
Abstract
Background
Vascular age is an alternate means of representing an individual's cardiovascular risk. Little consensus exists on what vascular age represents and its clinical utility has not been determined. We systematically reviewed the literature to provide a comprehensive overview of different methods that have been used to define vascular age, and to examine its potential clinical value in patient communication and risk prediction.
Design
This was a systematic review with data sources of PubMed and Embase.
Results
We identified 39 articles on vascular age, 20 proposed to use vascular age as a communication tool and 19 proposed to use vascular age as a means to improve cardiovascular risk prediction. Eight papers were methodological and 31 papers reported on vascular age in study populations. Of these 31 papers, vascular age was a direct translation of the absolute risk estimated by existing cardiovascular risk prediction models in 15 papers, 12 derived vascular age from the reference values of an additional test, and in three papers vascular age was defined as the age at which the estimated cardiovascular risk equals the risk from non-invasive imaging observed degree of atherosclerosis. One trial found a small effect on risk factor levels when vascular age was communicated instead of cardiovascular risk.
Conclusion
Despite sharing a common name, various studies have proposed distinct ways to define and measure vascular age. Studies into the effects of vascular age as a tool to improve cardiovascular risk prediction or patient communication are scarce but will be required before its clinical use can be justified.
Introduction
Cardiovascular diseases (CVDs) are a leading cause of morbidity and mortality worldwide. 1 The risk of developing symptomatic CVD varies greatly between individuals and can be predicted using various prediction models. Based on the predicted risk for CVD in the next 10 years, an individual can be classified into low, intermediate or high risk categories with their corresponding treatment options. 2 However, CVD risk is primarily driven by age and a young person with a significant elevated risk factor burden is still likely to have a low CVD risk score. Continuing exposure to high risk factor levels in these young individuals will likely lead to increased absolute CVD risk as they age. Therefore, early identification of high risk individuals when they are young and the implementation of risk factor modification, especially through lifestyle change, would have important health benefits.
Vascular age is a means of expressing cardiovascular risk as an age. It is thought to improve cardiovascular risk prediction models and may contribute to a better understanding of cardiovascular risk, especially as in young patients the long term effects of high risk factor levels can be concealed by a young age. Previous research indicates that vascular age is easily understood by patients and has a greater impact on care than presenting an estimated CVD risk score. 3 Furthermore, results from a randomized controlled trial have indicated that targeted communication about 10-year vascular risk leads to improved control of lipid levels. 4 Recent Canadian guidelines for the diagnosis and treatment of dyslipidaemia have recommended calculating and discussing a patient’s vascular age in order to improve the likelihood that patients will reach targeted lipid levels and better control their hypertension. This has shown to be especially useful, for young individuals where calculated 10-year risk scores are low. 5
Despite growing interest in vascular age, there is little consensus about the definitions of vascular age and alternative terms such as ‘heart age’ or ‘risk age’ have also been used. We systematically reviewed the current literature on vascular age to provide a comprehensive overview of the approaches that have been used to define and calculate vascular age, and to examine its potential value for risk prediction and improved patient communication.
Methods
Search strategy
Search syntax.
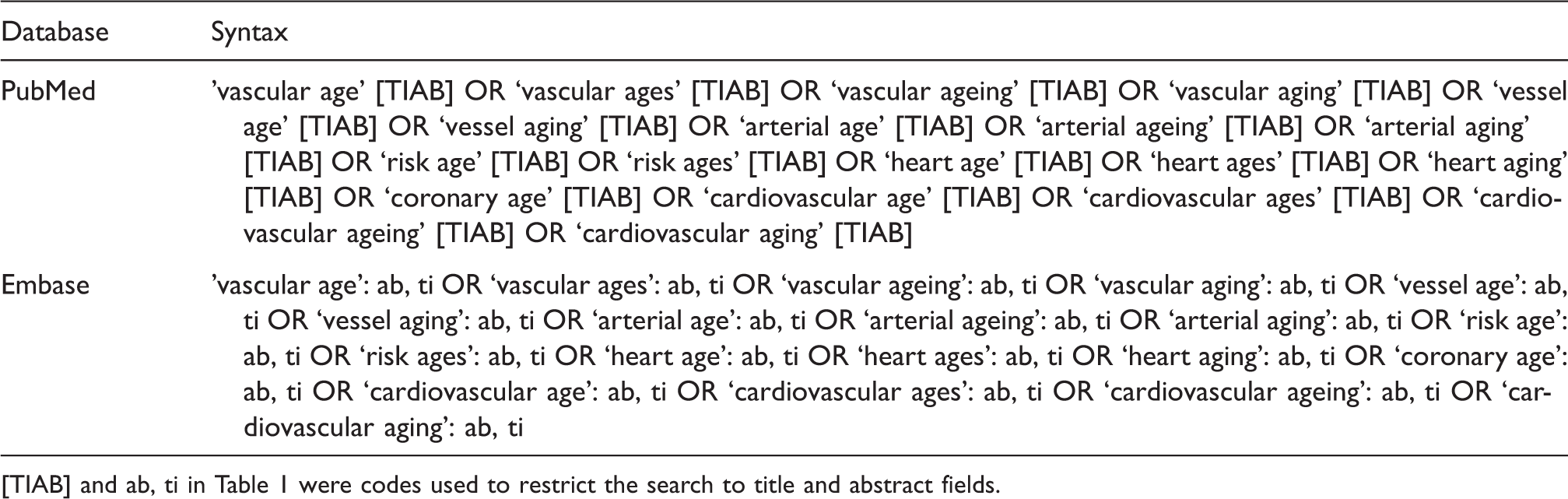
[TIAB] and ab, ti in Table 1 were codes used to restrict the search to title and abstract fields.
Screening and selection
After excluding exact duplicates, articles were screened on title and abstract. Studies were excluded if they reported on non-human experiments (in vitro, animal studies), were performed in children, did not determine vascular age or the method of defining vascular age was unclear. Secondary sources (reviews, editorials), conference abstracts and papers published in another language than English were also excluded. After title and abstract screening, all retrievable full text articles were screened using the same criteria as were used for the screening of the abstracts, with the addition that the method of defining or measuring vascular age (or synonym) was described. When multiple papers reported on the same cohort, we selected the paper with the largest number of participants. When many groups were mentioned, we calculated averages for more broad categories.
Data extraction
We extracted, whenever appropriate, data on study characteristics, definition of vascular age, proposed methods of defining vascular age, chronological and vascular age in the study, and the yield in cardiovascular risk prediction.
Results
Search strategy and study selection
Our systematic search resulted in 1965 unique articles of which 107 articles were eligible for full text screening. Of these 107 articles, 70 were excluded. From these 70 articles, six were not available in full text, 38 were conference abstracts, nine were not in English, five were secondary sources, six did not determine vascular age, one did not describe methodology and five were multiple reports on the same cohort.
Screening of the references yielded another two articles. Of the 39 selected articles, eight articles reported on concepts and methodologies of vascular age and 31 applied vascular age in a clinical setting. The flowchart of the search and selection process is provided in Figure 1. Characteristics of the included studies where vascular age was applied to a population are presented in Tables 2 and 3. Table 4 contains the results of the studies that examined the association between vascular age and cardiovascular disease.
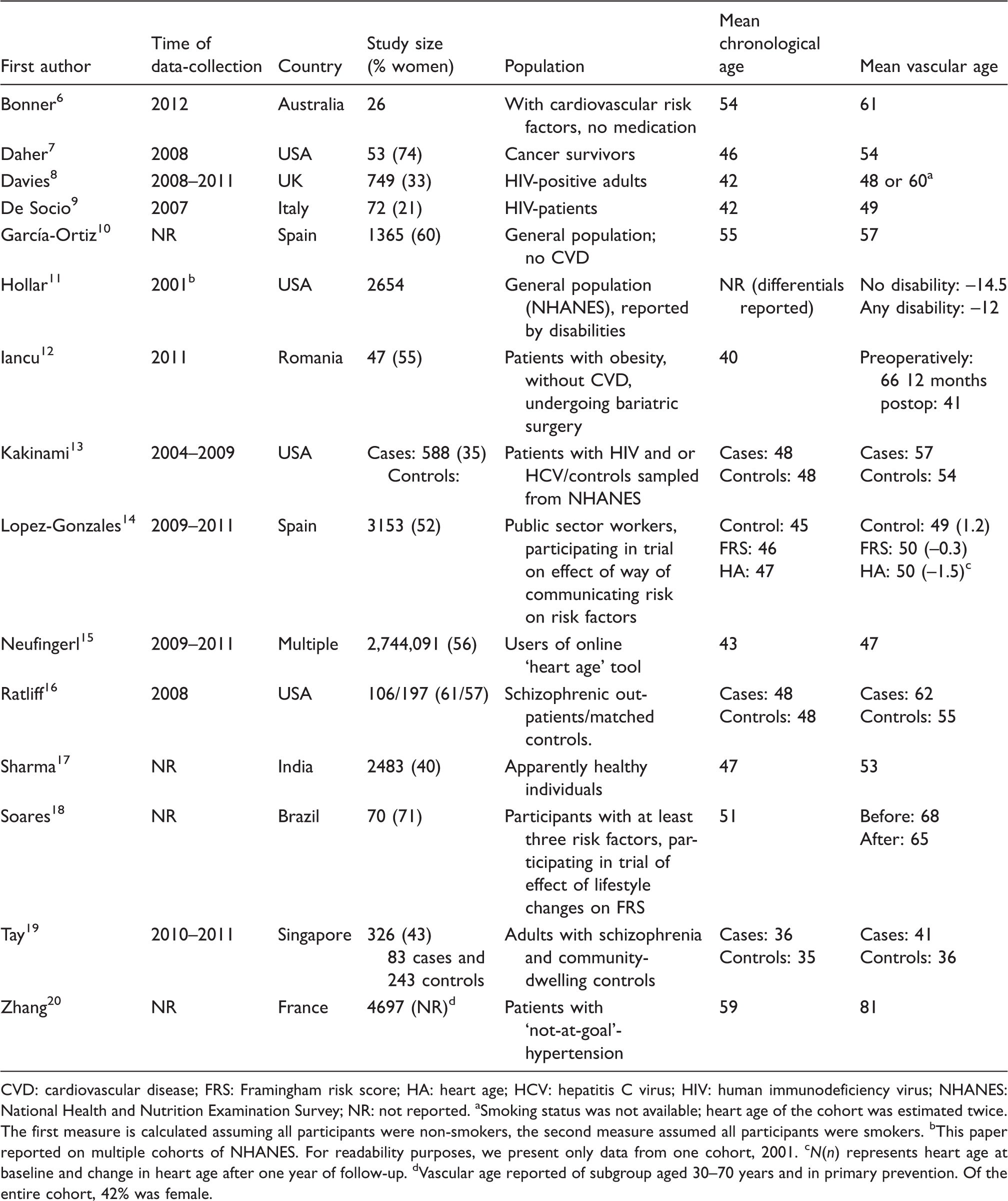
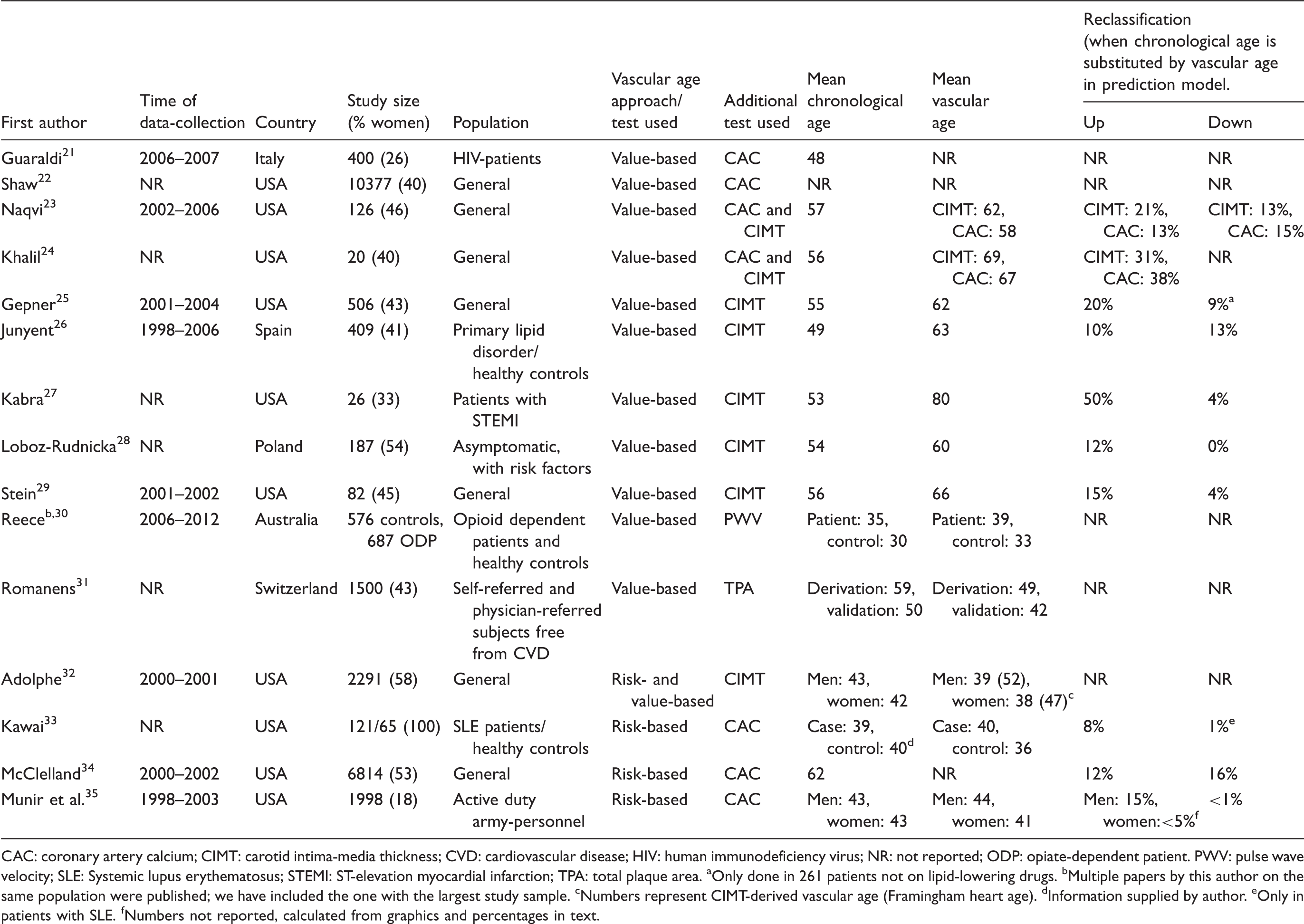
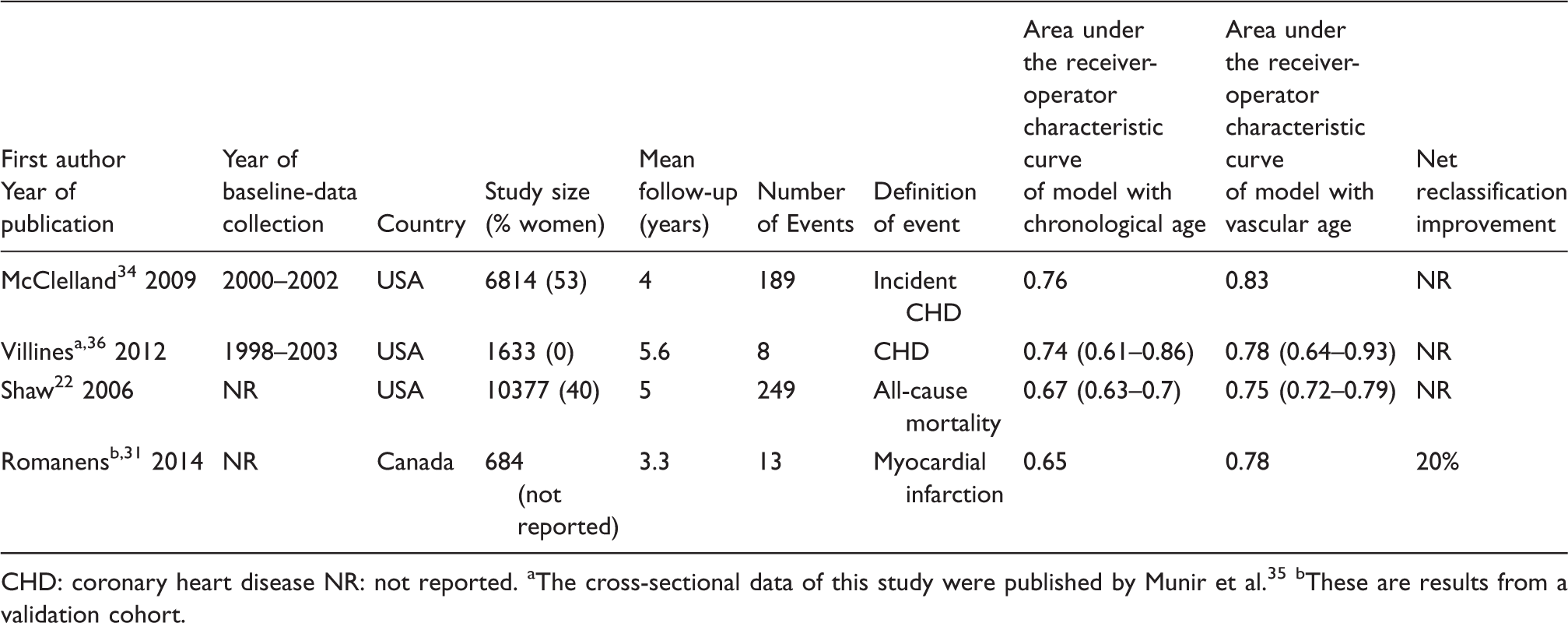
Flowchart of study selection. Details of studies that used vascular age in the context risk communication. CVD: cardiovascular disease; FRS: Framingham risk score; HA: heart age; HCV: hepatitis C virus; HIV: human immunodeficiency virus; NHANES: National Health and Nutrition Examination Survey; NR: not reported. Smoking status was not available; heart age of the cohort was estimated twice. The first measure is calculated assuming all participants were non-smokers, the second measure assumed all participants were smokers. This paper reported on multiple cohorts of NHANES. For readability purposes, we present only data from one cohort, 2001. N(n) represents heart age at baseline and change in heart age after one year of follow-up. Vascular age reported of subgroup aged 30–70 years and in primary prevention. Of the entire cohort, 42% was female. Details of studies using additional tests to determine vascular age in (patient) populations. CAC: coronary artery calcium; CIMT: carotid intima-media thickness; CVD: cardiovascular disease; HIV: human immunodeficiency virus; NR: not reported; ODP: opiate-dependent patient. PWV: pulse wave velocity; SLE: Systemic lupus erythematosus; STEMI: ST-elevation myocardial infarction; TPA: total plaque area. Only done in 261 patients not on lipid-lowering drugs. Multiple papers by this author on the same population were published; we have included the one with the largest study sample. Numbers represent CIMT-derived vascular age (Framingham heart age). Information supplied by author. Only in patients with SLE. Numbers not reported, calculated from graphics and percentages in text. Details on studies relating vascular age to cardiovascular disease. CHD: coronary heart disease NR: not reported. The cross-sectional data of this study were published by Munir et al.
35
These are results from a validation cohort.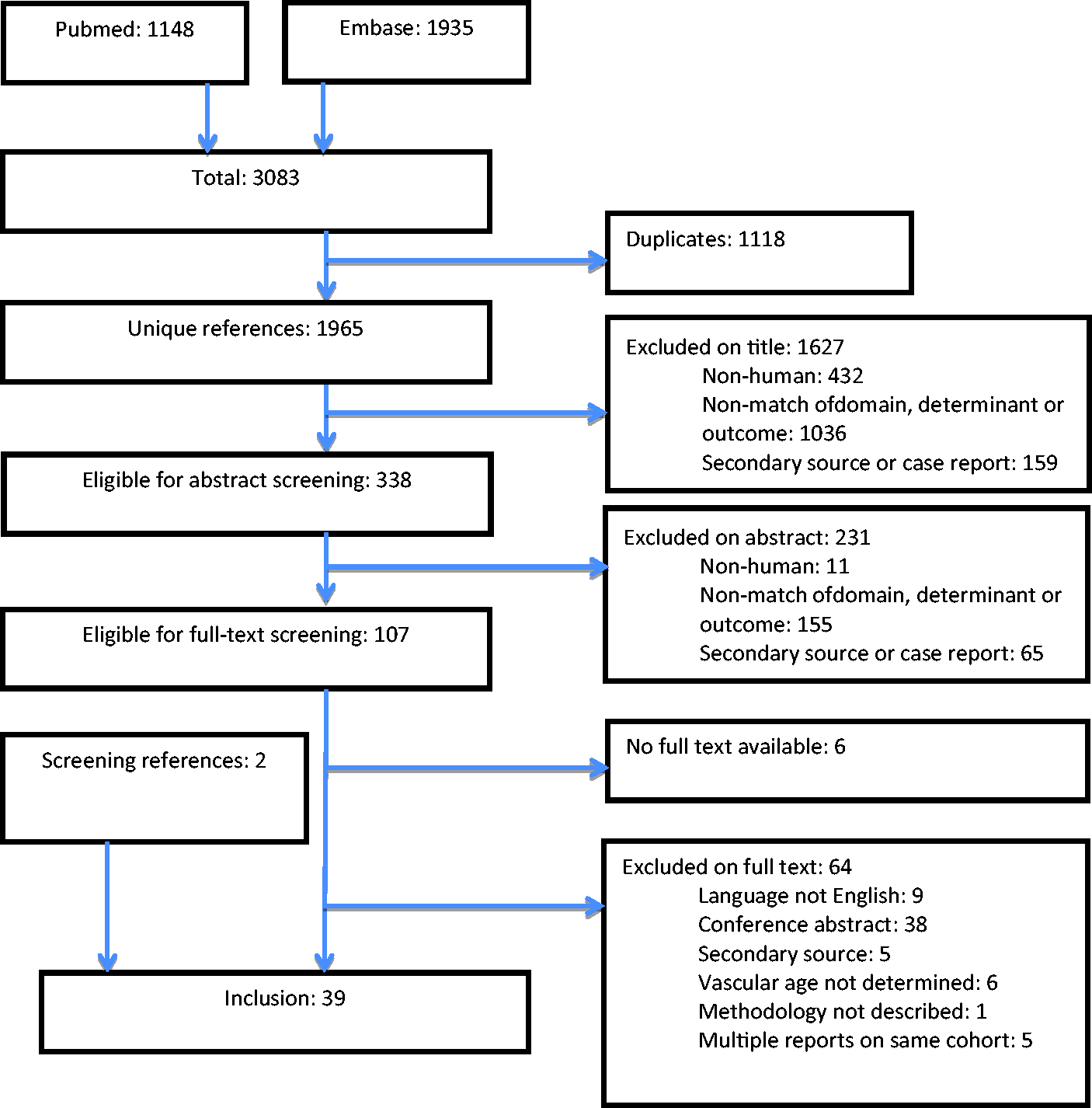
The use of vascular age in patient communication
Twenty papers6–20,37–41 proposed using vascular age as a means of communicating cardiovascular disease risk to patients. Of these 20 papers, five described methods of calculating vascular age37,38,40,41 and 156–20 applied these methods to populations. Vascular age was calculated by estimating the patient’s cardiovascular risk using an existing risk prediction model such as Framingham or Systematic Coronary Risk Evaluation (SCORE). This estimated risk score was matched with the age at which the risk was equivalent but all other risk factors were at ideal levels. For example, a 50-year old man who smokes, has a systolic blood pressure of 140 mm Hg, a High-density lipoprotein (HDL) cholesterol of 45 mg/dl and a total cholesterol levels of 200 mg/dl has an estimated cardiovascular risk of 19.3% according the Framingham risk score. The vascular age of this man would be 69, as this is the age at which a man with ideal risk factor levels (e.g. not smoking, a systolic blood pressure of 120 mm Hg and normal cholesterol levels) would also have an estimated cardiovascular risk of 19.3%. An illustration of translating cardiovascular risk scores to vascular age is presented in Figure 2.
Example of deriving vascular age from risk tables.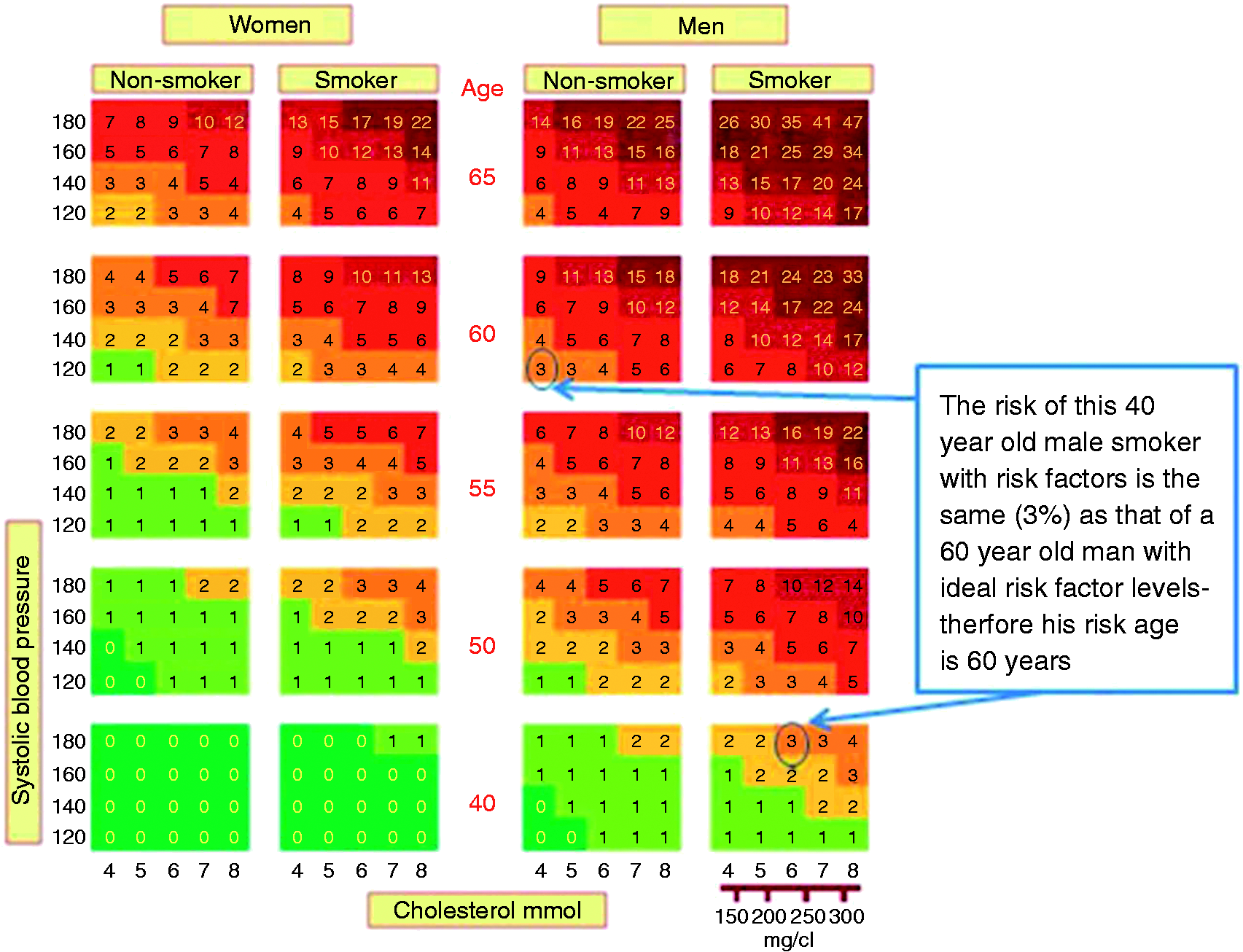
Various ways of translating risk models to vascular age have been proposed, but Framingham heart age 39 was the most commonly used method. Heart age exceeded the chronological age of study participants in all studies that applied heart age in a clinical setting, with the difference in means ranging from 2–26. A point-system derived by a similar approach to the Framingham heart age, but calibrated to the Japanese population was published by Yatsuya et al. 37
The effect on metabolic parameters of communication of the Framingham REGICOR-risk (REgistre GIroní del COR) or heart age on top of conventional medical advice alone was examined in a randomised controlled trial among 3153 public sector workers. After 12 months of follow-up, levels of metabolic parameters had improved significantly in both risk communication groups, but most profoundly in the heart age group. Furthermore, heart age had increased in the control group and decreased in the intervention groups. 14
Vascular age to improve cardiovascular risk prediction
Nineteen studies proposed to incorporate results of additional tests such as non-invasive imaging of atherosclerosis into the vascular age estimate, possibly to improve the performance of existing cardiovascular risk prediction models.21–36,42–44 Of these 19, three papers reported on methods42–44 and 16 applied these methods to populations.21–24,26–36
Eight studies used carotid intima-media thickness (CIMT)23–29,32 as an additional test, eight studies used coronary arterial calcification (CAC),21–23,24,33–36 one study used total plaque area (TPA)
31
and one study used pulse wave velocity (PWV).
30
The results from these additional tests were subsequently used to calculate the vascular age using either a value-based approach or a cardiovascular risk-based approach (Figure 3).
Example of deriving vascular age from an imaging test.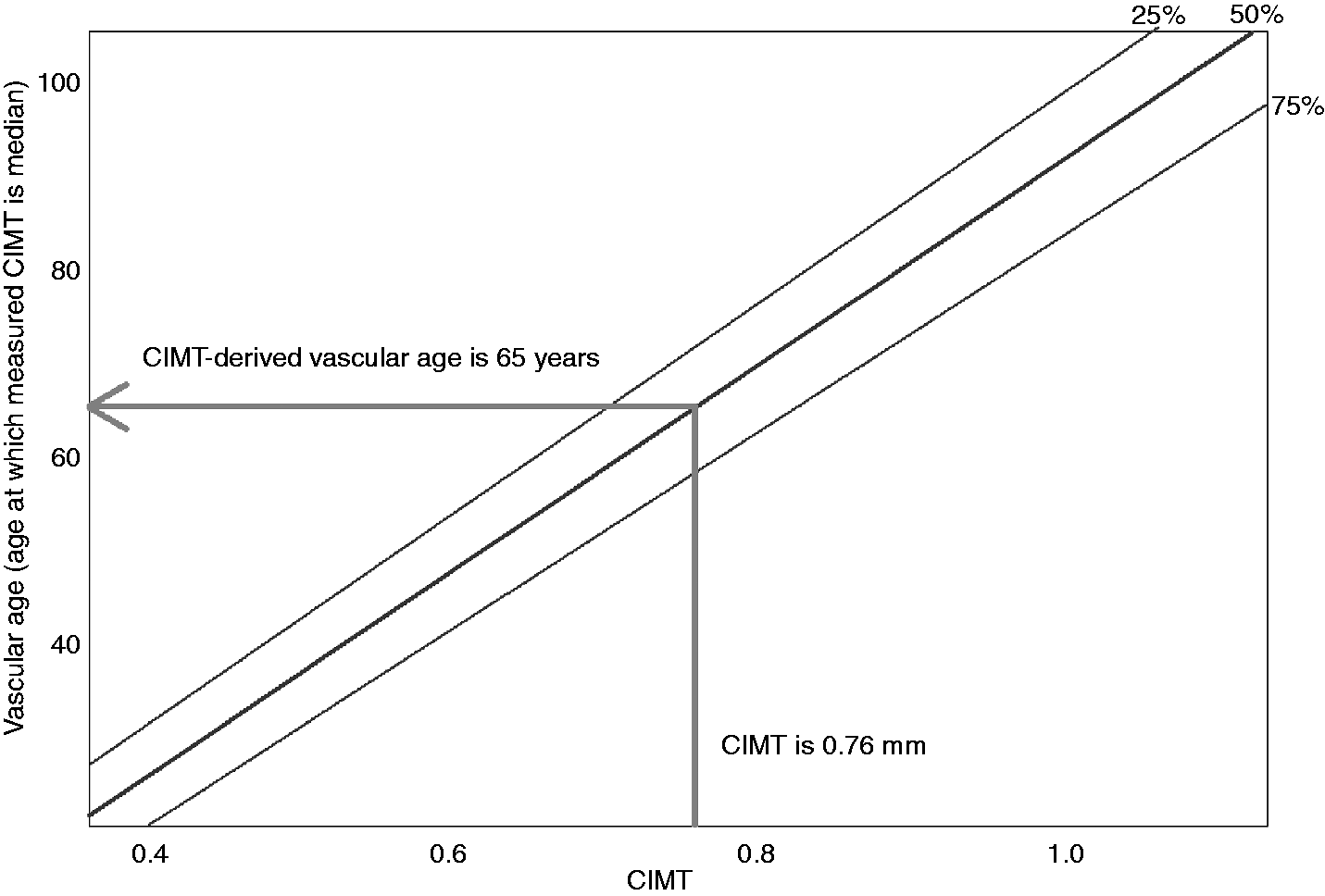
Value-based approach to calculate vascular age
In the 12 studies that used a value-based approach,21–32 vascular age was the age at which a participant’s result from an imaging test would equal the population reference values.
Stein and colleagues were the first to develop the value-based approach. 29 Using data from the ARIC study, they defined vascular age as the age at which the composite CIMT-value for an individual of a given race and sex would represent the median CIMT value in the ARIC study. A person with an above-average CIMT would be considered older, while a person with a below-average CIMT is considered younger. This vascular age can subsequently be used as communication tool or as substitute for chronological age in risk prediction models. A number of studies have applied this concept in various clinical settings (Table 2).
Mean vascular age was higher than chronological age in all but one study, with the differences ranging from 1–26.5 years. In the six cross-sectional studies that reported on risk reclassification using CIMT-derived vascular age, 10–51% of patients would have been classified to a higher risk category on the basis of their CIMT whereas 0–13% of the individuals were classified to a lower risk category. Two prospective studies showed that the ability of a prediction model to assign a higher predicted risk to future cases than to non-cases improved when chronological age was replaced by a test-derived vascular age in the Framingham risk score.22,31
Risk-based approach to calculate vascular age
We identified four33–36 studies that used a risk-based approach to define vascular age (Table 3). In the risk-based approach, vascular age is the age at which the risk for CVD equals the risk associated with the imaging-derived degree of subclinical atherosclerosis. Longitudinal data are required to calculate a risk-based vascular age; reflecting the intrinsic need for estimates on the association between age and future CVD risk, and atherosclerosis and future CVD risk.
McClelland et al. 34 were the first to propose and a risk-based approach in participants from the MESA study, they showed that the Receiver operating characteristic-Area Under the Curve (ROC-AUC) of the Framingham risk score increased from 0.76 in a model with chronological age to 0.83 in a model with CAC-derived vascular age. The calculator to estimate vascular age using the risk-based approach has been published on http://www.mesa-nhlbi.org/Calcium/ArterialAge.aspx, and has been used in two subsequent studies. Risk-based vascular age of patients with systemic lupus erythematosus was similar to their chronological age (40 vs 39 years) whereas the vascular age of healthy controls was 4 years lower than their chronological age (36 vs 40 years). 33 Vascular age was 44 in men and 41 in women among 1988 individuals, leading to upclassification in 15% of men and less than 5% of women, and to down classification in 1% of men. 35 Substitution of chronological age by CAC-derived vascular age in the Framingham risk score in men from this cohort increased the ROC-AUC from 0.74 (0.61–0.86) to 0.78 (0.64–0.93). 36
Discussion
The present systematic review on vascular age shows that studies have proposed different strategies to use vascular age as tool to communicate cardiovascular risk to patients or as a means to improve the performance of cardiovascular risk prediction models. Direct comparisons between different approaches to compute vascular age are currently lacking. Direct comparisons between different approaches to compute vascular age are currently lacking and data on its effectiveness in improving patient outcomes is scarce.
Vascular age in risk communication
Several studies have assessed whether vascular age as a means of communicating cardiovascular risk levels to patients leads to a better understanding of the level of risk and to improved adherence to therapies and lifestyle changes.6,14,15 A recent trial showed that informing patients about the Framingham REGICOR risk, or heart age, on top of conventional medical advice alone significantly improved metabolic parameters in both risk communication groups, but most profoundly in the heart age group. 14 Similarly, Soureti et al. compared the impact on participants' risk perceptions and intention to make lifestyle changes of communicating CVD risk in either the traditional format of a 10-year CVD percentage risk or as a heart age. 3 Heart age had a greater emotional impact in younger individuals at high CVD risk levels than use of a percentage CVD risk score and would therefore be more likely to promote healthier lifestyles. Furthermore, in a study to investigate patient experiences and understanding of online heart age calculators, despite misinterpretation of risk factor questions, the calculators prompted participants to consider lifestyle changes, irrespective of their heart age level. 6 Other studies have shown that the way physicians communicate the risks and benefits of medical care may influence patients' choices regarding treatment45,46 and their willingness to accept treatment. 47 Moreover, patient knowledge of their coronary risk profile has shown to slightly improve the efficacy of lipid therapy. 4
Lifetime risk has been suggested as an alternative way to present cardiovascular risk and to better reflect the long-term effects of exposure to risk factors than 10-year risk. Lifetime risk is fairly constant over a lifetime and may therefore be valuable in risk communication, especially in young- and middle aged individuals for whom 10-year risk is inherently low because of their age. Lifetime risk, however, may be less intuitive in risk communication than vascular age because lifetime risk is presented as a percentage and vascular age as an age. 48
A concept similar to vascular age, ‘lung age', has been used for smokers, when smokers were informed about their estimated lung age, smoking cessation was 7.2% higher than for patients who were not presented a lung age. 49 On the contrary, communication of the results of carotid imaging tests among smokers who were being motivated to quit smoking did not result in higher smoking cessation rates, 50 suggesting that more than a simple objective measurement is needed to motivate patients to improve their health behaviours and help them better understand their cardiovascular risk.
Vascular age in cardiovascular risk prediction
Cardiovascular risk prediction performs modestly at best and there are continuing efforts to improve it.51,52 In the present review, we have identified several studies that have proposed the use test-derived vascular age to achieve this goal. These studies have suggested replacing chronological age by vascular age under the premise that this better reflects an individual’s exposure to cardiovascular risk factors.
Most studies added the results of an imaging-based degree of atherosclerosis, primarily CIMT and CAC, to a standard cardiovascular prediction model, without substitution of age. 53 While CIMT was recently shown to have modest value when added to the Framingham risk score, 54 CAC has been shown to have provide significant improvements in cardiovascular risk prediction. However, a limitation for this approach is the need for individuals to have CAC scores greater than zero. In this review, risk-based vascular age was only calculated using the results of CAC tests and was shown to materially improve the discriminative ability of the risk prediction model.34,36 Whether such improvements are achievable using CIMT-derived risk-based vascular age needs to be determined. However, based on the results of previous studies where CIMT and CAC were added to a risk prediction model,53,54 it might be expected that predictive accuracy is better improved by substituting a CAC-derived vascular age to chronological age rather than using a CIMT-derived vascular age.
Next to the choice upon which measure should be used to base vascular age, the potential added value of vascular age in cardiovascular risk prediction is likely to depend on the way vascular age will be defined as well. We identified two distinct methods to define a test-derived measure of vascular age, i.e. a value-based approach and a risk-based approach. In the value-based approach, vascular age is based on the expected age of an individual based on the reference values derived from a healthy population. In the risk-based approach, vascular age represents the age where the cardiovascular risk estimated by imaging a patient’s atherosclerotic burden or another test result equals the calculated CVD risk based on age. Therefore, in a value-based approach vascular age is a direct translation of the result of a test, whereas in risk-based vascular age information is added.
Intuitively, the risk-based approach might make more biological sense since it matches the chronological age equivalent to the risk associated with a given level of atherosclerosis, and not to the age where an average person would be expected to have a certain level of atherosclerosis (i.e. the reference value-based approach). However, studies comparing these two different approaches are lacking and would provide further insights in the value of vascular age assessment in patient communication and for CV risk prediction.
Strengths and limitations
To our knowledge, this is the first systematic review on the concepts behind vascular age. Such a review is needed since the expression ‘vascular age' is increasingly used, yet the exact definition and the potential uses in a clinical setting remain ambiguous. A limitation of this paper is that the search and screening process were conducted by one author (KAG). This could have increased the possibility of missing some significant papers. However, we cross-checked the references listed in the selected papers and included relevant studies that were not identified in our initial search. Moreover, since the aim of our study was to provide an overview of the current concepts behind vascular age rather than to compare the different methods and evaluate their clinical application, definite conclusions about the value of vascular age are yet to be reached.
Conclusion
Despite sharing a common name, various studies have proposed distinct ways to define and measure vascular age. Studies into the effects of vascular age as a tool to improve cardiovascular risk prediction or patient communication are scarce but will be required before its clinical use can be justified.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared.