
Abstract
Background
Plasma choline has been associated with cardiovascular disease and nonalcoholic steatohepatitis.
Design
We sought to study relations of plasma choline and its metabolite betaine to long-term risk of acute myocardial infarction (AMI) and all-cause mortality according to smoking status, in patients undergoing coronary angiography for stable angina pectoris.
Methods
Samples were obtained before angiography from 2568 patients who were subsequently randomized in the Western Norway B-Vitamin Intervention Trial (WENBIT). Hazard ratios (HR) were calculated using multivariate Cox-regression and p-values were reported for trends over quartiles.
Results
Plasma concentrations of choline, but not betaine, were lower in smokers, and choline was positively associated with C-reactive protein and troponin T in nonsmokers, but not in smokers (p for interaction <0.03). During a follow up of 4.8 ± 1.4 (mean ± SD) years, 8.3% suffered from AMI and 6.1% died. In the total population, choline was not associated with AMI or all-cause mortality. However, comparing the highest vs. the lowest quartiles, plasma choline was associated with increased risk of AMI in nonsmokers (HR 2.63, 95% CI 1.56 to 5.51; p for trend = 0.013) and no risk in smokers (p for interaction < 0.001). Plasma choline significantly improved discrimination and reclassification when added to established cardiovascular risk factors. Plasma betaine was not associated with either endpoint.
Conclusions
In patients with stable angina pectoris, elevated plasma choline is associated with elevated troponin levels and increased risk of AMI in nonsmokers. These results motivate further research into the relation between choline metabolism, smoking, and atherothrombosis.
Introduction
Choline and betaine are methylamines involved in several vital metabolic pathways. Choline is a precursor of the neurotransmitter acetylcholine and a precursor and metabolite of phosphatidylcholine (PC). PC constitutes the largest pool of choline in most animal tissues, plays a major role in very-low-density lipoprotein metabolism, and is an essential component of cell membranes.1,2 In the mitochondria, choline can be oxidized to betaine, 3 which serves as an osmolyte and methyl donor for remethylation of homocysteine to methionine, catalysed by the enzyme betaine homocysteine methyl transferase. 4 We have previously demonstrated that choline and betaine have opposite associations with several components of the metabolic syndrome in the general population. 5
Recent studies suggest increased cardiovascular risk from dietary PC, associated with elevated plasma levels of trimethylamine N-oxide (TMAO). The proposed mechanism is gut microbe-dependent conversion of choline to trimethylamine, which is converted to TMAO in the liver and is a possible causal risk factor of cardiovascular disease.6,7 Choline has also been proposed as a biomarker of cardiac ischaemia 8 and coronary plaque destabilization.9,10 Elevated plasma choline levels have been attributed to increased activity of the enzymes phospholipase D and A2 in unstable plaques and ischaemic myocardium, which generate choline, or to disruption of the mitochondrial oxidation of choline to betaine.11,12 Additionally, high levels of plasma choline are seen in patients with nonalcoholic steatohepatitis, 13 which is a risk factor for coronary artery disease (CAD). 14
We have recently shown that plasma dimethylglycine, a metabolite in the choline oxidation pathway, is associated with increased risk of AMI in nonsmokers, but not in smokers. 15 Smokers have higher dietary intake 16 but lower plasma levels of choline. 5 Further, smoking is associated with numerous effects on phospholipid metabolism17–19 and is a major risk factor of CVD. 20 Thus, there may be an interrelationship between smoking, choline metabolism, and the risk of cardiovascular disease.
The main aims of the current investigation were to evaluate the associations of plasma choline and betaine levels to subsequent long-term risk of acute myocardial infarction (AMI) and all-cause mortality in patients undergoing elective coronary angiography for stable angina pectoris (SAP), and to explore effect modification by smoking.
Methods
Patient population
The current investigation is a prospective cohort study based on the Western Norway B Vitamin Intervention Trial (WENBIT), 21 a randomized, double-blind, placebo-controlled clinical trial conducted between 1999 and 2005. The primary objective of the study was to investigate whether homocysteine-lowering treatment with folic acid and vitamin B12, vitamin B6, or their combination could reduce cardiovascular events and mortality. Details on randomization and the vitamin regimen have been published elsewhere. 21 The study recruited a total of 3090 patients undergoing coronary angiography for suspected CAD. For the current investigation, patients with acute coronary syndromes (ACS) (unstable angina or AMI, n = 461), aortic valve stenosis (n = 56), and patients with missing values of plasma choline and betaine at baseline (n = 5), were excluded from the analyses. Thus, we studied totally 2568 patients with suspected SAP. Written, informed consent was obtained from all participants. The study was approved by the Regional Committee for Medical and Health Research Ethics, the Data Inspectorate, and the Norwegian Directorate of Health.
Data collection, biochemical analyses, and follow up
Clinical information and blood samples were obtained at baseline, and repeated blood samples were drawn after 1 month, 1 year, and at the end of the study among the majority of participants. Smokers included self-reported current smokers, those reporting having quit smoking within the last 4 weeks, and subjects with plasma cotinine >85 nmol/l. Plasma was usually sampled a few days before coronary angiography. The time of blood sampling and the number of hours since last meal were registered. Samples were prepared and immediately frozen at −80℃ until analysed at Bevital (http://www.bevital.no). Choline and betaine were measured in EDTA plasma by LC-MS/MS. 22 Troponin T was measured in serum by high-sensitivity troponin T assay on Modular E170 (Roche Diagnostics). The lower detection limit was 3 ng/l.
The WENBIT trial was terminated in 2005. Participants who died during follow up or were residing in Norway at the time of their final visit were included in this observational post-trial follow up until 31 December 2007; 23 post-trial follow up did not imply any continued study treatment, further blood sampling, or personal contact. Data on AMI were recorded as described previously. 21 Data on all-cause mortality were obtained by linking the unique personal identification numbers to the Cause of Death Registry of Norway.
Statistical analyses
Continuous variables are given as mean ± SD or medians (interquartile range) and categorical variables as percentages. Statistical differences were assessed with T-test, Mann–Whitney U, Kruskal–Wallis, and Fisher’s exact test, where appropriate. Median change of risk factors per quartile increase of choline was calculated using quantile regression, 24 adjusting for age, sex, and fasting status (yes vs. no) in nonsmokers and smokers, separately. The differences between the two groups were tested by adding the interaction term choline (quartiles) × smoking (yes vs. no) to models applied on the entire cohort. Survival was initially explored with Kaplan–Meier plots and log-rank tests. Subsequently, Cox regression analyses were conducted to calculate hazard ratios (HRs) for each quartile increment of plasma choline and betaine. For subgroup analyses of nonsmokers and smokers, we compared quartiles 2–4 to quartile 1. We used a simple model (Model 1) adjusted for age, sex, fasting status, smoking, and study site (0–1), and a fully adjusted multivariate model (Model 2) that additionally included body mass index, diabetes mellitus, left ventricular ejection fraction, estimated glomerular filtration rate, LDL-cholesterol, and medication at discharge from hospital (aspirin, beta-blockers, and statins). Effect modifications by smoking were tested by adding interaction terms to the models. Survival plots obtained by general additive model were inspected to rule out nonlinear risk associations. Log-log plots and plots of Schoenfeld residuals were performed to ensure that assumptions of proportional hazards were not violated. The annual event rate was calculated by dividing the total number of patients with events by the total number of patient-years of follow up. The incremental prognostic value of plasma choline was tested by pairwise comparison of areas under the curve (AUC) of receiver operating characteristics curves, derived from logistic regression models including the same covariates as the Cox models, with and without choline and its interaction term with smoking. The follow up was cut at 1000 days, which approximately was the shortest individual follow-up time. Goodness of fit was tested with the Hosmer–Lemeshow statistic. Continuous net reclassification improvement was calculated using the same logistic regression models. Analyses of repeated measures and estimation of the coefficients of reliability (CoR) were calculated using multilevel analyses. All tests were two-sided and p-values <0.05 were considered significant. Statistical analyses were performed using R (version 2.14.1) and SPSS version 18.0 (SPSS, Chicago, IL, USA).
Results
Baseline characteristics
Baseline characteristics.
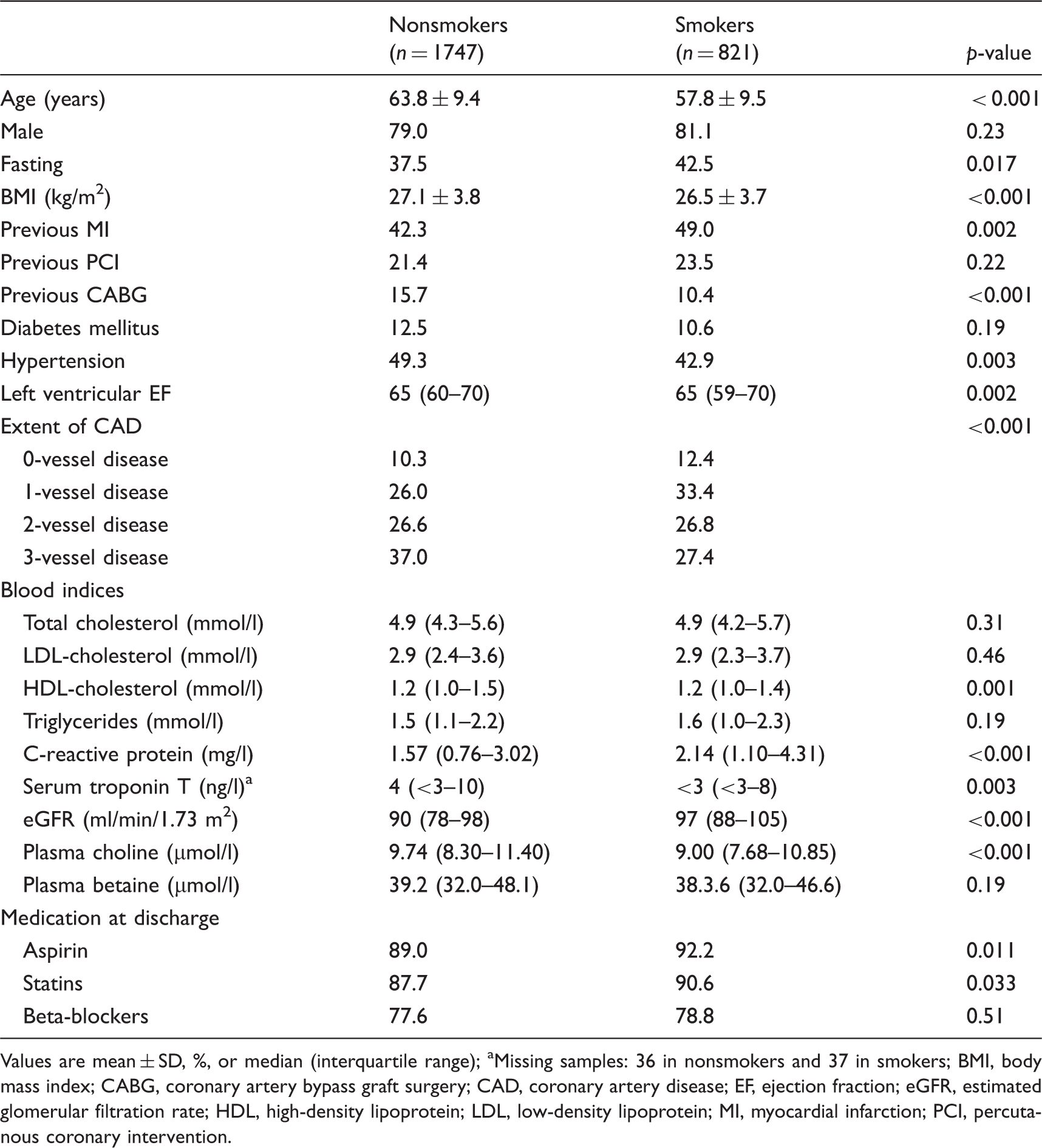
Values are mean ± SD, %, or median (interquartile range)
Missing samples: 36 in nonsmokers and 37 in smokers
BMI, body mass index; CABG, coronary artery bypass graft surgery; CAD, coronary artery disease; EF, ejection fraction; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MI, myocardial infarction; PCI, percutanous coronary intervention.
Associations between plasma choline and risk factors of cardiovascular disease
Change in risk factors for cardiovascular disease per increasing quartile of choline.
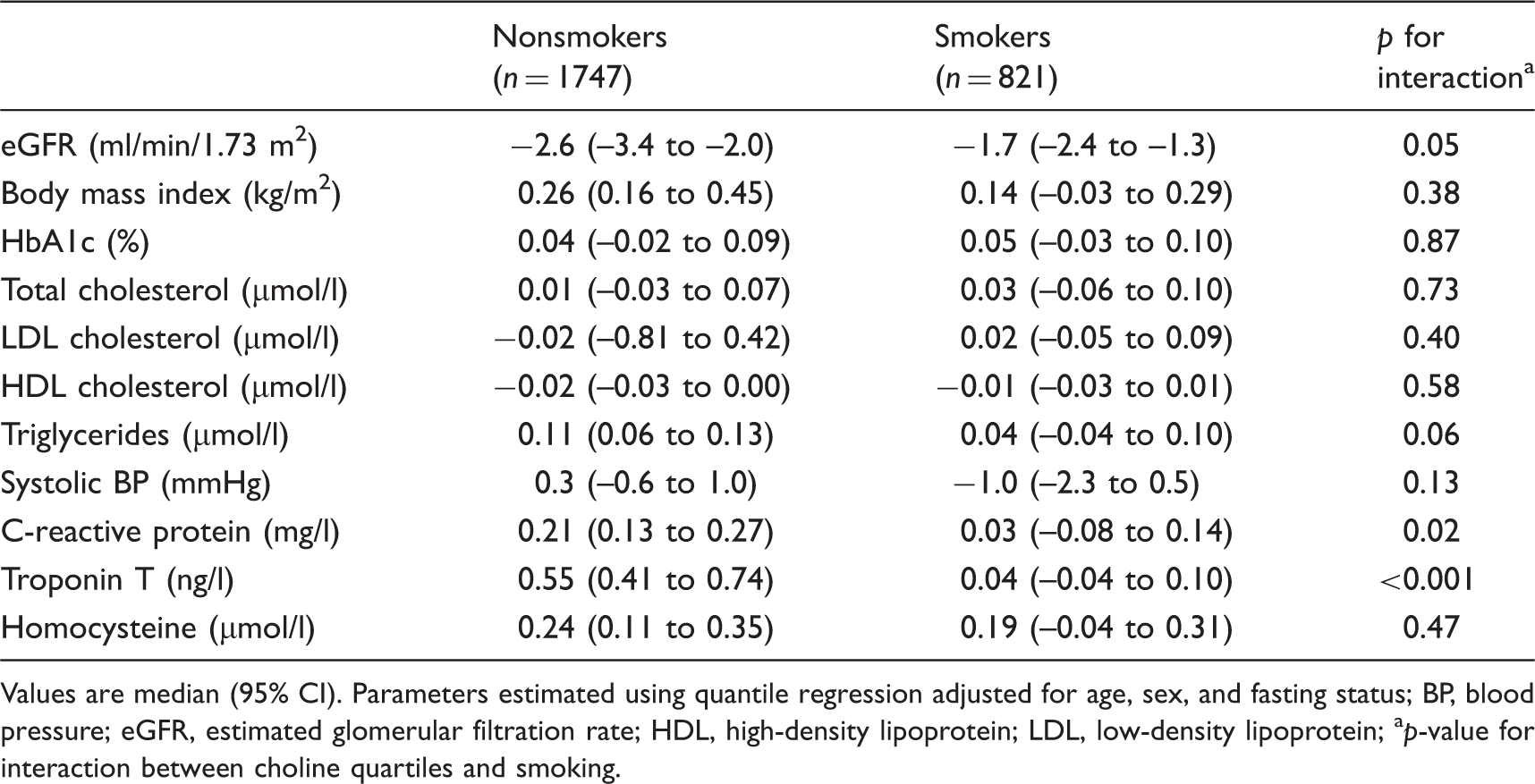
Values are median (95% CI). Parameters estimated using quantile regression adjusted for age, sex, and fasting status
BP, blood pressure; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein
p-value for interaction between choline quartiles and smoking.
Long-term prognosis of AMI and all-cause mortality
During a follow up of (mean ± SD) 4.8 ± 1.4 years, 8.3% suffered from AMI and 6.1% died. Baseline plasma choline and betaine were explored as potential predictors of future events. Figure 1 shows unadjusted Kaplan–Meier plots and log-rank tests of plasma choline quartiles as predictors of AMI in the entire cohort, and separately in nonsmokers and smokers. Overall, baseline plasma choline was associated with risk of future AMI in the total population (p = 0.036) and in nonsmokers (p < 0.001), but not in smokers. No relations were found between choline and all-cause mortality or between betaine and either AMI or all-cause mortality (data not shown).
Kaplan–Meier plots displaying survival free of acute myocardial infarction in the total population and in nonsmokers and smokers separately, according to quartiles of plasma choline.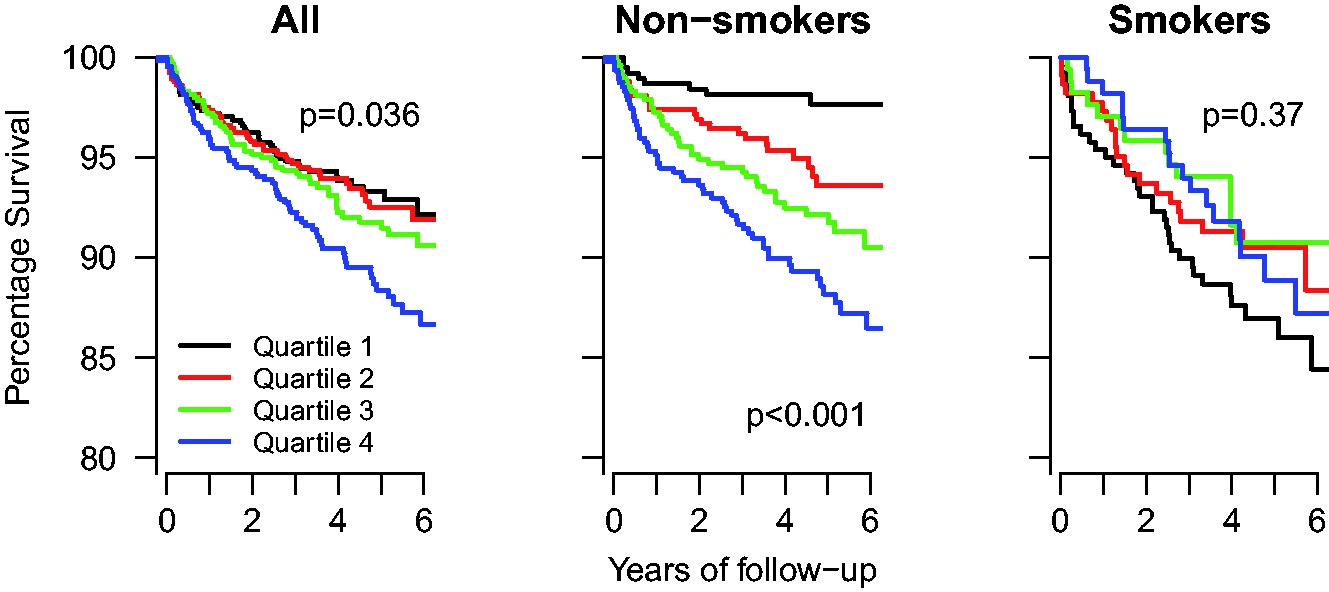
Risk of AMI and all-cause death according to concentrations of baseline plasma choline and betaine in patients with stable angina pectoris.
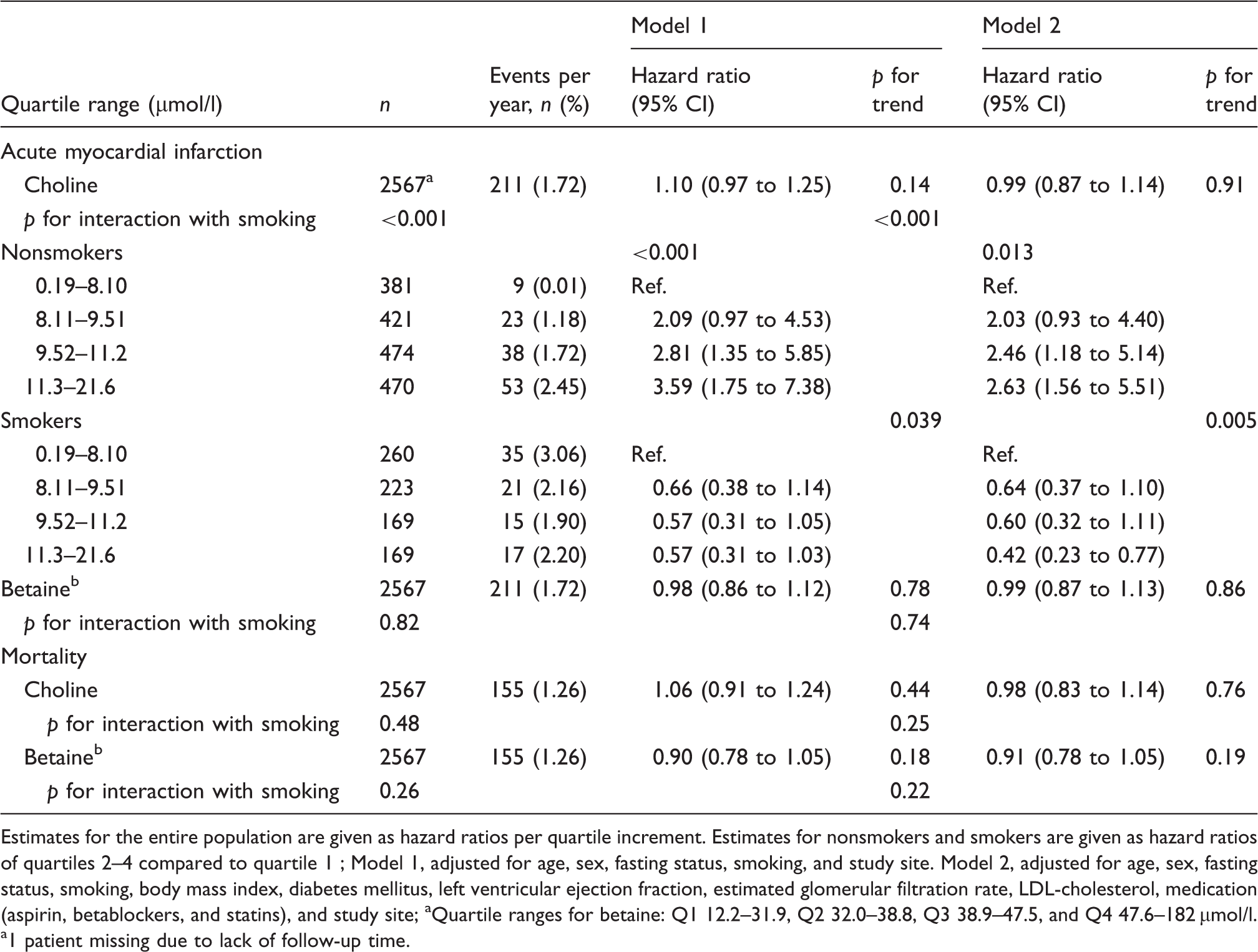
Estimates for the entire population are given as hazard ratios per quartile increment. Estimates for nonsmokers and smokers are given as hazard ratios of quartiles 2–4 compared to quartile 1
Model 1, adjusted for age, sex, fasting status, smoking, and study site. Model 2, adjusted for age, sex, fasting status, smoking, body mass index, diabetes mellitus, left ventricular ejection fraction, estimated glomerular filtration rate, LDL-cholesterol, medication (aspirin, betablockers, and statins), and study site
Quartile ranges for betaine: Q1 12.2–31.9, Q2 32.0–38.8, Q3 38.9–47.5, and Q4 47.6–182 µmol/l. a1 patient missing due to lack of follow-up time.
We then calculated risk of AMI in nonsmokers and smokers separately. In nonsmokers using model 1, the highest choline quartile, compared to the lowest, was associated with a HR of 3.59 (95% CI 1.75 to 7.38) and in model 2 with a HR of 2.63 (95% CI 1.56 to 5.51; Table 3). In smokers, the relation between risk and choline was in the opposite direction in both models 1 and 2 (HR 0.57, 95% CI 0.31 to 1.03, and 0.42, 95% CI 0.23 to 0.77, respectively; Table 3). No significant interaction was observed according to sex. Inclusion of CRP, troponin T, cotinine, study intervention with B-vitamins/placebo, or revascularization following baseline angiography (percutaneous coronary intervention or coronary artery bypass surgery) into model 2 did not substantially alter the results (HR in nonsmokers 2.65, 95% CI 1.27 to 5.56).
Evaluation of the survival models for AMI
We calculated change of AUC when adding choline and the interaction term between choline and smoking to logistic regression models, including the same covariates as in the Cox models (models 1 and 2), with AMI as the endpoint. In model 1, AUC increased from 0.632 (95% CI 0.586 to 0.679) to 0.670 (95% CI 0.627 to 0.714; p = 0.006) and in model 2 from 0.701 (95% CI 0.653 to 0.748) to 0.721 (95% CI 0.676 to 0.767; p = 0.023). Calculating continuous reclassification using model 2, 44.4% (95% CI 28.1 to 60.1%) of events were correctly reclassified, whereas 9.5% (95% CI 13.4 to 5.5%) of nonevents were wrongly reclassified (both p < 0.001). The continuous net reclassification index was 35.0% (95% CI 18.2 to 51.8%) (p < 0.001).
Effect modification of smoking by plasma choline
Figure 2 shows the hazard ratios of AMI in smokers vs. nonsmokers across quartiles of choline, calculated with Cox regression using model 2. In the lowest choline quartile, smoking was associated with a 6-fold increased risk of AMI compared to nonsmoking. The excess risk of smoking was inversely related to choline levels, and in the upper quartile smoking was not associated with incident AMI.
Hazard ratios for acute myocardial infarction in smokers compared to nonsmokers by multivariate Cox-regression across quartiles of plasma choline. Quartile ranges of choline: Q1 0.19–8.10, Q2 8.11–9.51, Q3 9.52–11.2, and Q4 11.3–21.6 µmol/l.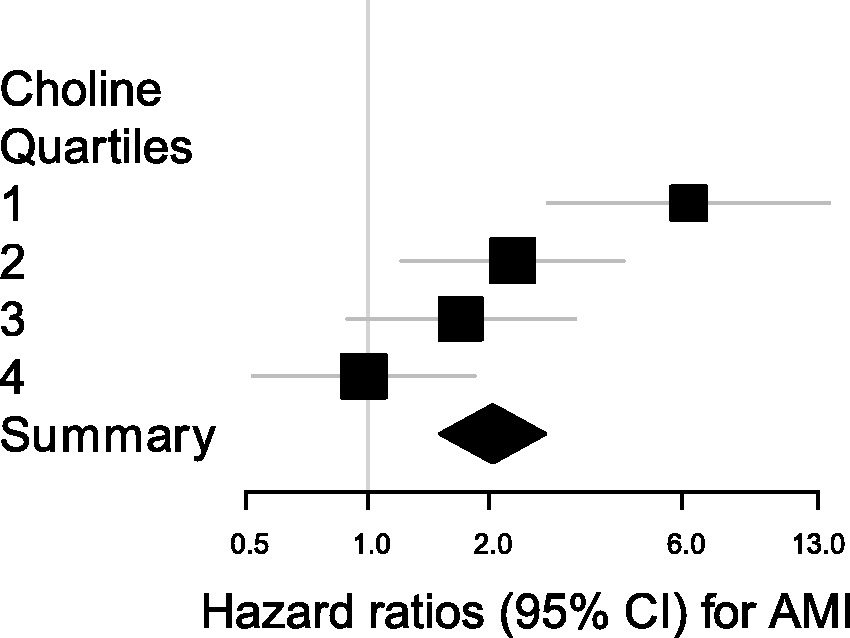
Long-term test-retest stability
To determine the intraindividual stability of plasma choline and betaine in patients who received placebo (n = 599), we estimated plasma levels at baseline and at three follow-up visits. Compared to baseline, plasma choline was mean 0.76 µmol/l (95% CI 0.55, 0.98 µmol/l) higher and plasma betaine 2.0 µmol/l (95% CI 1.2, 2.8 µmol/l) higher after 1 month. After 1 month, neither choline (0.06 µmol/l/year, 95% CI –0.01, 0.12 µmol/l/year; p = 0.081) nor betaine (0.2 µmol/l/year, 95% CI –0.1, 0.4 µmol/l/year; p = 0.21) changed significantly during follow up. The coefficients of reliability for choline and betaine were 0.45 and 0.65, respectively.
Discussion
Principal findings
In this prospective study of 2568 patients with suspected SAP, we have shown that smoking strongly modifies the association between plasma choline, serum troponin T, and risk of incident AMI. High levels of plasma choline were associated with elevated levels of troponin T and increased risk of incident AMI in nonsmokers, whereas no relation to troponin T or the risk of AMI were observed in smokers. Accordingly, the excess risk of smoking was primarily observed in patients with low choline, with a 6-fold increased risk of AMI in patients belonging to the lowest choline quartile (≤8.1 µmol/l). For the endpoint of AMI, inclusion of both choline and its interaction term with smoking significantly improved the AUC and net reclassification index. We observed no relation of choline with all-cause mortality, and plasma betaine was not associated with either endpoint.
Choline, betaine, and cardiovascular disease
In the current study, circulating choline and betaine levels are approximately at the same levels as seen in the general Norwegian population 5 and in patients with suspected CVD. 6 We confirmed that plasma choline is higher in males and lower in smokers. Elevated circulating choline levels25–28 but low levels of total choline-containing phospholipid levels 29 have been associated with adverse outcome in patients with ACS in several small studies. Low plasma betaine has also been associated with subsequent AMI in ACS patients. 30 In patients with SAP, plasma choline and betaine have, to our knowledge, not previously been explored as predictors of AMI or all-cause mortality. However, Wang et al. 6 reported a link between high intake of dietary choline and increased formation of atherosclerotic plaques in mice, likely mediated by increased production of TMAO. The same group also showed strong, dose-dependent, cross-sectional associations of plasma choline, betaine, and TMAO with the presence of CVD in patients undergoing elective cardiac evaluation. In a recent prospective study among patients undergoing elective coronary angiography, the same group showed that plasma levels of TMAO were associated with major cardiovascular events during 3 years of follow up; data on dietary intake or plasma levels of choline and betaine levels were not presented. 7 In contrast, two large prospective studies in the general population with follow up of 8 and 14 years found no associations between dietary intake of choline or betaine and incident CVD risk.31,32 Thus, the literature is somewhat inconsistent as to how choline and betaine relates with CVD. However, none of the aforementioned studies, in which substantial parts of the populations were smokers, stratified data according to smoking status. Analysing nonsmokers and smokers combined could have masked a diverging association with choline, as was observed with plasma levels in our data.
Possible pathomechanisms
Our results suggest that elevated choline is associated with the development of atherothrombosis in nonsmokers, among whom high choline was related both to higher risk of AMI and to higher CRP and troponin T levels. Since the predictive value of plasma choline was independent of both CRP and troponin T levels, high choline may be caused by a different mechanism, possibly through increased activity of phospholipase D. This enzyme generates choline and phosphatidic acid from PC and is involved in platelet activation and secretion of metalloproteinases, 33 both of which are crucial in developing atherothrombosis.34,35 As reported by Wang et al., 6 gut-flora-dependent production of TMAO from choline represents another possible pathomechanism. Further, plasma choline has been associated with the onset of nonalcoholic steatohepatitis, and is strongly negatively correlated with liver microsomal triglyceride transfer protein. 13 This protein is important to very low density lipoprotein secretion and activity is much lower in patients with nonalcoholic steatohepatitis. Thus, high plasma choline could indicate disturbed lipid assembly in the liver and possibly unrecognized nonalcoholic fatty liver disease, which is as an independent risk factor of CVD. 14
The lack of relationships between choline and CVD risk factors and incident AMI in smokers may be explained by the influence of smoking on choline and PC metabolism. Smoking changes the phospholipid composition and decreases the PC content of platelet membranes, 18 which can be important for the blood coagulation reaction. 36 Smoking also causes oxidative stress, 37 leading to fragmentation of PC, 17 which has been associated with atherosclerosis. 38 Considering that PC constitutes the largest pool of choline, it is plausible that these effects of smoking would also alter plasma choline levels, and to some extent be responsible for the diverging associations. Lastly, our results may be in line with a report showing an association between low dietary intake of choline and betaine and risk of lung cancer in smokers, but not in nonsmokers. 16
Mirroring the effect modification of choline by smoking, the excess risk of AMI in smokers was strongly modified by choline status, being 6-fold increased in patients with low levels and absent in patients with high levels. Taken together, choline levels appear to reflect different aspects of atherothrombosis in smokers and nonsmokers. However, as our study is observational we cannot draw conclusions regarding causality.
The potential importance of our findings is demonstrated by the significant improvement of the AUC and net reclassification index.
Strengths and limitations
The strengths of our study include its prospective design, large sample size, and repeated measurements. As personalized medicine becomes increasingly important, substratification to differentiate between individuals with distinct phenotypes can be valuable in risk evaluation and treatment. 39 A possible limitation of the study is that choline was measured only in plasma and not in whole blood, which has yielded higher risk estimates in patients with ACS. 11 Since we did not have data on dietary intake of choline and betaine, we cannot speculate to what degree intake and metabolism determined plasma levels.
Conclusions
In patients with SAP, high levels of plasma choline are associated with elevated levels of troponin-T and increased risk of incident AMI in nonsmokers, whereas smoking primarily is a risk factor in patients with low choline. Thus, choline status probably reflects different aspects of atherothrombosis in nonsmokers and smokers, which may help clarify diverging findings in previous studies on choline and CAD. Our findings should motivate further research into the relation between choline metabolism, smoking, and CAD.
Footnotes
Funding
This work was supported by the University of Bergen, Bergen, Norway, the Nordic Centre of Excellence Programme on Food, Nutrition and Health – MitoHealth, Bergen, Norway, and the Foundation to Promote Research into Functional Vitamin B12 Deficiency, Bergen, Norway.
Conflict of interest
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.