Pre-diabetes and diabetes mellitus: challenges for cardiac rehabilitation programs
I Cunha1, S Viamonte1, C Matos1, C Moreira1, A Barreira1, P Fernandes1, S Torres1
1Centro Hospitalar do Porto, Porto, Portugal
Topic: Sports cardiology
Purpose:Meta-analysis have shown the benefit of Cardiac Rehabilitation Programs (CRP) in the overall population; however there are limited data that specifically address CRP in diabetic and pre-diabetic patients, although such programs may be especially important in this group of patients. The aim of this study was to compare the benefit of a CRP between subjects with normal glucose regulation (NGR), abnormal glucose regulation (AGR) and diabetes mellitus (DM) in relation to the cardiovascular risk factors and functional capacity.
Methods:Observational prospective study, including patients with cardiac ischemic disease oriented to a multidisciplinary CRP between January 2012 and June 2014. Patients were divided into 3 groups: NGR, ARG and DM group. They all underwent a supervised aerobic moderate exercise training protocol, 2 times/week during 3 months. Several clinical, laboratory and treadmill stress test parameters were collected at the first visit of Phase II of the CRP and 3 months later, namely blood pressure, lipid profile (LDL-colesterol, HDL-colesterol, Triglycerides), blood glucose and glycated hemoglobin (HbA1c), body mass index (BMI) and waist circumference (WC), smoking habits, daily physical activity (International Physical Activity Questionnaires), functional capacity (maximal exercise capacity on treadmill stress test and Metabolic Equivalents (MET) achieved).
Results:540 patients were enrolled, 232 with NGR, 173 with ARG and 135 with DM. Patients with ARG and DM were significantly older (61.47±9.81 and 62.57±9.88 respectively vs 58.39±11.1 in NGR), but had comparable cardiovascular risk profile and functional capacity. Regarding cardiovascular risk factors, statistically significant differences were found between the three groups for BMI (p <0.001), WC (p<0.001), HDL- cholesterol (p = 0.010), triglycerides (p = 0.001) and functional capacity (total exercise time and MET p<0.001). DM patients had worse results for the previously mentioned parameters at baseline, followed by ARG patients. Assessing the evolution of these parameters between the first assessment point and after 3 months, there was a statistically significant improvement for some of them (WC p<0.01, blood glucose and HbA1c<0.01 and total exercise time<0.01), but this improvement was less significant for the DM group, followed by the ARG.
Conclusions:The results suggest that patients with pre-diabetes and DM may experience lesser benefit in some of the cardiovascular risk parameters, which indicates the need for a special intervention directed at these specific subgroup of patients.
P226
Gender-specific secondary prevention?
DR Thompson1, CE Kure1, Y Chan1, CF Ski1, MJ Carrington1, S Stewart1
1Australian Catholic University, Melbourne, Australia
Topic: Sports cardiology
Purpose:To explore the psychosocial determinants of a major acute cardiovascular event (MACE) during follow-up of a hospitalized cohort of patients with heart disease participating in a secondary prevention trial with differential outcomes according to gender Methods:Outcome data were analyzed (post-hoc) from a multi-centre cohort of patients (n=602) randomized to a home-based intervention (n=306) or standard care (n=296). Baseline psychosocial profiling comprised depressive status, physical and mental quality of life, social isolation and mild cognitive impairment. Multivariate analyses examined independent correlates of a two-year MACE (an unplanned cardiovascular-related hospitalization or all-cause mortality) on a gender-specific basis Results:The mean age of the cohort was 70 (+/-10) years, 171 (28%) were women and 377 (63%) had coronary artery disease. Within two years of index hospitalization, 165/602 (27%; 95% CI 24% to 31%) experienced a MACE: 114 (27%) men and 51 (30%) women (p=0.431). Independent correlates of a MACE in men were depressive status (OR 1.9; 95% CI 1.1 to 3.6, p=0.032), low physical quality of life (OR 0.98; 95% CI 0.96 to 1.0, p=0.027) and increasing Charlson Comorbidity Index (OR 1.1; 95% CI 1.0 to 1.3, p=0.004). In women, it was age (OR 1.1; 95% CI 1.0 to 1.1, p=0.008), mild cognitive impairment (OR 2.4; 95% CI 1.1 to 5.2, p=0.029) and site of recruitment and ongoing management (OR 2.3; 95% CI 1.1 to 4.9, p=0.029) Conclusions:Independent of clinical factors, different psychosocial factors (including the management team) appear to modulate cardiovascular-specific outcomes in men and women with heart disease
P227
Exercise barriers and relationship to self-efficacy for exercise in cardiac patients over 12 months in participants of a lifestyle change program
R Gallagher1, A Kirkness2, M Al-Harbi1, G Prebill1, W Shi1
1University of Sydney, Sydney Nursing School, Charles Perkins Center, Sydney, Australia
2Royal North Shore Hospital, North Shore Cardiovascular Education Centre, Sydney, Australia
Topic: Sports cardiology
Purpose:To describe exercise barriers in overweight and obese cardiac patients experience before, during and at completion of a lifestyle change program and determine if an independent association exists between these barriers and self-efficacy for exercise.
Methods:Participants (n = 131) of the Healthy Eating and Exercise Lifestyle Program (HEELP) identified their barriers to exercise and completed the self-efficacy for exercise survey at baseline, 4 (active phase) and 12 months (maintenance phase). HEELP includes 4 months of structured and supervised exercise followed by 8 months of home-based exercise delivered in a cardiac rehabilitation setting.
Results:The sample mean age was 63.6 years (SD 8.5), BMI of 31.4kg/m2 and 58% were male. The most common exercise barriers at all times was leg and/or feet problems (44%). Other common barriers at baseline such as lack of motivation (40.3%) and environment issues including bad weather (40.3%) declined over time. The mean number of barriers decreased from baseline 2.19 (SD 1.30) to four months 1.79 (SD 1.18) and 12 months 1.16 (SD 1.21) (RMANOVA P<.001). Only lack of motivation was associated with self-efficacy for exercise. In the regression models after adjusting for other key influences lack of motivation was associated with decreased self-efficacy for exercise at 12 months (B -2.44). Other influences were important, participants who had more depressive symptoms had lower self-efficacy for exercise at baseline (B = -.56) and 4 months (B = -.21) as did participants with higher BMI at 12 months (-.35). Higher self-efficacy for exercise occurred at baseline if people were male, both at 4 months (B = 1.83) and 12 months (B = 1.48) and if they met current exercise recommendations both at baseline (B = 1.50) and 12 months (B = 1.93).
Conclusion:Cardiac patients who are overweight or obese identify many exercise barriers which decrease over time participating in a lifestyle change program. Lack of motivation has a negative impact on self-efficacy for exercise and needs to be addressed, but importantly, other factors such as depression, sex, BMI and current exercise habits could also be addressed.
P228
Patient rehabilitation after pulmonary embolism, an observational, retrospective, single center study
F Noack1, B Schmidt1, M Amoury2, D Stoevesandt3, S Gielen4, B Pflaumbaum5, C Girschick5, A Schlitt5
1University Clinic Halle (Saale), Department of Medicine I, Halle, Germany
2University Clinic Halle (Saale), Department of Emergency Medicine, Halle, Germany
3University Clinic Halle (Saale), Department of Diagnostic Radiology, Halle, Germany
4University Clinic Halle (Saale), Department of Medicine III, Halle, Germany
5Paracelsus-Harz-Clinic Bad Suderode, Quedlinburg, Germany
Background:One-year mortality after pulmonary embolism (PE) is approximately 2.5% and bleeding events according to anticoagulant treatment are common. Current guidelines in Germany recommend rehabilitation after PE however, the rehabilitation process after PE is not well investigated.
Design/Methods:Data from consecutive PE patients who have been treated in a German rehabilitation clinic from 2006-2014 were retrospectively evaluated in this single-center study.
Results:422 patients were identified. The mean age was 63.9±13.5 years and 51.9% were female. Deep vein thrombosis was diagnosed in 55.5% of all cases. Tricuspidal regurgitation was found in most patients (61%), in 11.0% as moderate and in 3.4% as severe. Moreover, maximal systolic pulmonary artery pressure was increased (mean 33.9±12.7mmHg + central venous pressure). No serious adverse events such as recurrent DVT/PE or death were found. Three patients suffered from bleeding, which was clinically relevant in one. We applied a wide range of therapeutic interventions such as bicycle training with monitored heart rate in 86.7%, respiratory training in 82.5%, aquatic therapy/swimming in 40.1%, and medical training therapy in 14.9% of all patients. No relevant influence of any of the physical activity interventions on incidence of any AE was found.
Conclusion:The rehabilitation program after PE was safe as presented in this study. Echocardiography demonstrated that tricuspidal regurgitation was a common event and, in the majority of patients, pulmonary hypertension was likely, underlining the importance of serial echocardiography in patients after PE to detect pulmonary hypertension requiring treatment.
P230
Re-hospitalization rate and the evolution of systolic dysfunction under the influence of comprehensive rehabilitation program during the first year after coronary revascularization.
EB Vataman1, AA Grivenco1, DM Lisii1, SS Filimon1, LG Morcov1
1Institute of Cardiology, Chisinau, Moldova, Republic of
Topic: Sports cardiology
Purpose:To estimate the effectiveness of cardiovascular rehabilitation program on left ventricular systolic function and evolution of chronic heart failure in patients after coronary revascularization Materials and methods:190 patients (mean age 61.05 ± 0.8) with coronary heart disease, coronary revascularization subjects were divided into 2 groups depending on the implementation of the program of cardiovascular rehabilitation and secondary prevention. Group I - 89 patients- control group and group II -101 patients who had undergone the cardiovascular rehabilitation program. Initially there was no statistical difference in the age, gender, impaired coronary bed, the presence of old myocardial infarction, functional ?ass (?F) NYHA and the comorbidities. All patients were monitorised for 12 months.
The Results:The re-admission rate was high in both groups in the period of 6-12 months after the revascularization (group I 44.5% vs group II 13.3%, p <0.05). It was recorded a number of hospitalizations statistically significant in the control group comparatively with group II (78.9% vs 28.6%, p <0.05), with the prevalence of cardiac causes (group I 76.7% vs 25.7% , p <0.05). At 12 months of surveillance FC NYHA II was present in 41.8% patients in group I and 86.3% patients in group II (p <0.05). FC NYHA III - in 58.2% patients in group I and 5.5% patients in group II (p <0.05). EF at rest did not changed statistically significant in both groups, but after the dosed isometric exercise effort the EF increased by 11.46% (p <0.05) only in the rehabilitation group and was associated with improved wall motion score (Group I by 2.09% vs group II by 8.32%, p <0.05).
Conclusions:The application of cardiovascular rehabilitation program during the first year after coronary revascularization, have improved the left ventricular systolic function associated with a benign evolution of chronic heart failure and significantly reduced the rate of repeated hospitalizations.
Legend: *- significant differences between groups (p <0.05)
Parameters
Group 1
Group 2
Re-hospitalizations of cardiac causes
never, (n), %
21 (23,3%)
76 (72,4%)*
In the first 3 months, (n), %
12 (13,3%)
8 (7,6%)
In 3-6 months,(n), %
17 (18,9%)
7 (6,7%)*
In 6-12 months , (n), %
40 (44,5%)
14 (13,3%)*
P231
Musculoskeletal pain in patients with heart failure undergoing moderate and high intensity training
D Pereira Lima1, YGS Fontes1, SW Sties1, DC Bundchen1, AI Gonzales1, AV Souza1, T Carvalho1
1State University of Santa Catarina, Florianopolis, Brazil
Topic: Sports cardiology
Purpose:Exercise training reduce cardiovascular risk factors and has been recognized as an important and safe strategy for treating patients with heart failure (HF). However, factors as musculoskeletal pain, may represent a limiting factor for treatment, resulting in lack of progressive conditioning and exercise intolerance. The aim of this study was to investigate the influence of pain worsened by exercise in patients with heart failure undergoing moderate and high intensity training.
Methods:Twenty male patients (53.25 ± 8.87 years) with stable heart failure, left ventricle ejection fraction = 45%, were randomized for two groups: moderate continuous training (MCT) or high-intensity interval training (HIT). The subjects underwent 12 weeks of exercise training, three times per week, in MCT target zone of heart rate (HR) corresponding to anaerobic threshold (first ventilatory threshold) and in HIT the HR corresponding to respiratory compensation point (second ventilatory threshold) alternating with HR corresponding to anaerobic threshold (recovery period). Before and after the intervention were performed assessment of pain worsened by Musculoskeletal System Assessment Inventory (MSAI) and determination of VO2 peak by cardiopulmonary exercise testing. The data were analyzed using Shapiro-Wilk test, proportion comparison test (Med Calc), paired t test, t test for independent samples and the Mann Whitney U test, with significance level of 5%.
Results:The frequency of pain worsened by exercise percentage reduced only in HIT (11.1%, p = 0.92), while there was no change in the MCT. Only in HIT was observed significant increase in peak VO2 (from 21.07 ± 4.30 to 23.79 ± 5.26; p = 0.021). There was no significant difference in the gain of VO2 between patients with and without pain.
Conclusions:After 12 weeks of training was found that musculoskeletal pain did not influence the gain of cardiorespiratory fitness in patients with HF undergoing moderate or high intensity training.
P232
Heart rate response in transplant patients following a cardiac rehabilitation program
EM Cramaroc1, JI Castillo1, M Abeytua1, C Torres1, A Pintor1, T Martinez-Castellanos1, MA Ortega1, A Fernandez-Gonzalez1, DIEGO Ruiz-Molina1, F Fernandez-Aviles1
Purpose:Comparing the heart rate response in heart transplant patients versus ischemic heart disease patients after a cardiac rehabilitation program.
Methods:Comparative retrospective study involving 102 patients distributed into two groups: transplantation group (n = 50) and ischemic heart disease control group (n = 52), treated in a cardiac rehabilitation program (CRP) from June 2001 to July 2014. All of them were treated with CRP, during the first year after cardiac transplant (CT), consisting of a 50 minute session, performed 3 times a week for two months:warm-up, aerobic heart rate to certain training or modified Borg scale and stretching exercise.Exercise testing has been performed using the Bruce protocol before and after the training program.The following parameters have been collected in a database: time effort, basal heart rate and maximum reached, reserve heart rate and double product pre- and post-treatment. A statistical study has been performed using SPSS comparing both groups.
Results:There are 77 males and 25 females with an average age of 58 years. There are no statistical group differences in height, body mass index and cardiovascular risk factors. The diagnosis previous of CT was ischemic cardiopathie 50%, non-ischemic miocardiopathie 38% and others 12%.Regarding to the HR basal, pre- and post- treatment, no statistically significant differences between the two groups studied are found. In terms of maximum HR, time effort and METS reached pre- and post-treatment statistically significant differences in both transplant and ischemic heart disease groups are observed (table 1).
Conclusions:The basal heart rate is significantly higher in transplant patients as reserve heart rate improved in this group (P <0.05).This study demonstrates how after a short-term training program, a denervated heart behaves in a similar way to a heart with ischemic disease.
Safety and efficacy of pulmonary rehabilitation prior to surgery in patients with thoracic aortic disease -Importance of pre-operative respiratory tract clearance exercise
M Takeuchi1, Y Matsumoto1, S Kawamoto2, K Kumagai2, J Takahashi1, K Ito1, Y Sakata1, M Kohzuki3, Y Saiki2, H Shimokawa1
1Tohoku University Graduate School of Medicine, Department of Cardiovascular Medicine, Sendai, Japan
2Tohoku University Graduate School of Medicine, Department of Cardiovascular Surgery, Sendai, Japan
3Tohoku University Graduate School of Medicine, Department of Internal Medicine and Rehabilitation Science, Sendai, Japan
Topic: Sports cardiology
Purpose:The surgical procedures for thoracic aortic diseases (AD) such as aortic aneurysm are mostly invasive and are associated with pulmonary complications (PC), resulting in longer stay in intensive care unit (ICU). However, the strategy to prevent the complications remains to be elucidated. The pre-hospitalization period before surgery may be used to improve a patient's condition. Thus, we aimed to examine the safety of our pre-operative pulmonary rehabilitation (PR) program and its effects on post-operative PC and ICU stay before and after the implementation of the program in patients undergoing surgery for thoracic AD.
Methods:We retrospectively analyzed 265 consecutive patients who underwent surgery for thoracic AD and post-operative rehabilitation in our hospital between January 1, 2009 and December 31, 2013. Of these, 66 were excluded due to emergency surgery (n=27) and post-operative non-PC such as acute renal failure requiring hemodialysis or cerebral infarction (n=39). Pre-operative PR was performed (n=106, mean 9.1±8.0 days, 20 min/day) with ICU-assumed physical and respiratory exercises on the basis of active cycle breathing technique plus careful monitoring of blood pressure. All patients received conventional cardiovascular rehabilitation after the surgery. The decision for discharge from the ICU was subjectively made by an attending physician when the patient's physiologic status became stabilized (e.g. successful weaning from ventilator) and ICU monitoring and care were no longer needed.
Results:None of the patients presented adverse events of aortic rupture causing sudden death or emergency surgery during pre-operative PR. Among the patients undergoing major aortic replacement surgery, the mean length of ICU stay was significantly reduced in the group with pre-operative PR (+PR, n=84) than in that without it (-PR, n=64) (7.5±5.2 vs. 14.6±10.3 days, P<0.01). In addition, among the patients undergoing less invasive surgery of stent graft implantation, the stay was also significantly reduced in the +PR (n=22) than in the –PR (n=29) group (3.0±2.2 vs. 8.1±9.0 days, P<0.01). Age, gender, etiology of AD and pre-operative lung diseases were comparable between the +PR and –PR groups. Importantly, the length of ICU stay was significantly associated with post-operative PC (P<0.01).
Conclusions:The present study demonstrates for the first time the safety and potential importance of pre-operative PR program as a novel strategy to prevent longer ICU stay associated with PC in patients undergoing both invasive and less invasive surgery for thoracic AD.
P234
Effects of exercise training on heart rate response to exercise in heart transplant recipients
EG Ciolac1, RE Castro1, EA Bocchi2, GV Guimaraes2
1S?Paulo State University - UNESP, School of Sciences, Physical Education Department, Bauru, Brazil
2Heart Institute (InCor) - University of Sao Paulo Faculty of Medicine (FMUSP), Sao Paulo, Brazil
Background:Cardiac denervation following heart transplantation (HT) results in altered heart rate (HR) response to exercise, including delayed HR increase during exercise, lower levels of HR at maximal and submaximal efforts, and slow HR decrease after exercise cessation. Although exercise training (ET) has shown to improve most of these HR responses in healthy subjects, low is known about its effects in HT patients. Thus, the purpose of present study was to analyze the effect of ET on HR response to exercise in HT patients.
Methods:48 sedentary HT patients (age = 47 ± 3 years) were randomized in a 2:1 ratio to ET and control (CON) group, and performed a maximal graded exercise testing (GXT) before and after 12 weeks of follow-up. The ET consisted of thrice-weekly aerobic (30 min) and resistance training program (5 exercises) at intensity between 11 to 13 on the 6-20 rating of perceived effort scale. The HR change from resting to 40%, 60%, 80% and 100% of GXT workload, and the HR recovery at 1st, 2nd and 3rd min of GXT were compared between groups.
Results:ET was effective to improve cardiorespiratory fitness (8.6 ± 2.4 %) and exercise tolerance (18.3 ± 5.5 %) during follow-up (P < 0.01). Both groups did not improved HR change from resting to 40% and 60% of GXT workload. HR recovery also did not change during follow-up in both groups. However, the HR change from resting to 80% (10 ± 4 %) and 100% (9 ± 4%) of GXT workload were significant higher (P < 0.05) after ET (Figure 1) but not after CON follow-up.
Conclusion:Significant improvements were found in HR change from resting to 80% and 100% of GXT workload but not in HR recovery to exercise after the 12-week ET program. This result suggests that ET may be an effective tool for improving chronotropic incompetence but not HR recovery to exercise in heart transplant patients.
Conclusion:Significant improvements were found in HR change from resting to 80% and 100% of GXT workload but not in HR recovery to exercise after the 12-week ET program. This result suggests that ET may be an effective tool for improving chronotropic incompetence but not HR recovery to exercise in heart transplant patients.
P235
Safety and efficacy of cardiac rehabilitation programs in cardiac arrest survivors
Z Blazquez Bermejo1, R Dalmau Gonzalez-Gallarza1, CA Alvarez Ortega1, RA Mori Junco1, A Castro Conde1, E Lopez-De-Sa1, I Ponz De Antonio1, J Caro Codon1, D Gemma1, JL Lopez-Sendon1
1University Hospital La Paz, Cardiology, Madrid, Spain
Topic: Sports cardiology
Purpose:There is no data published about safety and efficacy of cardiac rehabilitation programs (CRP) in cardiac arrest survivors. The aim of this study is to analyse the impact of a CRP in these patients.
Methods:We retrospectively reviewed 33 patients included in a CRP after a cardiac arrest, between July 2006 and September 2014. The cause of cardiac arrest was acute myocardial infarction (AMI) in 78.8%, chronic ischemic heart disease in 12.1% and remained unknown in 9.1%. Therapeutic hypothermia had been used in 90.9% and initial rhythm was shockable in all patients. 64.3% of AMI were anterior. They had a mean of 1.52±0.97 severe-diseased vessels. An automatic defibrillator was implanted in 21.2%. We analysed the impact of CRPs on functional status and metabolic parameters.
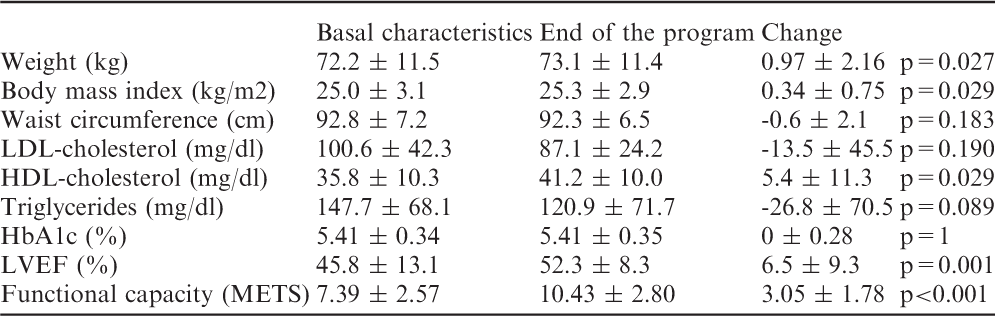
Results:See table. Mean age was 54.7±10.3 years and 87.9% were male. Mean duration of the program was 61.4±17.2 days. 6.5% of patients abandoned the program. One patient had a sudden cardiac death at his home after the basal visit, but before starting the program. No patient suffered any serious adverse event during the program. 26 patients (78.8%) were current smokers. 21 of this patients attended a 6-months follow-up inpatient visit: 85.7% remained abstinent from smoking (confirmed by co-oximetry <10 ppm).
Conclusions:CRPs in cardiac arrest survivors are safe, and they facilitate an improvement in life style, metabolic profile and functional capacity. There is a slight weight gain during the program, probably related to the significant weight loss during admission.
Basal characteristics
End of the program
Change
Weight (kg)
72.2 ± 11.5
73.1 ± 11.4
0.97 ± 2.16
p=0.027
Body mass index (kg/m2)
25.0 ± 3.1
25.3 ± 2.9
0.34 ± 0.75
p=0.029
Waist circumference (cm)
92.8 ± 7.2
92.3 ± 6.5
-0.6 ± 2.1
p=0.183
LDL-cholesterol (mg/dl)
100.6 ± 42.3
87.1 ± 24.2
-13.5 ± 45.5
p=0.190
HDL-cholesterol (mg/dl)
35.8 ± 10.3
41.2 ± 10.0
5.4 ± 11.3
p=0.029
Triglycerides (mg/dl)
147.7 ± 68.1
120.9 ± 71.7
-26.8 ± 70.5
p=0.089
HbA1c (%)
5.41 ± 0.34
5.41 ± 0.35
0 ± 0.28
p=1
LVEF (%)
45.8 ± 13.1
52.3 ± 8.3
6.5 ± 9.3
p=0.001
Functional capacity (METS)
7.39 ± 2.57
10.43 ± 2.80
3.05 ± 1.78
p<0.001
P236
Stratifying patients for cardiac rehabilitation - is it worth to rehabilitate low risk patients after an acute coronary syndrome?
S Aguiar Rosa1, A Abreu1, R M Soares1, P Rio1, I Rodrigues1, A Monteiro1, D Mesquita2, G Portugal1, T Alves1, R Cruz Ferreira1
1Hospital de Santa Marta, Cardiology, Lisbon, Portugal
2Hospital N.S. Rosario, Cardiology, Barreiro, Portugal
Topic: Sports cardiology
Purpose:Cardiac rehabilitation (CR) is a significant component in care for patients (pts) with cardiovascular disease. The American Association of Cardiovascular and Pulmonary Rehabilitation (AACPR) risk stratification criteria have been used to stratify CR pts according to the risk for clinical events and to adjust exercise training(ET) program. CR has been put in doubt for low risk pts. The aim of the present study is to compare the CR impact in pts with low (LR) vs moderate/high risk (MHR), according to AACPR criteria, in order to check the real functional benefit of CR for LR pts.
Methods:Retrospective analysis of consecutive pts who suffered an acute coronary syndrome(ACS) and underwent CR and cardiopulmonary exercise testing(CPET), between Jan/04 and Dec/13. A CPET was performed at baseline (pre) and after (post) 30 ET sessions. CPET parameters: peak oxygen uptake(pVO2), percentage of predicted pVO2(%predicted pVO2), minute ventilation/CO2 production(VE/VCO2) slope, VE/VCO2slope/pVO2 and peak circulatory power(PCP)(pVO2 x peak SBP). Also, the difference between pre and post pVO2(?O2) and %predicted pVO2(?redicted pVO2) were calculated. Pts were stratified according to AACPR criteria. Pts with left ventricular ejection fraction (LVEF)>50% and functional capacity>7.0 METs in preCPET were included in LR and the remaining pts in MHR.
Results:130 pts, 86% male, mean age 56.8±10.9 years were analysed. 113 pts (86.9%) had STEMI and 17pts (13.1%) NST-ACS. 47pts were classified in MHR and 83 pts in LR. Comparing both groups, CPET duration increased 2.53 minutes in MHR vs 1.4 minutes in LR (p=0.014) after CR. A trend to a greater improvement in pVO2 (?O2 3.4 vs 1.8; p=0.074) and %predicted pVO2 (?redicted pVO2 11.2%vs4.5%; p=0.087) was found in MHR. In MHR, 27 pts (57.4%) got an improvement in pVO2>10%. These pts trend to be younger (55.9±11.9vs60.7±5.3years; p=0.107) and with more impairment in left ventricular function (LVEF 41.9±9.1%vs48.2±11.0%; p=0.052) comparing with MHR pts without such improvement in functional capacity. Despite of a milder improvement, LR also benefitted to underwent CR, with an increase in pVO2 from 26.7±7.0 to 28.5±7.3 (p=0.012) and in CPET duration from 14.2±2.5 to 15.6±2.3 minutes (p<0.001).
Conclusion:1. Moderate/high risk pts, according to AACPR risk stratification criteria, seem to have more gain in functional capacity after cardiac rehabilitation, evaluated by CPET, comparing to low risk patient, being this benefit higher in lower LVEF pts. 2. Low risk pts, even though with smaller gain, also achieve a better functional capacity after cardiac rehabilitation.
P237
Measured versus self-reported body mass index in patients after an acute coronary syndrome undergoing cardiac rehabilitation
ZA Domagala1, P Dabrowski1, B Kurc-Darak1, K Womperski2, L Rusiecki3, E Sylwina-Krauz4, B Gworys1, D Kalka5
1Wroclaw Medical University, Department of Normal Anatomy, Wroclaw, Poland
2Center of Cardiac Rehabilitation, Ministry of Interior Hospital, Glucholazy, Poland
3Wroclaw Medical University, Department of Pathophysiology, Wroclaw, Poland
4Medinet Heart Center, Ltd., Cardiac rehabilitation, Wroclaw, Poland
5Centre for Men's Health , Wroclaw, Poland
Topic: Sports cardiology
Purpose:The basic anthropometric data (body weight and height), are some of the most frequently analyzed somatometric parameters. The easiest and most objective, and frequently used, method of assessing the degree of obesity is calculating the BMI (Body Mass Index). BMI is usually calculated based on declared data or measurements made on equipment with or without any certification, by healthcare staff. Obesity is one of the cardiac risk factor. Imprecise estimation of that risk factor might influence on future cardiac treatment. Therefore the question remains, whether declared somatic data help provide an accurate calculation of BMI in patients suffering from ischaemic heart disease. The aim of work was comparing the declared and actual BMI in patients suffering from coronary artery disease.
Material and Methods:The study population included 100 subjects, treated for coronary artery disease and undergoing the cardiac rehabilitation. The patients were asked to supply their body weight and height. At the same time a three-person study team took measurements, which were later the basis for verification and objective assessment of the data provided by the patients. The measurements were taken before noon, with the patient dressed only in undergarments. Body mass was determined with a certified Radwag scale, with measurement accuracy up to 0.00001kg. Body height was determined with a certified Holtain anthropometer, with measurement accuracy up to 0.00001m. Each measurement was taken three times and the mean of all three measurements was used for statistical analysis. The instruments used in the study are CE certified and in accordance with directive MDD93/42EEC on medical instruments and appliances. BMI was calculated as the patient's weight in kilograms divided by the squared height in metres. Statistical analysis was performed with Statistics 11.0 PL software.
Results:The analysis of mean results for the assessed group of patients has shown the presence of statistically significant differences between declared and actual data (BMIdeclared 27.94 vs BMIactual 29.58; p=0.000). The differences were observed for both male (BMIdeclared 27.67vs BMIactual 29.01; p=0.000) and female data (BMIdeclared 28.46 vs BMIactual 30.70; p=0.000) study population.
Conclusion:The differences between declared and actual data point to highly subjective self-assessment, which disqualifies the declared data in the context of monitoring of treatment and cardiac rehabilitation processes.
P238
The effect of physical exercise on quality of life in patients with paroxysmal or persistent atrial fibrillation, a randomized study.
S Hakmann1, AK Skielboe1, U Dixen1
1Hvidovre UniversityHospital, Copenhagen, Denmark
Topic: Sports cardiology
Purpose:Atrial fibrillation (AF), the most common cardiac arrhythmia, is associated with increased morbidity and mortality. Regular physical exercise is related to improved quality of life (QoL) and survival in healthy individuals and patients with cardiovascular disorder. Physical training is fully implemented in the standard rehabilitation of patients with ischemic heart disease and congestive heart failure. In clinical practice, there is no such offer to patient with AF, even though these patients often experience reduced exercise capacity and impaired QoL. The aim of this study is to determine if physical exercise improves QoL in patients with paroxysmal or persistent AF.
Methods:In a randomized clinical trial, 72 patients with AF (63 ± 9 years) were randomized to a three-month low-intensity or high intensity training program. The training consisted of aerobic exercise supervised by a physiotherapist. Eight weeks prior to the physical exercise, the patients completed a nurse-led rehabilitation program. Quality of life was measured with self-administered Short Form 36 questionnaire (SF-36), at baseline, before physical exercise (n= 52) and after physical exercise (n=52).
Results:Improved QoL were observed in the low intensity group in three of the eight SF-36 subscales: physical role functioning, vitality and mental health (p < 0.01). The SF-36 mental component summary scale also increased significantly after the low-intensity training period (p = 0.007). No change at the high intensity group was observed before and after training. There was no statistically significant difference in SF-36 between the groups at baseline, except for the subscale bodily pain, where the high intensity group have more pain than the low intensity group before training (p<0.05).
Conclusion:In patients with paroxysmal or persistent AF, a positive effect on QoL was observed after participation in a low-intensity aerobic exercise program, while no effect was observed from a high-intensity exercise program. This study may help to implement physical exercise as a part of rehabilitation to patients with AF.
P240
Impact of cardiac rehabilitation after acute coronary syndrome on functional capacity measured by cardiopulmonary exercise testing
S Aguiar Rosa1, A Abreu1, R M Soares1, P Rio1, I Rodrigues1, A Monteiro1, D Mesquita2, A Gaspar3, S Alves1, R Cruz Ferreira1
1Hospital de Santa Marta, Cardiology, Lisbon, Portugal
2Hospital N.S. Rosario, Cardiology, Barreiro, Portugal
3Hospital dos Capuchos, Internal Medicine, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Lifestyle intervention, including exercise habits, is a cornerstone in secondary prevention for patients (pts) with cardiovascular disease. Cardiac rehabilitation (CR) has a main role, including besides prevention, specific exercise training programs. The purpose of the present study was to assess the CR benefit on functional capacity after acute coronary syndrome (ACS), evaluated by cardiopulmonary exercise testing (CPET).
Methods:Retrospective analysis of pts who underwent CR after ACS, between January 2004 and December 2013. A CPET was performed at baseline and after 30 exercise training sessions. Exercise sessions were performed in hospital, twice a week, 60 minutes duration. The following parameters were evaluated: peak oxygen uptake (pVO2), percentage of predicted pVO2, minute ventilation/CO2 production (VE/VCO2) slope, VE/VCO2slope/pVO2, peak circulatory power (PCP), (pVO2 x peak systolic blood pressure).
Results:130 pts, 86% men, mean age of 56.8±10.9 years were analysed. Of these, 113 pts (86.9%) had ST-elevation myocardial infarction (STEMI) diagnosed and 17 pts (13.1%) non-ST-elevation ACS. Mean left ventricular ejection fraction was 54.3±10.1%. After CR, CPET showed: pVO2 increased from 25.6±6.7 to 27.9±7.2ml/kg/min (p<0.001); percentage of predicted pVO2 increased from 89.6±23.1% to 96.2±26.8% (p=0.006), VE/VCO2 slope decreased from 26.6±5.8 to 25.8±5.1 (p=0.042), VE/VCO2slope/pVO2 decreased from 1.13±0.4 to 0.99±0.5 (p<0.001), PCP increased from 4351.4±1437.1 to 4760.8±1389.6 mmHg.ml/kg/min (p<0.001). CPET duration also increased from 12.5±4.3 to 15.2±2.8 minutes (p<0.001). When STEMI pts were analysed separately, a greater improvement in functional capacity was observed, with an increase in pVO2 from 25.6±6.6 to 28.2±7.4 ml/kg/min (p<0.001). In non-ST-elevation ACS pts, only a mild increase in pVO2 after CR was demonstrated (25.6±7.3 vs 26.3±5.4 ml/kg/min, p=0.59), however a significant improvement in CPET duration was achieved (11.7±5.8 to 14.9±2.5 minutes, p=0.01).
Conclusion:Cardiac rehabilitation resulted in evident, objective, functional capacity benefit of ACS pts, particularly in STEMI (87% of CR pts). A significant improvement in CPET parameters was achieved after a 30 sessions exercise training program.
P241
Postoperative cardiac rehabilitation after implantation of left ventricular assist devices: Are there gender differences?
C Marko1, T Lackner2, E Xhelili3, M Feilmair3, D Zimpfer4, H Schima3, R Mueller5, F Moscato3
1Ambulatory Rehabilitation Center, Vienna, Austria
2Rehabilitation Center Felbring, Muthmannsdorf, Austria
3Center for Medical Physics and Biomedical Engineering, Medical University of Vienna, Vienna, Austria
4Medical University of Vienna, Department of Cardiac Surgery, Vienna, Austria
5Pensionsversicherungsanstalt, Vienna, Austria
Topic: Sports cardiology
Purpose:In studies concerning the postoperative rehabilitation of patients after implantation of left ventricular assist devices (LVAD) there are few data about the demographics and the outcome in women compared to men.
Methods:We retrospectively analyzed data from 104 patients (15 females, 89 males) who underwent cardiac rehabilitation between March 2010 and July 2014 after LVAD implantation. The exercise training consisted of interval bicycle training, strength training, training in walking and gymnastic groups. The change in intensity of the bicycle training (consisting of 12 modules with increasing intensity – e.g. module #1= 1W/5W, 60s/30s to module #12= 5W/150W, 60s/20s) as well as of strength for two muscle groups of the lower limbs were documented. Demographic data together with exercise training data and spiroergometry test data were analyzed, particularly focusing on the gender difference.
Results:Patients were admitted to the rehabilitation clinic (female vs male) 49±41 vs 48±38 days (p=0,442) after LVAD implantation for a period of 31±7 vs. 35±9 days (p=0,147). Female patients were younger than men (51±15 vs.59±9 years, p=0,122), had a lower range of comorbidities (Diabetes mellitus: 6,7% vs 32% p=0,048, chronic obstructive pulmonary disease 7 % vs 20% p=0,239) and suffered mostly from a dilatative cardiomyopathy (60% vs 33% p=0,041) and less from an ischemic cardiomyopathy (40% vs 62% p=0,113). Apart from smoking, which had the same incidence in both groups (40%) the cardiovascular risk profile was lower for women than for men (Hyperlipid?a: 27% vs 62% p=0,011, Hypertension: 7% vs 36% p=0,024). An improvement for women at the end of the rehabilitation was observed for the intensity of the bicycle ergometer training (Module #6±2 vs. #2±1, p=0.003), for the muscular strength (leg-press: 26±12 vs. 24±14 kg p=0.582, leg extensor: 8±5 vs.6±4, p=0.272) as well as for walking- and gymnastic training. Comparing the percentage of the reference value of peak.VO2, a better functional capacity was observed in women than in men (46 ±14 vs 39±13% p=0,079).
Conclusions:Even if the number of women participating in the program compared to men was lower, thus limiting the study, cardiac rehabilitation demonstrated to be effective also for women. Most likely the better functional capacity of women in the percentage of the reference value is in relation to their lower range of comorbidities and lower cardiovascular risc profile compared to men.
P242
Clinical outcomes in patients with ST-elevation myocardial infarction and partial revascularization included in a cardiac rehabilitation program
R A Mori Junco1, R Dalmau Gonzalez-Gallarza1, A Castro Conde1, O Gonzalez Fernandez1, C Alvarez Ortega1, Z Blazquez Bermejo1, J Caro Codon1, I Ponz De Antonio1, JL Lopez Sendon1
1University Hospital La Paz, Cardiology, Madrid, Spain
Background:Patients with acute ST-segment elevation myocardial infarction (STEMI) are effectively treated with emergency angioplasty. Although there is debate, current guidelines recommendations encourage the use of culprit only percutaneous coronary intervention (PCI) in patients with STEMI and multivessel disease, excluding cardiogenic shock. Little is known if a cardiac rehabilitation program influences prognosis for these patients.
Topic: Sports cardiology
Purpose:Determine the incidence of cardiovascular events, repeated coronary revascularization, hospital admissions for cardiovascular reasons and mortality in patients with acute STEMI and culprit vessel only intervention, included in a cardiac rehabilitation program.
Methods:We retrospectively reviewed 143 STEMI patients with multivessel disease and culprit only PCI, enrolled in a cardiac rehabilitation program, between July 2006 and November 2013.The cardiac rehabilitation program included physical training, dietary and pharmacotherapy counseling and a specific smoking cessation follow- up when needed. The outcome measured the incidence of cardiovascular events, new percutaneous coronary intervention, hospital admissions for cardiovascular reasons and mortality.
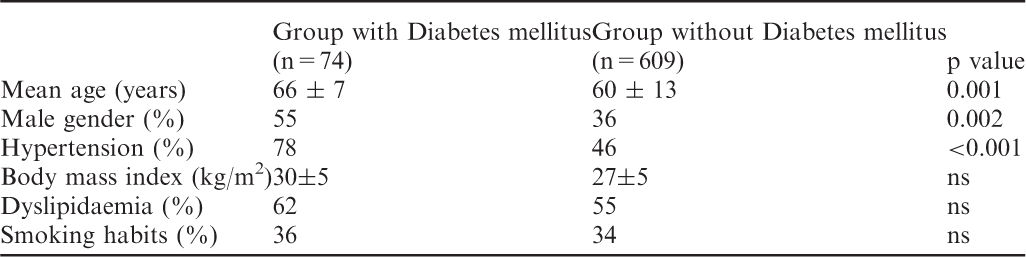
Results:In our study, mean age was 59.3 years and 87% of patients were male. 57.3% of them had hypertension, 34% had diabetes mellitus, 65.7% had dyslipidemia, 24.5% were obese, 52% were current smokers and 14.7% had previous coronary heart disease. The infarct location was the inferior surface in 49% and the anterior surface in 39.2%. 67 (55.5%) had stenosis of three arteries and 36 (25%) had severe left ventricular dysfunction. During a mean follow up of 43 months, cardiovascular events occurred in 23 (16.4%) patients; 12 (8.6%) experienced a non-ST segment elevation myocardial infarction (NSTEMI), 4 patients (2.9%) a new STEMI, 4 (2.9%) a stroke and 3 (2.1%) an acute peripheral artery disease. During follow up, 26 (18.6%) patients were hospitalized for cardiovascular reasons, 14 (10%) needed a revascularization for second time and 1 (0.7%) died.
Conclusions:In this group of patients with multivessel coronary disease who underwent culprit vessel only PCI for acute STEMI and were included in a cardiac rehabilitation program, the incidence of cardiovascular events was 16.4%, while the need of repeating a revascularization was 10%. The mortality rate (0.7%) was very low.
P243
The role of relaxation therapy in a cardiac rehabilitation program: a retrospective analysis of the effects on cardiovascular outcomes.
V De Simone1, G Castello1, L Fontana1, S Pasqualotto1, G Pasqualin1, S Armani1, F Filippi1, A Variola2, G Menegatti2, C Vassanelli1
1University of Verona, Verona, Italy
2University Hospital, Verona, Italy
Topic: Sports cardiology
Purpose:To establish the effects of psychological intervention (relaxation and guided imagery) on the recovery from a cardiac ischaemic event.
Methods:Patients (pts) with recent history of acute coronary syndrome (ACS) treated with coronary angioplasty recruited by our cardiac rehabilitation service from November 2012 to October 2013 were retrospectively evaluated. Our rehab program included exercise training, lifestyle counseling and clinical evaluations. A group (relaxation group) participated also in a relaxation training consisting of seven sessions of one hour and a half of guided imagery, muscular relaxation exercises and breathing techniques. 138 pts (90.6% males, mean age 58±9, 47.8% STEMI, 33.4% NSTEMI, 18.8% unstable angina) were evaluated; 40 was in the relaxation group. Pts unable to perform a cycle ergometer test (CET) and older than 75 years old were excluded. Cardiovascular outcomes (new coronary events, arrhythmias, clinical parameters and data derived by CET at baseline and at 6 months) were compared between pts experiencing relaxation or not (RL vs nRL).
Results:The incidence of new coronary events, arrhythmias and episodes of angina was higher in nRL group, but without statistical differences between the two groups. At the beginning of exercise training 70.3% pts (n = 97) had reduced exercise tolerance (ratio of the achieved and the predicted METs < .80); at six months, in the RL group there was significantly more pts than the nRL group who presented normal exercise tolerance (11 of 29 pts, 38% vs 13 of 68 pts, 19%; p .035). No significant differences were found in the trend of other important predictors of mortality obtained by CE as heart rate recovery (at first minute after peak exercise), chronotropic index, delta (peak-rest) heart rate, rate pressure product and ventricular arrhythmias in the recovery period. No statistical differences were found also in the lowering of LDL cholesterol values at baseline and at 6 monhts.
Conclusions:Even if relaxation therapy is shown not to clearly improve the prognosis of coronary heart disease (CHD) patients, it may constitute an important (and safe) tool of cardiac rehabilitation services for the role on the psychological well-being and quality of life. Small sample size does not allow an adequate statistical power to detect significant differences in the outcomes. The result on exercise tolerance will be confirmed in other larger and prospective studies, probably considering also other potential prognostic marker of cardiovascular death such as the QT dispersion and the heart rate variability.
P244
Automatic detection of exercise oscillatory ventilation in cardiopulmonary exercise testing: developing an accurate and practical graphical user interface.
J Cornelis1, K Poppe2, Q Claes2, M Deconinck2, T Van Assche2, P Beckers3, C Vrints3, D Vissers1, M Goossens2
1University of Antwerp, Department of Physiotherapy (REVAKI), Antwerp, Belgium
2University of Antwerp, Applied Engineering, Antwerp, Belgium
3University of Antwerp Hospital (Edegem), Department of Cardiology, Antwerp, Belgium
Topic: Sports cardiology
Purpose:Exercise Oscillatory Ventilation (EOV) is a prognostic marker assessed during a Cardio Pulmonary Exercise Test (CPET) predicting early mortality in patients with Chronic Heart Failure (CHF). Up till now a gold standard definition is not described. This case study implements four of the commonly used definitions of EOV into a Graphical User Interface (GUI) in order to automate, compare and objectively assess EOV in an accurate, practical and consistent way.
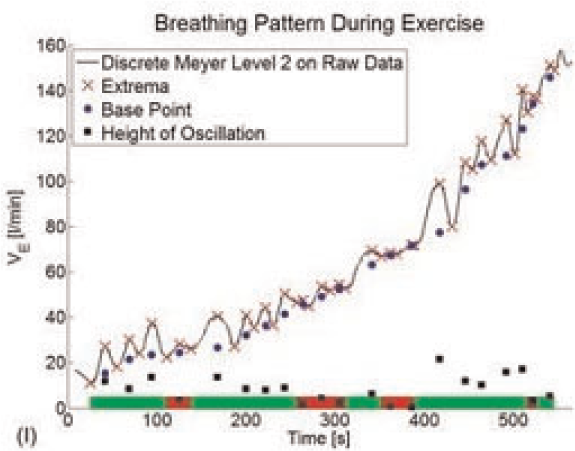
Methods:Breath-by-breath Minute Ventilation, collected during incremental CPET bicycle Ramp test (40Watt+20Watt/min) of a CHF patient with possible EOV, was analysed retrospectively. Several wavelet transformations were applied and compared, resulting in the use of a 2nd level discrete Meyer transformation. In order to quantify the oscillations, a local minima, -maxima and related time interval detection algorithm was implemented. This way the length between two local minima and the height of each oscillation could be determined. The number of oscillations according to the proposed criteria was recorded (marked zones in figure) and expressed as a percentage of the total exercise time.
Results:This novel GUI provides a visual presentation (see figure) of areas meeting the criteria according to the respective implemented definitions. In this case, EOV was present according all four formulae.
Conclusion:Automatic detection of EOV using a pre-programmed GUI could be a more valid and reliable method compared to visual or manual detection. It gives the possibility to overview the results of existing formulae at a glance. Moreover, this GUI could be integrated in existing CPET software making computerized analysis of EOV readily available.
EOV detection according to 1 definition
P245
Exercise functional capacity after aortic valve replacement in elderly patients - differences between transcathether versus surgical approach
G Portugal1, A Abreu1, A V Monteiro1, L Patricio1, D Cacela1, I Rodrigues1, P Pinto Teixeira1, S Silva1, R Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Background:Transcathether aortic valve replacement (TAVI) is an established treatment in severe aortic stenosis in high-risk or inoperable patients, and an alternative to surgical aortic valve replacement (SAVR). However there is few published data on the long-term effect of TAVI on functional exercise capacity in comparison to SAVR.
Aims:To assess the differences between exercise functional capacity after TAVI and SAVR, as assessed by cardiopulmonary testing (CPT) Methods:A total of 25 patients,15 post TAVI and 10 age-matched SAVR controls, were submitted to CPT utilizing a modified, low-intensity treadmill protocol adapted to frail, elderly patients. Data was collected on baseline characteristics and CPT parameters. Predicted VO2 max was calculated according to the Hansen equation. The main outcome was percentage of predicted peak VO2 consumption. Statistical significance was assessed utilizing the Fischer exact test or Mann-Whitney rank-sum test when appropriate.
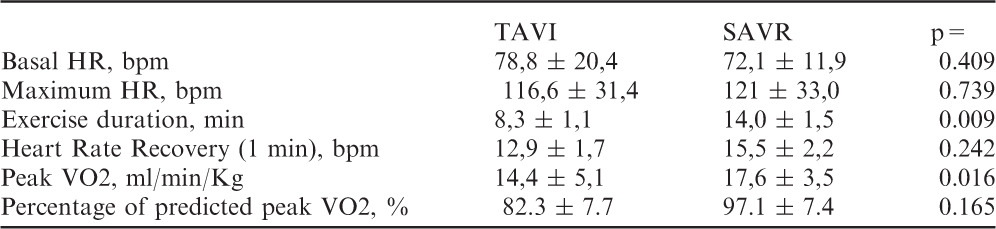
Results:No significant differences were found regarding age (80.0+/- 6.7 vs 80.1 +/- 3.7 yrs), body mass index (25.7+/-3.8 vs 27.8 +/-3.6), cardiovascular risk factors or ongoing medication (TAVI vs SAVR, p=NS for all). Mean time since implantation was 13.0 +/- 2.8 months in TAVI patients and 14.8 +/- 6.0 months after SAVR (p=NS). Both the logistic Euroscore (15.2+/-7.7 vs 8.8 +/- 3.7) and frailty index (9.4 +/-5.8 vs 7.4 +/-3.5) were higher in TAVI patients. CPT results are presented in table 1.
Conclusion:Despite being employed in a higher-risk population, no differences were found regarding age-corrected peak VO2 consumption after AVR in TAVI versus SAVR patients. At a mean follow-up of 13 months, TAVI afforded similar benefit regarding maximal oxygen consumption as SAVR.
TAVI
SAVR
p=
Basal HR, bpm
78,8 ± 20,4
72,1 ± 11,9
0.409
Maximum HR, bpm
116,6 ± 31,4
121 ± 33,0
0.739
Exercise duration, min
8,3 ± 1,1
14,0 ± 1,5
0.009
Heart Rate Recovery (1 min), bpm
12,9 ± 1,7
15,5 ± 2,2
0.242
Peak VO2, ml/min/Kg
14,4 ± 5,1
17,6 ± 3,5
0.016
Percentage of predicted peak VO2, %
82.3 ± 7.7
97.1 ± 7.4
0.165
P246
Characteristics of sarcopenia in patients with chronic heart failure
H Obata1, T Izumi2, H Watanabe1, W Mitsuma3, A Tomii4, T Sakai5, A Uehara2, T Minamino1
1Niigata University, Niigata, Japan
2Niigata Minami Hospital, Niigata, Japan
3Shinrakuen Hospital, Niigata, Japan
4Niigata Medical Center, Niigata, Japan
5Saiseikai Niigata Daini Hospital, Niigata, Japan
Background:While loss of skeletal muscle mass (sarcopenia) is a major determinant of reduced strength in aging individuals, some patients with heart failure also have sarcopenia. However, the characteristics of sarcopenia in patients with heart failure are not well known.
Methods:This prospective, multicentric study included patients with chronic heart failure who underwent phase 2 cardiac rehabilitation in our institutions. Sarcopenia was defined as the presence of both poor muscle function (low physical performance and/or low muscle strength) and low muscle mass measured by dual x-ray absorptiometry, according to the European Working Group guideline. The characteristics of sarcopenia in patients with heart failure were compared with those in age-matched control individuals from the general population in the literatures.
Results:This study included 49 patients (mean age, 68±13 years; 16 women [33%]). The mean left ventricular ejection fraction was 50±18, and the NYHA functional class was 1.9±0.7. There were 17 patients (35%) with sarcopenia, 27 patients (55%) with decreased muscle mass, 6 patients (12%) with low physical performance, and 28 patients (57%) with low muscle strength. Weight-adjusted appendicular skeletal muscle mass inversely correlated with age (r = -0.32; p = 0.027) and positively correlated with handgrip strength (r = 0.77; p < 0.001) and knee extension strength (r = 0.69; p < 0.001). Interestingly, weight-adjusted appendicular skeletal muscle mass inversely correlated with percent of lower limb fat (r = -0.34; p = 0.016). However, left ventricular ejection fraction did not correlate with skeletal muscle mass, muscle strength, or walking speed. When compared with control individual from the general population, the prevalence of low physical performance, muscle strength, and muscle mass was higher in patients with chronic heart failure.
Conclusions:In patients with chronic heart failure, the prevalence of sarcopenia was higher compared with that in the general population. Interestingly, their weight-adjusted appendicular skeletal muscle mass inversely correlated with percent of lower limb fat. Screening for sarcopenia and appropriate rehabilitation may be required in patients with heart failure.
P248
Improvement of cognitive functions and quality of life in patients with heart failure after exercise training
H Zauner1, G Wood2, J Altenberger1, HC Nuerk2, K Wallner1
1SKA-RZ Grossgmain (PV), Grossgmain, Austria
2University of Salzburg, Salzburg, Austria
IntroductionHeart failure with reduced ejection fraction is associated with impaired cardiac output consequently leading to reduced cerebral perfusion and in turn to cognitive deficits. The aim of the this study was to evaluate the outcome of physical exercise training on specific cognitive domains among patients with heart failure compared to controls not undergoing such training.
Methods:30 heart failure patients, NYHA classes II-III (mean ejection fraction 34%, SD±8.4), mean age (62.8±8.9 years) took part in this prospective non-randomized study. The training group (n=20) underwent a supervised resistance training on a bicycle 20 minutes a day, five times a week, for four weeks. The control group (n=10) patients did not undergo training. After initial measurement of echocardiogram, patients' cognitive functions were assessed in the domains of memory, general intelligence, attention, executive functions, quality of life and numerical cognition. After the training program, all measurements were repeated.
Results:Scores in the cognitive measures did not differ between control and training group in the pre-test. In the post-test, in contrast, the training group showed significant better scores in NPC-test of numerical abilities (concerning addition principles) (p=0.037), reaction time in divided attention (p=0.018), and health related quality of life (SF-36) score (p=0.037) while the control group did not improve in any measure of cognitive functioning. Comparisons between pre- and post-test confirmed that only the training group improved significantly in these assessment scores.
Conclusion:Regular exercise training in heart failure patients is associated with an improvement in selected cognitive functions and health related quality of life.
P249
Autonomic function after cardiac rehabilitation - which patients benefit most?
P Rio1, A Abreu1, R Soares1, T Pereira-Da-Silva1, A Viveiros Monteiro1, S Aguiar Rosa1, I Rodrigues1, M Afonso Nogueira1, P Pinto-Teixeira1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Reduced heart rate variability (HRV) has been documented to be a marker for prognosis in patients (pts) with cardiac disease. Cardiac rehabilitation (CR) enhances autonomic function and this seems to correlate with increased exercise capacity. The main objectives of this study to evaluate the effect of a 12-week training program on HRV and examine the correlation between this, the functional capacity and left ventricular ejection function (LVEF).
Methods:Retrospective analysis of consecutive patients (pts) who underwent CR program (2004-2013), in a single center. 24-hour Holter HRV study, cardiopulmonary exercise testing (CPET), echocardiogram and blood tests were performed at baseline and after 36 exercise training sessions. Exercise sessions were performed in hospital, three times a week, 60 minutes duration. The following parameters were evaluated: standard deviation of the average of NN intervals (SDNN), resting heart rate (RHR), HR reserve, peak oxygen uptake (pVO2), LVEF, HDL-cholesterol level and brain natriuretic peptide (BNP). Pts were analysed according to pre SDNN (<100 vs =100 ms).
Results:We analysed 168 pts, 85% male, mean age 57.3±10.4 years: Of these, 55% had ST-elevation myocardial infarction (STEMI) diagnosed, 25% non-ST-elevation ACS, 12% stable coronary artery disease and 8% heart failure. The analysis according to SDDN results is shown on the table.
Conclusion:Patients with baseline autonomic dysfunction had more significant improvement, after cardiac rehabilitation, in heart rate variability, functional capacity, left ventricular systolic function and brain natriuretic peptide.
*for the differences between the two groups.ns = not significant
SDDN < 100 (n=60)
SDNN =100 (n=108)
Parameters
Before CR
After CR
Variation
p value
Before CR
After CR
Variation
p value
p value*
SDNN ( ms )
80.9 ± 12.5
104.1 ± 34.7
23.1 ± 35.7
<0.001
143.3 ± 34.2
140.9 ± 40.2
- 2.4 ± 31.4
0.479
< 0.001
Basal HR ( bpm )
73 ± 12.9
70.9 ± 10.4
- 2.1 ± 9.9
0.122
70.5 ± 9.4
67.9 10.9
- 2.6 ± 12.1
0.037
ns
HR reserve ( bpm )
62.4 ± 19.2
66.8 ± 18.6
4.4 ± 17.9
0.042
68.4 ± 20.7
72.6 ± 21.9
4.1 ± 18.1
0.027
ns
pVO 2 (mL/Kg/min)
24 ± 6.8
26.4 ±7
2.5 ± 6.7
0.01
26.1 ± 6.8
27.7 ± 7.3
1.6 ± 5.3
0.007
0.04
pVO 2 (%)
86.9 ± 23.6
98.3 ± 30.5
11.4 ± 29.8
0.008
92.3 ± 24.6
95.1 ± 26.5
2.8 ± 23.2
0.269
0.048
LVEF (%)
50.6 ± 11.4
53.7 ± 11.3
3.1 ± 8.6
0.019
56.1 ± 9.7
56.3 ± 9.4
0.1 ± 8.1
0.898
0.045
BNP ( pg /mL)
252 ± 198.1
100.8 ± 75.7
- 151.2 ± 179
0.008
99.8 ±83
39.2 ± 24.2
- 60.6 ± 83.1
0.008
0.043
HDL (mg/mL)
38.9 ± 10.7
41.6 ± 11.1
2.7 ± 8.5
0.03
39.4 ±11
42.1 ± 9.5
2.7 ± 9.1
0.01
ns
P250
Sustained effects of heated water-based exercise training on blood pressure after detraining in patients with resistant hypertension.
GV Guimaraes1, LGB Cruz1, MM Fernandes-Silva1, RE Castro1, EA Bocchi1
1Heart Institute (InCor) - University of Sao Paulo Faculty of Medicine Clinics Hospital, Sao Paulo, Brazil
Background:In resistant hypertension (RH), water-based exercise training (HEx) has beneficial effects on blood pressure. The cessation of exercise training has been associated with a partial or complete loss of physiological adaptations, as a consequence of detraining period. Thus, the purpose of this study was to investigate the effect of 12 weeks of detraining after HEx on blood pressure in RH.
Methods:32 patients (HEx n=16; control n=16) were randomized and there was no lost of follow-up. HEx group was submitted to 36 sessions (60 min) in a heated pool (32o C) during 12 weeks, followed by 12 weeks of detraining period. Control group was evaluated during the same period and instructed to maintain their habitual activities. The 24-hour ambulatory blood pressure monitoring (ABP) was measured at baseline, after 12 weeks of intervention and after 12 weeks of detraining.
Results:Baseline office and ambulatory BPs did not differ between HEx and control group. At the end of training period (12 weeks), the HEx group had significantly lower systolic and diastolic BPs in than the control group, respectively, 24-hours (119.9±12 vs 143.7±23 mmHg, p=0.002; and 71.7±10 vs 83.1±9 mmHg, p=0.002); daytime (121.0±12 vs 149±22 mmHg, p=0.001; and 72.3±11 vs 83.1±8 mmHg, p>0.001) and nighttime (112.9±12 vs 136.2±19, p>0.001; and 66.4±10 vs 76.7±9 mmHg, p=0.007). After the 12 additional weeks of detraining, the ABPs in the HEx group were still lower than the control group for both systolic and diastolic measurements, respectively, 24-hours (129.7±19 vs 147.1±26 mmHg, p=0.03; and 75.6±12 vs 82.3±10,p=0.07), daytime (130.8±19 vs 152.1±24 mmHg, p=0.01, and 77.7±14 vs 87.1±9 mmHg, p=0.03) and nighttime (119.7±18 vs 141.3±25 mmHg, p=0.009, and 68.5±12 vs 77.0±12 mmHg, p=0.06), although the differences were attenuated.
Conclusion:These results indicate that the effects of HEx on blood pressure persist even after 12 weeks of its cessation in patients with resistant hypertension, although they may have been blunted over time.
P251
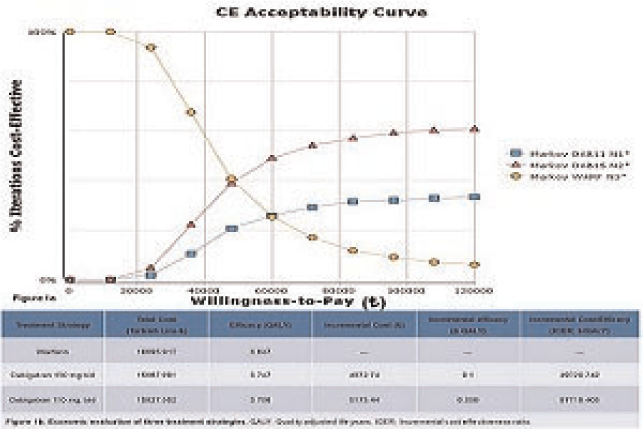
Clinical experience with combination therapy with Olmesartan and Amlodipine in treatment of resistant hypertension
C James1, S Tisheva1, A Yanakeva1, N Stancheva1, D Yakova1, M Hristov1, K Gospodinov1, T Chakolova1
1Medical University Pleven, Pleven, Bulgaria
Objective:The objective of this study is to analyse the effect of fixed dose combination therapy with Olmesartan/Amlodipine in the treatment of Resistant Hypertension.
Design:Questionnaire based cross sectional study among patients with Resistant Hypertension defined according to the ESC guideline for Management of Arterial Hypertension.
Method:The study was carried out among 128 patients admitted with history and 24 hour holter blood pressure monitor evidence for Resistant Hypertension in the Department of Cardiology between 1 st July 2012 and 31 st July 2014. Patients with history of Resistant Hypertension were screened with 24 hour holter blood pressure monitoring and those who fullfilled the criteria for Resistant Hypertension according to the ESC guideline for Management of Arterial Hypertension based on the treatment history and 24 hour holter blood pressure monitoring were included in the study after obtaining informed consent. Patients included in the study were started on therapy with Olmesartan/Amlodipine at fixed dose combination along with diuretic and Beta-Blocker. Patients were continued on this fixed dose combination therapy for 3 months. After the 3 month period patients were reassessed with control holter blood pressure monitoring to access the efficacy of the treatment and the circadian control of arterial blood pressure. Result:From the study it was observed that 90 patients (70.31%) had reached optimal control of arterial blood pressure by the fixed dose combination therapy with Olmesartan/Amlodipine. 20 patients ( 15.64%) had non optimal control of arterial blood pressure and 12 patients (9.37%) continued to be with resistant hypertension in-spite of the maximal dosage of the fixed dose combination therapy with Olmesartan/ Amlodipine. 6 patients (4.68%) discontinued the treatment due to pedal edema. We observed from the screening holter blood pressure monitoring that 38 patients (29.68%) with resistant hypertension were non-dippers and after the fixed dose combination therapy with Olmesartan/Amlodipine only 14 patients (10.93%) were non-dippers.
Conclusion:The study revealed that fixed dose combination therapy with Olmesartan/Amlodipine in patients with Resistant Hypertension has high efficacy and minimal side effects with good circadian control of arterial blood pressure.
P254
Gender differences in cardiovascular risk factors on attendants in a cardiac rehabilitation program.
A Roldan Sevilla1, R Dalmau Gonzalez-Gallarza2, T Roldan Sevilla3, A Castro Conde2, JL Lopez Sendon2
1University Hospital 12 de Octubre, Madrid, Spain
2University Hospital La Paz, Cardiology, Madrid, Spain
3Brigham and Women's Hospital, Anticoagulation Management Service, Boston, United States of America
Objectives:Traditionally, women have shown a different distribution in CVRF (Cardio-Vascular Risk Factors) in contrast to men, with higher prevalence of diabetes mellitus, hypertension, dyslipemia and obesity (mainly due to higher age), but lower tobacco consumption. It is useful to know the prevalence of CVRF over the population who participate in cardiac rehabilitation programs, in order to design more individualized programs.
Methods:We studied a cohort of 961 patients submitted to a cardiac rehabilitation program. Of which, 84% were male and 16% were female. We analyzed and compared the main CVRF between genders at the beginning of the program.
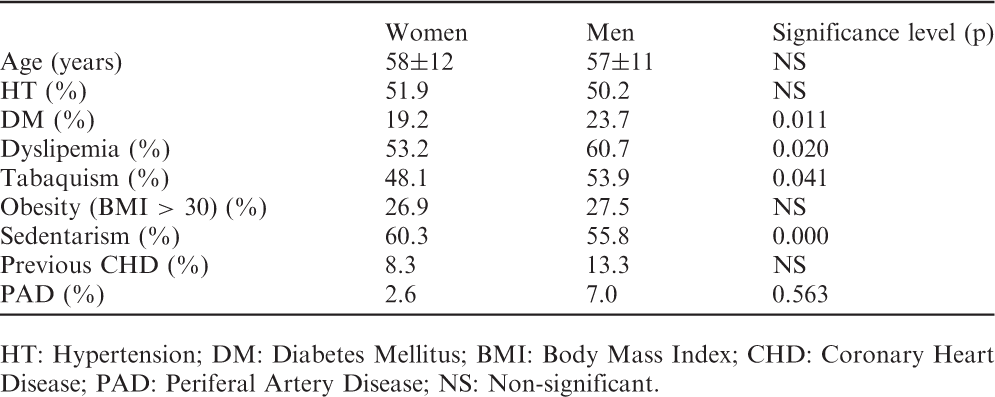
Results:Men and women presented differences in the distribution of the CVRF with higher prevalence in men of DM (diabetes mellitus) (23.7% vs. 19.2%; p=0.011), dyslipemia (60.7% vs. 53.2%; p=0.020), active tobacco smoking (53.9% vs. 48.1%; p=0.041) and a non-significant tendency to a higher proportion of previous cardiovascular disease condition. However, women have higher rate of sedentarism (55.8% vs. 60.3%; p0.000) with no differences in the presence of hypertension or obesity.
Conclusions:Despite both genders present similar CVRF profile, men present significant higher prevalence of DM and dyslipemia, and women are more sedentary people. These differences suggest that we must highlight the relevance of the physical exercise in women, and the diet control in men. In addition, we observed a tendency to a similar smoking habit in both genders, so we must promote the cessation of the tobacco use in both genders.
HT: Hypertension; DM: Diabetes Mellitus; BMI: Body Mass Index; CHD: Coronary Heart Disease; PAD: Periferal Artery Disease; NS: Non-significant.
Women
Men
Significance level (p)
Age (years)
58±12
57±11
NS
HT (%)
51.9
50.2
NS
DM (%)
19.2
23.7
0.011
Dyslipemia (%)
53.2
60.7
0.020
Tabaquism (%)
48.1
53.9
0.041
Obesity (BMI > 30) (%)
26.9
27.5
NS
Sedentarism (%)
60.3
55.8
0.000
Previous CHD (%)
8.3
13.3
NS
PAD (%)
2.6
7.0
0.563
P256
Functional capacity and inflammatory parameters in severe heart failure - does age matter?
G Portugal1, A Abreu1, M Oliveira1, M Mota Carmo1, L Branco1, S Silva1, A V Monteiro1, P Rio1, V Santos2, R Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
2Technical University of Lisbon, Human Motricity Faculty, Lisbon, Portugal
Background:Several mechanisms have been involved on the pathogenesis of heart failure. These include progressive left ventricular remodelling, neuro-hormonal imbalance, autonomic nervous system dysfunction, release of pro-inflammatory cytokines, endothelial dysfunction, and over-expression of vasoactive peptides such as brain natriuretic peptide. However, the role of advancing age on the interplay of these different mechanisms is unknown.
Aim:To understand the contribution of different mechanisms involved in heart failure and their differential effect in elderly versus younger patients.
Methods:Consecutive patients with advanced heart failure referred for CRT implantation between April 2011 and June 2014 were prospectively enrolled. Data was collected on baseline characteristics, and a comprehensive non-invasive assessment was performed, consisting of a transthoracic echocardiogram, 123-mIBG scintigraphy for assessment of autonomic system dysfunction, cardiopulmonary testing, reactive hyperemia, holter monitoring for heart rate variability and . The overall population was divided according to age (<65yrs or =65 yrs). Statistical analysis was performed utilising de Mann-Whitney or Chi-square test when appropriate.
Results:A total of 107 patients were included in the final analysis, mean age 67.4±11.8 yrs, 75 were male (70%) and 32 were female (30%). 33 patients (31%) were in NYHA class II, 72 (67%) NYHA class III and 2 (2%) NYHA class IV. After stratification for age, older patieents (>65 yrs) were more likely to have an ischemic etiology (33% vs 17%, p=0.050), have higher serum brain natriuretic peptide (657±626 vs 343±370, p=0.001) and more significant immune activation as assessed by serum TNF-alpha (2.8±1.6 vs 2.1±1.0, p=0.038). No differences were found regarding left ventricular systolic or diastolc dysfunction, cardiac autonomic denervation, endothelial dysfunction, oxygen consumption as assessed by CPT or heart rate variability.
Conclusions:In this population of patients with advanced heart failure, a higher prevalence of ischemic etiology, higher serum BNP and more significant immune activation was found on older patients. These results suggest that cardiac rehabilitation intervention may offer significant benefit in this population.
P257
Functional capacity in heart failure rats: characterization of the myocardial infarction model and effects of neuromuscular electrical stimulation and light emitting diode therapy
M Karsten1, L Capalonga1, VS Hentschke1, DD Rossato1, MP Dornelles1, P Dal Lago1
1Universidade Federal de Ci?ias da Sa?e Porto Alegre, Sciences of Rehabilitation, Porto Alegre, Brazil
Topic: Sports cardiology
Purpose:Heart failure (HF) compromises the functional capacity and leads to the appearance of fatigue, dyspnea, and exercise intolerance. Thus, the main goals of this study were: (i) characterize the model of HF in rats undergoing surgical induction of myocardial infarction (MI) through the functional capacity and maximal oxygen consumption (VO2max); and (ii) compare the effects of 8 weeks of intervention with light emitting diode therapy (LEDT), alone or combined with neuromuscular electrical stimulation (NMES) on hemodynamic function, functional capacity and aerobic power in rats with HF.
Methods:Study 1) were used male Wistar rats (230-280g) were divided into two groups: Sham (n=5) and HF (n=4); Study 2) Male Wistar rats were divided into 4 groups: Sham (n=6), Control-HF (n=4), LEDT-HF (n=6) and LEDT+NMES-?128;??128;?HF (n=7). The animals were subjected to an exercise test with gas analysis coupled in the metabolic box for rats (AVS Projects, S?Carlos, SP, Brazil), with incremental protocol performed at three time points (pre-MI, 6 and 14 weeks after MI mat). The MI was induced by ligation of the left coronary artery. In the statistical analysis using unpaired t test, one-way ANOVA or two-way ANOVA for repeated measures followed by post hoc (Student-Newman-Keuls), (p=0.05).
Results:There was no difference between groups in the pre-MI. Study 1) comparing the Sham rats with HF at 14 weeks, the Sham rats showed higher VO2max 57.8 ± 4.0 vs. 45.3 ± 14.4 ml/kg/min-1 (p=0.038), distance traveled 390.2 ± 58.9 vs. 275.1 ± 95.9 m (p=0.023) and the test duration 1058.4 ± 80.6 vs. 862 7 ± 180.8 s (p=0.035). In Study 2, comparing the 14th with the 6th week, the LEDT-HF and LEDT+NMES-?128;??128;?HF group was similar to Sham group behavior in variable speed, test duration and distance traveled, which were higher (p=0,05) than in the Control-HF group. In addition, the LEDT+NMES-HF group showed a decrease in VO2max 46.7 ± 10.7 vs. 55.3 ± 6.2 ml/kg/min-1 (p=0.045), and increased distance walked 256.5 ± 73.7 vs. 205.7 ± 75.9 m (p=0.047) and the duration of the test 819.1 ± 147.3 vs. 699.7 ± 176.6 s (p=0.018).
Conclusions:This model of HF in rats leads to changes in functional capacity and aerobic power; interventions promoted mitigating the deleterious effects of HF; and intervention LEDT+NMES was able to increase the functional capacity despite a decline in aerobic power in rats with HF.
P258
Characterization of submaximal exercise limitations in patients with chronic heart failure by using the ratio of cardiac output and oxygen uptake kinetics
R Spee1, VM Niemeijer1, J Jansen2, PFF Wijn3, PAFM Doevendans4, HMC Kemps1
1Maxima Medical Centre, Department of Cardiology, Veldhoven, Netherlands
2Eindhoven University of Technology, Department of Biomedical Engineering, Eindhoven, Netherlands
3Eindhoven University of Technology, Department of Applied Physics, Eindhoven, Netherlands
4University Medical Center Utrecht, Department of Cardiology, Utrecht, Netherlands
Topic: Sports cardiology
Purpose:Submaximal exercise capacity is impaired in CHF patients. Whether this is primarily due to central or peripheral limitations is still under debate. We investigated whether the rate of increase in cardiac output during submaximal exercise is related to the amount of de-oxygenation in exercising muscles.
Methods:Forthy three stable CHF patients performed a submaximal steady state exercise test with respiratory gas analysis on a cycle ergometer at 80% of the ventilatory treshold. Cardiac output was assessed by a radial artery pulse contour analysis method; skeletal muscle oxygenation was measured at the m. vastus lateralis by the tissue saturation index (TSI) using near infrared spectroscopy (NIRS).
Results:Mean ?uV?2 and ?uQ were respectively 60 s (+/-21s) and 62s (+/- 29s). ?uV?2 was significantly correlated with ?uQ (r=0.66, p<0.0001). Only in patients with a relatively slow increase in Q (?uQ/?uV?2 >1, n=22), there was a significant negative correlation between ?uQ and TSImin (r= -0.59, p<0.005), suggesting that submaximal exercise capacity in these patients is limited by the central hemodynamic response to exercise.
Conclusions:In CHF patients with a reduced Q response relative to metabolic demands, Q was inversely associated the amount of skeletal muscle de-oxygenation, suggesting a limiting role of central hemodynamics on submaximal exercise capacity in these patients. Whether these findings may be used for clinical purposes such as tailoring of interventional strategies remains to be determined.
Correlation between tauQ and TSImin
P259
Aerobic exercise training prevents diaphragm muscle weakness in an animal model of chronic heart failure
N Mangner1, TS Bowen1, S Werner1, T Fischer1, G Schuler1, A Linke1, V Adams1
1University of Leipzig, Heart Center, Leipzig, Germany
Background:Chronic heart failure (CHF) results in diaphragm muscle weakness, with increased oxidative stress and protein degradation directly implicated. Exercise training is known to exert both anti- oxidant and -catabolic effects. We therefore determined whether aerobic exercise training prevents diaphragm dysfunction following the onset of CHF.
Methods:Ligation of the left coronary artery to induce CHF (n=20; confirmed by echocardiography and histology) or sham operation (n=10) was performed on 8 wk old C57BL/6 mice. CHF mice were randomized to a group of treadmill exercise training (CHF-ET; 60 min at 15 m/min with 5 sessions per week) or sedentary (CHF-S). Ten weeks later, in vitro isometric force of diaphragm muscle fiber bundles was assessed, as was the activity in redox and proteasome enzymes.
Results:Compared to sham, specific force was depressed (p<0.05) between the frequencies of 80-300 Hz in CHF, with maximal tetanic force reduced by ~20% (26±1 vs. 20±1 N/cm2). This decrease in function in CHF was prevented by exercise training (p<0.05), with maximal force maintained (25±1 N/cm2). No differences were observed between groups in terms of the activity of redox enzymes (i.e., xanthine oxidase, NADPH oxidase, superoxide dismutase). However, proteasome activity was increased in CHF-S by 29% compared to sham and CHF-ET (p<0.05).
Conclusion:Diaphragm dysfunction induced by CHF was prevented by aerobic exercise training, and this was associated with reduced proteasome activation. These findings suggest exercise training may represent a beneficial therapeutic intervention in the treatment of respiratory muscle dysfunction in CHF, by specifically alleviating protein degradation.
P260
Effect of exercise training on the renin-angiotensin-aldosterone system in healthy individuals: a systematic review and meta-analysis
K Goessler1, MD Polito2, V Cornelissen3
1CAPES Foundation Education of Brazil, Bras?a, Brazil
2State University of Londrina, Londrina, Brazil
3KU Leuven, Leuven, Belgium
The aim of this systematic review and meta-analysis was to evaluate the effect of exercise training on parameters of the renin angiotensin aldosterone system (RAAS) in healthy adults and to investigate the relation with training induced changes in blood pressure. A systematic search was conducted and we included randomized controlled trials lasting =4 weeks investigating the effects of exercise on parameters of the RAAS in healthy adults (age =18 years) and published in a peer-reviewed journal up to December 2013. Fixed effects models were used and data are reported as weighted means and 95% confidence limits (CL). Eleven randomized controlled trials with a total of 375 individuals were included. Plasma renin activity was reduced after exercise training [n= 7 trials, standardized mean difference-0.25 (95%CL -0.5 to -0.001), p=0.049) whereas no effect was observed on serum aldosterone [(n= 3 trials; standardized mean difference-0.79 (-1.97 to +0.39)] or angiotensin II (n=3 trials; standardized mean difference -0.16 (-0.61 to +0.30)]. Significant reduction in systolic blood pressure -5.65 mmHg (-8.12 to -3.17) and diastolic blood pressure -3.64 mmHg (-5.4 to -1.91) following exercise training were observed. No relation was found between net changes in plasma renin activity (PRA) and net changes in blood pressure (P>0.05). To conclude, although we observed a significant reduction in plasma renin activity following exercise training this was not related to the observed BP reduction. Given the small number of studies and small sample sizes, larger well-controlled randomized studies are required to confirm our results and to investigate the potential role of the RAAS in the observed improvements in blood pressure following exercise training.
P261
Association of serum myokine with metabolic and endothelial function
YAEKO Fukushima1, YUTAKA Kimura1
1Hirakata City Hospital, Kansai medical health science center, Hirakata City, Japan
Background:and Purpose:Exercise provides clear beneficial effects to reduce weight and fat mass for obese patients. However the role of muscle to the metabolism and insulin resistance was not clear in obese people. We investigated association of serum myokine levels with detail body composition and exercise capacity in obese patients.
Methods and Results:We studied 55 obese patients (men: women/24:31, 46.5±13.1years,BW101.4±22.7kg,BMI 38.5±7.5,SMI7.9±1.2,) who visited our obesity clinic.BIA (Bio Impedance Analysis), DEXA (dual-energy x-ray absorptiometry), leg Extension power, and CPX (Cardio Pulmonary Exercise test) were performed. HOMA-IR as a maker of insulin resistance was evaluated from blood glucose and insulin level. RHI was a method to evaluate endothelial function, namely, reactive hyperemia peripheral arterial tonometry (RH-PAT), has been developed. RH-PAT is an index of endothelial function(RHI), indicating initial atherosclerotic lesions. Body compositions were evaluated based on the following parameters:height, body weight, BMI, SMI(Skeletal Muscle index) and ASM/Bw score and body composition. The simple correlation analysis between HOMA-IR, RHI and body compositions and serum myokine levels and any parameters was evaluated.Serum irisin levels were significantly and positively correlated with myostatin and follistatin(r=0.363, P<0.01)(r=0.508, P<0.01). Some significant relationships between serum other myokine levels and other parameters were noticed (P<0.01). Furthermore myostatin had positive correlation with any part of muscle mass volume and even SMI and ASM/Bw index. On the other hands, HOMA-IR and RHI had significant relationships with muscle mass volume. Especially in women, muscle mass volume of the trunk was positively correlated with irisin(r=0.392,P<0.05).
Conclusions:Retaining muscle mass volume with myokine especially irisin may play important role to insulin resistance and endothelial function.
P262
Physical activity and total serum antioxidant capacity in healthy men and in men with coronary heart disease
T Kostka1, A Gawron-Skarbek1, J Chrzczanowicz1, J Kostka2, D Nowak3, W Drygas4, A Jegier5
1Department of Geriatrics, Medical University of Lodz, Lodz, Poland
2Department of Physical Medicine, Medical University of Lodz, Lodz, Poland
3Medical University of Lodz, Department of Clinical Physiology, Lodz, Poland
4Medical University of Lodz, Department of Preventive Medicine, Lodz, Poland
5Medical University of Lodz, Department of Sports Medicine, Lodz, Poland
Topic: Sports cardiology
Purpose:The purpose of the study was to assess total antioxidant capacity (TAC) of blood serum in relation with habitual leisure time physical activity (LTPA) and aerobic capacity in a group of 90 men with coronary heart disease (CHD) aged 34.8-77.0 years and in 90 age-matched peers without CHD.
Methods:Two spectrophotometric methods were applied to assess TAC: Ferric Reducing Ability of Serum (TAC-FRAS) and 2.2-diphenyl-1-picryl-hydrazyl (TAC-DPPH) tests. During submaximal exercise test the aerobic capacity was evaluated and expressed as physical working capacity at 85% of the maximal heart rate (PWC85%HRmax). LTPA was estimated on the basis of energy expenditure earmarked for weekly recreational-sport activities (kcal·wk-1).
Results:CHD patients were characterized by higher values of overweight/obesity indices as body mass index (BMI), waist to hip ratio (WHR) and percentage of body fat in comparison with the men without CHD. CHD patients had higher values of TAC-FRAS (1.37±0.28 vs. 1.27±0.22 mmol FeCl2·L-1; p<0.05) but there were no group differences for TAC-DPPH (10.2±3.5 vs. 11.2±4.5 % reduction) and for uric acid (UA) concentrations. Healthy men were characterized with higher LTPA level and higher values of PWC85%HRmax, also when relative to body mass. Negative correlation was found between LTPA (also when calculated per kg of body mass) and TAC-DPPH in CHD patients. Moreover, in CHD patients, TAC-FRAS and UA were lower in subjects with higher aerobic capacity expressed as PWC85%HRmax/kg. Those associations were not found in healthy men (Table 1).
Conclusions:We conclude that TAC of blood serum is adversely related to LTPA and aerobic capacity in patients with CHD. UA, as the main determinant of serum TAC, may be responsible for those associations.
Table 1. Correlation coefficients of total antioxidant capacity measures and uric acid concentration to physical activity and fitness characteristics in men with and without CHD. * - p < 0.05, ?128; - p 㤠0.01
CHD patients
Healthy men
Variable
TAC-FRAS (mmol FeCl2?153;L-1)
TAC-DPPH (% reduction)
UA (mg · dL-1)
TAC-FRAS (mmol FeCl2·L-1)
TAC-DPPH (% reduction)
UA (mg · dL-1)
Energy expenditure for LTPA (kcal · week-1)
-0.12
-0.24*
-0.04
-0.04
-0.05
-0.16
Energy expenditure for LTPA (kcal · week-1· kg -1)
-0.14
-0.23*
-0.04
0.03
-0.02
-0.12
PWC85%HRmax(W)
-0.16
-0.0008
-0.14
-0.06
-0.04
-0.01
PWC85%HRmax/kg(W · kg -1)
-0.29*
-0.07
-0.26*
-0.08
0.03
-0.16
P263
Fast walking and resistance exercise program in cancer survivors
L Stefani1, GM Mascherini1, CP Petri1, LF Francini1, FB Buralli1, AC Cattozzo1, GG Galanti1
1University of Florence, Florence, Italy
Topic: Sports cardiology
Purpose:Physical Exercise is normally suggested in preventing metabolic risk factors especially in cancer patients. Despite aerobic exercise has been well studied, few data are available in case of combination with resistance exercise, particularly unsupervised. The study aims to assess the cardiovascular and metabolic impact of mixed exercises at moderate level, in cancer survivors .
Methods:15 survived breast cancer women aged 55.51 ± 10.94, were enrolled . BMI and circumferences of waist/hip were measured at the beginning and after 6 months of unsupervised exercise , as well as HR , BP, respiratory rate, Systolic and Diastolic Blood pressure and perceived exertion from CR10 scale, calculated at the 6MWT test. The unsupervised exercise program consisting on three sessions/ week for 6 months. The resistance exercises included a maximum of 20 strength repetitions, calculated from Hand Grip and Chair Test for strength for the upper and lower limbs. Aerobic training included 30 minutes of "fast walking" at 70% of own maximum HR calculated at 6MWT.
Results:Anthropometric parameters showed a trend toward an improvement: BMI (Kg/m2) T0: 28.90 ± 7.70 T6:28.84 ± 7.05. Waist (cm) T0:91.33 ± 16.97; T6 91.87 ± 17.10; Hip (cm) T0: 108.13 ± 16.37 ; T9 108.17 ± 15.04, body composition and hydration data showed on the contrary a significant improvement (Fm% T0:38.44 ±5.04 %, T6:37.65 ± 5.00 %, p<0.03; FFM % T0: 61.56 ± 5.04, T6: 62.35 ± 5.00 %, p< 0.03, TBW% T0: 49.26 ± 7.22 %, T6: 47.94 ± 5.97 % p<0.05). The respiratory rate is significantly reduced (T0: 31.15 ± 4.61 pm, T6: 29.42 ± 3.34 pm p<0.04).The functional parameters also showed a significant improvement of the number of repetitions at Chair Test (T0: 13.20 ± 4.84 rip, T6:15.31 ±3.54 rip, p< 0.01).
Conclusions:Combination aerobic and resistance exercise produces , in a short time, a significant improvement of those parameters associated to some cardiovascular risk factors involved on the overall quality of life. This effect is possible by using a program of "unsupervised " exercise.
P264
The influence "electrical storm" incidents on the quality of life and physical activity in patients after cardioverter defibrillator implantation.
E Smolis-Bak1, N Suska-Bak1, B Kazimierska1, I Kowalik1, A Maciag1
1National Institute of Cardiology, Warsaw, Poland
The aim of this study was to evaluate the level of physical activity, quality of life, anxiety, stress and depression in patients after implantation of cardioverter-defibrillator (ICD) who have experienced or not the incident electrical storm with multiple ICD interventions. There was 36 patients with ICD in aged from 39 to 83 years. Patients were divided into two groups: those who had a Storm (+) or no Storm (-) incident electrical storm. In the group Storm (+) significantly more often occurred loss of consciousness before ICD implantation and after discharge, than in the Storm (-). Also frequently found problems with life energy and vigor, which may limit the opportunities gainful employment and doing housework. Other parameters of quality of life were not different between groups. The level of stress and week-long physical activity was similar in both groups.
Conclusions:1. The incidence of electrical storm in ICD patients significantly increases the level of anxiety and influences the occurrence of mild depressive symptoms. 2. Electrical storm does not affect the increase in the level of stress and the week-long physical activity. 3. Electrical Storms limits the opportunities gainful employment and doing housework. 4. Frequent loss of consciousness in patients prior to ICD may indicate an increase in the frequency of electrical storms occurring after implantation of the device.
P266
Diabetes mellitus prevalence and risk profile at an urban population
R Rodrigues1, L Rassi1, S Goncalves1, AL Lourenco1, I Cuco1, Q Rato1, L Soares1
1Hospital Sao Bernardo, CHS, Setubal, Portugal
Introduction:The European guidelines of cardiovascular disease (CVD) prevention divides the diabetic individuals (ind) into two groups: high and very high risk, according the association or not to another cardiovascular risk factor (CVRF). The impact of this measure in the real world is questionable. Aim:To assess the prevalence of diabetes mellitus (DM) in a screening study of a current urban population and evaluate their cardiovascular risk profile and glycemic control. Methods:We performed a cross sectional study with 683 ind, evaluated in a screening carried out at an urban community during a month. The sample was divided into two groups according to the presence or absence of a previous diagnosis of DM. The groups were characterized and compared according to its risk profile, demographic and clinical aspects. Glycemic control was evaluated.
Results:Of the total population, 64% were female and the mean age was 57 ± 15 years. 74 ind (11%) had a previous diagnosis of DM. This ind were older, more often male and had a higher prevalence of hypertension (see table). All the diabetic ind of this sample had at least one additional CVRF. The average of the occasional capillary glycemia in ind with DM was 176±78 mg/dL. Conclusions:The prevalence of DM in this sample was similar to that described in international studies. All the ind with diagnostic of DM had other CVRF associated. In accordance with the recommendations of European Society of Cardiology for the prevention of CVD, all the diabetic ind were in very high risk for fatal cardiovascular events in 10 years. This finding leads one to question the practical utility of the differentiation of the type 2 diabetics on two risk levels.
Group with Diabetes mellitus (n=74)
Group without Diabetes mellitus (n=609)
p value
Mean age (years)
66 ± 7
60 ± 13
0.001
Male gender (%)
55
36
0.002
Hypertension (%)
78
46
<0.001
Body mass index (kg/m2)
30±5
27±5
ns
Dyslipidaemia (%)
62
55
ns
Smoking habits (%)
36
34
ns
P267
Newly diagnosed diabetes by screening is related to more extensive coronary artery disease in patients with acute coronary syndrome
SO Hafthorsson1, TA Bjarnason2, ES Oskarsdottir1, LB Kristinsdottir1, SH Lund3, B Kaernested2, FB Skuladottir2, I Olafsson2, TI Gudnason2, K Andersen2
1University of Iceland, Department of Health Sciences, Reykjavik, Iceland
2Landspitali University Hospital, Reykjavik, Iceland
3University of Iceland, Reykjavik, Iceland
Introduction:Patients with Acute Coronary Syndrome (ACS) often have undiagnosed glucose metabolism disorders which negatively affects their prognosis. The aim of this study was to evaluate whether derangement of glucose metabolism was related to the extent of Coronary Artery Disease (CAD).
Methods:ACS patients with no previous diagnosis of type 2 diabetes mellitus (DM2) were consecutively studied in a single center university hospital setting. Prediabetes and DM2 were diagnosed by fasting plasma glucose (FPG), HbA1c and standard oral glucose tolerance test performed 2-4 days after hospital admission and repeated 3 months after discharge. The extent of CAD was evaluated by Gensini score which grades severity and location of lesions as well as the cumulative effect of multiple lesions.
Results:Among 171 patients (77% male, average age = 63.3), 47% had normal glucose metabolism (NGM), 41% were diagnosed with prediabetes and 12% with DM2. The median Gensini score was 30.0 (16.0 – 48.8). The median Gensini score was 26.0, 28.5 and 37.0 for patients with NGM, prediabetes and DM2, respectively (p=0.07).
Discussion:ACS patients with no previously known metabolic derangement that are found to have DM2 by screening have more extensive CAD than patients with NGM. This underscores the importance of screening for metabolic derangements among patients hospitalized for ACS.
P268
Self reported diets for diabetes are inadequate in Switzerland
P Marques-Vidal1, P Vollenweider2, M Grange2, I Guessous3, G Waeber2
1University Hospital Center Vaudois (CHUV), Lausanne, Switzerland
2University Hospital Center Vaudois (CHUV), Department of Internal Medicine, Lausanne, Switzerland
3Geneva University Hospitals, Department of Community Medicine, Primary Care and Emergency Medicine, Geneva, Switzerland
Background:dietary measures effectively complement antidiabetic drug treatment, but little is known regarding the composition of antidiabetic diets in Switzerland.
Objective:To characterize the dietary intake of subjects aged 40 to 80 years according to diagnosis of diabetes and presence of a diet for diabetes.
Methods:cross-sectional study conducted between 2009 and 2012 on 4289 participants (2274 women) living in Lausanne, Switzerland, of which 299 (7%) reported a diagnosis of diabetes. 151 (51%) of them reported to follow a diabetic diet. Dietary intake was assessed using a validated food frequency questionnaire.
Results:compared to diabetic patients not on a diet, diabetic patients on a diet had a higher consumption of vegetables (mean±standard deviation: 1.8±1.3 vs. 1.4±1.0 portions/day), while no differences were found regarding all other food groups and nutrients (protein, carbohydrates, sugars, total fat, saturated, mono- and polyunsaturated fats, fibre) considered. Compared to participants not diagnosed with diabetes, patients with diabetes (with or without a diet) had a higher consumption of artificial sweeteners (0.3±0.7 vs. 0.4±0.8 and 0.8±1.0 times/day) and a lower consumption of honey/jam (0.5±0.5 vs. 0.4±0.4 and 0.4±0.4 times/day) or sugar (0.6±0.9 vs. 0.4±0.7 and 0.2±0.5 times/day) for participants not diagnosed with diabetes, diabetic patients not on a diet and diabetic patients on a diet, respectively. Diabetic patients on a diet also had a higher consumption of meat (5.6±3.6 vs. 4.8±2.9 portions/week) and a lower consumption of sugars (44.1±13.7 vs. 48.8±14.0 % total energy intake) than participants not diagnosed with diabetes.
Conclusion:in Switzerland, diabetic patients that report to follow a diet limit it to replacing sugar by artificial sweeteners and do not comply with current recommendations.
P269
Increased heart rate as important indication of unfavorable flow of acute coronary syndrome in type 2 diabetic patients
H Kyyak1
1Danylo Halytsky Lviv National Medical University, Family Medicine, Lviv, Ukraine
Type 2 diabetes mellitus (DM) is one of the most important independent risk factors of acute coronary syndrome (ACS). Its frequency reaches 35% among ACS patients. Scientific research indicates that increased heart rate is an undependent predictor of ACS complications. However, the impact of DM on the heart rate in patients with unstable angina is still not fully established. The aim of the investigation was to compare the results of 24 hour ECG monitoring in patients with unstable angina with and without DM.
Materials and methods:60 patients with unstable angina admitted to the cardiologic department were examined. Among them were 25 men and 35 women in the 60-75-year age group. Two main groups were created. The first one consisted of patients with unstable angina and type 2 DM (n=25), while the second one included patients with unstable angina without diabetes (n=35). The control group consisted of 40 patient at the age of 60.3±5.1 year without unstable angina and diabetes. 24 hour ECG monitoring was performed on the 5th - 7th day of hospitalization. All patients with unstable angina received acetylsalicylic acid, clopidogrel, nitrates, statins, angiotensin-converting enzyme inhibitors and beta-blockers. Ten patients (6%) underwent coronary angioplasty. Patients with acute heart failure (Killip II-IV) and with arrhythmias were excluded.
Results:The comparison of the heart rate of the patients suffering from unstable angina and DM with the patients from the control group and those with unstable angina without diabetes revealed significant differences. The average heart rate in the first group was 75.5 bpm, while patients without DM had average heart rate of 65.9 bpm, with 68.4 bpm in the control group . The minimal heart rate at night in patients with unstable angina and DM was 61.6 bmp, in patients without diabetes – 52.5 bmp and in control group – 54 bpm.
Conclusion:Patients with unstable angina and diabetes showed increased average heart rate and higher value of minimal heart rate at night in comparison with patients without diabetes. These changes characterize diabetic cardiomyopathy and neuropathy and cause worse prognosis of ACS. Results of heart rate examination give reasons for the prescription of higher doses of beta-blockers and/or If channels inhibitors and also more precise long-term control of heart rate in patients with unstable angina and diabetes.
P270
Vitamin D and glucose regulation in Icelandic patients with acute coronary syndrome
ES Oskarsdottir1, TA Bjarnason2, LB Kristinsdottir1, SO Hafthorsson1, SH Lund2, FB Skuladottir2, B Kjaernested2, I Olafsson2, G Thorgeirsson2, K Andersen2
1University of Iceland, Medical, Reykjavik, Iceland
2Landspitali University Hospital, Cardiology, Reykjavik, Iceland
Background/Objective:The role of vitamin D in the pathogenesis of diabetes has been debated but few studies have investigated this association in patients with Acute Coronary Syndrome (ACS). The objectives of this study was to explore a possible relationship between vitamin D levels (measured as s-25(OH)D) and blood glucose metabolism in ACS patients.
Methods:ACS patients (n=108, mean age=63.5±9.7 years, males=82%) with no previous diagnosis of diabetes or impaired glucose tolerance were consecutively included. Eight to 12 weeks after hospital discharge a standard oral glucose tolerance test (OGTT) was performed, as well as measurements of fasting plasma glucose (FPG), HbA1C and s-25(OH)D. Patients were then categorized into the groups normal glucose metabolism (NGM), impaired glucose tolerance (IGT) and type 2 diabetes (DM2), based on ADA guidelines.
Results:28% of the patients had normal blood glucose metabolism, 60% had impaired glucose tolerance and 12% were diagnosed with diabetes. The median (Inter Quartile Range (IQR)) s-25(OH)D value for patients with NGM, was 67.8 (47.0-87.8) nmol/L and 37% of these patients were vitamin D deficient (s-25(OH)D <50 nmol/L). The median (IQR) s-25(OH)D value for patients with IGT or DM2 was 51.9 (38.3-85.4) nmol/L and 46% of these patients were vitamin D deficient. The difference in s-25(OH)D levels and the proportion of vitamin D deficient patients between the two groups did not reach statistical significance. Negative correlation was found between s-25(OH)D and FPG levels (r=-0.21; p<0.05). There was also a trend towards a negative correlation between s-25(OH)D and HbA1C (r=-0.20; p=0.08). Logistic regression revealed that for every increase of 10 nmol/L, in vitamin D, the OR for IGT or DM2 decreased by 25% (OR=0.75; CI=0.60- 0.95; p<0.01).
Conclusions:There is a negative correlation between vitamin D and fasting plasma glucose. It is possible that low levels of s-25(OH)D might influence glucose metabolism and even be a risk factor in the pathogenesis of DM2. Interventional studies are needed to determine whether or not this association is causal.
P273
Prevalence of conventional cardiovascular risk factors in patients with acute coronary syndrome
G Abreu1, P Azevedo1, C Arantes1, J Martins1, C Braga1, C Quina1, C Vieira1, J Marques1
1Hospital de Braga, Cardiology, Braga, Portugal
Background:Primary prevention studies have shown that early detection and aggressive treatment of cardiovascular risk factors (CRF) prevent cardiovascular events. It is not well described the prevalence of CRF in patients, at the moment of admission due to acute coronary syndrome (ACS).
Aim:To determine the prevalence of CRF among patients admitted with ACS.
Methods:We analysed 4871 patients admitted consecutively in our coronary care unit with a diagnosis of ACS and included in a prospective registry, from January 2002 to October 2013. We studied the prevalence of conventional risk factors (diabetes, hypertension, smoking, dyslipidaemia) and compared findings according to gender and type of ACS: ST-elevation myocardial infarction (STEMI) vs. non-ST elevation myocardial infarction (NSTEMI).
Results:Men represented 75% (n=3658) of the total population, were younger than women (61.6±12,9 vs 70.9 ±11.8 years; p<0.001) and had more frequently body mass index = 25 kg/m2 (70.9% vs 62.3%; p<0.001). The most frequent CRF was hypertension (62.4%; n=3038), followed by dyslipidaemia (50.6%, n=2467), smoking (43.2%; n=2106) and diabetes (27.2%; n=1324). In women, the more common CRF were hypertension (75%) and dyslipidaemia (51.2%), whereas in men were smoking (54.4%) and dyslipidaemia (50.5%). We identify, at least, one CRF in 92,4% of all patients and two or three risk factors in 58.1%. Women had more frequently 2 CRF than men (40.1% vs 36.3%; p=0.011), although mean had, more often, 4 CRF (8.9% vs 4.1%; p<0.001). Previous history of cerebrovascular disease was more prevalent in women (8.6% vs 6.1%; p=0.002), but men had more often history of previous revascularization (9.8% vs 6.8%; p<0.001). On admission men presented more frequently STEMI (50.8% vs 43.5%; p<0,001) and less frequently renal dysfunction (17.2% vs 39.6%; p<0.001) and anaemia (18.8% vs 33.3%; p<0.001). Hypertension was the most prevalent CFR as in STEMI patients (56.6%) as in NSTEMI patients (67.9%), followed by smoking in STEMI patients (47.5%) and by dyslipidaemia in NSTEMI patients (55.7%).
Conclusion:We found at least one CRF in 92.8% of patients and two or three in more than half. Hypertension emerged as the major CRF in both forms of presentation of ACS.
P274
Can any coronary investigation be justified in a patient with a normal screening carotid examination?
M Matangi1, U Jurt1, D Brouillard1, D Armstrong1, A, Johri2
1Kingston Heart Clinic, Kingston, Canada
2Queen's University, Kingston, Canada
Background:Carotid screening to define cardiovascular risk is commonly undertaken. A CCA IMT of <1.00mm and the absence of carotid plaque is associated with a very low cardiovascular risk.
Methods:Patients with carotid ultrasound with the following criteria, males 40-70 years, females 50-70 years, no diabetes and no prior vascular events. The patients were divided into two groups, those with a CCA IMT <1.00mm and no plaque (low risk) and those with a CCA IMT =1.00mm with or without plaque (high risk). Patients or their surviving relatives were contacted by phone and any vascular events were confirmed by reviewing local hospital records, office records, or coroner's records. As patients often had multiple vascular events, only the first vascular event was used in this analysis. In the case of cardiovascular death, the death was taken as the only event for that patient. Maximal CCA IMT is measured in the far wall of the CCA offline using GE automatic edge detection software. Plaque score is calculated using the Rotterdam method, (0 to 6). Kaplan-Meier event free survival curves were constructed.
Results:The 5 year event free survival was 99.2% for the low risk group compared to 90% for the high risk group, P<0.0001, See Figure 1.
Conclusions:It is very difficult to justify any coronary investigation in a patient with a normal screening carotid as defined. Especially investigations involving any cardiovascular risk such as death, stroke, or MI (coronary angiography), or radiation exposure (coronary angiography, myocardial perfusion imaging, CT coronary angiography or CT calcium scoring). The event rate is so low over the next five years (0.16%/year) the risk/benefit ratio unacceptable. Wider use of carotid screening with atypical symptoms of CAD could lead to a reduction in unnecessary testing.
P275
Change of systolic blood pressure is independently associated with incident diabetes in a community-based cohort study in Korea
SW Lee1, HC Kim2, YM Yun3, DJ Kim4, KH Ha4, JM Lee2, I Suh2
1Yonsei University Graduate School, Department of Public Health, Seoul, Korea, Republic of
2Yonsei University College of Medicine, Department of Preventive Medicine, Seoul, Korea, Republic of
3Yonsei University College of Medicine, Cardiovascular and Metabolic Diseases Etiology Research Center, Seoul, Korea, Republic of
4Ajou University School of Medicine, Department of Endocrinology and Metabolism, Suwon, Korea, Republic of
A relationship between hypertension and diabetes has been reported, but the effects of blood pressure change on incident diabetes have not been fully investigated in the general population. We examined whether increasing blood pressure is associated with the risk of developing diabetes among community-dwelling Korean adults. Total 2280 participants (881 men and 1399 women), who were aged 27-87 years and free of diabetes and cardiovascular disease at baseline, were followed up for 1 to 7 years. Incident diabetes was defined as fasting glucose = 126 mg/dL or HbA1c = 6.5 % at follow-up examination, and/or physician's diagnosis of diabetes during the follow-up period. The effects of baseline level and change of systolic blood pressure (SBP) on the risk of incident diabetes were assessed by multivariate logistic regression analysis. During the follow-up period, newly-developed diabetes was observed among 4.9 % (43/838) of men and 3.5% (49/1399) of women. Baseline SBP was not significantly associated with incident diabetes after controlling for sex, age, body mass index, fasting glucose, smoking and alcohol consumption (odds ratio 0.91 per 10 mmHg, p = 0.19). However, SBP change during the follow-up period was significantly associated with incident diabetes (adjusted odds ratio 1.09 per 5mmHg, p = 0.04). Increased SBP, but not baseline SBP, was independently associated with the risk of diabetes in Korean adults.
P276
Cardiovascular risk factors among Portuguese immigration in Venezuela compared with Portuguese residents in Portugal
J A Marques Rodrigues1, C Aguiar2, C Fonseca3, MA Marques1, A Melone1, D Lopez1, A Cabrera1, J Delgado1, G D Empaire1
1Central University of Venezuela, Caracas, Venezuela
2Hospital Santa Cruz, carnaxide, Portugal
3Hospital CUF Belem, Lisbon, Portugal
Background:Cardiovascular disease is the leading cause of death in both Venezuela and Portugal. Previous studies have demonstrated how risk factors are modified in immigrants when compared to the ones they had in their home countries.
Objective:compare the prevalence of major cardiovascular risk factors (CRF) in the Portuguese immigrant population in Venezuela with those of the portuguese residents living in Portugal.
Methods:the results of Cluve (Portuguese-Venezuelan city) study that was performed in a representative sample of Portuguese immigrants in Venezuela, over 18 years, were compared to VIVA study results (CRF in Portugal). Both studies were conducted using the same evaluation questionnaire so the results are comparable. Data was tested for statistical significance by using descriptive statistics and comparison of proportions.
Results:major results are shown on table 1 Conclusions:Portuguese immigrants in Venezuela have a significant increase in percentage of obesity, high blood pressure and Cholesterol compared to general Portuguese population. Physical inactivity and smoking is significantly increase in original Portuguese population.
VIVA
CLUVE
P value
Mean age
46,9 +/-18.4
45.7 +/- 15.4
NS
Total population (%males)
10.008 (48%)
504 (48%)
% males NS
% university education
21%
49%
<0.0001
Physical inactivity
69%
49%
<0.0001
Smokers
31%
11%
<0.0001
Abdominal diameter > normal
46%
50%
NS
Overweight
40%
39%
NS
Obesity
10,2%
25%
<0.0001
High blood pressure
29,5%
41%
<0.0001
High Cholesterol level
40,4%
53%
<0.0001
P277
Cardiovascular risk factors among Portuguese immigration in Venezuela. CLUVE (ciudad luso Venezolana)
J A Marques Rodrigues1, MA Marques1, A Melone1, D Lopez1, A Cabrera1, G D Empaire1, J Delgado1, C Aguiar2, C Fonseca3
1Central University of Venezuela, Caracas, Venezuela
2Hospital Santa Cruz, carnaxide, Portugal
3Hospital CUF Belem, Lisbon, Portugal
Background:Cardiovascular diseases are the major cause of death in Venezuela and in Portugal. Portuguese immigration is one of the oldest and biggest migratory groups in Venezuela. Our study evaluates the cardiovascular risk factors (CRF) on Portuguese immigrants in Venezuela.
Objectivec:Assess the prevalence of the main cardiovascular risk factors in Portuguese immigrants to Venezuela Methods:Cross-sectional, epidemiological study, of a representative sample of Portuguese immigrants living in Venezuela, aged 18 years old or more.
Results:502 individuals, 48% male, mean age 45.7 ± 15.4 years, were evaluated. 4% of the population reported being diabetic and 11% current smokers. 39% were overweight, 25% obese. 49% of men had abdominal diameter greater than 102 cm. 52% of women had abdominal diameter greater than 88 cm. 41% had high blood pressure (HBP)(BP = 140/90), 55% cholesterol >190 mg%, 12% LDL >159 mg%, 28%, 30% low HDL . 55% does not performed regular physicial activity. 39% of the population has two or more modifiable risk factors. The diagnosis of the risk factors occurs later than 50 years old in more than 50% of the population. 50% of the patients with HBP and 40% of the patients with high cholesterol level did not know the diagnosis. 1 out of 2 patients with HBP who believes is controlled is not. 3 out of 5 patients with high cholesterol that believes they are controlled are not. Even a high education level, second generation did not show major differences regarding CRF knowledge or prevalence Conclusions:Portuguese immigrant community in Venezuela has a high CV risk profile with a late diagnosis of the CRF. There is a high level of acknowledge regarding the disease. A high percentage of the population does not reach treatment goals.
P278
Men born in 1913 followed to age 100 years
L Wilhelmsen1, M Dellborg1, L Welin2, K Svardsudd3
1Internal Medicine, Medicine, Gothenburg, Sweden
2Medicine, Medicine, Lidkoping Hospital , Lidkoping, Sweden
3Uppsala Clinical Research Center, Uppsala, Sweden
Objectives:To follow men from age 50 to 100 years.
Topic: Sports cardiology
Purpose:A representative 1/3 of all men born in 1913, Gothenburg, Sweden, was first examined in 1963 at age 50 and was re-examined at ages 54, 60, 67, 75, 80 and 100 years. Of 973 selected men, 855 (88%) were examined at age 50 and 10 (1%) were alive at age 100 years.
Results:Fifty% lived until 80 years and 13% to age 90. Cardiovascular disease was the most common cause of death. Dementia was recorded in 23% at age 100. Long survival was related to high age at death of the mother, non-smoking, high social class at age 50, and high maximum working capacity at a bicycle test at age 54 years. At age 100, the men had low/normal blood pressure. Serum troponin T, N-terminal PRO brain natriuretic peptide and C-reactive protein were elevated and indicated myocardial infarction and heart failure, but echocardiographic findings were normal.
Conclusions:Ten men (1% of the original sample) experienced their 100th birthday. Survival was related to non-smoking, mother's high age at death, high social class at age 50 and high working capacity at age 54. Reference levels for laboratory tests have to be adjusted for age.
P279
Adult stature components and systolic blood pressure in a Middle income country. Evidence from ELSA-Brasil.
P Lotufo1, SR Rodriguez-Lopes2, IM Bensenor1
1Hospital Universitario - University of Sao Paulo, Sao Paulo, Brazil
2Autonomous University of Madrid, Madrid, Spain
Topic: Sports cardiology
Purpose:Better childhood conditions -mainly inferred from height and leg length- are usually associated to lower levels of blood pressure during adulthood in high-income countries. However, evidence is mixed about the nature of these associations in low- and middle-income countries. Components of adult height as the total height, trunk and leg lengths, and leg-to-trunk ratio are important surrogate variables of early life conditions of growth and development of one individual. We assessed the hypothesis that early life conditions affect systolic blood pressure (SBP) during adulthood differently according to gender in the middle-income country like Brazil.
Methods:From 15105 participants aged 35-74 years enrolled in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil), we analyzed 13571 with information about components of height and systolic and diastolic blood pressures. Potential confounders were age, race, maternal education, participant education, waist circumference, weight change since age 20, smoking habit, alcohol consumption, physical activity, and use of anti-hypertensive medication. Multiple linear regression was applied for inference of associations among these variables. The results are from the full model of adjustment.
Results:Younger individuals were taller and had longer trunks and legs. White individuals have longer trunks and shorter legs compared to black participants. People whose mothers with lower education have shorter trunks and legs compared to those with a higher educational maternal background. For each 1-standard-deviation (1-SD) of total height, there was a decrease of SBP (mm Hg) of -0.803 (-1.226 to -0.380) for men, and -0.983 (-1.335 to -0.631) for women. For leg length (1-SD) there was an inverse correlation of SBP (mm Hg) among men by -0.444 (-0.880 to -0.009) and -0.915 (-1.284 to -0.546) among women. Trunk length (1-SD) was inversely associated to SBP (mm Hg) among men by -0.444 (-0.880 to -0.009) but not among women by -0.191 (-0.597 to 0.214). Leg-to-trunk ratio was inversely associated to systolic blood pressure among women, -0.669 (-1.014 to -0.324) but not among men, -0.182 (-0.583; 0.218). A "post-hoc" analysis revealed that the inverse association of height- SBP was more pronounced for participants who are White, with a college degree and who had a mother with high educational background.
Conclusion:The protective effect of the components of height on adult blood pressure reported in high-income countries is also present in a middle-income country like Brazil with few variations according to gender.
P280
Cognitive function, high blood pressure, grip strength, bad health and their association to CVD and all cause mortality among Muscovite population 55 years and older
S Shalnova1, Y Balanova1, A Deev1, A Kapustina1, V Konstantinov1, S Kukushkin1, M Shkolnikova2
1National Research Center for Preventive Medicine, Moscow, Russian Federation
2Research Clinical Institute of pediatrics, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:to determine whether cognitive function is associated to BP values, hand grip strength values, self-health assessment and their contribution into CVD and all cause mortality among Russian men and women 55 years and older.
Methods:The representative sample of 1,830 subjects was examined at the baseline survey of the Stress, Aging and Health study in Russia (SAHR). The SAHR is a prospective population-based cohort study that conducted in Moscow. Cognitive dysfunction is assessed by the Mini-Mental State Examination (MMSE) - a brief examination consisting of eleven questions intended to evaluate an adult patient's level of cognitive functioning. A maximum score is 30 points. MMSE < 24 points was defined as a decreased cognitive function (LMMSE). The hand grip strength test (HGST) was used as an easy, reliable, valid method of screening to identify older adults at risk of disability. Socio-demographic characteristics, blood pressure (BP), self heath assessment (SHA) questionnaire were included in the study protocol as well. High blood pressure (HBP=160/95mm Hg) and bad SHA were selected as variables of interest. Descriptive analysis for continuous variables and relative frequencies for categorical variables were done. Cox regression model was applied for link variable states to mortality risks: hazard ratios (HR) with 95%CI.
Results:LMMSE significantly increased with age from 7.7% to 41.6% in both sexes (p<0.01), as well as bad SHA from 13.3 to 26.8% (p<0.03). The HGST slightly decreased, mostly in men and HBP did not change significantly with age. The positive relations of LMMSE to HBP level (p<0.04) and bad SHA (p<0.0001) were found. The strong inverse associations between low MMSE and HGST were described earlier (p<0.0001). The multivariate Cox model for all cause mortality demonstrated strong relation with HBP (HR: 95%CI - 1.388: 1.101; 1.751, p<0.006), bad SHA (1.672: 1.308; 2.136, p<0.0001), and low and moderate HGST (1.457: 1.064; 1.995, p<0.0001) – sex-, age-adjusted. In CVD mortality categories of HGST were replaced by LMMSE (2.581: 1.586; 4,202). Impact of HBP and bed SHA was similar to all cause mortality.
Conclusion:relation between low cognitive performances, bad SHA, HBP and HGST were found among elderly Russians of both sexes. LMMSE contribution into CVD mortality is more important then HGST status. The SAHR Study is funded by grant No R 01AG026786 (NIA, USA)
P281
Financial status influences the management of co-morbidities and determines 10-year (2004-2104) cardiovascular disease incidence among Acute Coronary Syndrome patients.
V Notara1, D B Panagiotakos1, C Pitsavos2, Y Kogias3, P Stravopodis4, G Papanagnou5, S Zombolos6, Y Mantas7, C Stefanadis2
1Harokopio University, Athens, Greece
2Hippokration Hospital, University of Athens, Athens, Greece
3Cardiology Clinic, General Hospital of Karditsa, Karditsa, Greece
4Cardiology Clinic, General Hospital of Zakynthos Island, Zakynthos, Greece
5Cardiology Clinic, General Hospital of Lamia, Lamia, Greece
6Cardiology Clinic, General Hospital of Kalamata, Kalamata, Greece
7Cardiology Clinic, General Hospital of Chalkida, Chalkida, Greece
Topic: Sports cardiology
Purpose:To evaluate the association between financial status and 10-year risk for Acute Coronary Syndrome (ACS) and all-cause mortality regarding patients' adherence to medical treatment.
Methods:From October 2003 to September 2004, a sample of six Greek hospitals was selected and almost all consecutive 2172 ACS patients were enrolled. In 2013-14, the 10-year follow-up was performed in 1,918 participants (11% of the participants were lost to follow-up). Financial status was classified as low (<9.000?) moderate (<18.000?), good (<28.000?) and very good (>48.000?).
Results:Patients with "very good" financial status were more educated and physically active, reported fewer years of smoking and were less likely to have a history of diabetes, compared to those with the "low/moderate" financial status (p<0.001). There were no significant differences among the financial groups regarding the compliance to prescribed medication for the management of hypertension, diabetes and hypercholesterolemia (p=0.28, p=0.62 and p=0.48, respectively). The low–to–very good financial status all cause mortality rate was almost 1.7-to-1 (p<0.001); however, in the 10-yr incidence of CVD no statistically significant differences were observed (p=0.22). Multi-adjusted analysis revealed that good/very good financial status remained highly protective on the 10-year disease prognosis Conclusions:Low financial status seems to play a critical role in the long-term ACS prognosis. Health policies to tackle non-compliance to medication are needed to minimize the disease burden.
P282
Short-term effects of air pollution on acute myocardial infarction in Korea
KH Ha1, C Kim2, HC Kim2, DJ Kim3
1Ajou University School of Medicine, Cardiovascular and Metabolic Disease Etiology Research Center, Suwon, Korea, Republic of
2Yonsei University College of Medicine, Preventive Medicine, Seoul, Korea, Republic of
3Ajou University School of Medicine, Endocrinology and Metabolism, Suwon, Korea, Republic of
Introduction:Short-term fluctuations in and long-term levels of air pollutants have been found to be associated with increased cardiovascular, and/or higher hospitalization rates. Recent systematic literature review found associations with myocardial infarction (MI) to be significant except ozone. This study aims to evaluate the relations between air pollutants and emergency visits for acute MI in seven metropolitan cities of Korea, using a general additive approach.
Methods:Data on emergency departments (ED) visits case of acute MI in seven metropolitan cities (Seoul, Busan, Incheon, Daegu, Daejeon, Gwanguju and Ulsan, Republic of Korea) were obtained from the Health Insurance Review and Assessment Service (HIRA) from January 1, 2005, to December 31, 2008. Carbon monoxide, nitrogen dioxide, ozone, particulate matter =10 µm in aerodynamic diameter, and sulfur dioxide were considered, and increase of interquartile range were analyzed. General additive approach was applied, and area-specific conditional regression models were fitted, adjusting for national holidays and meteorological factors. Finally, pooled estimates were derived from random-effects meta-analyses.
Results:In random-effects estimates, carbon monoxide showed significantly association in lag1 (1.02; 95% CI, 1.01-1.03) lag0-1 (1.03; 95% CI, 1.01-1.06), lag0-2 (1.03; 95% CI, 1.01-1.06), and lag0-3 (1.03; 95% CI, 1.00-1.06). Nitrogen dioxide showed significantly association except lag3. Particulate matter =10 µm in aerodynamic diameter was significantly associated ED visits for acute MI in lag0-1 (1.02; 95% CI, 1.00-1.03) and lag0-2 (1.02; 95% CI, 1.01-1.03). Sulfur dioxide showed significantly association only lag1 model (1.01; 95% CI, 1.01-1.02). However, Ozone was not significantly associated in any lag model.
Conclusion:This study adds to evidence for a short-term association between air pollutants and acute MI.
P283
Depressive symptoms, blood pressure and hypertension. The Polish Norwegian Study (PONS)
G Vaidean1, M Manczuk2
1Mount Sinai School of Medicine, Institute of Translational Epidemiology, New York, United States of America
2The Maria Sklodowska-Curie Institute of Oncology, Warsaw, Poland
Background: The relationship between depressive symptoms, blood pressure (BP) and hypertension (HTN) is conflicting and confounded by prevalent cardiovascular disease burden and use of antidepressants.
Design and Methods:We used cross-sectional data of 10076 adults, ages 45 to 64 years free of cardiovascular diseases, cancer and psychotropic medication, participating in an ongoing cohort study in Poland. Depressive symptoms during the last 12 months were assessed by a 7-item mental health questionnaire. Hypertension was defined as previous diagnosis of HTN or current antihypertensive medication use. Healthcare services utilization was defined as hospitalization within the last 5 years and visits to the doctor within the last year.
Results:The prevalence of HTN was 30.25% among those without depression symptoms and 36.13% and 41.18 % among those with 7 or 6 depressive symptoms (p <.0001) respectively. The odds ratio (OR) for a depression score of 3 or higher was 1.20 (95% CI 1.09 - 1.32), after adjusting for age, BMI, LDL and HDL cholesterol. Both somatic and cognitive subscales were associated with the HTN status. Among those with HTN, BP control was achieved by 33.66% of those with nil and by 53.54% of those with 7 depressive symptoms (p < 0.05 ). Comparing highest vs. lowest depression scores, OR was 1.96 (95% CI 1.29-2.98) after adjusting for age, sex and healthcare services utilization. Among those not taking HTN drugs, we found a negative association between the severity of the depression and SBP, beta estimate (SE) was -0.63 (0.11) after adjusting for age, sex, smoking and BMI. We detected a modest positive association between ACE inhibitors use and the depression score (OR 1.25 , 95%CI 1.12- 1.41), after adjusting for age, sex, SBP, DBP. Among hypertensives, those with depressive symptoms had unfavorable profiles for smoking, sedentary lifestyle and total cholesterol: HDL ratio, compared to those without depressive symptoms.
Conclusion:Compared to those without depressive symptoms, individuals with higher depressive symptoms have higher prevalence of HTN, better BP control, lower SBP. HTN patients with depressive symptoms have several modifiable cardiovascular risk factors, in spite of higher healthcare services utilization.
P284
Acute coronary events in men and women aged 25-74 years in the MONICA registers in Flanders: age-standardized time trends (1983-2009) and main observations in 2009.
K Van Herck1, W Alvarado Hernandez1, S Gevaert2, N Popelier1, L Vandendaele1, P Vannoote1, G De Backer1, D De Bacquer1
1Ghent University, Department of Public Health, Ghent, Belgium
2Ghent University Hospital (UZ), Department of Cardiology, Ghent, Belgium
Topic: Sports cardiology
Purpose:to study gender-specific and age-standardized long-term trends in the attack rates of acute myocardial infarction (AMI) based on two MONICA registers (1983-2009 and 1999-2009).
Methods:Retrospective screening of regional and municipality mortality registers and hospital records. Records suggestive of an AMI in age- and residence-eligible people (25-69 before, and 25-74 since 1998) were classified using the MONICA methodology and case definition. GPs were invited to notify additional non-fatal, non-hospitalised events. Record forms consisted of personal characteristics (gender, date of birth and date of onset of the AMI), and medical and diagnostic data (hospital case or managed elsewhere; first or recurrent event; patient survival at 28 days; symptoms, ECG, serum enzymes and necropsy findings). Attack rates were standardised using the European reference population.
Results:Attack rates decreased in the 1980ies, and more rapidly in the 1990ies, in men and women. After 2000, the time trend in attack rates levelled off. Throughout the observations, the trend in men was more favourable than in women. Nevertheless, men (20/10,000) maintained 3-fold higher attack rates than women (7/10,000) in 2009. Attack rates for fatal cases show a consistent, slowly decreasing trend through 2009. In 2009, 10-15% and 5-7% of death certificates in men and women aged 25-74 years, respectively, mention a possible acute cardiac cause of death. Fatal cases mainly occur in the 70-74 years old (1/3, compared to 1/4-1/5 of non-fatal cases), and in the pre-hospital setting (2/3).
Conclusions:A clearly favourable trend in the attack rates of AMI since the 1980ies; that after 2000 only continued in fatal cases. However, the majority of fatal cases still fail to reach the hospital setting.
P285
Educational inequalities in the prognosis of atrial fibrillation among patients with cardiovascular disease in Norway in 2008-2012
R Akerkar1, G M Egeland1, G Sulo2, E Reikeraas1, G S Tell2, M Ebbing1
1Norwegian Institute of Public Health, Bergen, Norway
2University of Bergen, Bergen, Norway
Topic: Sports cardiology
Purpose:Cardiovascular disorders are associated with socioeconomic disparities. Atrial fibrillation (AF) is the most prevalent arrhythmia. It is associated with high mortality rates and constitutes an independent risk factor for thrombo-embolic events and heart failure. Our aim was to investigate the association between educational inequalities in the prognosis (mortality) of AF using 5-year period data of the patients with cardiovascular disease (CVD) in Norway from 2008 to 2012.
Methods:Patients hospitalized for the ?128;?index' AF event (defined as the first mentioned hospitalization for AF as primary diagnosis during the study period) were included in the study. They were followed until death or 31st December 2012 (end of follow up); whichever came first. The supplement data from the Cause of death Registry and level of education was provided by Statistics. The level of education variable was stratified into 3 classes; low (up to 10 years of compulsory education), medium (high school or vocational school) and high (college/university). The potential effect of education on AF prognosis (mortality) was assessed using Cox proportional hazards models. Three models were constructed. The first model was adjusted for age; the second model was further adjusted for gender and the third model was further adjusted for major comorbidities, including diabetes mellitus, chronic obstructive pulmonary disease, chronic renal failure and neoplasm. The hazard ratios (HR) for the medium and high education were compared to low education (the reference category).
Results:A total of 42432 patients (60 % were men) with mean (sd) age of 70 (13) years were included in the study. On average, patients with low education were older than those with medium and high education [77 (13) versus 70 (13) versus 66 (14) years]. By the end of 2012, 16% of these patients died. Mortality was lower for AF patients with medium and high education as compared to patients with low education: differences which persisted after adjustment for age, gender and major comorbidities: the HR (95% confidence interval) for medium education was 0.80(0.77, 0.85); and for high education the HR was 0.61(0.56, 0.66). The major causes of death among these patients were cardiovascular diseases (46%), malignant neoplasm (21%) and chronic lower respiratory diseases (10%).
Conclusion:Educational disparities in mortality among AF patients exist in Norway highlighting the need for further evaluation of the underlying causes for the educational gradient and the need for prevention and intervention programs.
P286
Peak oxygen uptake during the Incremental Shuttle Walk Test in Chagas heart disease
MM Lima1, R Alves2, H Costa2, PH Figueiredo1, C Fonseca1, KM Diniz1, MC Nunes2, AL Ribeiro2
1Federal University of Jequitinhonha and Mucury Valleys, Diamantina, Brazil
2Federal University of Minas Gerais, School of Medicine, Postgraduate Course of Tropical Medicine, Belo Horizonte, Brazil
Background:Chagas heart disease (CHD) patients may have a reduced functional capacity (FC). Field tests, as the Incremental Shuttle Walk Test (ISWT), can estimate peak oxygen uptake (VO2 peak). However, the relationship between the ISWT and the Cardiopulmonary Exercise Testing (TECP), the gold standard in the assessment of FC, is not well established in CHD patients. This study aimed to evaluate the FC of CHD patients by ISWT with direct measurement of VO2 peak and to compare these findings with data obtained from CPET. A secondary goal was to derive a regression equation to calculate the VO2 peak by ISWT.
Methods:Thirty-two CHD patients (81.3% women, 58.8±9.0 years) were evaluated by CPET and ISWT with direct measurement of VO2 peak.
Results:The distance walked in ISWT showed a positive correlation with VO2 peak from CPET and ISWT (r=0.456, p=0.009 and r=0.869, p<0.001, respectively). In the agreement analysis, the values of the differences between VO2 peak from CPET and ISWT showed absence of bias (mean bias ± 95% CI and mean -1.29 ± 5.09mL.kg.min). Based in real values of VO2 obtained from ISWT, one equation including sex, functional class and distance walked was provided to predict the VO2 values in this test by the formula 12.21+ ?(distance) x distance walked + ?(sex; female=1; male=0) + ? (Functional Class by NYHA) + ? (distance vs. sex).
Conclusion:This study showed the good correlation between distance walked in ISWT and VO2 peak directly measured in both tests, and additionally, provided an equation to calculate a predictive VO2 peak by ISWT, suggesting a good alternative to evaluate the FC of CHD patients, especially in locations where sophisticated testing is not available. Financial support: FAPEMIG; CAPES; CNPq.
P287
Determinants of serum brain-derived neurotrophic factor levels in Chagas heart disease patients
H Costa1, MM Lima2, AL Teixeira1, P Martinelli3, E Camargos3, G Sousa1, AC Souza1, MC Nunes1, AL Ribeiro1, MO Rocha1
1Federal University of Minas Gerais, School of Medicine, Postgraduate Course of Tropical Medicine, Belo Horizonte, Brazil
2Federal University of Jequitinhonha and Mucury Valleys, Diamantina, Brazil
3Federal University of Minas Gerais, Department of Morphology, Institute of Biological Sciences, Belo Horizonte, Brazil
Background:Autonomic dysfunction and progressive inflammatory process are common pathological findings in various degrees in Chagas heart disease (CHD), the most important clinical manifestation of Chagas disease. The brain-derived neurotrophic factor (BDNF) is a neurotrophin that plays an important role in the autonomic nervous system, inflammatory and metabolic events, being susceptible to regulation by physical activity. However, the determinants of serum BDNF levels in CHD patients remain unknown.
Objective:To determine the associated factors and predictors of serum BDNF levels in CHD patients.
Methods:Seventy-five CHD patients (48.36±8.01 years, 45 male) were selected for this study. All patients underwent clinical evaluation, echocardiography, the Cardiopulmonary Exercise Testing (CPET) and blood sampling for measurement of serum BDNF. The CPET was performed on a treadmill ramp protocol for assessment of peak oxygen uptake (VO2peak) and serum BDNF levels were determined by ELISA. Pearson or Spearman correlation tests were performed for data analysis. Backward multivariate linear regression analysis was performed to determine characteristics that were independently associated with BDNF levels.
Results:Serum BDNF levels correlated with age (r= -0.230; p=0.039), VO2peak (r= -0.426; p<0.001) and left ventricular ejection fraction (LVEF) (r=0.383; p=0.001) but not with gender (r=0.079; p=0.499) and body mass index (r=0.215; p=0.066). The multivariate analysis of these variables identified that only the VO2peak and LVEF are strong and independent predictors of BDNF levels (r=0.760; r2=0.578).
Conclusion:The BDNF is strongly determined by the maximal functional capacity and systolic function in CHD patients. Financial support: FAPEMIG; CAPES; CNPq.
P288
The prevention and management of the complication in the hypertensive population
M L De Rosa1, L Cerini2, M Cerini3
1University Hospital Federico II, Naples, Italy
2Economics and Menagment of Innovation andTechonology,Bocconi University, Milan, Italy
3Nuclear Dept, Politecnico of Milan , Milan, Italy
Guidelines based on blood pressure level for initiation of treatment of hypertension may be too costly compared with an approach based on absolute cardiovascular disease (CVD) risk, especially in developing countries.
Methods:and Results?128; Using a Markov CVD model, we compared 6 strategies for initiation of drug treatment?128; 2 different blood pressure levels (165/95 and 145/90 mm Hg) and 4 different levels of absolute CVD risk over 15 years (45%, 35%, 25%, and 15%)?128; with one of no treatment. We modeled a hypothetical cohort of all adults without CVD in Italy, now a multiethnic developing country over 15 years. The incremental cost-effectiveness ratios for treating those with 15-year absolute risk for CVD >45%, 35%, 25%, and 15% were Euro 550, 1100, 3000, and 6 100 ,respectively per quality-adjusted life-year gained, respectively. Strategies based on a target blood pressure level were both more expensive and less effective than treatment decisions based on the strategy that used absolute CVD risk of >15%. Sensitivity analysis of cost of treatments, prevalence estimates of risk factors, and benefits expected from treatment did not change the ranking of the strategies. National inpatient hospital costs for hypertensive patient with complications were nearly Euro 2.9 billion in 2013. The risk of hospitalization from cardiovascular disease is two to four times higher for women with diabetes and hypertension compared to women without diabetes.
Conclusions:Hypertension-associated morbidity and mortality is a major heath concern, however with appropriate treatment, hypertension can be managed and the associated sequelae, reduced. The key to controlling this disease depends on proper and timely, prevention, detection, evaluation and treatment. In Italy , current guidelines based on blood pressure levels are both more expensive and less effective than guidelines based on absolute risk of cardiovascular disease. The use of quantitative risk-based guidelines for treatment of hypertension could free up major resources for other pressing needs, especially in developing countries.
P289
Cost-effectiveness of dabigatran for stroke prevention in non-valvular atrial fibrillation in Turkey
UO Turk1, K Yuksel1, E Alioglu2
1Ege University, Medicine Development and Pharmacokinetic Research and Applicaton Center (ARGEFAR), Izmir, Turkey
2Central Hospital, Izmir, Turkey
Objective:Economic evaluation of dabigatran is done mostly in Western countries. It remains to be seen whether dabigatran will be cost effective in practice environment where warfarin is underused (1) and the costs of both warfarin and INR monitoring are cheap. This study evaluated the cost-effectiveness of dabigatran for stroke prevention in atrial fibrillation (SPAF) as a first time in Turkey.
Methods:A Markov model simulating the course of treatment and occurrence of clinical events in three treatment arms (warfarin, dabigatran 110 mg bid, dabigatran 150 mg bid) over the lifetime of patients was adapted to the Turkish context. Modelled outcomes also included quality-adjusted life years (QALYs), total costs and incremental cost-effectiveness ratios (ICERs).The cost of inpatient care was estimated on data of all inpatient hospital stays in 2014. The calculation of outpatient care costs was based on WATER Registry (2), expert interviews.
Results:Compared with warfarin, low and high dose dabigatran were associated with positive incremental net benefits of 0.059 and 0.1 QALYs respectively. In the economic analysis, high dose dabigatran dominated the low dose, had an ICER of 49720 ?(?18014) versus warfarin. ICER value of low dose dabigatran strategy versus warfarin was 87719 ?(?31782). (Figure 1a) Cost-effectiveness acceptability curves of three treatment strategies were presented in Figure 1b.
Conclusions:From the perspective of Turkish National Health System, dabigatran is an efficient strategy for the SPAF compared to warfarin; ICER value was below the 61740 ?(?22369)/QALYs threshold in high dose dabigatran strategy.
Figure 1
P290
Implementation and clinical and economic evaluation of primary prevention of cardiovascular disease in an organized team
N Pyrikova1, I Osipova2, O Antropova2, A Zaltsman1
2Altay State Medical University, Barnaul, Russian Federation
Objective:to evaluate the clinical and economic effectiveness of the organizational model of primary prevention of CVD in a group of men of railway transport.
Material and methods:operators and operator assistants locomotive depot (2010-2012). In the 1st group (224 employee, 39,8±10.3 years) implemented the organizational model of primary prevention of CVD: the school of health at the workplace and individual in-depth preventive counseling in conditions of clinic and rehabilitation centre of the locomotive depot. 2nd group (128 employee, 36,2±11,0 years) were under annual medical supervision (clinical examination and medical commission). Analysis of the temporary disability by CVD, the cost analysis (direct and indirect costs).
Results:On the background of the implementation of the organizational model of primary prevention of CVD for three years in the 1st group decreased the temporary disability by CVD per 100 workers: number of cases by 32.8%, the number of days by 34.6%, and the average duration of one case decreased by 5.8%. In 2010 in the 1st group the temporary disability by coronary heart disease was 0.4 cases per 100 workers, through three years of preventive measures in 2012 cases of coronary heart disease is not registered. During the three years of monitoring in 2012 in the 2nd group increased the number of cases temporary disability by CVD 19.2%, the number of days by 8.7%, the average duration of one case of CVD increased by 1.2%. Including fixed doublingthe temporary disability by coronary heart disease (from 0.8 cases in 2010 to 1.6 cases per 100 employees in 2012). Direct costs associated with CVD in 2012 in the 1st group was decreased by 41.6% compared to 2010, accordingly, by 41.0% decreased indirect costs. In the 2nd group in 2012 increased costs associated with CVD: direct by 20.6%, indirect - 27.5%. Thus, for the three years of implementation of the organizational model of primary prevention of CVD in the 1st group experienced a reduction in overall costs by 44.1%, in the 2nd group, where workers were under annual medical surveillance, - 24.3% increased cost.
Conclusion:Clinical and economic effectiveness of the organizational model of primary prevention is defined by the lower number of cases and days temporary disability by CVD by more than 30%, prevent coronary heart disease, reduce costs associated with CVD, on average, 40%.
P291
Is pre-employment echocardiography needed? 96.2 % of pre-employment echocardiograms are normal in Egyptians.
A Al-Habbaa1
1Al-Azhar University, Department of Cardiology, Cairo, Egypt
Objectives:We investigate the usefulness of mandatory pre-employment echocardiography.
Patients and methods:The study included 469 peoples referred for pre-employment echocardiographic assessment for detection of any abnormalities in cardiac structure or function. All subjects had been subjected to the following: Informed consent, Routine medical screening, Chest X-ray, Laboratory tests and transthoracic echocardiography assessment.
Results:A total of 469 subjects were examined, comprising of 316 males (67.38%) and 153 females (32.62%). The age range of the subjects was 20–50 years (mean 27.41 ± 7.45 years). The echocardiogram was normal in 96.2% of the subjects. The commonest abnormality detected was mitral valve prolapse; accounting for 1.5% of the subjects studied. Left ventricular diastolic dysfunction was the next most common abnormality accounting for 1.3% of the echocardiographic diagnosis. Bicuspid aortic valve was the next most common diagnosis accounting for 0.5% of our findings.
Conclusion:Normal echocardiogram was the commonest echocardiographic finding and mitral valve prolapse was the commonest abnormality detected. Ease of access to echocardiography may influence the mandatory indication in pre-employment strategy and policy makers should incorporate appropriateness criteria into their guidelines for pre-employment investigations.
Type of echocardiography abnormality
No, of subjects
Percentage of subjects
Mitral valve prolapse
7
1.5%
Left ventricular diastolic dysfunction
6
1.3%
Bicuspid aortic valve
2
0.5%
Aortic valve prolapse
2
0.5%
Left ventricular hypertrophy
1
0.2%
P292
How do vitamin D and PTH affect diurnal blood pressure rhythm?
M Kutlu Karadag1, OZLEM Secen1
1Elazig Education and Research Hospital, Cardiology, Elazig, Turkey
Nondipper hypertension(HT) is a strong predictor of cardiovascular complications. Vitamin D deficiency is associated with hypertension, coronary artery disease and heart failure. Also parathyroid hormone(PTH) may adversely affect cardiovascular health. In this study we aimed to investigate the effects of Vitamin D and PTH on diurnal BP in newly diagnosed hypertension(NDHT). The study included 100 subjects divided into three groups: 34 normotensive (19 male, 53,4±9,6 years), NDHT 33 dipper (18 male, 54.4±11.7 years) and 33 nondipper patients(12 male, 56.7±9.7 years). No statistically significant difference was found in terms of basic characteristics. All patients were subjected to transthorasic echocardiography, routine laboratory tests, Vitamin D and PTH levels and ambulatory blood pressure monitoring(ABPM). Mean log(Vitamin D) was significantly low in nondippers (normotensive: 1.0±0.4 vs Nondipper: 0.8±0.3 vs Dipper: 1.0±0.3 ng/ml, p<0.001). Mean log(PTH) was 1.8±0.2 pg/ml and it was significantly high in nondippers (Normotensive: 1.7±0.2 vs Nondipper: 1.9±0.3 vs Dipper: 1.7±0.2 pg/ml, p<0.001). All 24-hr, day and nighttime SBP and DBP and mean arteriel pressures(MAP) were significantly elevated in nondippers. Vitamin D levels was negatively correlated with all 24-hr SBP and DBP(r= -0.366, p=0.003, r= -0.295, p=0.018) , day and night-time SBP and DBP(r= -0.377, p=0.002, r= -0.660, p<0.001), and likewise with 24-hr, day and night-time MAP. PTH was positively correlated with all average SBP and DBP and corresponding MAP levels.
Conclusion:Our results suggest that Vitamin D deficiency and PTH excess have positive correlation with blood pressures and nondipper hypertension in newly diagnosed HT. They may be suggested to measure Vitamin D and PTH to predict nondipping and target organ damage.
P293
Noninvasive markers of arrhytmogenesis in patients with sleep apnea syndrome and arterial hypertension
S Lypovetska1
1Ternopil State Medical University, Ternopil, Ukraine
The associations between obstructive sleep apnea (OSA) with cardiovascular morbidity and mortality is well known, but underlying mechanisms are not entirely delineated. Cross-sectional study of 58 patients, aged 45-65 years old, 29 males and 15 females with arterial hypertension, who underwent Holter ECG with rheopneumogram. Demographics, cardiovascular risk factors, heart rate variability, QT intervals, microvolt T wave alteration were examined. Patients were divided in 3 groups according to sleep apnea hypopnea index (AHI): group 1 (AHI < 5, n=15), group 2 (AHI =5-29, n=12), group 3 (AHI> 30, n=11). Control group – 20 patients without breath disturbances.
Results:Positive test on microvolt T wave alteration was found in 36.3 % patients with severe and 41.6 % moderate OSA and in 1 patients of control group. Results of heart rate variability and QT interval are presented in table1. Decreased heart rate variability, predominating of sympathetic activity, rigid rhythm, transient prolonged QT interval especially at night were common for patients with severe and moderate OSA. Significant positive correlation was found between AHI and QT interval (p=0.03, r=0.3), QTc interval (p= 0.04, r=0.5), negative correlation between AHI and SDNN (p=0.04, r= -0.3) Conclusion:Decreased heart rate variability, predominating of sympathetic activity, prolonged QT interval and T wave alteration are important background for fatal arrhythmias and predictors of sudden cardiac death in patients with OSA .
Indeces
Control group
I group
II group
III group
QT
394.7±10.1
405.8±6.0
442.7±9.2*
435.3±2.8*
QTc
411.6±3.4
414.3±6.1
451.7±5.9*
453.6±3.5*
D(QT)
8.4±0.9
6.0±1.3
8.5±2.3
9.8±1.1
SDNN
138.6±6.9
152.6±14.5
82.4±6.2*
81.0±9.4*
rMSSD
38.3±3.6
53.0±13.9
66.6±18.0
59.9±12.9
SDANN
118.3±5.8
131.7±15.0
98.2±13.9
63.0±7.5*
pNN
14.0±2.4
8.7±1.7
8.0±1.7*
5.0±1.4
HF
80.2±12.9
79.8±8.9
92.9±10.4*
65.0±8.6*
VLF
1894.6±33.6
1702.2±59.5
1561.8±23.2
708.1±11.7*
LF
802.2±20.4
344.6±43.3
514.5±10.2
554.0±11.8
*p<0.05, comparing with control group
P294
Endothelin-1, matrix metalloproteinases-2, -9 and C-reactive protein such as markers of cardiovascular risk in hypertensive patients with type 2 diabetes
K Kostov1, A Dimitrova1, S Tisheva2, A Russeva3, A Blazhev4, M Atanasova4, I Tsinlikov5
1Medical University Pleven, Department of Pathophysiology , Pleven, Bulgaria
2Medical University Pleven, Department of Cardiology, Pleven, Bulgaria
3Medical University Pleven, Department of Clinical Laboratory, Pleven, Bulgaria
4Medical University, Department of Biology, Pleven, Bulgaria
5Medical University Pleven, Department of Internal medicine, Pleven, Bulgaria
Topic: Sports cardiology
Purpose:Endothelin-1 (ET-1) is one of the most potent vasoconstrictors found to date. It possesses significant proliferative, profibrotic and pro-inflammatory properties and can contribute to many aspects of vascular changes in arterial hypertension (AH) and diabetes. Matrix metalloproteinases-2, and -9 (MMP-2, MMP-9) may be related to increased synthesis of collagen and vascular changes in AH, but their effects in type 2 diabetes mellitus (T2DM) have not been fully explored. C-reactive protein (CRP) is an acute phase protein which is synthesized by hepatocytes in inflammation. The aim of the study was to compare serum concentrations of ET-1, MMP-2, MMP-9 and CRP in hypertensive patients with T2DM and vascular complications, with those of a control group of healthy individuals.
Methods:Patients were divided into two groups: Group1 (G1) - 20 normotensive individuals without diabetes and without cardiovascular disease, control group (male-8, female-12; SBP = 122.5±3.9 mmHg; DBP = 81.7±3.8 mmHg; mean age 39.05±15.3 years). Group 2 (G2) - 50 patients with T2DM and AH (male-21, female-29; SBP = 146.83±11.9 mmHg, DBP = 82.55±9.7 mmHg; mean age 63.5±11.0 years). ET-1 was determined by ELISA kit of "Biomedika", MMP-2 and MMP-9 by ELISA kit of the "R&D Systems", and the CRP – through immunoturbidimetric method with monoclonal anti-CRP antibodies. The analysis used the statistical program STATGRAPHICS.
Results:It was found that the serum concentrations of ET-1 in G2 (G2=8.0±6.8 pg/ml) were higher than those of G1 (3.5±1.7 pg/ml), because there are statistically significant differences between them (p=0.0160). There are also statistically significant differences of MMP-2 and MMP-9 between G2 and G1, respectively for MMP-2 - between G2 (36.5387±11.3 ng/ml) and G1 (29.8085±7.5 ng/ml) (p=0.0187) and for MMP-9 - between G2 (39.1386±20.2 ng/ml) and G1 (22.6847±8.0 ng/ml) (p=0.0013). The serum concentrations of CRP in G2 (8.42305 ± 7.9 mg/l) were also significantly increased compared to those of G1 (1.06565 ± 0.8 mg/l) (p <0.0001).
Conclusions:Our study showed that the serum concentrations of ET-1, MMP-2, MMP-9 and CRP were significantly increased in hypertensive patients with T2DM and vascular complications, thus making them reliable markers for assessment of cardiovascular risk.
P295
The prevalence of high office blood pressure among students of the Altai region
V Dekhar1, OAG Osipov Ag1, DVV Denisova Dv2, OIV Osipova Iv1, SIV Sopotova Iv3
1Altay State Medical University, Barnaul, Russian Federation
2State Organization "Research Institute of therapy and preventive medicine" Siberian Branch of RAMS, Novosibirsk, Russian Federation
3City hospital 4, Barnaul, Russian Federation
Topic: Sports cardiology
Purpose:To study the prevalence of elevated office blood pressure (BP) among students living in urban and rural areas of the Altai Territory.
Materials and methods:2,000 students of universities and colleges of Barnaul were surved in a specialized clinic with its own students health center based KGBUZ "City hospital, Barnaul". The age of examined was 18 - 24 years, (19,2 ± 0,03) . Most of the students were first-year students of the city and previosly living in villages. There were 64% girls and 36% boys among them, urban and rural residents 59% and 41%, respectively, university students were 51%, college students were 49%. Each respondent was conducted measurement office blood pressure using the sphygmomanometer according to the method Korotkov. Definition and classification of office blood pressure (mm Hg) was conducted in accordance with European guidelines for the treatment of hypertension.
Results:The average blood pressure among boys and girls was 117,7 ± 0,3 / 74,8 ± 0,2 and 112,4 ± 0,2 / 72 ± 0,1 (mm Hg), respectively. The overall prevalence of elevated office BP among students was 3,3% (114,5 ± 0,3 / 73,2 ± 0,2 mm Hg), of them with increased systolic (SBP) - 1.5% (144,6 ± 1,2 / 79,2 ± 1 mm Hg), with increased diastolic (DBP) - 1,1% (123,4 ± 2,2 / 90,5 ± 0,4 mm. Hg), systolic and diastolic - 0,7% (143,2 ± 1,2 / 92,6 ± 1 mm Hg). Elevated office BP among boys and girls was 5.1 and 2.2%, respectively, of them have increased SBP - 3 and 0.5%, DBP - 1.1 and 1.2%, systolic and diastolic - 1 and 0, 5%, respectively. Number of young men with high blood pressure more than 2.3 times as compared to girls (p = 0.001). Elevated SBP among boys found in 6 times more often than girls (p = 0.000). Prevalence of elevated office BP among urban and rural students was 3.1 and 3.5% of them with higher SBP - 1.2 and 1.7%, increased DAD- 1.3 and 1.1%, systolic and diastolic blood pressure - 0.6 and 0.7%, respectively.
Conclusion:Prevalence of elevated office BP among students of the Altai Territory was 3.3%. Young men in 2.3 times more likely to suffer high blood pressure, compared to girls, with increased systolic blood pressure occurs 6 times more often (p = 0.000).
P296
Impact of risk factors and target organ damage on the prognosis in hypertensive patients (a follow-up study)
I Tasic1, S Kostic2, D Mijalkovic3, M Rihter2, D Lovic4, G Lazarevic5, S Andonov2
1Universisty of Nis, Medical faculty, Institute for Therapy and Rehabilitation, Nis, Serbia
2Institute for Therapy & Rehabilitation , Niska Banja, Serbia
3Clinic Kardiomedika, Nis, Serbia
4Clinic for internal medicine Intermedica, Nis, Serbia
5Clinical Center, Clinic for Cardiovascular Diseases, Nis, Serbia
The stratification of total cardiovascular (CV) risk in different categories is based on blood pressure (BP) category, CV risk factors, asymptomatic organ damage and presence of diabetes, symptomatic CV disease or chronic kidney disease.
Aim:Our aim was to assess the impact of the above parameters on long-term prognosis in patients with arterial hypertension.
Methods:The study involved 126 non-smokers (47 men) aged 63±8.5 years on average, with primary hypertension (mean BP 158/90 mmHg) and without CV disease, followed up for at least 10 years. During the follow-up, 9 patients (7.1%) died (8 died of cardiovascular causes and 1 of lung cancer). Major cardiovascular events were observed in 32 patients (25.4%). Patients with CV events had a significantly higher left ventricular mass index (158.9±31.6 vs. 134±30.7 g/m2; p<0.001), more pronounced intima-media complex thickening (1.09±0.25 vs. 0.93±0.24; p<0.003), more common plaques in both carotid arteries (71.9% vs. 20%; p<0.001), and more common diabetes (44% vs. 19%; p<0.006). Out of the risk factors, these patients had significantly higher values of systolic blood pressure (164 vs. 157 mmHg; p<0.046), while there were no differences in body mass index and lipid status values. The patients who died were significantly older (70 vs. 63 years; p<0.03), with higher left ventricular mass index values (156 vs. 134 g/m2; p<0.06), thicker intima-media complex (1.14 vs. 0.93; p<0.001), more common plaques in both carotids (75 vs. 20%; p<0.001), more common diabetes (62.5% vs. 19%; p<0.005), and lower glomerular filtration rate (54 vs. 69; p<0.03). Among the patients with cancer (9 pts – 7.1%), plaques in both carotid arteries were more common (50% vs. 20; p=0.049) as well as diabetes (50% vs 19%;p<0.04).
Conclusion:Target organ damage in hypertension and diabetes are the best predictors of adverse events in patients with hypertension.
P297
Correlation of asymptomatic hyperuricemia with cardiovascular events at patients with hypertension and left ventricular hypertrophy
I Tasic1, V Skakic2, S Kostic2
1Universisty of Nis, Medical faculty, Institute for Therapy and Rehabilitation, Nis, Serbia
2Institute for Therapy & Rehabilitation , Niska Banja, Serbia
Introduction:Data about connection between increased values of uric acid, cardiovascular diseases and death exist even since 19th century. Demonstrated the relation between gout, hypertension, obesity and cardiovascular diseases.
Paper objective:Objective of our study is to determine connection between increased values of serum uric acid and cardiovascular events at patients with hypertension and left ventricle hypertrophy.
Material and methods:Fifty one patient with hypertension and echocardiography left ventricle hypertrophy (LVH) have been tracked for 15 years. At the beginning of the study the complete laboratory tests were done at all patients, with assessment of the metabolic status, and uric acid was measured in the serum. None of the patients had gout, or took drugs for urinary acid reduction. After including in the study all patients were subjected to a clinical examination, and also an electrocardiogram, echocardiography, exercise testing, and Holter monitoring were done. Blood pressure (BP) was measured in the ambulance and by 24h BP monitoring.
Results:patients were divided into two groups based on uric acid values in the serum. In the first group were patients with uric acid values > 375µmol/l (25 patients with average age of 53.9; 17 male - 68%, body mass index (BMI): 29.4±3.1), and in the second group were patients with urinary acid values <375 µmol/l (26 patients with average age of 57.1; 12 male – 46%, BMI: 27.2±3.3). Patients with asymptomatic hyperuricemia (group I) had higher average BP values measured by 24 h monitoring (mean 24h: 151.6±18.9 vs. 142.7±7.8, p<0.04; mean day: 155.4±19.1 vs. 145.8, p<0.03; mean night: 140.9±20.4 pr 132.5±11.2 mmHg, p<008), and higher maximal BP at the exercise testing (213.3±20.3 vs. 201.9±23.2 mmHg; p<0.09). There was no significant difference in the left ventricle mass index determined by echocardiography measuring (157.1±76.8 vs. 158.1±25.5 g/m2ns). During 15-year tracking 8 patients from the group I died (all from cardiovascular – CV death), and 7 patients had a major CV event (myocardial infarction, stroke, coronary artery bypass grafting or percutaneous coronary intervention). From the patients of the group II, 5 examinees died (3 from CV death), and 3 had a major CV event. Such difference has a statistically significant level (p=0.036).
Conclusion:15-year tracking of patients with hypertension and left ventricle hypertrophy showed a significant correlation of asymptomatic hyperuricemia at the beginning of examination with BP values measured by 24h monitoring and prospective cardiovascular events.
P298
Effect of changes in circadian rhythm on mortality in elderly hypertensive patients
L Gaspar1, M Bendzala1, I Gasparova2
1University Hospital Bratislava, Bratislava, Slovak Republic
2Institute of Biology, Genetics and Clinical Genetics, Comenius University, Bratislava, Slovak Republic
Topic: Sports cardiology
Purpose:Blood pressure values during the day are not constant. Blood pressure (BP) is significantly variable over time, the actual current BP level is influenced by many factors, some of which are accidental, but many of them are not affected by random effect, and are rhythmically repetive with different interval. Similar to many biological functions of the body, BP is affected mostly by circadian rhythm. In our five-year retrospective study in a group of older hypertensive patients we were observing the differences in diurnal index and differences between dippers, non-dippers and reverse-dippers, related to overall mortality.
Patients and Methods:In our study group we included 170 hypertensive patients, 34 (20 %) male and 136 (80 %) female, in age 75 to 84 years, enrolled in the years 2005 to 2007, with the ambulatory blood pressure monitoring (ABPM) at the beginning of observation. The study group was divided according the ABPM results into dippers group (40 patients, 23.5 %), non-dippers group (65 patients, 38.2 %) and reverse-dippers group (65 patients, 38.2 %). ABPM was performed with a Cardiosoft Tonoport V, General Electric, USA, equipment.
Results:During the 5-year observation period after ABPM we registered 69 deaths (40.9 %). 10 deaths (25 %) was in the dippers-group, 23 (35.4 %) in the non-dippers group and 36 (55.4 %) in the reverse-dippers group.
Conclusions:Between the groups divided according to the diurnal index to dippers, non-dippers and reverse-dippers, there was observed a significant difference in the number of reported deaths. The absence of normal physiological diurnal index, drop in BP during night period, was associated with higher mortality. We confirmed that disturbed diurnal rhythm is a risk factor for all-cause mortality, even in specific hypertensive population aged over 75 years.
P299
Hypertension control in a large multi-ethnic cohort in Amsterdam, the Netherlands: The HELIUS study
C O Agyemang1, MB Snijder1, EJ Beune1, BJ Van Den Born1, LM Brewster1, JJ Ujcic-Voortman1, N Bindraban1, G Van Montfrans1, RJ Peters1, K Stronks1
1Academic Medical Center of Amsterdam, Public Health, Amsterdam, Netherlands
Objective:Hypertension is a major problem among European ethnic minority groups. We assessed the current situation of hypertension prevalence and its management among a multi-ethnic population in Amsterdam, the Netherlands.
Methods:Data from the HELIUS study were used including 1352 Ghanaians, 1905 African-Surinamese, 1716 South-Asian Surinamese, 1870 Turks, 1260 Moroccans and 1864 European-Dutch aged 18-70 years. Comparisons among groups were made using proportions and age-adjusted prevalence ratios(PR).
Results:Hypertension prevalence ranged from 21% and 14% in Moroccan men and women to 53% and 62% in Ghanaian men and women. Except for Moroccans, PR of hypertension was higher in all the ethnic minority groups than in European-Dutch. Among hypertensives, ethnic minority groups generally had higher levels of hypertension awareness and BP lowering treatment than European-Dutch. Moreover, prevalence rates for the prescription of more than one BP lowering drug was higher in all ethnic minority groups compared with European-Dutch. By contrast, BP control levels were lower in all the ethnic groups than in European-Dutch, with control rates being significantly lower in Ghanaian men (26%, PR=0.46; 95% CI,0.33-0.63) and women (45%, PR=0.76; 0.62-0.92), African-Surinamese men (30%, PR=0.53; 0.39-0.73) and women (45%, PR=0.71; 0.59-0.85), and South-Asian Surinamese men (43%, PR=0.76; 0.59-0.97) and women (47%, PR=0.67; 0.55-0.52) compared with European-Dutch men (55%) and women (61%).
Conclusion:Our findings indicate poor BP control in ethnic minority groups despite more frequent use of multiple drug therapy, urging the need for targeted educational programs to improve BP control in ethnic minority groups, particularly among African and South-Asian origin groups.
P300
Lipoprotein a as a cardiovascular risk factor in German employees population - cardiovascular screening at work
J Gilis-Januszewski1, R Gottfried-Kwasniok2, T Gilis-Januszewski3, F Van Buuren2, D Horstkotte2, K-P Mellwig2
1Heart and Diabetes Center NRW, Ruhr-University of Bochum, Bad Oeynhausen, Germany
2Heart and Diabetes Center NRW, Ruhr-University of Bochum, Department of Cardiology, Bad Oeynhausen, Germany
3Heart and Diabetes Center NRW, Ruhr-University of Bochum, Clinic for Thoracic & Cardiovasc. Surgery, Bad Oeynhausen, Germany
Topic: Sports cardiology
Purpose:We evaluated the association between elevated lipoprotein a - Lp (a ?levels and distribution of cardiovascular risk factors and cardiovascular family history in employees of different companies.
Methods:240 employees (94 women und 146 men) of different companies undergoing a cardiovascular screening programme ("Unternehmen mit Herz") were enrolled in this study. Depending on Lp (a) levels two groups were separated (first group with Lp (a) levels <60 mg/dl und second group with Lp (a) > 60 mg/dl). Gender, age, BMI, cholesterol, low density lipoprotein (LDL), high density lipoprotein (HDL), triglyceride, Hba1c, systolic and diastolic pressure, history of hypertension, type 2 diabetes mellitus, dislipidemia, nicotine abuse and anamnestic family data of coronary disease history, stroke, type 2 diabetes and sudden cardiac death (SCD) was evaluated with respect to the Lp (a) levels.
Results:In the first group of 208 employees with Lp (a) <60 mg/dl (mean age 44 ± 10 years, 124 male and 84 female) HDL level was 53 mg/dl ± 13 , LDL 125 mg/dl ± 33, triglyceride 151 mg/dl ± 98, BMI 25 ± 4 and mean systolic pressure was 136 mmHg ± 15 mmHg. In the second group of 32 employees with Lp (a) >60 mg (mean age 43 ± 11years, 22 male and 10 female) HDL level was 57 mg/dl ± 14, LDL 135 mg/dl ± 42, triglyceride 123 mg/dl ± 64 (34-660 mg/dl), BMI 25 ± 4 and mean systolic pressure was 131 mmHg ± 14 mmHg. The differences between those two groups of employees regarding the following parameter like gender, age, BMI, cholesterol, LDL, HDL, triglyceride, Hba1c, systolic and diastolic pressure, history of hypertension, type 2 diabetes mellitus, dislipidemia, nicotine abuse and anamnestic family data of coronary disease history, stroke, type 2 diabetes and sudden cardiac death were not significant.
Conclusion:There was no significant dependence of Lp (a) levels on others cardiovascular risk factors and cardiovascular family history in employees of different companies.
P301
Role of non-HDL cholesterol as the target for lipid management in secondary prevention: comparison with LDL cholesterol levels
L Alvarez Roy1, E Martinez Paz1, N Rojo Prieto1, I Iglesias Garriz1, L Garcia Bueno1, A Garcia Del Egido1, M Montes Montes1, J Bayon Fernandez1, R Estevez-Loureiro1, F Fernandez-Vazquez1
1Hospital of Leon, Cardiology, Leon, Spain
Topic: Sports cardiology
Purpose:Non-HDL cholesterol (NHDLc) contains all potential atherogenic lipid particles and has been suggested as a potential better cardiovascular risk predictor than LDL-cholesterol (LDLc). We sought to investigate the efficacy of lipid therapy in a cohort of patients with an acute coronary syndrome (ACS) according to the target used LDLc vs. NHDLc and according to the goal recommended in current practice guidelines.
Methods:We recruited consecutive 119 patients (mean age 67±13 years, male 75.6%) who had an ACS either unstable angina or myocardial infarction. We measured the levels of total cholesterol, LDLc, HDLc, triglycerides and calculated NHDLc at the time of admission and one month after discharge. We assessed the type of lipid-lowering treatment and the dosage used.
Results:Eighty two patients (68.9%) were on intensive statin therapy, being atorvastatin 80 mg (n=40, 33.6%) the most frequently prescribed. We found a significative decrease in the concentrations of total cholesterol, LDLc (?-20.6 mg/dL) and NHDLc (?-29 mg/dL) compared to baseline measurements (p <0.0001). The relationship between baseline LDLc and NHDLc with the values obtained after 1 month was lineal (R2 0.613, p<0.0001; R2 0.71, p<0.0001 respectively). However, the relationship between baseline level and the percentage of reduction was logarithmic (p<0.0001). The objective of LDLc <70 mg/dL was achieved in 44.5% of our patients and the NHDLc goal (<100mg/dl) in 57.1% (p<0.0001). Moreover, this findings are independent of the dose or type of statin used.
Conclusions:NHDLc goal is achieved more frequently than LDLc target, irrespective of dosing/type of statin therapy. Whether the use of NHDLc as a target to treat these patients translates into an improvement in clinical events needs to be clarified.
P302
Associations between HDL molecular subfractions and oxidized LDL in a sample population stratified for other cardiometabolic risk factors
PF Fernandes Bispo1, PO Rodrigues1
1New University of Lisbon, CEDOC/FCM, Lisboa, Portugal
Topic: Sports cardiology
Purpose:The protective role of HDL molecular subfractions on mechanisms involving LDL particle modifications is one important issue nowadays, and far to be solved. For instance, inflammation can modulate HDL particles functional properties, by changing lipidomic and proteomic, and their association with other cardiometabolic risk factors, like oxidized LDL (oxLDL) a well-known CVD predictor. We previously showed, in this cohort, that endothelial lipase and the body mass index (BMI) were independent predictors of HDL molecular subfractions.
Methods:The sample population was composed by 81 consecutive adults from both genders. oxLDL was determined by ELISA (n=56), and HDL molecular subfractions (Large, L-HDL; Intermediate, I-HDL and Small, S-HDL) by using the polyacrylamide gel electrophoresis system (n=60). Significant differences among subgroups were determined using independent-samples t test after analyses for equality of variances by Levene's test.
Results:For entire population, oxLDL correlated positively with age, BMI, glucose, total cholesterol (total-c), triacylglycerols, LDL-c, ApoB and S-HDL, and negatively with L-HDL (p<0.05). After stratified for hsCRP (cut-off, 2.0mg/L) the associations between oxLDL and L-HDL and S-HDL remain significant in the subgroup hsCRP <2.0mg/L (rs= -0.506, p<0.01 and rs=0.587, p=0.001) and in the subgroup hsCRP =2.0mg/L (rs= -0.419, p<0.05 and rs=0.416, p<0.05), respectively. A similar pattern was observed after stratified for glucose (cut-off, 100.0mg/dL). For HDL-c (cut-off, 50.0mg/dL) the statistical significance magnitudes were quite similar in both subgroups, but with increase in the correlation strength in the subgroup HDL-c = 50.0mg/dL. Conversely, after stratified for LDL-c (cut-off, 120.0mg/dL) only the subgroup LDL-c <120.0mg/dL maintained the significance between oxLDL and L-HDL and S-HDL (rs= -0.439, p<0.05 and rs=0.474, p<0.01, respectively). No significant correlations were found with I-HDL (p>0.05), in any subgroup analysis. HDL-c significantly (and inversely) correlated with oxLDL only in hsCRP <2.0mg/L and LDL-c <120.0mg/dL subgroups.
Conclusions:Our data seems to 1) support the protective role of L-HDL particles against LDL-mediated modifications by oxidative mechanisms, in contrast with S-HDL; 2) the concomitant presence of inflammation and (hyper)glycemia effectively attenuate such associations; and 3) LDL-c concentrations above the cut-off point can abolish/blunt the associations between L- and S-HDL molecular subfractions and oxLDL, which deserves further detailed analysis.
P303
Mechanistic approach on endothelial lipase phosphatidylcholine-fatty acid specificity/interactions: from human-to-computational studies
PF Fernandes Bispo1, PO Rodrigues1, NM Bandarra2, R Bernardino3
1New University of Lisbon, CEDOC/FCM, Lisboa, Portugal
2IPMA, DivAv, Lisboa, Portugal
3ESTM-IPLeiria, GIRM, Peniche, Portugal
Topic: Sports cardiology
Purpose:Changes in fatty acids profile and their ratios were common features observed in the Met Synd, obesity, diabetes or CVD, and associated with clinical outcomes. We recently reported that endothelial lipase (EL) mass positively associated with EPA/AA ratio in human Red Blood Cells (RBCs) membrane's. EL, a head-to-tail homodimer with a catalytic triad constituted for Ser-His-Asp, is essentially a PLA1 but also presents lysophospholipase (LysoPLA1) activity, if acyl migration takes place, towards mainly HDL. The current data extent and complement previous observation, by using computational models.
Methods:Computational DFT methods were used to analyse the structure and electronic properties of several non-zwitterionic 16:0-sn2-PC molecular species. The global minimum configurations were used for the final optimization study.
Results:Endothelial lipase showed a positive trend with 18:1(n-7+n-9) and 20:5n-3 (EPA) and negative with 18:2n-6 and 20:4n-6 (AA), and weak associations with 22:5n-3 (DPA) and 22:6n-3 (DHA), in RBCs. Geometric optimization B3LYP/6-31G(d,p) data indicate for 16:0-DPA-PC and 16:0-DHA-PC the lowest energy as isolated molecules, and both PC species showed the lowest and the highest C?#137;-C?#137; distances, 21.02 `and 30.81 l respectively. No significant differences were observed between 16:0-18:1n-9-PC and 16:0-AA-PC in case of C?#137;-C?#137; distances. However, the latter showed the lowest C=O(sn1)-C=O(sn2) and Ca-Ca distances and the former the highest one. Interestingly, in 16:0-EPA-PC the distances between N-choline and the carbon atoms in glycerol backbone are significantly lower 6.53 l 5.59 `and 5.37 l for CG1, CG2 and CG3, compared with others PC molecular species and mainly with 16:0-AA-PC (8.62 l 7.25 `and 6.36 l respectively). The CG1 on glycerol backbone for 16:0-AA-PC showed the lowest partial Mulliken charge (+0.038 a.u.) compared with other sn2-PC molecular species (e.g. +0.065 a.u. for EPA).
Conclusions:The lower distances between nitrogen and the carbon in sn1 of glycerol backbone can interfere with ester bond in this position and changes the specificity and/or the steric hindrance for catalytic triad of EL. The differences in acyl chain region can influence the packing properties of PC molecular species in monolayers/bilayers, and also EL activity. The present results put forward the role of EL as PLA1 and lysoPLA1, and some of the differences found here can also influence the levels and/or the speed of acyl migration, and the resulting hydrolytic products of EL.
P304
Obesity and body mass index in acute coronary syndrome: evaluation of the outcomes during hospitalization and at one-year follow-up
J G Goncalves Pereira1, D Moreira1, B Marmelo1, A Delgado1, L Abreu1, R Silverio2, L Ferreira Dos Santos1, J Oliveira Santos1
1Hospital Sao Teotonio, Cardiology, Viseu, Portugal
2Hospital Sao Teotonio, Internal Medicine, Viseu, Portugal
Topic: Sports cardiology
Purpose:It is a known fact that obesity, as an individual component of the Metabolic Syndrome, is closely related to cardiovascular disease. However, it seems that obese patients with acute coronary syndrome tend to have better short-term outcomes, often referred to as the "obesity paradox". In this study the authors compare mortality rates during hospital stay and at one year follow-up in obese and non-obese patients. Furthermore, body mass index (BMI) values are compared between the deceased and surviving populations.
Methods:In a retrospective study of patients admitted to the Cardiology Department of a centralized hospital for acute coronary syndrome, the authors analyze the BMI and clinical outcome during hospitalization and one year after discharge. It was considered obesity when BMI was superior to 30 kg/m2. Statistical analysis was made using SPSS v17.
Results:The study population consists of 1121 patients, 68.9% male, age 69.12±12.67 years old, of which 215 (19.1%) were obese. Patients were divided into 2 groups, the Obese group – group A (70.2% male, age 64.68±12.87 years old) and the Non-obese group – group B (68.6% male, 70.16±12.41 years old), with no statistical differences in sex (p=0.643) or age (p=0.365). No statistical significance was observed when comparing mortality between group A and group B during hospitalization (11.2% vs 7.4%; p=0.069) and at one-year follow-up (2.3% vs 5.3%; p=0.100). When comparing BMI values based on outcome during hospitalization, the group of deceased patients vs surviving patients showed the following values: 27.05±4.50 kg/m2 vs 27.31±4.10 kg/m2 (p=0.562). However, a statistical difference was observed when comparing BMI values after one-year follow-up, the results were 25.48±2.47 kg/m2 vs 27.37±4.18 kg/m2 (p= 0.015).
Conclusions:The study of this population showed no significant differences in outcome between obese and non-obese patients, thus not in accordance with the "obesity paradox". However, when comparing BMI, although no difference was found during hospitalization, there was a significantly higher BMI in the surviving patients after the one-year follow-up. This corroborates findings in several studies in which it is acknowledged that overweight patients with coronary disease have a lower risk of cardiovascular and total mortality than patients in the low and normal weight groups.
P305
Analysis of the prevalence of metabolic syndrome in patients with atrial fibrillation in the region of Pleven, Bulgaria
D Yakova1, S Tisheva1, M Hristov1, C James1, S Ohri1, A Yanakeva1, N Stancheva1, K Gospodinov1
1University Hospital Georgi Stranski, Department of Cardiology, Pleven, Bulgaria
Aim:To analyse the prevalence of metabolic syndrome (MS) in patients with Atrial fibrillation (AF).
Methods:and Materials: The study was conducted among 115 patients admitted to First Clinic of Cardiology, University Hospital - Pleven, Bulgaria between the 1st of April to the 1st of October 2014 with documented evidence of Atrial Fibrillation. Patients were examined for the prevalence of arterial hypertension, diabetes, dyslipidaemia and obesity. Data from current and previous medical records, together with a 24-hour ECG record, was analysed. We examined the pre and postprandial blood glucose levels, lipid profile, waist circumference, treatment of arterial hypertension and dyslipidaemia. Patients were classified with MS according NCEP ATP III criteria. . We searched for the relation between the components of Metabolic Syndrome and incidence of atrial fibrillation.
Results:From the studied population with Atrial Fibrillation 54 patients were diagnosed with Metabolic Syndrome, of which 26 are men and 28 women. Of the patients with Metabolic syndrome and atrial fibrillation 24 patients are with paroxysmal atrial fibrillation and 30 are having chronic atrial fibrillation. 79 patients are with waist circumference above the upper limit, 42 of which are men and 37 women. 104 patients have arterial hypertension and atrial fibrillation of which 60 are male and 44 are female.
Conclusion:Metabolic Syndrome is widely spread among patients with atrial fibrillation in the studied population. A tight correlation between any of the components of the metabolic syndrome and the atrial fibrillation was found. This correlation is caused not only by the effects of the separate components, but also because of their additive mechanism of the components of Metabolic Syndrome.We observed strong correlation between the number of components of Metabolic Syndrome with the incidence of Atrial Fibrillation. .
P307
Has metabolic syndrome a paradoxical effect on long-term outcome of patients with established coronary artery disease?
A T Timoteo1, M Mota Carmo2, C Soares1, R Cruz Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
2New University of Lisbon, Faculty of Medical Sciences, Lisbon, Portugal
In the general population, obesity has a significant impact on prognosis. However, in populations with established cardiovascular disease it is described a paradoxical effect of obesity. Also with metabolic syndrome (MS), several meta-analysis showed the unfavourable impact of MS in the occurrence of cardiovascular events, although the impact in stable coronary disease is debated. We sought to analyse in a population of patients with coronary artery disease the long-term prognostic impact of MS.
Methods:We included patients admitted electively for coronary angiograhy. All patients had documented significant coronary artery disease and were submitted to coronary angioplasty. Patients were divided in two groups according to the presence of MS (AHA/NHLBI definition) in the baseline evaluation. In a five-year follow-up, we evaluated the occurrence of all-cause mortality, cardiovascular hospitalisation and a composite of both endpoints.
Results:In our study, we included 548 patients, 76% males, with a mean age of 65 ± 10 years. From these, 95% had hypertension, 16% were smokers, 36% had diabetes and 71% had hyperlipidemia. In 59.3%, MS was present. In previous history, 23% had a previous myocardial infarction, 34% coronary angioplasty and 7% coronary artery bypass grafting. In the follow-up, there were 36 deaths (6.6%) and 246 patients (44.8%) were re-admitted for cardiovascular reasons. Patients with MS did not have higher incidence of death (7.1% vs. 5.8%, p=0.687), cardiovascular admission (47.7% vs. 40.8%, p=0.111) or the composite endpoint (51.4% vs. 43.9%, p=0.087). Kaplan-Meier curves weren't significantly different in patients with and without MS for the three endpoints considered. MS wasn't a predictor of mortality (OR 1.23, 95% CI 0.61 – 2.48), cardiovascular admission (OR 1.32, 95% CI 0.94 – 1.87) or death / cardiovascular admission (OR 1.35, 95% CI 0.96 – 1.90), even after adjustment for the other baseline characteristics. Smoking and age were the only independent predictors of mortality.
Conclusion:MS isn't a predictor of outcome (mortality, cardiovascular hospitalisation or death / cardiovascular hospitalisation) in a long-term follow-up in patients with established coronary artery disease. Also we did not found any paradoxical effect.
P308
Visceral adipose tissue influences on coronary artery calcifications at young and middle-age groups using computed tomography angiography
R Abazid1, MOBADA Kattea1, HANAA Saqqah1, SAWSAN Sayed1, OSAMA Smettei1
1prince sultan cardiac center, burydah, Saudi Arabia
purpose: Visceral adipose tissue (VAT) is considered as risk factor for coronary artery disease (CAD). However, there are limited data on the relationship between VAT and CAD in young and middle-age patients. The purpose of the study is to evaluate the impact of excessive VAT on subclinical coronary atherosclerosis and coronary artery calcifications (CAC) in young and middle-age groups using multislice computed tomography (MSCT).
Methods:This study is a single center, cross sectional, study held in the cardiac center, where eligible patients (n=159) under the age of 61 years, with chest pain and mild to moderate probability to have CAD were enrolled. Coronary calcium score (CCS) and epicardial adipose tissue (EAT) were measured at the level of left main (LM) coronary artery, while VAT was measured at the level of iliac crest.
Results:the average age were (48 ± 8 years) .the mean VAT were (38±21cm2) with no significant difference between men and women (38±22 vs. 37±19. P=0.8) respectively. Student t-test analysis showed significantly higher VAT in patients with detectable CAC than patients with no CAC (48±24 vs. 33±18 .P = 0.00002) respectively. Univariate regression analysis showed that VAT and EAT, are strong predictor for CAC [hazard ratio (HR)1.034 ,95% CI(1.016-1.052). p<0.001 and (HR) 1.344,95% CI (1.129-1.601) p=0.001] respectively.
Conclusion:Excessive visceral adipose tissue (VAT) is significantly associated with positive coronary artery calcification. VAT can strongly predict subclinical coronary artery disease in individuals at young and middle-age groups.
P309
Non-lab predictors of metabolic syndrome from sonographic lipometry
A Ryabikov1, Z Guliev1, S Malyutina2, YU Ragino2, N Yasyukevitch2, EU Veryovkin2
1Novosibirsk State Medical University, Novosibirsk, Russian Federation
2Institute of Internal Medicine SB RAMS, Novosibirsk, Russian Federation
Topic: Sports cardiology
Purpose:Novel ultrasonic approach for subcutaneous and abdominal fat measurement is proposed for assessment of body fat distribution. The relationship between ultrasonic lipometric indicators and cardio-metabolic profile in a general population was not studied. We investigated the relationship between subcutaneous and premesenteric fat layer and metabolic factors / syndrome (MS) and in a population-based sample.
Methods:We used the data from a random population sample (n=163; men/women aged 18-64) examined by EPOGH Project. Subcutaneous fat (subCF) thickness and preperitoneal fat (prePF) thickness and width were measured on transverse images with conventional ultrasound probes on the abdominal midline in subxiphoid region and validated against CT (n=40). CVD risk factors and anthropometric measures (body mass index, BMI; waist-to-hip ratio, WHR; skin fold) were evaluated. MS was defined by IDF, 2006 criteria. Correlates of fat measures were assessed in multivariable linear regression. Prediction of MS by subCF and prePF was tested in ROC analysis.
Results:Image acquisition and online measurements were feasible in 100% . Mean subCF thickness was of 1.25cm (SD 0.55), mean prePF thickness was of 1.52cm (SD 0.63). Both fat measures were associated with BMI, WHR, and skin fold. Determinants of subCF thickness were female sex (p=0.042), systolic blood pressure (SBP) (p=0.051), insulin (p=0.034). Determinants of prePF thickness were SBP (p=0.001), insulin (p=0.03), and total cholesterol (p=0.037). Additionally, prePF was negatively associated with HDL-C (p=0.021). In ROC curve analysis prePF thickness and width were strong predictors of MS with AUC=0.78 ( p<0.0001) and AUC=0.82 (p<0.0001), correspondingly. In age- and sex-adjusted logistic regression prePF thickness >1.6cm, and prePF width >7.0 cm significantly increased risk of MS (OR=4.5, p=0.016 and OR=4.5, p=0.015; respectively). The subCF thickness >1.3cm increased risk of MS with OR=4.9, p=0.027.
Conclusion:Ultrasonic lipometric indicators of subcutaneous and preperitoneal fat are independently associated with insulin, SBP, female sex (subCF). Additionally, prePF but not subCF was positively associated with total cholesterol and negatively with HDL-C. All ultrasonic measures increased risk of MS in dose-dependent fashion. Threshold values of 1.6 cm for prePF thickness, 7.0cm for width, and 1.3 cm for subCF thickness were predictive for MS. Sonographic indicators are supposed to be screening "non-lab" measure for central adiposity and MS. The study was based on data from EU IC15-CT98-0329-EPOGH.
P310
Associations of regular physical activity with cardiovascular risk factors in young adults
J Jurkovicova1, Z Stefanikova1, K Hirosova1, M Samohyl1, L Argalasova1, J Babjakova1, L Sevcikova1
1Faculty of Medicine Comenius University, Bratislava, Slovak Republic
Topic: Sports cardiology
Purpose:The beneficial effects of physical activity (PA) on health outcomes are generally well understood and physical inactivity is an important and modifiable CVD risk factor. We aimed to assess the effect of PA on selected CVD risk factors in the sample of young healthy subjects.
Methods:In the cross sectional study from the sample of 1,583 university students (26.1% of men) in mean age 22.8±1.5 yrs examination included standardized questionnaire on life-style characteristics (including self-reported leisure time PA), and dietary habits. Objective measurement included anthropometric data, BP and blood lipids (TC, TG, HDL-C). LDL, BMI, TC/HDL, log TG/HDL and total cardiovascular risk using Relative risk (RR) SCORE chart were calculated. The sample was divided into two groups according to duration and frequency of vigorous leisure time PA and compared: (i) low PA–LPA (123 men, 527 women), and (ii) high PA–HPA (290 men, 643 women) levels.
Results:The HPA group of men had lower body fat percentage (p=.023), waist/height index (p=.036), TC/HDL (p=.003), log TG/HDL (p=.007), resting HR (NS), RR (NS), and higher lean body mass (p=.030) and HDL-C (p=.009). The HPA group of women presented with higher lean body mass (p=.001), HDL-C (NS), lower resting HR (p=.000), TG (p=.028), and RR (NS). Bivariate analysis (age adjusted) showed positive relation of regular PA with HDL-C (p=.003) in men and with BMI in women (p=.009), and inverse relation with waist/hip ratio (p=.006), TC/HDL (p=.007), log TG/HDL (p=.008), and energy balance (p=.002) in men, and with TG (p=.026), log TG/HDL (p=.011), resting HR (p=.000) and energy balance (p=.000) in women, respectively. Multivariate linear regression model confirmed significant positive association of PA with HDL-C in men and with lean body mass in both sexes, inverse association with TG and resting HR in women, and with log TG/HDL in both sexes. In both sexes of HPA group were lower prevalence of smokers, and generally better dietary habits, especially lower consumption of fast-food, sweets and sugar sweetened beverages.
Conclusions:Our findings suggest the positive effects of regular moderate/vigorous PA on selected cardiometabolic risk factors and healthier body composition for both men and women. The regular PA has the beneficial health effects not only per se, but likely through healthier life style and/or dietary habits, too. However, this indicates that long-term prevention strategies should be developed to increase physical activity and cardiorespiratory fitness early in life, with the goal of promoting a physically active lifestyle.
P312
Total and leisure-time physical activity is associated with reduced mortality in the elderly cohort of the MOLI-SANI Project
S Costanzo1, A Di Castelnuovo1, M Persichillo1, A De Curtis1, M Bonaccio1, C Cerletti1, MB Donati1, G De Gaetano1, L Iacoviello1
1Department of Epidemiology and Prevention. IRCCS Istituto Neurologico Mediterraneo Neuromed, Pozzilli, Italy
Topic: Sports cardiology
Purpose:Physical inactivity is a major public health problem associated with increased mortality risk. The aim of this study was to examine the possible association of total and leisure-time physical activity with all-cause mortality among Italian elderly women and men.
Methods:Elderly individuals (N= 4,939, 50% men, aged =65 years) were studied within the MOLI-SANI cohort; the latter was randomly recruited from the general adult population of Molise Region, in Southern Italy. Physical activity was assessed by a structured questionnaire (24 questions on working and leisure time (sport, walking, gardening)) and expressed as daily energy expenditure in metabolic equivalent task-hours. The cohort was followed-up for mortality for any cause for a median of 4.3 years. The ascertainment of vital status was carried out through linkage with demographic rosters. Total and leisure-time physical activity (as continuous variables) and their association with total mortality was assessed using multivariable Cox proportional hazard models.
Results:During follow-up, 352 deaths occurred in 4,939 subjects aged 65-97 years at enrollment. Total physical activity was inversely associated with total mortality, with a reduction of 18% (95% CI: 1-33%, p= 0.045) for a 4 MET-hrs/day increase (multivariable model, table). Moreover, similar reduction (15%, 95% CI: 4-25%, p= 0.0085) was observed when leisure-time physical activity only was considered . These associations were still present, although not statistically significant, when either CVD or cancer mortality were considered separately.
Conclusions:An increase in total or leisure time physical activity of 4 MET-hrs/day (approximately a 30 min. brisk pace daily walk) was associated with a 15% reduction in total mortality in a general elderly population.
Hazard Ratio and 95% CI for Death by Increase of 4 MET-hrs/day
Total Physical Activity
HR (95% CI)
P value
Age and sex adjusted
0.77 (0.63-0.93)
0.0084
Multivariable model*
0.82 (0.67-0.99)
0.045
Leisure time Physical Activity
Age and sex adjusted
0.80 (0.71-0.91)
0.0004
Multivariable model*
0.85 (0.75-0.96)
0.0085
*Diabetes, CVD and cancer history, smoking, BMI, alcohol intake, educational, income, caloric intake.
P313
Moderate to vigorous physical activity is inversely associated with arterial stiffness in post-myocardial infarction patients
A J Alves1, N Oliveira1, G Silva1, L Campos2, M Teixeira3, F Ribeiro4, J Oliveira1
1University of Porto, Research Center in Physical Activity, Health and Leisure, Faculty of Sport, Porto, Portugal
2Hospital Center of Vila Nova de Gaia/Espinho, Physical Medicine and Rehabilitation Department, Vila Nova de Gaia, Portugal
3Hospital Center of Vila Nova de Gaia/Espinho, Cardiology Department, Vila Nova de Gaia, Portugal
4University of Aveiro, School of Health Sciences, Aveiro, Portugal
Background:Carotid-femoral pulse wave velocity (cf-PWV) as an indicator of aortic wall stiffness have shown an independent predictive value for cardiovascular and all-cause mortality. In addition, physical activity (PA) showed an independent association with several measures of arterial stiffness in young healthy adults.
Topic: Sports cardiology
Purpose:To analyze whether regular PA was correlated with cf-PWV and derived measures of central pressure and augmentation index in post-myocardial infarction patients.
Methods:In this cross-sectional study, 86 consecutive patients were assessed, 6 weeks after suffering an acute myocardial infarction, for clinical variables, anthropometrics, PA and arterial stiffness. PA was recorded in an accelerometer that participants wore for seven consecutive days. Arterial stiffness was evaluated using measures of cf-PWV, and central and peripheral pulse pressure (PP) and augmentation index adjusted to heart rate at 75 bpm (AIx@75).
Results:cf-PWV showed a moderate negative association with total weekly time spent in moderate (r=-0.284) vigorous (r=-0.412) and moderate to vigorous PA (r=-0.308). Vigorous PA was also inversely associated with aortic systolic pressure (r=-0.302) and AIx@75 (r=-0.318). No association was found between cf-PWV and total weekly time spent in light PA. In addition, cf-PWV was significantly lower in physically active patients (=150 minutes of moderate PA per week) compared with those who were less physically active (7.8 ± 1.9 m/s vs. 8.9 ± 2.4 m/s, p<0.05). These results remained significant after adjustment for age, gender, medication, diabetes and obesity.
Conclusions:Our data show that moderate to vigorous PA is inversely associated with arterial stiffness in post-myocardial infarction patients.
P314
Features of personal-adaptive potential in women with acute myocardial infarction
I A Leonova1, N Tretyakova1, S Boldueva1
1North-Western Sate Medical University named I.I. Mechnikov, St-Petersburg, Russian Federation
Studies of personality characteristics and behavioral characteristics that influence the development of myocardial infarction (MI) are few and relate to men.
Objective:to study the characteristics of personality-adaptive capacity in women with MI.
Materials and methods:60 women with MI (mean age 49 ± 8,6 years) and 38 patients without coronary artery disease (CAD) (mean age 50 ± 7,7 years). Questionnaires Hardiness Survey (SR Maddi), Life style index and method for psychological diagnosis coping mechanisms were used.
Results:Hardiness in the group of women with MI was 74,64 ± 2,6 points, the women in the control group 77,71 ± 1,95 points. On scales "Involvement", "Control", "Acceptance of risk" was not obtained significant differences between women with MI and control group. Women with high levels of Hardiness seek medical help faster compared with patients with lower levels of Hardiness (p = 0,01). A significant relationship indicator "involvement commitment» to-income patients (p = 0.01) and the parameter "control" - with the debut of CAD as MI (p = 0.04). In the presence of a history of angina were observed higher values of the parameter "control» in individuals with lower functional class of angina (p = 0.04), suggesting that the patient tried to control the course of the disease, following the advice of a doctor. The study of LSI has shown that "Denial» and «Substitution» at women with MI were more pronounced as compared to women in the control group (p <0.05). The degree of severity indicators "Denial» and «Compensation" have a direct correlation with the duration of pain and eventually seeking medical care (r = 0,29 p = 0,03 and r = 0,36 p = 0,007, respectively). The "Extrusion» has a connection with recurrent MI (p = 0,048), «Projection" with the development of early postinfarction angina (p = 0.049). It was shown a significant correlation "Substitution" and the development of ventricular arrhythmias (p <0.05). It was no significant differences in the use of coping strategies in women with MI and control group. But it is shown that in women with MI presented less adaptive cognitive coping strategies (40%) and is dominated by the adaptive emotional (60%) and behavioral coping strategies (53.3%).
Conclusion:In women with MI not changed the level of "resilience" and among parameter "negation" and "substitution", which leads to the fact that patients are not really aware of the severity of their illness and try to cope with the stress of being distracted from their own state.
P315
Type D personality and polyvascular disease in patients with coronary artery disease: gender related differences
A N Sumin1, EV Korok1, OI Raich1, RA Gayfulin1, AV Bezdenezhnyh1, OL Barbarash1
1RAMS Scientific-Research Institute for Complex Studying of Cardiovascular Diseases, Kemerovo, Russian Federation
Background:Non-coronary atherosclerosis in patients with coronary artery disease (CAD) has adverse prognostic significance. Although gender related differences of risk factors and clinical manifestations of atherosclerosis are well known, they are still poorly understood in patients with polyvascular disease (PolyVD). Gender effect on the relationship between type D personality and the presence of PolyVD has not been studied yet.
Objective:To study the prevalence of type D personality based on the presence of PolyVD and gender related differences.
Material and methods:709 patients with stable CAD were examined and treated in the NII KPSSZ for the period from 1 February 2009 to 31 January 2010. Patients were assigned into four groups according to their gender and the presence of PolyVD: Group 1 – females without PolyVD (n = 108), Group 2 – females with PolyVD (n = 23), Group 3 – males without PolyVD (n = 471), Group 4 – males with PolyVD (n = 107). PolyVD was diagnosed as a combination of stenotic lesions >50% of two or more arteries. The presence of type D personality before CABG was evaluated with the Type D Scale (DS14) Results:Type D personality was diagnosed more frequently in the presence of PolyVD both in males (43.9%) and females (52.2%), than in patients with isolated coronary lesions (p <0.001). PolyVD patients of both genders had higher levels of negative excitability and social inhibition (Table 1).
Conclusion:Type D personality in CAD patients was more frequent in the presence of PolyVD than without it, regardless of gender (p <0.05). The relationship between the presence of type D personality and PolyVD may be regarded as one of the mechanisms of adverse effect of type D personality on prognosis in CAD patients
PolyVD – polyvascular disease; * - p<0.05 in comparison with females without PolyVD; # - p<0.05 in comparison with females suffering from PolyVD; $ - p<0.05 in comparison with males without PolyVD
Parameters
Females (n=131)
Males (n=578)
p
without PolyVD (n=108)
with PolyVD (n=23)
without PolyVD (n=471)
with PolyVD (n=107)
Type D, n (%)
13 (15.9)
12 (52.2)*
80 (17.0)#
47 (43.9)* $
<0.001
Negative excitability, scores
6,5 [5;9]
10 [7;12] *
7 [6;9]#
9 [6;12]*$
<0 . 001
social inhibition, scores
8 [7;9]
10 [8;13] *
8 [7;9] #
10 [7;12] * $
<0.001
P316
How our emotions affect dietary habits? - results from Russian ESSE-RF epidemiological study
OP Rotar1, E Dubinina2, E Isaeva3, S Gudkova4, R Libis3, D Duplyakov4, V Solntsev1, A Alehin2, A Konradi1, E Shlyakhto1
1Federal Almazov Medical Reseach Centre, Saint-Petersburg, Russian Federation
2Herzen State Pedagogical University, Saint-Petersburg, Russian Federation
3Orenburg State Medical Academy, Orenburg, Russian Federation
Purpose:The aim of our study was to estimate the association of psychoemotional status with unhealthy dietary habits in general population of 3 Russian cities: Saint-Petersburg, Orenburg and Samara.
Design:As a part of all-Russian epidemiology survey ESSE-RF random sampling of 4800 inhabitants (Saint-Petersburg, Orenburg, Samara) 25-64 years stratified by age and sex was performed. All participants signed informed consent and filled in the questionnaire regarding risk factors, concomitant diseases, medication, education, income and nutrition. Depression and anxiety were assessed by HADS. Anthropometry and fasting lipids, glucose (Abbott Architect 8000 (USA), Roche-diagnostics) were performed. All multivariable logistic models were adjusted for sex, age, education and income. We adjusted results for concomitant conditions: 12,1% of participants had cardiovascular diseases, 49,9% – gastrointestinal diseases, 4,8% – diabetes mellitus (excluded in the analysis of sweets consumption).
Results:Total sample of 1941 (40.4%) men and 2859 (59.6%) women were investigated. Increased level of anxiety was detected in 50,9% of responders (= 8 points HADS) and depression in 30,1% (= 8 points HADS). Depression was revealed more often in females, in older participants and subjects with low income. Participants with depression preferred animal fat (OR=1,94, CI 95%=1,49-2,54, p<0,001) and had decreased consumption of sugar and cakes (OR=0,83, CI 95%=0,73-0,94, p<0,01). Intake of sausages and meat by-products were significantly higher in depressive patients (OR=1,61, CI 95%=1,37-1,89, p<0,001) only if they didn't have signs of anxiety (OR=1,23, CI 95%=1,06-1,43, p<0,01). Chances to consume sweets were the highest in the presence of anxiety and low income in the youngest age group: males (OR=3,67, CI 95%=1,02-13,14, p<0,05) and females (OR=6,59, CI 95%=1,73-25,05, p<0,01).
Conclusions:Eating behavior appears to be associated both with depression and anxiety as well as the income. Depression is associated with twice higher consumption of unhealthy animal fat. In contrast to anhedonia in depression young participants with low income and anxiety like to eat sweets.
P317
What has changed in quality of life perception of children since theKiGGS study in Germany
J Mueller1, T Giegerich1, J Elmenhorst1, R Oberhoffer1
1Institute of Preventive Pediatrics, Technische Universit?M?, Munich, Germany
Objective:Health-related quality of life (HrQoL) is a multidimensional concept including self-reported measures of physical and mental health. The German Health Interview and Examination Survey for Children and Adolescents" (KiGGS) has established reference values for children and adolescents in the years 2003 to 2006. This study evaluated a current cohort of children and adolescents for their HrQoL and compared them with the KiGGS cohort from almost ten years ago.
Patients and Methods:From April 2012 to July 2013, we prospectively examined 386 apparently healthy children (13.4 ± 2.2 years, 171 girls) and their parents for their childrens HrQoL using the KINDL® self-report and parents-report questionnaire. Data were compared to the established reference value from Ravens-Sieberer and colleagues from 2007.
Results:Children and adolescents presented a better HrQoL (103.6 ± 13.2 % of predicated reference value, p<.001) compared to the KiGGS cohort. Also their parents rated the HrQoL of their kids better than the cohort ten years ago (103.4 ± 12.6 % of predicated reference value, p<.001). There were no gender differences, but a trend that mothers assumed higher HrQoL in daughters and, vice versa, fathers in sons. There was good agreement in the inter-individual assessment of HrQoL in children and their parents with a low coefficient of variance of only 5.8%.
Conclusions:Health-related quality of life in children and adolescents has increased within the last years and parents assess the HrQoL of their children and adolescents almost as well as their kids do.
P318
Just ask the patient: Assessing the demand for psychosocial counselling in cardiac patients
EK Kunschitz1, O Friedrich2, J Sipoetz1
1Hanusch Hospital, Vienna, Austria
2Karl Landsteiner Institute for Scientific Research in Clinical Cardiology, Vienna, Austria
Background:Psychosocial factors play an important role in the pathogenesis of coronary artery disease (CAD). Because of limited resources in the current health care environment it is important not only to identify patients with psychosocial risk load but also to single out those, who are motivated to engage in additional therapy and therefore most likely will benefit from further treatment. An obvious way to identify patients with a potentially high level of commitment is to assess the patients' request for treatment. Our study aimed to assess patients request for psychosocial counseling (PC) with a patient self-administered questionnaire (ADAPT) Methods:233 patients (age: 54.5±13.4, 57.5% male) referred for exercise stress testing to the outpatient cardiac care unit Wien Mitte answered the ADAPT. The SF-36 Quality of Life and the Hospital Anxiety and Depression Questionnaire (HADS) were used to investigate if the request for PC is consistent to impairment of generic quality of Life and the presence of mental distress.
Results:31.8% of the patients expressed moderate or strong demand for PC. They reported significantly lower scores in all SF-36 domains than the norm population except for General Health. Request for PC was strongly associated to positive indicators of mental distress: Compared to patients without demand for PC patients demanding PC showed significantly more often SF-36 MCS-scores <42 (55.0% vs. 17.4%; OR: 5.8), SF-36 Mental Health-scores <53 (47.8% vs. 18.8%; OR: 4.0), HADS-Anxiety-scores >7 (59.7% vs. 26.4%; OR: 4.1) and HADS-Depression-scores >7 (32.8% vs. 14.3%; OR: 2.9).
Conclusion:Our study shows that the patients' request for PC reflects impairment of generic health status and psychological risk load, thereby indicating that screening for patient's subjectively perceived demand for PC is an adequate method in order to select patients for clinical trials, to optimize the allocation of health care resources and to improve therapeutic strategies in a patient-centred way.
P319
Teaching preventive cardiology in ufa bashkortostan russian federation
H M Lipman1, J Rosenthal2, R Meakin2
1International Cardiac Healthcare & RiskFactor Modification, London, United Kingdom
2University College London, Primary Care & Population Health, London, United Kingdom
Introduction:There is no specific undergraduate teaching of preventive cardiology (PC) in the Russian Federation. Postgraduate teaching is patchy and poorly standardised. With the agreement of the President and Government of the Republic of Bashkortostan, ICHARM & University College London developed and delivered a ten seminar introductory taught course in PC for doctors in Bashkortostan. This was the first time that foreigners had taught PC to Russian medical staff in their home country Methods:The seminars were delivered in Ufa, July 2014. These covered epidemiology and risk factors, medical and lifestyle management, programme implementation and evaluation. They were taught in an interactive manner with the assistance of a Russian interpreter by two British doctors who also wrote the course. The programme included small group discussion and (the novel approach of) role play. Presentations utilised printed dual translation of slides and data both in written and spoken form. Following these, delegates completed evaluation forms (covering content, diversity and relevance to their practice). 18 of the delegates were trained to teach subsequent courses to their colleagues in the nine Republic regions, with oversight from the Republican Cardiological Centre, Ufa.
Results:120 Russian doctors, all involved in either primary or secondary CVD prevention, from Ufa and the 8 administrative regions attended. A total of 445 seminar evaluation forms and 83 course forms were returned. The great majority rated the course very highly [scores 4 or 5 (scale 0-5) for Content/Presentation/Value/ Enjoyment]. Written comments praised the teaching methodology, & the systematic approach taken to both risk assessment and patient and population management.
Discussion:This is the first report of post graduate training in preventive cardiology within Bashkortostan. We show that a PC course can be adapted and delivered successfully in translation using modern teaching methods to an audience whose prior experience is more didactic. We believe that the ICHARM/UCL Preventive Cardiology course would be useful in a variety of international settings. Training of trainers is an essential component for long term success through capacity building, and the knowledge that a uniform approach to PC teaching and management is being applied.
P320
Screening adolescent blood donors for future cardiovascular disease risk
S Eason1, M Sayers1, S Goudar1
1Carter BloodCare, Bedford, United States of America
Topic: Sports cardiology
Purpose:Cardiovascular disease is the major cause of premature death in Europe and the United States. High cholesterol is associated with increased future risk of cardiovascular disease which can progress asymptomatically for years. Identification of young individuals at risk, information about the prevalence of risk in this group and knowledge as to how this risk changes over time would be valuable. Since our blood program performs routine total non-fasting serum cholesterol on all donors at each donation, we decided to investigate adolescents (age 16-19) for their distribution of cholesterol levels and changes in each individual's level over a five year period.
Methods:Participants in the study were healthy volunteers presenting at school sponsored blood drives and qualified as blood donors. Total non-fasting serum cholesterol measurements (Beckman Coulter AU680) were evaluated at their first blood donation in 2009, when they were 16-19 years of age, using residual blood drawn for routine infectious disease screening. A subsequent measurement was taken on the same individuals when they presented for donation five years later in 2013. While not a requirement for qualification as a donor, individuals were given the option of declaring their ethnicity.
Results:Review of donor records revealed 1730 donors, 968 females and 762 males, donating blood in years 2009 and 2013. When first tested, 83 (4.8%) of the participant group had a cholesterol greater than 200 mg/dL (ã5 mmol/L). When reviewed by gender, 5.7% of the females and 3.6% of the males had cholesterols greater than 200 mg/dL (ã5 mmol/L). On subsequent testing five years later, 194 donors (11.2%) had cholesterols greater than 200 mg/dL (ã5 mmol/L). The percentage of women with cholesterols greater than 200 mg/dL (ã5 mmol/L) increased to 10.7% and for men, to 12%. In a review of changes by ethnicity, the largest percentage change occurred in Hispanic females. In that group 3.5% had an elevated cholesterol in 2009 and 8.5% in 2013.
Conclusions:Addition of total non-fasting serum cholesterol to routine screening of blood donors provides an opportunity for insights into cardiovascular risk amongst adolescents. This study shows not only that young adults can be identified who are at a higher risk for cardiovascular disease, but also that these individuals, if they are regular blood donors, can be followed over time to monitor changes in their risk.
P321
Follow-up of congenital heart disease
M Chave1, P Marques-Vidal2
1University of Lausanne, Lausanne, Switzerland
2University Hospital Centre Vaudois (CHUV), Department of Internal Medicine, Internal Medicine, Lausanne, Switzerland
Topic: Sports cardiology
Purpose:To assess the prevalence, characteristics, and quality of follow-up of CHD patients hospitalized in a university hospital.
Methods:Retrospective study using data on all patients with CHD who came to a university hospital in Switzerland (hospitalization or outpatient visits) between 2002 and 2014. We included all patients with an ICD-10 code from Q20 to Q26. We evaluated the characteristics of the entire patient population and the presence of follow-up (defined as 2 or more visits to the hospital) among Swiss patients only.
Results:We identified 1919 patients with CHD, of which 1039 were Swiss and 558 younger than 18. Most non-Swiss patients came from Africa through humanitarian programs and 81% were children. Non-Swiss patients presented with more severe CHD: 64.4% had malformation of cardiac septa (19.3% tetralogy of Fallot) versus 56.5% (3.2% tetralogy of Fallot) among Swiss patients; 7.1% of non-Swiss had malformations of aortic and mitral valves, versus 15% among Swiss patients (p<0.001). Among Swiss patients, only 228 (21.9%) underwent follow-up. Of those 228, 206 (90.4%) were followed according to guidelines (no interval greater than 3 years between visits). Multivariate analysis showed increasing age (p for trend<0.001) and less severe CHD to be negatively associated with follow-up, and living in a region close to the hospital to be positively associated with follow-up (see figure).
Conclusion:In Switzerland, prevalence and characteristics of CHD using hospital data can be severely biased if humanitarian patients are not excluded. Follow-up of CHD is not optimal, namely among adults and less severe forms of CHD.
Factors associated with follow-up
P322
Indirect economic loss from cardiovascular disease in the Ryazan region as one of the typical regions of Russia
E Philippov1, S Iakushin1
1Ryazan State Academician I.P. Pavlov Medical University, Ryazan, Russian Federation
Economic costs of CVD in the United States account for 1-3% of the gross domestic product. Indirect losses can be four times larger. In China, the direct damage from the CVD is estimated at 4% of gross national income ($ 40 billion). Over a 10-year period, the value of the world care for patients with high blood pressure amounted to $ 1 trillion.
Objective:To evaluate the inderect economic loss from CVD in the Ryazan region.
Methods:The calculation of economic losses as held on the basis of official statistics, and on the basis of data obtained in the MERIDIAN-RO study. The study included 1622 persons aged 25-64 years without diagnosed CHD (mean age - 43,4 ± 11,4 years, 46.2% male) randomly selected by sectional sample. Estimated the number of disabled people, their economic and social parameters, the number of sheets of disability and the main causes for the year preceding the survey.
Results:In calculating the indirect losses from CVD in the Ryazan region, it was found that they make up 4.9% of the gross regional product. Annual loss of profits in gross regional product of mortality was 24 585 250.8 euros, disability - 4560 915.9 euros, morbidity - 10 013 610.3 euros. Total economic losses from the CVD was 39 159 777.0 euros. More than half (54.7%) of all indirect losses from CVD were associated with mortality, the remaining losses are distributed approximately equally between disability (23%) and morbidity (22.3%).
Conclusion:Indirect economic losses from CVD in terms of per capita Ryazan region are very high, and in 2012 amounted to 4.9% of gross regional product. The greatest contribution to them brings mortality (54.7%), which entails the need to intensify preventive and therapeutic measures to reduce its level in the Ryazan region. It is necessary to improve the measurement and increase the number of parameters for the calculation of economic losses and assess the effectiveness of different prevention and treatment programs aimed at reducing mortality, disability and morbidity from CVD in the region.
P323
Risk factors prevalence in patients admitted at a cardiology ward: changes over a 10-year time.
A T Timoteo1, S A Rosa1, C Soares1, R C Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
Background:In patients with heart disease there is an increased prevalence of risk factors for coronary artery disease. Many efforts have been made in the past years to improve risk factor recognition, identification and treatment. We intended to study the prevalence of cardiovascular risk factors in a wide range of years in patients admitted at a cardiology ward.
Methods:Prospective study of all patients admitted electively at a single-centre Cardiology ward during a 10-year period for an elective procedure (coronary intervention or other). Patient data were collected in a dedicated database. We divided the patients in three groups according to year of admission: Group 1 (2004 – 2007, n=3536), Group 2 (2008 – 2011, n=5585) and Group 3 (2012-2014, n=4473). We studied the prevalence of hypertension, active smoking, hyperlipidemia, diabetes as well as previous history of coronary artery disease.
Results:We included 13594 patients in the study, mean age 64 ± 14 years, 60% males. Age at admission increased significantly across groups (62 ± 13, 63 ± 14 and 66 ± 13 years, respectively, p<0.001). There was also an increase in the proportion of male patients (58.8%, 59.4% and 61.9%, p=0.007). Body mass index was similar between groups (mean 27.5 Kg/m2 in all groups). Also a previous history of myocardial infarction (11.9%, 13.4%, 15.4%, p<0.001) and coronary revascularization (15.1%, 18.0%, 20.0%, p<0.001) increased. Both the prevalence of arterial hypertension (79.0%, 81.6%, 84.7%, p<0.001) and hyperlipidemia (73.7%, 75.7%, 80.7%, p<0.001) increased linearly. For smoking there was a small and transient decrease in Group 2 (10.9%, 7.7%, 10.7%, p<0.001) and for diabetes a small and also transient increase in Group 2 (34.7%, 44.5%, 34.9%, p<0.001).
Conclusions:Both hypertension and hyperlidemia increased, probably related with a better identification and treatment of cases. For smoking, a decrease was observed in 2008 – 2011, that is associated with important national campaigns and measures to reduce smoking, but with an undesirable increase in recent years, probably related with the financial crisis installed in more recent years. On the contrary, for diabetes, we managed to reduce he expected increase in prevelance in more recent years. Several events for the promotion of better lifestyles (both for nutrition and exercise) are probably related with this reduction, although no significant difference was found for body mass index.
P325
Gender specific analysis of cardiovascular risk factors prevalence in patients with premature coronary artery disease
R Pracon1, K Kryczka1, M Kruk1, G Broda1, E Ksiezycka1, M Demkow1, B Lubiszewska1
1National Institute of Cardiology, Warsaw, Poland
Topic: Sports cardiology
Purpose:The incidence of premature coronary artery disease (CAD) is increasing, yet data on risk factors for developing CAD prematurely is scarce. Knowledge of risk factors is needed for estimation of cardiovascular risk as well as assessment of disease probability and effective employment of preventive measures in this young population of patients. The current case-control, gender specific study reports the relationship between traditional cardiovascular risk factors and occurrence of premature CAD.
Methods:Consecutive female (age <55yrs) and male (age<45yrs ) patients with CAD defined as presence of at least one major epicardial coronary artery narrowing of =50% on coronary angiography or troponin-positive acute coronary syndrome were enrolled. Age- and sex-matched, apparently healthy control subjects were concurrently recruited. Both cases and controls underwent dedicated questionnaires, physical examination, and blood laboratory testing in a single central laboratory in search for cardiovascular risk factors. Adjusted odds ratios (OR) were calculated and interaction analysis of modifying effect of gender on risk factors associations with CAD was performed. P-value of =0.05 was considered significant.
Results:The cohort included 670 women (W) (age 49.5±4.2yrs), and 530 men (M) (age 39.4±4.5yrs). Smoking (OR for W 5.77; and M 3.52), parental history (OR for W 1.78; and M 1.21 ), physical activity (OR for W 0.60; and M 0.26), hypercholesterolemia (OR for W 1.73; and M 3.04), hypertension (OR for W 2.78; and M 1.59), diabetes (OR for W 3.81; and M 2.12), obesity (OR for W 1.76; and M 2.88) were all associated with premature CAD (p<0.05 for all). By interaction analysis smoking (p=0.07) and diabetes (p=0.09) tended to be stronger correlates of the disease in women, whereas hypercholesterolemia (p=0.05), physical activity (p<0.05), and obesity (p=0.05) were stronger predictors of premature CAD in men.
Conclusions:All seven traditional cardiovascular risk factors studied were related to the incidence of premature coronary artery disease with trends for stronger associations of smoking and diabetes in women and stronger associations of hypercholesterolemia, physical activity, and obesity in men.
P326
Relationships of traditional risk factors, calculated cardiovascular risk, carotid intima-media thickness and plaque
N Katamadze1, L Berstein1, Y Grishkin1
1North-western state medical university named after I.I.Mechnikov , Saint-Petersburg, Russian Federation
Topic: Sports cardiology
Purpose:Significant variance in carotid intima-media thickness (cIMT) and prevalence of atherosclerotic plaque was reported in subjects free of clinical cardiovascular disease with equal calculated risk. We investigated the relationships between the cardiovascular risk factors (RF), cardiovascular risk calculated by the standard scoring algorithm, cIMT and carotid plaque.
Methods:In 217 pts aged 54,3±8 years with =1 traditional cardiovascular RF and no evidence of atherosclerotic cardiovascular disease risk estimation was performed using the SCORE chart. All pts underwent ultrasound study of 3 carotid segments which included assessment of ?MT and the presence of atherosclerotic plaques with calculation of TPA as the sum of plaques cross-sectional areas.
Results:184 (85%) of pts had low or moderate risk (SCORE <5%). The cIMT values were 0,8±0,15 mm in common carotid artery (CCA), 1,29±0,5 mm in bifurcation and 0,82±0,4 mm in internal carotid artery (ICA). Carotid plaques were present in 83 (38%) pts, including 58 (32%) pts with SCORE <5%; median TPA was 0 [0,16] cm2. The level of risk by SCORE was positively associated with cIMT in all 3 carotid sites and TPA (?0,04, 95% CI 0,04-0,05 for CCA; 0,07, 95% CI, 0,04-0,09 for BIF; 0,03, 95% CI 0,02-0,04 for ICA; 0,04, 95% CI 0,03-0,05 for TPA, respectively, p<0,0001 for all). However, the impact of specific RF on cIMT in various segments was unequal. Higher CCA cIMT was found in subjects with hypertension (?0,06 mm, 95% CI 0,008-0,11, p=0,02) and dyslipidemia (?0,07 mm, 95% CI 0,01-0,13, p=0,01). Higher cIMT in bifurcation was associated with smoking (?0,2 mm, 95% CI 0,12-0,36, p<0,0001) and heredity (?0,16 mm, 95% CI 0,01-0,3, p=0,03). cIMT in ICA was related to hypertension (?0,09 mm, 95% CI 0,03-0,15, p=0,006) and smoking (0,07 mm, 95% CI 0,01-0,12, p=0,01). In multivariable regression models, age, pack-years of smoking, diastolic blood pressure, non-HDL cholesterol, body mass index were identified as independent predictors of cIMT and plaque. However, the degree of carotid cIMT and TPA variability explained by cardiovascular RF was modest - 29%, 19,1% and 9,4% for cIMT in CCA, bifurcation and ICA, respectively, and 24% for TPA.
Conclusions:The extent of carotid atherosclerosis is parallel to cardiovascular risk as calculated by SCORE algorithm, however atherosclerotic plaque is found in 1/3 of low- and moderate-risk pts. Effect of traditional RF on carotid arteries is segment-specific. Common RF explain only up to 29% of carotid atherosclerosis variability with a maximum impact on CCA cIMT and TPA.
P327
Prognostic impact of LDL-cholesterol levels on a real life population of patients with stable coronary artery disease.
A T Timoteo1, S A Rosa1, C Soares1, R Cruz Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
Background:LDL-cholesterol (LDL-C) levels showed a direct relationship with the occurrence of cardiovascular events in previous randomised clinical trials both in the general population and in patients with coronary artery disease (CAD). We sought to evaluate if in a "real life" population with CAD this relationship is also significant and direct.
Methods:Study in patients admitted for coronary angiography due to stable angina and with significant CAD (= 70% stenosis in any coronary vessel or 50% for left main). We evaluated demographic, risk factors, previous cardiac history, medication and laboratorial variables on admission. Patients were divided in three groups according to LDL-C levels on admission (< 70 mg/dL; 70-120 mg/dL and =120 mg/dL). Major Adverse Cardiac Events (MACE) - occurrence of death, non-fatal myocardial infarction or revascularization in a 3-year follow-up.
Results:We include in the analysis 2203 patients with documented CAD, with a mean age of 67 ± 9 years, 74% males. Patients with low LDL-C were less frequently smokers but more hypertensive, diabetic and with more previous history of CAD (myocardial infarction / coronary revascularization). They were also more frequently on statin therapy. The inverse was observed in patients with high LDL-C. During the 3-year follow-up there were MACE in 4.9% of the patients (death in 3.8%), with the highest incidence in the group with low HDL-C, followed by the intermediate group and lowest in the high LDL-C group (6.5%, 5.7% and 3.3%, respectively, Log-rank, p=0.030). By logistic regression analysis, MACE predictors were the presence of diabetes and renal insufficiency. With the intermediate group of LDL-C as the reference group, the high LDL-C level group was associated with a better prognosis and the low level group had the same impact. In multivariate analysis adjusted for the presence of diabetes, renal function and statin use, the presence of high LDL-C levels remained as an independent predictor of better outcome (OR 0.60, 95% CI 0.38 – 0.97, p=0.035). Low LDL-C wasn't significantly different from the intermediate group in outcome prediction (OR 1.10, 95% CI 0.61 – 1.98, p=0.756).
Conclusions:LDL-C had a paradoxical impact in the ocurrence of MACE in patients with stable CAD on long-term follow-up, independently of the presence of diabetes or renal failure, as well as the use of statins. The better baseline clinical profile of the high LDL-C group might explain the results, but multivariate analysis corrected this bias. An explanation must be sough in subsequent studies, particularly if other registries confirm our findings.
P328
Motor ability and cardiovascular risk stratification in children and adolescents with congenital heart disease
J Mueller1, M Aberl2, D Gaser2, R Oberhoffer2, P Ewert3
1German Heart Center and Institute of Preventive Pediatrics, Technische Universit?M?, Munich, Germany
2Institute of Preventive Pediatrics, Technische Universit?M?, Munich, Germany
3German Heart Center, Hospital rechts der Isar at the Technical University of Munich, Munich, Germany
Objective:Several studies have shown that patients with congenital heart diseases (CHD) have a higher cardiovascular risk, reduced exercise capacity and impaired motor abilities. Primary prevention of those risk factors starts already in childhood. We therefore launched a prospective study in children and adolescents with CHD, evaluating cardiovascular risk factors like blood pressure, arterial stiffness, intima-media wall thickness and waist-to-hip ratio. Moreover, we assessed motor ability with the Fitnessgram® and health-related quality of life with the KINDL® questionnaire.
Patients and Methods:From August 2014 to November 2014, we prospectively examined 146 children with various CHD (12.6 ± 3.2 years, 47 girls) for their cardiovascular risk factors (body weight, body height, waist and hip circumference, systolic and diastolic blood pressure) and their motor skills. Reference value for motor skills were obtained from 840 healthy children in the project "Sternstunden" in Bavaria from 2011 to 2013. Normative Values for blood pressure and body mass index (BMI) were obtained from the national health report of the Robert Koch Institute from 2013.
Results:Children with CHD had significantly higher systolic blood pressures (z-score: +0.92; p<.001) and tended to higher diastolic blood pressures (z-score: +0.21; p=.072) compared to actual German reference values. Their waist-to-hip ratio was also slightly increased (z-score: +0.30; p<.001) Compared to the reference group of healthy children, their motor skills were impaired with regard to curl-ups (CHD: 17.2 vs Healthy: 23.5, p<.001), trunk lift (CHD: 19.2cm vs Healthy: 24.8cm, p<.001, Sit and Reach (CHD: -5.2cm vs Healthy: -0.2cm, p<.001) and Shoulder Stretch (CHD: -11.1cm vs Healthy: -6.9cm, p<.001) Conclusions:Current children with CHD still have impaired motor skills and an increased cardiovascular risk for cardiovascular diseases in comparison to healthy peers. Strategies for primary prevention are needed to overcome those burdens in this more and more aging cohort.
P330
Impact of statin therapy in patients with low LDL-cholesterol and acute coronary syndrome.
A T Timoteo1, T Pereira Silva1, M L Papoila2, S A Rosa1, M L Ferreira1, R Cruz Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
2New University of Lisbon, Faculty of Medical Sciences, Lisbon, Portugal
Background:Statins showed a significant prognostic impact in patients with Acute Coronary Syndromes (ACS) in randomised clinical trials and are one of the most prescribed drugs in ACS registries. In real life populations, the beneficial impact of statins is usually less significant when adjusted for other variables with clinical impact. We sought to evaluate in a real life population of patients with ACS the prognostic impact of statin therapy, particularly in patients with low LDL-cholesterol (LDL-C) on admission.
Methods:Consecutive patients included in a single centre registry of ACS. We evaluated demographic, risk factors, previous cardiac history, laboratorial and treatment variables. Primary endpoint was the occurrence of all-cause mortality at one-year follow-up. The impact on outcome was studied with Cox proportional hazards (PH) regression analysis. We used Schoenfeld and Martingale residuals to assess PH assumption and to find cutpoints for some of the continuous predictors.
Results:We included 1670 patients, with a mean age of 64 ± 13 years, 69% males. In our population, 56% presented with ST-segment elevation ACS and 23.1% were on statin therapy at admission. After admission, 92.9% were treated with statin. In-hospital mortality was 5.2% and 8.9% at one-year follow-up. Only 7.8% had a basal LDL-C = 70 mg/dL. They were more frequently on statins before admission (34.6 vs. 22.1%) and less after admission (86.9 vs. 93.4%). Patients with low LDL-C showed a worst outcome (one-year mortality 21.5% vs. 7.9%, Log-rank, p<0.001) that might be explained by a worst baseline clinical profile. In fact, after adjustment for other variables, LDL-C remains as an independent predictor of mortality (HR 1.72, 95% CI 1.12 – 2.66, p=0.014). By univariate analysis, statin use after admission is a protective factor against mortality (HR 0.57, 95% CI 0.35 – 0.95, p=0.031) but after multivariate analysis it is no longer an independent predictor of outcome (HR 1.04, 95% CI 0.62 – 1.75, p=0.879). Beta-blockers remain as an independent protector against mortality (HR 0.44, 95% CI 0.31 – 0.62, p<0.001). In a separate analysis, in patients with high LDL-C, statin therapy isn't a predictor of outcome (HR 1.07, 95% CI 0.59 – 1.93, p=0.834), as well as in the group with low LDL-C (HR 0.84, 95% CI 0.27 – 2.60, p=0.766).
Conclusions:Although statin therapy is widely used after ACS, no benefit from this therapy was observed in a real-life population with ACS, opposite to what was found for BB. These results are independent of admission levels of LDL-C. These findings should be confirmed in larger registries.
P331
Risk of cardiovascular disease in patients with osteoarthritis: Results from the MUST-Heart study
S Rollefstad1, E Ikdahl1, IK Eeg1, A Mathiessen2, N Oesteraas2, B Slatkowsky-Christensen2, HB Hammer2, TK Kvien2, IK Haugen2, AG Semb1
1Diakonhjemmet Hospital, Preventive Cardio-Rheuma Clinic, Department of Rheumatology, Oslo, Norway
2Diakonhjemmet Hospital, Department of Rheumatology, Oslo, Norway
Topic: Sports cardiology
Purpose:Controversies exist regarding whether patients with osteoarthritis (OA) have an increased risk of cardiovascular (CV) disease. Our aim was to evaluate the CV risk and presence of established CV disease in a population-based OA cohort.
Methods:The Musculoskeletal pain in Ullensaker STudy (MUST) is a cross-sectional investigation comprising a thorough clinical examination, recording of CV risk factors in addition to radiographic evaluation of hands, hips and knees of persons with self-reported OA. Of the 604 persons examined, 438 fulfilled the American College of Rheumatology classification criteria for OA in the hand, knee and/or hip joints. CV risk was calculated by the Systematic Coronary Risk Evaluation (SCORE) algorithm for persons without CV disease, not using lipid lowering and/or antihypertensive medication (OA n=200 and non-OA n=87). An estimated CV risk <5% for experiencing a fatal myocardial infarction coming 10 years is defined as low to medium risk, while =5% is the cut off for initiation of CV preventive pharmacotherapy.
Results:The median CV risk for patients with OA [1.40 (IQR 0.65, 2.92)] was significantly higher compared to non-OA [0.99 (IQR 0.52, 1.92)] (p=0.02). The difference in the CV risk was related to higher age (p<0.001), but not to total cholesterol (p=0.07), systolic blood pressure (p=0.13) or to the OA diagnosis. Only 17/200 (8.5%) of the OA patients and 3/87 (3.4%) of the non-OA persons had a CV risk =5% (p=0.12). The presence of established CV disease was comparable for those with (n=72/438, 16.8%) and without OA (n=34/166, 21.1%) (p=0.23). Inflammatory biomarkers were in the normal range for the whole study population, with no difference between OA and non-OA (p=0.30 and 0.10).
Conclusions:Inhabitants with OA in a Norwegian municipality had an overall low risk of CV disease and did not have higher prevalence of established CV disease compared to non-OA.
P333
Electrical instability and left ventricle remodelling in patients with stable ischemic heart disease and anaemia
M Krestjyaninov1, OV Shameeva2, RH Gimaev3, VA Razin3, H Halaph4
1Ulyanovsk Regional Hospital of War Veterans, Functional diagnostics, Ulyanovsk, Russian Federation
2Ulyanovsk Regional Hospital of War Veterans, Ulyanovsk, Russian Federation
3Ulyanovsk State University, Ulyanovsk, Russian Federation
4Ulyanovsk Regional Hospital of War Veterans, Arterial Hypertension Centre, Ulyanovsk, Russian Federation
In the 21 century the number of people suffering from ischemic heart disease (IHD) continues to increase in the world. In this regard great attention is paid to study the factors contributing for IHD. Experimental and clinical studies have shown that ischemic or hypertrophied myocardium is very sensitive for a slight decreasing of haemoglobin which is expressed in more severe left ventricle (LV) remodelling and more frequent development of arrhythmias. The purpose of the study is to evaluate relations between LV remodelling, QT dispersion (marker of myocardium electrical instability) and anaemia in patients with stable IHD. Were examined 43 patients (the mean age 52 (9) years) with IHD 2-3 functional class and anaemia 1-2 grade and 22 patients with IHD without anaemia (mean age 45 (10) years). In all patients were performed ECG in 12 standard leads, evaluation of QT interval duration, corrected dispersion of QT interval (QTdc), EchoCG (ASE/EAE recommendations 2005) and also were evaluated total haemoglobin (Hb), erythrocytes in 1 liter (Er). Statistical significance was defined at the level of methods for p <0,05. As it can be seen from the table in anaemic patients values of QT interval duration, wall thickness and LV mass were higher then in patients without anaemia. Correlation analysis showed relations between QTdc and IVSd (R=0.37; p=0.026) and between QTdc and Hb (R=-0.32; p=0.046). Thus, the results of the study show that in patients with ICD anaemia can be not only predictor of LV remodelling but also be predictor of electrical instability of myocardium.
Results are shown as M (SD) for parameters with normal distribution and as Me (q25; q75) for parameters with distribution different from normal.
Parameters
Anaemic patients
Patients without anaemia
p
n=43
n=22
Hb, g/l
106 (11)
142 (17)
<0.001
IVSd, mm
10.8 (1.7)
9.8 (1.5)
0.027
PWTd, mm
10.6 (9.4; 11.7)
9.8 (8.3; 11.1)
0.139
LV mass, g
206 (65.5)
169 (42)
0.039
LV mass/BSA, g/m²
103.2 (83; 125)
91.3 (18)
0.091
QT, ms
430 (407; 450)
410 (35)
0.035
QTdc, ms
52 (32; 99)
60 (36; 84)
0.8
P335
Framingham Risk Score versus HeartScore as a stratification tool for the prevention of cardiovascular diseases. Do they differ when aplied to a specific employee's population?
DENISE Cortes1, EDUARD Costa Pinto1, MARCIO Carvalho1, ANTONI Lucas Da Nobrega2, ANA Pimentel Mendonca1, ADRIAN Arantes1, ROSANG Oliveira1
1Funda? de Assist?ia e Previd?ia Social do BNDES - FAPES, Rio de Janeiro, Brazil
2Medicina e Ci?ia, Rio de Janeiro, Brazil
Introduction:The early diagnosis of coronary artery disease and the identification and treatment of modifiable risk factors to atherosclerosis constitute key points in the field of Primary Care Medicine. Risk assessment tools like the Framingham (F) and HeartScore (HS) are widely used to predict a person's chance of having an adverse cardiac event in the next 10 years. The purpose of this study was to determine whether there is a significant difference between (F) and (HS) results when these risk assessment tools are simultaneously applied to the employees' of specific public company.
Methods:Employees of a Brazilian public bank were enrolled in a institutional program dedicated to the prevention of cardiovascular diseases. Workers were stratified in two different clinical groups: Low Risk and Non Low Risk by two well known heart risk assessment tools, the (F) and the (HS). This survey took place in May 2013.
Results:Two hundred seventy eight employees were enrolled by this study. There were 176 men (63.3%, mean age 42y, SD 10y) and 102 women (26.7%, mean age 45y, SD 10y). Two hundred fifteen patients (77 %) were considered as low risk individuals by the (F) score. Sixty three employees (23%) were classified as (F) non low risk workers. An intermediate cardiovascular risk was observed in 41 of them (15% of total) and a high cardiovascular risk in the remaining 22 (8%).The mean (F) score of the 278 patients was 6.71% (SD 6.86), showing a population of low average cardiovascular risk. Two hundred and five workers (73.7%) were stratified as non low risk patients by (HS).They could be distributed in three groups: intermediate 188 (67 % of the whole population), high 13 (4.5 %) and very high 4 (1.5%) cardiovascular risk. Seventy three (27%) of all employees were considered of low risk by the (HS) survey. The mean (HS) in the whole population was 1.5 (SD 1.8) classifying them as an intermediate cardiovascular risk. Nevertheless, 149 patients (53.5%) had their low (F) risk upgraded to a higher risk (HS)classification. On the other hand, 14 patients (5 %) that were classified as moderate or high risk by (F) criteria had their risk levels downgraded by the (HS). These differences between (F) and (HS) reached statistical significance (p < 0.01).
Conclusion:In our small study population, (F) and (HS) results disagreed regarding the cardiovascular risk classification of at least 50% of the enrolled patients. This inconsistency was not observed in foreign medical publications. We point out, however, to the inexistence of other Brazilian studies dealing with this subject.
P336
Differences in lifestyle habits between patients with low, midle and high risk for cardiovascular diseases
K Kranjcevic1, V Bralic Lang1, B Bergman Markovic2, D Vrdoljak3, J Vucak4, D Ivezic Lalic5
1Health Center Zagreb West, General practice office, Zagreb, Croatia
2University of Zagreb School of Medicine, Zagreb, Croatia
3University of Split, Split, Croatia
4General practice office, Suko?an, Croatia
5General practice office, Kutina, Croatia
Topic: Sports cardiology
Purpose:to compare the lyfestile habits (alcohol consumption, smoking and physical activity) in patients with low, midle and high risk for cardiovascular diseses.
Methods:Data from a multicentric, prospective and intervention study titled Cardiovascular Risk and Intervention Study In Croatia – family medicine (CRISIC-fm) from 2010 was used. Fifty-nine family doctors from all over Croatia participated in the study and every doctor including up to 55 patients aged 40 to 69, who had visited their office for any reason from May to July 2010 and signed the informed consent to participate. Ten-year risk of fatal cardiovascular disease (CVD) was calculated using the Systematic Coronary Risk Evaluation (SCORE) chart for high-risk countries. The criteria listed in ESC Guidelines were used to identify low, moderate, high and very high risk groups for cardiovascular diseaseS. Alcohol consumption, smoking and physical activity were recorded and compared between the moderate and high risk groups. Excessive alcohol consumption was defined with =20 g of ethanol per day for men and =10 g for women. Physical activity was considered as sedentary, mild, moderate and intensive. All participants who smoked or had stopped smoking within a year before the beginning of the study were considered to be smokers. Descriptive statistical methods were used to describe sample characteristics and ? test was used to compare the correlation between categorical variables. Statistical program SPSS for Windows (11.5, SPSS Inc., Chicago, Illinois, 2002) was used for data processing.
Results:Fifty-nine family medicine doctors included 1957 participants (47.7% men and 52.3% women) aged 40 to 69, out of which 249 (12.7%) were categorized as low, 1059 (54.1%) as moderate, 345 (17.6%) as high and 304 (15.5%) as very high risk subjects for fatal CVD. Difference between the moderate and high risk groups was found in the presence of older age (P< 0.001), male sex (P< 0.001) and excessive alcohol consumption (P< 0.001) in the high risk group. Sedentary lifestyle was found more offten in high and very high CVD risk group and moderate physical activity in moderate and low CVD risk group (P< 0.001). There was no difference in smoking between examined groups (P= 0.079).
Conclusion:Unhealthy lifestyle habits are strongly associated with increased risk for cardiovascular diseases. Public health and family doctors need to improve the adoption of healthy lifestyles habits in population, especially in high risk patients for CVD.
P337
Ankle brachial index: validation of tools to promote their determination
GO Perea1, M Corneli1, G De Bono1, F Belcastro1, R Henquin1, R Ronderos1
1Instituto Cardiovascular de Buenos Aires, Ciudad Aut??a de Buenos Aires, Argentina
Objective:The ankle-brachial index (ABI) is a tool for the diagnosis and management of peripheral arterial disease; and a marker of atherosclerosis. The objective of this study is to determine the correlation of ABI measured by the Doppler pocket in relation to registered ABI at the echo Doppler vascular laboratory.
Methods:We evaluated the ABI in patients referred to the echo Doppler vascular laboratory for an arterial lower limb study between March 2014 to August 2014. ABI was assessed by Doppler pocket and then by pulsed Doppler at the echo vascular laboratory Results:250 patients, 66% were men, mean age 65 years were included. The mean Doppler resting ABI with pocket Doppler was 1.07 and the ABI registered in the vascular laboratory was 1.09. The Bland-Altman method was used to demonstrate the correlation between the two measurements. The mean difference between the measurements of the two methods was -0.004 in the right limb (p=0.06) and in left limb of 0.001 (p = 0.7)(Figure1).
Conclusions:Our study demonstrates that ABI measurements with the pocket Doppler and pulsed Doppler at the vascular laboratory are consistent and can be replaced with each other. These results give us another chance to go in search not only of peripheral arterial disease but a great prognostic marker for cardiovascular disease.
Figure 1. Bland-Altman plot.
P338
Impact of asymptomatic atherosclerosis on cardiovascular risk stratification and consequences for lipid lowering prevention in patients with inflammatory joint diseases
A G Semb1, S Rollefstad1, E Ikdahl1, J Hisdal2, TK Kvien1, IC Olsen1
1Diakonhjemmet Hospital, Oslo, Norway
2Oslo University Hospital, Aker, Oslo Vascular Center, Oslo, Norway
Background/Objectives:Patients with carotid plaque (CP) should receive intensive lipid lowering treatment (LLT). Due to the high frequency of CP in patients with inflammatory joint diseases (IJD), we evaluated the impact of CP on cardiovascular disease (CVD) risk stratification and consequences for lipid lowering prevention in patients with IJD.
Methods:CVD risk stratification in IJD patients (n= 334) was performed using the systematic coronary risk evaluation (SCORE) algorithm, in addition to ultrasound of the carotid arteries. Cross-tabulations, Chi2 and ROC curves were used to calculate sensitivity and specificity for the SCORE algorithm. The ROC curves closest point (0.1) and 80 % sensitivity were used for optimizing CV risk classification.
Results:Two hundred and forty nine patients with IJD had a SCORE <5 %, indicating no need for LLT. However, 98 (39.4 %) of these patients had CP and should receive intensive LLT. In patients with a calculated SCORE >5 % & <10 % + LDL>2.5 mmol/L (n=58), where moderate LLT is recommended, 38 (65.5 %) patients had CP and should therefore be classified to receive intensive LLT. Thus, patients with CP who were wrongly classified to receive no (low+moderate CVD risk) or only moderate (high CVD risk) instead of intensive LLT, was 39.4 % and 65.5 %, respectively. Taken together, 136/307 (44.3 %) of these patients would receive inadequate LLT (Table). The sensitivity (correctly classifying patients with IJD + CP): 0.39/specificity: 0.83. Optimizing SCORE cut off for very high risk, by area under the ROC curves' closest point (0, 1) (resulted in SCORE 2%) or 80% sensitivity (resulted in SCORE 1.6%) did not improve correct CVD risk stratification in congruence with recommended standards.
Conclusion:Carotid ultrasound contributes to optimized CVD risk classification with consequences for CVD preventive LLT in patients with IJD.
P340
Strategies for increasing the adherence to regular physical activity sessions
S S Busnatu1, M Raileanu1, C Sinescu1
1University of Medicine and Pharmacy Carol Davila, Cardiology, Bucharest, Romania
Topic: Sports cardiology
Purpose:Efficient prevention of cardiovascular disease can produce great benefits for patients and for the health systems. It is well known that regular physical activity represents one of the few protective factors in the primary and secondary prevention of cardiovascular diseases. A key aspect for better optimization of the prevention programs is to find a solution for increasing the adherence to regular physical activity.
Methods:This was an observational cohort study conducted on 108 patients, age 40-70 years with a stable cardiovascular condition. The first group consisted of 52 patients that performed a one week lifestyle intervention program which took place during August. Patients received a vegetarian personalized nutritional plan, medical educational lectures and 5 physical activity sessions. The second group of patients have been randomly selected from the patients that came during August into the Cardiology Department for medical checkup. During the checkup this group has been informed on the importance of performing regular physical activity and on practical ways of performing it in order to improve the cardiovascular fitness. They also received nutritional counseling for reducing their cardiovascular risk. The primary endpoint of the study was to compare the adherence at performing regular physical activity, in accordance with the minimal European recommendations, in both groups after two months.
Results:Initially, from the first group only 21% performed the minimal physical activity recommended by the European Society of Cardiology. After two months, from ending the one week intervention program, 74% still kept performing the minimal weekly recommended physical activity. From the second group, that performed the medical checkup in the hospital, initially, only 12% performed the minimal physical activity recommendations with a slight increase to 21% after 2 months period. Chi Square Test (p<0.01) showed a greater adherence in performing physical activity for patients that took part at the one week intervention, comparing to those that received indications from the hospital. It has also been noticed that patients under 50 years had a higher increase in performing regular physical activity(p<0.01) Conclusions:Short term interventions on health education, nutritional counseling and physical activity training seem to be more efficient than simple oral indications in order to increase the adherence to the current physical activity recommendations. This type of events have the potential to improve prevention programs.
Are rollercoasters heart stoppingly fun ? ECG monitoring during high speed and high G-force theme park rides in healthy children
GE Pieles1, VL Husk2, T Blackwell1, D Wilson1, CA Williams3, G Stuart1
1Bristol Heart Institute, Congenital Heart Disease, Bristol, United Kingdom
2University of Bristol, Bristol, United Kingdom
3University of Exeter, Children's Health & Exercise Research Centre (CHERC), Exeter, United Kingdom
Topic: Sports cardiology
Purpose:Theme park rides induce catecholamine release and exert acceleration and high G-forces, which may induce pathological arrhythmias as shown in previous aviation studies. Whilst these G-forces are significantly higher and for longer than those at theme parks, arrhythmia induction during rollercoaster rides in children has not been previously investigated. This pilot study set out to investigate the effect of G-forces and acceleration during rollercoasters on heart rhythm in healthy children.
Methods:Twenty healthy volunteers (9 male) aged 11 – 15 (mean 13.3±1.4) were recruited. Prior to study commencement each participant had a normal 12-lead ECG, mean resting HR of 80±9.6 b?153;min-1. At the theme park participants wore 2-lead ECG monitors, which recorded continuously from 5min before the rollercoaster (mean ride length 82±36s) until 20min after.
Results:Overall, total ECG recording time was 13h 20min and 4 rides were assessed. Maximum G-force was 5G (mean 4.7±0.2G). Maximum speed was 130 km?153;h-1 (mean 92±48.2 km?153;h-1). The highest mean HR (165±21.9 b?153;min-1) was observed on Ride 1 which had the lowest G-force (4.5G), but one of the highest speeds (100 km?153;h-1). The highest G-force ride (5G, Ride 4), with a lower speed, showed heart rates 24 b?153;min-1 slower than Ride 1 [95% CI 9/40, p<0.004]. Nineteen out of twenty participants experienced sinus tachycardia (HR >100 b?153;min-1), with 434 episodes of tachycardia recorded, but no pathological arrhythmias were found. Anticipatory tachycardia (mean HR of 126±15 b?153;min-1) within 5min before the ride was frequently observed. During rides the mean tachycardia was 160±19 b?153;min-1, which was 97.5% greater than baseline HR. Recovery HR within 20min after the ride (mean HR 124±17 b?153;min-1) was 56% greater than resting HR.
Conclusions:The recorded ECG data showed there is significant sinus tachycardia in response to anticipation, stress, catecholamine release and G-forces exerted by rollercoasters. This study will serve as control data to investigate heart rhythms during rollercoaster rides in children with congenital heart disease. Overall it provides reassuring data that G-forces experienced on rollercoasters do not illicit pathological arrhythmias in healthy children.
P342
Differences in determining the incidence of pathological ECG athlete - level differences and reasons
V Pavlov1, AV Pachina1, VV Deev1, VA Badtieva1, VV Nikolaev1
1Moscow scientific and practical center medical reabilitation and sport medicine - Sportmed Clinic, Moscow, Russian Federation
ECG is one of the most important methods of screening examinations athlete. According to data an athlete ECG analysis may show changes that are interpreted as pathological. However, the picture is variable ECG athlete so that even the current recommendations and trying to improve them have not yet given complete clarity. The goal of the study to compare our findings on pathological ECG professional athletes with already existing in the world.
Materials and methods:The study included 5434 person professionally involved in soccer at a high level and have experience of sports as a professional at least five years.
Results and discussion:Among the players a high level of life-threatening ECG changes are relatively rare - they were observed, according to our data, 12 athletes (0,22%). However, the disturbances of the electrical activity of the heart, leading to the need for monitoring and control, recorded at an average of 60 players (1,1%) cases. This is significantly different with some data experts in sports cardiology, examine the population of athletes at different levels. Thus, in the current literature on the ECG athlete in Europe, discusses the importance of pathological ECG athlete about 10% - slightly less than in women, and little more than that of men. This may be due to the fact that we examined athletes of the highest level, and associated 'natural' selection of athletes at the early stages of their careers, as well as other reasons. Thus, the diagnosis of the anterior branch of the blockade of left bundle branch block is based on a statement of fact a sharp left axis deviation. Often, this conclusion is wrong, as is often the position of the electrical axis of the heart (EOS) in the frontal plane can not be determined, because of its significant deviations in other planes due to hyperactivity of the right heart. We also note the ventricular pre-excitation syndromes hyperdiagnosis, especially in children and adolescents with normal acceleration AV conduction and the presence waves on the ascending portion of the complex QRS, which is a consequence of physiological athlete incomplete the right branch block. The presence of negative T waves in the right precordial leads may be due to physiological athlete for incomplete right bundle branch block, rather than a manifestation of pathological remodeling.
Conclusions:1. The differences of the incidence of pathological ECG athlete are often very significant. 2. They are associated with different categories athletes included in the study, and different qualifications and experience of practitioners in the field of sports cardiology
P344
New shirt-based electrocardiogram device for cardiac screening and performance status in professional soccer players: comparative study with treadmill ergospirometry
O Fabregat Andres1, A Munoz-Macho2, S Pina-Buded2, A Calvente-Nomdedeu2, G Adell-Beltran2, H Uso2, S Morell1
1University General Hospital of Valencia, Valencia, Spain
2Villarreal CF SAD, Medical Service, Villarreal, Spain
Topic: Sports cardiology
Purpose:Prevention of cardiac events during practice of competitive sports has emerged as a fundamental task of sports medicine. New technologies with remote wireless monitoring systems integrated into clothing could facilitate the screening of heart disease in collective sports. Nuubo's dynamic ECG is a new three-lead ECG wireless monitoring system that incorporates an electronic device attached to a biomedical shirt that transmits ECG signal via Bluetooth®. Our aim was to evaluate the feasibility of Nuubo system during a field stress test carried out by soccer players, comparing results with treadmill ergospirometry as test reference. Methods:19 male professional soccer players of a Spanish second division B team (19.2±1.6 years) were studied. Wireless electrocardiographic monitoring during a Yo-Yo intermittent recovery test level 1 in soccer field was firstly performed. Subsequently, in a period no longer than 4 weeks, each player underwent cardiopulmonary exercise testing in hospital. Results:During Yo-Yo test, ECG signal was adequate and interpretable in 16 players (84.2%). In other 3 players, ECG artefacts did not allow a proper analysis of the signal. Estimation of maximum oxygen consumption was comparable between two exercise tests (VO2 max 53.3±2.4 vs. 53.7±3.0 mL/kg/min for Yo-Yo test and ergometry respectively; intra-class correlation coefficient 0.84 [0.63-0.93] p<0.001). No ventricular extrasystoles or other arrhythmias were detected in any player during both exercise tests (Table 1). Conclusions:The use of Nuubo's technology allows an accurate three-lead electrocardiographic recording and estimation of reliable performance variables during exercise testing in field, and provides a new perspective to cardiac remote monitoring in team sports as soccer.
QUANTITATIVE VARIABLES
Intra.class correlation coefficient (95% CI)
p value
Baseline heart rate
0.95 (0.87-0.97)
<0.001
Peak heart rate
0.61 (0.21-0.83)
0.003
VO2 max
0.84 (0.63-0.93)
<0.001
QUALITATIVE VARIABLES
Kappa Index
p value
Adequate baseline ECG
1
<0.001
Adequate peak ECG
0.45
0.018
Atrial or ventricular premature complexes
1
<0.001
P346
Electrocardiographic predictors of increased left ventricular mass in elite athletes
G Finocchiaro1, H Dhutia1, E San Damaso1, A Malhotra1, M Papadakis1, S Sharma1
1St George's University of London, London, United Kingdom
Background:and aims: Studies in sedentary cohorts have demonstrated a poor correlation between electrocardiographic (ECG) criteria for left ventricular hypertrophy (LVH) and left ventricular mass (LVM). Despite the high prevalence of ECG criteria for LVH in athletes, limited information is available about their correlation with LVM. The aim of this study was to assess the value of a number of ECG parameters in predicting increased LV mass in elite athletes.
Methods:We reviewed 340 consecutive athletes (mean age 20±5 years, 55% males, 88% Caucasian), who underwent ECG and echocardiogram as part of their pre-participation cardiac evaluation. Left ventricular mass was calculated using the American Society of Echocardiography (ASE) formula and indexed for body surface area. Cut-off for increased LVM was 115 g/m2 in males and 95 g/m2 in females.
Results:The table depicts the ECG characteristics. An increased LVM was observed in 63 (19%) athletes. Although the prevalence of increased LVM was similar in both genders (18% males vs. 20% females, p=0.59), the demographic and ECG predictors were gender specific. In male athletes, age >22 years (OR: 3.52, 95% CI: 1.53 to 8.16, p=0.003), QRS duration >100 msec (OR: 3.70, 95% CI 1.58 to 8.66, p=0.002) and positive Sokolov-Lyon (SL) criterion for LVH (OR: 2.99, 95% CI 1.27 to 7.01, p=0.011), were independent predictors for increased LVM. The combination of these parameters had a sensitivity of 66% and a specificity of 80% and showed an area under the curve of 0.75; 95% CI=0.68-0.81, p<0.001. In female athletes, only voltage criterion for left atrial enlargement was independently associated with increased LVM (OR: 11.67, 95% CI 1.79 to 75.66, p=0.01) with a sensitivity of 55% and specificity 73%.
Conclusions:Electrocardiographic indices of increased LVM are gender specific in elite athletes. All ECG indices are of limited value in female athletes, while the combination of QRS duration >100msec and positive SL voltage criterion demonstrate reasonable predictive value in adult, male athletes.
P348
The emergency response facilities and secondary prevention strategies across professional football clubs in England
A Malhotra1, H Dhutia1, T Richards1, S Cheadle2, M Walker1, V Gabus1, M Papadakis1, I Beasley2, S Sharma1
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
2The Football Association, Medical Department, Wembley Stadium, London, United Kingdom
Topic: Sports cardiology
Purpose:The sudden cardiac arrest (SCA) of a professional athlete is usually high profile and well-publicised. However, such catastrophes can affect those competing at any level, not just in the upper echelons of sport. This study aimed to assess the emergency response planning and prevention strategies across a wide range of professional football clubs from all divisions in England, in line with current EACPR and Football Association (FA) guidelines.
Methods:Between June and October 2014, 60 professional clubs (15 from each division) received a questionnaire enquiring about planning for the cardiovascular safety of their players. This included 4 domains: cardiac screening; emergency planning; provision and training of automated external defibrillators (AEDs); and emergency services. Responses for each domain were allocated a mean score and added together to give an overall cardiovascular safety score out of 10.
Results:Table 1 shows the scores of each domain according to division. The Premier League achieved the highest overall cardiovascular safety score and scored highest or equal highest in each domain, than each of the lower divisions. There was less correlation between the other scores in the lower divisions. Division 2 outperformed Division 1 in AED provision and training. Division 1 exceeded the Championship in the domains of emergency planning and emergency services.
Conclusions:This study demonstrated that Premier League football clubs are better prepared to maintain the cardiovascular safety of their players than clubs in lower divisions. All divisions have demonstrated some degree of emergency planning in line with EACPR and FA guidance, with most providing AED facilities. However, improvements can be made in a number of areas. Emergency response facilities should be readily available to all athletes, not just those at the highest level.
Emergency responses by division
Domain for Emergency Response Strategies
Mean scores: Premiership
Championship
Division 1
Division 2
Cardiac screening (out of 3): Awareness of FA programme/ Participation in FA programme/ Participation in additional screening
2.62
2.33
2.00
2.13
Emergency Planning (out of 2): Plan in place/ Documentation of plan
1.77
1.33
1.67
1.38
AED provision and training (out of 4): Awareness of FA AED guidelines/ Resuscitation training for staff/ AED available on match day/ AED available at training
3.77
3.67
3.33
3.38
Emergency Services (out of 1): Presence of ambulance for players on match day (1)
1.00
0.83
1.00
0.75
Total points out of 10
9.16
8.16
8.00
7.64
P349
Pre-participation screening of adolescent athletes: a comparison of ECG criteria
A Malhotra1, M Walker1, H Dhutia1, R Narain1, A Merghani1, L Millar1, K Dodd1, J Ah-Fong1, M Papadakis1, S Sharma1
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
Topic: Sports cardiology
Purpose:Recommendations for interpretation of the athlete's electrocardiogram (ECG) has evolved in recent years, namely with the European Society of Cardiology (ESC, 2010), Seattle (2013) and more recently, the Refined (2014) criteria. A principle aim of these developments has been to improve the sensitivity and specificity for identification of young athletes at risk of sudden cardiac death and reduce false-positive rates. Whether these criteria are effective in adolescents is yet to be validated. Our study aimed to compare these criteria in a large cohort of adolescent (aged 14-17 years) athletes.
Methods:Between July 1998-August 2012, 7993 adolescent, professional male footballers aged between 14 and 17, were assessed through pre-participation screening. This included a history, examination, 12-lead ECG and echocardiogram. A retrospective analysis of the ECG data was undertaken by 2 cardiologists with the application of the ESC, Seattle and Refined criteria.
Results:Athletes were aged 16.1±1.5 years and were all male. 87.8% were Caucasian, 10.3% were Afro-Caribbean and the remainder were Oriental and South-East Asians. 1017 (12.7%) subjects were deemed to have an abnormal ECG when the ESC criteria were applied. This compared with 312 (3.9%) athletes against the Seattle criteria (p<0.0001). The Refined criteria reduced this further to 155 (1.9%, p<0.0001). By comparison to the ESC criteria, the Refined criteria significantly reduced the rate of ECGs deemed abnormal by 85% (p=0.0001). By comparison to the Seattle criteria, the Refined criteria significantly reduced the rate of ECGs deemed abnormal by 50% (p=0.0001). Rates of abnormal ECGs differed by criteria predominantly due to variations in T wave inversion criteria, and cut offs for QT intervals and right bundle branch block.
Conclusions:Recent developments of recommendations for interpretation of the athlete's ECG, most significantly through the Refined criteria, shows a reduction in the number of adolescent athletes deemed to have cardiac abnormalities. Our results suggest that current screening criteria are applicable in adolescent athletes as well as older counterparts. The Refined criteria will further improve the specificity of screening and therefore reduce the burden posed by high false-positive rates.