Young Investigator Award II - Prevention & Epidemiology and Sports Cardiology
Friday, 09 May 2014, 16:30-18:00
295
The impact of adopting new ECG interpretation criteria when screening an ethnically diverse cohort of athletes
NR Riding1, C Adamuz1, MG Wilson1
1Aspetar Orthopaedic and sports medicine hospital, Doha, Qatar
Topic: Rhythm Disorders/Sudden death (Sports Cardiology)
Introduction: Controversy still remains regarding the correct methodological approach when undertaking cardiovascular screening in athletes; predominantly focused upon the inclusion of the resting 12-Lead electrocardiogram (ECG). Antagonists continue to argue that unacceptably high false-positive rates warrant its exclusion. However recently, several groups of international experts have proposed new ECG interpretation criteria in the attempt to allow an athlete s ECG to be more accurately interpreted ('Seattle criteria', and Gati et al (2013)). Aim: To assess the specificity and sensitivity of 1) the Seattle Criteria and 2) the Gati Criteria against the validated2012 European Society of Cardiology (ESC)recommendations for 12-Lead ECG interpretation in athletes, within ethnically heterogeneous cohort of athletes.
Methods: 2361 male athletes presented at our institution for cardiovascular screening between Nov 2010 and Sept 2013. All athletes underwent a 12-lead ECG, personal symptom and family history questionnaire, brachial artery blood pressure assessment and a anthropometric and physical examination by a sports cardiologist. ECGs were assessed against three established recommendations; 1) 2012 ESC guidelines, 2) Seattle Criteria and 3) Gati Criteria – who propose the removal of isolated axis deviation and atrial enlargement from the abnormal criteria diagnostic algorhythm.
Results: From 2361 athletes screened, when using the ESC guidelines, 473 (20%) athletes presented an abnormal ECG. This was lowered to 206 (8.7%) and 165 (7%) when employing the Seattle and Gati Criteria respectively. Specificity improved from 81.57 to 90.91 and 93.4% when employing the two new criteria s respectively. The greatest improvement contributors to both criteria s were the reclassification of QTc cut-offs (increasing from >440 to >470ms and shortening from<360 to <320) together and the now considered benignity of T-wave inversion in V1-4 among African/Afro Caribbean athletes. Seven athletes with hypertrophic cardiomyopathy were identified by all 3 criteria, except for 1 athlete who presented with a normal ECG, but was identified via a positive physical examination. Consequently, sensitivity of 90.91% was demonstrated for all 3 criteria.
Conclusions: Whilst specificity remains the same, the continued improvements in ECG interpretation has led to enhanced specificity rates, and although the true false positive rate remains very high, both the Seattle Criteria and Gati Criteria reduce the number of unnecessary tests and associated cost incurred through further testing.
296
Differentiating physiological left ventricular hypertrophy from hypertrophic cardiomyopathy in athletes: Proposed echocardiographic protocol
A Malhotra1, N Sheikh1, A Siva1, H Dhutia1, H Dores1, L Millar1, A Merghani1, R Narain1, S Sharma1, M Papadakis1
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
Topic: Exercise/ Exercise training (Sports Cardiology)
Purpose: The differentiation between physiological left ventricular hypertrophy (LVH) and morphologically mild hypertrophic cardiomyopathy (HCM) is crucial and an erroneous diagnosis has potentially serious consequences.Day to day clinical practice most commonly utilises transthoracic echocardiography (ECHO) for this purpose.
The British Society of Echocardiography (BSE) recently produced a diagnostic algorithm to facilitate the differentiation between these two entities. This study aimed to validate the recommended echocardiographic parameters.
Methods: A cohort of 56 competitive athletes with LVH (maximal wall thickness >12mm) was evaluated. Of these, 19 were athletes with physiological LVH while 37 were diagnosed with HCM based on the results of comprehensive evaluation including cardiac MRI, familial evaluation and gene testing. The ECHO data were analyzed for 4 parameters: 1) S, average of septal and lateral walls (cm/s): >9 LVH vs <9 HCM; 2) E/A: >1 LVH vs <1 HCM; 3) E, average of septal and lateral walls (cm/s): >9 LVH vs <9 HCM; 4) E/E : <12 LVH vs >12 HCM.
Results: Athletes with physiological LVH were younger (24.7 vs 29.1 years, p=0.03) and exhibited a lower maximum left ventricular wall thickness (13.2 vs 16.4mm, p=0.05) compared to the athletes with HCM. A summary of the sensitivity, specificity, positive (PPV) and negative (NPV) predictive values of individual parameters to identify athletes with HCM is presented in table 1.
Conclusions: The current BSE guidelines are informative in helping differentiate physiological LVH from HCM in athletes. However, their sensitivity in identifying athletes with HCM is poor. Prior knowledge of patient demographics, clinical history and additional investigations should be taken into consideration to aid the interpretation of the echo data.
Table 1
Echo parameter
Sensitivity
Specificity
PPV
NPV
S' <9 cm/s
43%
84%
84%
43%
E/A ratio <1
5%
95%
56%
34%
E' <9cm/s
38%
100%
100%
45%
E/E' >12
14%
100%
100%
37%
297
How does the right ventricle adapt to high intensity endurance exercise? Insights from segmental myocardial deformation imaging
M Sanz1, G Grazioli1, B Bijnens2, C Pajuelo1, E Guasch1, E Subirats3, B Brotons4, R Brugada3, E Rocca3, M Sitges1
1Barcelona Hospital Clinic, Barcelona, Spain
2ICREA, Institució Catalana de Recerca i Estudis Avançats, Barcelona, Spain
3University of Girona, Girona, Spain
4Catalan Sports Council, Barcelona, Spain
Topic: Exercise/ Exercise training (Sports Cardiology)
Background: Endurance exercise competitions have shown a transient negative effect on global right ventricular (RV) performance (dilation and worsening function), but wide variability exists among individuals. We aimed at understanding the physiologic response to exercise of the RV performance in different individuals undergoing similar competitions.
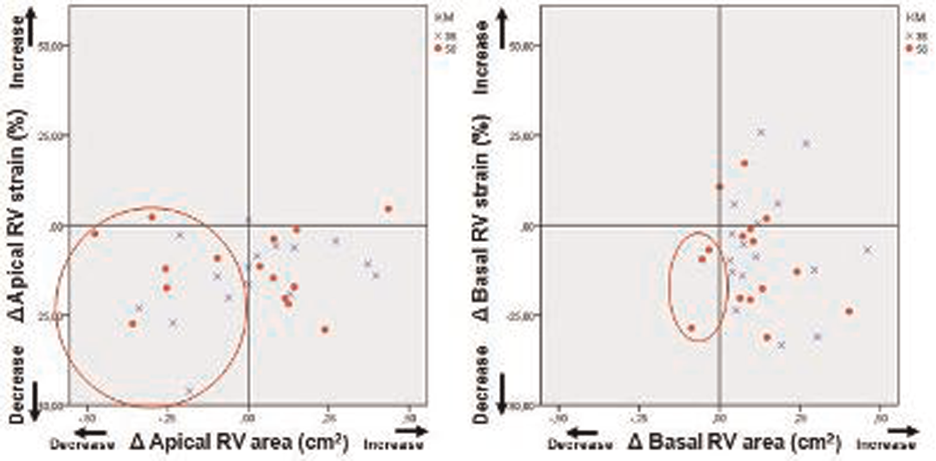
Methods: Echocardiography was performed at baseline and immediately after a cross-running race in 32 healthy adults, running 35 (n=16) and 56 km (n=16) distances. Analysis consisted on standard and speckle tracking echocardiographic assessment of RV and LV. RV basal (inflow) and apical regions were separately analyzed from the apical 4 chamber view.
Results: Global peak systolic RV strain significantly reduced after the race (?% -10.4%, p<0.01) while RV area increased (?% +9.27%, p<0.01) with a global increase in RV stroke volume (?% +18.0%, p<0.01). Figures show the change in apical and basal RV strain and area in the different individuals. The basal segment of the RV showed a major contribution by larger increases in size and strain as compared to the apex of the RV to the increased demand by exercise. Despite most runners showed an increase in either segmental RV strain or size (area) or both, some (red circles) showed drecrease in both size and strain depicting a group with worse adaptation of the RV to exercise.
Conclusions: The basal part of the RV contributes more to the ncrease in stroke volume during exercise. A proportion of individuals showed worse adaptation of the RV performance to exercise mainly by the inability of the RV apex to increase its size and deformation. The early identification of this ability, whether it is genetic or acquired among different individuals, should be investigated in further research.
298
Quantifying the impact of maintenance and changes of lifestyles on risk of cardiovascular disease and all-cause mortality: the doetinchem cohort study
G Hulsegge1, HA Smit2, YT Van Der Schouw2, ML Daviglus3, WMM Verschuren1
1National Institute for Public Health and the Environment (RIVM), Bilthoven, Netherlands
2University Medical Center Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, Netherlands
3Northwestern University, Department of Preventive Medicine, Chicago, United States of America
Topic: Other risk factors (Prevention & Epidemiology)
Background: It is not fully understood to what extent changes in lifestyle over time influence the risk of cardiovascular disease (CVD) and death among healthy adults, since most studies assessed lifestyle at a single point in time.
Objectives: To investigate the association of maintenance and changes in lifestyle profiles over 5 years with risk of CVD and all-cause mortality.
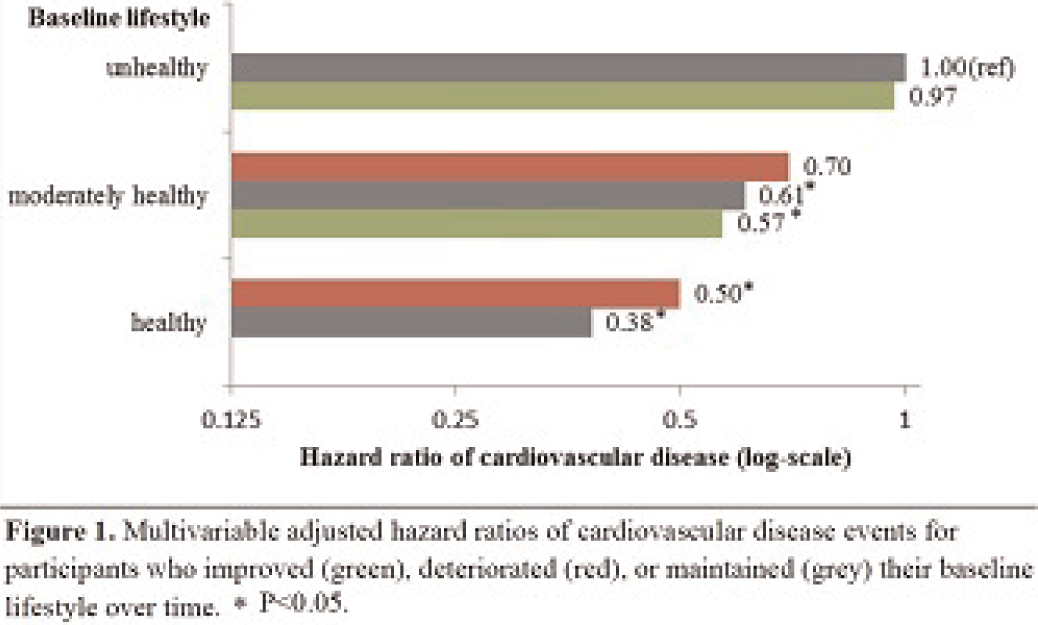
Methods: Healthy lifestyle factors (HLF), i.e., healthy diet, physically active, not smoking, moderate alcohol consumption, sufficient sleep duration, and normal weight were assessed among 5,290 CVD- and cancer-free adults aged 25-65 years in 1993-1997 (baseline examination). Participants were categorized as having unhealthy (0-2 HLF), moderately healthy (3-4 HLF), or healthy (5-6 HLF) lifestyles. They were subdivided as maintained, improved, or deteriorated HLF 5 years later (1998-2002). Multivariable-adjusted hazard ratios (HRs) and 95% confidence intervals (95%CI) for combined fatal and non-fatal CVD and all-cause mortality following the risk-change period were estimated using Cox proportional hazards models.
Results: Individuals who maintained their HLF had 62% lower risk of CVD (HR: 0.38, 95%CI: 0.23-0.64) (Figure 1) and 54% for all-cause mortality (HR: 0.46, 95%CI: 0.27-0.77) than those who maintained unhealthy lifestyles. In general, compared to maintenance of HLF, improvement and deterioration of HLF were associated with better or worse HRs than their baseline risks for CVD and all-cause mortality, respectively.
Conclusions: Maintenance of a healthy lifestyle is associated with significant and independent low risk of CVD and all-cause mortality. Effort is needed to improve the adoption and maintenance of a healthy lifestyle.
Figure 1.
299
The european obese model: the shape of things to come
L Webber1, D Divajeva1, TIM Marsh1, M Brown1, T Wijnhoven1, J Breda1
1National Heart Forum, London, United Kingdom
Topic: Obesity (Prevention & Epidemiology)
Purpose: Noncommunicable diseases (NCD) are the biggest cause of death in Europe. Trends in obesity pose a new threat that needs to be quantified at National and Regional level. It is also putting unsustainable burden on already struggling health systems. This paper projects the future burden of Coronary Heart Disease (CHD) and stroke to 2030 in all 53 WHO European-Region countries based on current and past obesity trends. It also tests the eventual impact of effective obesity interventions upon the future disease burden.
Methods: A two module modelling process was used. Module one uses a non-linear multivariate, categorical regression model fitted to cross-sectional country-specific Body Mass Index (BMI) data. Module 2 uses a micro simulation programme to produce longitudinal projections to 2030. The effect of three hypothetical interventions on the future disease were tested: Baseline intervention, BMI trends go unchecked; intervention 1, BMI trends decrease by 1%; intervention 2, BMI levels decrease by 5%.
Results: By 2030, rates CHD and stroke are projected to reach an average of 1604 cases per 100,000 of the population across Europe. The highest increased incidence of CHD and stroke was projected in Austria, Latvia and Turkey where >2500 cases were predicted by 2030.
Conclusions: Modelling future disease trends is important for policy makers in realistically allocating resources and implementing policies that prevent disease incidence. Future research will allow real policy interventions to be tested, however better surveillance data on NCDs and their risk factors are particularly important if accurate estimates of future trends are to be quantified.
300
Seasonality of cardiovascular mortality: a worldwide analysis of 61 million deaths
C Gubelmann1, S Gonseth1, H Marti-Soler1, S Stringhini1, P Bovet1, P-C Chen2, B Wojtyniak3, D Tsai1, T Zdrojewski4, P Marques-Vidal1
1University Institute of Social and Preventive Medicine Lausanne (IUMSP), Lausanne, Switzerland
2National Taiwan University, Taipei, Taiwan
3National Institute of Public Health, Warsaw, Poland
4Medical University of Gdansk, Department of Hypertension and Diabetology, Gdansk, Poland
Topic: Other risk factors (Prevention & Epidemiology)
Purpose: Cardiovascular disease (CVD) mortality has been shown to follow a seasonal pattern. Whether this pattern is factual or due to misclassification errors remains controversial. We aimed at assessing seasonality in CVD mortality based in data from many countries in different geographical locations, using cancer mortality as a control.
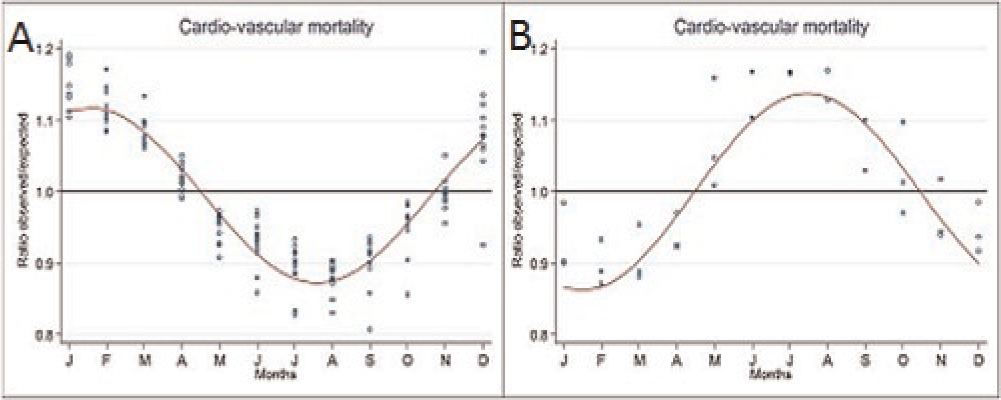
Methods: Mortality statistics were drawn from 19 countries, amounting to over 61 million deaths (16.8 for CVD and 11.9 for cancer). Seasonality for CVD and cancer mortality was analyzed using the cosinor function. The association between seasonal variation (peak to nadir difference) of CVD and cancer mortality and a country s latitude was also assessed.
Results: Mortality from CVD showed a consistent seasonal pattern. In the northern hemisphere, the number of CVD deaths was higher than expected in winter (December-January) and lower than expected in summer (July-August) months (Figure A, data adjusted for age, density of doctors, density of hospital beds and GDP per capita). Virtually no seasonal variation was seen in countries close to the equator, while an inverse pattern was found in the Southern hemisphere with more CVD deaths in July-August than in December-January (Figure B). Seasonal variation was smallest near the equator and increased with latitude till ±40○ in both hemispheres. In the Northern hemisphere, seasonal variation tended to decrease after 40○ latitude, while no such pattern was found in the Southern hemisphere. For cancer mortality, there was little or no seasonal variation in nearly all countries (data not shown).
Conclusions: CVD mortality varies according to season, being higher in winter and lower in summer. This seasonal pattern is associated with a country s latitude.