Abbott Architect analyser. The homeostatic model assessment (HOMA) was calculated from fasting glucose and insulin levels using a standard formula. 35
To confirm changes in dairy intake on different diets, plasma levels of the phospholipids 15:0 pentadecanoic acid and 17:0 heptadecanoic acid or margaric acid, which are known to be derived from dairy food, 36 were measured from blood samples taken in ethylene-diamine-tetra acetic acid tubes. Phospholipids were extracted with AR Methanol and fatty acid methyl esters formed by trans methylation. 37 Serum phospholipid fatty acid composition was assessed by gas chromatography (Hewlett Packard 6890 Gas Chromatograph with a SGE BPX70 column and a Flame Ionisation Detector), with levels expressed as the percentage of the total weight of the fatty acids.
The National Cancer Institute Diet History Questionnaire, 38 a validated food frequency questionnaire was used to assess all dairy and red meat intake during the preceding 3 days at baseline and 1 month. Questions on dairy and meat intakes were unchanged but those related to alcohol, fruit, vegetables, grains and sweeteners were not included. This shortened FFQ was not separately validated. Serving sizes were defined using the United States Department of Agriculture criteria. 39 For example, one serving size was equivalent to 250 ml 3% milk, 250 ml yogurt, 500 ml 1.5% milk or 1/3 cup cheddar cheese. The total dairy fat content ingested in g/day was calculated based on the reported intakes of each food, and the fat content from manufacturers’ labels. 40
Statistical analysis
Demographic data, baseline and 1-month visit measurements and change in these measurements between baseline and 1 month were summarized as mean and standard deviation or frequency and percentage as appropriate. C-reactive protein was log transformed. Sixty in each group was estimated to give 80% power to detect a treatment difference with a two-sided 0.05 significance level, if the true difference in BP between treatments is 3.5 mmHg with a SD of 7.
Baseline characteristics and scores were compared across the three arms using the analysis of variance (ANOVA). Differences in measurements between the arms at 1 month were also assessed using analysis of covariance (ANCOVA) adjusting for the baseline scores. All p-values resulted from two-sided tests. We adjusted for change in waist circumference and weight to assess effects on HOMA, BP, TC, HDL-c, LDL-c, HDL/LDL Ratio and total triglyceride (TG). The effect of each intervention for all variables was summarized as standardized mean difference (SMD). Statistical analyses were performed with SAS software version 9.3 (SAS Institute, Cary, NC).
Results
One-hundred and seventy-six of 180 randomised participants completed the study (Figure 1). The mean age of the population was 47 years (IQR 38–55), and 70% of the participants were female. Participants had normal weight with an average body mass index of 24.5 (SD 4.0), and were normotensive with an average BP 110/70 (SD10/8) mmHg. Nine participants met the criteria for the metabolic syndrome according to the American Heart association criteria.
41
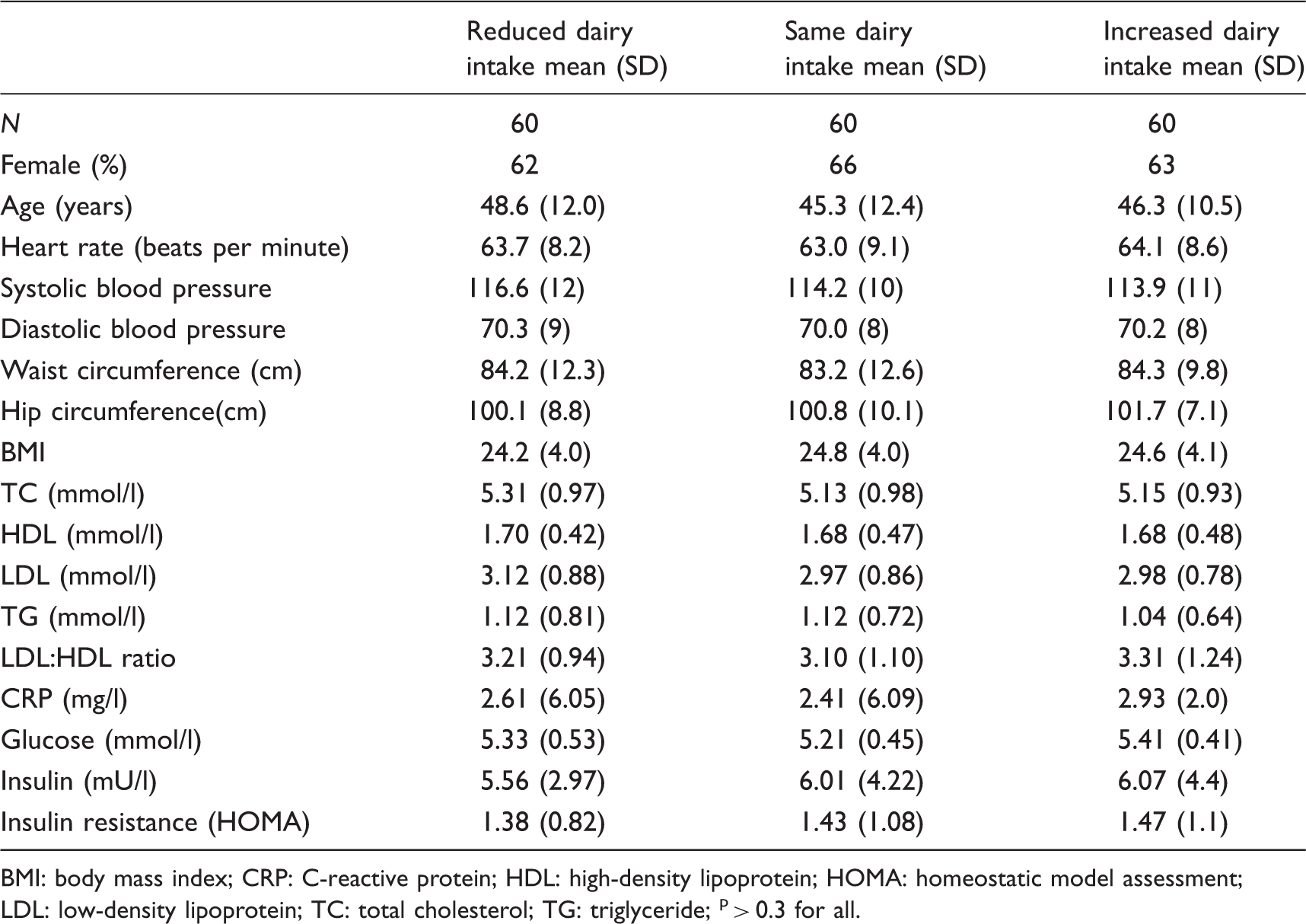
There were no significant differences in baseline characteristics by dietary group (Table 1).
Study flow chart. Baseline characteristics according to randomisation BMI: body mass index; CRP: C-reactive protein; HDL: high-density lipoprotein; HOMA: homeostatic model assessment; LDL: low-density lipoprotein; TC: total cholesterol; TG: triglyceride > 0.3 for all.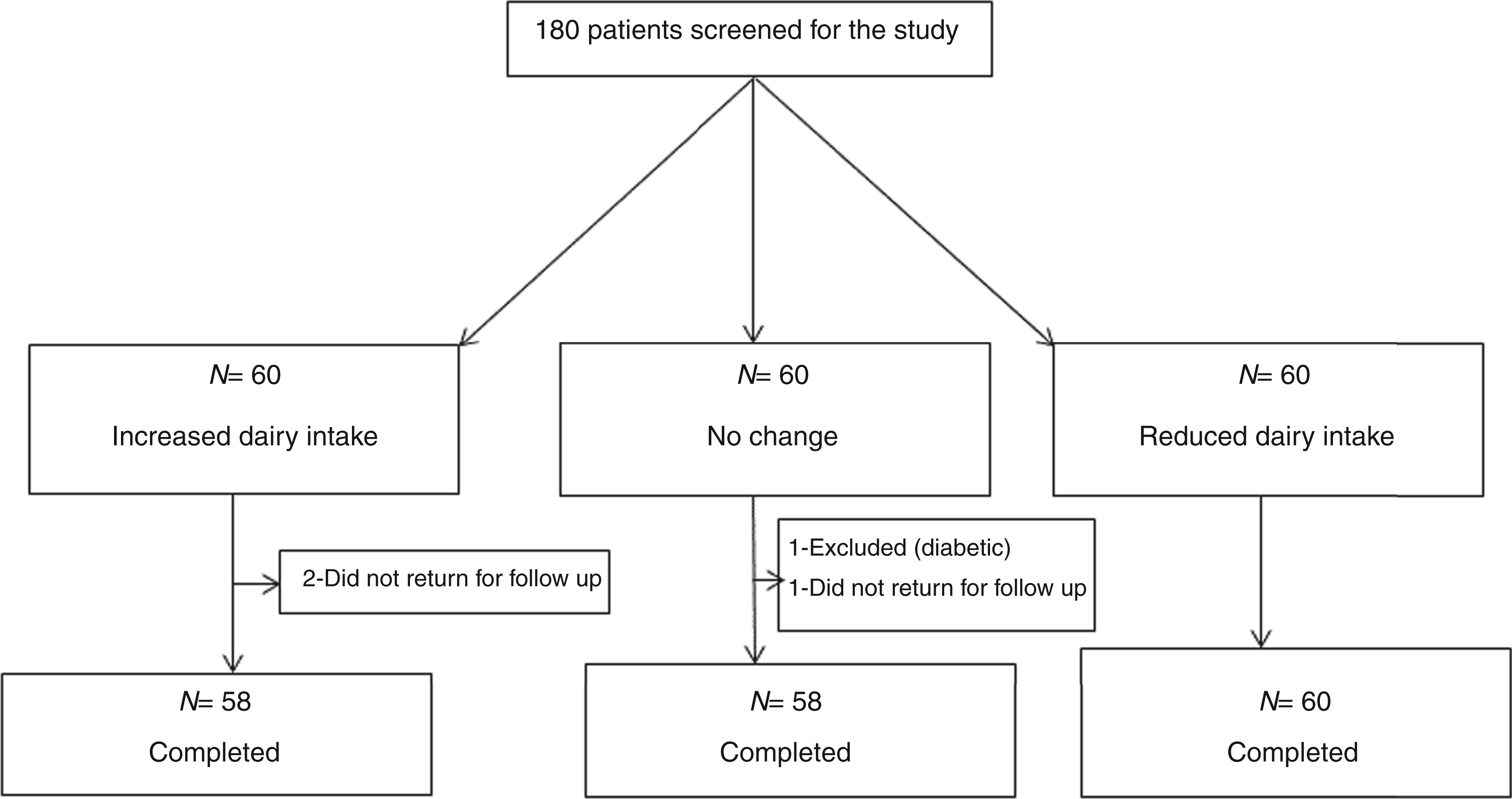
Dairy intake and plasma fatty acid levels at baseline and 1 month from the food frequency questionnaire for each randomised group
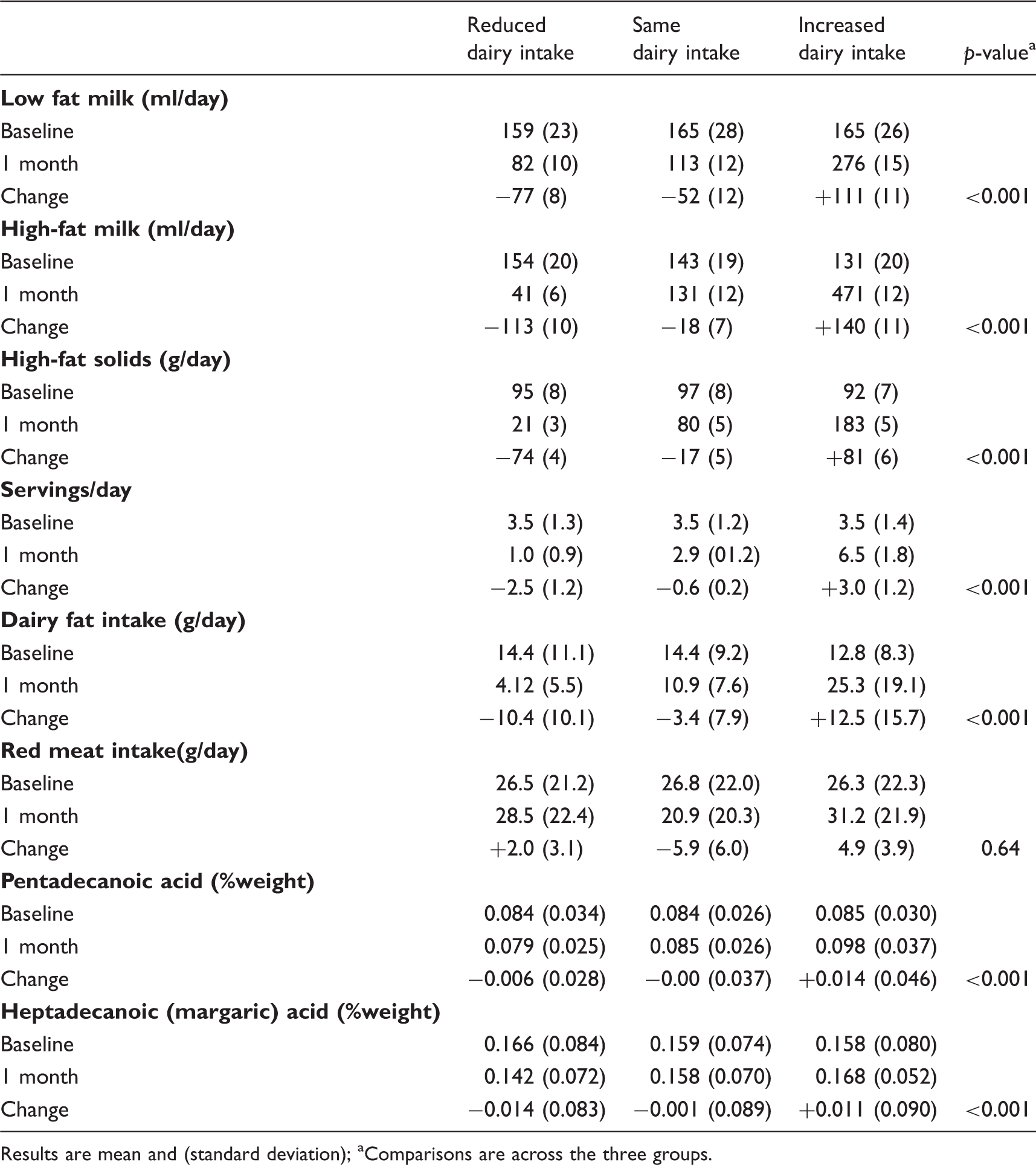
Results are mean and (standard deviation)
Comparisons are across the three groups.
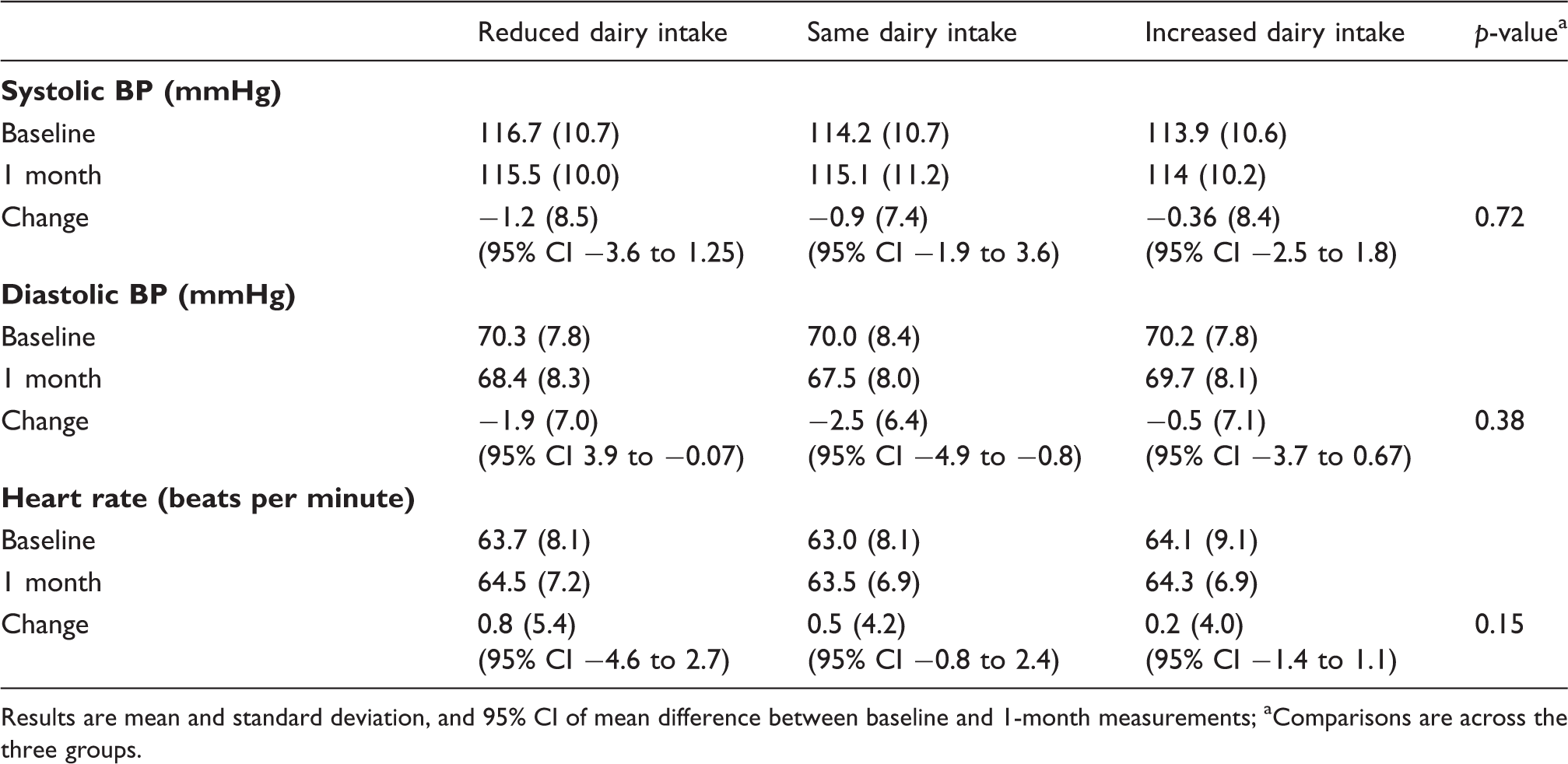
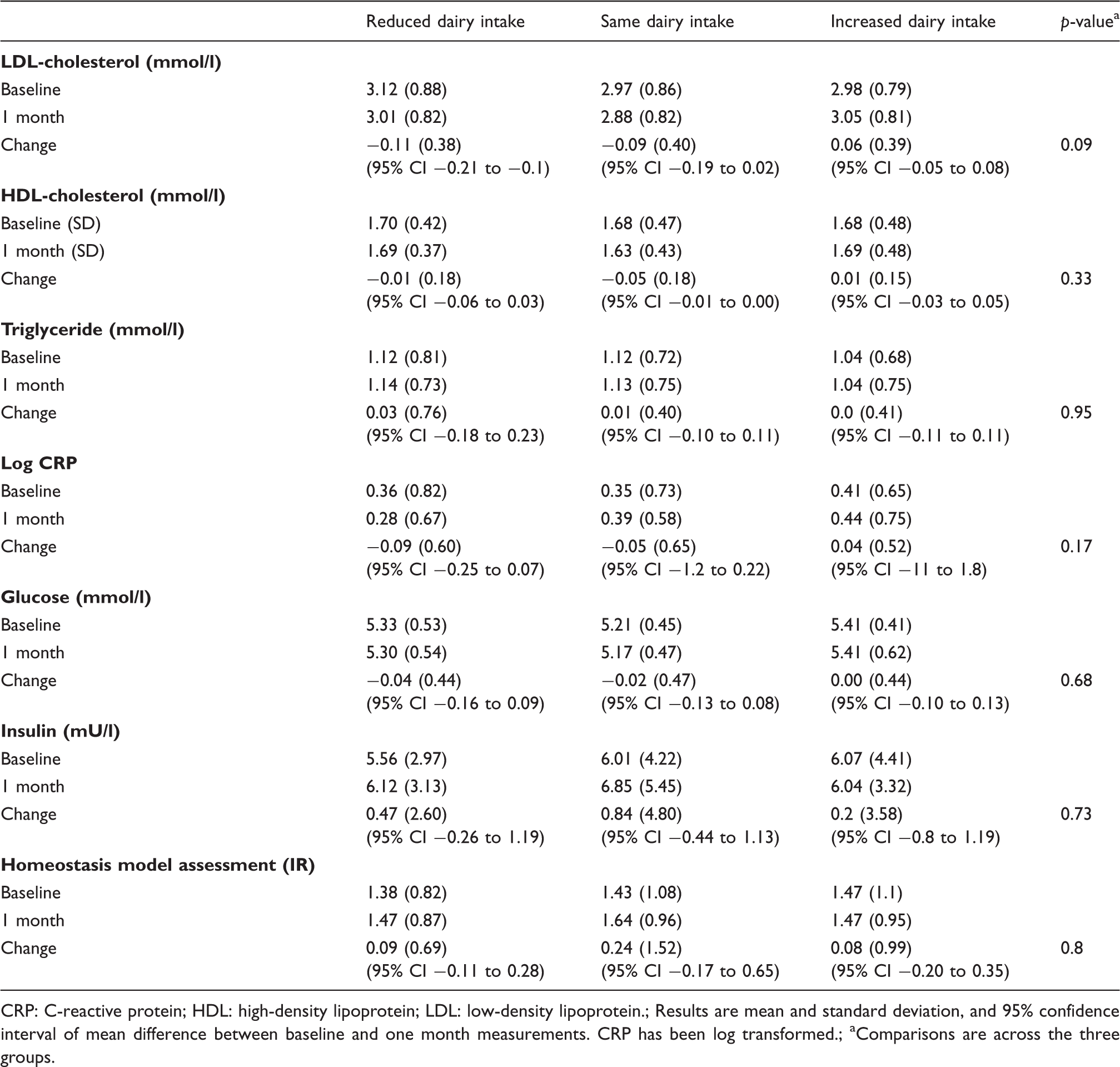
There was no clinically or statistically significant change in systolic BP, diastolic BP, heart rate (Table 3), low or high density lipoprotein, triglycerides, C-reactive protein, glucose, insulin and insulin resistance (HOMA) (Table 4) at 1 month between the three randomised groups (Table 4). For all comparisons, the 95% CI excluded effect sizes of 20%,
42
except for HOMA and CRP where the 95% CI were 30% (Figure 2).
The effect of dairy on individual cardio-metabolic risk factors, presented as effect size with 95% CI. BP: blood pressure; CRP: C-reactive protein; HDL-c: high density lipoprotein cholesterol; HOMA: homeostatic model assessment; LDL-c: low-density lipoprotein cholesterol. The effects of changing dairy on blood pressure (BP) and heart rate Results are mean and standard deviation, and 95% CI of mean difference between baseline and 1-month measurements Comparisons are across the three groups. Effects of changing dairy on lipids, C - reactive protein and insulin resistance as calculated using HOMA model CRP: C-reactive protein; HDL: high-density lipoprotein; LDL: low-density lipoprotein. Results are mean and standard deviation, and 95% confidence interval of mean difference between baseline and one month measurements. CRP has been log transformed. Comparisons are across the three groups.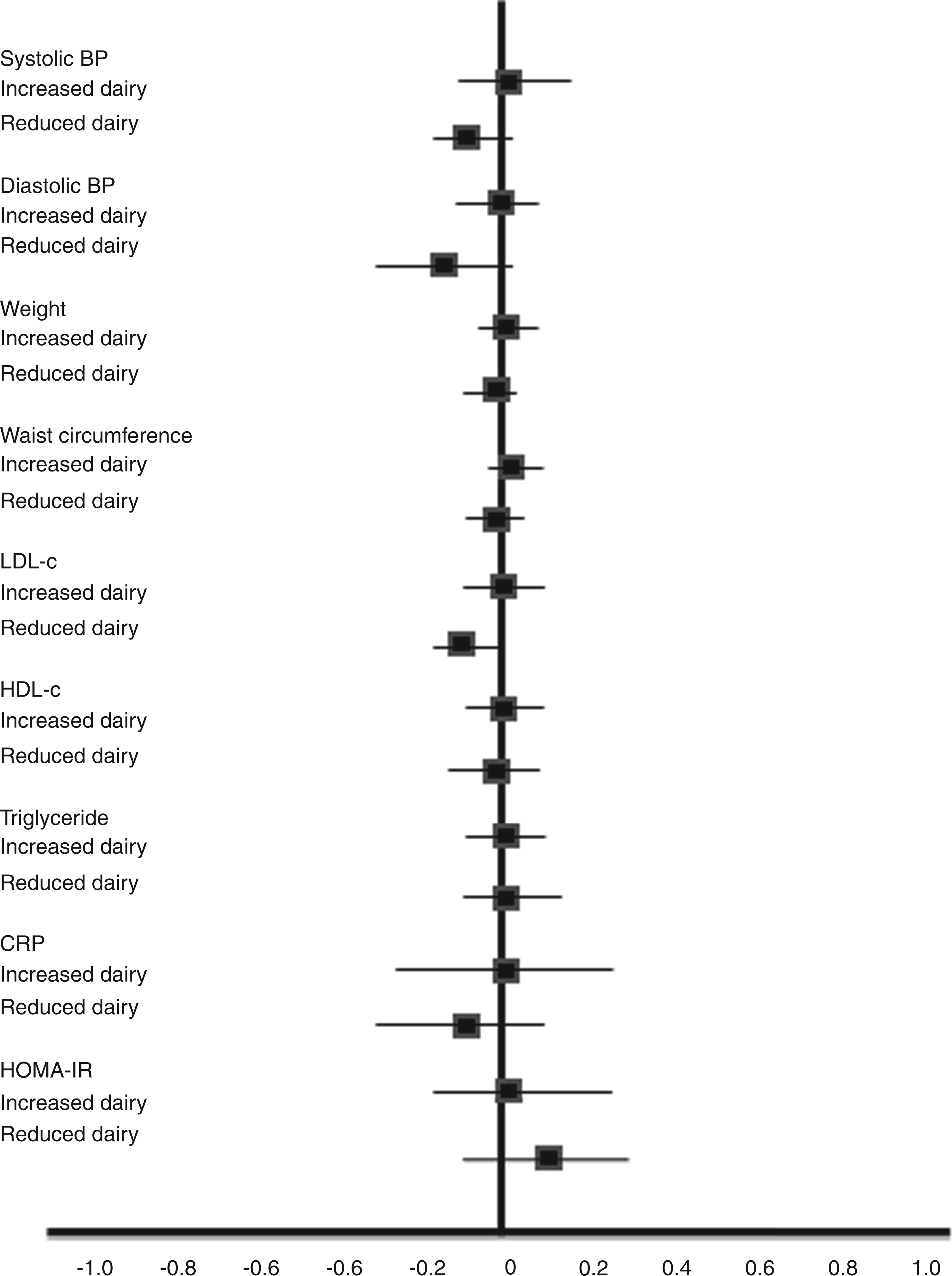
Effects of changing dairy on weight, waist and hip circumference
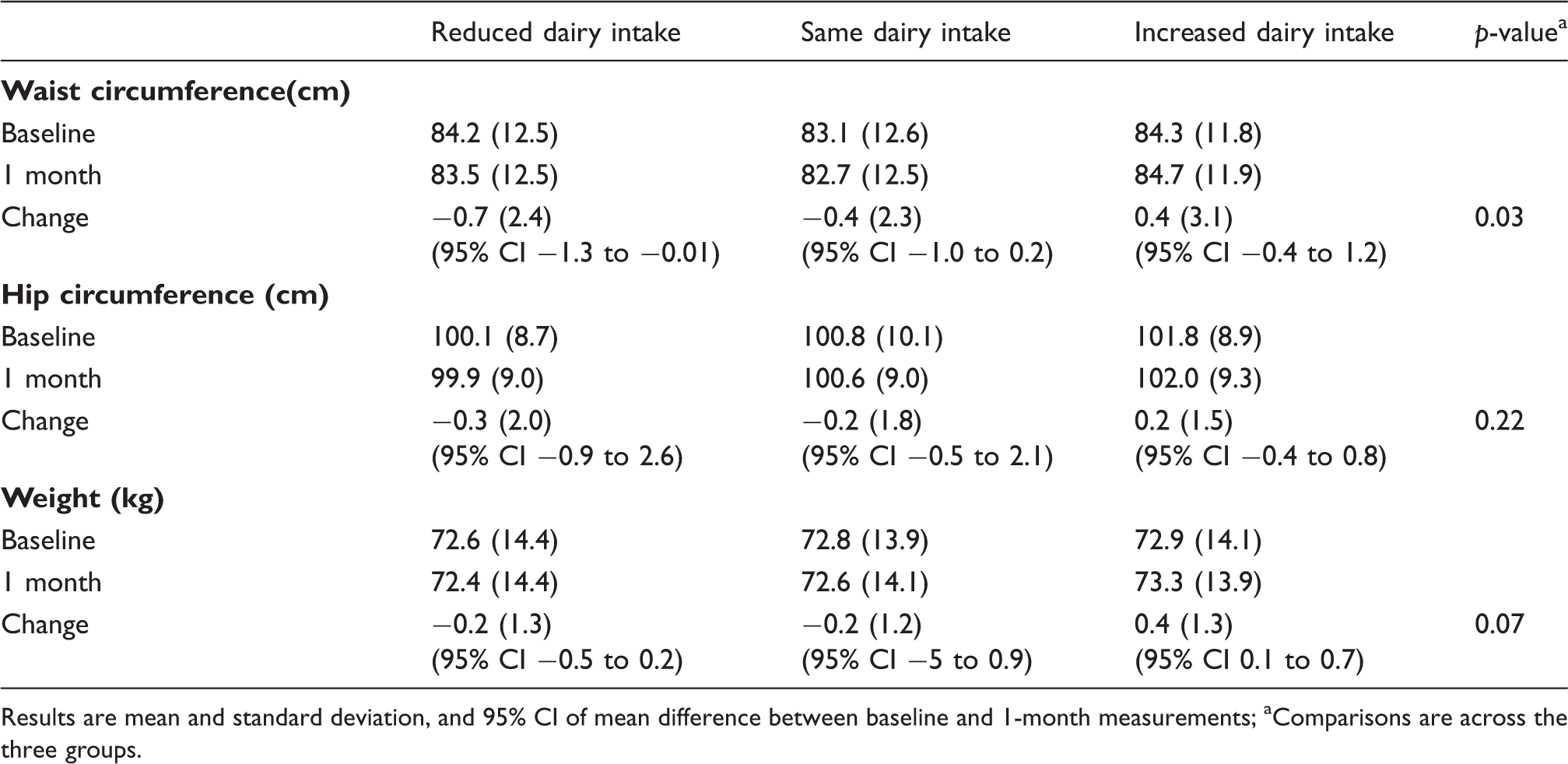
Results are mean and standard deviation, and 95% CI of mean difference between baseline and 1‐month measurements
Comparisons are across the three groups.
Comparison between randomised groups expressed as the standardised mean difference (95% CI)
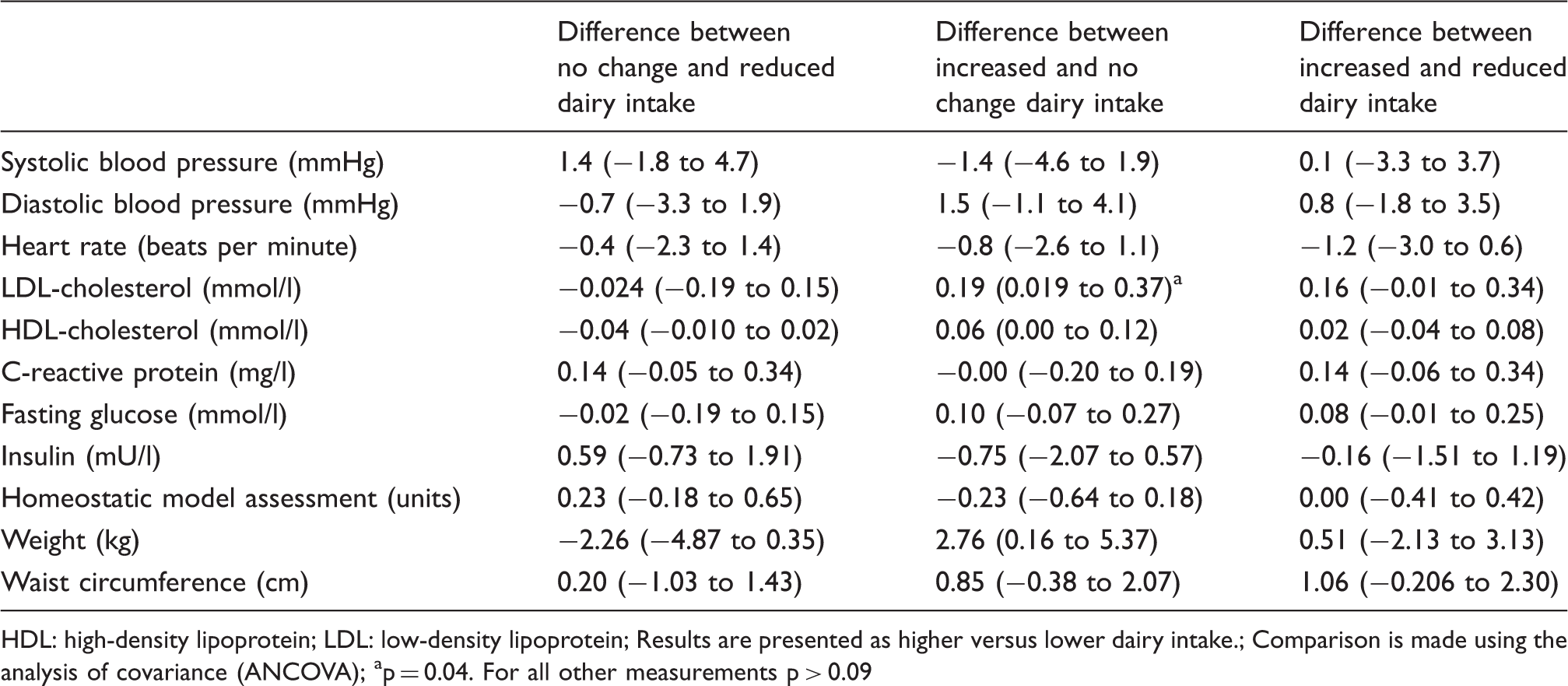
HDL: high-density lipoprotein; LDL: low-density lipoprotein
Results are presented as higher versus lower dairy intake.
Comparison is made using the analysis of covariance (ANCOVA)
p = 0.04. For all other measurements p > 0.09
Discussion
In the INTERHEART 43 and INTERSTROKE 44 studies, the major cardiovascular risk factors hypertension, central obesity, lipids and diabetes mellitus, accounted for about 70% of risk. In this study, change in dairy food intake for 1 month had no significant effect on these major cardiovascular risk factors. Another risk factor predictive of acute cardiovascular events is high sensitivity CRP (HsCRP). 45 In observational studies, dairy is associated with lower levels of HsCRP, 46 but in this study HsCRP was similar on higher and lower dairy intakes. The 95% CI for effect size is 20%, 42 which suggests that advice to modify dairy intake alone is likely to have little or no effect on the cardiovascular risk factors measured.
Much of the previous evidence on the associations between dairy food and cardio-metabolic risk factors is from large population-based studies. In these studies, higher dairy food intake has been associated with lower levels of inflammatory markers, 46,47 lower blood pressure, 10,11,48 less insulin resistance or diabetes 9,10,22,49 and lower body weight. 9,13,20,49 –52 However, observational studies do not allow reliable evaluation of causality because of the potential for bias from confounders. For example, higher dairy intake is associated with better social economic status and higher educational attainment, 53 –55 factors that are also associated with less obesity and lower cardio-metabolic risk. 56,57
Previous evidence on the effects of dairy on cardio-metabolic risk from randomised clinical trials is limited. Most studies have been small and assessed only one cardiovascular risk factor. 31,50,51,58 In the Dietary Approaches to Systolic Hypertension (DASH) 23 study, dairy was estimated to lead to a small reduction in blood pressure. However, the DASH study included multiple interventions with increased fruits, vegetables and low-fat dairy foods and had reduced amounts of saturated fat, total fat and cholesterol, so the impact of dairy compared with other interventions such as reduced total fat consumption could not be reliably assessed.
In this study, decreasing dairy intake was associated with a small decrease in waist circumference and weight. This does not support the suggestion that increasing dairy intake aids weight loss. Change in dairy food also had no effect on fasting glucose, insulin or HOMA. Observational studies suggest that increased dairy consumption could have a favourable effect in persons with insulin resistance, 9,10,13,20,21 but limited data from randomised studies also found no association between dairy intake and insulin resistance. 30,31,33,59,60 Although cardiovascular prevention guidelines have suggested reducing high-fat dairy food to lower saturated fat consumption, 1 –3 evidence that change in dairy food influences plasma lipid levels is also limited. 29,33,59,60 In the current study, LDL and HDL cholesterol levels were similar after both increasing and decreasing dairy intake, but the 95% CI included an approximately 0.37 mm/l increase in LDL cholesterol on the high dairy food intake.
This study was designed to evaluate the real-world effect of dietary advice usually given to patients. 2,3,8 This contrasts with studies which have controlled intake with prepared meals, 23,58 supplementary dairy products, 33,61 –63 or focus on specific types of dairy such as fermented vs. unfermented dairy, 64,65 cheeses vs. whole milk. 66 –68 These studies are often predicated on the assumption that specific dairy foods contain different concentrations of fatty acid isomers, which may affect health. However, most diets contain dairy food from a range of sources and results of these focused studies are hard to apply to the general population.
At present, several authoritative guidelines focus on specific food groups and place dairy as an integral part of a healthy diet, 2 recommending at least three servings per day. This study suggests that the shift in focus of recent guidelines 3,4,8 and researchers 69,70 from specific food groups, like dairy, to broader dietary patterns is appropriate.
Limitations and strengths
The study evaluated the impact of simple advice, similar to that given as part of usual health care, and consistent with most current dietary guidelines that focus on food groups and dietary patterns. 3,4 The study was not designed to evaluate effects of changing different types of dairy food, such as high- or low-fat dairy. However, no clear association was observed between change in dairy fat and change in any cardio-metabolic risk factor. Detailed food frequency questionnaires assessed the types of dairy food ingested and the self-reported changes in dairy intake were large and clinically relevant. Compliance to randomised groups was objectively assessed by measuring plasma fatty acid levels of 15:0 and 17:0. Evaluating effects of both increasing and reducing dairy intake allowed evaluation of the dose response if present. It is possible that the duration of dietary change was too short to influence the cardio-metabolic risk factors. However, in experimental studies the effects of dietary change on blood pressure, weight, insulin resistance and cholesterol have been observed within 1 month, 23 and adherence to longer-term dietary change in a clinical trial is difficult. 71 The study evaluated healthy volunteers in part to reduce confounding from effects of disease and treatments which influence cardio-metabolic risk. Further study is needed to evaluate long-term effects in patients with the metabolic syndrome and cardiovascular disease, but it is likely these will be similar to those in healthy volunteers.
Conclusion
Dietary advice to change dairy intake for 1 month had no significant effects on major cardiovascular risk factors. These observations suggest that dairy food can be included as part of a normal healthy diet without adverse effects on cardio-metabolic risk.
Footnotes
Funding
The ADHB Charitable trust and Green Lane Research and Educational Fund provided financial support for the study. A report was submitted to the funders following completion of the study. The funders had no role in study design, data collection or analysis, or the decision to publish.
Conflict of interest
All authors declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work.