
Abstract
Aims
Children conceived by assisted reproductive technology (ART) display vascular dysfunction. Its underlying mechanism, potential reversibility and long-term consequences for cardiovascular risk are unknown. In mice, ART induces arterial hypertension and shortens the life span. These problems are related to decreased vascular endothelial nitric oxide synthase (eNOS) expression and nitric oxide (NO) synthesis. The aim of this study was to determine whether ART-induced vascular dysfunction in humans is related to a similar mechanism and potentially reversible. To this end we tested whether antioxidants improve endothelial function by scavenging free radicals and increasing NO bioavailability.
Methods and results
In this prospective double-blind placebo controlled study in 21 ART and 21 control children we assessed the effects of a four-week oral supplementation with antioxidant vitamins C (1 g) and E (400 IU) or placebo (allocation ratio 2:1) on flow-mediated vasodilation (FMD) of the brachial artery and pulmonary artery pressure (echocardiography) during high-altitude exposure (3454 m), a manoeuver known to facilitate the detection of pulmonary vascular dysfunction and to decrease NO bioavailability by stimulating oxidative stress. Antioxidant supplementation significantly increased plasma NO measured by ozone-based chemiluminescence (from 21.7 ± 7.9 to 26.9 ± 7.6 µM, p = 0.04) and FMD (from 7.0 ± 2.1 to 8.7 ± 2.0%, p = 0.004) and attenuated altitude-induced pulmonary hypertension (from 33 ± 8 to 28 ± 6 mm Hg, p = 0.028) in ART children, whereas it had no detectable effect in control children.
Conclusions
Antioxidant administration to ART children improved NO bioavailability and vascular responsiveness in the systemic and pulmonary circulation. Collectively, these findings indicate that in young individuals ART-induced vascular dysfunction is subject to redox regulation and reversible.
Introduction
Studies in experimental animals and humans demonstrate that adverse events during early life cause alterations of cardiovascular function that may increase cardiovascular risk later in life. 1 The recent observation of generalized vascular dysfunction in children conceived by assisted reproductive technology (ART) provides another example of this problem, but the underlying mechanism is unknown.2,3 To provide insight into underpinning mechanisms we studied ART mice. We found that ART mice display endothelial dysfunction and arterial hypertension 4 which are related to decreased vascular endothelial nitric oxide synthase (eNOS) expression and nitric oxide (NO) synthesis caused by epigenetic alterations of the eNOS gene. 4
We speculated that a similar mechanism contributes to vascular dysfunction in ART children. In humans with endothelial dysfunction, antioxidant vitamins improve endothelial function by scavenging free radicals and increasing NO bioavailability.5,6 To test this hypothesis, we performed a prospective double-blind placebo controlled study in ART and control children to assess the effects of a four-week antioxidant supplementation with vitamins C and E on systemic and pulmonary vascular function during high-altitude exposure (3454 m), a manoeuver known to facilitate the detection of pulmonary vascular dysfunction and to decrease NO bioavailability by stimulating oxidative stress.7–9
Methods
Study design
This was a single-center, randomized, double-blind, placebo-controlled trial in ART and age- and gender-matched healthy control children. The participants were exposed to high altitude (3554 m) during 48 h, the first time without any treatment, the second time after four weeks with oral supplementation with antioxidant vitamins or placebo (Figure 1). The allocation ratio was 2:1 for treatment with antioxidant vitamins or placebo.
Flow chart of the study design. ART: assisted reproductive technology.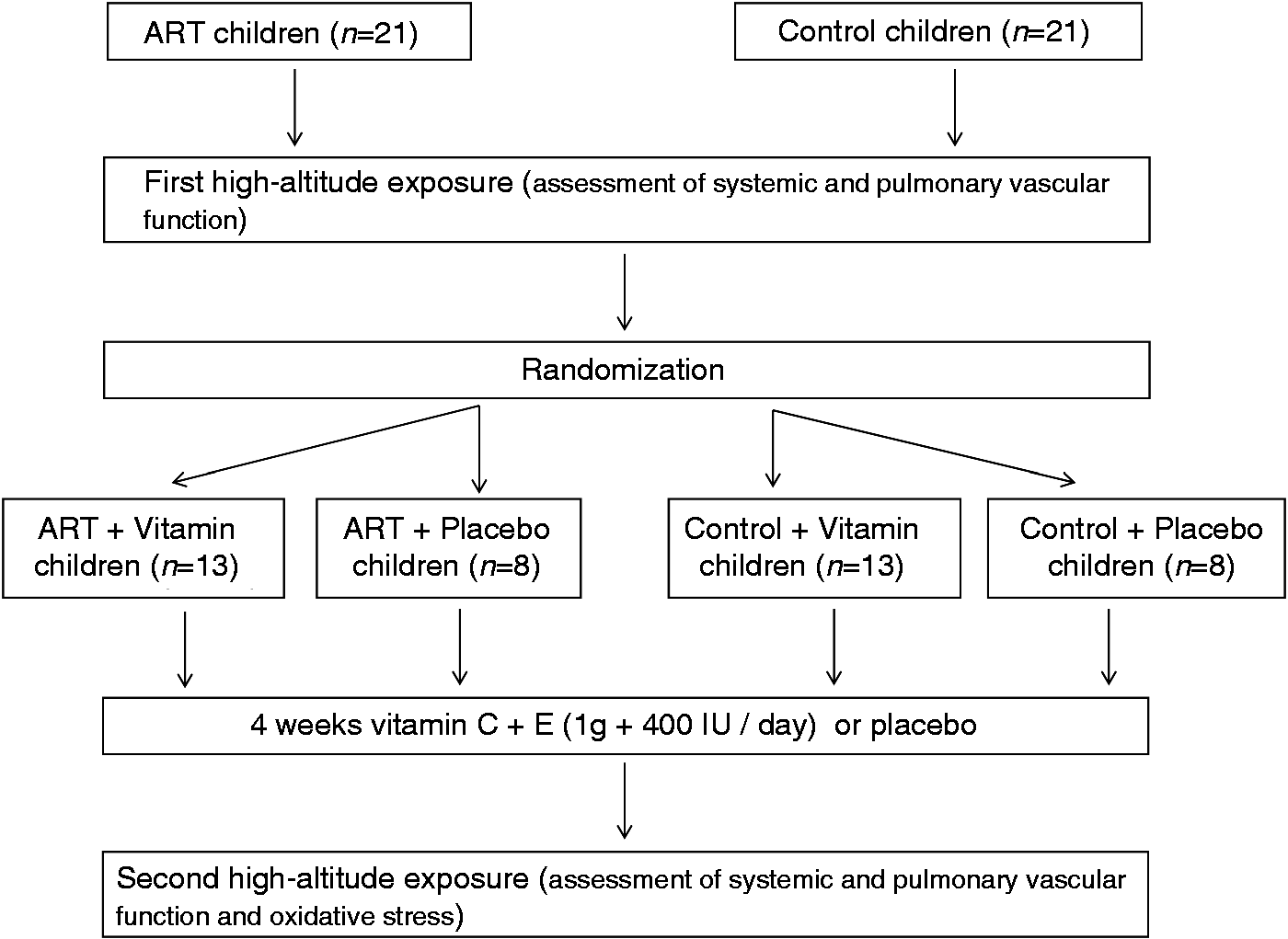
Participants
We recruited 21 children conceived by ART and 21 age-and gender-matched healthy controls. Children conceived by ART and control children who had participated in a previous high-altitude study 3 were contacted by letter, and those who agreed to participate and met the inclusion criteria were recruited. Inclusion criteria were: singletons, born at term (>37 weeks gestational age) with normal birth weight (>2500 g) and without any gestational or perinatal complications. Exclusion criteria included any acute illness or medical treatment, high altitude (>2500 m) exposure during the last three months preceding the study. None of the participants was taking any antioxidant/anti-inflammatory preparations/supplements known to influence the redox state.
Setting and data collection
All measurements were performed at high altitude (Jungfraujoch, 3554 m, Switzerland). The children ascended to the high-altitude research station by train and spent two days and two nights at this laboratory. Measurements were performed on the morning before descent.
Interventions
Five weeks before the second high-altitude exposure, each participant received two packs, one labeled vit C/placebo (60 pills, one pill containing 500 mg ascorbic acid, Burgerstein Vitamin C retard, ref. 08164/09 or corresponding placebo) the other labeled vit E/placebo (30 pills, one pill containing 400 IU α-tocopherol, Burgerstein Vitamin E, ref. 263226 or corresponding placebo), with the personal code, the name and surname of the participant and the starting and finishing date of the treatment. Beginning on the date indicated on the packs, for 28 days each participant took two pills every morning from the pack labeled vit C/placebo and one pill from the pack labeled vit E/placebo. The total daily dose was 1 g vitamin C and 400 IU vitamin E. To assess adherence, each participant completed a daily questionnaire and the number of remaining pills was counted at the end of the treatment. Participants were encouraged to follow a low nitrate/nitrite diet prior to and throughout the duration of the study with specific instructions to avoid fruits, salads and cured meats. 10
Procedure
The protocol was approved by the institutional review board on human investigation of the University of Lausanne (Protocol # 17/09), Switzerland, and was registered (www.clinicaltrials.gov; registration No. NCT00837642). All parents provided written informed consent. Randomization was performed via a computer-based system generating an allocation sequence in randomly varying blocks. All participants and investigators were blinded.
Main outcome and measures
Primary outcomes were: changes in systemic vascular function assessed by flow-mediated vasodilation (FMD) of the brachial artery and carotid-femoral pulse wave velocity (PWV), and changes in pulmonary vascular function assessed by estimation of pulmonary artery pressure using Doppler echocardiography. The secondary end point was the intra-individual change in the plasma concentration of nitric oxide.
Assessment of systemic vascular function
Systemic vascular function was examined after 15 min of rest in the supine position in a temperature-controlled room (22℃) using gold standard methods to non-invasively assess endothelial function and arterial stiffness.11–13 Systemic conduit artery endothelial function was assessed by measuring the increase of the brachial artery diameter evoked by reactive hyperemia induced by a pressure cuff placed around the distal forearm with a high-resolution ultrasound probe (Acuson Sequoia C 512; Acuson Siemens, Mountain View, California, USA) and using an automatic wall tracking software (FMD Studio, Computer Vision Group, Pisa, Italy) according to international guidelines14,15 and as previously described.3,16–18 The coefficient of variation between two measurements in the same 30 subjects 24 h apart was 5.2%. 3 FMD was expressed as the maximal percentage change in vessel diameter from baseline.
Large artery stiffness was assessed non-invasively by measuring carotid-femoral PWV with the Complior device (Artech Medical, Pantin, France) according to international guidelines as described previously.3,18 The coefficient of variation between two measurements in the same 30 subjects 24 h apart was 6.3%. 3
Assessment of pulmonary vascular function
To estimate systolic pulmonary artery pressure and cardiac output, echocardiographic recordings were obtained with a real-time, phased-array sector scanner (Acuson Sequoia C 512; Acuson Siemens, Mountain View, California, USA) as previously described.3,17,19,20 Briefly, after tricuspid regurgitation had been localized with Doppler color-flow imagining, the pressure gradient between the right ventricle (RV) and the right atrium (RA) was calculated using the modified Bernoulli equation. In children at this altitude, the intra- and inter-observer variability of the RV-RA pressure gradient measurements (n = 30) was 5.1 and 6.0% respectively. 20 Cardiac output was assessed as previously described 20 and cardiac index was calculated by dividing cardiac output (l/min) by the body surface area (m2).
Arterial oxygen saturation and heart rate
Transcutaneous arterial oxygen saturation and heart rate were measured at a fingertip with a pulse oxymeter (OxiMax N-65, Nellcor, Pleasanton, California, USA).
Metabolic assessment
All subjects provided a 12-hour overnight-fasting, resting, blood sample from a catheter located in a forearm antecubital vein. Samples were immediately centrifuged at 600 g (4℃) for 10 min; the supernatant (K-EDTA plasma) was snap-frozen without delay and stored under liquid nitrogen prior to transport (Cryopak CP100; Taylor-Wharton International) for batch analysis.
Nitric oxide (NO)
Ozone-based chemiluminescence (OBC Model 280i; NOA, Sievers, Boulder, Colorado, USA), arguably the most sensitive technique for the molecular detection of NO in human blood was employed for the detection of plasma and red blood cell (RBC) bound NO metabolites.
Samples (20 µl) were analyzed for the total concentration of plasma NO (nitrate + nitrite + S-nitrosothiols) by vanadium (III) reduction. 21 All calculations were performed using Origin/Peak Analysis software. The intra- and inter-assay coefficients of variation were 7% and 10%, respectively.
Ascorbate radical
Direct detection of the long-lived ascorbate radical (A•–) was employed as a measure of “global” free radical formation using X-band (9.79 GHz) electron paramagnetic resonance spectroscopy (Bruker, Karlsruhe, Germany) as previously described. 16 K-EDTA plasma (1 ml) was injected into a high-sensitivity multiple-bore sample cell (AquaX, Bruker Instruments Inc., Billerica, USA) and the characteristic doublet of A•– (aH β = 1.76 G) was recorded 12 min after the end of plasma recovery by signal averaging three scans with the following parameters: resolution, 1024 points: microwave power, 20 mW; modulation amplitude, 0.65 Gauss (G); receiver gain, 2 × 105; time constant, 40.96 ms; sweep rate, 0.25 G/s and sweep width, 15 G. All spectra were filtered identically using Bruker WinEPR 2.11 software and the double integral calculated using Origin software. The intra- and inter-assay coefficients of variation were both <10%.
Antioxidants
Plasma was stabilized and deproteinated by adding 900 µl of 5% metaphosphoric acid (Sigma Chemical, Dorset, UK) to 100 µl K-EDTA plasma. Ascorbic acid was subsequently assayed by fluorimetry based on the condensation of dehydroascorbic acid with 1,2-phenylenediamine. 22 Concentrations of lipid soluble antioxidants were determined using HPLC.23,24 The intra and inter-assay coefficients of variation were both <5%. Due to limited place for transportation of samples under liquid nitrogen, antioxidants were assessed only during the second high altitude exposure, following prophylaxis with antioxidant vitamins or placebo.
Statistical analysis
A prospective sample size calculation was performed on the basis of previously reported data in ART children 3 and in children exposed to high altitude. 17 Assuming an intra-individual difference in FMD of 1.5% as a clinically significant change (standard deviation (SD) of 1.5%, power >0.90; α = 0.05), we calculated that 13 subjects were required, assuming no dropout.
Statistical analysis was done with the GraphPad Prism 5 software package (GraphPad Software Inc, San Diego, California, USA). Paired and unpaired two-tailed t-tests were used for group comparisons of continuous variables. A value of p < 0.05 was considered to indicate statistical significance. Unless otherwise indicated, data are given as mean ± SD.
Results
Participant characteristics.
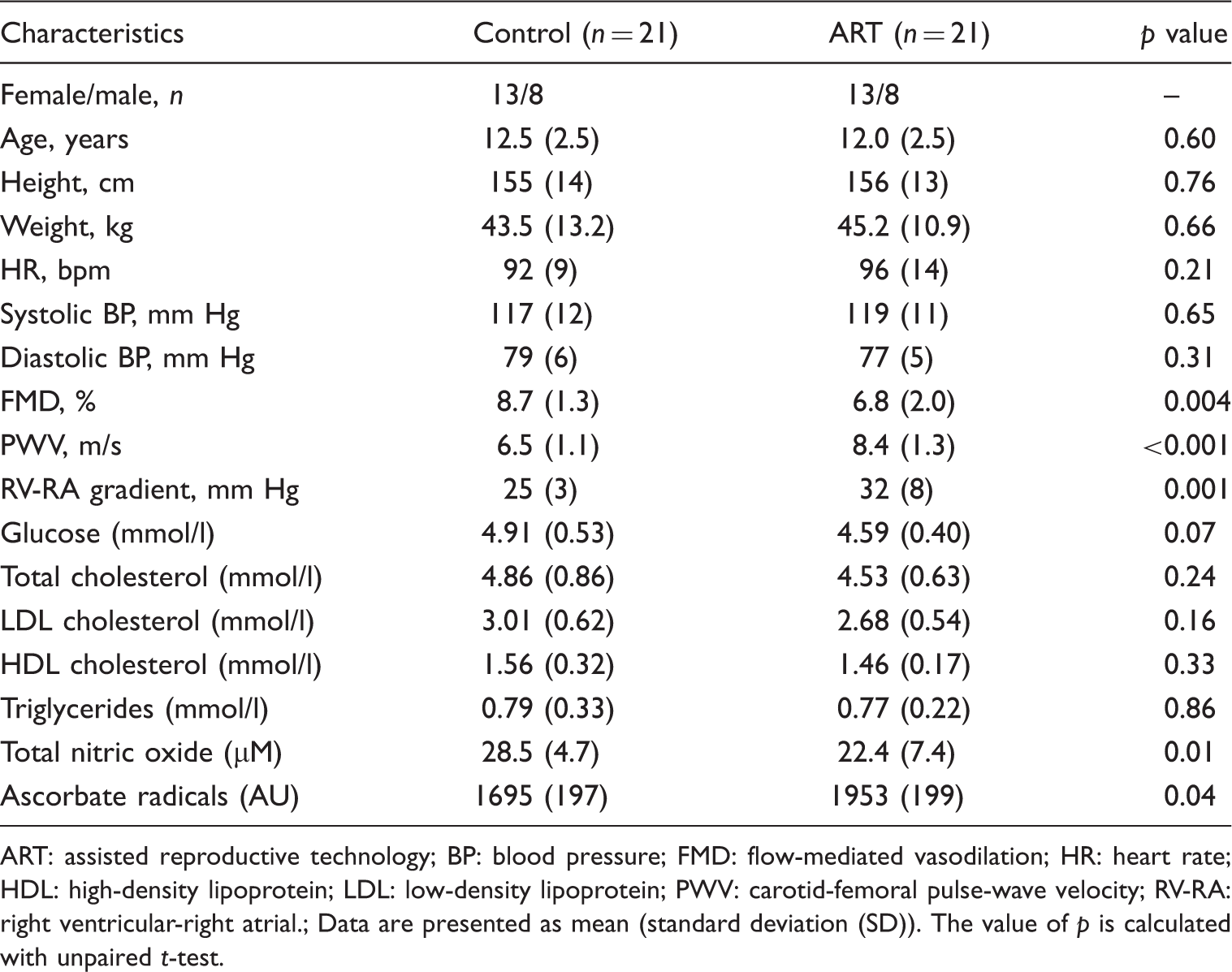
ART: assisted reproductive technology; BP: blood pressure; FMD: flow-mediated vasodilation; HR: heart rate; HDL: high-density lipoprotein; LDL: low-density lipoprotein; PWV: carotid-femoral pulse-wave velocity; RV-RA: right ventricular-right atrial.
Data are presented as mean (standard deviation (SD)). The value of p is calculated with unpaired t-test.
Vascular data
Antioxidant supplementation significantly improved systemic endothelial function in ART children (Figure 2(a), Table 2), whereas it had no detectable effect in control children (Table 2). Similarly, antioxidant administration tended (p = 0.06) to attenuate vascular stiffness in ART children, but had no effect in control children (Table 2). Placebo administration had no detectable effect on flow mediated vasodilation (6.5 ± 1.8 vs 7.2 ± 1.5%, placebo vs vitamin, p = 0.25) or pulse wave velocity (7.9 ± 1.3 vs 7.3 ± 0.9 m/s, before vs after placebo, p = 0.22) in ART children and control children (data not shown).
Hemodynamic and metabolic effects of antioxidant administration in assisted reproductive technology (ART) children. Effects of four-week oral antioxidant supplementation with vitamins C and E on (a) flow-mediated vasodilation (FMD), (b) right-ventricular-to-right atrial pressure gradient (RV-RA gradient), (c) plasma total nitric oxide (NO) and (d) plasma ascorbate radical (A-) in ART children. Data represent mean ± standard error of the mean (SE) for 13 children. VIT: vitamin. Systemic and pulmonary vascular function during high altitude exposure in assisted reproductive technology (ART) and control children before and after four weeks of treatment with vitamin C and E. BP: blood pressure; FMD: flow-mediated dilation; HR: heart rate; PWV: carotid-femoral pulse wave velocity. RV-RA: right ventricular – right atrial. CI: Cardiac Index: SaO2: arterial oxygen saturation. Data are presented as mean (standard deviation (SD). The value of p is calculated with paired t-test.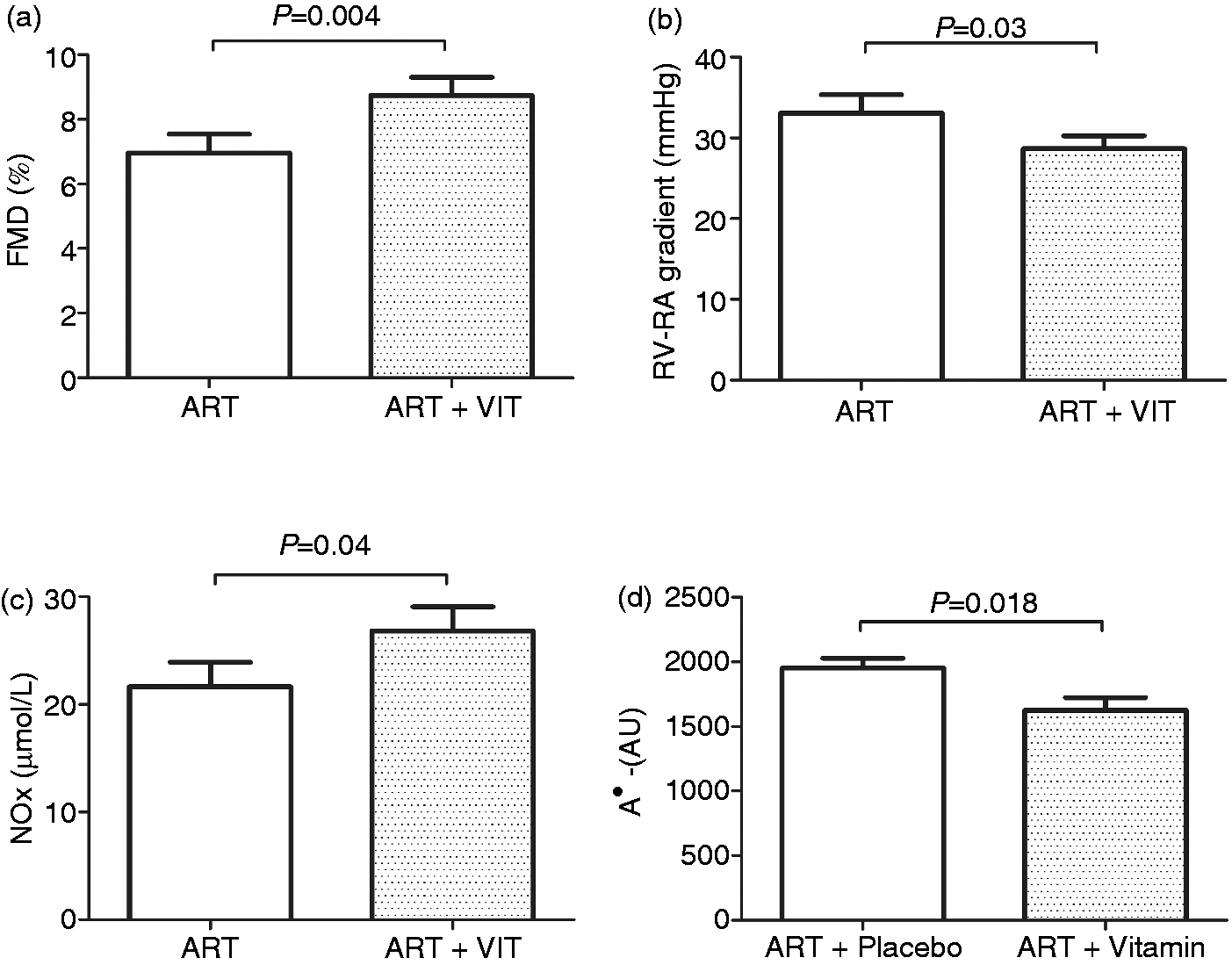
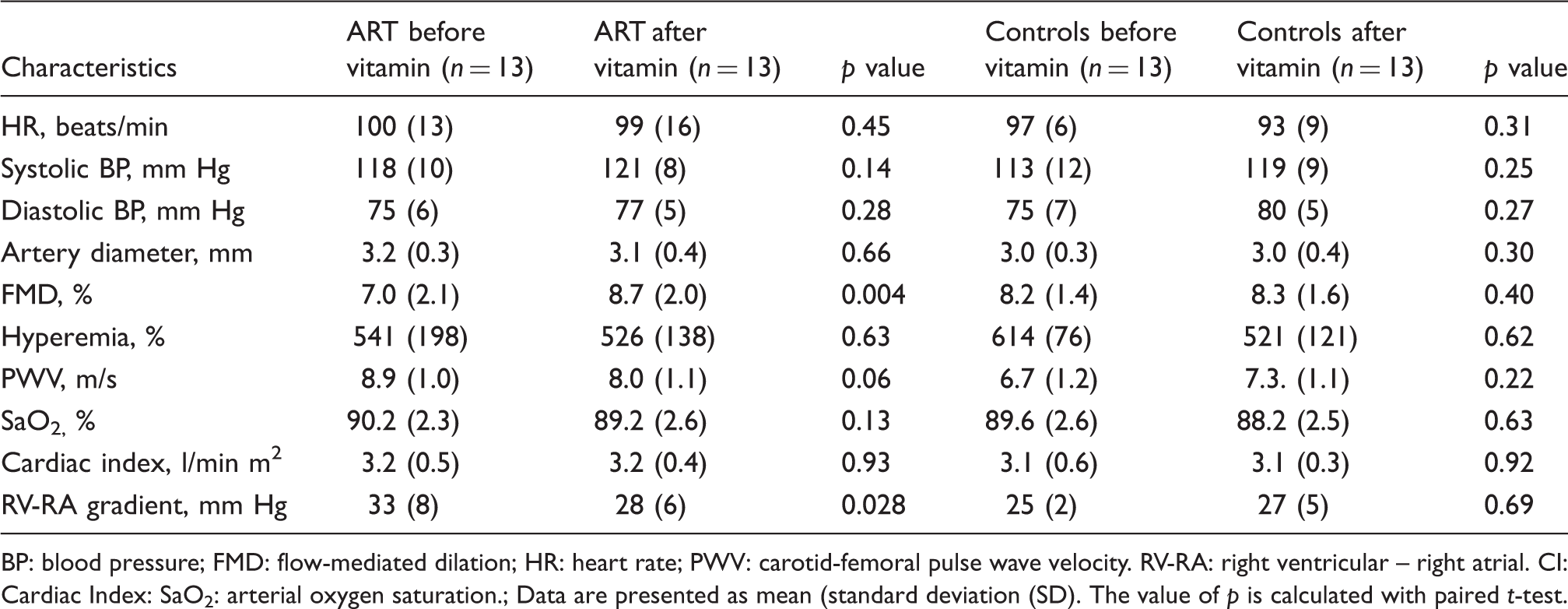
The RV-RA gradient was significantly lower in ART children after four weeks of antioxidant treatment (Figure 2(b), Table 2), whereas it remained unchanged in control children (Table 2). Placebo administration had no detectable effect on pulmonary artery pressure in ART (32 ± 7 vs 29 ± 3 mm Hg, p = 0.24) and control children (data not shown). Antioxidant administration did not alter heart rate, arterial blood pressure, cardiac index or arterial oxygen saturation (Table 2) in the two groups.
Metabolic data
Table 1 shows that plasma A•– was significantly elevated in ART compared to control children (1953 ± 199 vs 1695 ± 197 AU, p = 0.04) whereas total plasma NO was significantly lower in ART than in control children (22.4 ± 7.4 vs 28.5 ± 4.7 µM, p = 0.01). In participants receiving placebo, ascorbate (81.4 ± 8.9 vs 76.8 ± 12.0 µmol/l, p = 0.48, ART vs controls) and α-tocopherol levels (28.0 ± 2.2 vs 26.7 ± 2.5 µmol/l, p = 0.31, ART vs controls) were comparable in ART and control children.
Ascorbic acid and α-tocopherol were significantly higher during vitamin C and E than during placebo administration in ART and control children (data not shown), confirming compliance with the intervention. Antioxidant treatment normalized plasma A•– (1625 ± 328 AU, p > 0.05 vs controls, p < 0.02 vs ART plus placebo: Figure 2(d)) and significantly increased plasma nitric oxide (from 21.7 ± 7.9 to 26.9 ± 7.6 µM, p = 0.04) in ART children (Figure 2(c)), whereas it had no detectable effect on these two variables in control children (data not shown). Placebo administration had no detectable effect on plasma A•– and plasma NO in the two groups.
Discussion
The steadily increasing use of ART has allowed millions of infertile couples to have children, who now make up 2–4% of births in industrialized countries. 25 The recent observation of systemic vascular dysfunction and premature atherosclerosis in young apparently healthy ART children suggests that millions of individuals may possibly be at increased cardiovascular risk later in life. 3 In line with this concern, in mice generated by ART vascular dysfunction and arterial hypertension are associated with a decreased life span. 4 Here, we show for the first time that vascular dysfunction in ART children is associated with increased oxidative stress and decreased plasma nitric oxide. Antioxidant administration normalized oxidative stress and plasma nitric oxide and improved endothelial function in the systemic and pulmonary circulation. These data provide proof of principle that in young individuals ART-induced vascular dysfunction is subject to redox-regulation and eminently reversible.
Systemic endothelial dysfunction is considered to represent the first step in the development of atherosclerosis and has consistently been demonstrated in children at increased cardiovascular risk.5,26–28 Similarly, elastic artery stiffness is another independent cardiovascular risk predictor.13,29 Here, we found that oral supplementation with antioxidant vitamins for one month normalized systemic endothelial function and tended to improve arterial stiffness. Improvement of vascular function in ART children was not limited to the systemic circulation, as evidenced by the normalization of the altitude-induced increase of pulmonary artery pressure, an effect that was not related to changes in altitude-induced hypoxemia, since vitamin administration had no effect on this parameter. These favorable effects of antioxidant administration on systemic and pulmonary vascular function were specific for ART children, since vitamins had no detectable effect on vascular function in control children.
The present data also provide insight into potential mechanisms underpinning ART-induced vascular dysfunction in these young children. In mice, ART-induced vascular dysfunction is related to epigenetic alterations of the eNOS gene leading to decreased eNOS expression in vascular tissue and decreased plasma NO. 4 Here, we found that oxidative stress was increased in ART children and associated with significantly lower plasma NO compared to control children. Vitamin administration normalized oxidative stress and plasma NO in ART children. Restoring NO bioavailability was associated with normalization of systemic endothelial function. In line with this observation, antioxidant vitamin administration has been shown to improve endothelial function in children at increased cardiovascular risk. 5 Taken together, these observations suggest that defective NO synthesis and increased oxidative stress contribute to ART-induced vascular dysfunction in humans.
However, we would like to emphasize that given the differences in biomolecular rate constants as outlined, for vitamin C (as but one example), to compete effectively with NO for any given concentration of superoxide, its concentration within the plasma and extracellular fluids must exceed that of NO by a factor of 105. This would equate to a supraphysiological (pharmacologically-induced) circulating ascorbate concentration of ∼ 10 mmol/l 30 which is clearly two orders of magnitude greater than the concentrations achieved through oral administration.
Thus we, like others,31,32 can only speculate as to the precise mechanisms that allow oral antioxidant prophylaxis to increase NO bioavailability and improve vascular function. These vitamins have the capacity to scavenge other radical species including peroxyl and alkoxyl radicals. Indeed, our previous studies have demonstrated that a single oral dose of these chain-breaking antioxidants can improve endothelial-dependent vasodilation and blood flow due to their ability to selectively scavenge alkoxyl radicals detected by electron paramagnetic resonance (EPR) spin-trapping. 33 Given that alkoxyl radicals have previously been associated with vascular endothelial dysfunction, 34 their reduction may prove one of the fundamental mechanisms underpinning the vascular improvements observed in the current study. Though speculative, the liberation of vascular NO may prove the consequence rather than simply the cause of a free radical-mediated improvement in blood flow and associated elevation in shear stress.
Equally, though beyond the scope of the present study, ascorbate has the capacity to preserve the intracellular concentration of reduced glutathione, an important thiol species that plays a central role in the regulation of intracellular redox state. 35 Depletion of reduced thiol leads to decreased synthesis of NO in cultured endothelial cells subsequent to a reduction in NO synthase activity and/or bioavailability of essential cofactors including flavin adenine dinucleotide (FAD), tetrahydrobiopterin, and nicotinamide adenine dinucleotide phosphate (NADPH). 36 Increased availability of reduced thiol species has also been shown to potentiate the effects of NO on shear stress–mediated NO release. 37 Thus, it has been suggested that elevated intracellular ascorbate following oral prophylaxis (equivalent to the plasma concentrations achieved in the present study) could increase the bioavailability of reduced thiol and thus improve FMD through increased synthesis of NO and/or stabilization of NO. 31
Large clinical studies showed contrasting results regarding the effects of antioxidant vitamins on cardiovascular morbidity and mortality risk.38–40 However, most studies failing to demonstrate favorable effects included patients at high cardiovascular risk with established atherosclerotic changes that are unlikely to be reversible with antioxidant therapy. In contrast, studies in children and adults with increased cardiovascular risk, but no established atherosclerosis, showed favorable effects of antioxidants on systemic endothelial function.5,6 Our results in ART children should be interpreted in this context, suggesting that interventions normalizing vascular oxidative stress and nitric oxide bioavailability may have a favorable effect on cardiovascular outcome in this specific population.
Study limitations
Surrogate markers of vascular function that are independent predictors of future cardiovascular risk27,32 were assessed in this study since, given the young age of the ART population, at this time it is impossible to investigate clinical cardiovascular endpoints. While the sample size was relatively small, power analysis was adequate and the results of this double-blind controlled study were significant and entirely consistent with those of previous studies in ART children 3 and ART mice, 4 making false-positive findings unlikely. As the aim of our study was to assess the effects of antioxidant vitamin administration on systemic and pulmonary vascular function, measurements were made at high altitude, since pulmonary vascular dysfunction can only be detected under hypoxic conditions. We did not examine the effects of antioxidant vitamins on systemic vascular function at low altitude. However, because endothelial dysfunction in ART children is comparable at low and high altitude (Rimoldi, unpublished observation), it is likely that vitamins would also have had favorable effects on systemic vascular function at low altitude. In line with this speculation, antioxidants have favorable effects on endothelial dysfunction in ART mice (Rexhaj et al., unpublished observations).
While antioxidant vitamins improved flow-mediated vasodilation in ART children, we could not detect a significant improvement of reactive hyperemia (i.e. the microvascular reactivity to transient ischemia). It is possible that the method used to assess microvascular reactivity was not sensitive enough to detect this effect.
Finally, for ethical reasons we did not assess nitroglycerin-induced vasodilation because at high altitude nitroglycerin-induced cerebral vasodilation is known to trigger/aggravate acute mountain sickness.
Conclusion
This study shows for the first time that oral supplementation with vitamins C and E improves systemic and pulmonary vascular function in ART children demonstrating the potential reversibility of vascular dysfunction in this population. We speculate that interventions aimed at normalizing oxidative stress and NO bioavailability may have a favorable effect on cardiovascular outcome in this population.
Footnotes
Acknowledgments
The authors are indebted to the study participants; to the International Foundation High Altitude Research Stations Jungfraujoch and Gornergrat for providing the facilities at the Jungfraujoch; to the custodians for the support of their activities, to Siemens (Zürich, Switzerland) for providing the echocardiographic equipment and to Burgermeister AG (Rapperswil, Switzerland) for the gift of vitamins and corresponding placebo.
Funding
This work was supported by grants from the Swiss National Science Foundation, the Placide Nicod Foundation, the Eagle Foundation, the Leenaards Foundation and the FABER Foundation.
Conflict of interest
None declared.