
Abstract
Background
Atrial natriuretic peptide (ANP) is released from the atria (on cleavage of proANP) in response to elevated intra-atrial pressure and wall stretch. Clinical data on proANP are still limited, mainly due to limitations in assaying the protein, which recently have been solved. ProANP is elevated in cardiovascular disease and predicts outcome in heart failure. However, knowledge of the prognostic value in acute myocardial infarction remains limited.
Methods
We prospectively included 680 patients with STEMI treated with primary-PCI, from September 2006 to December 2008. Blood samples were drawn immediately before PCI. Plasma MR-proANP was measured using an automated processing assay. Endpoints were all-cause mortality (n = 137) and the combined endpoint (n = 170) of major adverse cardiovascular events (MACE) defined as cardiovascular mortality and admission due to recurrent MI, ischaemic stroke or heart failure.
Results
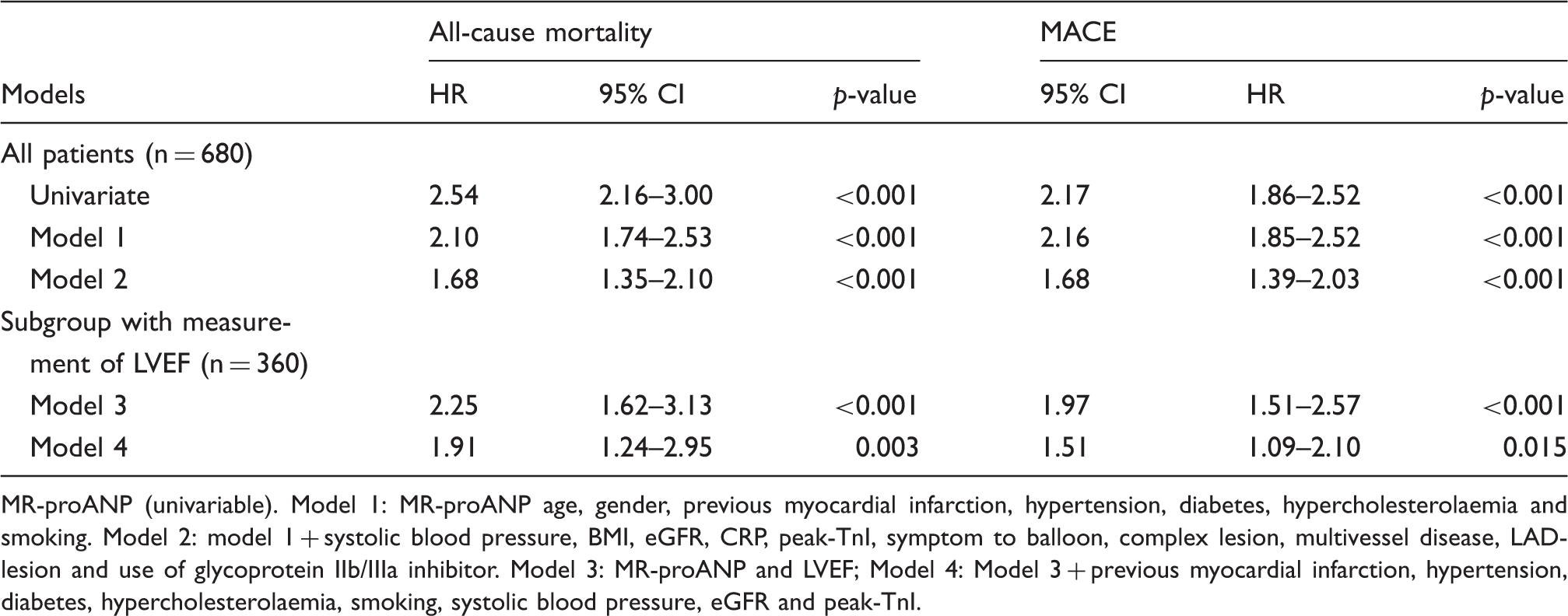
During 5-year follow-up, MR-proANP was associated with increased risk of all-cause mortality and MACE (both p < 0.001). After adjustment for confounding risk factors (age, gender, hypertension, diabetes, hypercholesterolaemia, smoking, previous MI, BMI, eGFR, CRP, peak-TnI, symptom-to-balloon time, multivessel disease, complex lesion, LAD-lesion and use of glycoprotein inhibitor), MR-proANP remained an independent predictor of all-cause mortality and MACE – hazard ratio: 1.68 (95% CI 1.35–2.10; p < 0.001) and 1.68 (95% CI 1.39–2.03; p < 0.001) per standard deviation increase in MR-proANP.
MR-proANP significantly increased C-statistics and reclassified 26% of the patients for all-cause mortality and 34% for MACE into higher or lower risk categories, matching actual event rates more accurately.
Conclusions
Plasma MR-proANP independently predicts all-cause mortality and MACE in patients with STEMI.
Introduction
In response to volume load and myocardial stretch, cardiomyocytes synthesize and release brain natriuretic peptide (BNP) and atrial natriuretic peptide (ANP) as well as precursor molecules (i.e. proBNP and proANP). 1 BNP and proBNP have been investigated extensively; they are elevated in stable coronary artery disease (CAD), heart failure (HF) and acute myocardial infarction (AMI). They are strong predictors of future cardiovascular events and mortality and used in the clinic both for the diagnosis of HF and to guide treatment.2–5
By contrast, clinical data on ANP and proANP are limited, mainly due to difficulties in correct measurement of ANP and proANP in the past.6,7
On cleavage of proANP, ANP is released from the atria in response to elevated intra-atrial pressure and wall stretch. Although enzymatic degradation still occurs, proANP is much more stable in plasma compared to ANP. 6
ProANP provides diagnostic and prognostic information in both chronic and acute HF.8,9 ProANP concentrations are elevated in CAD, which predicts outcome in patients with unspecified chest pain; however, data on AMI and especially ST-segment elevation myocardial infarction (STEMI) is still limited.10,11
Accordingly we measured mid-regional proANP (MR-proANP) capable of detecting all fragments of proANP in the circulation in a large group of STEMI-patients in order to assess the long-term prognostic value of proANP and to compare it with established risk factors and risk scores.
Methods
Study population
Between September 2006 and December 2008 we prospectively enrolled 680 STEMI patients treated with primary percutaneous coronary intervention (pPCI) at Gentofte University Hospital, Denmark (a high-volume PCI-centre with on-site cardiac surgeons currently performing >1500 PCI procedures a year). 12 Inclusion criteria were: patients admitted due to a suspected STEMI with presence of chest pain for >30 minutes and <12 hours, and persistent ST-segment elevation ≥2 mm in at least two contiguous precordial ECG-leads or ≥1 mm in at least two contiguous limb ECG-leads or a newly developed left bundle branch block. Exclusion criteria were: patients unable to provide informed content or a non-significant troponin I (TnI) increase (≤0.5 µg/l) – no occlusion on coronary artery angiography or coronary artery bypass surgery was elected instead. A total of 735 patients was included, but 55 were excluded due to missing MR-proANP values.
Standard subsequent medical treatment included daily aspirin 75 mg, clopidogrel 75 mg (for 12 months), lipid-lowering drugs (statins) and β-receptor antagonists.
We defined hypertension as a history of hypertension and use of blood pressure-lowering drugs on admission. Patients were considered to have diabetes mellitus if they were treated with glucose-lowering drugs at time of admission. Hypercholesterolaemia was defined as treatment with cholesterol-lowering drugs at time of admission. Echocardiography was performed by specialists at our institution on 342 patients (51%) using Vivid 7 or E9 (GE Healthcare, Horten, Norway) 1–3 days after admission. Left ventricular ejection fraction (LVEF) was obtained using the modified biplane Simpson method.
Endpoints were all-cause mortality and major adverse cardiovascular events (MACE) defined as cardiovascular mortality or readmission due to a new AMI, ischaemic stroke or symptomatic HF. CV mortality was defined as the primary cause of death from periphery artery disease, ischaemic heart disease, HF or stroke. AMI was classified as admission to hospital due to chest pain and a significant increase of troponins. Ischaemic stroke was classified as admission to hospital due to neurological symptoms (focal neurological deficit) and a positive cerebral CT scan. Symptomatic heart failure was classified as admission to hospital with clinical signs of heart failure (dyspnoea, fatigue and pulmonary oedema/stasis).
All patients were followed for 5 years, and follow-up was 100% complete (n = 680). Data on mortality were obtained though the civil registration system and the National Causes of Death Registry, which provides information from physicians on causes of death according to the ICD-10 classification. Follow-up data on re-admissions were obtained using data from the highly validated National Patient Registry provided by ICD-10 codes. 13 All events found using these registries were carefully validated using medical records (e.g. laboratory tests, operative reports, hospital charts etc.) and possibly misclassified events were excluded.
The study was approved by the local scientific ethical committee and The Danish Data Protection Agency, and complied with the 2nd Declaration of Helsinki. Informed consent was obtained from all participants.
Laboratory methods
Blood samples were drawn from the femoral sheath before the pPCI procedure. Blood was allocated to 4 ml EDTA containers and within 30 min centrifuged at 10,000 RPM for 10 min. Plasma was stored in nunc cryotubes at −80℃ until analysis in a blinded fashion in a dedicated core laboratory. MR-proANP was measured using an automated processing assay (Automated platform, Kryptor Compact Plus, Brahms, Germany) capable of detecting all fragments of proANP in the circulation, regardless of endeoproteolytic cleavage. Assay performance has previously been published. 14 TnI levels were measured at baseline and again after 6 and 12 hours with the commercially available immunoassay from Siemens healthcare, Immulite 2500 STAT, with serial measurements available in all patients. Peak-TnI was defined as the highest value. C-reactive protein (CRP) and creatinine were assayed by routine laboratory methods. Estimated glomerular filtration rate (eGFR) was calculated on the basis of serum creatinine, age and gender using the MDRD formula. 15
Statistical analysis
Baseline characteristics.
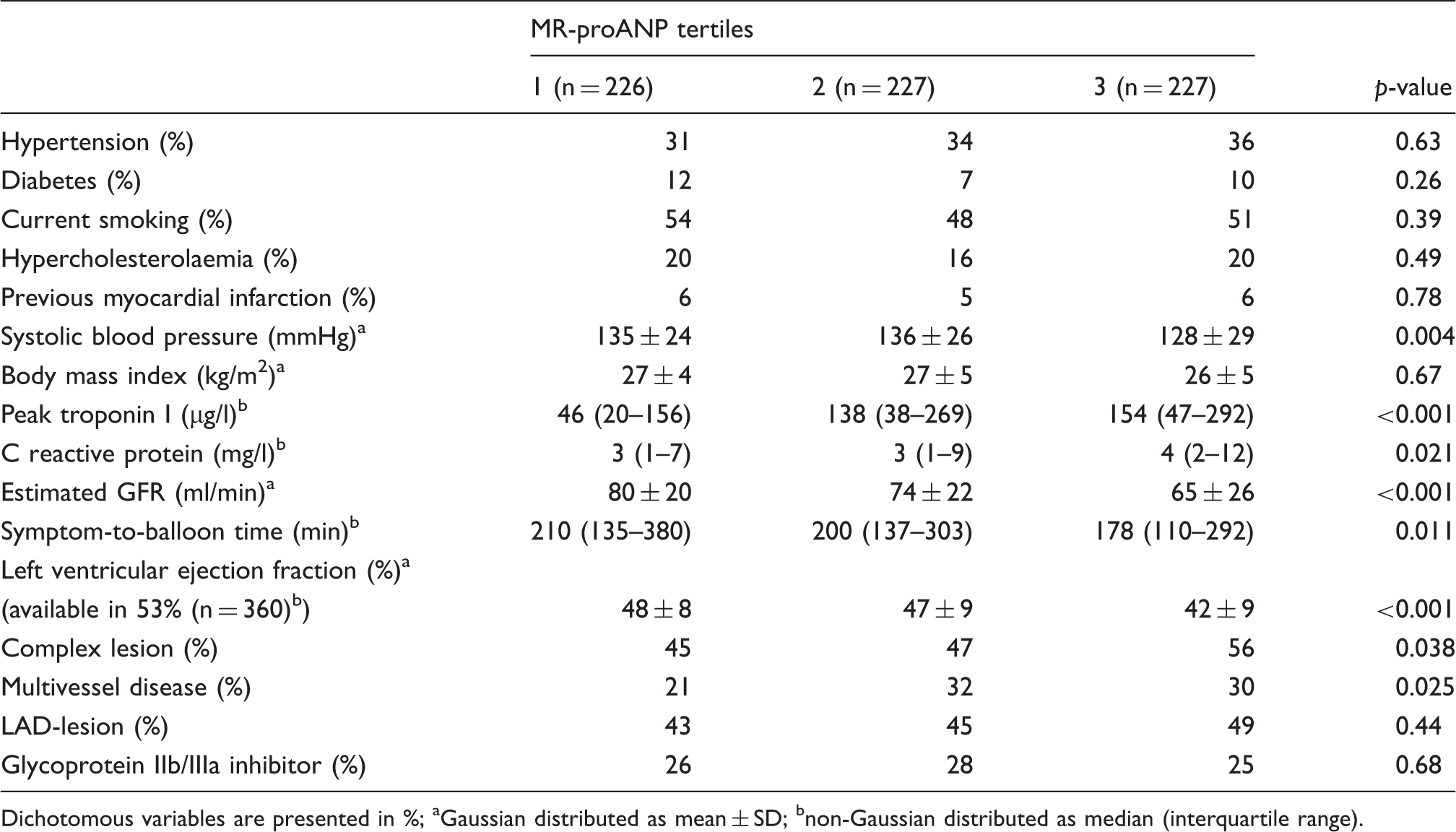
Dichotomous variables are presented in %; aGaussian distributed as mean ± SD; bnon-Gaussian distributed as median (interquartile range).
Results
Patients were 63 ± 12 years old and 74% were male. The plasma level of MR-proANP (geometric mean (5th to 95th percentile)) was higher in females (216 µg/l (74–671 µg/l)) vs males (161 µg/l (58–514 µg/l)) and associated significantly with age (r = 0.47, p < 0.001). Baseline characteristics in Table 1 are presented as tertiles of MR-proANP adjusted for age and gender. As seen, MR-proANP associated positively with peak-TnI levels and inversely with systolic blood pressure, eGFR and LVEF.
Comparison with peak-TnI and CRP
During 5 years of follow-up, all-cause mortality was 20% (n = 137) including 50% (n = 68) due to CV-causes and a total of 25% (n = 170) reached the combined endpoint of MACE.
ROC-curves for MR-proANP, peak-TnI levels and CRP are presented in Figure 1, showing that MR-proANP performed superiorly compared to CRP and especially peak-TnI levels for both endpoints. C-statistics for MR-proANP were significantly higher compared to peak-TnI levels (0.72 (0.68–0.77) vs. (0.56 (0.51–0.61), p < 0.001) and CRP (0.66 (0.61–0.71), p = 0.047) for all-cause mortality. Similarly for MACE, C-statistics for MR-proANP were higher compared to peak-TnI levels (0.69 (0.65–0.73) vs 0.55 (0.50–0.60), p < 0.001) and CRP (60 (0.55–0.65), p = 0.002).
ROC-curves for MR-proANP, peak-Troponin I and C-reactive protein (all logarithmically transformed) for all-cause mortality (a) and MACE (b).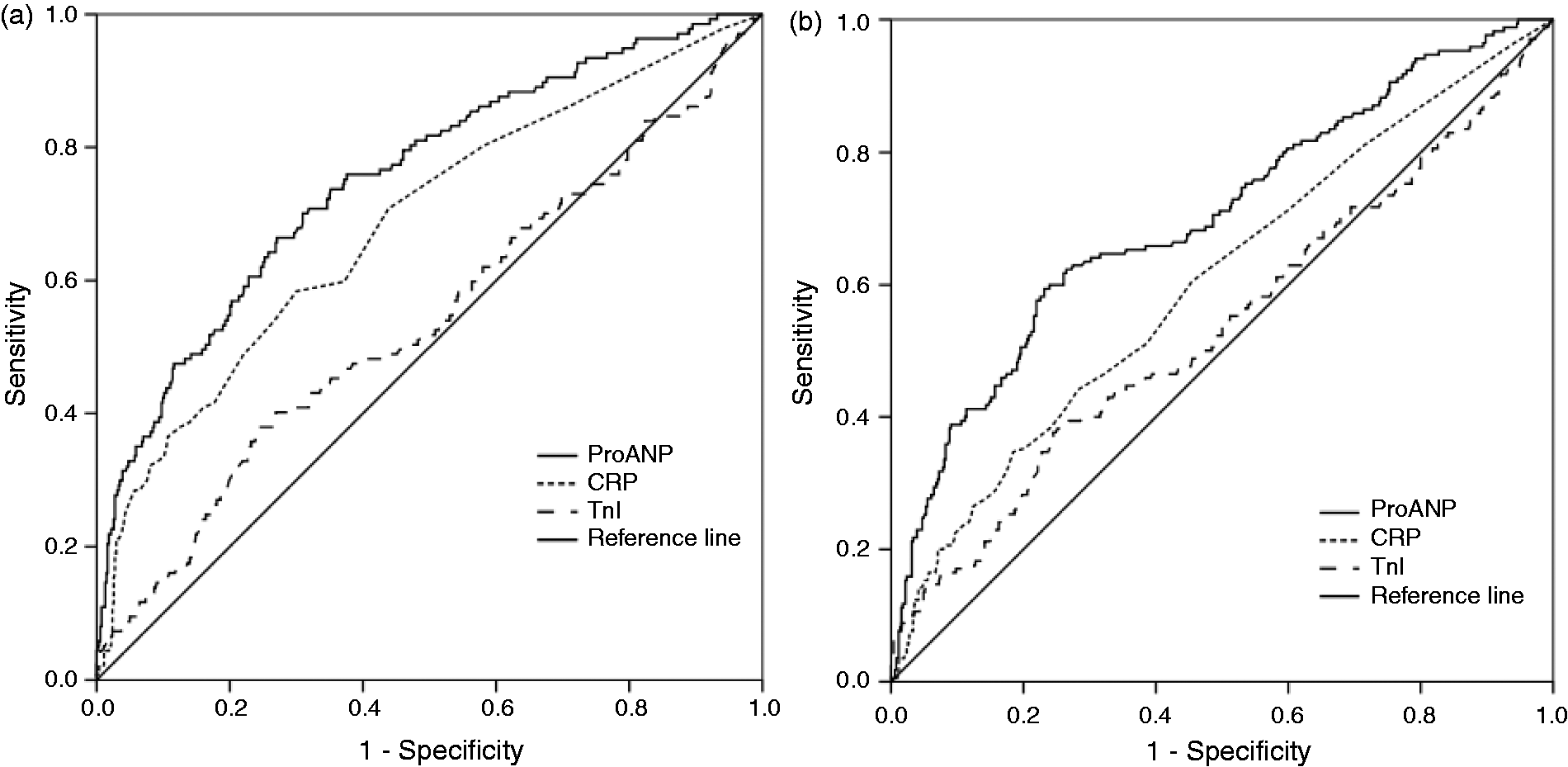
MR-proANP and outcome
Kaplan-Meier curves demonstrated a significant association between MR-proANP and all-cause mortality and MACE (Figure 2). The results were confirmed in both univariable and several multivariable Cox-regression analyses (Table 2). As seen, MR-proANP was an independent predictor of all-cause mortality and MACE in all models.
MR-proANP and risk of all-cause mortality (a) and MACE (b). MR-proANP and risk of all-cause mortality and MACE. MR-proANP (univariable). Model 1: MR-proANP age, gender, previous myocardial infarction, hypertension, diabetes, hypercholesterolaemia and smoking. Model 2: model 1 + systolic blood pressure, BMI, eGFR, CRP, peak-TnI, symptom to balloon, complex lesion, multivessel disease, LAD-lesion and use of glycoprotein IIb/IIIa inhibitor. Model 3: MR-proANP and LVEF Model 4: Model 3 + previous myocardial infarction, hypertension, diabetes, hypercholesterolaemia, smoking, systolic blood pressure, eGFR and peak-TnI.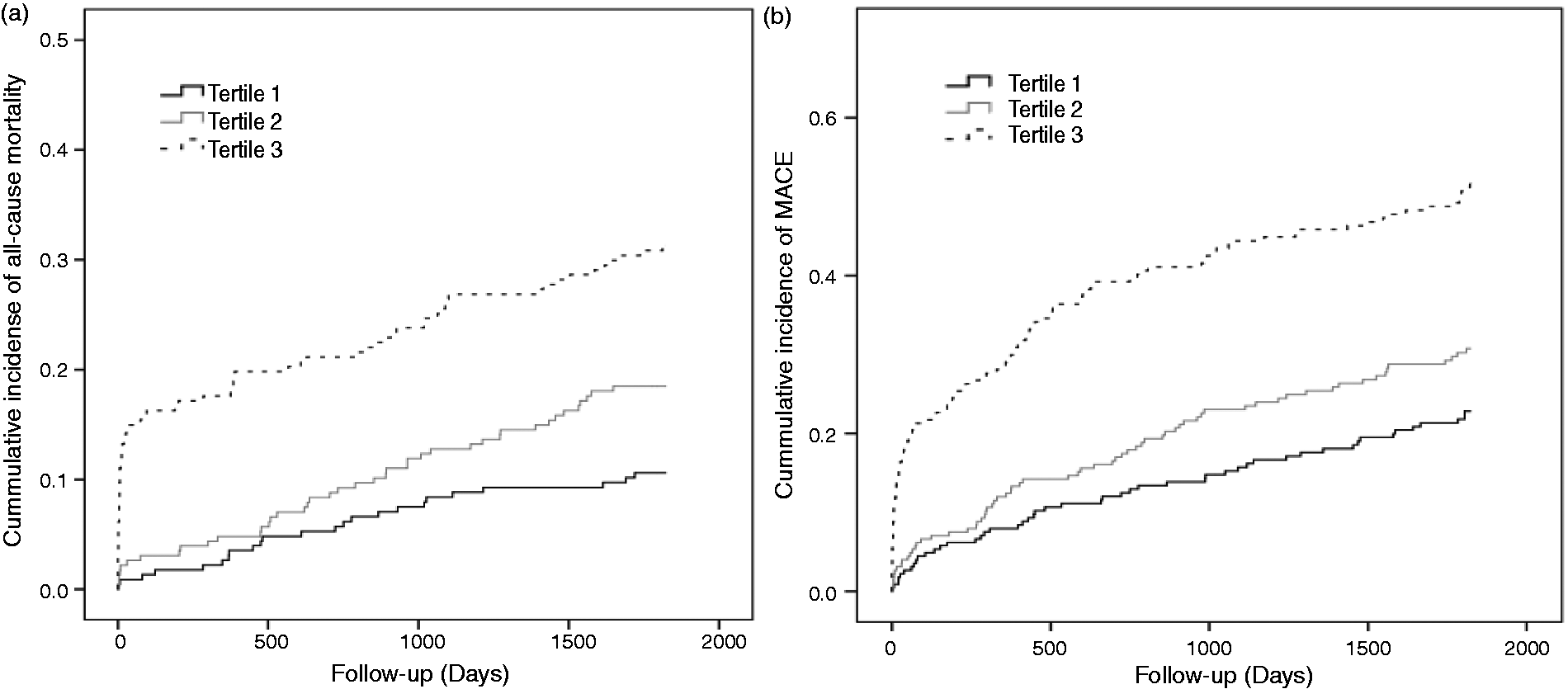
For the prediction of all-cause mortality, addition of MR-proANP improved C-statistics for model 2: 0.76 (0.72–0.80) vs 0.72 (0.67–0.76), p = 0.006 and model 3: 0.80 (0.76–0.83) vs 0.77 (0.73–0.81), p = 0.013. Similarly for MACE, MR-proANP improved C-statistics for model 1: 0.71 (0.67–0.75) vs 0.65 (0.61–0.70), p = 0.004 and model 2: 0.73 (0.69–0.77) vs 0.71 (0.67–0.75), p = 0.038.
Risk reclassification after addition of MR-proANP; (a) all-cause mortality; (b) MACE.
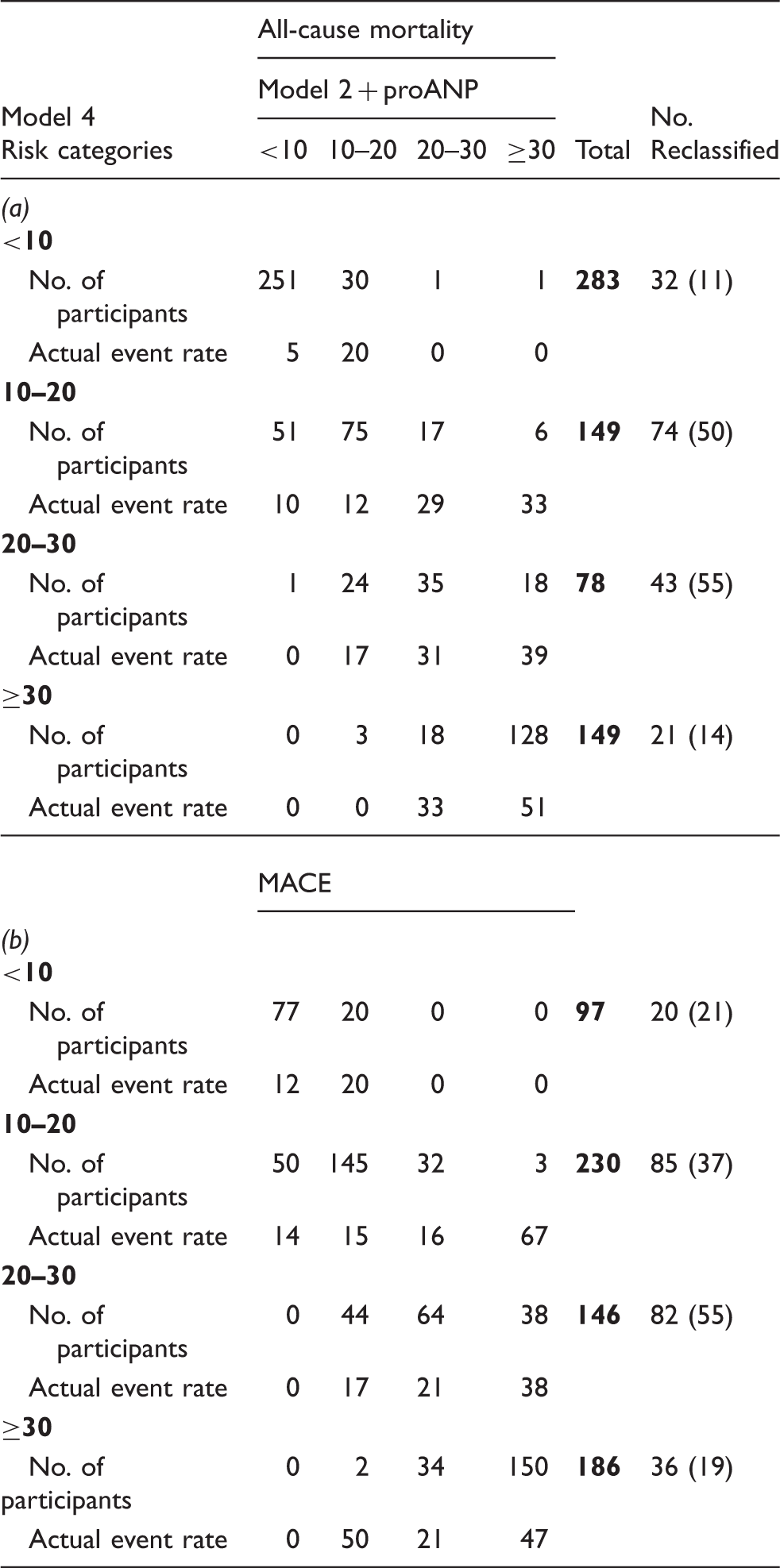
As shown for all-cause mortality (Table 3(a)), the proportion of patients reclassified was relatively low for those with a 5-year risk of less than 10% (11%). However, 50% and 55% of all patients estimated to be at 10–20% or 20–30% were reclassified into higher or lower risk categories. Table 3(a) also shows that actual event rates matched well with the predicted in almost all risk categories; a total of 170 patients (26%) were reclassified, of which 168 (99%) were placed into more accurate risk categories.
Table 3(b) presents similar analyses for risk of MACE. Again, there was improved matching of observed and predicted risks after the addition of MR-proANP; of the 223 patients (34%) reclassified, all but 2 (99%) were placed into more accurate risk categories.
Calculating continuous NRI yielded similar results; 0.37 (95% CI: 0.15–0.59) for all-cause mortality and 0.34 (0.10–0.50) for MACE.
MR-proANP and LVEF
Due to the fact that echocardiography was only performed at our institution in 53% of the patients (n = 360), LVEF was not included in the initial multivariable models. Importantly, no significant differences in baseline variables were found between patients examined with echocardiography at our institution, compared to patients transferred back to their primary hospital for post-PCI treatment.
In the subgroup with measurement of LVEF (n = 360), MR-proANP correlated significantly with LVEF (r:-0.27, p < 0.001). Further adjustment for different combinations of all other baseline variables did not impact this association significantly, as MR-proANP remained highly significantly associated with LVEF in all models (p < 0.001). Figure 3 shows LVEF according to tertiles of proANP adjusted for all variables in Table 1.
MR-proANP and left ventricular ejection fraction.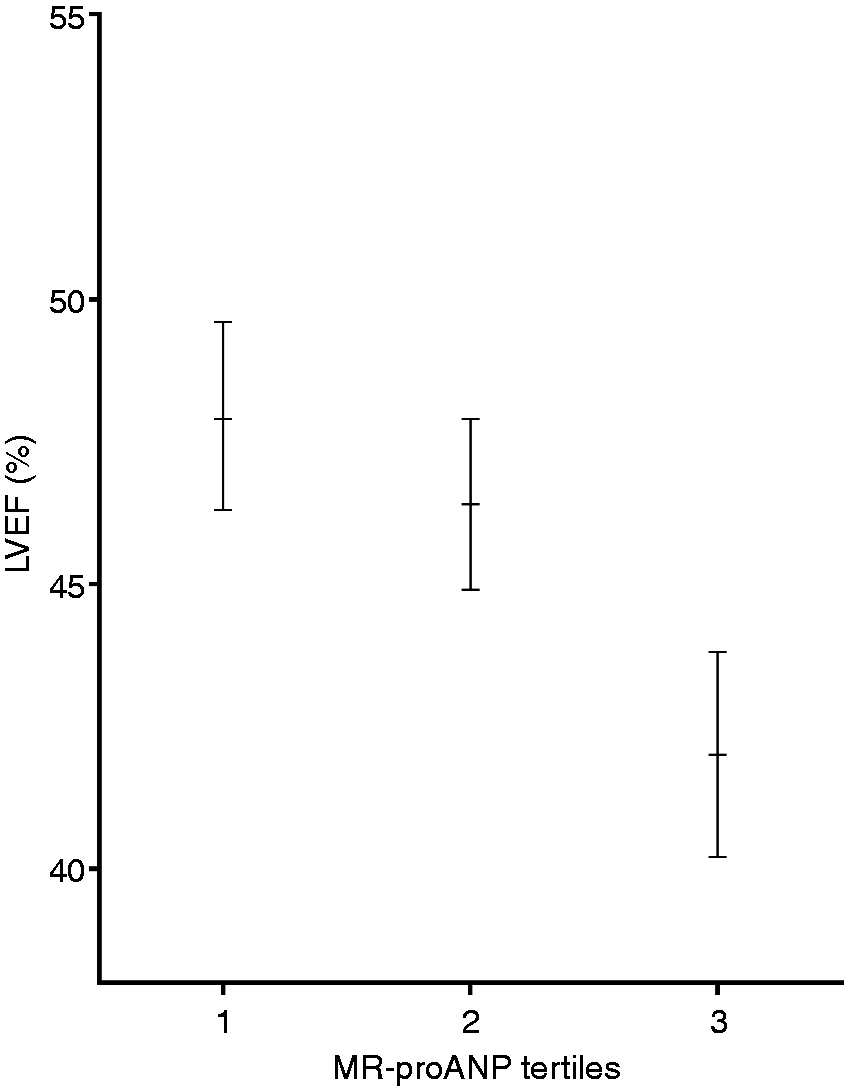
We then evaluated the impact of LVEF on the prognostic performance of MR-proANP with regard to risk of all-cause mortality and MACE. When adjusted for LVEF, MR-proANP associated strongly with all-cause mortality (HR (95% CI) 2.25 (95% CI: 1.62–3.13), p < 0.001) and MACE (1.97 (1.51–2.57), p < 0.001) per standard deviation increase in MR-proANP. Even when further adjusting for age, gender, cardiovascular risk factors (hypertension, diabetes, hypercholesterolaemia, smoking) and all variables highly associated with MR-proANP (peak-TnI, eGFR and systolic bloodpressure (model 4)) MR-proANP remained an independent predictor of all-cause mortality and MACE (Table 2).
Discussion
In brief, the present study shows that MR-proANP is an independent predictor of both all-cause mortality and MACE in patients with STEMI. With regard to risk stratification, MR-proANP performs superiorly to standard blood tests such as CRP and TnI. MR-proANP also significantly improved discrimination and reclassified patients into better fitting risk categories.
The precursor proANP is released in an equimolar ratio to the active hormone (ANP) but the concentration of proANP is about 10-fold that of ANP due to avoidance of receptor binding, and protein interaction and half-life are much longer; accordingly measurement of the pro-hormone (C-terminal or the inactive fragment N-terminals of proANP) are preferred.1,7,16 Early evaluations of the prognostic performance of proANP were discouraging. 17 However, it is now recognized that this was caused by a suboptimal assay design. 6 NT-proANP is degraded by exoproteases into sub-fragments not detectable by the assay. 7 Accordingly measurements of NT-proANP underestimate the real concentrations of proANP. Recently developed immunoassays for the more stable MR-proANP (used in the present study) have been demonstrated to detect all fragments making it robust against truncation. Recent studies measuring MR-proANP have shown promising results.
An association between MR-proANP and outcome in unselected patients with chest pain has been found in several studies.11,18,19 In a study of pure AMI patients Khan et al. reported an independent association between MR-proANP and 1-year mortality and re-admission with heart failure. 20 However, this population was a mixture of N-STEMI and STEMI patients and blood samples were taken in the days following the infarction. As the authors found a decrease in MR-proANP on day 2, they speculated that MR-proANP at admission could be even more useful. Indeed this hypothesis is supported by the work of Tzikas et al. who demonstrated that MR-proANP was released very quickly into the circulation during AMI. 19 We were able to extend these findings to long-term follow-up in patients with STEMI treated with pPCI, showing that MR-proANP improved risk stratification beyond cardiovascular risk factors and biochemical measurements.
The fact that MR-proANP is superior in predicting outcome compared to peak-TnI levels has previously been shown by Haehling et al.; however they only measured TnI at admission, whereas TnI is known to peak in the subsequent days. 18 Therefore, peak TnI levels are probably better suited as a marker of myocardial necrosis, especially in patients with STEMI who are admitted to hospital under 2 hours from onset of symptoms. However, even when using peak-TnI levels, MR-proANP significantly outperformed TnI. Thus, MR-proANP is not only better at risk stratifying patients compared to TnI; only one measurement is needed, making it faster and easier to interpret.
MR-proANP is not only stimulated by haemodynamic stress but also by myocardial ischaemia, as demonstrated by Sabatine et al. in patients undergoing cardiac stress exercise testing. 21 Thus, in patients with AMI, the release of MR-proANP is initiated prior to myocardial necrosis and TnI, 19 which may explain the strong association with outcome.
To the best of our knowledge this is the first study reporting an association between MR-proANP and TnI levels. Troponins have been measured together with MR-proANP in several studies but probably due to the heterogenic populations possible associations with troponins were not reported.11,18–20 Jarai et al. reported an insignificant correlation between MR-proANP and TnI in a study of 120 patients; however, it is likely that the insignificant association was caused by the relationship between MR-proANP and myocardial ischaemia, as 64% of the patients had unstable angina pectoris and thus TnI in the normal area. 22
Finally we found an association between MR-proANP and LVEF as previously described in patients with HF and CAD.23,24 In 797 patients with HF, Moertl et al. showed that MR-proANP associated inversely with LVEF and outperformed BNP and NT-proBNP in the prediction of all-cause mortality and CV mortality. Importantly MR-proANP still predicted mortality when LVEF was included in the models. 23 We were able to confirm this in patients with STEMI, demonstrating that MR-proANP carries prognostic information beyond LVEF.
Study limitations and strengths
A comparison between MR-proANP and B-type natriuretic peptides (BNP or proBNP) would have been of great interest, as it is suggested that MR-proANP may be superior to BNP/proBNP in predicting outcome due to higher biological stability of the molecule and midregional assay; 23 unfortunately, measurements of these hormones were not available. Echocardiography was only performed in 53% of the patients (n = 360) due to patients being transferred back to their primary hospital for post-PCI treatment. Strengths include the long follow-up time resulting in a large number of events.
Footnotes
Funding
The study was supported by the Foundation of Aase and Ejnar Danielsen.
Conflicts of interest
None to declare.