Improved efficiencies in cardiac rehabilitation through service redesign
A Maiorana1, J Smith1, J Garton-Smith2, J Redfern3, A Bremner4, D Hendrie5, J Rankin1, L Dimer6, T Briffa4
1Royal Perth Hospital, Cardiology, Perth, Australia
2Royal Perth Hospital, Perth, Australia
3The George Institute for Global Health, Sydney, Australia
4The University of Western Australia, Perth, Australia
5Curtin University, Perth, Australia
6Heart Foundation, Perth, Australia
Topic: Sports cardiology
Purpose:Cardiac rehabilitation (CR) is widely recommended following acute coronary syndrome (ACS) but is both underutilised and under-resourced. An alternative model of CR for cost effective secondary prevention (ACCES) was implemented and evaluated at a West Australian tertiary hospital. The project aimed to increase the proportion of patients receiving four guideline-advocated CR components: an initial assessment, individualised plan, education and follow-up, through service redesign in an environment of unchanged staff resources.
Methods:Patients discharged from cardiology wards with a primary diagnosis of ACS 1/4/2013-31/3/2014 (ACCES group) were compared to patients discharged 1/4/2011-31/3/2012 (controls). Patients transferred directly to another hospital for continuing cardiology care, aged >80 years, or deceased within four weeks of discharge were excluded. A quality improvement framework involving key stakeholders (74 patients, 52 hospital staff, 18 General Practitioners) was undertaken to inform processes to support change. Ward nurses assumed a more active role in inpatient CR, supported by a new CR needs assessment tool. This enabled CR specialist nurses to focus on post discharge service provision. An automated referral process was established that generated a daily list of eligible patients for follow-up by CR staff post discharge.
Results:The ACCES model was associated with a significant increase in the provision of each one of the four CR components (Table 1) and resulted in a near doubling in the proportion of patients who received all four components, culminating in follow-up. This equates to an increase of 264 patients per 1000 admissions.
Conclusion:Clinical service redesign was associated with efficiencies in CR, doubling patient numbers serviced for no additional staffing. This finding has important implications for the many CR programs that have limited staff resources or relatively low levels of uptake. Improved access to CR is associated with changing the clinical course post ACS.
Component
Controls (n=999)
ACCES (n=862)
P-value
Initial assessment
723 (72.4)
835 (96.9)
<0.001
Individualised CR plan
544 (54.5)
648 (75.2)
<0.001
Education
504 (50.5)
638 (74.0)
<0.001
Follow up
291 (29.1)
478 (55.5)
<0.001
P453
Effect of different protocols for cardiac rehabilitation phase I in the performance of six-minute walk test in patients after coronary artery bypass grafting
M Zanini1, RM Nery2, AD Da Silveira1, RP Buhler1, JB De Lima1, GC Nascimento1, FS Santos1, R Stein1
1Federal University of Rio Grande do Sul, Porto Alegre, Brazil
2Hospital de Cl?cas de Porto Alegre, Porto Alegre, Brazil
Topic: Sports cardiology
Purpose:After coronary artery bypass graft (CABG) patients reduce functional capacity, pulmonary function and respiratory muscle weakness. Our aim was to compare 2 different protocols of cardiac rehabilitation phase 1 after CABG in relation to distance walked in six-minute walk test (6MWT) at the time of hospital discharge.
Methods:In this randomized clinical trial, subjects were assessed on the day of hospitalization (before surgery) using the 6MWT. After surgery they were randomized to Group I (respiratory therapy, physical exercise of upper and lower limbs, progressive distance walking and inspiratory muscle training) and Group II (respiratory therapy and inspiratory muscle training). All patients underwent the intervention twice a day for 6 days. All patients were evaluated at the time of discharge.
Results:Nineteen patients (G1, n=9; G2, n=10) were evaluated. After randomization, clinical and functional characteristics were the same in the 2 groups. The mean age was 58 ± 5 years (G1) and 59 ± 8 years (G2), with a male predominance. The distance walked pre and postoperative was: G1; 409 ± 63 vs 375 ± 74 and Group II; 384 ± 71 vs 275 ± 77. There was difference (P = 0.01) between groups after seven days postoperatively.
Conclusions:A protocol that incorporates physical exercise of the upper and lower limbs and progressive distance walking to respiratory therapy and inspiratory muscle training seems to improve functional capacity after CABG. This protocol elicits the potential benefits of a more extensive phase 1 rehabilitation program.
P454
Individualized combined exercise is superior to group based exercise in improving health related quality of life in heart disease patients
JW Christle1, A Schlumberger1, M Halle1, A Pressler1
1Technical University of Munich, Department of Prevention and Sports Medicine, Munich, Germany
Topic: Sports cardiology
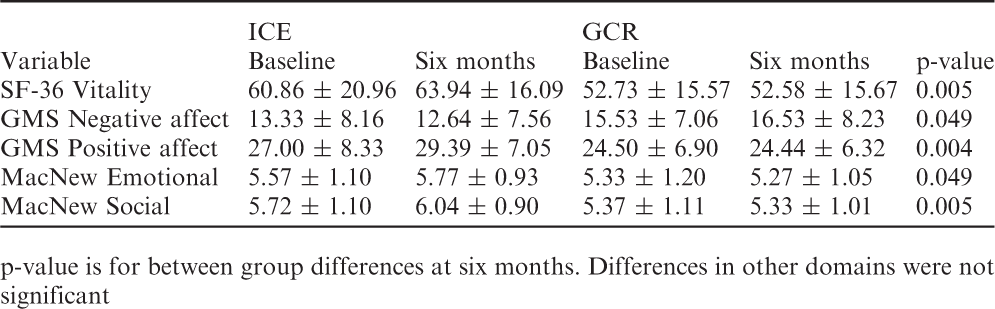
Purpose:Improving health- related quality of life (HRQoL) is an important goal in phase III cardiac rehabilitation (CR). Patients with heart disease and low exercise capacity (< 6 MET) have higher risk for future cardiac events and lower HRQoL compared to low risk patients. There is few data on this form of therapy and HRQoL, and no studies comparing traditional group based CR to other modes of exercise therapy on HRQoL in moderate to high risk patients. The current study compared the weekly individualized combined exercise (ICE) with group-based CR (GCR) on changes in HRQoL in heart disease patients with low exercise capacity.
Methods:Seventy patients (70 ± 9 y, 38% female) with AHA class C risk status performed cardiopulmonary exercise testing and were randomized 1:1 to once-weekly ICE or GCR for six months. ICE consisted of 30 minutes of endurance exercise at 60-70% VO2peak and two sets of five large muscle-group resistance exercises at 40-60% of one-repetition maximum. At baseline and six months, HRQoL was assessed by SF-36, GMS and MacNew instruments.
Results:ICE was significantly superior to GCR in improving vitality, emotional and social health, and positive and negative affect.
Conclusions:ICE has a more positive influence on HRQoL in heart disease patients with moderate to high cardiovascular risk status compared to GCR.
p-value is for between group differences at six months. Differences in other domains were not significant
ICE
GCR
Variable
Baseline
Six months
Baseline
Six months
p-value
SF-36 Vitality
60.86 ± 20.96
63.94 ± 16.09
52.73 ± 15.57
52.58 ± 15.67
0.005
GMS Negative affect
13.33 ± 8.16
12.64 ± 7.56
15.53 ± 7.06
16.53 ± 8.23
0.049
GMS Positive affect
27.00 ± 8.33
29.39 ± 7.05
24.50 ± 6.90
24.44 ± 6.32
0.004
MacNew Emotional
5.57 ± 1.10
5.77 ± 0.93
5.33 ± 1.20
5.27 ± 1.05
0.049
MacNew Social
5.72 ± 1.10
6.04 ± 0.90
5.37 ± 1.11
5.33 ± 1.01
0.005
P455
Improvement of flow mediated dilatation in patients with coronary disease after 6 months cardiac rehabilitation
I H Jung1, K J Rhee1, H Y Lee1, Y S Byun1, C W Goh1, B O Kim1
1Inje University, Seoul, Korea, Republic of
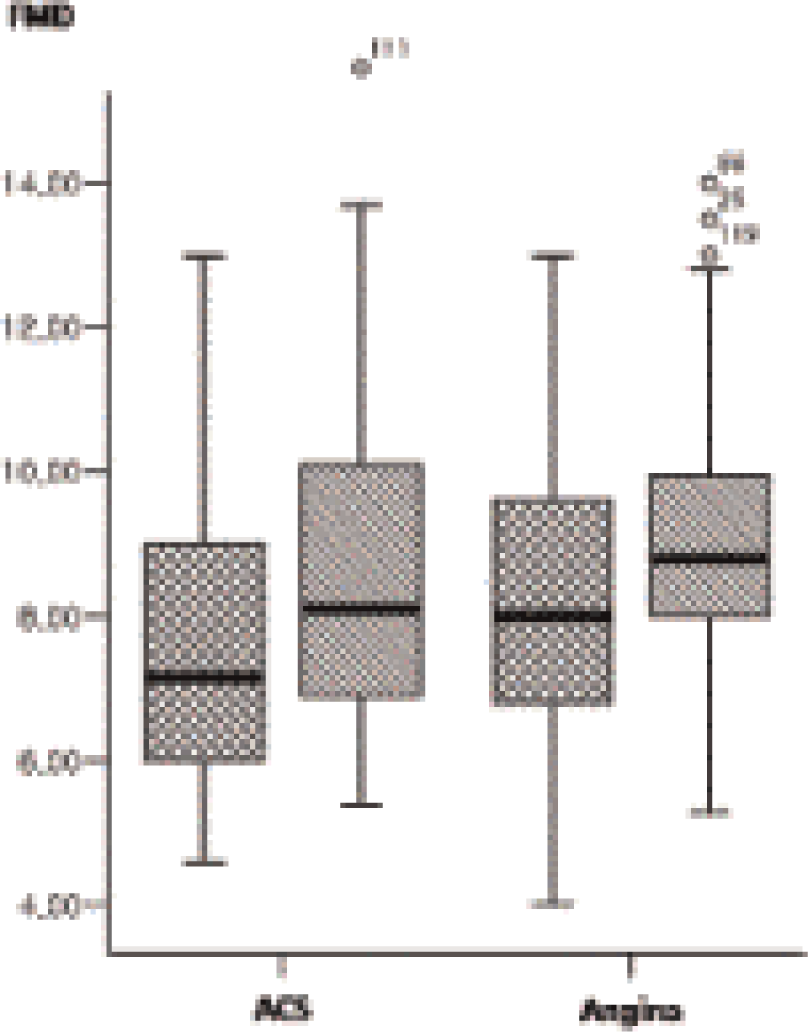
Background:Flow-mediated dilatation (FMD) is one of the accepted techniques to assess endothelial function, which has been well known as an independent predictor of cardiovascular outcomes. And also, every recent major evidence-based guideline regarding the management and prevention of coronary heart disease provides a class 1 level recommendation for referral to a cardiac rehabilitation program (CR). We investigated whether the endothelial function of the patients who had received percutaneous coronary intervention (PCI) was improved or not after 6 months CR.
Methods:We evaluated the relationship between FMD in 119 patients (104 males, mean age; 54.9 ± 9.1 years) who had treated with PCI. The patients were divided into 2 subgroups; 69 patients with acute coronary syndrome and 50 stable angina patients. All patients were examined on the second or third day after PCI, and 6 months from discharge. They received CR after discharge according to the study protocol.
Results:There was no significant difference of FMD at baseline (8.1% in angina vs. 7.7% in ACS, p=0.18) and 6 months follow-up (9.2% vs. 8.9%, p=0.61) between the patients with angina and ACS. However, FMD which was measured after 6 months CR was significantly improved on both groups (increase by 1.1% in angina; 0.1-2.0, p=0.03 vs. 1.1% in ACS group; 95% CI: 0.5-1.8, p=0.002).
Conclusion:Even though there was no significant difference of FMD on ACS and angina patients, FMD was improved after CR program in patients with PCI. And this beneficial effect was noted equally on both groups. Our results support that improvement of endothelial function is one of the important effect of CR reducing cardiovascular risk in patients with coronary disease.
P456
The Samba protocol for cardiac rehabilitation
TC Carvalho1, AI Gonzales1, HO Braga1, SW Sties1, LS Mara1, GD Carvalho1, AS Netto1, DP Lima1, PAB Araujo1, AV Souza1
1State University of Santa Catarina, Florianopolis, Brazil
Topic: Sports cardiology
Purpose:The ballroom dancing has been proven effective in improving cardiorespiratory capacity in patients with cardiovascular disease. The Brazilian samba dance modality is very popular and can be performed in differences intensities. The aim of this study was to develop and evaluate a Samba protocol aiming physical training in cardiac rehabilitation.
Methods:Fifteen patients with stable coronary artery disease (CAD), aged 60.74 ± 5.96 years, underwent maximal cardiopulmonary exercise test with determination of heart rate (HR) corresponding to the peak VO2 and first and second ventilatory thresholds. During six sessions, patients underwent twenty Samba steps, in three music tempo classified by a metronome in slow, medium and fast. Posteriorly, underwent three sessions for verify the HR behavior and perception of effort. Descriptive analysis was used to characterize the sample and check the HR, the t test or Wilcoxon test were used to compare the HR behavior (in different sessions) with significance level of 5%.
Results:In samba sessions patients remained most of the time (86.57% ±4.17) between 60 and 90% of HRpeak, which is the zone proposed for rehabilitation training. When considering the target zone ideal, with HR situated between the ventilatory thresholds, patients remained 76.79 ±2.28 time. While patients danced they reported perception of mild to moderate effort.
Conclusion:The patients showed good adaptation to Samba Protocol, which is able to be adopted as a proposal for training in cardiac rehabilitation.
P457
The impact of aerobic exercise training with vascular occlusion in patients with chronic heart failure
Y Tanaka1
1Yodogawa Christian Hospital, Osaka, Japan
Topic: Sports cardiology
Purpose:Aerobic exercise training is an important adjunct to medical therapy in patients with chronic heart failure (CHF). However, the effect of aerobic exercise training with vascular occlusion in patients with CHF on improving exercise capacity is unknown. This study aimed to evaluate the impact of aerobic exercise training with vascular occlusion in patients with CHF.
Methods and Results:Twenty patients with CHF due to ischemic cardiomyopathy (New York Heart Association functional class I to II) were randomized to an interventional exercise group (IG, n = 10) or a control exercise group (CG, n = 10). Exercise was performed at an intensity of 40–70% of the maximum peak VO2/W for 15 min three times a week for 6 months. Patients in the IG group remained seated on the saddle of the cycle ergometer with their feet on the pedals. Pneumatic tourniquets (width: 90 mm, length: 700 mm) were applied to the proximal ends of their thighs with appropriate pressure resulting in a 20–40 mmHg increase in the systolic blood pressure that is required for vascular occlusion (209 ± 8.0 mmHg). We evaluated the safety and efficacy of the intervention, and its effect on exercise capacity and serum brain natriuretic peptide (BNP) level. There were no significant differences between the 2 groups at study entry (IG vs. CG; age: 55.0 ± 4.7 vs. 55.5 ± 4.5 years; height: 153.6 ± 7.2 vs. 152.6 ± 7.1 cm; weight: 66.1 ± 4.9 vs. 66.3 ± 4.9kg; ejection fraction: 51.5 ± 4.7 vs. 48.4 ± 4.7%; peak VO2/W: 16.0 ± 6.5 vs. 13.8 ± 5.4 mL·kg-1·min-1; BNP: 92.9 ± 10.0 vs. 88.5 ± 9.3 pg/mL; right thigh circumference: 43.0 ± 4.7 vs. 42.8 ± 4.3 cm; left thigh circumference: 43.2 ± 4.7 vs. 42.7 ± 4.3 cm). Peak VO2/W in the IG group significantly increased compared with that in the CG group (29.1 vs. 12.4%, p < 0.05), and the change in the serum BNP level was significantly larger in the IG group than in the CG group (-31.0 ± 7.6 vs. 5.0 ± 6.4 pg/mL, p < 0.05).
Conclusion:These results suggest that aerobic exercise training with vascular occlusion can improve exercise capacity and serum BNP levels in patients with CHF without serious adverse events.
P458
Exercise capacity improvement and sustainability with cardiac rehabilitation: is there a role for left ventricular systolic dysfunction?
G Pestana1, JA Rocha2, M Tavares-Silva1, R Pinto1, AR Godinho1, JD Rodrigues1, V Araujo1, FP Parada2, MJ Maciel1
1Sao Joao Hospital, Cardiology, Porto, Portugal
2Sao Joao Hospital, Physical Medicine and Rehabilitation, Porto, Portugal
Topic: Sports cardiology
Purpose:Cardiac rehabilitation (CR) improves exercise capacity in acute coronary syndrome (ACS) patients. Exercise capacity itself is independently associated with improved quality of life and reduction of subsequent cardiovascular events. Still, important gaps remain in our understanding of how impaired systolic function (SF) affects the response to exercise capacity.?128;¨ We aimed to assess how the degree of initial systolic dysfunction (SD) might affect exercise capacity improvement and sustainability after CR in post-ACS patients.
Methods:?128;¨We conducted a post-hoc analysis of prospectively collected sociodemographic, clinical and functional data from 527 consecutive patients referred to CR after hospitalization for ACS. Patients were stratified as having normal SF (ejection fraction =55%), mild (45-54%) or moderate to severe (<45%) SD as evaluated by echocardiogram before discharge. Exercise capacity was evaluated as the maximum duration of a treadmill stress test using the Bruce protocol, assessed before and after the exercise training program and at 12 months follow-up. Patients with missing data were excluded.?128;¨ We used a mixed model (between-within group) analysis of variance (ANOVA) to compare exercise capacity response to CR and differences across SD groups.
Results:?128;¨207 patients were included in the analysis, with mean age 54 years (ranging from 27 to 91 years); 85% were male. 126 patients (60.9%) had normal SF, 45 (21.7%) had mildly impaired SF and 36 (17.4%) had moderate or severely impaired SF.?128;¨ All groups showed similar improvements in exercise capacity throughout CR (within groups: Wilk's lambda=0,481, p<0,001; between-groups: p=0.474). After CR exercise capacity increased from 8min28sec to 10min19sec in the normal SF group, from 8min33sec to 10min31sec in the mild SD group and from 8min02sec to 9min50sec in the moderate or severe SD group (p<0.001 for all comparisons). This was followed by a trend towards decreasing exercise capacity at 12 months, only marginally significant in the normal SF group (10min19sec to 10min, p=0.06).
Conclusions:CR effectively increases exercise capacity in ACS patients, an effect independent of baseline systolic dysfunction. This effect, however, tends to weaken with time after conclusion of exercise training. Therefore, it is mandatory not only to develop strategies to improve patient referral and participation in CR but also to assure sustainability of this results over time.
P459
Addressing inequalities in cardiovascular health: a novel cardiac rehabilitation programme in a socio-economically disadvantaged community
ME Cupples1, J Turnbull2, J Cunningham3, C Mcmaster4
1UKCRC Centre of Excellence for Public Health Northern Ireland (NI), Belfast, United Kingdom
2West Belfast Partnership, Belfast, United Kingdom
3Belfast Health and Social Care Trust, Cardiac Rehabilitation, Belfast, United Kingdom
4Public Health Agency, Northern Ireland, Belfast, United Kingdom
Topic: Sports cardiology
Purpose:Age-standardised death rates for cardiovascular disease (CVD) in West Belfast, an area of high socioeconomic disadvantage in Northern Ireland (NI), are 1.5 times higher than the national average (129 v 81/ 100,000). A community based initiative (Healthy Hearts in the West) was designed to address this inequality, by aiming to raise people's awareness of risk factors and to support self-managed lifestyle changes. In response to a recent report which highlighted the need for collaboration between public, community, voluntary and private sectors to build mutual reliance and respect in addressing the social determinants of health inequalities, a novel cardiac rehabilitation (CR) programme was also designed for the community.
Method:The programme was developed using a logic model approach, building on local knowledge and social, cultural and material assets. It was set up in January 2012. Patients who had experienced an acute cardiac event or intervention were invited to attend an 8-week programme, in a community centre. A multidisciplinary team delivered a similar programme as had been delivered in a local hospital but the CR nurses, in addition, developed links with community health and social care staff and volunteers to facilitate patients' access to counselling and complementary therapy services within the centre. Good communication was established with others involved in patients' care: information about attendance, risk factors, psychosocial health status, and medication was posted to the cardiologist and general practitioner at the start and completion of the programme, and when indicated. Patients formed links with community groups, to encourage maintenance of active and healthy lifestyles. Changes in risk factors were measured and patients' perceptions of the programme were assessed by postal questionnaire.
Results:Overall, 41.9%(137/327) of eligible patients attended in the first year: uptake of CR in NI was 38% during the previous year, with lower uptake in areas of socio-economic disadvantage. Patients also attended a range of community services, including smoking cessation and alcohol and weight management; 30(22%) attended counselling, 53(39%) received complementary therapy; 96(70%) enrolled in follow-up programmes. Questionnaire data indicated that the on-site services facilitated achievement of goals and promoted attendance; 94%(63/67) of respondents said they would recommend the programme to others.
Conclusions:Our findings suggest that a community-based collaborative approach can support the delivery of CR and help address health inequality related to cardiovascular risk.
P460
Effects of cardiac rehabilitation in young patients after an acute coronary syndrome.
M Sanchez Martinez1, S Del Prado Diaz2, R Dalmau Gonzalez-Gallarza2, A Castro Conde1, D Hernandez Munoz3, C Vindel Martinez3, A Araujo Avendano3, H Arranz Rodriguez3, M Marin Santos3, JL Lopez Sendon2
1University Hospital Virgen de la Arrixaca, Department of Cardiology, Murcia, Spain
2University Hospital La Paz, Madrid, Spain
3Hospital Cantoblanco, Madrid, Spain
Topic: Sports cardiology
Purpose:We aim to analyze the cardiovascular risk profile and impact of cardiac rehabilitation program (CRP) in young patients after an acute coronary syndrome (ACS). From a cohort of 833 patients, were analyzed retrospectively patients =45 years of age included in the CRP between August 2006 and March 2014.
Results:116 consecutive patients (91.1% male, mean age 39.9 ± 4.4 years) were included. The most common indication for cardiac rehabilitation was ST elevation myocardial infarction (STEMI) in 93% of cases with anterior location (45%). Percutaneous coronary intervention (PCI) was made in 99.1% of cases and complete revascularization was achieved in 85% of patients. The presence of classical cardiovascular risk factors was high: 21.6% hypertension, 12% diabetes; 62% of patients were dyslipidemic, 25.9% obese (mean BMI 28 ± 5 kg/m 2), 77.6% smokers with a mean 28.7 pack-years and a 61.2% of them had =2 CVRF. A quotient TG / HDL> 3.5 (indirect measure of insulin resistance) in 73.1% of patients were detected. 87.1% underwent a standard PRC, with a dropout rate of 13.8%. Most of them had a good basal functional capacity with a mean of 9.6 ± 2.4 METS. At the end of the CRP, control target LDL <70 mg / dl was achieved in 55.7% of cases, HDL> 35 mg/dl in a 48.5% and TG <150 mg/dl in a 75, 2%. Smoking abstinence confirmed by co-oximetry were 74.2% and 65.1% at 3 and 6 months respectively. Significant reductions in LDL cholesterol, TG, quotient TG / HDL and abdominal circumference (p <0.001) as well as an increased HDL (p <0.03) were obtained. At discharge, a significant functional improvement was observed with a mean of 12.6 ± 2.1 METS (p <0.001).
Conclusions:In young patients, smoking is the main risk factor for developing ACS. Cardiac rehabilitation is useful for improving the lipid profile, insulin resistance, functional capacity and to consolidate tobacco abstinence.
BMI: body mass index; EFLV: ejection fraction of left ventricle.
Variable
Baseline levels (Mean ±standar deviation)
Discharge levels (Mean ±standar deviation)
Relative (%)
95% CI
p
BMI (kg/m2)
28,12±4,96
27,78±4,49
1,21
[-0,06-0,37]
0,155
Abdominal circumference (cm )
99,71 ±12,01
97,8 ±10,84
1,9
[1,43-2,77]
<0,001
Hemoglobin A1c (%)
5,9±1,59
5,68±0,63
4,37
[-0,09-0,61]
0,14
EFLV (%)
49,41±12,9
52,17±9,9
5,59
[-9,26- -4,77]
<0,001
Functional capacity (METS)
9,65±2,4
12,63±2,17
30,88
[-3,51- - 2,61]
<0,001
P461
Exercise capacity improvement in cardiac rehabilitation: role of echocardiographic modifications/adaptations
J C Duarte Rodrigues1, MTS Tavares Silva1, GP Pestana1, RP Pinto1, AG Godinho1, FM Filipa Melao1, VA Vitor Araujo1, JAR J Afonso Rocha2, FP Fernando Parada2, MJM Maria Julia Maciel1
1Sao Joao Hospital, Department of Cardiology, Porto, Portugal
2Sao Joao Hospital, Department of Physical and Rehabilitation/ Exercise Training/Cardiac, Porto, Portugal
Topic: Sports cardiology
Purpose:In the evaluation of patients with acute coronary syndromes (ACS), echocardiography has a pivotal role in non-invasive diagnosis and risk stratification. Exercise capacity after ACS is a strong predictor of future cardiovascular morbidity and mortality and can be effectively modified by exercise training/cardiac rehabilitation (CR). However, the exact mechanisms of improvement in exercise tolerance after cardiac rehabilitation program are not fully understood. We aimed to evaluate the contribution of echocardiographic features in exercise capacity increase in CR setting.
Methods:Patients admitted to CR within 3 months of ACS were included. Transthoracic echocardiograpy study was performed at baseline (within 48-72 h after hospital admission), at the end of two-month CR program consisting of biweekly exercise training sessions and at 12 months follow-up. An estimate of left ventricular filling pressure was made using pulsed wave (PW) Doppler and Tissue Doppler Imaging (TDI), in particular, E/e' (the ratio between peak early mitral inflow velocity (E) and the average of the peak early septal and lateral annulus velocity (e') that indicates left ventricular diastolic function. Other conventional measurements were also made. Serial treadmill exercise test were performed during all phases.
Results:A total of 333 patients (86.5 % male), aged 53± 9.5 years were referred to CR after ACS between 2009 and 2013. No significant differences of E/e' values were seen at the three phases despite a trend towards decreased relaxation time (8.3± 2.7 for phase 1; 8.1± 2.6 for phase 2; 7.9 ± 2.1 for phase 3). The gain in exercise capacity was substantial after the 12 months follow-up period (p < 0.001 for phase 2 and 3) and it was significantly correlated with E/e' value (r= -0.42; p< 0.001). Despite improvement in left ventricular ejection fraction (p< 0.001 for phase 2 and 3) no other correlations were found between exercise capacity and other echocardiographic measurements.
Conclusions:Exercise training in post-acute myocardial infarction patients results in a significant improvement in exercise capacity with a potential role of diastolic ventricular function exercise-induced modifications.
P462
Cardiac rehabilitation after acute coronary syndrome - do all patients have the same benefit?
S Aguiar Rosa1, A Abreu1, R M Soares1, P Rio1, I Rodrigues1, A Monteiro1, D Mesquita2, A Gaspar3, S Silva1, R Cruz Ferreira1
1Hospital de Santa Marta, Cardiology, Lisbon, Portugal
2Hospital N.S. Rosario, Cardiology, Barreiro, Portugal
3Hospital dos Capuchos, Internal Medicine, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Cardiac rehabilitation(CR) demonstrated to improve exercise capacity in patients(pts) with acute coronary syndrome(ACS). The aim of this study is to understand, after CR, which pts benefit the most in functional capacity(FC).
Methods:Retrospective analysis of consecutive ACS pts who underwent CR and cardiopulmonary exercise testing(CPET), Jan/04 and Dec/13. CPET was performed pre and post CR. CPET parameters: peak oxygen uptake(pVO2), %of predicted pVO2, minute ventilation/CO2 production(VE/VCO2) slope, VE/VCO2slope/pVO2 and peak circulatory power(PCP) (pVO2xpeak SBP). The difference between prepVO2 and postpVO2(?O2) was calculated. Pts were analysed according to pre pVO2(<20vs=20ml/kg/min) and left ventricular ejection fraction(LVEF)(<50vs=50%). Results:130pts, 86% male, mean age 56.8+10.9years. 113pts had STEMI. Both pVO2<20ml/kg/min (pVO2A)(31pts) and pVO2=20ml/kg/min (pVO2B)(99pts) had FC improvement after CR (table). pVO2A showed a greater increase in pVO2 than pVO2B (?O2 4.39±7.31vs0.85±5.67; p=0.049). In pVO2A 71% of pts got an increase in pVO2>10% comparing to 40% in pVO2B(p=0.0029). There was a CPET parameters improvement in LVEF<50% (LVEFA)(34pts) and LVEF=50% (LVEFB)(96pts), particularly in pVO2 and CPET duration. In LEVFA pVO2 increased from 24.8±6.3 to 28.1±7.1ml/kg/min (p=0.003) and CPET duration from 13.6±2.4 to 15.2±3.3minutes (p=0.002). In LVEFB pVO2 (25.9±7.0 to 27.8±7.4ml/kg/min; p=0.005) and CPET duration (13.3±3.3 to 15.3±2.5 minutes; p<0.001) increased. A greater ?akVO2 was documented in LVEFA than in LVEFB (3.37±5.67vs2.72±8.51; p=0.681) and more pts had pVO2 increase>10% in LVEFA (55.9% vs 44.8%; p=0.266).
Conclusion:Worst baseline FC pts have more improvement after CR, evaluated by CPET. LV dysfunction pts seem to have more benefit with CR program.
pVO2<20 (n=31)
pVO2=20 (n=99)
CPET parameters
Before CR
After CR
p-value
Before CR
After CR
p-value
Peak VO2 (ml/kg/min)
17.7±1.8
22.1±7.2
0.002
28.1 ±5.6
29.7±6.2
0.004
%predicted peak VO2
68.6±12.3
86.5±33.0
0.008
96.3±21.7
99.3±24.0
0.181
VE/VCO2 slope
29.2±6.1
28.6±5.8
0.425
25.8±5.5
24.9±4.8
0.062
PCP (mmHg.ml/kg/min)
2863.7±581.6
3746.9±1432.0
<0.001
4817.3±1302.2
5078.3±1219.4
0.043
(VE/VCO2slope)/pVO2
1.67±0.41
1.42±0.61
0.02
0.95±0.28
0.86±0.39
0.001
Duration (minutes)
10.5±3.2
13.2±2.4
<0.001
13.2±4.5
15.9±2.6
<0.001
P463
The relationship between carotid intima-media thickness and baroreflex sensitivity in coronary patients
M Gois1, RP Simoes1, VC Kunz1, SCM Moura-Tonello1, P Driusso1, HS Hirakawa1, N Montano2, A Porta3, AM Catai1
1Federal University of Sao Carlos, Physical Therapy, Sao Carlos, Brazil
2University of Milan, Department of Clinical Sciences, Milan, Italy
3University of Milan, Department of Technologies for Health, Milan, Italy
Topic: Sports cardiology
Purpose:to evaluate the relationship between carotid intima-media thickness (IMT) and baroreflex a-index in two groups: coronary artery disease patients and healthy subjects.
Methods:37 subjects between 45 and 65 years old were divided in 2 groups: coronary artery disease patients (CAD group, n=18) and healthy subjects (H group, n=19). The patients of CAD group had a diagnosis of CAD confirmed by coronary angiography examination. The carotid ultrasound was performed in the supine position with a 12 MHz linear transducer. The common carotid intima-media thickness (IMT) was evaluated 1 cm from to the carotid bifurcation and site of carotid plaques were excluded of the measurement. The IMT of the wall was evaluated as the distance between the lumen–intima interface and the media–adventitia interface and the average of three measurements from the right and left common carotid artery was used for analyses. The subjects remained at rest for 10 minutes and the data were collected in the standing position. The recording of R-R interval (R-Ri) of the ECG was performed in the MC5 lead and the arterial pressure (AP) was recorded by a finger plestysmographic device (Finometer Pro, Finapres Medical Systems). Signals were sampled at 1000 Hz and the visual inspection of series (R-Ri and SAP) was performed in order to select the sections with the highest signal stability. Ectopic beats were excluded and 256 consecutives data points were used in the analysis. The BRS a index was calculated using a cross-spectral analysis by a bivariate autoregressive model between R-Ri and SAP in the LF frequency (LF): 0.04 Hz a 0.15Hz. The data distribution was verified by the Shapiro–Wilk test and the data were expressed in mean and standard deviation. One-way ANOVA test was applied to compare age and anthropometrics variables. Pearson's test was used to verify the correlation between the carotid IMT and BRS a index. Type 1 error occurrence was established at 5% for all tests (a = 0.05).
Results:there were no differences in age (H=52.89±7.10; CAD=57.86±6.26 years), weight (H=81.9±12.2; CAD=76.4±16.8kg), height (H=1.74±0.08; CAD=1.67±0.07m) and body mass index (BMI), (H=27.19±3.56; CAD=27.20±4.61 kg/m2) between the groups. Non-significant correlation coefficient was observed between carotid IMT and BRS a-index (r=-0,13 and p=0,35).
Conclusions:There were no correlation between IMT and baroreflex a-index in the standing position suggesting that these variables cannot be replaced for each other.
P465
Effectiveness of high intensity interval training on cardiac remodelling in cardiac resynchronization therapy responders and non-responders: a randomized control trial
VT Santos1, A Abreu2, R Pinto1, X Melo1, P Cunha2, M Oliveira2, R Ferreira2, LB Sardinha1, B Fernhall3, H Santa Clara1
1University of Lisbon, Faculty of Human Kinetics, Lisbon, Portugal
2Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
3University of Illinois, College of Applied Health Sciences, Chicago, United States of America
Background:A growing body of evidence suggests that high intensity interval training (HIIT) leads to major benefits in cardiac remodelling parameters in patients with chronic heart failure (CHF). However, up to 30% of patients receiving cardiac resynchronization therapy (CRT) do not have a positive clinical or reverse remodelling response. CRT response was determined based on the a sustained improvement of =1 NYHA functional class and echocardiographic evidence of reverse remodelling (defined as an increase in LVEF of = 15%).
Topic: Sports cardiology
Purpose:Since HIIT and CRT modalities have a different mode of action, the purpose of this study was to assess the effects of CRT on cardiac remodeling of left ventricular mass in clinical responders and non-responders.
Methods:We studied 42 patients (mean age: 67±10.6 years), left ventricular ejection fraction (LVEF) at baseline (27±7%) in CHF III–IV NYHA functional class, referred for CRT. Patients were randomized in two groups: an exercise group (ExG) (n=21) who underwent a supervised HIIT program at 90-95% peak heart rate, 2 times a week for 6 months, and a control group (CG) (n=21) who underwent CRT. LVEF, systolic and diastolic volumes and left ventricular mass were evaluated with echocardiography. Paired samples t-tests and non-parametric Mann–Whitney test were used to evaluate overall changes in echocardiographic outcomes. Differences between groups, changes over time within each group and any interaction were assessed by two-way repeated measures.
Results:Among responders in the ExG, [n= 14 (70%)], we found a significant decrease (22%) in the left ventricular mass (baseline values 328.3±32.8 g and at 6 months 256.4±27.5 g, p<0.05), that could not be explained by changes in VO2peak or mean arterial pressure. There were no significant differences in left ventricular mass in responders in the CG (baseline values 322.8±23.0 g and at 6 months 291.6±57.5 g, p>0.05). In both responders groups there were a significant decrease in NYHA (ExG: 2.92±0.5 to 1.33±0.5, p=0.000 and CG: 2.78±0.4 to 1.22±0.7, p=0.000) and systolic volumes (ExG: 128.7±48.9 ml to 88±51.5 ml, p=0.004 and CG: 162.7±77.4 ml to 119.8±58.8 ml, 0.002), and an increase in LVEF (ExG: 27.5±6.8% to 42.08±9.4%, p=0.000 and CG: 25.09±8.9% to 42.09±7.5%, p=0.000).
Conclusion:In CRT responders patients, an HIIT program leads to further improvements in cardiac remodelling.
P466
Favorable effects of the in-patient transitional care for elderly patients with congestive heart failure: a 3-month follow-up.
L Dalla Vecchia1, M Monelli1, A Lucini1, C Lastoria1, F Di Paola2, R Furlan2
1Salvatore Maugeri Foundation, IRCCS - Center of Milan, Milan, Italy
2Internal Medicine - Humanitas Clinical and Research Center, Rozzano, Milan, Italy
Topic: Sports cardiology
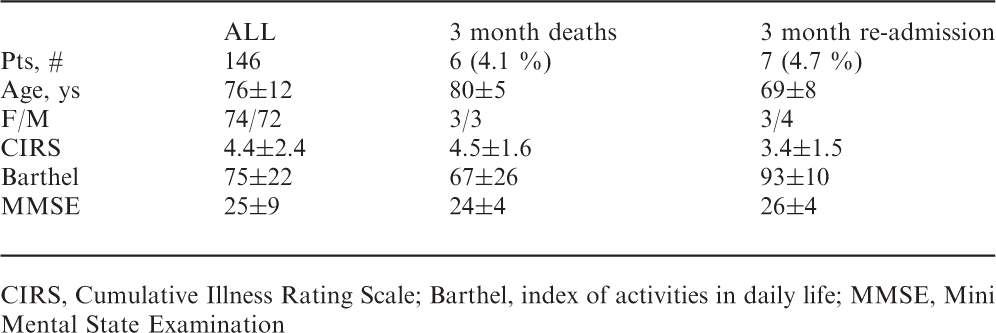
Purpose:Heart Failure (HF) is a main reason for hospitalization among older adults. HF hospitalization has poor prognosis with a mortality and readmission rate approaching 15% and 30%, respectively, within 30-60 days. In Italy, the Sub-Acute Care (SAC) represents a novel form of transitional in-patient care for older adults following an acute HF. Aim of the present study was to analyze the effects of this approach.
Methods:We selected all the HF pts discharged from our SAC department from January to October 2013. Telephone contacts were established to determine the 3 month follow-up.
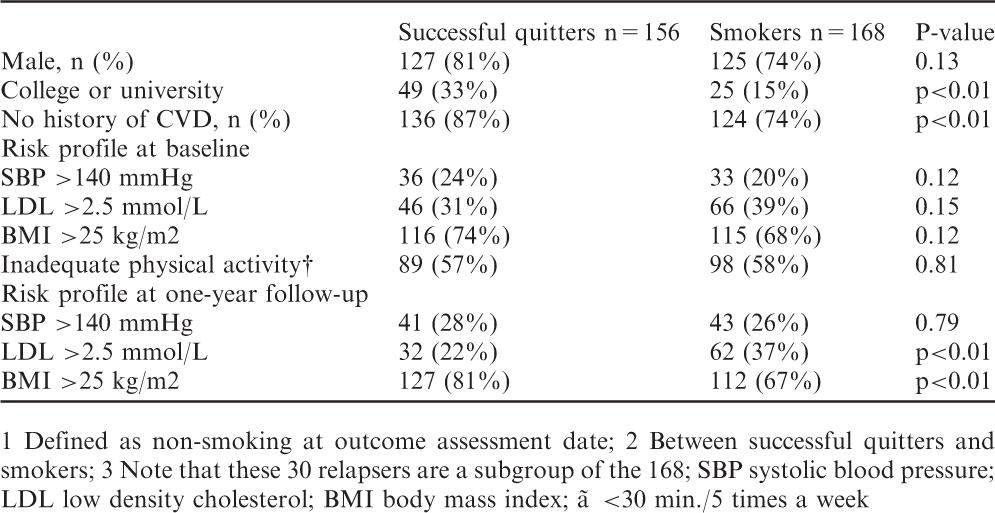
Results:149 patients were discharged home after a program of titration of medical therapy, management of comorbidities, education, and individualized training. 144 patients were interviewed by phone. The relative Registry Office (RO) was contacted for the missing pts. Ultimately, out of the 146 pts (3 were lost as they moved) included in this retrospective study, 6 (4.1%) died within 3 months (3 for HF), 7 (4.7%) were readmitted to the hospital (3 for HF). Clinical characteristics are shown in the table.
Conclusions:We found a favorable effect of a transitional in-patient care on the 3-month mortality and hospital readmission rate in HF patients, suggesting a positive effect in terms of quality of life and financial costs. Although hospital admission could simply herald disease progression, there is some evidence that hospital related interventions also contribute to poor outcomes, through increased neuro-hormonal and inflammatory activation, haemodynamic compromise, end-organ damage, and worsening of comorbidities. A period of care aimed to manage these complications might represent a key factor to improve outcomes.
CIRS, Cumulative Illness Rating Scale; Barthel, index of activities in daily life; MMSE, Mini Mental State Examination
ALL
3 month deaths
3 month re-admission
Pts, #
146
6 (4.1 %)
7 (4.7 %)
Age, ys
76±12
80±5
69±8
F/M
74/72
3/3
3/4
CIRS
4.4±2.4
4.5±1.6
3.4±1.5
Barthel
75±22
67±26
93±10
MMSE
25±9
24±4
26±4
P467
Changes on anxiety and depression in patients with heart disease into cardiac rehabilitation program
P Perafan1, O Quintero1, A Murillo1, CJ Herrera1, D Espinosa1, DC Carrillo1, JS Villadiego1
1fundacion valle del lili, cali, Colombia
Topic: Sports cardiology
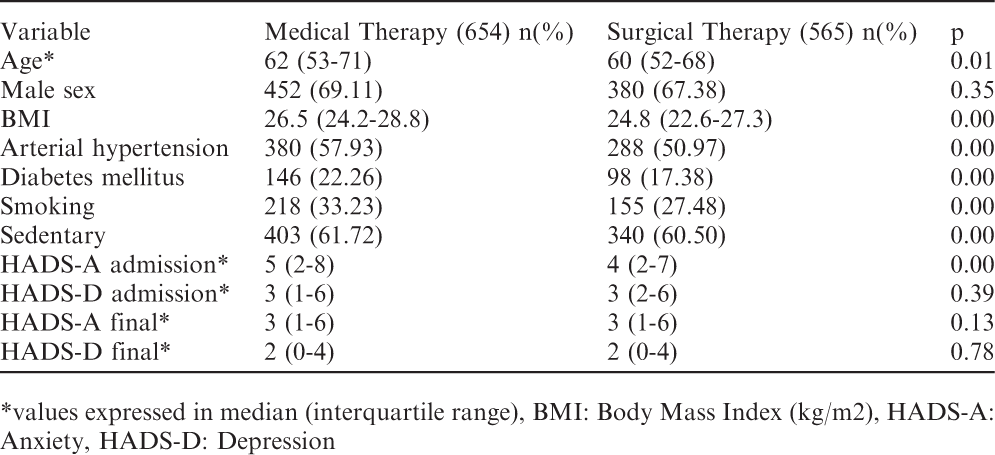
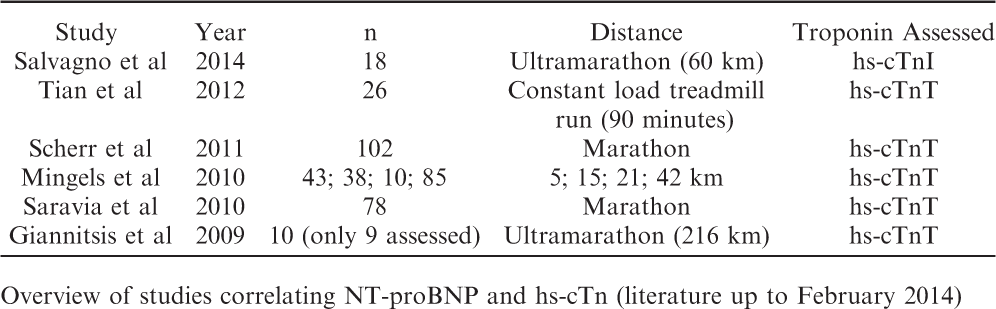
Purpose:To determine the prevalence of anxiety and depression disorders in patients with cardiovascular disease on medical or surgical management admitted to the cardiac rehabilitation program (CRH).
Methods:Retrospective study of patients with cardiovascular disease with medical or surgical management between January 2005 to December 2013. Adults screened for anxiety and depression with the Anxiety Hospital and Depression Scale (HADS) at admission and at the end of the program were included. Cardiac transplant patients were excluded. Demographic variables stratified by medical or surgical management and scales of HADS were compared for each group at the entry and the end of the RHC Results:1219 patients were included. The median age was 61 y/o, 68% males and 58% have some degree of obesity. On admission, the median HADS-Anxiety was 3 and 11% of patients had anxiety by the scale. The median HADS-D was 3 and 5.71% had clinical depression. 37 patients had anxiety and depression. At the end of RHC there were improvement in anxiety score (mean 1.875, 95% CI 1.6-2.14 p=0.00) as well as for depression (mean 1.46 95% CI 1.2-1.72 p=0.00). For surgical therapy the diference in HADS-A was 1.48 (95% CI 1.18-1.78 p=0.00) and depression 1.83 (95% CI 1.53-2.12 p=0.00).
Conclusions:RHC programs decrease mortality in patients who have the indication. At the end of RHC program there were improvement in anxiety and depression scales.
*values expressed in median (interquartile range), BMI: Body Mass Index (kg/m2), HADS-A: Anxiety, HADS-D: Depression
Variable
Medical Therapy (654) n(%)
Surgical Therapy (565) n(%)
p
Age*
62 (53-71)
60 (52-68)
0.01
Male sex
452 (69.11)
380 (67.38)
0.35
BMI
26.5 (24.2-28.8)
24.8 (22.6-27.3)
0.00
Arterial hypertension
380 (57.93)
288 (50.97)
0.00
Diabetes mellitus
146 (22.26)
98 (17.38)
0.00
Smoking
218 (33.23)
155 (27.48)
0.00
Sedentary
403 (61.72)
340 (60.50)
0.00
HADS-A admission*
5 (2-8)
4 (2-7)
0.00
HADS-D admission*
3 (1-6)
3 (2-6)
0.39
HADS-A final*
3 (1-6)
3 (1-6)
0.13
HADS-D final*
2 (0-4)
2 (0-4)
0.78
P468
Treatment of myocardial ischemia in Cardiac Rehabilitation
M Abeytua1, JI Castillo-Martin1, C Torres1, EM Cramaroc1, A Pintor1, T Martinez-Castellanos1, MA Ortega1, A Fernandez-Gonzalez1, D Ruiz-Molina1, F Fernandez-Aviles1
Purpose:Phisical exercise with or without ischemic preconditioning produces cytoprotective molecular adaptations and reduces almost all pathophysiological mechanisms of ischemia / reperfusion. The aim of this study is to assess possible improvement of the ischemia in patients treated in Cardiac Rehabilitation with ischemic preconditioning.
Methods:8 patients were studied with previous acute coronary syndrome undergoing coronary reperfusion. All patients had the following features: A) effort angina pectoris grades I to III / IV. B) ischemia diagnosed with conventional stress test. C) ischemia in stress echocardiogram. Patients were treated in cardiac rehabilitation program for 3 months (36 sessions), with treadmill exercise for 20 minutes below the threshold positivity in the stress test. Later load was increased until ischemia in 12-lead electrocardiogram, holding ischemia for 5 minutes, if clinically was tolerated without other complications.
Results:Thresholds angina and ischemia started later at the end of the program in 8 patients. METS increased from 5 to 6.5 in 5 of them. Conventional treadmill test became negative in the other 3. Myocardial ischemia segments, unchanged in 2 patients, improved in 4 and became negative for ischemia in the other 2. . Angina and ECG changes returned without other complications. One patient suffered pre-syncope. Another time the training was stopped by frequent premature beats and bigeminism.
Conclusions:Ischemia training improvement tolerance to ischemia and in some cases ventricular function during exercise. Large randomized research are needed to study its superiority to regular train
P469
Home-based exercise training in coronary artery bypass grafting patients
S Pomeshkina1, E Loktionova1, Y Argunova1, N Arkhipova1, O Barbarash2
1Federal State Budgetary Institution Research Institute for Complex Issues of Cardiovascular Diseases, Rehabillitation Laboratory, Kemerovo, Russian Federation
2Federal State Budgetary Institution Research Institute for Complex Issues of Cardiovascular Diseases, Kemerovo, Russian Federation
Objective:To evaluate the efficacy and safety of home-based exercise training (HBET) as a part of outpatient rehabilitation program for patients, who have undergone coronary artery bypass grafting (CABG).
Material:112 patients (mean age 56.8 ± 5.5 years) with coronary artery disease (CAD), who have undergone CABG, were examined. One month after CABG, patients were enrolled into three groups, comparable in demographic and clinical characteristics: Group 1 with supervised cycling training (CT) (n = 35), Group 2 – home-based walking training (HBWT) (n = 36) and the comparison group (n = 41). Subjects did 3 trainings per week for 3 months. Patients were examined 1 month, 4 months and one year after CABG.
Methods:Echocardiography (ECHO-CG), the 6-min walk test (6MWT), bicycle ergometer (BE) with drug therapy.
Results:4 months after CABG ECHO-CG findings reported positive dynamics of left ventricular ejection fraction (LVEF) in Group 1 (p = 0, 01), in Group 2 (p = 0,03) and in the comparison group (from 54.5 ± 4.9 to 58.9 ± 5.7%, p = 0,04). However, this dynamics was more significant in Group 1 and 2. The assessment of effects of different types of cardiac rehabilitation on exercise capacity was performed by measuring the 6MWT in patients, undergoing CABG. The obtained results reported that increased exercise capacity 4 months after CABG was found in Groups 1 and 2 in comparison with the baseline (p = 0.02 and p = 0.04, respectively). There was no significant increase of walking distance in patients without HBET. A 6-minute walk test distance was significantly higher in Group 1 after 4 months compared to patients without HBET in the corresponding period (p = 0.01). Group 2 reported the tendency to higher exercise capacity 4 months after CABG, compared to patients without HBET (p = 0.06). There were no significant changes in the dynamics of exercise capacity in all groups comparing one year and 4 months findings after CABG. However, Group 1 and 2 reported significantly better values than those without HBET (p = 0.01 and p = 0.01, respectively). The assessment of effect of different types of cardiac rehabilitation on exercise capacity with the BE in patients, undergoing CABG, reported its increase in three groups 4 months after CABG. Thus, exercise capacity was higher in Group 1, compared to Group 2 (p = 0.03) and in patients without HBET (p = 0.04). The group differences leveled off one year after CABG.
Conclusion:Home-based walking training is safe and results in the optimization of cardiac hemodynamic parameters, increased exercise capacity; thus, it is less efficient than supervised cycling training.
P470
One year outcomes of combined use of warfarin and oral antiplatelet agents in patients with chronic obstructive pulmonary disease, atrial fibrillation and acute coronary syndrome.
J Ramazanov1, T Batyraliyev2, I Pershukov3, A Omarov4, Z Karben2, L Shulzhenko5, L Petrakova2, B Sidorenko6, Y Belenkov7
1Central Hospital of Oil Workers, Cardiology, Baku, Azerbaijan
6Presidential Medical Center , Moscow, Russian Federation
7Lomonosov State University, Moskow, Russian Federation
Background:Although atrial fibrillation (AF) occurs frequently in patients with chronic obstructive pulmonary disease (COPD) and hospitalized with acute coronary syndrome (ACS), strategies for prevention of thromboembolic complications are poorly characterized. We sought to examine exposure to warfarin and P2Y12 inhibitors and clinical outcomes among patients with COPD, AF and ACS.
Material and Methods:Patients age >65 years hospitalized in our clinics with primary diagnosis of ACS and a secondary diagnoses of COPD and AF between 2008 and 2012 were identified and included in interclinic Registry. Medication exposure was ascertained during a 90-day period following the index discharge using guidelines drug claims. Among patients who were alive and not readmitted during the ascertainment period, we examined the cumulative incidence of all-cause mortality and all-cause readmission by medication exposure at 1 year.
Results:A total of 1266 patients met the inclusion criteria. Among the 722 patients (61%) who were alive and not readmitted during the 90-day ascertainment period, 27.0% received warfarin, 38.9% received P2Y12 inhibitors, 10.2% received combination therapy, and 23.9% received neither therapy. Readmission rates were high in all groups at 1 year ( warfarin-47.5%, P2Y12 inhibitors-46.6%, combination therapy-38.0%, and neither therapy-39.3%), and the overall 1-year mortality rate was 12.5%.
Conclusion:Among old patients with COPD, AF and ACS, combination therapy with warfarin and P2Y12 inhibitors was uncommon during the 90-day ascertainment period, and more than one-quarter of patients had no claims for warfarin or P2Y12 inhibitors. Rates of all-cause readmission and mortality within 1 year of hospitalization for ACS were high.
P471
Exercise capacity evolution and readaptation impact after LVAD HeartWare implantation.
M Lamotte1, M Antoine2, G Van Nooten2
1Erasme Hospital (ULB), Physiotherapy and cardiac surgery department, Brussels, Belgium
2Erasme Hospital (ULB), Cardiac surgery department, Brussels, Belgium
Background:LVAD are more and more efficient and proposed to an increased amount of heart failure patient. Actually, 20000 devices have been implanted around the world and approximately 1500 are now implanted yearly. Those device allow not only to reduce the mortality of the patient, but also lead the patient on a more optimal status to the transplantation when, as in our country actually, only the "bridge to transplant" indication is recognized.
Population:Our data are based on a population of 50 consecutive patients implanted on a period of three years, by the continuous "HeartWare®" device. The variable are measured during 80 maximal cardiopulmonary exercise testing (CPET : VO2, VCO2, Ve, RER, ãÎ). Tests are realized at 1, 6, 12 and 24 month after implantation. Some of our patients follow a structured rehabilitation.
Results:The exercise capacity (VO2p) of our patient at one month is 46 % of de predicted value (PV), for a RER of 1.27 and a Ve/VCO2 slope of 36. At 6 month, mean workload is 77 W (47 % of PV), mean VO2p 16.8 ml/:kg.min (55 % of PV), mean Ve/VCO2slope is 35.4, mean Ve reserve is 55 %. Mean individual VO2p increase from 1 to 6 month but is stable or slightly decrease from 6 to 12 month after implantation. In the same time, their weight is increasing and the Ve/VCO2 slope also. We observe a large variation between patients. For example, at six month, VO2p varies from 33 to 98 % of the predicted value. The maximal workload achieved is actually 180 Watts (6 month) and illustrate the possible recovery of some patient after such an intervention. An important factor that explains those differences is the participation to a rehabilitation program as illustrate on a sub-group of our patient who complete the program. Our readapted patients seems to be older (50 versus 44 year old, NS), their exercise capacity are higher (VO2p : 67 versus 45 % of PV, p<0.01, Workload : 58 versus 36 % of PV, p<0.001) and the Ve/VCO2 slope seems to be lower (33 versus 37, NS).
Conclusions:LVAD allows the patient to recover an active life and allow them to follow a structured exercise rehabilitation program. At six month, the exercise capacity is severely depressed in some patient but nearly restored in some other particularly if a rehabilitation program is performed. Unfortunately, after the first six month (active period of rehabilitation), the exercise capacity decrease and the mean weight of the patient increase. This underline the importance of a structure supervised rehabilitation on a long term basis.
P472
Left ventricular versus biventricular assist devices: does it make a difference in exercise capacity?
I D Laoutaris1, S Adamopoulos1, A Dritsas1, A Gkouziouta1, L Louca1, P Sfyrakis1
1Onassis Cardiac Surgery Center, Athens, Greece
Topic: Sports cardiology
Purpose:Due to lack of donor hearts, patients with ventricular assist devices (VAD) are increasing. We aimed to investigate whether patients with left VAD (LVAD) present with a better functional capacity compared to patients with biventricular support (Bi-VAD), late after device implantation.
Methods:Out of 23 patients with VAD (Berlin Heart GmbH, Germany) bridged to HTx, 11 patients with LVAD (9 males/2 females) and body mass index (BMI) 25.8±3.9, kg/m2, of mean age 38.4±15.1 years, classified according to Interagency Registry for Mechanically Circulatory Support (INTERMACS) scale as 1 (n=1), 2 (n=10) and 12 patients with Bi-VAD (12 males) and BMI 23.9±3.9 kg/m2 of mean age 37.3±14 years, INTERMACS 1 (=3), 2 (n=4), 3 (n=5) underwent cardiopulmonary exercise testing for measuring peak oxygen consumption (peakVO2), and the 6-minute walk test (6MWT), 6±3.7 months post-implantation.
Results:The LVAD group was matched with the BiVAD group for age, gender and BMI. Exercise capacity in patients with LVAD vs. patients with BiVAD as assessed by peakVO2 (14.9±3 vs. 16.3±3.8 ml/kg/min, p=ns), as well as exercise time (8.3±2.9 vs. 9.2±2.1 min), VE/VCO2 slope (37.8±7.4 vs. 40±5.3, p=ns), VE (45.8±12.9 vs. 55.8±15.9 L/min, p=ns), and VO2 at anaerobic threshold (11.6±4 vs. 12.5±4.6 ml/kg/min, p=ns) respectively, did not differ significantly. The 6MWT distance was comparable between LVAD patients and Bi-VAD patients (439±87 vs. 493±59 meters, p=ns).
Conclusion:There were no differences in neither maximal or submaximal exercise capacity between patients with LVAD and Bi-VAD long-term after device implantation, Our findings indicate that exercise capacity in patients with VAD is independent of univentricular or biventricular support.
P473
The effects of table tennis training on cardiac autonomic dysfunction in persons with spinal cord injury
G Vogiatzi1, E Kouidi1, V Tsimaras2, K Christoulas3, A Deligiannis1
1Aristotle University of Thessaloniki, Sports Medicine Laboratory, Thessaloniki, Greece
2Aristotle University of Thessaloniki, Laboratory of Developmental Pediatrics and Special Education , Thessaloniki, Greece
3Aristotle University of Thessaloniki, Laboratory of Ergophysiology-Ergometry, Thessaloniki, Greece
Cardiac autonomic nervous system (ANS) dysfunction is a frequent complication in people with spinal cord injury (SCI). Due to altered sympathetic-parasympathetic balance (reduced overall sympathetic activity below the level of injury and unopposed vagal outflow), cardiovascular complications, as dysrhythmias and cardiac arrest, are often. The effects of exercise training on ANS dysregulation in SCI remain unclear. Thus, the aim of the study was to examine the effects of a long-term table tennis program on cardiac ANS in quadriplegics. Fourteen males (aged from 32 to 47 yrs old) with chronic spinal cord injury (C6-C7 level) without other disease participated in the study. They were randomly divided into 2 groups: seven quadriplegics (Group A), followed a six-month program with table tennis, three times per week, while the other 7 (Group B), served as controls. Additionally, 7 healthy sedentary men (aged 40.0 ± 6.1 yrs old- Group C) were used as healthy controls. At baseline and the end of the study, all persons underwent 24hour ambulatory ECG monitoring for heart rate variability (HRV) measurements based on time- and frequency domain analysis and assessment of upper-limb exercise tolerance and muscle strength. In group A, HRV was continuously monitored during table tennis by a HR monitor (Polar S810i) to evaluate the acute ANS response to exercise.
Results:At baseline, there were no significant differences in long-term HRV indices between the two patient groups. On the other hand, SDNN was lower in group A compared to C (109.0±9.4 vs 146.5±8.8 ms, p<0.05), while the differences in the rMSSD, LF, HF and LF/HF weren't significant. At the end of the study, group A showed an increase in SDNN (116.7±6.5 vs 109.4±9.4 ms, NS), rMSSD (48.5±4.8 vs 41.2±6.2ms, p<0.05), LF (72.7±12.4 vs 56.9±8.4nu, p<0.05), HF (51.8±12.4 vs 39.7+±12.8 nu, NS) and a decrease in LF/HF (1.43±0.6 vs 1.40±0.4, NS) compared to the pre-training values. After training, resting upright posture short ANS measurements showed that the rMSSD and HF were decreased by 8.3% and 10.7% (p<0.05), while LF and LF/HF did not change significantly; as response to acute exercise, the reduction of rMSSD and HF and the increase of LF and LF/HF were significantly higher after training. Moreover, table tennis training significantly improved upper limbsmaximal exercise tolerance by 69.9% and muscle strength by 35.7%.
Conclusion:Our results indicate that a 6-month table tennis training program in quadriplegics has the potential to promote a better balance between sympathetic and vagal activity, mainly during upright posture at rest and exercise.
P474
The influence of different training modalities on the effect of exercise training in patients with chronic heart failure: a meta-analysis
T Vromen1, JJ Kraal1, N Peek2, G Van Valkenhoef3, J Kuiper4, HM Kemps5
1Dept of Medical Informatics, Academic Medical Centre, Amsterdam, Netherlands
2University of Manchester, Health e-Research Centre, Inst. of Population Health, Manchester, United Kingdom
3University Medical Center Groningen, Dept. of Epidemiology, Groningen, Netherlands
4University Medical Center Groningen, Dept of epidemiology, Groningen, Netherlands
5Maxima Medical Centre, Department of Cardiology, Veldhoven, Netherlands
Introduction:Studies have convincingly shown beneficial effects of exercise training (ET) on physical fitness and quality of life and to hospital admissions in patient with chronic heart failure (CHF). Aerobic exercise training for CHF patients is therefore strongly recommended in current guidelines. In recent years, there has been a debate in the literature about appropriate training intensities in aerobic ET. Previous systematic reviews indicated that the differences in outcomes of ET might not be caused by training intensity alone, but by other training parameters as well.
Topic: Sports cardiology
Purpose:To determine which ET parameter (aerobic training frequency, intensity, duration and volume) is the strongest determinant of exercise training effects on maximum oxygen uptake (pVO2).
Methods:A systematic search in EMBASE and MEDLINE was performed for papers published between 1 april 2007 and 1 september 2013, comparing ET with usual care or other training modalities in adult CHF patients. Only randomized controlled trials were included that reported peak oxygen uptake as an outcome measure. Univariate meta-regression analyses were performed on the following training parameters: training intensity (%pVO2), session duration (minutes), weekly session frequency, program duration (weeks), session energy expenditure (EE, intensity*duration), weekly EE (frequency*session EE) and total EE (program duration*weekly EE).
Results:Twenty-one trials were included, accounting for a total of 1093 patients. Overall, weekly session frequency appeared to be the best predictor for improvement in exercise capacity (p=0.0009), with 0,30 ml/min/kg increase in peak VO2 for every extra session per week (95% CI 0.12-0.47). Total EE (0,16 ml/min/kg 95% CI 0,06-0,26 per 100J/kg), weekly EE (0,97;0,31-1,6 per 100J/kg) and session intensity (0,69; 0,05-1,34 per 10% increase in exercise intensity) were also associated with increase in exercise capacity (p=0.0027, p=0.0039 and p=0,0347 respectively). For session EE, program duration, and session duration no association with exercise capacity was found. For all modalities there was little to none heterogeneity in the effect size (I2 ranging from 0 to 28%) indicating that there was little unmeasured confounding.
Conclusion:Weekly session frequency was the strongest predictor of change in peak oxygen uptake in CHF patients undergoing exercise training.
P475
Baseline titer of short physical performance battery and ten-meter walking speed determine six-minute walk distance above 300 meters after the ambulatory independent discharge for elderly PROgram
A Uehara1, H Obata2, Y Izumi1, H Watanabe2, T Izumi1
1Niigataminami Hospital, niigata, Japan
2Niigata University Graduate School of Medical and Dental Sciences, Department of Cardiovascular Biology and Medicine, niigata, Japan
Topic: Sports cardiology
Purpose:In countries such as Japan, which have an aging society and few births, there is a large population of elderly patients with frailty that requires repetitive hospitalization due to various diseases. With the Ambulatory Independent Discharge for Elderly PROgram (AIDE-PRO), patients are discharged from the hospital on achieving independent gait. We investigated the factors contributing to achieving a 6-min walk distance (6MWD) more than 300 m after the AIDE-PRO to return home-stay.
Methods:We evaluated 58 consecutive patients (mean age, 82 years; 31 women [53 %]) who were discharged on achieving independent gait, with a short physical performance battery (SPPB) score less than 12 points before the AIDE-PRO. The AIDE-PRO consists of stretching, lower limb muscle and balance strengthening, and aerobic exercises. The outcome assessment was SPPB score, isometric knee extension muscle strength (IKEMS), functional reach test (FRT), one leg standing time (OLST), 10-m walking speed (10MWS), and 6MWD before and after the AIDE-PRO.
Results:After 30 days of rehabilitation, the IKEMS, FRT, OLST, and 10MWS values improved significantly from 31 % to 35 %, 21 cm to 26 cm, 5 s to 12 s, and 0.77 m/s to 0.98 m/s, respectively. The balance test, gait speed test, and chair stand test scores of the SPPB significantly improved from 2.8 to 3.6, 2.2 to 3.0, and 1.9 to 2.8, respectively. As a result, the total SPPB score improved from 6.8 at baseline to 9.5 points after rehabilitation, and 13 patients (22 %) attained a perfect score. After the AIDE-PRO, 27 patients achieved a 6MWD of 284 m. These patients were divided into two groups according to their 6MWD after the AIDE-PRO. Group A comprised 13 patients with a 6MWD more than 300 m, and Group B comprised 14 patients with a 6MWD less than 300 m. Age and rehabilitation period was 78 years and 30 days, respectively, in Group A, and 83 years and 36 days in Group B, respectively, with no significant difference in both groups. Before the AIDE-PRO, IKEMS, FRT, OLST values did not significantly differ between two groups (Group A: 29 %, 26 cm, 12 s; Group B: 28 %, 20 cm, 3 s). The SPPB scores for Group A and Group B, respectively, were as follows: balance test, 3.4 and 2.6; gait speed test, 2.5 and 1.9; chair stand test, 2.6 and 1.9; total score, 8.5 and 6.4. Group A showed better SPPB scores than Group B, with a significantly higher total SPPB score. The 10MWS was significantly faster in Group A than Group B (0.91 m/s vs. 0.69 m/s).
Conclusions:The baseline titer of total SPPB score and 10-m walking speed determine achieving a 6MWD more than 300 m after the AIDE-PRO .
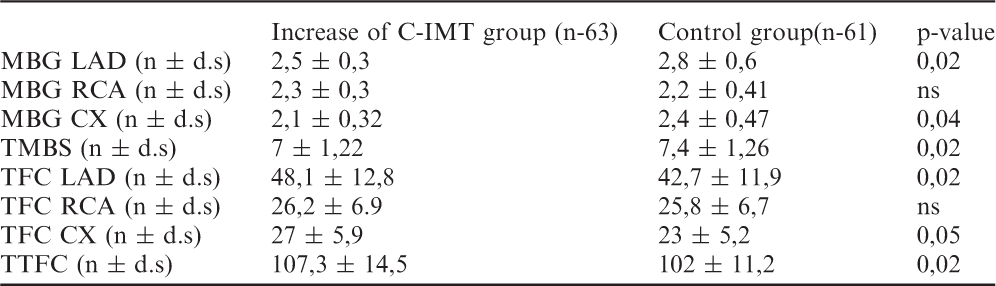
?variation in %
With Diastolic Dysfunction
Without Diastolic Dysfunction
Parameters
Before CR
After CR
? , %
p value
Before CR
After CR
? , %
p value
NT_proBNP ( pg /mL)
1173 ±1503
471 ±432
-35.2 ±43.5
0.021
462 ±543
157 ±154
-50.2 ±30.7
<0.001
pVO2 (mL/Kg/min)
23.3 ±7.3
25.2 ±26.9
11.9 ±27.6
ns
26.0 ±6.5
27.9 ±7.1
9.5 ±29.2
0.003
VE/VCO2 slope
26.7 ±5.9
26.8 ±5.4
-2.8 ±23.5
ns
25.6 ±5.1
24.9 ±4.4
-1.1 ± 16.1
0.048
LVEF (%)
46.8 ±12.9
49.0 ±11.7
9.3 ±29.4
ns
54.8 ±9.5
56.1 ±9.8
3.4 ±14.7
ns
GLS (%)
-14.9 ±2.9
-15.9 ±2.6
10.4 ±33.1
ns
-15.3 ±3.9
-16.5 ±3.9
16.8 ±18.1
0.049
E/ératio
27.2 ±54.9
13.0 ±9.7
-16.8 ±53.9
0.002
7.8 ±1.7
7.9 ±1.7
4.66 ±28.7
ns
P476
Impact of cardiac rehabilitation on diastolic dysfunction: is there a positive effect?
P Rio1, A Abreu1, R Soares1, S Aguiar Rosa1, T Pereira-Da-Silva1, A Viveiros Monteiro1, I Rodrigues1, M Afonso Nogueira1, S Silva1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Diastolic dysfunction is common in patients (pts) with coronary artery disease. Exercise training improves exercise capacity of these pts, primarily duo to peripheral adaptations. The contribution of left ventricular (LV) diastolic filling is not yet well understood. The aim of the present study is to evaluate the impact of cardiac rehabilitation (CR) in pts with diastolic dysfunction (WDD).
Methods:Retrospective analysis of consecutive pts with coronary artery disease (CAD) who underwent CR program (2004-2013), in a single center. Cardiopulmonary exercise testing (CPET), echocardiogram and blood tests were performed at baseline and after 36 exercise training sessions. Exercise sessions were performed in hospital, three times a week, 60 minutes duration. Peak oxygen uptake (pVO2), left ventricular ejection fraction (LVEF), global longitudinal strain (GLS), ratio early diastolic pulse wave Doppler and Tissue Doppler Imaging (E/e') and natriuretic peptides (NT_proBNP) were evaluated. Patients were divided and analysed according to diastolic function estimated by E/A ratio, E/e' ratio and left atria dimension.
Results:We analysed 169 pts, 83% male, mean age 57.2±10.4 years. There were 55 (33%) pts WDD and 114 (67%) without diastolic dysfunction (WODD). Comparing both groups, NT_proBNP decrease 35.2% in WDD vs 50.2% in WODD (p=0.03), GLS increase 16.8% in WODD vs 10.4% in WDD (p=0.045) and E/e' ratio decrease 16.8% in WDD vs and increase of 4.7 in WODD (p=0.03).
Conclusion:Patients with diastolic dysfunction achieved significant benefit in diastolic function, with a statistical significant decrease of E/e' ratio. On the contrary, they did not obtain greater increase in global longitudinal strain and reduction in NT_proBNP, comparing to patients without diastolic function.
P477
Neuroendocrine response to Heated water-based Exercise training on resistant hypertensive patients: a randomized controlled Trial (HEx trial)
L G B Cruz1, GV Guimaraes1, EA Bocchi1
1Heart Institute (InCor) - University of Sao Paulo Medical School, Sao Paulo, Brazil
Background:Heated water based EXercise training (HEx) is a new alternative intervention in cardiac rehabilitation, and it has been studied about its effects on cardiovascular adaptations; but still there is no data is about neuroendocrine effects of this training. This study examines the effects of HEx on neuroendocrine response in resistant hypertensive patients.
Methods:This is a parallel, randomized controlled trial. 125 nonconsecutive sedentary patients with resistant hypertension from a hypertension outpatient clinic in a university hospital were screened; 44 patients fulfilled the study requirements and had their blood analyzed for the concentration of plasma catecholamines (dopamine, adrenaline and noradrenaline), endothelin -1, nitric oxide (NO), plasma aldosterone concentration and plasma renin activity (PRA) than the patients were divided in two groups, one group was trained in a heated pool (32oC) for 12 weeks , 3 times a week; and the other group was the control group. The sessions were performed for 60 minutes and were consisted of callisthenic exercises and walking inside the pool. The control group was asked to maintain habitual activities. After 12 weeks all patients repeated the blood tests.
Results:44 patients (HEx n=28; control n=16) were randomized; there was no loss during the follow-up and no adverse events occurred during the study. HEx decreased plasma concentration of dopamine (from 145±88 to 26±21 ng/ml, p<0.0001), adrenaline (from 353±156 to 169±93 ng/ml, p=0.009), noradrenaline (from 720±255 to 307±137 ng/ml, p=0.001), andothelin-1 (from 42±14 to 26±8 pg/ml, p=0.003), aldosterone (from 94±48 to 77±22 pg/ml, p=0.006) PRA (from 35±14 to 3±3 mmHg ng/ml/H, p<0.0001); and increased NO (from 25±7 to 77±22 uM, p= 0.001).The control group after 12 weeks did not have any changes on blood analysis results.
Conclusion:HEx was able to improve important neuroendocrine adaptations in resistant hypertensive patients. These effects suggest that HEx may be a potential new therapeutic approach in these patients.
P480
The role of Pacemaker remote follow-up in early detection and management of lead complications and patient medical care.
O Al-Razo1, E Gonzalez1, M Alejandre1, T Represa1, J Silvestre1, JM Mesa1
1University Hospital La Paz, Department of Cardiac Surgery, Madrid, Spain
Introduction:In the recent years, several studies have demonstrated that (PM) remote follow-up is safe, cost effective and reliable in early detection of arrhythmia and lead complications. In this study we report our experience in PM remote follow-up and the impact of using this technology on patient's medical care.
Patients and methods:2200 patients with PM were included in the remote follow-up clinic between February 2008 and November 2014 (1000 patients with CareLink, Medtronic, 727 patients with Home monitoring, Biotronik, 285 patients with Merlin.net, St. Jude Medical and 188 patients with Latitude, Boston Scientific). They patients were completely followed up by remote monitoring after the third month post implant.
Results:396 (18%) arrhythmia alert were reported (atrial fibrillation and/or atrial tachycardia). In 20% of these alerts, a new onset atrial fibrillation was diagnosed. A complete event informs were sent to these patients to be delivered to their cardiologist. Thirty-seven alerts for lead dysfunction were received, most of which were due to lead impedance changes. Sixteen cases of lead displacement were diagnosed and one case of rupture of lead insulation.
Conclusions:This study demonstrates that PM remote follow-up is effective in early detection of lead problems and arrhythmias and thus plays an important role in the prevention of patient's morbidity.
P481
Telerehabilitation in coronary artery disease (TRIC-Study), 12 months data
K Wallner1, J Altenberger1, S Klausriegler1, B Kogler1, I Mairinger1, R Mueller1, R Rieder1, H Zauner1
1SKA-RZ Grossgmain (PV), Grossgmain, Austria
Topic: Sports cardiology
Purpose:The aim was to evaluate feasibility, efficacy and safety of home-based telerehabilitation following shortened inpatient cardiac rehabilitation in comparison to a regular inpatient cardiac rehabilitation program in patients suffering uncomplicated coronary artery disease (CAD).
Methods:This prospective non-randomised parallel group study assigned 45 male patients for shortened 2 weeks inpatient rehabilitation followed by a 10 weeks telerehabilitation program (TRG) versus 47 patients who completed a conventional 4 weeks inpatient rehabilitation program (CG). Outcome measures were assessed after 12 months using cardiopulmonary function (Watt (W)peak, Wpeak/kgBW(Bodywight), WVAT1(ventilatory aerobic treshold1), VO2peak/kg, VO2VAT1/kg, With L(lactate)2mmol/l, With L(lactate)4mmol/l), laboratory parameters (total cholesterol (TC), high density lipoprotein (HDL)-C; low density lipoprotein (LDL)-C; TC/HDL-C quotient)), physical parameter (body weight (BW); body mass index (BMI), waste circumference (WC), body fat (BF)).
Results:Baseline demographics were equally distributed between the groups, except age (CG younger). No adverse events were observed in both groups during rehabilitation. After 12 month in the TRG (n=41), Wpeak (+23,.1%; p<0.001), Wpeak/kgBW (+24.7%; p<0.001), WVAT1 (+11.2%; p=0.014), VO2peak/kg (+7.4%; p=0.008), and VO2VAT1/kg (+4.7%; p=ns) were increased. In the CG (n=45) only Wpeak and Wpeak/kgBW increased by +3.5% (p=ns) and +3.2% (p=ns) respectively. In contrast WVAT1, VO2VAT1/kg and VO2peak/kg decreased by -15.1% (p= 0.002), -11.1% (p= 0.006), and -1.3%(p= ns) respectively. The difference between TRG and CG was highly significant for VO2VAT1/kg (p=0.016), Wpeak (p=0.019), Wpeak/kg (p=0.005), and WVAT1 (p=0.002). In TRG concentrations of LDL-C (-22.7%; p< 0.001), TC (-14.5%; p< 0.001), TG (-17.2%; p=ns), and TC/HDL-C (-16.9%; p= 0.001) decreased significantly during the twelve months. HDL-C (+1.2%; p=0.087) did not increase statistically significant. In CG non of the laboratory parameters statistically significant changed. After 12 months except HDL-C all parameters showed a statistically significant difference between the groups in favour of the TRG. Physical parameters showed no statistical significant difference within and between the two groups after twelve months. Conclusions:Home-based telerehabilitation can be regarded as safe and feasible for patients with uncomplicated CAD. In addition we could show significant improvements due to physical fitness and change in risk factors in the TRG compared to regular four weeks inpatient rehabilitation.
P482
What is the impact of telemonitoring on the continuity of care for heart failure patients?
A Malhotra1, H Dhutia1, W Lewis1, M Papadakis1, J Ah-Fong1, L Mccloughan2, J Hanley2, P Fairbrother2, B Mckinstry2, H Pinnock2
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
2University of Edinburgh, Centre for Population Health Sciences, Edinburgh, United Kingdom
Topic: Sports cardiology
Purpose:Management of congestive heart failure (CHF) costs the UK health service £625 million per year with costs expected to rise worldwide as patient numbers increase along with a greater burden on resources. Telemonitoring (TM) aims to delivering a cost-effective, patient-centred service with increased continuity of care through the use of audio, video and other telecommunication technologies. The efficacy of TM is debated. This study investigates the impact of TM on the continuity of care from the perspective of patients with CHF and their health care providers (HPs).
Methods:NHS Lothian created a TM pilot service to monitor their CHF patients and assess its effects. A qualitative design was used to evaluate participants' views between June 2013-14. 18 patients and 5 HPs underwent interviews which were recorded, transcribed and analysed. The key themes of continuity of care to be assessed were reassurance and accessibility, trust, relationship continuity and management continuity.
Results:Reassurance and accessibility- Patient groups were positive about TM offering a sense of security and reassurance. Patients felt more involved with their management through the daily recording of their physiological parameters. HPs were positive about monitoring patients on a daily basis. There were concerns that TM may encourage patients to adopt a sick dependency role. Both groups responded positively about data accessibility with measurable quantitative data being transmitted directly to a healthcare professional. Trust- Both groups were positive about TM fostering trust between the HP and the patient. Relationship continuity- Patient groups were negative about relationship continuity. Many patients noted they would have preferred to have seen their own GP. HPs reported that TM would work better if they knew the patient. Management continuity- Patient groups were positive about the integration of technology as part of their management and found use of the technology to be relatively easy. HPs found there was insufficient information to adequately plan management. There was insufficient information about pre-existing decisions. A lack of communication between HPs and a lack of clarity as to leadership was noted.
Conclusion:Both groups acknowledged that TM had an overall positive effect on continuity of care with the management of people with CHF. Relationship continuity and management continuity issues need to be overcome to meet the objectives of the service. Further work is also required to ascertain the quantitative effects of TM on CHF and overall cost-effectiveness of the TM service.
P484
Heart rate variation during cardiopulmonary exercise testing in patients with heart failure: don't forget the basics
S Guerreiro1, A Ferreira1, M Mendes1
1Hospital de Santa Cruz, Lisbon, Portugal
Topic: Sports cardiology
Purpose:to assess the prognostic value of a novel index combining heart rate (HR) reserve and recovery in patients with heart failure undergoing cardiopulmonary exercise testing (CPET).
Methods:Retrospective, single-centre study of 144 patients with heart failure and depressed left ventricular ejection fraction (111 males, mean age 54±11 years) who underwent CPET between June 2009 and August 2013. Patients who were not taking beta-blockers and/or were not in sinus rhythm were excluded. Patients were classified in quintiles of HR reserve and HR recovery. Quintile categorizations were summed in a score ranging from 2 to 10. The prognostic value of this score was compared with classic CPET parameters: peak oxygen uptake (peak V02) and minute ventilation-carbon dioxide production relationship (VE/VCO2 slope). The primary endpoint was a composite of death from any cause or heart transplantation.
Results:During a median follow-up of 3.1 years (interquartile range 2.0-3.9), 22 patients died and 10 others received a heart transplant. The incidence of the primary endpoint was significantly higher for lower HR index scores (Fig1). In Cox regression analysis, the prognostic power of the HR index was not shown to be independent of peak V02 (HR 0.92; IC 0.77-1.10, p=0.37). Despite this, its discriminate ability as measured by the area under the ROC curve was good (AUC 0.71, 95%CI 0.62-0.81, p<0.001), and only tendentiously inferior to the discriminative ability of peak V02 (AUC 0.79, 95%CI 0.72-0.87, p<0.001), p=0.08 for the difference between the two AUCs.
Conclusions:Among patients with heart failure, the HR index score is a marker of bad prognosis. Our findings suggest that this simple non-invasive parameter can be used as an alternative to V02 measurements in settings where CPET is not available.
P485
Exercise evaluation in young adults after repaired coarctation of the aorta: is bicuspide aortic valve a threat?
A Monteiro1, A Abreu1, A Agapito1, P Rio1, SA Rosa1, I Rodrigues1, TP Silva1, MA Nogueira1, S Silva1, RC Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Background:Bicuspid aortic valve (BAV) is one of the most congenital cardiac conditions. In coarctation of the aorta (ACo), BAVs are common, but their relation with exercise hemodynamic response is unknown. The purpose of this investigation was to study the impact of BAV in successful surgical repaired ACo using exercise stress doppler echocardiography.
Methods:Thirty consecutive patients (51.9% male) were studied after ACo repair (age at repair 3.3+/-2.6 years) and underwent, at 30.1 ± 8.25 years of age, an exercise treadmill testing with echocardiographic examination. The following parameters were evaluated: peak and mean doppler gradients and velocities in ascendant and descendent aorta (at rest and at maximum stress).
Results:All patients underwent test exercise (15.93 ± 4.0 minutes) with no severe complications such as syncope, ischemic or arrhythmic events. Fifty percent of the patients had evidence of BAV (Group A). At maximum stress, Group A presented a significant increase in peak gradient and velocity in descendent aorta (respectively from 24.4 ± 10.8 to 50.5 ± 22.8; p<0.001 and from 2.36 ± 0.8 to 3.38 ± 0.9; p<0.001). In patients with tricuspid aortic valve (Group B), peak gradient and velocity in descent aorta also raised respectively from 22.1 ± 7.3 to 51 ± 16.4 (p<0.001) and from 2.17 ± 0.4 to 3.33 ± 0.8 (p=0.013). However, although an overall similar increase in doppler echocardiographic findings, when comparing both BAV and non BAV patients, no significant differences were found in descendent aorta parameters (?ak gradient 23.3±18.8 vs 32.6±17.5, p=0.998; ?ak velocity 0.65±0.7 vs 0.65±0.8, p=0.223). The same trend was verified in ascendant aorta values.
Conclusions:BAV in AoC patients was frequent. Despite BAV patients seem to have a smaller increase in aorta doppler parameters, this didn't seem to be different or more danger when compared to patients with normal aortic valves.
P486
Stroke in Chagas disease: impact of a rehabilitation program
A Souza1, HS Costa1, GR Sousa1, MMO Lima2, LL Gusmao1, F Almeida1, LAP Sousa1, MOC Rocha1, MCP Nunes1
1Federal University of Minas Gerais, School of Medicine, Postgraduate Course of Tropical Medicine, Belo Horizonte, Brazil
2Federal University of Jequitinhonha and Mucury Valleys, Diamantina, Brazil
Topic: Sports cardiology
Purpose:Regardless of cardiac manifestation, ChD is a well-defined risk factor for stroke. ChD and stroke are stigmatizing diseases and can determine important sequelae, so long-term rehabilitation becomes needed. This study aimed to investigate the effects of an aerobic training program on the functional capacity and quality of life (QOL) in chagasic stroke patients (ChSP), comparing with chagasic patients without stroke (ChPWS).
Methods:This was a prospective study, carried out at the University of Minas Gerais, Belo Horizonte, Brazil. The inclusion criteria included: ChD with or without stroke; 30 - 65 years; ability to walk for 20 minutes; clinical stability for at least 3 months. Patients were excluded if they present severe aphasia, pain or serious imbalance during gait, pacemaker or other cardiac, neurological or systemic disorders. The functional capacity evaluation was performed through the 6-minute walk test (6MWT), and the 6MWT distance was calculated. The Brazilian version of the 36-Item Short-form Health Survey (SF-36) questionnaire was used to measure patients' QOL. All volunteers, with or without stroke, participated in a 12-weeks aerobic training program conducted 3 times a week, supervised by physiotherapists. Each session was tailored to individual limitations and included 5-10 min warm up, 30 - 40 min walking, and 5 - 10 min cooling down. Training intensity was calculated using the Karvonen formula and gradual adjustments were done along the training program period in order to achieve target HR training intensity.
Results:Eleven ChSP and nineteen ChPWS were included. There was no diference between groups regarding age, sex and clinical conditions. The data were analysed for delta values (? = end - baseline). After intervention, both of groups had significant increases in functional and QOL parameters (p<0,05). Compared with the ChPWS, the ChSP showed more significant increases in QOL: ? domains general health (11,8 vs. 21,9; p=0,02), ? functional classification (12,6 vs. 20,5; p=0,02), ? domains general health (11,8 vs. 21,9; p=0,018), ? physical aspects (12,8vs. 20,1; p=0,03), ? general health status (12,1vs. 21,4; p=0,005) and ? vitality (11,2 vs. 22,9; p=0,000). There was no difference between ChSP and ChPWS in ? 6MWT distance (16,4 vs. 13,9; p=0,471), and ? pain (13,4 vs. 19,1; p=0,085), and ? social aspects (14,1 vs. 17,9; p=0,268), and ? emotional aspects (16,7 vs. 13,4; p=0,328).
Conclusion:In ChSP, aerobic training was safe and associated with a major improvement in functional capacity and QOL, in many aspects, more significant than ChPWS.
P487
High-intensity interval training in patients with cancer - a pilot study
LDT Trachsel1, HG Gottschalk1, CD Deluigi1, PE Eser1, MW Wilhelm1
1Bern University Hospital, Preventive Cardiology & Sports Medicine, Bern, Switzerland
Topic: Sports cardiology
Purpose:Cardiorespiratory fitness (peak VO2) is an important predictor for overall mortality in healthy subjects and patients with cardiovascular diseases and cancer. High-intensity interval training (HIIT) is a relatively new training modality that improves cardiorespiratory fitness. Superiority of HIIT to the established moderate intensity continuous exercise modality (MICE) has been demonstrated in cardiac patients. We investigated the effects of HIIT on peak VO2 in patients with cancer in an outpatient rehabilitation setting.
Methods:In February 2013, the ambulatory rehabilitation program at our institution was extended to cancer patients. In the first six months patients completed a 3-month program with 2 to 3 supervised sessions of MICE/week. After six months, HIIT was introduced in the program and patients performed MICE in the first month, followed by 2 months of HIIT. Data was analyzed retrospectively for the present study. Measurements included clinical status and cardiopulmonary exercise testing before start and after completion of the program. Relative changes in peak VO2 and work rate were compared between groups using independent t-tests or Mann-Whitney tests as appropriate.
Results:A total of 20 consecutive patients (14 females) with a diagnosis of cancer (breast cancer 50%, lymphoma 40%) were included in the analysis. 10 patients performed MICE and 10 patients HIIT. Compliance was comparable between groups with a mean of 30 sessions in the MICE group (83%) and 31 sessions (87%) in the HIIT group (p=0.53). There were no sex differences between the groups. Mean age tended to be younger in HIIT (42.4 vs. 49.4 years, p=0.08). Baseline values of BMI (24.6 kg*m-2 vs. 24.8 kg*m-2, p=0.92), peak VO2 (25.6±3.5 vs. 26.3±5.7 ml*kg-1*min-1, p=0.75), work rate (1.90±0.41 vs. 1.97±0.38 Watt*kg-1, p=0.71) and percentage of predicted work rate (85%±18%vs. 94%±23%, p=0.34) were comparable between groups. In HIIT, there was a significantly greater increase in peak VO2 (25% vs. 1%; p=0.001) and peak work rate (31% vs. 18%, p=0.03) over the training period, compared to MICE. No adverse events related to HIIT occurred.
Conclusion:In our small study, HIIT was well tolerated in cancer patients and led to a significantly greater improvement of cardiorespiratory fitness, compared to the more established MICE modality.
P488
P.U.E.D.E.S., a new approach for an old challenge in sports medicine.
M A Fernandez-Gomez1, D Cascado-Caballero2, J L Sevillano-Ramos2
1University of Seville, Sports Medical Unit. SADUS, Seville, Spain
2University of Seville, Robotics and Technology of Computers Laboratory, Seville, Spain
Topic: Sports cardiology
Purpose:Integrated into an online platform, an adapted and expanded version of the position stand from the EACPR (1) is presented, for the assessment of cardiovascular risk (CVR) in relation to the practice of physical activity (PA). This prototype considers the valuation of a wider population, including young people over 18 years and the full range of intensities of PA and sports.
Methods:A web platform has been created with multiple functions and roles to facilitate the cardiovascular (CV) and metabolic (M) evaluation in the field of sports medicine. The target population is students and staff of our University (N:50000). The module for the clinical evaluation is based on electronic versions, adapted from previously proposed self-administered questionnaires (Q). The aim is twofold: first, to control the level of PA using the international PAQ (IPAQ) long form; and second, to check the health status using both a PA Readiness Q (PARQ) adapted form and an expanded American Heart Association-American College of Sports Medicine (AHA-ACSM) form (1, 2), which includes personal history, CVR factors, and a more detailed family history, as indicated elsewhere (3). A number of functions have been implemented that automate the management and evaluation of the collected data, which ultimately generate recommendations, always based on scientific evidences. As reference, we use clinical practice guidelines (e.g. to estimate CVR or M risk (4)) and the positioning of Expert Groups (1, 2). Furthermore, based on the previously proposed algorithms (AL) to promote health in adults over 35 years through PA (1), we extend them to include young people over 18 years and to add other types of PA, such as high intensity or competitive sports.
Results:Adapted questionnaires and expanded decision AL, developed for sedentary and active subjects, are integrated into the web platform prototype (5). A first set of 53 subjects have used the platform and provided feedback about usability and acceptability issues. Their comments have been used to improve the site's friendliness and ease of use.
Conclusions:The modifications and adaptations performed on the decision AL allow an automated valuation and generation of recommendations focused on the practice of healthy PA, tailored to each subject. In addition, the platform would permit not only individual but also group or population assessments and early preventive actions on CV and M prevalent diseases.
P491
Cardiovascular preventive medication and achievement of treatment targets in patients with osteoarthritis: Results from the MUST-Heart study
S Rollefstad1, E Ikdahl1, N Oesteraas2, TK Kvien2, AG Semb1
1Diakonhjemmet Hospital, Preventive Cardio-Rheuma Clinic, Department of Rheumatology, Oslo, Norway
2Diakonhjemmet Hospital, Department of Rheumatology, Oslo, Norway
Topic: Sports cardiology
Purpose:Undertreatment and poor goal attainment of blood pressure (BP) and lipids in both primary and secondary prevention has been reported in the general population. Our aim was to evaluate cardiovascular (CV) primary and secondary preventive treatment and attainment of recommended goals in patients with osteoarthritis (OA) in the Musculoskeletal pain in Ullensaker STudy (MUST).
Methods:The MUST is a population-based postal survey and a comprehensive clinical examination of persons with self-reported OA (n=630), of which 438 fulfilled the American College of Rheumatology criteria for OA. In the MUST-Heart study, usage of primary and secondary CV preventive medication as lipid lowering agents (LLA), anti-hypertensive medication (a-HT) and anti-thrombotic medication (AT) (acetylsalicylic acid and dipyridamole) was recorded. Guideline recommended BP goal is =140/90 mmHg, and low density lipoprotein cholesterol (LDL-c) goals for primary/secondary prevention are =2.5/=1.8 mmol/L, respectively. Attainment of BP and lipid targets for patients on the respective medications were evaluated.
Results:Secondary or primary CV prevention was indicated in 72 and 26 patients, respectively. The female/male ratios 45/27 and 5/21 and the median (IQR) age was 68.5 (65.0, 75.8) years and 66.5 (65.0, 73.8) years. Total Cholesterol (TChol) was: 5.17 (1.25) (SD) mmol/L/5.97 (1.19) mmol/L, high density lipoprotein cholesterol (HDL-c): 1.49 (0.46) mmol/L/1.22 (0.29) mmol/L, LDL-c: 2.97 (1.06) mmol/L/3.82 (1.06) mmol/L, BP was 140.5 (18.7)/82.4 (8.3) mmHg/155.7 (14.5) mmHg/87.2/10.1 mmHg, for the secondary/primary prevention groups. Of the 72 patients with diagnosed CV disease, 38 (52.8%) were using LLA, 47 (65.3%) a-HT medication and 25 (34.7%) were on AT medication. Of the 125 patients (without CV disease) who had hypertension, 57 (45.6%) used a-HT medication. Of the 26 patients with a calculated CV risk by SCORE =5%, 2 (7.7%) used LLA.Of the patient who were using a-HT medication, BP goal attainment was 20/47 (42.6%) and 0/57 (0%) for patients in the secondary and primary prevention groups. Of all patients using LLA, patients with CV disease achieved goals for TChol were 12/38 (31.6%) and LDL-c: 9/38 (23.7%).
Conclusions:There was a substantial underuse of cardio-protective drugs in persons with OA in the MUST-Heart study, which resulted in poor attainment of recommended BP and lipid targets. The goal achievement of BP and lipids in patients with OA was even lower than what is reported for the general population.
P493
Markers of arterial stiffness according to daily monitoring and office measurement in patients with diabetes in combination with hypertension
V Oleinikov1, NV Sergatskaya1, LI Gusakovskaya1, NT Nagapetyan1
1Penza State University, Penza, Russian Federation
Objective:a comparative assessment of the indicators characterizing the structural and functional properties of the vascular wall in patients with type 2 diabetes mellitus (DM) and arterial hypertension (AH) and hypertensive patients without metabolic disorders.
Methods:The study involved 73 people aged 40 to 65 years. Group 1 included 46 patients with type 2 diabetes. Obligatory condition was the presence of hypertension of 1-2 degrees, the average age - 56,4 ± 8,6 years, body mass index (BMI) - 35,3 ± 5,9 kg/m2; systolic blood pressure (SBP) - 147,5 (140; 160) mm Hg, diastolic blood pressure (DBP) - 90 (80, 95) mm Hg. Group 2 included 27 patients with hypertension, the average age - 53,7 ± 9,0 years, BMI - 24,1 (23,2; 27,5) kg/m2; SBP - 145 (143; 157,5) mm Hg, DBP - 95 (90; 100) mm Hg. Patients were matched for age, sex, height, office SBP. Structural and functional properties of the large arteries were assessed by ambulatory blood pressure monitoring (ABPM) and rigidity by Vasotens technology. The mean daily values of the central (aortic) pressure: SBPpao, DBPao, PPao were determined. Among the stiffness parameters the augmentation index in the aorta (Aixao), the propagation time of the reflected wave (RWTT), stiffness index (ASI) and the maximum rate of blood pressure increase (dPdt)max were analyzed.
Results:The patients did not differ on the SBPao level: in diabetic patients - 126 (119; 139) mm Hg, AH - 129 (125; 133) mm Hg. In patients with DM the values of DBPao were significantly lower (80,9 ± 8,8 mm Hg), than in patients with hypertension - 88,9 ± 7,9 mmHg (p <0,01). PPao in the studied groups was 46 (41; 53) and 38 (35; 44) mm Hg, respectively (p <0.01). Among the parameters characterizing the stiffness of the peripheral arteries in diabetic patients the prevalence of ASI values (167 (149; 220) mm Hg) and (dPdt)max (637 (534; 764) mm Hg/s) has been reported, in contrast to those in subjects with hypertension (147,5 (132; 177), and 526 mm Hg (480; 627) mmHg/s, respectively) (p <0,01). Whereas the RWTT parameter in group 1 had significantly lower value (128,7 ± 11,04 ms), than in group 2 (143 (137; 149) ms) (p <0,01). Parameter Aixao in diabetic patients was 26,9 ± 14,7%, in patients with hypertension - 26,7 ± 12,1% (ns).
Conclusions:the observed differences in central hemodynamics and vascular stiffness in patients with type 2 diabetes mellitus in combination with hypertension compared with patients suffering from hypertension without metabolic disorders are due to severe structural changes of arteries of different caliber.
P494
Diabetes: the most important predictor of new cardiovascular events after acute coronary syndrome?
R Ferreira1, J Neves1, A Gonzaga1, M Bastos1, J Santos1
1Centro Hospitalar do Baixo Vouga, Cardiology, Aveiro, Portugal
Topic: Sports cardiology
Purpose:Coronary heart disease is a chronic condition and patients who have recovered from an acute coronary syndrome are at high risk for new events and premature death.
Methods:Retrospective observational analysis of 431 patients admitted on a coronary intensive care unit with acute coronary syndrome for 2 consecutive years. Patients were followed-up until the 31st october 2013 or until another event (new acute coronary syndrome, stroke, heart failure, arrhythmia or cardiac death).
Results:431 patients were included, 72.4% were male, with mean age of 67 ± 13 years, 27.6% with the previous diagnosis of Diabetes. During the mean follow-up of 22 ± 10 months, 73 cardiovascular events were recorded and 48 deaths, 15 of which were of cardiac cause. On Cox multivariate analysis adjusted to potential confounding factors (diabetes, hypertension, dyslipidemia, obesity and tabagism) only diabetes (with Hazzard Ratio of 0.61; IC 95% 0.368-1.011; p< 0.05) was sustained as an independent predictor of new cardiovascular events. Comparing diabetic versus non diabetic patients, diabetic had higher values of glycaemia on admission, serum creatinine, pro-B-type natriuretic peptide and C-reactive protein. They also had higher values ?128;??128;?of systolic blood pressure and heart rate on admission. Atrial fibrillation and electrocardiographic dynamic changes in the inferior wall were also more frequent in this group. Killip class IV (2.5% vs 1.6%), severe depression of left ventricle ejection fraction (11% vs 10%) and 3-vessel disease (32.6% vs 12.8%) were more prevalent in the diabetes group. Non-diabetic patients were younger and had higher values of hemoglobin, troponin I and total cholesterol.
Conclusion:Diabetes was the only cardiovascular risk factor that was sustained as a predictor of new cardiovascular events. Thus, patients with acute coronary syndrome present an opportunity for targeted screening for diabetes and institution of effective management strategies aimed to improve cardiovascular outcome.
P495
The experience of the "School of self-control for patients with type 2 diabetes" (SSCD2) at the outpatient stage
EN Martsynik1, LN Pastarus2, LD Kalashnikova3, MA Chukmasova4, VN Burchak2, IV Tyshchenko1
1SE Dnipropetrovsk medical academy, Dnipropetrovsk, Ukraine
2CE Dnipropetrovsk city clinical hospital 9, Dnipropetrovsk, Ukraine
3Dnipropetrovsk Regional Society of patients with diabetes, Dnipropetrovsk, Ukraine
Purpose:to study the importance of SSCD as a guide to action for patients (pts) with type 2 diabetes (D) on ways to improve the efficiency of treatment and quality of life (QL).
Methods:SSCD was organized in 2001 under the auspices of the Society pts with diabetes. Pts were informed about SSCD by district endocrinologists, during admission and through media. Lessons of 45-60 minutes once in 2 weeks in groups of 30-60 pts were held at different sites by leading endocrinologists and specialists in diabetic foot (DF) and retinopathy. The cycle of 6 lessons included lectures, questions and answers, the issuance of booklets, brochures, definition using glucometer glycemia (G) to all pts, training of calculation individual diets and correction of medication in different situations. Topics: the concept and diagnosis of D, self-control (SC), HbA1c monitoring, diet and physical activity in D, diabetic drug therapy and its correction, diagnosis and monitoring of chronic complications, the patient's behavior in unusual situations. All the participants with their consent were surveyed using specially designed questionnaire.
Results:during 10 yrs 2243 listeners were registered. Each year SSCD was visited by 223 ± 25 pts with D (36.6% men, 63.4% women, mean age 58.3 ± 3.4 yrs). 89.5% of participants - the inhabitants of Dnipropetrovsk, 10.5% - the inhabitants of the nearby districts. 60.8% of registered pts visited full course, 11.8% listened to course 2-3 times. After determining of G 39.8% of pts needed individual counseling of the doctor to correct medication and diet and about 3% required urgent hospitalization. All surveyed pts had raised awareness about D and assessed the usefulness of the training: 74.3% for self-construction diet, 81.2% for self-foot care and prevention of DF, 88.9% for the understanding of necessity of regular SC. 44.8% pts expressed a desire to continue learning. For many pts SSCD became a kind of Club where they shared their experiences of life with D. 65.2% of participants noted the positive socio-psychological impact of SSCD: the increasing interest in communication, improving mood, reducing negative attitudes towards D. 41.3% of pts noted: use of the acquired knowledge helps them better to live with D.
Conclusions:SSCD had demonstrated expediency of the work. Training in the SSCD had raised the awareness of pts about D, contributed to the understanding of their role in the health-care process and of the importance of SC to improve the QL. To improve the efficiency the work of SSCD should be systematic, constant, and innovative, with using educational and analytical tools.
P496
A contemporary health check-up as a one-time intervention with individual lifestyle coaching can substantially lower diabetes risk in patients with pre-diabetes - the PF study
J Scholl1, P Kurz2
1Dr. Scholl Prevention First GmbH, Prevention First R?im, R?im am Rhein, Germany
2Dr. Scholl Prevention First GmbH, Prevention First M?, R?im am Rhein, Germany
Topic: Sports cardiology
Purpose:A recent Cochrane meta-analysis concluded, that general health check-ups were useless. (1) The data that were used mainly stemmed from the 60s to 80s of the past century, when neither the knowledge nor the means of preventive interventions were comparable to the current possibilities. We examined the impact of a one-time contemporary health check-up on the risk of progression from pre-diabetes to diabetes.
Methods:Between 2001 and 2014, n=1852 men (age 46,0±6,4 years) und n=960 women (age 46,3±5,6 years) participated at least twice in a health check-up offered to them by their respective employer. All participants gave a written consent to the scientific evaluation of the check-up results. Details of the health check-up have been described elsewhere. Pre-Diabetes was defined according to the ADA Definition (IFG =100 mg/dl and/or HbA1c =5,7-6,4%). A separate analysis was done using only an HbA1c =6,0-6,4% and/or IFG =100 mg/dl. Patients who fulfilled the criteria for pre-diabetes received a motivational lifestyle coaching including an understandable explanation of the pathophysiology of insulin resistance and its relation to diet, exercise, and diabetes risk. All patients were provided with a individualized exercise prescription (endurance and resistance training) and an individual dietary counselling with the objective to follow a Mediterranean-style low-glycemic-load diet.
Results:744 of 1852 men (40,2%) and 248 of 960 women (25,8%) fulfilled the criteria for pre-diabetes. Within a follow-up of 3,9 years in men and 3,5 years in women only 2,55% of men and 0,81% of women with pre-diabetes progressed to type 2-diabetes. This translates into a very low progression rate of 6,5/1000 person-years in men and 2,3/1000 person-years in women. If HbA1c 6,0-6,4% was used instead of 5,7-6,4%, the respective rates were 7,2/1000 in men and 3,8/1000 in women. A recent meta-analysis of 70 prospective studies reported a much higher progression rate from pre-diabetes to type 2-diabetes of 35/1000 up to 70/1000 person-years depending on the definition used for pre-diabetes.(2) Conclusion:In this the evaluation of a contemporary health check-up as a one-time intervention with motivational lifestyle coaching we observed an exceptionally low progression rate from pre-diabetes to type 2 diabetes, which clearly demonstrates the effectiveness of this strategy for diabetes prevention.
P497
Prevalence of the cardiovascular risk factors in bulgarian female population
N Runev1, E Manov1, S Naydenov1, T Donova1
1UMHAT Alexandrovska, Sofia, Bulgaria
Objective:To evaluate the risk profile and the level of control of some modifiable cardiovascular risk factors (RF) in Bulgarian female population.
Methods:Pooled data from 3 cross-sectional studies, organized by the Working group of the Bulgarian Society of Cardiology on cardiovascular risk in women. These studies were performed between year 2011 and 2014, including consecutively a total number of 214 women, mean age 58.5±11.7 (22-87) years. The clinical investigations included: blood pressure (BP) measurement, waist circumference (WaC), height, weight and body mass index (BMI) calculation. All women completed a questionnaire, specifying the presence of cardiovascular risk factors and diseases as well as some demographic characteristics. Using a self-assessment test introduced by the National U.S Diabetes Association we assessed the risk for development of type 2 diabetes mellitus (DM) among the non-diabetic women.
Results:Arterial hypertension is the most prevalent cardiovascular risk factor present in 72.4% (n=152), followed by overweight/obesity – 63.9% (n=106), dyslipidemia – 31.0% (n=65), type 2 DM – 14,5,7% (n=31), smoking – 10.3% (n=22) and hormone-replacement therapy with oestrogenes – 4.2% (n=9). The mean value of the systolic and diastolic BP is 139.5±18.8 (90-194) and 86.9±12.1 (60-120) mmHg respectively. The mean value of BMI is 28.4±6.4 (18-51) kg/m2 and WaC – 95.4±15.8 (56-132) ?¼. The calculated risk for development of type 2 DM in the non-diabetic female population is 9.88±4.4 (0-20).
Conclusion:Arterial hypertension is the most prevalent RF for cardiovascular complications among the analyzed Bulgarian female population, followed by overweight/obesity and dyslipidemia. The risk for development of type 2 DM in the non-diabetic women is moderate to high. The control of the most common modifiable cardiovascular RF remains unsatisfactory despite the available non-pharmacological and pharmacological options.
P498
Mortality risk due to electrocardiographic disturbances in elderly Russian population
S Shalnova1, G Muromtseva1, A Kapustina1, A Deev1, Y Balanova1, E Tuaeva1, S Evstifeeva1, D Smirnov1, M Shkolnikova2
1National Research Center for Preventive Medicine, Moscow, Russian Federation
2Research Clinical Institute of pediatrics, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:to assess the prevalence of major and minor electrocardiographic (ECG) abnormalities, as well as their impact into all cause and CVD mortalities among Muscovites aged=55 years.
Methods:The data came from a population-based sample of 1876 Muscovites aged=55 years who participated in SAHR (Survey on Stress, Aging, and Health in Russia).During a median of follow-up period of 5.36 years, 332 deaths were identified. Standard 12-lead ECG was recorded. ECG abnormalities were divided into six groups (using Minnesota code (MC)): major QQS (MC: 1.1,1.2 without 1.2.8.), major ischemia (MC: 4.1,4.2, 5.1,5.2 without 3.1, 3.3), conduction defects (CD) (MC: 6.1,6.2,7.1), atrial fibrillation (AF) (MC:8.3) and minor QQS abnormalities (MC: 1.2.8, 1.3.-), minor ischemia (4.1- 4.4, 5.1-5.4 with 3.1, 3.3). Cox regression to estimate hazard ratios (HR) for an association between ECG abnormalities and CVD and total mortality was performed.
Results:The prevalence of major ECG abnormalities was slightly higher among men than among women (26.7% vs 22.4%, p <0.05), whereas minor ECG – in women (21.9% vs 17.5%, p<0.05). The most difference between sexes was found in groups of major QQS (8.1% vs 2.8%, p<0.01) in men and women, respectively. The prevalence of all abnormalities increased with age. While using Cox regression model with entire ECG block of ECG variables (age, sex-adjusted) for total mortality the following were significant. AF (HR 1.630, 95%CI: 1.096; 2,423), CD (3.017: 1.743; 5.219), major ischemia (1.610: 1.184; 2.189), minor ischemia (1.338: 1.009; 1.772).
Conclusions:The prevalence of major ECG abnormalities was slightly higher among men. AF and CD have much greater effect on mortality in comparison with middle-aged subjects.
Variables
RR
95%CI
p-level
Atrial fibrillation or flatter
1.837
1.142
2.956
0.0122
Conduction defects
3.163
1.589
6.298
0.0010
QQS MAJOR
1.736
1.135
2.653
0.0109
QQS MINOR
0.731
0.358
1.495
0.3906
ISCHEMIA MAJOR
1.707
1.150
2.533
0.0080
ISCEMIA MINOR
1.546
1.082
2.211
0.0168
P499
Age and sex differences of risk factors associated with obesity in Saint-Petersburg inhabitants.
A Orlov1, O Rotar1, M Boyarinova1, A Alieva1, E Dudorova1, V Solntsev2, E Baranova2, A Konradi1, E Shlakhto2
1Federal Almazov Medical Research Centre, Hypertension Department, Saint-Petersburg, Russian Federation
2Federal Almazov Medical Research Centre, Saint-Petersburg, Russian Federation
Objective:The aim of our study was to estimate age and sex characteristics of obesity-related risk factors (RF) in general population of St.Petersburg, Russia. Design and methods. As a part of all-Russian epidemiology survey ESSE-RF random sampling of 1600 Saint-Petersburg inhabitants 25-64 years stratified by age and sex was performed - (573 (36%) men and 1027 (64%) women). All subjects were stratified in 4 age decades: 25-35 (309 subjects (19,3%)), 36-45 (316 (19,8%)), 46-55 (457 (28,6%)) and 56-65 (518 (32,4%)) y/o. All participants signed informed consent and filled in the questionnaire regarding physical activity, education, and nutrition. Anthropometry (weight, height with body-mass index (BMI) calculation, waist circumference (WC)) was performed.
Results:The high education had 277 (47,3%) men and 504 (49,1%) women. No impact of educational level on behavioral RF was observed. Obesity was more often detected in females according to different WC criteria: 88 sm for females/102 sm for males - in women 667 (46%), in men 291 (30%) (?=30,7, p<0,001) and 80 sm for females/ 94 sm for males – 470 (66%) and 168 (51%) (?=41,4, p<0,001). No differences in obesity prevalence were found according to BMI criteria – in 178 (31%) women and 352 (35%) men. The increase of obesity with age was found: BMI - 1,6 kg/m2/decade ((?1,6, 95% CI 1,4 - 1,8), p<0,001), WC in women - 5,2 sm/decade (?5,2, 95% CI 4,5 - 6,0, p<0,001) and WC in men – 2,8 sm/decade (?2,8, 95% CI 1,8 – 3,6), p<0,001). Optimal level of physical activity (walking>300 minutes/day) was equally documented in both genders - 540 (61,2%) women and 286 (58,9%) men. It was higher in the oldest age group (301 (70%)), compared with any younger subgroup (p<0,001). Walking time/week increased in 30 min/decade (?30, 95% CI 13 – 46), p<0,001). Interestingly, no association between physical activity level and BMI or WC was found. Daily intake of sweets was recorded higher in women 539 (52,5%) than in men 228 (39,8%), (?=23,7, p<0,001); it was associated with obesity only in subjects older 45 y/o (by BMI, ?=12,7, p<0,001).
Conclusions:The increase with age of obesity prevalence and BMI and WC was observed, 2 times higher (by WC) in females. Education was not associated with lifestyle behavior. Surprisingly, physical activity lower in younger age groups, which may be connected with increased sedentarism in modern lifestyle in European population including Russia.
P500
The prognostic impact of antithrombotic drugs in acute coronary syndromes: the results of a National Registry database
D Caldeira1, I Cruz1, G Morgado1, AC Gomes1, C Martins1, H Pereira1
1Hospital Garcia de Orta, Department of Cardiology, Almada, Portugal
Topic: Sports cardiology
Purpose:The antithrombotic drugs are essential for the treatment of patients with Acute Coronary Syndromes (ACS). The availability of multiple drugs, enables a number of possible combinations that does not have robust evidence to support their use. In this work we intended to evaluate the impact of these drugs and their combinations on the prognosis of patients with ACS.
Methods:We used data from the ACS National Registry on consecutive patients registered between October 2010 and October 2013. We sought data about population characteristics, prior/inhospital use of antithrombotic drugs (antiplatelet and anticoagulant), and antithrombotic drugs prescriptions at discharge. The prognostic impact of these drugs and their most common combinations was evaluated in terms of mortality and cardiovascular (CV) hospitalization at 1 year. Data were analyzed using Cox regression to estimate the hazard ratio (HR) and 95% confidence intervals (95%CI).
Results:There were 8186 patients with ACS included in the National Registry. The inhospital mortality was 3.9%. The composite of mortality and CV hospitalization at 1 year was 22%, with 16.4% of the events owing to CV hospitalizations. About 60 % of the patients were not taking any antithrombotic drug prior to the index event. The absence of antithrombotic drugs was more common in patients with ACS and ST-segment elevation (STEMI) [76.5 %] compared to patients with ACS without ST-segment elevation (NSTEMI) [49.2 %]. Evaluating all combinations of antithrombotic drugs, it was found that the strongest predictor of 1-year mortality was the previous use of acetylsalicylic acid (HR 1.34, 95%CI 1.01-1.78) or other antiplatelet drugs, after multivariable logistic regression analysis. Regarding the composite outcome of mortality and CV hospitalization within 1 year, prior dual antiplatelet therapy (HR 1.39, 95%CI 1.03-1.88, p=0.03), and the inhospital use of dual antiplatelet plus Glycoproteins IIbIIIa inhibitors plus Unfractionated Heparin plus Enoxapation, showed significant association with this composite endpoint (HR 1.89, 95%CI 1.09-3.31, p=0.025 ). This latter antithrombotic drugs combination was associated with increased risk CV readmission after discharge (HR 3.36, 95%CI 1.47-7.68, p=0.004).
Conclusions:About one fourth of ACS patients with STEMI and 50% of patients NSTEMI had antithrombotic drugs previous to the index event. Patients that received prior single or dual antiplatelet therapy were associated to significantly increase of the risk death and CV readmission.
P502
Education status as a predictor in the 10-year (2004-2014) all cause mortality and cardiovascular disease incidence, among Acute Coronary Syndrome patients, in Greece.
V Notara1, D B Panagiotakos1, C Pitsavos2, Y Kogias3, P Stravopodis4, G Papanagnou5, S Zombolos6, C Stefanadis2
1Harokopio University, Athens, Greece
2Hippokration Hospital, University of Athens, Athens, Greece
3Cardiology Clinic, General Hospital of Karditsa, Karditsa, Greece
4Cardiology Clinic, General Hospital of Zakynthos Island, Zakynthos, Greece
5Cardiology Clinic, General Hospital of Lamia, Lamia, Greece
6Cardiology Clinic, General Hospital of Kalamata, Kalamata, Greece
Topic: Sports cardiology
Purpose:To investigate the association between education status and 10-year risk for Acute Coronary Syndrome (ACS) and all-cause mortality.
Methods:From October 2003 to September 2004 a sample of 6 Greek hospitals was selected and almost all consecutive 2,172 ACS patients were enrolled. In 2013-14, the 10-year follow-up (2004-2014) was performed in 1,918 participants (88% participation rate). Education status was classified as low (<9 years of school), intermediate (9-14 years) and high (>14 years). Results:The low–to–high education status all cause mortality rate was 2.1-to-1 (p<0.001); the 10-yr incidence of CVD was higher in the low education status as compared with the middle and high (42% vs. 30% vs. 35%, p<0.001); no gender-by-education group interactions on the investigated outcomes were observed. Moreover, patients in the highest education group were more physically active, had better financial status and were less likely to have hypertension, diabetes and ACS, compared to those with the lowest educational level (p<0.001); when the aforementioned patients' characteristics were accounted for, together with lifestyle habits, no mediating effect as regards the significance of education status on all-cause mortality and ACS incidence was observed.
Conclusions:Low educated ACS patients were at higher risk for death or recurrent events, irrespective of their clinical and lifestyle characteristics. Nevertheless, the highly educated patients should not be considered as entirely protected due to their social status; public health policies should be targeted on different social groups to eliminate the overall burden of cardiovascular disease morbidity.
P503
Differences in prevalence of depressive symptoms and other cardiovascular risk factors between urban and general population.
J Piwonski1, T Zdrojewski2, A Piwonska1, M Rutkowski2, P Bandosz2, Z Gaciong3
1National Institute of Cardiology, Warsaw, Poland
2Medical University of Gdansk, Gdansk, Poland
3Medical University of Warsaw, Warsaw, Poland
Topic: Sports cardiology
Purpose:In many worldwide populations there was a difference in territorial prevalence of classical risk factors. The urbanization can multiply the risk of prevalence of cardiovascular risk factors in the urban population. We analyzed the CVD risk factors profile of residents of the capital of Poland in comparison to general adult Polish population.
Methods:The data on Warsaw population (1081 persons; 870, aged 20+, examined in 2012 in the frame of WAW-KARD study and 207 persons, aged 20-74, examined in 2011 as a part of EHES study). The data on general population came from NATPOL 2011, a representative sample of Polish population (N=2413, aged 18-79, screened in 2011). Questionnaire, physical examination and laboratory data were collected.
Results:Analyzing major CVD risk factors we found hypertension to be much more prevalent in Warsaw residents - 42% (54% in men and 44% in women) than in general population - 32% (respectively 35% and 31%), the same with increased (=5.0mmol/l) total cholesterol level that was found in 77% of Warsaw residents (76% in men and 79% in women) vs 62% in general population (61% in men and 63% in women). Also mean total cholesterol concentration was higher in Warsaw population (men-5,4mmol/l, women-5,5mmol/l) than in general population (men-5,1mmol/l vs 5,2mmol/l). The opposite situation was observed in smoking habit that was more prevalent in general population [16% of regular smokers among Warsaw residents (19% in men and 15% in women) vs 27% in general population (respectively 32% and 24%)]. Both analyzed populations did not differ in obesity (27% in both) and diabetes prevalence (respectively 6% and 5%). Besides, Warsaw residents presented more often depressive symptoms compared to general population, especially women (men: 28% vs 23%; women: 46% vs 36%).
Conclusions:Big city residents presented more cardiovascular risk factors compared to general population, more often had hypertension, hypercholesterolemia and depressive symptoms compared to the general population.
Baseline mental cumulative summary score
1st quartile n=50 in %
2nd quartile n=50 in %
3rd quartile n=50 in %
4th quartile n=51 in %
p-value
Rehospitalisation during 12 months
48
34
23
24
0.019
HADS-Anxiety=8, during 12 months
58
46
20
10
0.000
Blood pressure < 140/90 mmHg, 12 months
62
53
68
82
0.02
LDL cholesterol, 12 months
50
30
45
41
0.41
HbA1c < 6.5%, 12 months
92
80
91
84
0.32
Waist M/F < 102/88 cm, 12 months
39
57
58
70
0.004
Smoking at admission
54
49
42
22
0.001
Physical activity=30 min = 5 days/week at baseline
36
48
42
76
0.000
P504
Challenges in researching CVD inequalities between Aboriginal and non-Aboriginal Australians - examples of trusted approaches that do not always work
JM Katzenellenbogen1, D Derrick Lopez1, P Bradshaw1, FM Sanfilippo2, THK Teng1, MW Knuiman2, MST Hobbs2, SC Thompson1
1The University of Western Australia, Western Australian Centre for Rural Health, Perth, Australia
2The University of Western Australia, School of Population Health, Perth, Australia
Topic: Sports cardiology
Purpose:Using 3 separate studies, we illustrate how age-standardisation, Global Registry of Acute Coronary Events (GRACE) risk scores and multiple regression were unable to adequately elucidate inequalities in cardiac disease and care between Aboriginal and non-Aboriginal Western Australians.
Methods:Study 1, a cohort incidence study, used linked hospital admissions and death data to determine disparities in age-standardised incidence of myocardial infarction (MI) between the two populations aged 25-74. Study 2 assessed the performance of the GRACE risk score for predicting mortality in Aboriginal acute coronary syndrome (ACS) cases using clinical data from medical notes and linked mortality records. In Study 3, linked data and multiple regression modelling were used to control for demographic, co-morbidity and admission factors, to investigate disparities in transfers to urban hospitals for rural Aboriginal MI patients. The impact of these factors on rate ratios was assessed through progressive adjustment of covariates in regression models (Table).
Results:Study 1: The age-standardised Aboriginal to non-Aboriginal incidence rate ratio for MI (25-74 years) was 4.4, yet the rate ratio was 16.4 for 25-4 years, reducing with age to 2.7 for 65-74 years. Study 2: The mean GRACE scores and crude mortality were lower for Aboriginal ACS patients, with evidence of under-estimation of the risk of death to 6 months from hospital discharge. Study 3: see Table.
Conclusions:Age-standardisation diluted the inequality in MI incidence. The dominance of age in GRACE models means that risk may be underestimated given the younger age of Aboriginal cases. Adjustment through progressive regression models explains disparities in access to services, leading to interpretations of ?128;?no difference' when the inequalities lie in the dissimilar distributions of risk factors. Researchers should use statistical tools critically when studying inequalities in cardiac health and care between main and disadvantaged populations.
P505
Economic crisis influences adherence to medication and determines all-cause mortality and cardiovascular (CVD) prognosis among Acute Coronary Syndrome patients, in Greece.
V Notara1, D B Panagiotakos1, C Pitsavos2, Y Kogias3, P Stravopodis4, G Papanagnou5, S Zombolos6, Y Mantas7, C Stefanadis2
1Harokopio University, Athens, Greece
2Hippokration Hospital, University of Athens, Athens, Greece
3Cardiology Clinic, General Hospital of Karditsa, Karditsa, Greece
4Cardiology Clinic, General Hospital of Zakynthos Island, Zakynthos, Greece
5Cardiology Clinic, General Hospital of Lamia, Lamia, Greece
6Cardiology Clinic, General Hospital of Kalamata, Kalamata, Greece
7Cardiology Clinic, General Hospital of Chalkida, Chalkida, Greece
Topic: Sports cardiology
Purpose:To investigate the impact of the recent economic crisis on medication adherence and its potential long-term effect on the management of co-morbidities among Acute Coronary Syndrome (ACS) patients.
Methods:From October 2003 to September 2004, a sample of six Greek hospitals was selected and almost all consecutive 2172 ACS patients were enrolled. In 2013-14, the 10-year follow-up was performed in 1,918 participants (88% participation rate). Adherence to medical treatment was recorded through self-reports and patients' financial status was classified as low (<9.000?) moderate (<18.000?), good (<28.000?) and very good (>48.000?).
Results:During the 10-year of follow up, the overall all-cause mortality was n=703 (32.4%) (31.6% in men, 34.8% in women, p=0.17); causes of death were AMI 52.8%, stroke 8.3%, other CVD 8.3%, cancer 8.7% and the rest 21.9% were due to other causes. The overall-cause mortality for the "low" financial status patients was 29.4 % vs 17.6% of the "very good" financial group (p<0.001); while the 10-year CVD incidence rate was 31.4% vs 39.2% (p=0.22), respectively. 38% of the "low" financial status patients reported poor compliance due to economic restraints compared to "very good" financial group (20.8%). Accordingly, 23.8% of the "low" financial status patients have replaced drugs to more affordable vs 12.2% of the "good" financial group; whereas satisfaction with the public health care services was higher among "good/very good" financial groups as compared to "low/moderate" groups.
Conclusions:Decreased medical compliance is an important clinical and public health issue. Discontinuation of medical treatment results in adverse disease prognosis, increased mortality rates and impose a large economic burden in healthcare services among societies. Adherence involves a multi-dimensional approach that encompasses behavioural and social interventions. There is no argument that management of medical adherence in ACS patients should be a priority in health policy agenda regarding secondary prevention strategies.
P506
N-3 LC PUFAs in infant formula and blood pressure in early childhood
LPM Pluymen1, CSPM Uiterwaal1, GW Dalmeijer1, HA Smit1, CK Van Der Ent2, L Van Rossem1
1University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
2University Medical Center Utrecht, Department of Pediatric Respiratory Diseases, Utrecht, Netherlands
Topic: Sports cardiology
Purpose:The protective effect of breastfeeding on risk levels for cardiovascular diseases (CVD) might be explained by its content of n-3 long chain polyunsaturated fatty acids (LC PUFAs). Since 2007, most infant formulas are supplemented with these fatty acids. We assessed whether children who received supplemented formula had a lower blood pressure than children who received unsupplemented formula.
Methods:We used the ongoing WHeezing Illnesses STudy LEidsche Rijn (WHISTLER), a birth cohort that included children who were born between 2001 and 2011. Data on infant feeding was obtained by questionnaire. At age 5 (currently: all children born before May 2007), blood pressure was measured. We performed linear regression analyses on 202 children who had complete data on type of formula feeding and blood pressure. Analyses were adjusted for predictors of blood pressure.
Results:5 year old children who received infant formula with n-3 LC PUFAs (n=15) had a lower systolic (-3.68 mmHg, 95% CI -7.67, 0.32) and diastolic ( -2.32 mmHg, 95% CI -6.32, 1.67) blood pressure (adjusted for smoking during pregnancy, birth weight and gestational age), compared to children who received unsupplemented formula (n= 187). After additional correction for BMI, the association with systolic blood pressure was slightly attenuated (-3.05 mmHg, 95%CI -6.93, 0.83) while the association with diastolic blood pressure remained the same.
Conclusions:These results suggest a protective effect of n-3 LC PUFAs in infant formula on blood pressure in early childhood. Further follow-up will increase power to draw firmer conclusions on whether the protective effect remains.
P507
Self-reported physical activity is associated with cardio-pulmonary exercise testing parameters in a large population-based cohort from Northeast Germany
M Bahls1, R King1, S Gross1, T Ittermann2, M Doerr1
1University Medicine of Greifswald, Internal Medicine B, Greifswald, Germany
2University of Greifswald, Institute for Community Medicine, Greifswald, Germany
Introduction:Increasing physical activity (PA) in the general population is an important tool for the prevention of cardiovascular diseases. Increased PA is believed to improve cardiopulmonary exercise capacity. Cardiopulmonary exercise testing (CPET) is the gold standard for assessing physical fitness. For large population-based cohorts CPET applicability is limited because of its expensive and time consuming nature. Thus, questionnaires are often used to measure PA behavior. Unfortunately, very few of these questionnaires have been validated against physiological parameters of CPET. We measured PA behavior with a questionnaire in a large population-based cohort from Northeast Germany and related the results with maximal oxygen consumption (VO2peak) and oxygen consumption at the anaerobic threshold (VO2@AT).
Methods:Cross-sectional data of 1,708 subjects (49% male; age: 25 – 85 years) from the follow-up of the Study of Health in Pomerania (SHIP-1) were used for analysis. PA behavior was assessed using an adapted Baecke questionnaire. VO2peak and VO2@AT were measured during standardized CPET on a cycle ergometer using a modified Jones protocol. All adjusted models were corrected for sex, age, body mass index and smoking status. An adjusted linear regression was fitted to scores related to voluntary [sports score (SS), sports index (SI), and leisure time index (LTI)] as well as involuntary PA scores [work index (WI)].
Results:SS [? 138.24 (95%-CI: 117.08; 159.39) ml/min], SI [? 197.99 (95%-CI: 171.76; 224.22) ml/min] and LTI [? 129.00 (95%-CI: 99.12; 159.88) ml/min] were significantly positively associated with VO2peak and VO2@AT [SS: ?2.04 (95%-CI: 1.76; 2.32) ml/min/kg; SI: ? 2.97 (95%-CI: 2.62; 3.31) ml/min/kg; LTI: ? 1.99 (95%-CI: 1.60; 2.39) ml/min/kg]. A significantly inverse relationship was found between WI and VO2peak [? -44.46 (95%-CI: -79.15; -9.76) ml/min] as well as VO2@AT [? -0.51 (95%-CI: -0.97; -0.05) ml/min/kg].
Conclusion:Scores from the adapted Baecke questionnaire were strongly related with VO2peak as well as VO2@AT. Therefore, this questionnaire may be used in large population-based cohorts to assess PA behavior as a marker for cardiopulmonary exercise capacity. Interestingly, Baecke scores based on leisure time and voluntary PA had a positive relationship, while items asking about PA at work had an inverse association with cardiorespiratory fitness. Consequently, increasing voluntary PA is the key to prevent future cardiovascular diseases.
14
Greater excess risk of all-cause mortality and vascular events in women than in men with type 1 diabetes: a systematic review with meta-analysis
SAE Peters1, RR Huxley2, G Mishra2, M Woodward1
1University of Oxford, The George Institute for Global Health, Oxford, United Kingdom
2University of Queensland, Brisbane, Australia
Background:Studies have suggested that the mortality rate associated with type 1 diabetes differs between women and men. We performed a meta-analysis to provide the most reliable estimates of any sex differences in the effect of type 1 diabetes on risk of all-cause and cause-specific mortality.
Methods:PubMed MEDLINE was systematically searched for all studies published between January 1, 1966 and March 24, 2014. Eligible studies had to have reported sex-specific estimates of the standardized mortality ratio (SMR) associated with type 1 diabetes either for all-cause mortality or cause-specific mortality. Random effects meta-analyses with inverse variance weighting were used to obtain sex-specific SMR and their pooled ratio (women:men) for all-cause mortality, and mortality due to coronary heart disease, stroke, cardiovascular disease, renal disease, cancer, and accident and suicide associated with type 1 diabetes.
Results:Data from 23 studies including 93,846 individuals and 6,434 events were included. The pooled ratio of the women: men SMR for all-cause mortality was 1.43 (95% CI: 1.19-1.72), for incident stroke 1.37 (1.03-1.81) and for renal disease 1.44 (1.02-2.05). For coronary heart disease events the sex difference was more extreme; the pooled ratio of SMR was 2.54 (95% CI: 1.80–3.60). There was no significant evidence of a sex difference for mortality associated with type 1 diabetes from cancer, or from accident and suicide.
Conclusion:Women with type 1 diabetes have more than a 40% greater excess risk of all-cause mortality, and double the excess risk of vascular events, compared with similarly affected men.
P508
Educational inequalities in receiving PCI are influenced by patient's age: A CVDNOR project
E Sulo1, O Nygard2, SE Vollset1, G Sulo1, J Igland1, G Egeland3, M Ebbing3, GS Tell1
1University of Bergen, Department of Global Public Health and Primary Care, Bergen, Norway
2Haukeland Hospital, Institute of Medicine, University of Bergen, Department of Heart Disease, Bergen, Norway
3Norwegian Institute of Public Health, Department of Health Registries, Bergen, Norway
Topic: Sports cardiology
Purpose:Health outcomes are associated with socioeconomic inequities which are also influenced by in inequities in receiving treatment. We aimed to explore possible educational inequities in receiving percutaneous coronary intervention (PCI) among patients with an incident (first) acute myocardial infarction (AMI) and whether inequities vary by age.
Methods:– All hospitalized AMI patients aged 35-89 years in Norway during 2001-2009 were obtained from the Cardiovascular Disease in Norway project. Information on highest attained education was obtained from The Norwegian Education Database and categorized into primary, secondary and tertiary. Educational inequities in receiving PCI were explored using Poisson regression analysis. An interaction between age and education was found (p<0.01), analyses were therefore stratified by age. Results are expressed as relative risk (RR) and 95% CI of receiving PCI treatment for secondary or tertiary versus primary (reference category) education.
Results:Of 104,836 patients hospitalized with an incident AMI [mean age (SD) 71.1 (12.7) years; 37.3% women), 30.2% received PCI within 28 days. Overall, patients with secondary or tertiary education had higher rates of PCI compared to those with primary education only [RR=1.12, 95% CI; 1.10 - 1.14 and RR=1.21, 95% CI; 1.17 - 1.24, respectively]. Educational inequities (both for secondary versus primary and tertiary versus primary comparisons) were associated with increasing age.
Conclusion:– Middle-aged and elderly patients with secondary or tertiary education had higher PCI rates compared to those with primary education only. Further studies should evaluate whether such differences are explained by differences in risk factors and disease severity.
Education inequities in receiving PCI
P509
Expected effect of ESC recommendations on diet and physical activity, on CAD attack rate in northern Spain: the REGICOR Study.
IR Degano1, M Grau1, I Subirana1, J Vila1, R Elosua1, J Marrugat1
1Hospital del Mar Medical Research Institute (IMIM), Barcelona, Spain
Purpose: To estimate the effect of ESC recommendations on diet and physical activity (PA) on coronary artery disease (CAD) attack rate in a European region with low CAD risk.
Methods:The CASSANDRA model, based on the Framingham-REGICOR CV risk function, was used to estimate CAD attack rate until 2025. The model was applied using the demographic distribution of the REGICOR population (Girona, Spain), the prevalence of CV risk factors at baseline (2005), the probable trend of CV risk factors until 2025, and the effect of diet and PA recommendations on hypercholesterolemia and hypertension prevalence. The latter was obtained by multiple linear regression, assuming the maximum expected effect of recommendations on blood pressure and LDL cholesterol to the candidate population.
Results:CAD attack rate is expected to increase in Girona until 2025 (267 to 298/100,000 in men, and 75 to 84/100,000 in women, 4th scenario Figure). If those not following current recommendations on diet and PA did so, a smaller increase would be expected (267 to 279/100,000, and 75 to 81/100,000) based on the decrease of hypercholesterolemia and hypertension prevalence (3rd scenario Figure). In men, this reduction mimics the expected by the probable trends on diabetes and smoking prevalence (-3.8% and -1.85%, 2nd scenario Figure). In women, the observed reduction would compensate the expected increase (75 to 87/100,000) by the probable trends on diabetes and smoking prevalence (3.3% and 3.6%).
Conclusions:Current diet and PA recommendations are predicted to reduce CAD attack rates in a low risk European region. In women, this reduction would compensate probable unfavorable trends on diabetes and smoking. The effect of diet and PA recommendations in European regions with higher CAD risk would probably be larger.
Predicted CAD attack rate in Girona
P510
Is the hypertriglyceridemic-waist phenotype important in coronary heart disease prediction? A cohort Norway and CVDNOR Linkage Study
G Egeland1, J Igland2, O Nygard3, G Sulo2, GS Tell2
1Norwegian Institute Of Public Health, The Cardiovascular Registry, Bergen, Norway
2Dept of Global Public Health and Primary Care, Bergen, Norway
3Haukeland University Hospital, Bergen, Norway
Topic: Sports cardiology
Purpose:To evaluate the utility of the hypertriglyceridemic-waist phenotype in the prediction of coronary heart disease.
Methods:Men (n=55,560) and women (n=60,551) participants of regional Norwegian health surveys (Cohort Norway) who were free of heart disease at baseline (1994-2003), were followed through 2009 by record linkages to The Cause of Death Registry and hospital discharge diagnoses through the CVDNOR project. Hazard ratios (HR) and 95% confidence intervals (CI) for acute myocardial infarction (AMI) associated with the phenotype was evaluated in multivariate Cox regression adjusting for conventional risk factors: baseline age, daily smoking, systolic blood pressure (mm Hg), self-reported diabetes, HDL-C and nonHDL-C (mmol/L), and frequency of alcohol consumption.
Results:During a mean follow-up of 11.5 yrs, 2,538 men and 1,086 women developed an AMI. Prevalence of an enlarged waist (>102 cm for men, and >88 cm for women) increased from the lowest to highest quartile of triglycerides for men (4.9% to 22.5%) and women (6.5% - 42.1%; P for trend < 0.01). The presence of an enlarged waist and elevated triglyceride (>1.7 mmol/L) was associated with a HR for AMI of 1.68 (95% CI 1.48-1.90) for men and 1.95 (95% CI 1.66-2.29) for women compared to those with normal waist and triglyceride level after adjusting for age, smoking and time since last meal. However, when considering all conventional risk factors no significant association was observed between the phenotype and AMI.
Conclusion:The phenotype had no utility beyond that of conventional risk factors in predicting AMI. Similar to metabolic syndrome, we foresee limited practical applications of the hypertriglyceridemic-waist phenotype in the clinical management of patients or in population-based risk prediction algorithms.
P511
4-second exercise test: normative values for healthy adults aged 18 to 81 years old
CG Araujo1, CL Castro2, JF Franca2, PS Ramos3
1Federal University of Rio de Janeiro, Heart Institute Edson Saad/CLINIMEX, Rio de Janeiro, Brazil
2Exercise Medicine Clinic - CLINIMEX, Rio de Janeiro, Brazil
3Faculty of Medical Sciences - SUPREMA, Therezinha de Jesus Hospital, Juiz de Fora, Brazil
Topic: Sports cardiology
Purpose:Physiological reflexes primarily modulated by vagus allow heart rate to decrease and to increase rapidly after a deep inspiration followed by fast limb movements. These are the physiological basis of the 4-s exercise test (4sET) that has been pharmacologically validated (Clin Autonom Res 1992) for the evaluation of vagal modulation on the cardiac chronotropism. The aim of the study was to establish reference values for the 4sET results in healthy adults.
Methods:Revising 4sET data from 1994 to 2013 and after application of rigid inclusion/exclusion criteria, we obtained a sample of 1,605 healthy adults (61% men) aged between 18 and 81 years old. In the 4sET, a cardiac vagal index (CVI) was obtained by calculating the ratio between the duration of two electrocardiogram RR-intervals: 1) after 4-s of a fast full inspiration and immediately before start to pedal the cycle and 2) at the end of 4-s of fast unloaded (no resistance added) cycling.
Results:CVI was negatively related to age (r=-.33; p<.01) and the linear regression's intercepts and slopes were similar to men and women (p>.05) and so, the results for subjects of both genders were grouped for further analysis. Considering the heterocedasticity and the skewness of CVI distribution as related to age, it was preferable to report the reference values as percentiles to eight different age-groups (years): 18-30 (N=282), 31-40 (N=449), 41-45 (N=260), 46-50 (N=239), 51-55 (N=128), 56-60 (N=110), 61-65 (N=76) e 66+ (N=61). It was found that CVI median values progressively declined from 1.63 to 1.24.
Conclusions:Availability of CVI's age-percentile reference values would possibly facilitate a broader clinical application of the 4sET, a simple, valid and safe tool to assess the vagal modulation of the chronotropic response.
P512
Ivabradine increases haemodynamic exercise performance after cardiac transplantation : a prospective study
J Jaussaud1, MA Billes1, H Douard1
1Hospital Haut Leveque, Bordeaux-Pessac, France
Introduction:Cardiac graft denervation induces permanent sinus tachycardia that can be reduced with If channel antagonist Ivabradine. We aim to investigate the impact of long term Ivabradine treatment on cardiopulmonary performance in heart transplant recipients.
Methods:This prospective cross-over study included 16 patients (12 males; 53± 8 years) transplanted since 5 ± 4 years with stable sinus rhythm and normal graft systolic function. Each patient performed a cardiopulmonary exercise test after a 3 months period without and after 3 months of Ivabradine therapy (5 mg bid) in a randomized order.
Results:Heart rhythm (HR) at rest, at first ventilatory threshold and at peak exercise were significantly reduced (99±5 bpm to 77±7 bpm (p < 0.001); 123±9 bpm to 103±11 bpm (p < 0.001) and 151± 9 bpm to 134±11 bpm (p<0.001)). A trend to an improvement of peak aerobic (VO2 max) and exercise performance (from 20± 5 to 21±5 ml/kg/min and from 110± 33 to 116± 43 watts -p=ns-) and at ventilatory threshold (14±3 to 15±5 ml/kg/min -p=ns-) were observed. VE/VCO2 slope was stable (from 35± 6 to 36± 5 - p = ns-). Nevertheless, peak oxygen pulse was significantly increased by Ivabradine therapy from 46 +/- 6 % to 55± 8 % of theorical value -p = 0.03- assessing a probable improvement of stroke volume during exercise. No side effect nor significant changes in immunosuppressive drug dosages were detected during treatment periods. Blood pressure were not statically changed during exercise measurements.
Conclusion:Despite a slight but not significant improvement in oxydative and exercise capacities, chronic Ivabradine therapy in heart transplant recipients induces a significant increase of peak exercise stroke volume assessed by oxygen pulse. This could be explained by a significant reduction of HR and then a longer left ventricular diastolic filling time during exercise.
P514
Seasonal changes of 24-hour arterial stiffness parameters in two regions of the Russian Federation. Results of the cohort study.
V M Gorbunov1, MI Smirnova1, MM Loukianov1, SA Boytsov1, DA Volkov1, AD Deev1, YN Koshelyaevskaya1
1National Research Center for Preventive Medicine, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:The arterial stiffness variability may be one of the causes of blood pressure seasonal variations in hypertensive patients. The investigation of this problem in Russia deserves particular interest due to great contrasts in climate conditions across different regions. The aim of the study was to assess the dynamics of arterial stiffness (winter vs. summer) in two sites of Russia – Ivanovo ("north") and Saratov ("south").
Methods:We included patients from general population who visited ambulatory clinics for various reasons. The main inclusion criterion was office blood pressure 130/85-139/89 mm Hg or long-term antihypertensive therapy. Ambulatory blood pressure monitoring (ABPM) was performed twice: in winter (December-February) and in summer (June-August). The interval between ABPMs was 6 months±7 days. The selection criteria for ABPM records were: duration =23.5 hours =56 readings per 24 hours. The ABPM waveforms were analyzed by an automatic algorithm calculating the central pulse wave parameters from the peripheral pulse wave.
Results:1423 patients completed the first visit - 641 from Ivanovo (mean age 52±9 years, 244 men), 782 from Saratov (mean age 58±12 years, 449 men). The data of 745 patients with adequate quality of both ABPMs were analyzed. We found no seasonal or intraregional differences for pulse wave velocity (see table). At the same time, the values of both augmentation indices were higher in winter.
Conclusions:Our results show the decrease of 24-hour arterial stiffness associated with higher temperature. Further individual analyses of these data, as well as prospective studies in this field, are needed.
PWV - pulse wave velocity, AIx - Augmentation index, ao - aortic, b - brachial, s - summer, w - winter, * - p<0,05 (w vs. s), *** - p<0,001 (w vs. s), ^^^ - p<0,001 (Ivanovo vs. Saratov), ^^^^ - p<0,0001 (Ivanovo vs. Saratov)
Parameter (M±SD )
Ivanovo
Saratov
PWVw m/s
11,6±1,4
11,7 ±7,4
PVWs m/s
11,6 ±1,9
11,6 ±4,8
AIxbw %
-17,0 ±21,7
-12,6 ±22,3^^^
AIxbs %
-19,9 ±23,5*
-10,8 ±35,2^^^^
AIxaow %
21,0 ±12,3
24,4 ±14,6^^^^
AIxaos %
18,6 ±13,4***
24,2 ±15,3^^^^
P515
Prognosis masked hypertension in five years
I Osipova1, A Miroshnichenko2, O Antropova1, N Pyrikova1, A Zaltsman2
1Altay State Medical University, Barnaul, Russian Federation
Objective:explore prognosis masked hypertension in men with occupational stress without cardiovascular disease (CVD).
Materials and Methods:A total of 99 drivers and their assistants. Conducted identification of hypertension and masked hypertension. The survey was conducted at intervals of five years. The masked hypertension determined from the stress test "Mathematical expense." The test was positive for growth in systolic blood pressure (sBP) > 7% and/or increment of heart rate > 10%. Identified 2 groups: the first group - a man with a masked hypertension (n = 40, age 42,8 ± 9,8 years); 2nd group - men with normal blood pressure (BP) (n = 59, age 42,3 ± 8,4 years).
Results:In both groups, according to stress test a marked rise in BP and heart rate. The highest values ?128;??128;?of BP and heart rate were the men of the 1st group. Important growth indicators, since it was he who reflects stress reactivity examined. In men, the first group compared with the second stress test on the increase sBP was 2.2 times higher (p < 0,001) increase in heart rate 2.3 times higher (p < 0,001). Increase in diastolic BP (dBP) in the 1st group was higher by 24% (p < 0,05). Risk factors in the 1st group compared with the second: a history of CVD met 2,2 times more often (? = 9,22, p < 0,002) (58% in the 1st group and 27% in the 2nd group); smoking status 1,8 times more often (frequency 77,5%) (? = 11,9, p < 0,0005); abdominal obesity is 2,3 times more often (? = 6,69, p < 0,001) (42.4% in the 1st group and 18.6% in the 2nd group); Hypercholesterolemia was defined more by 2,3 times (? = 10,07, p < 0,001) and was 55%. After 5 years, have been re-examination of the two groups of men with a diagnosis of hypertension and masked hypertension. For 5 years, hypertension was detected in 25% (10 of 40) - all of these men belonged to the group of individuals with masked hypertension. After 5 years, the stress test was positive in the same men as in the first survey, which indicates the constancy of stress reactivity hemodynamics.
Conclusions:The incidence of hypertension in individuals with masked hypertension within 5 years is 25%. Application of a stress test "Mathematical account" allows to diagnose in the early stages of hemodynamic changes and start timely prevention. Stress-reactivity is stable hemodynamic changes in the cardiovascular system and in the presence of additional risk factors such as smoking, hypercholesterolemia, and abdominal obesity, realized within five years hypertension.
P516
Circadian blood pressure profile in patients with decompensated chronic pulmonary heart in combination with arterial hypertension.
N Aidargalieva1, A Teleusheva1
1Kazakh National Medicine University, Almaty, Kazakhstan
The purpose:This study examined the circadian blood pressure profile in patients with decompensated chronic pulmonary heart (dCPH) disease in combination with arterial hypertension (AH) of the 1st and 2nd degrees using ambulatory blood pressure monitoring (ABPM).
Materials and Methods:102 patients were studied using ABPM. The mean age was 65,6 ± 2,9 years. The patients were divided into 3 groups: the first group - 36 patients with dCPH of functional class (FC4) (NYHA) and combined with AH of the 1st degree RF4, second – 36 patients with dCPH of FC4 (NYHA) associated with AH of the 2nd degree RF4, 3rd control group included 30 patients with dCPH FC4 (NYHA).
Results:Patients with dCPH have an increase of night diastolic blood pressure (DBP) to 80,05±2,7mm.Hg (normally 75 mm.Hg) (p<0,05), which is likely due to increase of pulmonary hypertension and the absence of nocturnal physiologic blood pressure decrease, which may be a sign of the formation of the so-called "pulmonary" arterial hypertension. At association of AH 1 and 2 degree the increase of night DBP was higher (86,05±1,7mm.Hg and 100,1±1,8 mm.Hg) (p<0,01), than in patients with dCPH, which was possibly due to a combination of "pulmonary" diastolic hypertension and superimposed arterial hypertension. In patients with AH the time indices significantly increase, which testify to marked impact of load falling on target-organs not only due to an increase of blood pressure, but also to decompensation of cardiopulmonary failure. So, time index of systolic BP (TISBP) in 1st group in daytime increased up to 65,7 ± 4,7% and in 2nd group up to 87,4 ± 2,7% (p <0.05). Time index of DBP (TIDBP ) was up to 43,5 ± 4,9 (p <0.01) in patients in 1st group, and 74,1 ± 3,0% (p <0.01) – in 2nd group. In the night in 2nd group TISBP made 93,05 ± 4,3% (p <0.01), in 1st group - 77 ± 4,8%. TIDBP at night was equal to 90,9 ± 4,3% (p <0.01) in the 2nd group. In 1st group this index was equal to 79,5 ± 8,1%. Mean pulse pressure was increased up to 63,83 ± 1,3 mm Hg (p <0.01) in 2nd group, that was 15% higher than in the 1st group (norm of PBP is 53 mm Hg). The magnitude of the morning rise of DBP in 2nd also increased, it was 10% above the norm reaching 40,3 ± 3,7 mm Hg (p <0.01).
Conclusions:The result revealed that the features of hypertension in patients with decompensated chronic pulmonary heart disease is a significant increase of night DBP, increase of pulse pressure and the value of morning rise in DBP, the increase of the load on the target organs. All above-mentioned may lead to an increased risk of cardiovascular complications.
P517
Serum neurokinin b levels in newly diagnosed non-dipper hypertensive patients
C Dursun Akkoyun1, A Akyuz1, A Seref1
1Namik Kemal University Faculty of Medicine, Tekirdag, Turkey
Topic: Sports cardiology
Purpose:Cardiovascular diseases are more common in patients with non-dipper hypertension (NDHT) compared with those with dipper hypertension (DHT). The purpose of this study is to evaluate the serum neurokinin B levels in DHT and NDHT patients.
Methods:The study population consisted of newly diagnosed hypertensive patients who were not under antihypertensive treatment. A total of 77 patients were evaluated with ambulatory blood pressure monitoring and divided into two groups as NDHT (n=42) and DHT (n=35). Plasma neurokinin B levels were measured with ELISA method.
Results:Serum neurokinin B levels were significantly higher in the NDHT group compared with the DHT group (254(180-888) pg/mL and 207(116-752) pg/mL, respectively; p=0.024). There is a positive correlation between the mean nighttime systolic blood pressure and plasma neurokinin levels (r=0.590; p<0.001). On regression analysis, neurokinin B level was found to be only related to mean nighttime systolic blood pressure (Unstandardized ? ?2.02 ±9.59; p<0.001). Conclusion:In conclusion, plasma neurokinin B level is higher in patients with NDHT indicating an unfavorable cardiovascular prognosis, and it can be used for the diagnosis and the follow up of the NDHT patients.
BP: blood pressure, bpm=beats per min. ?he difference between systolic BP in nighttime and daytime
Nondipper Hypertension (n=42)
Dipper Hypertension (n=35)
P value
Daytime systolic BP, mmHg
145±15
144±13.5
0.321
Daytime diastolic BP, mmHg
91±11
92±10.5
0.550
Nighttime systolic BP, mmHg
141±18
125±11
0.039
Nighttime diastolic BP, mmHg
87±11
80±9.5
0.253
?ystolic BP
3.6(0-9)
13(10-23)
<0.001
?iastolic BP
5.5(1-10)
15(11-28)
<0.001
Heart rate, bpm
85.3±10.7
83.6±11.2
0.496
Daytime heart rate, beats/min
85.3±10.7
83.6±11.2
0.496
Nighttime heart rate, beats/min
68.3±10.3
67.6±11.4
0.694
Neurokinin B, pg/ml
254(180-888)
207(116-752)
0.024
P518
The changes of systemic inflammation markers in women with arterial hypertension depending on reproductive age
OM Bilovol1, LR Bobronnikova1, IA Ilchenko1
1L.T.Malaya Institute of Therapy, Clinical Pharmacology, Kharkiv, Ukraine
Topic: Sports cardiology
Purpose:To establish the relationship between the markers of systemic inflammation and cardiovascular parameters in women with arterial hypertension (AH) of different reproductive ages.
Methods:The study involved 86 women with stage II hypertension (mean age 52.4 ± 2.42 years) with different reproductive function according to STRAW classification. The following data were analyzed: C-reactive protein (CRP), interleukin-6 (IL-6), estradiol, echocardiography, the carotid intima-media thickness (CIMT), endothelium-dependent vasodilation (EDVD) of the brachial artery, ambulatory blood pressure monitoring (ABPM). The control group included 20 healthy women (mean age - 51.6 ± 0.8 years).
Results:The levels of CRP and IL-6 in women with AH were 42% and 45% higher than the ones in the control group (CRP: 4.68 ± 0.14 mg/ml, control group 2.12 ± 0.06 mg/ml; p <0.05; IL-6: 8.76 ± 0.27 ng/L, control group 4.16 ± 0.08 ng/L; p <0.01). The increasing age of women with AH was characterized by elevation of systemic inflammation markers (early and late reproductive age in comparison with the control group: CRP 24% and 39% higher, IL-6 30% and 51% higher, respectively). Estradiol levels weakly correlated with IL-6 (r = -0.27, p <0.05) in women with premenopause. The moderate correlation between estradiol and CRP, IL-6 levels was found in women with postmenopause (r = -34, r = -0.40, p <0.01), respectively. The indexes of systemic inflammation were associated with changes of the cardiovascular parameters in women with hypertension and postmenopause: the level of IL-6 correlated with myocardial mass index, CIMT and EDVD of brachial artery (r = 0.29, r = -0.34, r = -0.37, p <0.01, respectively), the CRP level correlated with CIMT and EDVD values (r = 0.38, r = -0,35, p <0.01, respectively). At the same time no correlation was found between pro-inflammatory markers and ABPM indexes.
Conclusions:The activation of systemic inflammation can be considered as a pathogenetic factor of adverse influence of menopause on the cardiovascular system in women with arterial hypertension.
P519
Insufficient knowledge of adults in Poland on criteria of arterial hypertension and its complications. Results of the NATPOL 2011 Survey
K Suligowska1, M Gajewska2, J Stokwiszewski2, P Bandosz1, Z Gaciong3, B Wojtyniak2, M Rutkowski1, D Cianciara2, B Wyrzykowski4, T Zdrojewski1
1Medical University of Gdansk, Department of Prevention and Education, Gdansk, Poland
2National Institute of Cardiology, National Institute of Public Health - National Institute of Hygiene, Warsaw, Poland
3Medical University of Warsaw, Department of Internal Medicine, Hypertension and Angiology, Warsaw, Poland
4Medical University of Gdansk, Department of Hypertension and Diabetology, Gdansk, Poland
Background:Arterial hypertension is one of the most widespread cardiovascular disease risk factors. Among the basic conditions of effective prevention, detection and treatment is appropriate knowledge in the general population about hypertension.
Material and methods:The analysis was based on the results obtained in the research program NATPOL 2011. The survey covered a representative sample of adults in Poland: 2413 randomly selected subjects aged 18–79 years [1245 females (F) and 1168 males (M)]. Rated answers to the two open questions on upper limits of normal blood pressure and complications of untreated hypertension were assessed and calculated with regard to age, gender, education and place of residence. Statistical analysis was performed using multivariate logistic regression. To simplify the analysis of results, for upper limits of normal blood pressure were taken: 139–140 mm Hg and 89–90 mm Hg, for systolic and diastolic blood pressure, respectively Results:Studies indicate that in Poland knowledge of blood pressure within normal limits is small. In terms of age (18-39 years; 40-59 years; 60-79 years) only 5.5%; 10.8%; 9.6% W and 5.9%; 7.8%; 6.1% M answered the questions correctly. Considering education (basic/essential; average; higher) percentage of W providing correct answers was 4.8%; 9.5%; 10.4%, and the percentage of M 3.4%; 9.4%: 8.4%. Furthermore, there was a very large discrepancy between the declared and actual knowledge of Poles, on the upper limits of normal blood pressure (for W: 79.4% vs. 8.4%; for M: 74.8% vs. 6.7%). Among all respondents in 2413 only 3 persons (0.1%) reported fully correct criteria HTN. Among the most frequently mentioned by respondents HTN complications were heart disease (69.8%), and stroke or cerebral ischemia (66%). In very little is known relationship between untreated HTN, and renal failure (11%) and blurred vision (7.7%). The study showed no significant differences in the knowledge W and M on the knowledge of the upper limits of normal blood pressure and complications of untreated HTN. Exceptions were: stroke (W: 72.1%; M: 59.6%), kidney damage (W: 14.4%; M: 7.4%) and blurred vision (W: 9.1%; M: 6.2%), where the women showed significantly better knowledge.
Conclusions:Knowledge of Poles about HTN criteria and complications that can be caused untreated HTN is insufficient. Therefore, it is necessary to conduct intensive educational activities in this field, and the results should provide guidance for the planning and implementation of these activities.
P522
Lipid abnormalities remain high among hypertensive patients with stable CHD: results of the Dyslipidemia International Study (DYSIS) II Russia
RG Oganov1, V Kukharchuk2, AK Gitt3, B Ambegaonkar4, V Ashton4, M Horack3, D Lautsch5, P Brudi4, O Maneshina6
1State Research Centre for Preventive Medicine, Moscow, Russian Federation
2Institute of Clinical Cardiology named after A.L. Myasnikov of the Federal State Institution, Moscow, Russian Federation
3Stiftung Institut fur Herzinfarktforschung, Ludwigshafen am Rhein, Germany
4Merck Sharp & Dohme Corp., Whitehouse Station, United States of America
5MSD, Wien, Austria
6MSD, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:Despite treatment with lipid lowering therapy (LLT), patients with coronary heart disease (CHD) and hypertension continue to have elevated lipid abnormalities putting them at risk for future cardiovascular events. We aim to identify the prevalence of lipid abnormalities and unmet needs among hypertensive patients with stable CHD in Russia currently on LLT.
Methods:DYSIS II is a multicenter, observational cross-sectional chart review conducted from November 2012-July 2013 in 93 outpatient care centers in Russia. Eligible adult patients had a documented history of CHD (past acute coronary syndrome (ACS) events >3 months before enrollment), full lipid profile available 0-12 months prior to enrollment, on LLT for =3 months or not treated at all, and were not participating in randomized clinical trials involving medication. Patient characteristics, risk factors, treatment patterns, and laboratory values were collected. LDL-C lipid target achievement was assessed based on local guidelines. Patients were identified as having hypertension based on data collected through the study case report form.
Results:Among 567 hypertensive stable CHD patients (74.8% male, mean age 62.5 ± 9.3 years), 95.2% had hypercholesterolaemia, 80.1% history of ACS, 71.9% previous percutaneous coronary intervention or coronary artery bypass graft, 61.6% left ventricular hypertrophy, 53.5% family history of CHD, 40.9% congestive heart failure, and 18.6% type 2 diabetes mellitus. 93.7% (n=531) of patients were on LLT (99.4% statin and 9.2% non-statin), with only 11.3% achieving LDL-C <70 mg/dl. Mean atorvastatin equivalent dose was 21 ± 13 mg/day, 8.7% of treated patients received combination therapy with 2.1% receiving ezetimibe plus statin.
Conclusion:Approximately 89% of LLT treated hypertensive patients with stable CHD in Russia did not achieve the recommended LDL-C target. Additional effective lipid lowering strategies are needed among these very high risk patients to prevent future cardiovascular events.
LLT Treated Patients n=531
Low density lipoprotein (LDL) cholesterol
106.9 ± 35.3 mg/dl
Total cholesterol
178.8 ± 40.8 mg/dl
Triglycerides
141.0 ± 70.3 mg/dl
Non-HDL cholesterol
133.3 ± 39.7 mg/dl
P523
Pleiotropic effects of rosuvastatin in patients with chronic obstructive pulmonary disease and dyslipidemia
E Samorukova1, G Rosliakova2, T Adasheva1, V Zadionchenko1
1Moscow State Medical and Dental University, Therapy and family medicine, Moscow, Russian Federation
2City Hospital of St. Vladimir, laboratory diagnostics, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:to analyze the 3-Hydroxy-3-Methyl-Glutaryl Coenzyme A (HMG-CoA) reductase inhibitor rosuvastatin influence on chronic low-grade systemic inflammation, endothelia dysfunction and clinical current in patients with chronic obstructive pulmonary disease (COPD).
Methods:we investigated 60 patients men (age 64 ± 7,6 years) with COPD II-III stages (Global Initiative for Chronic Obstructive Lung Disease 2011) in remission period. The patients were without myocardial infarction, stroke, coronary artery disease. We used of a risk estimation system such as SCORE (Systematic Coronary Risk Estimation) to estimate total cardiovascular risk our patients. A calculated SCORE was 11.31±4 (high and very high risk). The patients were divided into 2 groups. One group (40 patients) received rosuvastatin 5-10 mg during one year. The other group was control (20 patients). The target level for low-density lipoprotein-cholesterol (LDC-?) was = 1,8 mmol/l. The basic therapy COPD did not change. The patients used the combination of anticholinergic agents (ipratropium bromide, tiotropium bromide) with beta-2-adrenomimetic fenoterol. High sensitivity C-reactive protein (hs-CRP), vascular cell adhesion molecule type 1 (VCAM-1) were estimated before and after the treatment period. We analyzed spirometry (severity of airflow limitation), quantity of exacerbations. The symptoms of COPD, health status were analyzed using the St. George's Respiratory Questionnaire (SGRQ) before and after the rosuvastatin treatment.
Results:all patients reached target values LDC-?. Hs-CRP decreased from 4.5 [3,3; 8,77] mg/l to 3,2 [1,2; 4,1] mg/l (p<0,001). VCAM-1 – marker of endothelial dysfunction decreased from 1066,6 [870; 1381] ng/ml to 795,2 [(670; 1020] ng/ml (p<0,001). The symptoms activity of COPD decreased from 76,3 ± 23,1 to 60,8±11,3 (p<0,05). There was a 21% decrease of COPD exacerbations (p < 0,001). Forced expiratory volume in 1 second (FEV1) 5.2% increase was revealed (p=0,002). The control group did not have statistically significant dynamics in a year.
Conclusions:rosuvastatin has anti-inflammatory and endothelial protective effects, improves lung function, and reduces the exacerbations number in patients with COPD. It is important because chronic systemic inflammation and endothelia dysfunction are basic mechanisms of vascular impairments and development of cardiovascular diseases in patients with COPD.
P524
Rosuvastatin induced carotid plaque regression in patients with inflammatory joint diseases: The RORA-AS study
S Rollefstad1, E Ikdahl1, J Hisdal2, IC Olsen3, I Holme4, HB Hammer3, GD Kitas5, TR Pedersen6, TK Kvien3, AG Semb1
1Diakonhjemmet Hospital, Preventive Cardio-Rheuma Clinic, Department of Rheumatology, Oslo, Norway
2Oslo University Hospital, Aker, Section of Vascular Investigations, Oslo, Norway
3Diakonhjemmet Hospital, Department of Rheumatology, Oslo, Norway
4Oslo University Hospital, Ullevaal, Department of biostatistics, epidemiology and health economics, Oslo, Norway
5Dudley Group NHS Foundation Trust, West Midlands, United Kingdom
6Oslo University Hospital, Ullevaal, Centre of Preventive Medicine, Oslo, Norway
Topic: Sports cardiology
Purpose:Patients with rheumatoid arthritis (RA) and carotid artery plaques (CP) have increased risk of acute coronary syndromes. Statin treatment with low density lipoprotein cholesterol (LDL-c) goal < 1.8 mmol/L is recommended for patients with CP in the general population. In the ROsuvastatin in Rheumatoid Arthritis, Ankylosing Spondylitis and other inflammatory joint diseases (RORA-AS) study, the aim was to evaluate the effect of 18 months intensive lipid lowering with rosuvastatin on change in CP height.
Methods:Eighty-six patients (60.5% female) with CP and IJD [RA (n=55), ankylosing spondylitis (n=21) and psoriatic arthritis (n=10)] were treated with rosuvastatin to obtain LDL-c goal. CP height was evaluated by B–mode ultrasound.
Results:Age was 60.8±8.5 years (mean±SD). At baseline, median number and height of CP was 1.0 (range 1-6) and 1.80 mm (IQR 1.60, 2.10). Change in CP height after 18 months rosuvastatin treatment was -0.19±0.35 mm (p<0.001). Baseline and change in LDL-c was 4.0±0.9 mmol/L and -2.3±0.8 mmol/L (p<0.001). Mean LDL-c level during 18 months rosuvastatin treatment was 1.7±0.4 mmol/L. The degree of CP height reduction was independent of the LDL-c level exposure during the study period (p=0.36). Attainment of LDL-c < 1.8 mmol/L or the change in LDL-c did not influence the degree of CP height reduction (p=0.44 and p=0.46, respectively). The higher the CP was at baseline - the larger height reduction after 18 months with rosuvastatin treatment (p< 0.001). Joint disease activity during the study period was inversely associated with change in CP height (p=0.02), so that patients with the highest disease activity had the smallest change in CP height and vice versa.
Conclusion:This is the first clinical study showing that intensive lipid lowering with statin induced regression of atherosclerosis in patients with IJD. Our results indicate that joint disease activity may influence the effect of anti-atherosclerotic treatment.
P525
Patients with dyslipidemia on a diet have a healthier dietary intake than the general population
P Marques-Vidal1, P Vollenweider2, M Grange2, I Guessous3, G Waeber2
1University Hospital Center Vaudois (CHUV), Lausanne, Switzerland
2University Hospital Center Vaudois (CHUV), Department of Internal Medicine, Lausanne, Switzerland
3Geneva University Hospitals, Department of Community Medicine, Primary Care and Emergency Medicine, Geneva, Switzerland
Background:dietary measures effectively complement hypolipidemic drug treatment, but little is known regarding the composition of hypolipidemic diets in Switzerland.
Objective:To characterize the dietary intake of subjects aged 40 to 80 years according to diagnosis of dyslipidemia and presence of a hypolipidemic diet.
Methods:cross-sectional study conducted between 2009 and 2012 on 4289 participants (2274 women) living in Lausanne, Switzerland, of which 1370 (32%) reported a diagnosis of dyslipidemia, of which 242 (18%) reported a hypolipidemic diet. Dietary intake was assessed using a validated food frequency questionnaire.
Results:compared to participants with dyslipidemia not on a diet, those on a diet consumed more fruits (mean±standard deviation: 2.5±1.9 vs. 1.9±1.7 portions/ day), vegetables (1.6±1.0 vs. 1.4±0.9 portions/day) and fish (1.9±1.4 vs. 1.6±1.1 portions/week) and less meat (4.5±2.7 vs. 5.2±2.9 portions/week). They also had a higher intake of total carbohydrates (50.1±8.6 vs. 47.1±8.3 % total energy intake), monounsaturated (39.9±5.4 vs. 39.4±4.3 % total fat) and polyunsaturated (15.6±4.3 vs. 14.2±4.1 % total fat) fatty acids and a lower intake of total fat (34.2±7.4 vs. 36.6±7.0 % total energy intake) and saturated fatty acids (35.1±6.2 vs. 37.8±5.7 % total fat). Finally, participants with dyslipidemia on a diet complied to more nutritional recommendations (2.1±1.0 vs. 1.7±0.9) than participants with dyslipidemia but not on a diet. Compared to non-dyslipidemic participants, participants with dyslipidemia on a diet had a higher consumption of fruits, fish and total carbohydrates, mono and polyunsaturated fats, and a lower consumption of total and saturated fats.
Conclusion:when implemented, hypolipidemic diets lead to a healthier dietary intake than in the general population.
P526
Self-perception of salt consumption and its intake among adults living in three urban units in Praia, Cape-Verde
D Alves1, Z Santos1, M Amado2, R Simoes1, I Craveiro1, J Cabral1, L Lapao1, A Delgado3, A Correia4, L Goncalves1
1Institute for Hygiene and Topical Medicine, Lisbon, Portugal
2Faculty of Science and Technology UNL, Lisbon, Portugal
3Directorate-General of Health - Cape-Verde, Praia, Cape Verde
4National Center for Health Development - Cape-Verde, Praia, Cape Verde
Topic: Sports cardiology
Purpose:Cardiovascular diseases are the main cause of death in Cape-Verde (35% of deaths by noncommunicable diseases, estimated to account for 69% of total deaths) [WHO 2014]. It was estimated that 47.7% of men and 38.4% of women over 25 years suffer from Hypertension [WHO 2013]. High levels of dietary sodium (consumed as common salt) are associated with raised blood pressure and adverse cardiovascular health [Dariush et al. 2014]. Kerry at al. (2005) stated that in many sub-Saharan African countries, particularly in less urbanized settings, the main source of dietary sodium is from salt added to food for preservation, taste and in the cooking process. The guideline for salt daily consumption is up to 5000mg/day (equivalent to 2000mg/day of sodium) [WHO 2012]. This study aimed to analyze self-perception of salt consumption and sodium daily intake.
Methods:A Food Frequency Questionnaire (FFQ) was applied, as part of the UPHI-Stat questionnaire, to a random sample of 1912 participants from three urban units in Praia (Formal, Informal and Transition) to assess self-perception of salt consumption in diet. A 24-hour dietary recall was applied, in order to assess sodium daily intake, to 599 participants.
Results:According to FFQ, in an ordinal scale - none, low, medium and high - 44.1% and 50.9% of the sample referred low and medium salt consumption, respectively. The participants from Formal unit referred a higher percentage of low and a lower percentage of medium consumption. The median sodium daily intake for the sub-sample was 3156mg/day [IQR: 1901-4948], with Transition unit presenting a lower value (2451mg/day [IQR: 1599-4124]) than the other two units (p<0.001). Therefore, 73.7% of this sub-sample did not comply with the recommendation. Moreover, 3.7% presented a sodium daily intake higher than 10000mg/day (5.1% in Informal unit). The non-compliance with the recommendation was 83.3% and 61.8% in Informal and Transition units (p<0.001) and, by sex, 79.9% and 70.4% on men and women, respectively (p=0.024). Analyzing the quantity of sodium intake for each category of self-perception of salt consumption, it was found that at least 70% of participants presented sodium daily intake above the recommendation, for all categories.
Conclusions:In the study urban units, sodium daily intake does not fit nutritional and dietary recommendations, even though their self-perception of salt consumption by FFQ was mainly referred as low or medium consumption. This demonstrates the emerging need for specific content development within the public health and community nutrition for the development of food skills.
P527
Oleacein translation from extra virgin oil to stabilization of atherosclerotic plaque.
M Naruszewicz1, A Filipek1, ME Czerwinska1
1Medical University of Warsaw, Department of Pharmacognosy and Molecular Basis of Phytotherapy, Faculty of Pharmacy., Warsaw, Poland
Topic: Sports cardiology
Purpose:Oleacein is one the most abundant compound of phenolic fraction of extra virgin olive oil. Taking into account anti-oxidative and anti-inflammatory effects of oleacein, we examined its potential influence on the stabilisation process of carotid plaque ex vivo. A direct effect of oleacein on the macrophage phenotype were also evaluated.
Methods:The effect of oleacein on MMP-9, MMP-9/NGAL, IL-10, HO-1 and HMGB1 secretion from human carotid atherosclerotic plaques obtained from TIA patients were measured by ELISA assays. The expression of CD 163 and IL-10 in macrophage cells was determined by Flow Cytometry. The expression of CD163 receptor was confirmed by Real-time quantitative RT-PCR.
Results:We have shown that oleacein in dose-dependent manner (from 5 to 20µmol/L) significantly decrease secretion of proteases, such as MMP-9 and complex MMP-9/NGAL as well as HMG1 and TF by the plaque stimulated by LPS. At the same time we observed increase IL-10 and HO-1 secretion. Complexes of oleacein with hemoglobin and haptoglobin 1-1 and 2-2 stimulate the expression of CD163 macrophage scavenger receptor and IL-10. This process can lead to changes macrophage phenotype cells from pro-inflammatory M1 to anti-inflammatory M2.
Conclusions:Oleacein may play significant role in the stabilization of human carotid plaque and could be potentially useful in the reduction of the risk of ischemic stroke.
P529
Inverse association between central obesity and arterial stiffness in Korean subjects with metabolic syndrome: a cross-sectional cohort study
1Keimyung University Hospital Dongsan Medical Center, Cardiology, Daegu, Korea, Republic of
2Yonsei Cardiovascular Hospital, Yonsei University College of Medicine, Cardiology Division, Seoul, Korea, Republic of
Introduction:Metabolic syndrome (MetS) is associated with increased risks of diabetes and atherosclerotic cardiovascular disease. Whether central obesity (CeO) is a prerequisite for the diagnosis of MetS in the International Diabetes Federation (IDF) definition is a substantial issue because it may influence the clinical value of MetS for predicting subclinical atherosclerosis.
Methods:We investigated the relation between MetS, as defined by the National Cholesterol Education Program–Adult Treatment Panel III criteria, and arterial stiffness measured using brachial-ankle pulse wave velocity (baPWV) according to CeO status in 2,560 healthy Korean subjects who participated in a community-based cohort study.
Results:The prevalence of MetS was 40%; 85% of MetS subjects had CeO. The prevalence of diabetes was higher in MetS subjects than in non-MetS subjects (30 vs. 8%, p<0.001). The number of MetS components (MetSN) was correlated with baPWV (r=0.311, p<0.001). In a subgroup analysis of MetS subjects, the prevalence of diabetes was not significantly different in MetS subjects with and without CeO. MetS subjects without CeO had higher baPWV than those with CeO (1654±315 vs. 1578±270 cm/s, p=0.002). Multiple regression models revealed that CeO was inversely associated with baPWV in MetS subjects.
Conclusion:Despite the significant correlation between MetSN and arterial stiffness, there appeared to be an inverse association between CeO and arterial stiffness in MetS subjects. In contrast to the IDF definition, CeO might not be crucial for the diagnosis of MetS in healthy Koreans having multiple metabolic risk factors with respect to subclinical atherosclerosis reflected in arterial stiffness.
P530
The obesity paradox and survivors of ischemic stroke
P Wohlfahrt1, F Lopez-Jimenez2, A Krajcoviechova1, M Jozifova1, O Mayer3, J Vanek3, J Filipovsky3, E Llano4, R Cifkova1
1Thomayer University Hospital, Center for CV Prevention, Prague, Czech Republic
2Mayo Clinic, Rochester, United States of America
3Center of Preventive Cardiology, 2nd Department of Internal Medicine, Charles University, Medical Fa, Pilsen, Czech Republic
4University of Texas Southwestern Medical School, Dallas, United States of America
Background:While obesity is a risk factor for stroke and achieving normal weight is advocated to decrease stroke risk, the risk associated with obesity and weight loss after stroke has not been well established.
Aim:To assess the association of obesity at the time of stroke admission and weight loss after stroke with total mortality.
Methods:We analyzed 736 consecutive patients (mean age 66±11 years, 58% male) hospitalized for their first ischemic stroke. Body weight at hospital admission and at the outpatient visit during follow-up was used in the analysis.
Results:After multivariate adjustment, obesity at admission was associated with lower mortality risk as compared with normal weight (HR 0.50, p=0.03). At the outpatient visit, with a median follow-up time of 16 months, 21% of patients had lost >3kg of weight. Stroke severity, heart failure, transient ischemic attack and depression after stroke were independently associated with significant weight loss. Weight loss >3kg was associated with increased mortality risk (HR 5.87, p=0.001) independently of other factors. Similar results were seen when weight loss was defined as losing over 3% of baseline weight, (HR 4.97, p=0.004). Weight gain >5% of the baseline weight tended to be associated with better survival when compared with no weight change (long-rank test p=0.07).
Conclusions:Normal weight at hospital admission and weight loss after ischemic stroke are independently associated with increased mortality. Overweight and obesity at baseline do not decrease the risk associated with weight loss.
P531
Assessing the risk for cardiovascular diseases using PROCAM/HeartScore in obese patients. A survey with 960 employees
S Hossain1, A Raethling1, R Gottfried1, T Bitter1, O Oldenburg1, G Noelker1, K Gutleben1, D Horstkotte1, KP Mellwig1
1Heart and Diabetes Center NRW, Ruhr-University of Bochum, Department of Cardiology, Bad Oeynhausen, Germany
Topic: Sports cardiology
Purpose:Obesity has long been identified as important risk factor for a number of health problems. Body Mass Index (BMI) is the most frequently used measure to determine levels of body fat, provides a proxy measure of total adiposity (the amount of fat around the body). The aim of the present project is to apply the PROCAM and HeartScore for association of adiposity with morbidity and mortality of cardiovascular diseases in employees of different companies undergoing a cardiovascular screening program.
Method:960 employees of different companies were investigated between May 2013 –September 2014. The cardiovascular risk was determined using the PROCAM score (allows the early detection of the risk of contracting a disease thereby providing the possibility of a timely prevention, especially in high risk groups whose disorders have not manifested clinically yet) and HeartScore (The tool for predicting and managing the risk of heart attack in Europe).
Results:We examined 388 women and 572 men (age 43±10.77 years). 134 employees (13.96%) had BMI values above 30 kg/m2. The PROCAM-Score was = 20 in 5 employees of the adiposity group (3.73%) and in 14 of the non-adiposity group (1.90%). HeartScore was = 5 in 19 patients (14.18%) of the adiposity group and in 55 patients (6.66%) of the non-adiposity group. Increased systolic and diastolic blood pressure (> 140 / > 90 mmHg) was found in 31.34 % of the obese patients and in 13.44 % of the non-obese group. However there was a slightly higher amount of smokers in the obese group (36.57%) compared to the non-obese group (34.99%). The percentage of high LDL-Cholesterol levels was almost double in the obese group (20.9 % vs. 11.86 %). The percentage of high HbA1c values was almost five times higher in the obese group (14.93 % vs. 3.15 %). There was an approximate 3:1 ratio of males to females in our obese collective.
Conclusion:Although there was only a small percentage of obese employees (~15%), the significant higher risk for cardiovascular disease was apparent in both score systems (more than double). Therefore extensive diagnostic measures in prevention are required.
Total number
BMI (kg/m2) (mw/range)
HeartScore total number
PROCAM total number
HeartScore (mw/range)
PROCAM (mw/range)
Group A (BMI >30)
134/960= 13.96%
33.04±3.53/ 30 - 47.9
19/134= 14.18%
5/134= 3.73%
2.17±2.24/ 1 - 16
5.50±7.32/ 0 - 54
Group B (BMI<30)
826/960= 86.04%
24.03±3.05/ 16.3 - 29.9
55/826= 6.66%
14/826= 1.69%
1.74±1.84/ 1 - 15
3.02±5.25/ 0 - 45
P532
Comparison of anthropometric indices as predictors of cardiovascular disease risk factors in portuguese adult population: importance of waist-to-height ratio
A M Pereira1, R Palma Dos Reis2, R Rodrigues1, S Gomes1, AC Sousa1, E Henriques1, M Rodrigues1, S Freitas1, D Pereira1, MI Mendonca1
1Hospital Dr. Nélio Mendon? Research unit, Funchal, Portugal
2New University of Lisbon, Cardiology, Lisbon, Portugal
Background:Obesity is associated with diabetes mellitus, hypertension, dyslipidemia and increased cardiovascular disease (CVD) risk. Anthropometric indeces, such body mass index (BMI), waist circumference (WC), and waist-to-height ratio (WHtR), were evaluated as predictors of the presence of CVD risk factors in Portuguese adults.
Methods and Results:The study contained a 2555 representative sample of Portuguese adults 1952 male aged 52.5 ± 8.2 years and 603 female aged 53.5 ± 8.8 years. All anthropometric indices correlated significantly with fasting glucose level, systolic and diastolic Blood Pressure, Tryglicerides and inversely with the high-density lipoprotein (HDL-C) level (p<0.0001). The WHtR showed higher correlation with CVD risk factors than WC and BMI in both men (p<0.0001, r correlation of 0.21,0.20,0.18,0.15 and -0.2 respectively) and female (P<0.0001, 0.28,0.27,0.24,0.3,-0.37). Regarding Diabetes, Hypertension and Low HDL-C the area under the receiver (AUCs) operating characteristic (ROC) curve for WHtR was higher than that for WC or BMI in the male group. In female group the ROC curve increased from the BMI to WC, beeing highest for WHtR. WC was a better predictor for High cholesterol and LDL in men. The AUCs for WHtR were highest for Diabetes (AUC=0.74 and Hypertension (AUC=0.74) in female group and male group (AUC=0.66 and AUC=0.68). The WHtR cut-off value to predict diabetes mellitus, hypertension, and dyslipidemia was approximately 0.57 in men and 0.58-0.62 in women. The WC cut-offs varied from 92 to 101 cm in men and from 88 to 97 cm in women. The optimal BMI cut-off point varied from 21.7 to 29.1 kg/m2 in women and from 26 to 29 Kg/m2 in men.
Conclusions:WC or WHtR were better predictors of CVD risk factors than BMI in Portuguese Adult Population.
P533
Pericardial adipose tissue may play an important role in the course of coronary artery disease
J Henzel1, R Pracon1, K Kryczka1, M Marczak2, M Demkow1
1National Institute of Cardiology, Coronary Artery and Structural Heart Diseases Dept., Warsaw, Poland
2National Institute of Cardiology, Cardiovascular MRI Laboratory, Warsaw, Poland
Topic: Sports cardiology
Purpose:Obesity is associated with greater prevalence of coronary artery disease (CAD), however, lower mortality was noted in obese patients with CAD ('obesity paradox'). It may be hypothesized that metabolically active pericardial adipose tissue (PEAT) impacts coronary collateral circulation development by secreting wide range of vasoactive cytokines, and thus may influence the course and prognosis of CAD. In this study we sought to compare quantity of PEAT as well as body mass index (BMI) between patients presenting with chronically occluded left anterior descending coronary artery (LAD) and acute anterior myocardial infarction with ST-segment elevation (STEMI).
Methods:Consecutive patients presenting between 2008 and 2013 with chronically occluded LAD (CTO) or anterior STEMI with LAD as culprit artery and who also had myocardial viability assessed by means of MRI were retrospectively enrolled. Myocardial viability assessment with cardiac MRI was performed within 1 month of coronary anatomy assessment. PEAT quantity was obtained from MRI images by manually tracing EAT area in 4 chambers view and expressed in cm2. Traditional cardiovascular risk factors were collected by telephone and medical records review.
Results:57 patients (mean age 62.9 ± 9.9 yrs, 12.1% women) were included in the CTO group and 33 patients (mean age 59.8 ± 10.6 yrs, 27.3% women) were included in the STEMI group. There was no significant difference in BMI between the CTO and STEMI groups (27.2 ± 0.5kg/m2vs. 27.2 ± 5.0kg/m2respectively, p=0.99). However, average PEAT quantity was significantly higher in CTO compared to STEMI group (50.3 ± 23.0 cm2vs. 36.9 ± 16.1 cm2respectively, p=0.004). This association remained significant after adjustment for age, sex, BMI and traditional cardiovascular risk factors such as hypertension, diabetes, dyslipidaemia, tobacco use and family history (p=0.014, OR 1.04).
Conclusions:Despite comparable BMI scores, patients presenting with anterior STEMI had less PEAT compared to those with chronically occluded LAD. Pericardial distribution of adipose tissue may therefore play an important role in the course of CAD.
P535
General and central obesity measurement associations with markers of chronic inflammation and type 2 diabetes
SR Millar1, IJ Perry1, CM Phillips1
1University College Cork, Epidemiology and Public Health, Cork, Ireland
Topic: Sports cardiology
Purpose:Inflammation has been suggested a possible mechanism linking adiposity with type 2 diabetes. Central obesity indicated by waist circumference (WC) measurement is thought to be a greater risk factor for chronic inflammation compared to general obesity characterised by body mass index (BMI). However, evidence for this association is still equivocal. In this study we compare biomarker relationships with BMI and WC measures and type 2 diabetes. We examine a range of pro-inflammatory cytokines, acute-phase response proteins, coagulation factors, white blood cell counts and a combination of these markers to determine which measurement is more strongly associated with diabetes-related inflammation.
Methods:This was a cross-sectional study involving a random sample of 2,002 men and women aged 50-69 years. Correlation and logistic regression analyses were used to explore general and central obesity measurement relationships with non-optimal biomarker levels, biomarker combinations and type 2 diabetes.
Results:When compared with BMI, WC was more strongly related to a majority of inflammatory markers, adverse biomarker clustering and type 2 diabetes. In multivariable analysis, only WC remained significantly associated with type 2 diabetes (OR: 2.96, 95% CI: 1.93-4.55) after adjusting for BMI (OR: 0.73, 95% CI: 0.49-1.10) four or more markers (OR: 4.67, 95% CI: 2.64-8.27) and other potential confounders.
Conclusions:These data suggest that central obesity is a greater risk factor for type 2 diabetes and associated chronic inflammation. However, our results also demonstrate that the relationship between obesity and inflammation cannot be completely accounted for by surrogate adiposity measures.
P536
Impact of type D personality on adverse cardiovascular prognosis in patients in one year after coronary artery bypass grafting
OI Raykh1, AN Sumin1, EV Korok1, AV Osokina1, MG Moskin1
1Research Institute of Complex Problems of cardiovascular disease, Kemerovo, Russian Federation
Psychosocial stress is acknowledged as one of risk of development of cardiovascular pathology. The interrelation between existence personality type D and prevalence of atherosclerosis is recently established. However, predictive value of type D personality in different cultures and the countries are not fully understood.
Topic: Sports cardiology
Purpose:Study aim was to investigate the association of type D personality with the development of cardiovascular complication in patients in one year after coronary artery bypass grafting (CABG) in russian patients.
Materials and Methods:Evaluation of psychological status and combined risk of nonfatal (strokes, nonfatal myocardial infarctions, repeat procedures of revascularization and hospitalization due to relapse or progression of angina pectoris) and fatal (general and cardiovascular mortality) cases before and in one year after CABG. Patients with chronic ischemic heart disease (n=683, 127 (18.5%) females and 556 (81.5%) males, mean age=57,7±7,3 years.) who had had CABG were included in the study. Who were formed in two groups: patients with the presence of type D (n= 152) and patients without type D (n=531). The study of the psychological status was carried out using questionnaire DS-14, validated in Russian.
Results:During the one year frequency of fatal cases in both groups amounted 0.40% and 0.38% (p=0,145), in turn nonfatal end-points in group with type D amounted 31.8%, and 14.6% in group without type D (p=0,049). Statistically significant correlation between their probability and type D (p=0.002), type 2 diabetes mellitus (p=0,01), multifocal atherosclerosis (p=0,003). Presence of type D personality at initial examination increased 3.21 times combined risk of nonfatal and fatal cases (odds ratio[OR] 3.21, 95% confidence interval [CI] 2,02-6,14, p=0.002).
Conclusion:Accumulated proofs indicate that in detection of patients at risk of development of stress induced cardiac complications after CABG it is reasonable to use approach which involves consideration of personality type.
P537
Relationship between psychological state, quality of life scale scores and left ventricular mass index in hypertensive patients
G F Andreeva1, A D Deev1, V M Gorbunov1, O V Molchanova1
1State Research Center for Preventive Medicine, Moscow, Russian Federation
Objective:The aim of our study was to determine psychological and quality of life (QL) LVH possible predictors in untreated stable hypertensive patients. Design and Methods:We studied 90 hypertensive patients (40 males and 50 females; mean age 52,6 ± 1,1 years). Ambulatory blood pressure (ABP) monitoring (Spacelabs 90207) was performed twice in each patient at interval of 3-4 days after the 2 weeks washout period. After the ABP monitoring each patient completed the Russian version of the psychological questionnaire "Minnesota Multiphasis Personality Inventory" (MMPI) and QL questionnaire (J. Siegrist and all.,1989). Only patients with stable hypertension (daytime ABP ³140/90 mmHg) and normal psychological scale scores (40-60 T-balls) were included into the study. Left ventricular mass index (LVMI) (L. Teichholtz 1976) was measured using echocardiography (Acuson 128XP). We analyzed the following evaluation and basic MMPI scales: L – lie scale, F – aggravation scale, K – correction scale, 1 (Hs) – hypochondria, 2 (D) – depression, 3 (Hy) – hysteria, 4 (Pd) – psychopathy, 6 (Pa) – rigidity of affect, 7 (Pt) – psychasthenia, 8 (Sc) – schrizothemia, 9 (Ma) – hypomania.
Results:The mean ABP avd LVMI in the examined group were (M± SD): 24-hour systolic BP – 140,2 ± 11,2; 24-hour diastolic BP- 90,1 ± 8.2, LVMI – 122,1±21,9 g/m2. We found an adverse correlation between LVMI and scale 9 scores (level of activity, energy, good mood; r=-0.32, p<0.05). There were no significant links between LVMI and QL scales scores.
Conclusions:Hypertensive patients with low level of activity, energy, mood have higher probability of development of LVH. It is possible that scale 9 scores are psychological LVH predictors. QL scales scores probably have no prognostic value.
P538
Subdepression in patients with prior myocardial infarction: association with clinical characteristics of chronic coronary artery disease and comorbidities
O Tsygankova1, D Platonov2, T Kostyuk2, E Zubrykina2
1Novosibirsk State Medical University, Novosibirsk, Russian Federation
Purpose:To assess the prevalence of subdepression in patients with prior myocardial infarction (MI) and associated clinical characteristics of chronic coronary artery disease.
Material and methods:In outpatient clinic, 245 patients of both sexes aged 35-60 years with prior MI were interviewed for current symptoms and history, and examined for cardiac status (vital signs, ECG, Holter, echo, stress test), as well as for mood disorder with Zung questionnaire. Subdepression (SbD) was defined as 50-59 points at Zung's scale. Patients with more serious mood disorders (60+ points) were excluded from analysis. Multiple clinical and instrumental factors were assessed: stable angina (SA) and its grade, chest pain (CP) of any type, symptoms of chronic cerebral ischemia (SCCI), symptoms of arrhythmia (SAr), symptoms of low limb ischemia (SLLI), time to prior MI (TMI), arterial hypertension (AH), obesity (Ob), family history of heart disease (FHHD), ventricular arrhythmias (VA), Q waves (QW) and ischemic ST depression (ISTD) on ECG and Holter, systolic and diastolic dysfunction (SDF, DDF) on echo, functional capacity (FC) in stress test. Univariate logistic regression analysis was done sequentially with SbD as dependent categorical variable and all mentioned factors to identify significant associations and select factors for further multivariate stepwise backward logistic regression analysis. Odds ratios (OR) were calculated from regression coefficients with 95% confidence intervals.
Results:Overall SbD was found in 29 (22.8%) men and 42 (35.6%) women. In univariate analysis, OR of SbD for female sex was 2.2 (1.3-3.9), age >50 years – 2.8 (1.5-5.0), SA – 7.0 (2.4-20.5), CP – 9.2 (2.1-39.6), SCCI – 4.7 (2.2-10.3), TMI >1 year – 2.2 (1.3-4.0), FHHD – 2.1 (1.2-3.9), VA – 1.9 (1.1-3.4), ISTD – 2.3 (1.2-4.2), FC < 75 W – 4.8 (2.1-11.0). No statistically significant associations were found between SbD and SAr, SLLI, AH, Ob, QW, SDF, DDF. In multivariate model (overall accuracy 0.80, pseudo-R square by Neigelkerke 0.495), independent associations with SbD were confirmed for older age (OR 2.8; 1.5-5.2), presence of CP (OR 3.7; 1.1-12.4), low FC (OR 2.3; 1.1-4.6), TMI >1 year (OR 2.2; 1.1-4.2), presence of SCCI (OR 3.3; 1.4-7.7). Female sex was no longer a significant factor (OR 1.9; 0.5-7.2). Presence of any type CP, as well as low FC were more important factors than presence of SA and its grade.
Conclusion:Special attention should be reasonably paid to SbD and its multiple associated and predisposing factors to improve medical care and potentially prevent the post-MI patients from overt depression.
P539
Subdepression in patients with prior myocardial infarction: association with demographic and socioeconomic factors
O Tsygankova1, D Platonov2, T Kostyuk2, E Zubrykina2
1Novosibirsk State Medical University, Novosibirsk, Russian Federation
Purpose:To assess the prevalence of subdepression in patients with prior myocardial infarction (MI) and associated demographic and socioeconomic factors.
Material and methods:In outpatient cardiology clinic, 245 randomly selected patients of both sexes aged 35-60 years with prior MI were examined with complex questionnaire for education (Ed), income (Inc), occupation (Oc), family status (FS), and subdepression (SbD, defined as 50-59 points at Zung's scale). Patients with more serious mood disorders (60+ points at Zung's scale) were excluded from further analysis. Univariate, bivariate and multivariate stepwise backward logistic regression analysis was done with SbD as dependent categorical variable, and sex, age, Ed, Inc, Oc, FS as independent categorical factors without and with interaction modes. Odds ratios (OR) were calculated from regression coefficients with 95% confidence intervals (CI).
Results:Overall SbD was found in 29 (22.8%) men and 42 (35.6%) women. In univariate analysis, ORs of SbD were 2.2 (1.3-3.9) for female sex, 2.8 (1.5-5.0) for older age (above median), 2.8 (1.4-5.5) for lower Ed (Ed other than higher), 3.9 (2.1-7.4) for lower Inc (below median), 4.5 (2.5-8.3) for lack of Oc, and 4.4 (2.4-8.2) for living without family. In multivariate model (overall accuracy 0.75), independent associations with SbD were confirmed for female sex (OR 1.8; 1.1-3.0), older age (OR 2.3; 1.2-4.6), lower Inc (OR 2.4; 1.2-4.9), lack of Oc (OR 2.9; 1.5-5.8), and lack of family (OR 3.8; 1.9-7.7). Positive multiplicative interactions were found in bivariate logistic regression models for SdD between female sex and all above mentioned factors: older age, lower Inc, lower Ed, lack of Oc, and lack of family, – stressing the fact of excessive female vulnerability to numerous hazardous factors for mood disorders. In multivariate regression models for SbD that were separately built for men and women the above mentioned variables behaved somewhat differently: in men the most important factors associated with SbD were lower Inc (OR 3.2; 1.2-8.4) and lack of family (OR 2.6; 1.2-5.8), in women – lack of Oc (OR 13.2; 2.6-66.4), lack of family (OR 8.9; 2.9-27.3), and older age (OR 3.0; 1.1-8.8). It has to be pointed out that in females the regression model explained the SbD variability to much greater extent than in males (pseudo-R square by Neigelkerke 0.515 vs 0.118).
Conclusion:Special attention should be reasonably paid to gender aspects of SbD and its multiple associated and predisposing factors to improve medical care and potentially prevent the post-MI patients from overt depression.
P540
Is watching national team matches in World Cup Soccer 2014 on TV and associated with increasing of ventricular arrhythmia?
T Shiozawa1, K Shimada1, G Sekita1, H Hayashi1, H Tabuchi1, S Yamagami2, S Suwa3, M Sumiyoshi4, Y Nakazato5, H Daida1
1Juntendo University Graduate School of Medicine, Department of Cardiology, Tokyo, Japan
2Juntendo Tokyo Koto Geriatric Medical Center, Department of Cardiology, Tokyo, Japan
3Juntendo University Shizuoka Hospital, Department of Cardiology, Izunokuni, Japan
4Juntendo University Nerima Hospital, Department of Cardiology, Tokyo, Japan
5Juntendo University Urayasu Hospital, Department of Cardiology, Urayasu, Japan
Background:Psychological triggers such as emotional stress increase the incidence of acute cardiovascular events. The association between soccer championships and the risk of cardiovascular events are controversial. World Cup Soccer (WCS) involving the national team might be a trigger strong enough to induce cardiac arrhythmia. However, there are no reports which investigated the relationship between WCS and cardiac arrhythmia in the Japanese population.
Methods:We assessed 28 patients who were evaluated ischemic changes and/or arrhythmia by 24-hour Holter ECG during WCS 2014 in 4 Cardiology Divisions. The patients were divided into two groups [Watching group (n=10) patients who watched WCS on live-TV on June 20 (Japan vs. Greece) or July 25, 2014 (Japan vs. Colombia), and No-watching group (18 patients)]. The heart rates, arrhythmia, and ischemic changes were evaluated.
Results:There were no significant differences of clinical characteristics, heart rates, frequency of premature atrial contractions, and ischemic changes between the two groups. The frequency of premature ventricular contractions (PVCs) were significantly higher in the Watching group than in the No-watching group (2893±3657 vs. 237±472, P=0.005). Notably, the frequency of PVCs were significantly higher during live-TV in the Watching group than in the No-watching group (124±187 vs. 3.3±5.4, P=0.0003). No sustained ventricular tachycardia or fibrillation was recorded.
Conclusions:A significant association between watching WCS and the frequency of PVCs was observed. These data suggest that emotional stress while watching national team soccer matches may induce stress-related cardiovascular events.
P541
Evaluation of the efficacy of cardiovascular prevention in the framework of the World Heart Day
N Pogosova1, A Evdokimova1, A Ausheva1
1National Center for Preventive Medicine, Moscow, Russian Federation
On the eve of World Heart Day, which is held annually around the world on September 29 at the initiative of the World Heart Federation, a number of activities were organized on September 22-29, 2014 in the state medical organizations of the public healthcare system by the Ministry of Healthcare of the Moscow city (currently more than 12 million people live in Moscow according to the official data). The aim of these activities was to attract attention of inhabitants to modern possibilities of prevention of cardiovascular diseases (CVD), risk factors and CVD complications, importance of timely referral, and new approaches in treatment of CVD. As a part of these activities a campaign «Is your patient's cholesterol level optimal?" has been held. In the frame of this campaign patients of the public healthcare system of the Moscow city, who have passed health-checks in the first quarter of 2014, were invited to out-patient clinics for re-examination of total cholesterol. The aim was to assess the effectiveness of a previously recommended lifestyle changes and/or lipid-lowering medications. 2392 patients participated in the campaign, of this 835 patients (during health-checks in the first quarter of 2014) were diagnosed to have coronary heart disease and 1557 patients - high CVD risk (>5% risk according to the high-risk countries SCORE scale). More than half of patients reported that they followed a low-fat diet, up to 16% noted that they had increased their physical activity, although less than 1.5% gave up smoking. Every third patient without coronary heart disease has been recommended statins. Special attention was paid to the minority of patients with slight negative (11%) or without dynamics (7%) of total cholesterol. In most patients was found an improvement of cholesterol level. The results served as the basis of analysis of clinical cases without positive cholesterol dynamics in preventive departments.
P542
Time to medical treatment and one-year survival after an acute coronary event according to the first medical contact unit (primary care or hospital): results from the ERICO study.
I S Santos1, AC Goulart1, RCO Santos1, ALX Kisukuri1, RM Brandao1, D Sitnik1, HL Staniak1, MS Bittencourt1, PA Lotufo1, IM Bensenor1
1University of Sao Paulo, Sao Paulo, Brazil
Topic: Sports cardiology
Purpose:The importance of timely and efficient first medical contact (FMC) in the acute coronary syndrome (ACS) treatment is widely recognized. However, little is known about the outcomes of individuals who initially seek a primary care unit for an ACS event. The aim of the present study is to determine if FMC at primary care (PC-FMC) or at hospital (H-FMC) are determinants of time to medical treatment and/or one-year survival in the Strategy of Registry of Acute Coronary Syndrome (ERICO) study.
Methods:The ERICO study is a cohort study of individuals treated for an ACS event between 2009 and 2013 in Hospital Universit?o, a community hospital in the borough of Butant?S?Paulo, Brazil. Follow-up was performed at 30 days, 180 days and one year after the index event, by telephone contact. We revised data from 701 ERICO participants (87 with PC-FMC and 614 with H-FMC). We used Wilcoxon test to determine if time from FMC to the administration of aspirin, clopidogrel and heparin (in individuals with non-ST elevation ACS) and thrombolysis (in individuals with ST-elevation ACS) was different according to the FMC unit. We built Cox regression models adjusted for age, sex and ACS subtype to study if the FMC unit predicted one-year survival in the sample.
Results:Administration of aspirin, clopidogrel and heparin was almost universal (100.0%, 97.7% and 97.7% in PC-FMC and 98.5%, 96.6% and 96.4% in H-FMC groups. Individuals with non-ST elevation ACS in the PC-FMC group received aspirin earlier than in the H-FMC group (median time, 2.40 vs 2.53 hours, p<0.001). There was also a trend towards an earlier administration of aspirin in ST-elevation ACS patients in the PC-FMC group (median time, 0.70 vs 1.13 hours, p=0.075). Time to thrombolysis in ST-elevation ACS patients was non-significantly lower in H-FMC group (median time, 1.03 vs. 1.15, p=0.19). Complete vital status data was available for 669 (95.4%) participants. We had eight (9.9%) and 67 (11.4%) deaths during follow-up in the PC-FMC and H-FMC groups, respectively. FMC unit was not a predictor for one-year survival in this sample. The adjusted hazard ratio for PC-FMC was 1.03 (95% confidence interval 0.50–2.16).
Conclusions:Our findings suggest that primary care can be a suitable setting for the evaluation of acute chest pain, once timely evaluation, safe transportation and access to hospital treatment are warranted. Respecting the characteristics of local health systems, policy makers should consider to organize such strategy for the system-of-care during a suspected ACS event.
P544
The impact of cardiovascular risk reduction on subsequent sickness absence
C Fernandez-Labandera1, C Catalina-Romero1, M Cabrera Sierra1, L Quevedo-Aguado1, M Ruiz-Moraga1, LM Ruilope2, MA Sanchez-Chaparro3, P Valdivielso3, A Gonzalez-Quintela4, E Calvo-Bonacho1
1Ibermutuamur, Madrid, Spain
2Doce de Octubre Hospital, Madrid, Spain
3UGC Medicina Interna. Hospital Universitario ?128;?Virgen de la Victoria?128;?. , M?ga, Spain
4Department of Internal Medicine, University of Santiago de Compostela, Santiago de Compostela, Spain
Topic: Sports cardiology
Purpose:We have recently demonstrated that an increased CV risk promotes a significant increase in length and cost of sick leave episodes. Now we assess the impact of the improvement in cardiovascular risk (CVR) on sickness absence.
Methods:Prospective cohort study of 179,186 workers from the ICARIA (Ibermutuamur Cardiovascular Risk Assessment) study. Workers' CVR was assessed by the SCORE system in two consecutive years (365 ±90 days). Cardiovascular risk was categorized in low and moderate-to-high and subjects were finally classified in four groups created according to the change or stability between the two measures of their CVR: always low CVR (166,547), worsening in CVR (4,321), improvement in CVR (3,422), and always moderate-to-high CVR (4,896). 1-year follow up was carried out to assess sickness absence. The total count of sickness absence days during 1-year follow-up was the outcome in Poisson regression analysis in order to test the differences in sickness absence among the four groups. Always moderate to high CVR workers were the reference group. Rate Ratios (RR) were adjusted by sex, age, occupation, changes in smoking consumption and previous sickness absence. The improvement in CVR, and always moderate-to-high CVR groups were compared in order to clarify the specific cardiovascular risk factors that improved from the first to the second CVR assessment (chi-squared test).
Results:After adjusting for covariates, the group of workers that improved their CVR showed a reduced count of sickness absence than always moderate-to-high CVR group (RR=0.91, 95%CI: 0.84-0.98). Such decrease was observed when non-work-related (RR=0.89, 95%CI: 0.81-0.96) and cardiovascular diseases (RR=0.66, 95%CI: 0.61-0.71) were considered separately, but not in the case of occupational injuries and work-related diseases (RR=0.96, 95%CI: 0.87-1.05). The most striking differences between the groups of workers with moderate-to-high CVR improving or not their CVR in the second assessment were lower percentages of smokers (51.3 vs.69.5, p=<0.001) and that of workers with high blood pressure (55.1vs. 81.7, p<0.001) in the group that improved CVR.
Conclusion:The change in CVR level throughout a 1-year period is significantly associated with changes in the subsequent sickness absence. Our results suggest that the improvement in CVR level from moderate-to-high to low CVR is associated with a decrease in sickness absence during the next year. Smoking cessation and better control of blood pressure were the main differences between workers who improved and not improved their moderate-to-high CVR.
P545
Gender Differences in Risk Factors for Atrial Fibrillation
N Yagihara1, H Watanabe1, T Watanabe2, Y Aizawa3, T Minamino1
1Niigata University Graduate School of Medical and Dental Sciences, Department of Cardiovascular Biology and Medicine, Niigata, Japan
2Niigata Health Foundation, Niigata, Japan
3Tachikawa General Hospital, Nagaoka, Japan
Introduction:There have been various risk factors for atrial fibrillation (AF) such as cardiac and non-cardiac diseases, and atherosclerotic factors (e.g., diabetes, hypertension, and obesity). The aim of this study was to investigate the gender differences in the impact of risk factors on development of AF in the general population.
Methods:This community-based prospective observational cohort study was based upon an annual health check-up program in Niigata, Japan. The annual examination consists of interviews about medical history, physical examinations, blood examinations, urine tests, chest radiographs, and 12-lead electrocardiograms. This study included 223,877 individuals without AF at baseline who were followed more than one year (152,322 women [68%]; age, 61±12 years).
Results:During a follow up of 5.9±2.4 years, AF developed in 1,840 men (incidence, 4.55; 95% confidence interval, 4.34-4.76) and 1,107 women (incidence, 1.21; 95% confidence interval, 1.14-1.28). Men developed AF from younger age compared to women. In women, development of AF was rare before the age of 60 years and thereafter the incidence of AF increased steeply. Among atherosclerotic risk factors, obesity and hypertension were associated with risk of development of AF in both genders. However, impaired glucose tolerance was associated with AF only in men but not in women, and low HDL-cholesterol was associated with AF only in women but not in men. Elevated triglycerides were not associated with AF in each gender. Decreased LDL-cholesterol was associated with AF in both genders, supporting the cholesterol paradox in AF as we and others have recently identified. Heart disease and metabolic syndrome were associated with increased risk of AF in both genders. Elevated uric acid was associated with AF in women but not in men, and chronic kidney disease was associated with AF in women but the association was weak in men. Non-alcoholic fatty liver disease was associated with risk of AF in women but not in men.
Conclusion:The age-dependent trends in the incidence of AF and the effects of various risk factors on development of AF were different between men and women. Our study indicates that the pathogenic of AF is affected by gender.
P548
Gender differences in the severity and in-hospital treatment of patients with an acute myocardial infarction (AMI)
S Myftiu1, I Sharka1, XH Belshi1, E Saja1, E Sulo2, A Shkoza3, G Sulo2
1"University Hospital Center ""Mother Theresa""", Department of Cardiology, Tirana, Albania
2Department of Global Public Health and Primary Care, Bergen, Norway
3University Hospital Center Mother Theresa, Department of Biomedical Sciences, Tirana, Albania
Topic: Sports cardiology
Purpose:Gender differences in the characteristics of patients with an AMI can influence the treatment and explain (partially or totally) the observed gender differences in survival. We aimed at exproring gender differences in AMI severity and treatment among patients hospitalized at the University Hospital Center.
Methods:A total of 266 consecutive patients [mean age (SD), 64.9 (12.2) years; 22.6% women] were included in the study. Information on socio demographic variables, coronary risk factors, treatment and severity of the disease (defined as congestive heart failure and major arrhythmias) were obtained from the patients' journal by two cardiology residents. Logistic regression models were used to explore gender differences in severity and in-hospital treatment among AMI patients. Models were adjusted for age. Results are expressed as odds ratios (OR) and 95% CI for women versus men.
Results:Women were more likely to be obese (OR=2.46; 95% CI, 1.10-5.51) and have diabetes (OR=2.14; 95% CI, 1.15-3.99) but smoked less than men (OR=0.08; 95% CI, 0.04-0.17) while no gender differences were observed with regard to hypertension and dyslipidemia. Clinical manifestation of AMI (defined as presence of major arrhythmias and/or congestive heart failure) was more severe among women (OR=2.16; 95% CI, 1.16-4.01). Women were also less likely to receive PCI (OR=0.45; 95%CI, 0.20-0.98) and aspirin (OR=0.30; 95%CI, 0.10-0.90) compared to men while no gender differences were observed with regard to receiving statins, beta-blockers and ACE-inhibitors/ARBs.
Conclusions:- Further studies including information on pre-hospitalization conditions are required to further explore reasons for such gender differences in some risk factors and treatment of the acute phase of MI.
P549
First evidence for occurrence of exercise oscillatory ventilation in a general population at cardiovascular risk: insights from the EURO(pean) EX(ercise) population-based study
M Pellegrino1, G Generati1, F Bandera1, V Donghi1, V Labate1, E Alfonzetti1, M Gaeta2, O Ferraro2, S Villani2, M Guazzi1
1IRCCS Policlinico San Donato, Heart Failure Unit, San Donato M.se, Italy
2University of Pavia, Unit of Biostatistics and Clinical Epidemiology, Pavia, Italy
Background:Cardiopulmonary exercise testing (CPET) allows functional evaluation of cardiopulmonary diseases. Among CPET variables, exercise oscillatory ventilation (EOV) identifies heart failure patients with worse prognosis, but the occurrence is not described in literature in the general population at risk for cardiovascular (CV) diseases without previous CV events. We aimed at assessing the prevalence of EOV in a general population enrolled in the EUROEX study.
Methods:557 healthy subjects (age 60±14 years; male 51%) underwent maximal CPET (personalized incremental ramp protocol). A subgroup (n=205) also underwent rest echocardiography.
Results:A prevalence of 16% EOV was observed. The EOV group showed higher prevalence of diabetes (n=24, 25% vs n=67, 14%; p<.05) and female sex(n=69, 75% vs n=216, 47%; p<.05); an impaired exercise tolerance, of all VO2-related variables (peak VO2 and % of predicted VO2, O2 pulse, VO2@AT) and ventilator efficiency; a lower heart rate (HR) at peak exercise and heart rate recovery (HRR). Echocardiographic data showed a reduction of end-systolic dimensions of both ventricles and right atrial area in the EOV Group (n=41 vs n=164). At a multivariate analysis the EOV determinants were: TAPSE (OR: 0.16; p: 0.03); E/A (OR: 0.07; p: 0.04); BMI (OR: 1.12; p: 0.09).
Conclusion:EOV patients exhibited a higher prevalence of diabetes, worse exercise performance and ventilation efficiency. These findings may provide the bases for a more in-depth prediction of CV risk.
Variables
EOV (n=93)
No EOV (n=464)
P Value
Age, y
64±13
59±14
<.01
BMI, kg/m2
33±7
29±5
.07
Peak VO2, ml/kg/min
15.1±3.8
20±7.2
<.01
Peak O2pulse, ml/beat
9.6±3
11.3±3.8
<.01
VE/VCO2 slope
27.7±4.6
25.7±3.6
<.01
Peak HR, bpm
125±21
135±23
<.01
HRR, beats
14±9
16±9
<.05
LV end-systolic volume index, ml/mq
13.5±4
15.5±6
<.05
Right atrial area, cmq
14.8±4
16.8±4
<.01
RV end-systolic area, cmq
6.9±1.6
7.8±2
.01
TAPSE, mm
23.6±3
25.2±4
.07
P550
Arterial hypertension control and association with other risk factors in remote period after myocardial infarction and ischemic stroke.
A V Yagensky1, I Sichkaruk1, M Pavelko1
1Lutsk City Hospital, Lutsk, Ukraine
Objectives:In Ukraine cardiovascular mortality is one of the highest in Europe. Arterial hypertension (AH) is one of the most important modifiable risk factors and its active control is a cornerstone of primary and secondary prevention. Design: Secondary prevention assessment was performed in Ukrainian city Lutsk in representative sample of 235 patients after ischemic stroke (PostIS) (age 62,6 ± 10,3 years, 124 men) and 312 patients after myocardial infarction (PostMI) (age 62,2 ± 9,9 years, 218 men) selected from 2229 patients hospitalized in one city hospital. The home-based blood pressure (BP), anthropometric measurements, questionnaire, and laboratory tests were performed.
Results:The trend to higher AH prevalence was found in PostIS patients (88,9% vs 83,6%, p=0,09). AH was treated in the same proportion of patients (88,6 PostIS and in 87,7% PostIM), but BP goals of <140/90 mmHg was reached only in 11,9% PostIS and 21,3% PostIM patients (p=0,007). This finding corresponded with higher BP in PostIS patients (systolic 161,8±28,0 vs 156,0±26,8 mmHg in PostIM, p=0,02, diastolic 95,7±13,7 vs 92,7±15,0 mmHg, p=0,02). Worse AH control in PostIS patients was associated with less tight physician control (35,4% vs 64,7% PostMI patients contacted to doctor during last 3 months, p=0,004), taking less antihypertensive drugs (1,7±0,8 vs 2,0±0,9 in PostMI; p=0,001), lower physical activity (46,0% in PostIS vs 62,0% in PostMI had regular activities; p=0,004). Both groups had similar compliance to treatment (73,0% and 71,9%). No difference in BP self-monitoring, prevalence of obesity, smoking, diabetes, lipids, glucose and hs-CRP levels was detected. Thus, the main reason for the difference between PostIS and PostMI patients is the worse physician control in PostIS patients.
Conclusions:Inadequate AH control was found in both PostIS and PostMI patients. The worse situation in PostIS patients first of all is due to the worse physician control. Active efforts in guidelines implementation should be made to improve situation.
P552
Higher prevalence of cardiac abnormalities including diastolic dysfunction in gout patients with low cardiovascular risk profile using cardiac MRI and echocardiography
EOF Van Gorselen1, MS Stob2, J Van Es3, IL Meek4, LJ Wagenaar3, HE Vonkeman5, C Von Birgelen6
Purpose:Gout is associated with increased cardiovascular (CV) morbidity and mortality. To investigate gout-specific CV pathology a pilot study was performed to study cardiac abnormalities on echocardiography and MRI in low CV risk profile gout patients.
Methods:10 male patients with chrystal proven gout were recruited from the Arthritis Center Twente CardioVascular Disease database. For inclusion only one of the following CV risk factors smoking, hypercholesterolemia or hypertension was allowed. Exclusion criteria were previous CV disease, age <18 or >75 years, kidney dysfunction, diabetes mellitus and BMI > 30.
Results:Median age was 61.5 years, median BMI was 26 kg/m2, no current smoking. 50% of patients had no CV risk factors. Three patients had elevated blood pressure; median SBP was 138 mmHg, DBP 79 mmHg. Two patients used statins. Median LDL was 2.9 mmol/L. Eight out of 10 patients used urate lowering medication and median serum urate was 0,59 mmol/L. One patient did not undergo echocardiography. 70% had diastolic dysfunction. One patient had asymptomatic atrial fibrillation, 4 left ventricular hypertrophy with concentric remodelling, 3 valvular calcification without significant stenosis and 1 had dilatation of the ascending aorta. Cardiac MRI showed no myocardial edema, but in one patient late gadolinium enhancement and in two regional wall motion abnormalities.
Conclusions:Low CV risk profile gout patients had substantial cardiac abnormalities on echocardiography and cardiac MRI, in particular diastolic dysfunction. The presence of gout-specific CV risk is suggested. Non-invasive cardiac imaging may be useful to detect early subclinical CV pathology.
LV: left ventricle, EF: ejection fraction, LAVI: left atrial volume index, RV: right ventricle
LV function echocardiography
LV function MRI
2D EF (%)
55.4 (51.1-65.6)
LVEF (%)
59,5 (52.2-66.6)
3D EF(%)
57.5 (43.2-63.0)
RVEF (%)
57.3 (51.0-65.0)
LV mass/BSA (g/m2)
79,7 (50.6-101.2)
LV mass/BSA (g/m2)
48.5 (31.0-60.0)
Diastolic dysfunction grade (n=)
Normal
3
LAVI (ml/m2)
29,0 (19-35)
I
5
II
2
E/A ratio
0.87 (0.76-1.20)
P553
Effect of primary cardiovascular prevention on the prevalence of metabolic syndrome
S Masnaghetti1, AM Lucioni1, M Peraro1, S Freri1, A Mazzola1, RFE Pedretti1
1IRCCS Foundation Salvatore Maugeri, Department of Cardiology, Tradate, Italy
Topic: Sports cardiology
Purpose:Metabolic syndrome (MS) is strongly related to cardiovascular events. We tested if the prevalence of MS was reduced in the otupatients referred to our primary cardiovascular prevention programme.
Methods:Aims of primary cardiovascular prevention programmes are to control risk factors, to improve adherence to healthy behaviour and therapy and to prescribe targeted diagnostic evaluation. Visits at baseline and control at 1 year were performed. Counselling on diet and physical activity were given. Optimization of therapy was attempted and diagnostic tests were proposed. IDF and NCEPT ATP III definitions of MS were considered. In the outpatients referred to our primary cardiovascular prevention programme (66 women and 80 males) prevalence of MS and its determinants at baseline and 1 year were compared.
Results:Diagnosis of MS was impossible in 7 women and 4 men at baseline and in 4 women and 3 men at 1 year according to IDF criteria and in 5 women and 4 men at baseline and 4 women and 3 men at 1 year according to NCEPT ATP III criteria. At 1 year a significant improvement in HDL and diastolic blood pressure control and a reduction of the prevalence of MS according to NCEPT ATP III criteria in whole population (p 0,04) and in women (p 0,03) and to IDF criteria in men (p 0,04) were achieved. Results are resumed in table 1.
Conclusion:In patients referred to primary cardiovascular prevention programme a significant improvement of HDL cholesterol and diastolic blood pressure control was achieved. Prevalence of MS was significantly reduced in total population and in women according to NCEPT ATP III and in men according to IDF criteria.
Population
women
men
baseline
1 year
p
baseline
1 year
p
baseline
1 year
p
Waist (cm)
mean (SD)
104,94 + 21,89
105,48 + 15,55
0,78
102 + 65,76
102 + 17,52
0,87
107 + 72,12
109 + 8,49
0,61
Systolic blood pressure (mm Hg)
mean (SD)
136,99 + 16,32
137,37 + 18,48
0,85
134 + 14,14
137 + 20,39
0,48
139 + 7,07
138 + 7,07
0,66
Diastolic blood pressure (mm Hg)
mean (SD)
83,12 + 8,35
81,02 + 8,61
0,03
81 + 14,14
79 + 8,5
0,18
85 + 7,07
82 + 0
0,1
HDL cholesterol (mg/dl)
mean (SD)
47,36 + 18,81
51,47 + 17,30
0,04
52 + 6,36
55 + 18,91
0,34
44 + 19,09
49 + 48,79
0,06
Tryglicerids (mg/dl)
mean (SD)
134,22 + 83,08
124,42 + 58,46
0,28
119 + 50,91
116 + 50,46
0,74
147 + 187,38
131 + 101,82
0,3
Fasting glycaemia (mg/dl)
mean (SD)
104,34 + 43,51
106,26 + 38,29
0,69
106 + 44,55
107 + 41,92
0,9
103 + 12,02
105 + 100,41
0,65
Metabolic Syndrome(IDF)
N (%)
80 (59 %)
76 (55%)
0,24
34 (58%)
38 (61%)
0,47
46 (61%)
38 (49%)
0,04
Metabolic Syndrome (NCEPT ATP III)
N (%)
67 (49%)
56 (40%)
0,04
36 (59%)
28 (45%)
0,03
31 (41%)
28 (36%)
0,42
P554
Is low diffusion lung capacity a predictor for cardiac remodeling?
S Altarev1, M Katsyuba2, Y Slepynina1, O Polikutina1, V Karetnikova1
1Research Institute for Complex Issues of Cardiov. Dis. - Siberian Branch RAMS Institution Scientific, Kemerovo, Russian Federation
2Kemerovo Cardiology Centre, Emergency Cardiology Department #1, Kemerovo, Russian Federation
Cardiac remodeling after myocardial infarction remains a frequent complication and, despite recent advances in acute coronary syndrome treatment, in some cases, seems unavoidable. There is evidence that cardiac remodeling is associated with myocardial damage size, coronary arteries patency, coronary revascularization, or inflammation status but a few data exist that explain interconnection between diffusion lung capacity and cardiac remodeling. So, our hypothesis is that low diffusion lung capacity is a predictor for cardiac remodeling in one year after myocardial infarction.
Methods:Patients with ST elevated myocardial infarction hospitalized within 24 hours from symptoms onset were included in the study. Diffusion capacity of lung for carbon monoxide (DLCO) was measured on 10th to 14th days after a patient had been admitted to the hospital. Transthoracic cardiac echo was done on 10th hospital stay day and in one year after myocardial infarction. The statistical analysis was done with statistical software package SPSS for Windows, version 13.0 (SPSS Inc., USA). Factors independently associated with cardiac remodeling were determined with the discriminant analysis. A logistic regression analysis was done to see if a low DLCO was an independent predictor for cardiac remodeling. A p<0.05 was considered statistically significant.
Results:107 patients (mean age 56.1±9.3 yrs) were included in the study, of which 88 (82%) males. In one year after myocardial infarction, 31 patients (29.0%) developed cardiac remodeling. Univariate analysis showed that early (by 10th hospital stay day) cardiac remodeling, patients' age, body mass index, left ventricle ejection fraction, mean pulmonary artery pressure, low DLCO, number of coronary arteries with stenosis >50%, and inflammation status were predictors for cardiac remodeling. Discriminant analysis revealed that independent predictors for cardiac remodeling were low DLCO, early myocardial remodeling, and number of coronary arteries with stenosis >50% (Wilks' Lambda 0.47, p<0.001). This model allowed 88.5% of cases to be correctly classified with area under the ROC-curve 0.84 (95% confidence interval 0.73 to 0.95, p<0.001). A logistic regression analysis showed that, after adjustment for all possible confounding factors, low DLCO increases possibility for cardiac remodeling to be seen with odds ratio 13.8 (95% confidence interval 2.1 to 91.8, p=0.007).
Conclusions:our data showed that cardiac remodeling in one year after myocardial infarction could be associated with low diffusion lung capacity.
P556
Cardiovascular risk factors and systemic endothelial function in patients with erectile dysfunction
S Krasnyak1, OI Apolikhin1, EA Efremov1, YI Melnik1, SD Dorofeev1, VV Simakov1
1Research Institute of Urology, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:Myocardial infarction and ischemic stroke are the main causes of death in adult males. According to many studies, time interval from onset of erectile dysfunction (ED) to cardiovascular complaints is 2-3 years and to vascular accident (myocardial infarction or stroke) - 4-5 years. The highest predictive value of ED as a marker of vascular disease is manifested in patients aged 40-59 years. In addition, the identification of ED may indicate the presence of these disorders in a patient in a latent form, according to some authors.
Materials and methods:We conducted an assessment of endothelial function in 143 men complaining of erectile dysfunction (42,6 ± 6,8 years). All patients filled the International Index of Erectile Function questionnaire (IIEF). Waist circumference, blood pressure, blood chemistry and penile duplex Doppler ultrasound were also assessed.
Results:Among patients with ED incidence of risk factors of cardiovascular disease was: dyslipidemia - 68%, hypertension - 38%, abdominal obesity - 37% insulin resistance - 21%. Furthermore, the presence of risk factors somatic diseases and diseases of the heart and vascular distribution varied forms of ED in severity. Thus, in patients without accompanying cardiovascular system, mild ED occurred in 25% of cases, moderate ED - 38%, the average - 28% of patients, severe ED - 14%. For patients with cardiovascular these figures were 18%, 30%, 28% and 24%, respectively. The regression analysis and determination of the Spearman rank correlation coefficient (p < 0.05) was performed. The analysis shown a high degree of correlation of endothelial dysfunction with increased blood glucose more than 6.0 mmol/l (r = 0,73), moderate with a waist circumference greater than 94 cm (r = 0,65), age (r = 0,63), increased triglycerides (r = 0,6), decreased high density cholesterol levels (r = 0,5), increased low density cholesterol (r = 0,48), reduced number of points by IIEF (r = 0,45), the lowest degree of association with the identified reduced peak systolic velocity (r = 0,31), low Index of resistance (r = 0,29), end diastolic velocity (r = 0,18), elevated blood pressure> 130 mm Hg (r = 0,24), retention time of blood flow in deep dorsal vein > 15 minutes (r = 0,11).
Conclusion:The evaluation of postcompressive reactive hyperemia index is a highly accurate method of assessing systemic endothelial function in the complex diagnosis of ED. ED is a predictor of cardiovascular dysfunction, and it is necessary to examine not only the local penile blood flow, but also to assess systemic endothelial function.
P557
Differences in an adjusted index of diastolic function in apparently healthy obese young patiens
An adjusted index of diastolic function, easily determined by tissue doppler velocities measured at the level of mitral annulus (Ea/(Sa x Aa)), showed prognostic value in general population. Nevertheless, its value has not been sufficiently studied in population at risk. Obesity carries out a higher risk. We study the presence of differences in this index in a population of apparently healthy obese patients.
Methods:376 patients (44.7% from them with obesity, Body Mass Index 33,9 vs 25.7), without a known cardiovascular disease were studied by conventional and tissue Doppler echocardiography. Anthropometric, biochemical and blood pressure mesurements were obtained, and risk score determined (DORICA score, a Framingham formula validated on Spanish bariatric surgery patients). The adjusted index of diastolic function and the rest of parameters were compared between obese and not obese patients. Predictors for that index were investigated by linear regression methods, considering the above mentioned parameters, sex, age, and heart rate.
Results:Mean age was 42.2 years. 85% were male. We found no differences in cardiac dimensions indexed by body surface. Left ventricle from obese patients was slighty more hyperdinamic (LVEF 74 vs 69%;p 0.012) . The adjusted diastolic index was a 20.41% inferior in obese patients (0.1057, SD 0.05 vs. 0.1328, SD 0.06) (Difference of means 0.027;IC95% 0.01-0.044)(p 0.001). The predictor factors for this index were Body Mass Index, Abdominal Perimeter, Total Cholesterol Levels, and the DORICA Risk Score.
Conclusions:The Adjusted Index of Diastolic Function determined by tissue Doppler was diminished in obese patients. This index correlates with Risk Score and Total Cholesterol. Its prognostic value is being investigated in this on-going study.
P558
The role of cardiovascular risk factors in patients with rheumatic heart diseases
D Bursacovschi1
1State University of Medicine and Pharmacy, Chisinau, Moldova, Republic of
Introduction:Rheumatic heart diseases lead to chronic heart failure and reduced quality of life in many patients. Ischemic heart disease represents the major role in the structure of morbidity and mortality worldwide. Traditional risk factors for vascular disease are important in, but do not fully account for, the increased risk of ischemic heart disease in population.
Purpose and Objectives:To evaluate cardiovascular risk factors and appreciate the risk of cardiovascular death in patients with rheumatic heart diseases.
Materials and Methods:We examined a sample of 65 patients with rheumatic heart diseases according to the diagnostic criteria. We applied the SCORE scale and divided the sample into two groups. The first one with SCORE <5% (30 patients) and the second one with SCORE =5% (35 patients).We assessed traditional and novel risk factors of cardiovascular diseases by clinical and laboratory methods, and made a comparative analysis of modern risk factors.
Results:The study group included 26 men (40%) and 39 women (60%) with mean age 59.5 +0.03. In the study group predominated mitral valvulopathy in 46 (70.7%) patients vs 19 (29.2%) patients with aortal one. From the traditional risk factors the most significant ones for the increased cardiovascular risk were outlined by hypertension in 22 (62.9%) cases, followed by dyslipidemia - 19 (54.3%) cases and obesity - 10 (28.6%) cases. From modern risk factors a major role had the left ventricular hypertrophy assessed on ECG which was found mainly in patients with SCORE =5% - 10 (28.6%) patients vs 6 (20%) patients with SCORE <5%. Also, the patients with SCORE =5% had a higher prevalence of other modern risk factors, such as: metabolic syndrome, a high CRP level, a low glomerular filtration rate, and a high level of anxiety determined by using Spilbenger test. On the other hand, the patients with SCORE <5% were appreciated mainly with concentric hypertrophy, in 7 (23.3%) cases vs 5 (14.3%) cases in patients with SCORE =5%. Therefore, the concentric hypertrophy is considered being a negative factor for the cardiovascular events.
Conclusion:Patients with rheumatic heart diseases have an increased cardiovascular risk, influenced not only by traditional risk factors, but also by the modern ones.
P559
Subclinical atherosclerosis is associated with increased SCORE risk values in a population without cardiovascular disease
O Mitu1, F Mitu1, M Roca1, I-C Roca1, M-M Leon1, M Mitu1, L Arhire1, O Nita1, L Mihalache1, M Graur1
1University of Medicine and Pharmacy "Gr. T. Popa", Iasi, Romania
Topic: Sports cardiology
Purpose:Cardiovascular diseases (CVD) represent the main cause of mortality worldwide. European guidelines recommend the use of SCORE risk chart in asymptomatic subjects with no evidence of CVD. However, the risk charts have their limitations particularly in the moderate risk population for assessing the real CV risk. The aim of our study was to determine whether subclinical atherosclerosis is associated with increased SCORE values in a population free of CVD.
Methods:In the current prospective study, we have randomized from an urban general population 71 subjects free of any CVD and medical treatment, aged 35-75. All participants underwent the following: CV risk factor assessment, systolic and diastolic blood pressure (SBP, DBP) measurement and CV risk evaluation by applying SCORE chart. Subclinical atherosclerosis was determined by multiple investigations: left ventricular mass index (LVMI) and ejection fraction (EF) by echocardiography, intima-media thickness (IMT) and carotid plaques by carotid ultrasound, ankle-brachial index (ABI) and aortic stiffness parameters (pulse wave velocity – PWV, augmentation indexes, central SBP). All measurements were performed by the same operator with the same device. The study was approved by the University ethics committee and all participants signed an informed consent. The statistical analysis was performed in SPSS v 16.0.
Results:Mean age of participants was 49.93±9.4 years, with 34% male gender. Mean SBP and DBP were 125.93±16.0, respectively 79.85±12.26 mmHg. IMT was 0.83±0.12 mm while PWV was 7.99±1.65 m/s. The SCORE risk in this population was moderate: 2.34±1.94. Among the markers of subclinical atherosclerosis, an increased SCORE risk was positively associated with higher IMT and presence of carotid plaques (r=0.47, p<0.001; and r=0.70, p<0.001), SBP and DBP (r=0.41, p=0.001; and r=0.35, p=0.002) and LVMI (r=0.25, p=0.03). Regarding aortic stiffness markers, PWV and aortic SBP were directly correlated with high SCORE risk (r=0.29, p=0.01; and r=0.4, p=0.001). No positive correlations were found between increased SCORE risk and lower EF or ABI.
Conclusions:High SCORE values are strongly associated with markers of subclinical atherosclerosis such as increased IMT, carotid plaques, left ventricular hypertrophy, PWV or central SBP. The use of these methods can modify the risk assessed by SCORE chart if subclinical atherosclerosis is evidenced, especially in asymptomatic population with moderate risk.
P560
Features of the vascular remodeling in men with prehypertension
V Kondakov1, O Antropova1, I Osipova1, E Besklubova2
1Altay State Medical University, Barnaul, Russian Federation
Aim:to explore the features of vascular remodeling in patients with prehypertension compared with hypertension. All patients were divided into groups: the 1-st - 30 men with prehypertension (PHTN), second - 30 men with diagnosed hypertension (HTN), control group-30 healthy volunteers. The age was 46.1±8.3, 47.7±8.5 and 48.1±7.4 years. The CV risk factors, atherosclerosis markers, endothelium dependent vasodilatation (EDVD) were evaluated. The arterial stiffness and central systolic blood pressure (CBP) were performed on the SphygmoCor (AtCor Medical Pty Limited.).
Results:PHTN patients were at a comparable rate of modifiable risk factor, has a lower incidence of abdominal obesity (16%), compared to the HT patients - (40%) (p <0.05). ABI <0.9 was found in 30% and 38% of patients in the 1st and 2nd group, 18% in the control group (p <0,005). IMT was 0,7 ± 0,02 and 0,8 ± 0,08 mm in both groups. Carotid atherosclerosis were diagnosed in 30% of the PHTN and 55% of HTN (p <0,005), 17% in the control (p <0,005). Endothelial dysfunction was found in 57.6% In the 1st group and in 42.4% in 2nd (? = 5,6, p <0.05). The combination of endothelial dysfunction and atherosclerosis was in the 54.3% for the 1st group and 82,1% - 2nd , (p <0,05). Arterial stiffness index (SI) was 5,5 ± 1,85 m/s in the control group, 7,20±1,99 m/s in the 1st group, 8,90±1 85 m/s in the 2nd, which is higher than in the control group (p <0,005). The reflection index (RI) was higher in the both test groups compared to control (35,46 ± 14,50%, 36,59 ± 15,43% and 30,39 ± 13,43% respectively, p <0,005). AI in the groups was comparable with healthy volunteers. PWV> 10 m/s was found in 3% and 5% in the 1st and 2nd groups, respectively. According to the age, among the 31-50 years old patients, 80% in the 1st group and 70% in the 2nd had a higher then a normal PWV (6.6 m/s). At the age of 50, 66% in the 1st group and 50% in the 2nd group had the result higher than 8.5 m/s. AIx and AIx75 in HT patients were higher than in the control group by 10% (p <0,005), Spa at 20 mm Hg (p <0,005).
Conclusions:PHTN men under the age of 55 years have a lower incidence of carotid atherosclerosis and comparable signs of lower limbs atherosclerosis, comparable incidence of arteriosclerosis. However, these figures differ from healthy patients. Already at the age of 31-50 years, the majority of patients (80%) have indicators of vascular stiffness, not corresponding to the normal values. In these patients there is a tendency to increasing CBP. Endothelial dysfunction in PHTN is more common than in patients with hypertension, but it is less combined atherosclerosis.
P561
Does admission hyperglycaemia add prognostic value to the GRACE score?
JL Martins1, R Ferreira1, J Viana1, JA Santos1
1Centro Hospitalar do Baixo Vouga, Cardiology, Aveiro, Portugal
Introduction:Hyperglycaemia at admission (AH) is a well documented major risk factor for mortality in the acute coronary syndrome (ACS). However, this parameter is not included in risk prediction scores, including Global Registry of Acute Coronary Events - GRACE (GS).
Methods:We studied 431 consecutive patients admitted to our coronary care unit with an ACS [age: 67 ± 13 years, 26% female, 30,6% STEMI]. Our primary endpoint was the occurrence of all-cause mortality at mean follow-up of 22 ± 10 months. Patients were categorized in 6 groups according to their AG combined with GS. The ability of the two logistic regression models (GS categorized alone and in combination with AG as continuous variable or using the cutoff >140) to predict death was asseded by binary logistic regression, calculating ROC curves and the corresponding areas under the curve (AUC). Comparative analysis between different AUC was performed by non-parametric method described by DeLong. Continuous net reclassification improvement (NRI) were also calculated.
Results:The best cut-point for AG was 140 mg/dl (sensitivity 63% and specificity 60%), and 42,9% of the patients had increased levels. This group was elderly, had more prevalence of hypertension, hyperlipidemia and worse renal function. GRACE score and troponin levels were also more elevated and had more frequent Killip class =2 and FEVE =35%. In multivariate Cox analysis adjusted to potential confounding factors (gender, obesity, hemoglobin level, pro-BNP, prior events, hyperlipidemia, grace score and AG), only AG (HR 1,004; IC 95% 1,000-1,007; p = 0,035), and GS (HR 1,02; IC 95% 1,003-1,02; p = 0,006) were sustained as independent predictors of mortality. AG = 140 was associated to lower survival at follow up (32,6±0,9 vs 35,5±0,6 months, log rank test p=0,006). The inclusion of AG, as a continuous variable, in a logistic regression model with GS, increased the area under the ROC curve from 0.647 to 0.705 (p=0.01) and was associated with an improvement in the NRI (30,6% [ 0.0091 - 0.6023 ]; p-value: 0.04), suggesting effective reclassification. Nevertheless when used as categorical variable in a logistic regression model with GS, the increased area under the ROC curve was only 0,02 without statistical signification (p=0,57).
Conclusion:In our study AG had a predictive cardiovascular prognosis when added to GS. The addition of AG to the GS may further improve risk stratification and prediction of mortality in patients with ACS.
P562
Circulating microRNAs can predict future fatal myocardial infarction in healthy asymptomatic individuals
A Bye1, H Roesjoe2, G Da Silva1, T Follestad1, J Nauman1, T Omland2, U Wisloeff1
1Norwegian University of Science and Technology, Trondheim, Norway
2Akershus University Hospital, Oslo, Norway
Background:Cardiovascular disease (CVD) is the predominant cause of morbidity and mortality in developed countries. To manage this pandemic, improved tool for CVD risk prediction, including more sensitive biomarkers is needed. Recently, microRNAs (miRs) have emerged as promising biomarkers of disease, as large amounts of stable miRs can enter the circulation. Previously, increased circulating levels of miR-1 and miR-423 have been associated with myocardial infarction (MI) and heart failure, respectively. This imply that expression profiles of circulating miRs may have potential as a multi-biomarker tool that could offer more sensitive analysis for determination of CVD risk. The main objective of this study was to assess whether circulating miRs can predict future fatal MI in currently healthy individuals.
Methods:This is a retrospective study analyzing participants from the Nord-Tr?ag Health Study part 2 and 3 (HUNT2 and HUNT3). 368 miRs were analyzed in serum samples collected from 112 apparently healthy men and women (40-70 years) without any signs of CVD, where half of them suffered from fatal MI within the next 10 years, and the other half still reported to be healthy 10 years after. The cases and controls were age- and gender matched, and the controls were chosen to ensure no significant differences in BMI, cholesterol, glucose, triglycerides and blood pressure between the groups. 16 candidate miRs from the screening cohort were further analyzed in a new cohort of 50 cases and 50 controls, selected on the same criteria as the screening cohort. DIANA miR-Path software was used to search for pathways associated with the differentially expressed miRs. Logistic regression analyses were performed using SPSS to find the miRs that best predicted future MI.
Results:In the screening cohort, 20 miRs were significantly differentially expressed between the cases and controls (p<0.05). A significant over-representation of miRs associated with cardiac hypertrophy were found among the differentially expressed genes (n=13, p<0.01). Based on the results from the screening cohort, the best prediction model of future MI consisted of a combination of 4 different miRs, providing a sensitivity of 84.2 % and a specificity of 72.7 %. (The results from the validation cohort will be ready in time for the conference.) Conclusion:The preliminary results from this study suggest that circulating miRs may represent early biomarkers of future MI in apparently healthy individuals.
P563
Social determinants of daily smoking in the cross-sectional survey in Brno, Czech Republic, 2013-2014. Preliminary results
NK Movsisyan1, O Sochor1, E Kralikova2, R Cifkova3, H Ross1, I Tomaskova1, J Fiala1, V Soska1, R Prosecky1, F Lopez-Jimenez4
1International Clinical Research Center, St. Anne's University Hospital Brno, Brno, Czech Republic
2First Faculty of Medicine and General Teaching Hospital, Prague, Czech Republic
3Charles University of Prague , Center for Cardiovascular Prevention of the First Faculty of Medicine, Prague, Czech Republic
4Mayo Clinic, Rochester, United States of America
Topic: Sports cardiology
Purpose:Smoking as a major modifiable risk factor contributes to excess morbidity and mortality worldwide. The social gradient in smoking varies across time and place. The purpose of this study was to identify the socioeconomic determinants of daily smoking in a cross-sectional survey in Brno, Czech Republic.
Methods:A population-based survey was conducted in 2013-2014 to assess cardiovascular risk factors in a stratified random sample of Brno residents aged 25-64. This study assessed the respondents' socioeconomic status through two proxy indicators, the average monthly household income and educational attainment. Data analysis included descriptive statistics and the chi-square test.
Results:The analysis included the first 1954 respondents, of which 55.1% were women; mean age 47.5 years (±11.3). A total of 21.6% of the respondents had primary or apprenticeship education while 39.3% had secondary or special post-secondary, and 39.0% had higher education. Respondents with low, middle and high income represented 35.2%, 31.1%, and 16.2% of the sample, respectively; those in the lowest and highest income strata comprised 8.7% each. Daily smoking prevalence was 22.2% in the analyzed population sample, 20.7% for women and 23.9% for men (p=0.09). Prevalence of daily smoking was inversely proportional to income strata and level of education, (p<0.001 for trend for both). No significant differences in daily smoking prevalence between men and women were found in the total analyzed sample; however, men smoked significantly more than women in the low (p=0.03) and very low (p=0.05) income groups.
Conclusion:This study found remarkable social inequalities in daily smoking in a population sample of the second largest city in Czech Republic. To improve the population health and promote health equity, future interventions should address the smoking-related inequities, possibly by enhancing access to smoking cessation services and tailoring awareness campaigns to the less advantaged population.
P564
Comparison of smoking habits between Jewish and Arabic youth in Israel
E Klainman1, I Gilboa1, A Yarmolovsky1, G Fink1
1Pulmonary Institute, Kaplan MC, Exercise Physiology U., Rehovot, Israel
Aim of study:To investigate and compare the smoking habits and behavior between Jewish and Arabic youth in Israel.
Material and Methods:5353 high school students were studied. 51% were males, 54% Jews and 46% Arabs. Among the Arabs – 40% were Muslims, 38% Bedouins, 16% Christians and 6% Druzzians. All participants were asked to fill a detailed and intensive questionnaire including general habits and behavior at school and home, smoking habits or smoking trials, physical activities, eating habits among others.
Results:454 out of the 5353 participants (8.5%) reported of constant smoking, while 40.4% of the total participants reported about smoking history in their families. The vast majority (81.7%) of the 454 smokers were males. 191 (42.1%) of them were Jews and 263 Arabs, a significant difference of 15% which might indicate a higher cultural trend of smoking within the Arabic population in Israel. On the other hand, only 13.7% (36) among the Arabic smokers were females compared to 24.6% (47) of the Jewish smokers. As referred to general habits and behavior, no significant differences between the two populations were observed on time of cellular phone conversations or Facebook chats. But, when compared to the whole group, the smokers used those two communication tools much more than the total group – 15.7% vs 6.6% and 23.7% vs 11.7% respectively, for more than five hours daily. A slitter difference of book readers were observed between the smokers and the total group: 5.5% vs 3.6%, respectively, but when compared between Arabs and Jews in the whole group, 7% of the Arabs used to read more than 5 hours daily compared to only 1% of the Jews. 45.3% of the whole group used to eat breakfast regularly compared to 39% of the smokers. 9.6% of the smokers are acting physically more than 9 hours weekly, compared to 7.4% of the total group. 2% of the Jewish compared to 3.2% of Arabs smokers have started smoking under the age of 7 years.
Conclusions:The Arabic youth tend to adapt smoking habits in Israel more than the Jewish ones. The finding of 2-3% of smokers who started smoking under the age of 7 is worrying and might recommend an adequate education even from the kindergarten ages. Significant differences in habit trends were observed between the smokers and the nonsmokers, and less differences or none between the Arabic and the Jewish smokers.
P565
Setting up a smoking cessation service - what can we expect from the first year?
D Schneider1, A Meienberg1, A Deman1, T Burkard1
1University Hospital Basel, Basel, Switzerland
Topic: Sports cardiology
Purpose:According to the WHO, smoking is the single most important preventable cause for premature death worldwide. Since different guidelines support to offer specialised tobacco treatment programs to smokers, we started a physician-led smoking cessation service (SCS) at a tertiary university hospital in 2012. SCS consultations on an individual basis were done by junior-physicians, supervised by senior physicians with special interest in smoking cessation. The present study presents our results of the first year of the SCS according to self-reported quit-rate and patient satisfaction.
Methods:In this cross-sectional study we included all patients (pts) consulting our SCS between 1.6.2012 – 31.5.2013. Baseline and treatment characteristics were obtained from pts charts. Pts were contacted by telephone or if not possible by letter for a standardized interview or questionnaire in February 2014 and self-reported smoking status and satisfaction with consultations (0=low, 10=high) were asked.
Results:80 pts had their first SCS consultation during the first year. Follow-up (FU) data could be obtained from 68 pts, the remaining 12 were considered to be smokers. Mean FU was 430±95 days after their first SCS consultation. 41% of pts were male, mean age was 54±12 years, median Fagerstr?ependency Level was 5 [4-7], 79% of pts had at least 1 smoking-associated comorbidity. Mean number of consultations was 2.9±2.3. 28.8% of all pts reported to be persistent abstinent (PA) over the past 7 days. Factors associated with PA were number of consultations and use of vareniclin. Comparing pts with =2 vs. >2 consultations PA rates were 20% vs. 40% (p=0.05). Median patient satisfaction was 8 [6-10], with 86.8% of pts stating that they would recommend the SCS to other smokers.
Conclusion:Our results show, that it is feasible to achieve persistent abstinence rates of 30% after a mean FU of 61 weeks and a high patient acceptance of the SCS - even in the first year. Our outcome in real-life pts is comparable to results of smoking cessation trials and could encourage further centers to set up a SCS.
P566
Success of smoking cessation is associated with immediacy of quitting after an acute coronary syndrome
M Snaterse-Zuidam1, WJM Scholte Op Reimer2, M Minneboo3, HT Jorstad3, SM Boekholdt3, G Terriet4, RJG Peters3
1Amsterdam University of Applied Sciences, School of Nursing, Amsterdam, Netherlands
2Amsterdam University of Applied Sciences, School of Nursing/Academic Medical Center, Amsterdam, Netherlands
3Academic Medical Center, University of Amsterdam, Department of Cardiology, Amsterdam, Netherlands
4Academic Medical Center of Amsterdam, General Practice, Amsterdam, Netherlands
Background:Guidelines stress the importance of smoking cessation and recommend intensive follow-up. Successful nonpharmacological strategies for smoking cessation in cardiovascular disease (CVD) patients are, however, still scarce. Methods:We used data from the Randomised Evaluation of Secondary Prevention for ACS patients coordinated by Outpatient Nurse SpEcialists (RESPONSE) trial (n=754). The study was designed to quantify the impact of a hospital-based nurse-coordinated prevention programme. For the current analysis we included all smokers (324/754 (43%)). Results:The majority of successful quitters succeeded to quit immediately after the event and remained quitted up to one year of follow-up, without extra help (128/156 (82%)). Having higher education (33% vs. 15%, p<0.01) and no history of CVD (87% vs. 74%, p<0.01), were associated with successful quitting. Conclusion:The majority of successful quitters had stopped immediately after their ACS. It was in their own ability to quit and they remain quitted up to one-year follow-up. There is no evidence to support relapse prevention in ACS patients who stop smoking immediately after the event, and our study indicates that there is no need for it.
1 Defined as non-smoking at outcome assessment date; 2 Between successful quitters and smokers; 3 Note that these 30 relapsers are a subgroup of the 168; SBP systolic blood pressure; LDL low density cholesterol; BMI body mass index; ?128; <30 min./5 times a week
Successful quitters n=156
Smokers n=168
P-value
Male, n (%)
127 (81%)
125 (74%)
0.13
College or university
49 (33%)
25 (15%)
p<0.01
No history of CVD, n (%)
136 (87%)
124 (74%)
p<0.01
Risk profile at baseline
SBP >140 mmHg
36 (24%)
33 (20%)
0.12
LDL >2.5 mmol/L
46 (31%)
66 (39%)
0.15
BMI >25 kg/m2
116 (74%)
115 (68%)
0.12
Inadequate physical activity?
89 (57%)
98 (58%)
0.81
Risk profile at one-year follow-up
SBP >140 mmHg
41 (28%)
43 (26%)
0.79
LDL >2.5 mmol/L
32 (22%)
62 (37%)
p<0.01
BMI >25 kg/m2
127 (81%)
112 (67%)
p<0.01
P568
Correlations between NT-proBNP and high sensitivity cardiac troponin in runners - literature review and current perspectives
E Vilela1, R Bettencourt-Silva2, M Passos Silva1, JPL Nunes3, V Gama1
1Hospital Center of Vila Nova de Gaia/Espinho, Department of Cardiology, Vila Nova de Gaia, Portugal
2Sao Joao Hospital, Department of Endocrinology, Diabetes and Metabolism, Porto, Portugal
3Faculty of Medicine University of Porto, Porto, Portugal
Topic: Sports cardiology
Purpose:Running is a physiologic human activity. Recent reports have described high-sensitivity cardiac troponin (hs-cTn) elevation in runners, apparently without associated cardiac damage. Similar data has been published concerning natriuretic peptides. NT-proBNP is of importance for the diagnosis and prognosis of heart failure. The aim of our work was to present the current state of the art concerning the relationship, if any, between NT-proBNP and hs-cTn after running. This would help explain the phenomenon of hs-cTn elevations after running.
Methods:A literature search was conducted on three databases (Pubmed, ISI and Scopus) up to February 2014. The queries used were "brain natriuretic peptide AND running", "BNP AND running", "NT-proBNP AND running". Additional records were identified through review of the literature. Studies comprising less than ten participants or written in languages other than English were excluded. Studies selecting participants based on a specific pathology were outside the scope of our review, which intended to describe a healthy (or presumably healthy) population.
Results:A total of 460 articles were found, and of those 6 reported correlations between NT-proBNP and hs-cTn. A total of 409 runners were evaluated. In 5 articles (400 runners), no correlation was described between NT-proBNP and hs-cTn. Only one report (assessing 9 ultramarathoners) described a correlation between these biomarkers - peak levels of NT-proBNP being significantly higher in those who had hs-cTnT above the 99th percentile value.
Conclusions:Most reports do not present a correlation between hs-cTn and NT-proBNP levels. This supports the notion that they may represent different mechanistic pathways. More studies, with a larger number of participants, are needed to confirm this hypothesis.
Overview of studies correlating NT-proBNP and hs-cTn (literature up to February 2014)
Study
Year
n
Distance
Troponin Assessed
Salvagno et al
2014
18
Ultramarathon (60 km)
hs-cTnI
Tian et al
2012
26
Constant load treadmill run (90 minutes)
hs-cTnT
Scherr et al
2011
102
Marathon
hs-cTnT
Mingels et al
2010
43; 38; 10; 85
5; 15; 21; 42 km
hs-cTnT
Saravia et al
2010
78
Marathon
hs-cTnT
Giannitsis et al
2009
10 (only 9 assessed)
Ultramarathon (216 km)
hs-cTnT
P569
Evaluation of left ventricular mass in adolescent athletes
H Krysztofiak1, A Folga2
1Mossakowski Medical Research Centre, Warsaw, Poland
2National Center of Sports Medicine, Warsaw, Poland
Changes in body height and mass in adolescents limit the accuracy of indexing of left ventricular mass and make it difficult to compare left ventricular mass (LVM). The study was undertaken to evaluate changes of LVM in adolescent athletes and to compare methods of LVM indexing. Sixty nine athletes (58 boys and 11 girls; age 8-19) practicing sports with predominance of high dynamic component (HD) and 23 (15 boys and 8 girls; age 9-18) practicing sports with predominance of low dynamic component (LD), who underwent echocardiography during preparticipation examination, were included in this retrospective, cross-sectional study. The HD and LD groups were similar in terms of age, body mass and height. Each group was also divided into two subgroups, based on median for age: HD into one subgroup above the median (AHD) and the second below the median (BHD) and the LD group into ALD and BLD subgroup, respectively. LVM indexed to BSA (LVM/BSA), to height raised to an exponential power of 2,7 (LVM/H2,7) and to body mass (LVM/BM) and relative wall thickness (RWT) were calculated. Correlations and t tests were used for statistical testing. LVM indexes were higher in HD vs LD: LVM/BSA 79,0±14,1 vs 69,3±8,2 g/m2, p<0,005; LVM/H2,7 33,1±5,6 vs 28,0±3,8 g/m(2,7), p<0,0001 and LVM/BM 2,42±0,35 vs 2,10±0,24 g/kg, p<0,0001. There was no difference in RWT between HD and LD. When only girls were taken into account there were no differences in LVM indexes in HD vs LD, but if only boys were take into account the indexes were different (LVM/BSA 80,5±14,6 vs 70,0±9,0 g/m2, p<0,01; LVM/H2,7 33,6±5,8 vs 27,5±3,9 g/m(2,7), p<0,0005 and LVM/BM 2,45±0,34 vs 2,12±0,24 g/kg, p<0,0005) and RWT was different (0,35±0.04 vs 0,32±0,03, p<0,01) in HD vs LD, respectively. In subgroups, LVM/BSA was higher in ALD vs BLD (74,1±7,6 vs 65,0±6,3, p<0,005) but there were no differences in LVM/H2,7 and LVM/BM between the subgroups. In AHD subgroup, LVM/BSA and LVM/H2,7 were higher compare to BHD (88,4±15,2 vs 71,8±7,8, p<0,0001; 35,1±6,7 vs 31,5±3,8, p<0,01, respectively) but there was no difference in LVM/BM between AHD and BHD, although the body mass was different in both groups (70,0±13,6 vs 38,2±10,7 kg, p<0,0001), respectively. In correlations between age and the LVM indexes there was low correlation with LVM/BSA (r2=0,28, p<0,0001) and there were no correlations with LVM/H2,7 and LVM/BM. Exercise, with high dynamic component, during development period, give additional impact for the left ventricle growth. Indexing to height, but also simple indexing to body mass, seems to be better than to BSA, because not confounded by age.
P570
Prevalence of ECG abnormalities in novice versus experienced endurance runners and normal controls
J Sydow1, P Aagaard1, C Holmquist1, B Mogensen2, H Skuladottir2, T Pottgiesser3, F Braunschweig4
1Karolinska Institute, Cardiology unit, Stockholm, Sweden
2Karolinska University Hospital, Department of Cardiology, Stockholm, Sweden
3University of Freiburg, Dept of Cardiology, Freiburg, Germany
4Karolinska University Hospital, Dept of Cardiology, Stockholm, Sweden
Analysis of the 12-lead ECG is recommended as part of pre-participation evaluation prior to endurance sport events but misinterpretation is common. The prevalence of ECG abnormalities in recreational, middle-aged or elderly endurance runners is not well established. Furthermore, the impact of different levels of training experience on this prevalence has not been characterized.
Methods:We studied 770 subjects: 1) 279 first-time participants (novice; NOV) in the world's largest cross-country race (Liding?pet, 30 km); 2) 279 age- and gender matched subjects who had participated at least 6 times before (experienced; EXP); 3) 212 controls (CON), randomly invited from the general population, with similar age- and gender characteristics, without significant cardiovascular disease or training background. A 12-lead ECG was taken after 5 minutes of rest. All participants underwent a brief physician exam and filled in a questionnaire about medical history and training habits.
Results:All groups had a mean age of 52 years and included 21% women. NOV, EXP and CON had an average of 3.3, 4.7 and 1.0 hours/week of endurance training during the past 4 months (p<0.001). Main results are shown in table. Common training related ECG changes (1st degree AV-block, early repolarization (ER), Sokolow criteria of left ventricular hypertrophy) were more common in NOV and EXP than CON. More NOV and EXP had ECG abnormalities that may require additional evaluation (QTc above 440 ms and inverted T-waves). CON had a higher heart rate (HR) and shorter QRS compared with NOV and EXP.
Conclusion:Training related ECG alterations are common in recreational, middle-aged or elderly endurance runners compared with normal control subjects. The prevalence of these ECG changes does not significantly further increase in experienced versus novice runners. Only a minority of athletes had ECG abnormalities requiring additional evaluation. Knowledge about the prevalence of ECG abnormalities is important for all clinicians involved in the care and/or pre-participation evaluation of endurance race participants.
*:p<0.001 compared with NOV or EXP. #:<0.05 compared with NOV
HR (bpm)
QRS (ms)
AV-block I (%)
ER (%)
Sokolow (%)
Inverted T (%)
QTc>440ms (%)
NOV
58.2
97.0
8.2
29.7
11.5
3.6
9.0
EXP
56.5#
97.9
11.1
36.2
16.1
3.6
8.6
CON
64.2*
93.7*
1.4*
7.1*
4.2*
0.5*
0.5*
P571
High intensity endurance training in women is associated with atrial structural and functional remodelling.
L Sanchis Ruiz1, M Sanz1, B Bijnens2, G Giraldeau3, G Grazioli1, M Marin1, M Sitges1
1Hospital Cl?c, Barcelona, Spain
2Instituci??talana de Recerca i Estudis Avan?s (ICREA), Barcelona, Spain
3Montreal Heart Institute, Montreal, Canada
Topic: Sports cardiology
Purpose:High intensity training has been associated with atrial remodelling and atrial arrhythmias in men. However, few data has been reported about female athletes. Our purpose was to analyze atrial performance in female endurance athletes.
Methods:We included 35 women: 18 athletes (>10 hour/week endurance training) and 17 controls (<3 hour training/week). Left and right atrial (LA and RA) function was assessed using 2D echocardiography to determine atrial ejection fraction (EF) and atrial strain-rate by speckle-tracking: a-wave strain-rate (SRa) as a surrogate of atrial contractile function and s-wave (SRs) as a surrogate of atrial reservoir function.
Results:Mean age was similar in both groups (36.9±5 vs.37.4±6 y.o., p=0.489). Atrial indexed volumes [ml/m2] were larger in the athlete group (LA 27.1±6 vs 15.8±4, p<0.001; RA 22.3±4 vs 14.3±4, p<0.001) with no differences in EF [%] (LA 48±13 vs 44±17, p=0.42; RA 34±15 vs 31±17, p=0.53). SRa (s-1) was reduced in both atria in athletes as compared to controls (LA -1.59±0.47 vs -2.01±0.55, p=0.021; RA -1.91±0.39 vs -2.35±0.56, p=0.025). SRs (s-1) was only reduced in the RA of athletes without differences in the LA as compared to controls (LA 1.68±0.41 vs 1.67±0.44, p=0.932; RA 2.01±0.32 vs 2.35±0.05, p=0.536).
Conclusions:The atria of female athletes shows specific remodelling as compared to sedentary females, with larger size and lower deformation at rest, particularly for the RA. These findings are similar to those observed in male athletes and indicate a potential larger contractile reserve but at the cost of larger atrial wall stress.
Atrial size and function
P572
Upper limits and clinical correlates of blood pressure response to exercise in Olympic athletes.
S Caselli1, A Vaquer Segui1, R Assorgi1, B Di Giacinto1, E Lemme1, FM Quattrini1, FM Di Paolo1, C Pisicchio1, A Spataro1, A Pelliccia1
1Institute of Sport Medicine and Science CONI, Rome, Italy
Purpuse:We sought to define the upper limits of blood pressure response in elite athletes and describe clinical and morphologic characteristics of those with higher values.
Methods:1,930 athletes, divided according to type of sport (skill, power, mixed and endurance) underwent cardiac evaluation, with echocardiography and maximal bicycle exercise test.
Results:Peak Systolic and Diastolic Blood Pressure (SBP and DBP) were 184±22 mmHg and 74±8 mmHg. The 95th percentile were 220mmHg in male and 200mmHg in female for SBP and 90mmHg in male and 80mmHg in female for DBP; 116 athletes (6%) had either SBP and/or DBP above the 95th percentile for gender. Clinical and echocardiographic characteristics of these are shown in table. Stepwise regression analysis showed that: peak SBP was explained by maximum workload (R2=0.34, p<0.001) with basal SBP, left ventricular wall thickness and body surface area (BSA) showing lower additional value (R2=0.47, p<0.001). Peak DBP was explained by basal DBP (R2=0.20; p<0.001) with a lower additional value for age, BSA and maximum workload (R2=0.27; p<0.001).
Conclusion:the present study shows the normal blood pressure response to exercise that could be implemented in athletes's evaluation to identify hypertensive individuals.
Normal exercise BP
High exercise BP
p value
Age (years)
25 ± 6
25 ± 6
0.219
Positive Family Hx (n,%)
445 (25%)
35(30%)
0.173
BSA (m2)
1.89 ± 0.23
2.00 ± 0.25
<0.001
Basal SBP (mmHg)
114 ± 11
124 ± 10
<0.001
Basal DBP (mmHg)
73 ± 7
77 ± 7
< 0.001
Basal Heart rate (bpm)
58 ± 11
57 ± 10
0.318
Max Heart Rate (bpm)
166 ± 10
165 ± 10
0.235
Max workload (Watts)
242 ± 59
261 ± 62
0.001
LV Wall thickness (mm)
9.6 ± 1.2
10.1 ± 1.1
<0.001
LV diameter (mm)
52 ± 5
54 ± 5
<0.001
EF (%)
65 ± 6
65 ± 6
0.954
LA diameter (mm)
34 ± 4
36 ± 4
<0.001
LV Mass (mm)
191 ± 55
214 ± 58
<0.001
E/A
1.9 ± 0.5
1.9 ± 0.4
0.974
P573
Right ventricle remodeling in female endurance athletes
M Sanz1, G Giraldeau2, B Bijnens3, J Marin1, G Grazioli1, M Sitges1
1Barcelona Hospital Clinic, Barcelona, Spain
2Montreal Heart Institute, Montreal, Canada
3ICREA, Instituci??talana de Recerca i Estudis Avan?s, Barcelona, Spain
Background:High intensity endurance exercise has been related with a specific right ventricle (RV) remodeling. Most of studies though, have been conducted on male athletes, having so far few data available in female. Our aim was to analyze RV remodeling and response to exercise in female athletes as compared with untrained females.
Methods:19 highly trained female athletes (> 10 hours endurance training/week) and 21 control age-matched (<3 hours sport/week) were included. In all subjects an echocardiography at rest and at maximum effort was performed. Analysis consisted on standard and speckle tracking echocardiographic assessment of both ventricles. RV segmental strain was also determined at the base (inlet), mid and apical regions of the RV free wall.
Results:At rest, LV volume was larger in athletes than in controls (62,5 ± 8,2 vs 45,6±6,9 ml/m2) with no differences in LV systolic function. RV size was also larger in athletes (10,5 ± 1,40 vs 7,8±1,5 cm2 / m2) with no differences in RV global systolic function. Segmental RV deformation analysis showed no differences between the two groups. With exercise, both groups increased cardiac output (CO) proportionally to the amount of exercise performed (%?CO: 210,2±40,3 vs 158, 6± 49,0; Watts : 174,1±27,8 vs 118,1±20,0). Thus, the increase in LV strain was higher in athletes group (+33,5 ± 14,6 vs +23,1 ± 11,7). However, the increase in RV global strain was lower in athletes ( +13,5 ± 10,4 vs +20,6±13,8) and mainly induced by an increase in RV basal segmental strain (Figure).
Conclusion:We confirmed a similar pattern of RV remodeling in female athletes to that previously observed in male athletes characterized by RV dilatation and a major contribution of its basal segment to the increased demand in cardiac output during exercise.
Changes in LV and RV Strain
P574
An investigation of cardiac disease in british army recruits in whom a murmur is detected during the initial medical: a retrospective observational study
AT Cox1, DE Cannie2, I Parsons3, R Chamley3, E Behr1, D Wilson3, S Sharma1, RG Bogle2
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
2St George's Healthcare NHS Trust, London, United Kingdom
3Royal Centre of Defence Medicine, Birmingham, United Kingdom
In military populations cardiac conditions are a potentially preventable cause of mortality and morbidity. Many of these conditions are identifiable with a history and physical examination and investigation with ECG or echocardiogram.
Aims:To establish the prevalence of cardiac conditions, in British Army recruits, in whom a murmur is detected.
Methods:Recruits were screened with a questionnaire and physical examination by military occupational physicians. Those with cardiac symptoms, a history suspicious for cardiac disease, or with hypertension on examination, were referred to their civilian Primary Care Doctor for further investigation. Those recruits with an isolated murmur on auscultation underwent an ECG, echocardiogram and cardiology review in a military clinic and are the subject of retrospective review in this study.
Results:Over a seven year period 11,420 consecutive recruits aged 15-32 years were evaluated. Cardiac disease was strongly suspected or diagnosed in 921 recruits; a positive predictive value (PPV) of 8.06%. Of these 298 (2.61%) were conditions associated with an increased risk of sudden death, including 98 (0.85%) recruits with probable cardiomyopathy, 22(1.9%) recruits with accessory pathways and 30 (0.26%) recruits with possible channelopathies. A bicuspid aortic valve was seen in 124 (1.09%) recruits of which 84 (67.7%) demonstrated valvular dysfunction, aortopathy, coarctation of the aorta or left ventricular dysfunction. Males accounted for 89.0% of the population and 91.9% of those with disease; no male disease preponderance was seen (p=0.117).
Discussion:When detected by occupational physicians, as part of a cardiac screening program, an isolated murmur has a low PPV, but does identify potentially serious structural abnormalities in asymptomatic individuals. This study also characterises a significant burden of incidental heart muscle and primary electrical diseases in a young, fit and asymptomatic population. Many of the conditions discovered are not associated with a murmur and in the absence of an ECG would have been overlooked had an incidental murmur not been present. The addition of a routine ECG to the British Army cardiac screening protocol should therefore be considered in order to improve the detection rate of potentially serious cardiac diseases.
P575
Right ventricular echocardiography in the elderly: first results of ActiFE-Ulm study
R Laszlo1, T Baumann1, D Dallmeier2, K Machus1, J Klenk3, D Rothenbacher3, W Koenig2, JM Steinacker1
1University of Ulm, Division of Sports and Rehabilitation Medicine, Department of Internal Medicine II, Ulm, Germany
2University of Ulm, Department of Internal Medicine II, Ulm, Germany
3University of Ulm, Institute of Epidemiology and Medical Biometry, Ulm, Germany
Introduction:Concerning cardiac function and physical capacity, importance of the right ventricle (RV) is more and more attended. Echocardiographic image quality in the elderly is often poor due to a steep cardiac axis with consecutive impossibility of correct probing, poor identifiability of RV free wall or ageing-lung emphysema.
Methods:ActiFE-Ulm study (Activity and Function in the Elderly with a focus on physical activity and co-morbidities) is a population-based cohort study including a representative sample of people = 65 years old living in the region of Ulm, Germany. Feasibility of right ventricular echocardiography was evaluated in a cardiovascular follow-up of 631 of 1506 subjects of this population (mean age 77.0 ± 5.8 years, 58% male).
Results:Sufficient B-mode echocardiography of the right ventricle (apical 4-chamber view) was possible in only 35% of all subjects (nomenclature see ref. 1): RVD1 38 ± 7 mm, RVD2 34 ± 8 mm, RVD3 76 ± 11 mm, RVEDA 23.3 ± 6.0 cm2, RVESA 13.7 ± 4.2 cm2, RVFAC 41 ± 10 %. Right atrium (RA) could be described adequate in only 38% (endsytolic): RA-area 18.7 ± 5.1 cm2, RA (transverse) 41 ± 8 mm, RA (longitudinal) 50 ± 7 mm. In contrast, right ventricular outflow tract (RVOT) and TAPSE was assessable in 87% (RVOT) and, respectively, 93% (TAPSE) of all subjects: RVOTd 36 ± 6 mm, RVOTs 20 ± 7 mm, RVOT-SF 45 ± 14 %, TAPSE 25 ± 5 mm. Tissue-doppler images (RV free wall 1 cm below TV-annulus) of adequate quality were assessed in 88% of all subjects: S' 13.7 ± 2.9 cm/s (n=572), E' -10.6 ± 3.1 cm/s (n=570), A' -15.6 ± 3.8 cm/s (n=544 of 600 subjects without AF during examination), IVCT 83 ± 21 ms (n=558), Ejct 284 ± 42 ms (n=557), IVRT 60 ± 26 ms (n=559), MPI (Tissue) 0.52 ± 0.16 (n=557).
Conclusion:RV echocardiography in the elderly is often a challenge: not every right ventricular echocardiographic parameter was assessable due to the above-mentioned limitations. Nevertheless, a basic statement concerning right ventricular morph and function was possible in almost every elderly person.