
Abstract
Background
Most individuals at high cardiovascular disease (CVD) risk worldwide do not receive any or optimal preventive drugs. We aimed to determine whether fixed dose combinations of generic drugs (‘polypills’) would promote use of such medications.
Methods
We conducted a randomized, open-label trial involving 623 participants from Australian general practices. Participants had established CVD or an estimated five-year CVD risk of ≥15%, with indications for antiplatelet, statin and ≥2 blood pressure lowering drugs (‘combination treatment’). Participants randomized to the ‘polypill-based strategy’ received a polypill containing aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg and either atenolol 50 mg or hydrochlorothiazide 12.5 mg. Participants randomized to ‘usual care’ continued with separate medications and doses as prescribed by their doctor. Primary outcomes were self-reported combination treatment use, systolic blood pressure and total cholesterol.
Results
After a median of 18 months, the polypill-based strategy was associated with greater use of combination treatment (70% vs. 47%; relative risk 1.49, (95% confidence interval (CI) 1.30 to 1.72) p < 0.0001; number needed to treat = 4.4 (3.3 to 6.6)) without differences in systolic blood pressure (−1.5 mmHg (95% CI −4.0 to 1.0) p = 0.24) or total cholesterol (0.08 mmol/l (95% CI −0.06 to 0.22) p = 0.26). At study end, 17% and 67% of participants in polypill and usual care groups, respectively, were taking atorvastatin or rosuvastatin.
Conclusion
Provision of a polypill improved self-reported use of indicated preventive treatments. The lack of differences in blood pressure and cholesterol may reflect limited study power, although for cholesterol, improved statin use in the polypill group counter-balanced use of more potent statins with usual care.
Introduction
The long-term use of effective preventive drugs is inadequate among people at high cardiovascular disease (CVD) risk, including those with established disease. 1 This is particularly the case in lower income countries; however, large gaps also exist in relatively wealthy economies with highly developed healthcare resources. 2 In Australia, recent primary care audits have shown prescription rates of indicated combinations of blood pressure (BP) lowering drugs, statins and antiplatelets as low as 30%–50%.3,4 Actual use is likely to be even lower, given known inadequate adherence to prescribed medicines. 5
Reasons for inadequate use of indicated medications are multiple and complex. 6 Barriers to doctors’ adoption of evidence-based treatments can include lack of time or guideline awareness, multiplicity of guidelines and insufficient resources.7–11 Inadequate adherence to prescribed medications is associated with multiple prescriptions with complex dosing regimens, inadequate knowledge and psychosocial issues.12–14 Patients may adopt strategies to reduce costs, including not filling prescriptions and omitting doses.15,16 A strategy based on using fixed-dose combination therapy (‘polypills’) with generic components may help reduce treatment gaps, by reducing costs, complexity of drug regimens and therapeutic inertia. However, theoretical concerns exist that the lack of flexibility associated with fixed combinations may limit tailoring of individual medications, leading to less optimal risk factor control. There is also concern that polypill use may deflect attention from lifestyle measures to prevent CVD.
To address this uncertainty, an international series of trials has been designed to evaluate the effectiveness of a polypill-based strategy on promoting use of indicated CVD preventive drugs (www.spacecollaboration.org). These trials have a similar design, with each protocol adapted to maximize relevance to local processes of healthcare delivery. We report the results of a randomized controlled trial in Australia.17–19 Indigenous Australians experience a particularly high burden of CVD 20 and the Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) study specifically included a substantial number of Indigenous Australians attending Aboriginal Medical Services.
Methods
Kanyini GAP was a prospective, randomized, open-label clinical trial. The protocol has been published. 18 Ethics approval was granted by appropriate committees in all relevant jurisdictions and each participant provided written informed consent.
Participants
Men and women aged ≥18 years at high CVD risk, defined as either established CVD (history of coronary, ischaemic cerebrovascular, or peripheral vascular disease) or an estimated five-year CVD risk of ≥15% (using the Framingham risk equation, including a 5% increment for Aboriginal or Torres Strait Islander identification) 21 were eligible. Each participant had to have, in their doctor’s view, indications for all and no contraindications to any component of at least one of two polypills – version 1 (containing aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg, atenolol 50 mg) or version 2 (containing aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg, hydrochlorothiazide 12.5 mg). Participants were excluded if it was felt clinically inappropriate to alter medications.
Randomization and treatment
Central, computer-based randomization to polypill-based strategy or usual care was stratified by primary healthcare centre, type of indication (established CVD versus high risk), Indigenous identification and level of preventive treatment at baseline.
All participants were treated by their regular doctor following randomization. No attempt was made to influence the management of usual care participants. Those allocated to the polypill-based strategy were prescribed one of the polypill versions at the discretion of their doctor, to be taken at a time suggested by the doctor. No attempt was made to influence any other aspect of their management. The doctor could, at any time, change prescription to the alternative polypill version, add drugs on top of the polypill, or withdraw the polypill and substitute individual drugs of their choice.
Prescription and dispensing of the polypill occurred in the same way as for other medications. This mostly involved doctors providing patients with written prescriptions, and patients presenting the prescriptions to designated local pharmacies where all drugs (including the polypill) were dispensed. Out-of-pocket expenses for the polypill were incurred identically to those for any other drug listed in the Pharmaceutical Benefits Scheme, which is the government subsidy programme through which most drugs are obtained in Australia. 22 At one extreme, patients ineligible for any concessions were charged the standard co-payment (approximately AUD$35/month for each medication). At the other extreme, the polypill was dispensed without charge at Indigenous health services operating under the Section 100 scheme of the National Health Act. 23
Trial procedures
Participants attended the primary healthcare centres for trial assessments at randomization and 12 month intervals thereafter. All participants were also reviewed one month post-randomization and at intervening six month intervals, but these could be conducted by telephone. BP (measured with the Omron 705CP II device) and fasting lipids (measured at local laboratories) levels were obtained at baseline, 12 months, 24 months and the final visit. Self-reported use of all medications was assessed at each visit, recorded as the number of days on which medication was taken in the immediately preceding week. Other follow-up information obtained included perceived barriers to adherence, quality of life (EQ5D questionnaire), occurrence of cardiovascular, renal and other serious adverse events and reasons for stopping cardiovascular medications.
Outcomes
Primary outcomes were self-reported use of indicated combination treatment (antiplatelet, statin and ≥2 BP lowering therapies for ≥4 of the previous seven days) at study end; and changes in systolic BP and total cholesterol from baseline to study end.
Pre-specified secondary outcomes included self-reported combination treatment use at 12 months; combination treatment prescriptions at the study end; reasons for stopping cardiovascular medications; changes in lipid fractions; quality of life; serious adverse events; cardiovascular events (coronary heart disease, heart failure leading to death or hospitalization, cerebrovascular or peripheral arterial disease events); and renal events (new onset microalbuminuria (albumin:creatinine ratio 3.0–33.9 mg/mmol), progression to macroalbuminuria (albumin:creatinine ratio >33.9 mg/mmol) or at least a 50% decrease in estimated glomerular filtration rate from baseline to a level <60 ml/min per 1.73 m2). All potential cardiovascular and renal events were independently adjudicated by a blinded expert committee. To reduce potential bias related to the open study design, print-outs from the automated BP measurement devices and laboratory cholesterol reports were inspected during study monitoring.
Sample size and statistical analysis
Accounting for 10% deaths and loss to follow-up, inclusion of 1000 participants was estimated to provide 90% power (2α = 0.05) to detect a 30% absolute improvement in self-reported combination treatment use with the polypill-based strategy, assuming this would be 50% with usual care at the end of follow-up. This provided 90% power to detect at least 3 mmHg difference in systolic BP and 0.20 mmol/l difference in total cholesterol, assuming standard deviations of 14 mmHg and 0.9 mmol/l, respectively.
The relative risk of self-reported use of combination treatment at study end was calculated using log-binomial regression including randomized treatment. Analyses of change in systolic BP and total cholesterol were conducted using longitudinal linear mixed models including all values collected during follow-up. Models included treatment, visit, treatment-by-visit interaction, and the baseline systolic BP or total cholesterol. Correlations between repeated measurements were modelled using a compound-symmetry structure. Adjusted analyses of the primary endpoints were performed by adding age, sex, type of study centre, Indigenous status and type of indication (high risk versus established CVD) as covariates.
Type of study centre, baseline use of combination treatment, presence of established CVD, age, sex, presence of diabetes mellitus, smoking status and polypill choice (ascertained from the doctor pre-randomization) were used to pre-specify subgroup analyses. For each subgroup, the primary analysis was repeated after adding the subgroup variable and its interaction with treatment. Heterogeneity was assessed based on the significance of the interaction term. Continuous secondary endpoints were assessed using longitudinal mixed models. Differences in incidence of cardiovascular and renal outcomes were analysed using Cox models after checking the proportional hazard assumption.
All analyses were conducted on an intention-to-treat basis without imputation of missing data. While formal adjustments for multiple tests were not made, findings are interpreted in the light of the number of comparisons made and the significance level of the result. 24
Results
Enrolment and follow-up
A total of 623 participants were randomized from 33 centres (12 Aboriginal Medical Services) between January 2010 and May 2012 (Figure 1). Failure to recruit the planned number of participants reflected insufficient resources to continue enrolment. Median follow-up was 20.7 months in the polypill group and 18.1 months in the usual care arm. No systematic difference in follow-up visits was identified, and this small difference appears to have occurred by chance.
Registration, randomization and follow-up of study participants.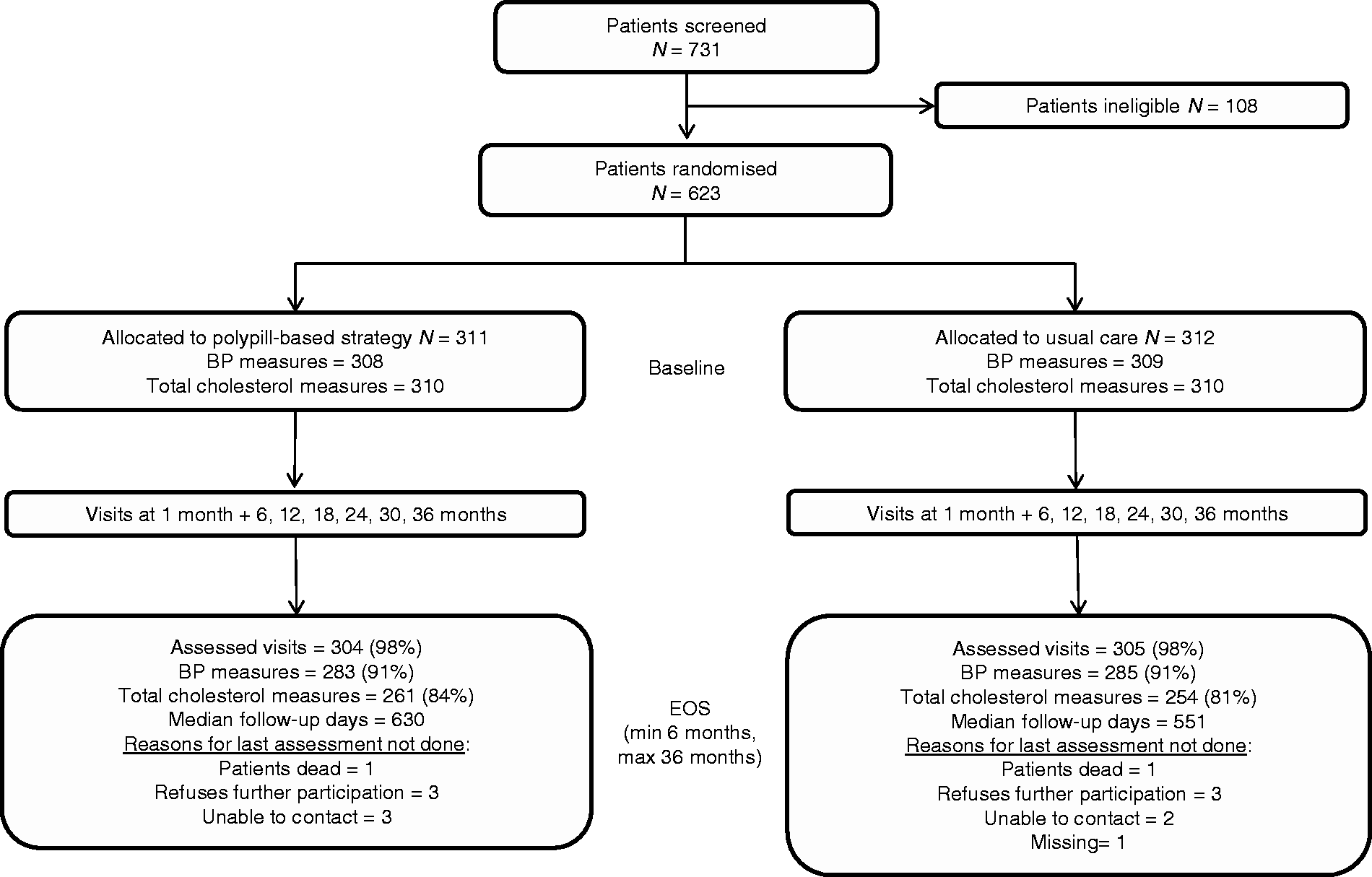
Baseline characteristics of participants
Baseline characteristics.
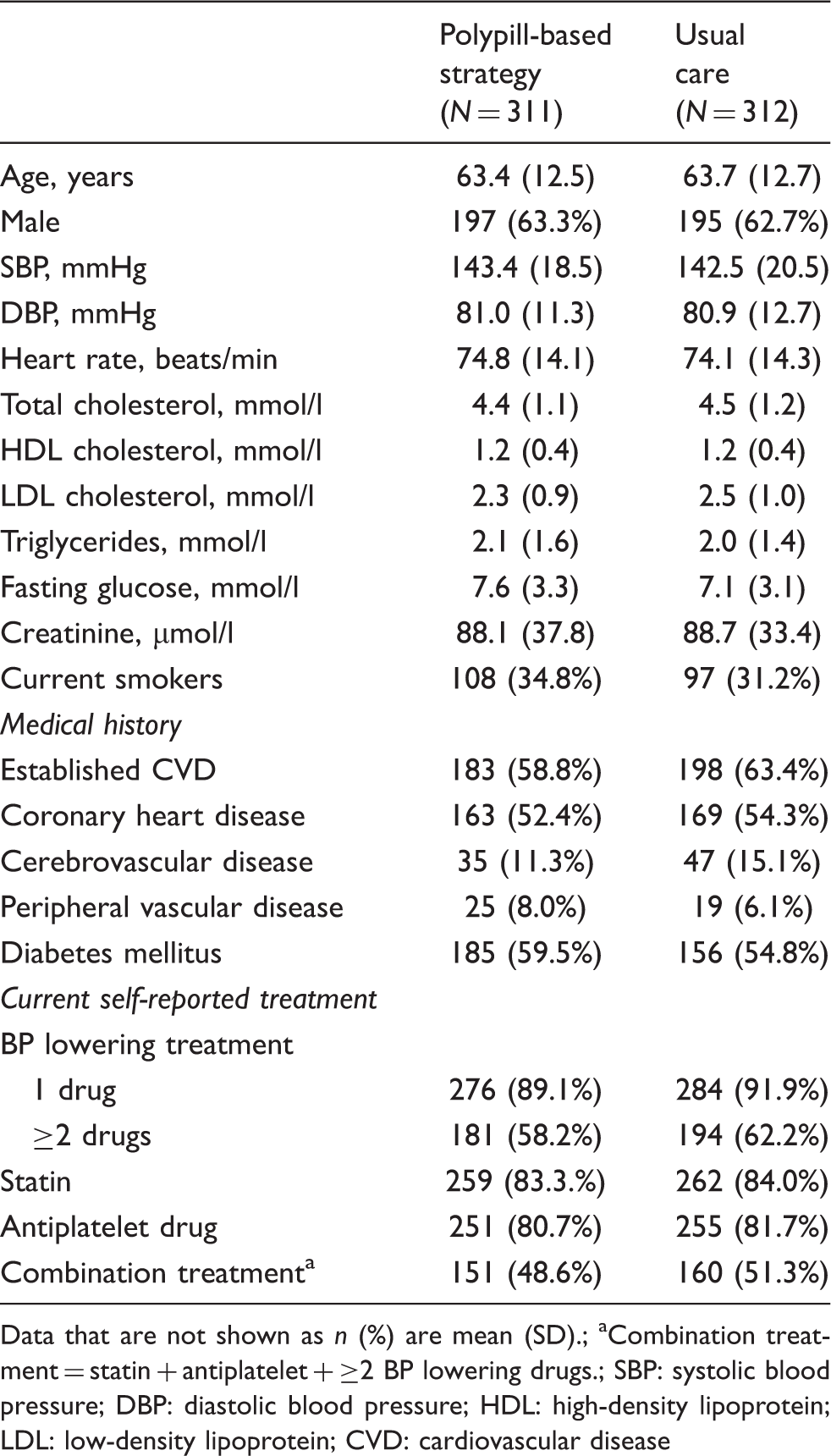
Data that are not shown as n (%) are mean (SD).
Combination treatment = statin + antiplatelet + ≥2 BP lowering drugs.
SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; CVD: cardiovascular disease
Effects on primary outcomes
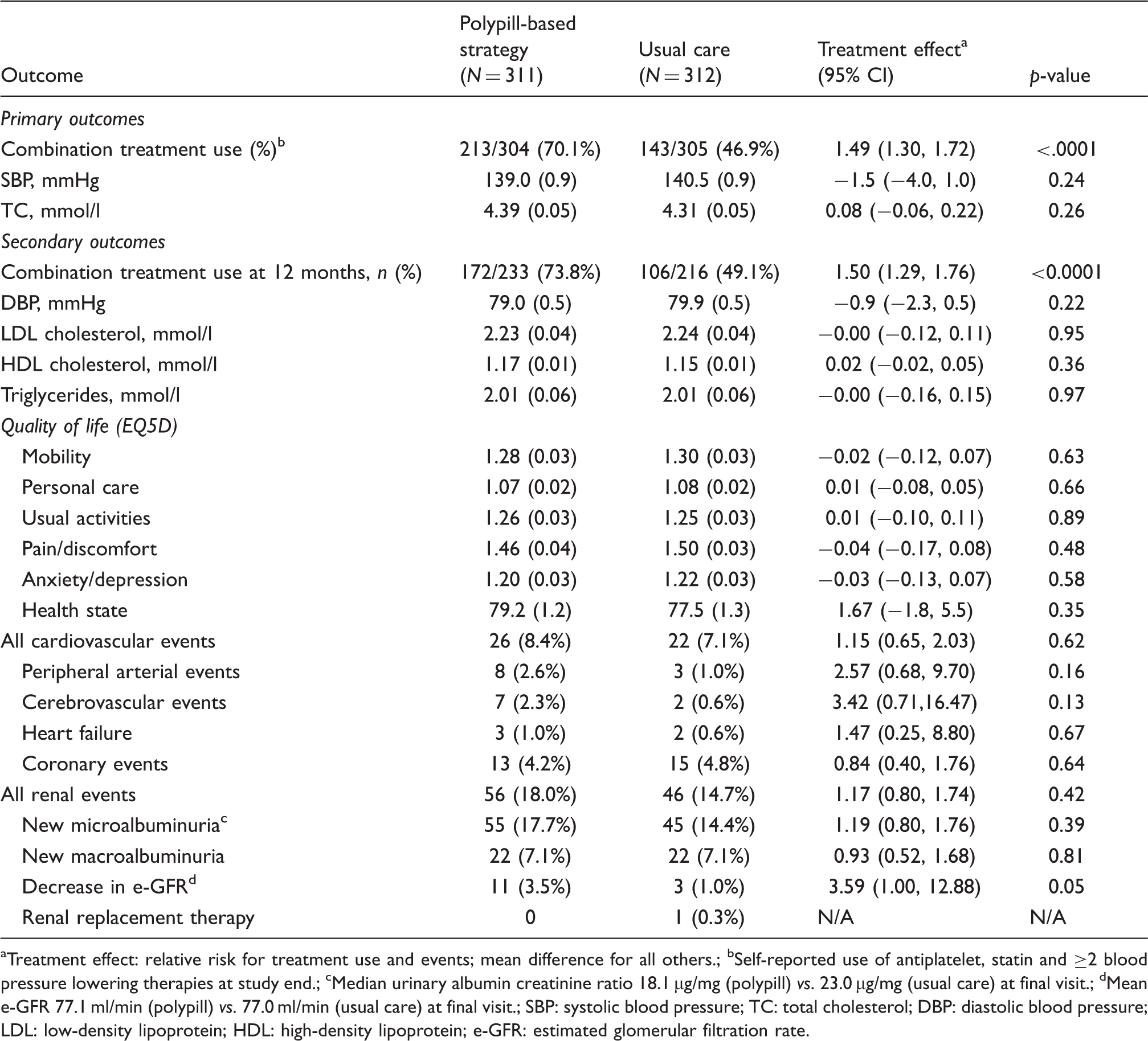
At study end, 70.1% of participants in the polypill-strategy group reported use of combination treatment, compared with 46.9% of the usual care group (relative risk (RR) 1.49; 95% confidence interval (CI) 1.30 to 1.72; p < 0.0001) (Table 2; Figure 2). This 23.2% absolute difference (95% CI 15.1% to 30.5%; p < 0.001) resulted in a number needed to treat of 4.4 patients (95% CI 3.3 to 6.6). Medication use of individual treatment modalities was also significantly improved with the polypill-based strategy for statins (RR 1.08 (95% CI 1.00 to 1.17)) and ≥2 BP lowering drugs (RR 1.31 (95% CI 1.17 to 1.46)), with a borderline non-significant effect for antiplatelets (RR 1.09 (95% CI 0.99 to 1.17)). With an alternative definition of combination treatment (statin, antiplatelet and ≥1 blood pressure lowering drug), the polypill-based strategy remained superior (RR 1.15; 95% CI 1.04 to 1.27; p = 0.006). This was also the case when combination treatment was defined as a statin and ≥2 BP lowering drugs (RR 1.40 (95% CI 1.23 to 1.59)).
Self-reported use of combination treatment by randomized group over follow-up. Effects of polypill-based strategy on primary and secondary outcomes. Treatment effect: relative risk for treatment use and events; mean difference for all others. Self-reported use of antiplatelet, statin and ≥2 blood pressure lowering therapies at study end. Median urinary albumin creatinine ratio 18.1 µg/mg (polypill) vs. 23.0 µg/mg (usual care) at final visit. Mean e-GFR 77.1 ml/min (polypill) vs. 77.0 ml/min (usual care) at final visit. SBP: systolic blood pressure; TC: total cholesterol; DBP: diastolic blood pressure; LDL: low-density lipoprotein; HDL: high-density lipoprotein; e-GFR: estimated glomerular filtration rate.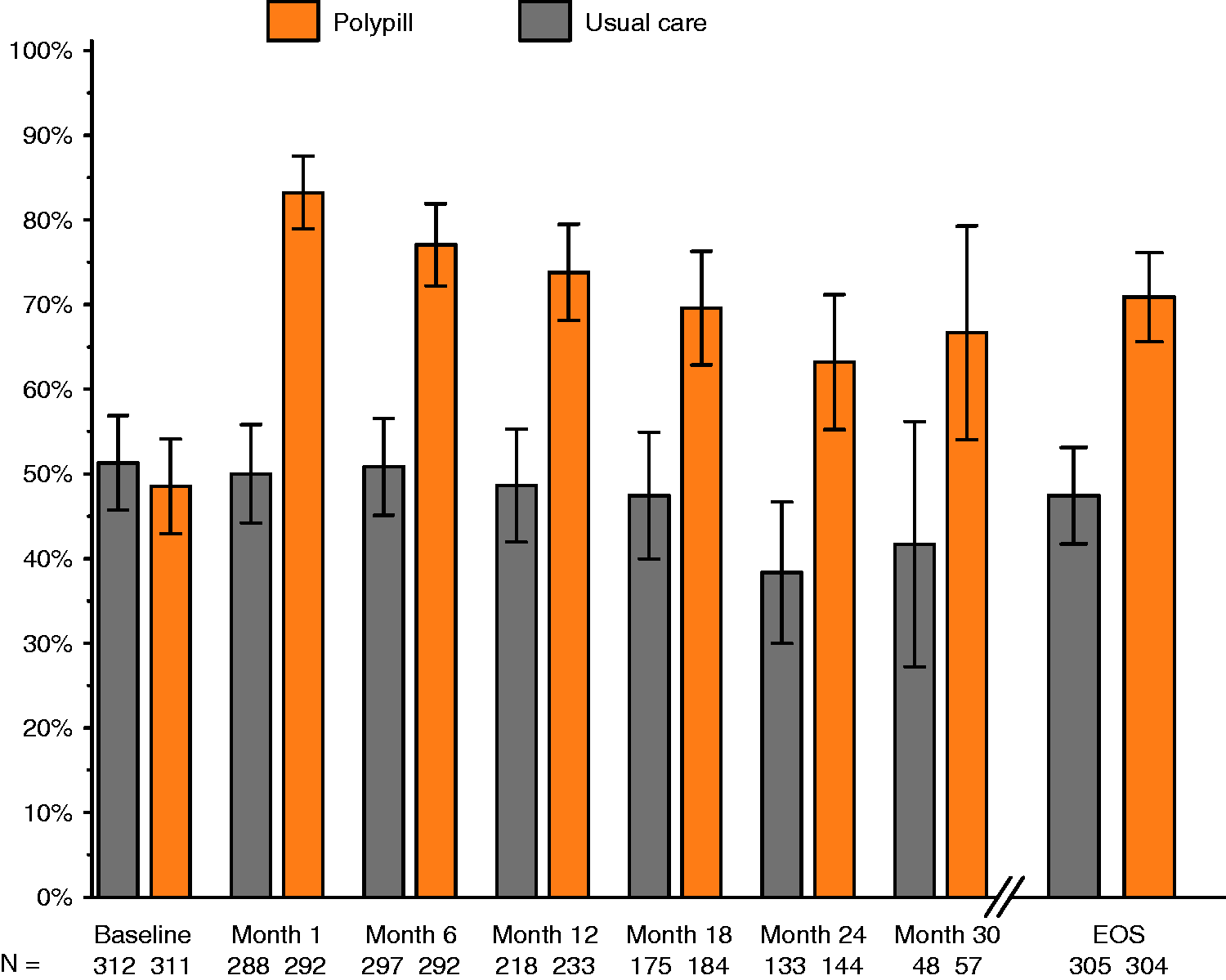
Statin use was also examined in greater detail. At baseline, 72% of participants using statins were taking atorvastatin or rosuvastatin; at study end this proportion was 67% and 17% in the usual care and polypill groups, respectively.
There were no significant differences between randomized groups for changes in systolic BP or total cholesterol (Table 2). Sensitivity analyses using end of study values showed only mean differences for systolic BP of −2.6 mmHg (95% CI –5.6 to 0.4 mmHg) and for total cholesterol of 0.08 mmol/l (−0.09 to 0.36 mmol/l).
Treatment effects on primary outcomes in pre-defined participant sub-groups
Pre-specified subgroup analyses are illustrated in Figure 3. For combination treatment use, two strong effect modifiers were identified – greater improvement with the polypill-based strategy if participants were not taking combination treatment at baseline and if participants had been included in the study on the basis of high-risk primary prevention (both p for heterogeneity <0.001). These variables were highly correlated. At study entry, 33.1% of participants reported combination treatment use in the high-risk primary prevention group, compared with 61.0% in the established CVD group. In 16 pre-specified BP and cholesterol subgroup analyses only one significant interaction was observed for total cholesterol and diabetes, which should be considered in light of multiple comparisons.
Primary outcomes in pre-specified subgroups.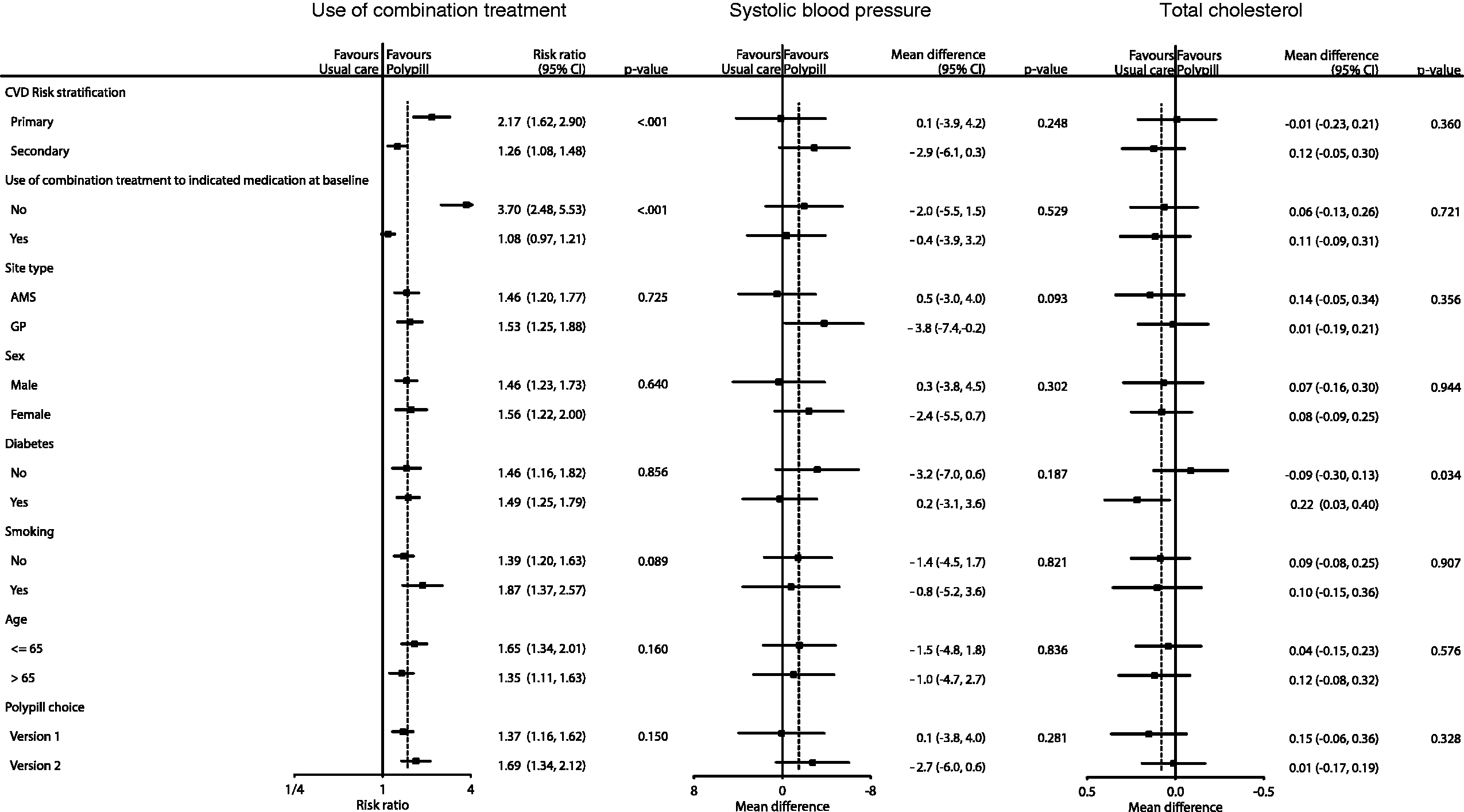
Effects on secondary outcomes
Table 2 summarizes the effects on secondary outcomes. Prescription of combination treatment at study end was greater among polypill group participants compared with those in usual care (RR 1.54; 95% CI 1.36 to 1.74; p < 0.001). Amongst participants prescribed combination treatment at study end by their usual doctor, the proportion reporting combination treatment use was higher in the polypill group than in the usual care group (82.2% vs. 72.0%; p = 0.016). There were no significant differences between randomized groups for changes in lipid fractions, quality of life measures or in the occurrence of cardiovascular or renal events. At least one serious adverse event was reported among 46.3% of participants allocated polypill-based strategy and 40.7% of those in the usual care group (p = 0.16) (Supplementary Table 1 online).
Polypill was discontinued in 90 (28.9%) patients randomized to the polypill group, with four patients subsequently recommencing polypill. The main reasons for permanent discontinuation were treating doctor decision (41.8% of withdrawals), patient choice (17.4%), cessation by a specialist or during hospitalization (15.1%), cough (15.1%) and dizziness/hypotension (5.8%). Among those who stopped polypill, 25 patients (27.8%) reported combination treatment use through separate medications at the final study visit.
Effects on lifestyle measures and related programs
Body weight (mean 88.7 vs. 88.7 kg), waist circumference (mean 106.3 vs. 107.3 cm) and body mass index (mean 31.0 vs. 31.5 kg/m2) were similar in the polypill and usual care groups at study end, and did not change significantly from baseline. Self-reported time engaged in moderate or vigorous physical activity, participation in exercise programmes, dietician consultations or diet programme use and participation in smoking cessation programmes were also similar between groups (data not shown).
Discussion
In contemporary Australian primary care, a polypill-based strategy for CVD prevention in high risk populations significantly improved self-reported use of indicated drug treatments. This was not accompanied by clear effects on systolic BP or total cholesterol levels. Improved use of combination treatment with a polypill-based strategy was greatest among individuals not taking combination treatment at study entry and among those who had not yet experienced a cardiovascular event.
The study failed to recruit the numbers of participants originally planned as a result of limited resources and was therefore under-powered to demonstrate significant differences in BP and cholesterol. The adherence outcome was a composite of adherence to all three treatment modalities, but there were smaller adherence improvements for each individual treatment modality. For BP, the most relevant improvement was in combination BP lowering medication from 58% to 76%. However, since combination BP lowering versus placebo achieves around a 10 mmHg systolic BP (SBP) difference in patients with similar BP profiles, this 18% absolute difference would be expected to result in only a 1.8 mmHg difference in SBP. This is virtually identical to the point estimate of intervention effect on SBP and entirely consistent with the CI around this estimate. The polypill-based strategy achieved similar cholesterol levels as usual care, in which more than two-thirds of patients received atorvastatin or rosuvastatin. Effectively, increased use of statins in the polypill group compared with usual care (84% vs. 77%) likely counter-balanced the use of more potent statins with usual care.
Availability of the polypill increased prescription of and patient adherence to prescribed indicated combination treatment for CVD prevention. This suggests that the beneficial effects of the polypill-based strategy are mediated through influencing behaviour of both the doctor (higher levels of prescription) and the patient (greater adherence to prescribed treatments).
The Kanyini GAP trial was designed to be highly pragmatic with the prescribing, dispensing and payment for polypill occurring identically to what would be usual care, if the polypill were to be marketed in Australia and subsidized through the Pharmaceutical Benefits Scheme. All patient care was provided through existing primary healthcare practices, with rural and remote communities included to ensure that ‘real-life’ variations in healthcare delivery were captured. This approach ensured that the results would be directly relevant to contemporary medical care. Nonetheless, prescription rates were higher than contemporary practice in both groups,3,4 suggesting that the study findings may be an underestimate of effects if a polypill strategy were to be implemented.
The study had other limitations. Trials that are unavoidably unblinded can have unintended differences between groups in diagnostic and therapeutic intensity that are difficult to measure. In this trial, the open design could have resulted in differential over-reporting of medication use, although consistent rates of this outcome pre- and post-randomization in the usual care group provides some reassurance. Also, including at least two BP lowering drugs in the definition of combination treatment could be questioned, although many patients with established CVD will have indications for at least two classes and most typically require a minimum of two BP lowering drugs to achieve targets. 25 Furthermore, antiplatelet use for high-risk primary CVD prevention remains controversial. Sensitivity analyses with alternative definitions of combination treatment that include only one BP lowering drug or exclude antiplatelets showed that the polypill-based strategy remained superior. However, of crucial importance, the treating doctor had to be satisfied that all components of at least one version of the polypill were indicated to include a patient in the study.
In 2005–2007, Indigenous Australians had an average life expectancy at birth that was 11.5 years and 9.7 years, respectively, less than that of their non-Indigenous male and female counterparts. 26 Subgroup analyses indicate that the polypill-based strategy was similarly effective in improving combination treatment use among participants from Aboriginal Medical Services and mainstream practices. As much of the premature mortality in Indigenous communities is attributable to cardiometabolic diseases,20,27 consistent relative benefits in averting cardiovascular events resulting from improvements in medication use might translate to particularly important absolute reductions in disease events, and contribute to closing the gaps in health outcomes.
The results of Kanyini GAP are consistent with those of the recently published UMPIRE trial, 28 which utilized a very similar protocol in a larger trial population (2004 participants from India, Ireland, the Netherlands and the United Kingdom). In UMPIRE, the polypill-based strategy was associated with a 33% (95% CI 26% to 41%) relative increase in combination treatment use, with significantly lower levels of systolic BP (−2.6 mmHg) and low-density lipoprotein (LDL) cholesterol (−0.11 mmol/l). Taken together, the UMPIRE and Kanyini GAP findings indicate comparable effects of the polypill-based strategy across diverse communities and health systems. In both trials, treatment effects were greatest among patients not taking combination treatment at baseline. This is a very large patient group in both richer and poorer countries globally, even if only considering those with established CVD. 2 The results of the two trials indicate that stepping these undertreated patients up to polypill-based care is safe and effective, in comparison with usual care. With a very small number needed to treat (NNT) to improve overall medication use, the potential role of polypill-based strategies in such populations globally is substantial.
In summary, cardiovascular polypills are likely to have a useful role in improving use of preventive treatments of known efficacy among individuals with established or at high risk of developing CVD. The availability of a range of polypills with variations in components and dosages would improve the flexibility of treatment options, although further trials would need to determine the extent to which this would translate to greater improvements in outcomes. From a policy perspective, key considerations will be patient and healthcare provider acceptability, as well as the potential impact on healthcare expenditure by governments and individuals. These will be addressed in forthcoming economic and process evaluations in Kanyini GAP.
Footnotes
Funding
This work was supported by the National Health and Medical Research Council of Australia (grant numbers 457508, 571281 and 632810).
Disclaimer
The funder and Dr Reddy’s Laboratories (who provided polypills free of charge for the trial) had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author contributions
AP and LB had full access to all of the data in the trial and take responsibility for the integrity and accuracy of the data analysis. AP, AC, NR and AR conceived and designed the study. LB and SB analysed the data. AP, AC, AR and LB wrote the first draft of the manuscript. DP, TU, AB, SJ, BN, GSH, NR, AT, RW and CMR contributed to the writing of the manuscript. AP, AC, DP, TU, AB, SJ, RW, CB, HB, NH, BM, CMR, LS and ST were responsible for study management and acquisition of data.
Conflict of interest
The George Institute for Global Health recently secured an exclusive global licence for the polypills used in this trial following a decision by Dr Reddy’s Laboratories Ltd not to proceed with taking the products to market because of existing regulatory requirements. The George Institute for Global Health has received funding from Dr Reddy’s Laboratories to support the secretariat of the SPACE Collaboration. AP, AC, DP, SJ and AR have received funding from Dr Reddy’s Laboratories to attend a SPACE Collaboration Investigators Meeting.
Acknowledgement
This trial is registered with the Australian New Zealand Clinical Trial Registry ACTRN126080005833347.
Appendix 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.