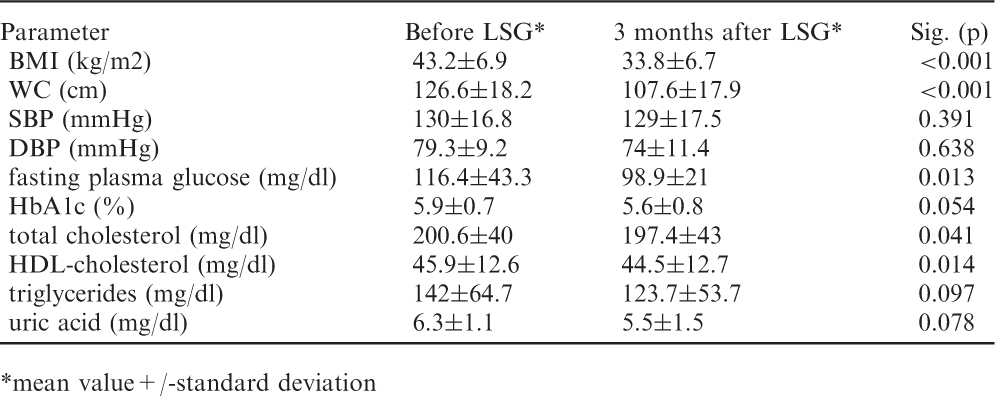
Adaptation to interval hypoxia-hyperoxia improves exercise tolerance and cardio-metabolic profile in patients with coronary artery diseases
O Glazachev1, F Kopylov1, E Zagaynaya1, E Dudnik1
1I.M. Sechenov First Moscow State Medical University, Moscow, Russian Federation
Background:Cardiac rehabilitation is an important component of complex treatment in stable CAD patients. It is generally known exercise-based cardiac rehabilitation is effective in reducing total and CV mortality, morbidity progression and hospital admissions. In our study we use normobaric intermittent hypoxic-hyperoxic training (IHHT) as a new alternative cardio-protective technique, experimentally proved and introduced in our pilot studies (2011-2013).
Methods:From September 2011 to October 2014 we enrolled 46 patients with CAD, class II-III, Canadian Cardiovascular Society (18 men, 28 women; 63,6±8,7 years, 16 – with prior MI) randomly divided to receive 15 sessions of IHHT (IHHT group, n=27) and to breath with the same machine by normoxic gas mixture (placebo group, n=19) in 3 weeks. For IHHT group each breathing session consisted of 5-7 hypoxic periods (12-10% oxygen, 4–6 min) with 3-min hyperoxic (35% oxygen) intervals. Duration of hypoxic and hyperoxic episodes was set up following the results of hypoxic test (on a feed-back principle from SaO2 min, ReOxy Cardio device). Controls inhaled normoxic air only via the same facial mask. Study participants were advised not to change medications, nutrition and levels of physical activity during the study period. Cardiopulmonary exercise test on treadmill (peak VO2, METs, time to fatigue, anaerobic threshold – AT), EchoCG, ECG, blood and biochemical determinations were performed for all patients 2-3 days before IHHT course, 2-3 days after and 30 days later IHHT program.
Results:At the study beginning demographic characteristics and prevalence of risk factors were similar in both groups. After 3 weeks of breathing program in patients of IHHT group peak VO2 and AT increased significantly already after (p=0,027, p=0,036) and 1 month after IHHT completion (p=0,019, p=0,011). No changes have been revealed in controls. Improved exercise tolerance and aerobic capacity in IHHT group were accompanied with significant hypotensive effects (stable decrease of SBP and DBP), decrease of total cholesterol level, triglycerides, mild reticulocytosis, positive dynamics in myocardial contractile function (EchoCG), significant improvements in all scales of Seattle Angina Questionnaire.
Conclusion:Normobaric intermittent hypoxic-hyperoxic training might increased exercise tolerance reducing cardio-metabolic risk-factors in patients with stable CAD and can be useful in cardiac rehabilitation. Further studies are needed to determine the influence of IHHT on MACE and to compare IHHT with exercise-based cardiac rehabilitation.
P579
Non-cardiac readmissions are reduced in patients attending a nurse-coordinated prevention program: results from the RESPONSE randomised clinical trial
HT Jorstad1, WJM Scholte Op Reimer1, JGP Tijssen1, RJG Peters1
1Academic Medical Center, Amsterdam, Netherlands
Topic: Sports cardiology
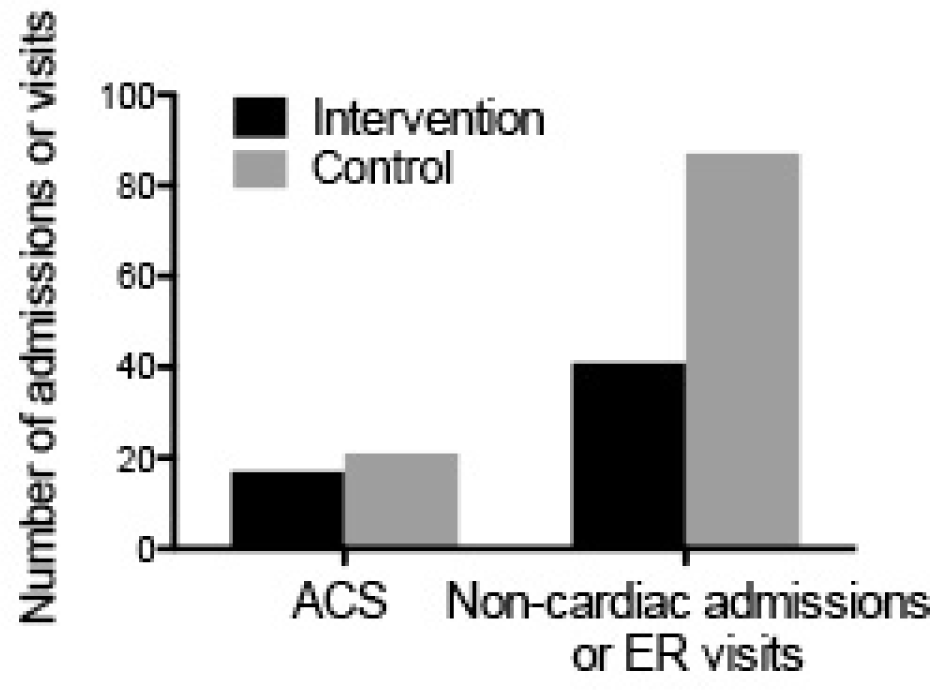
Purpose:To quantify the impact of an outpatient nurse-coordinated prevention program (NCPP) on hospital readmissions and emergency room (ER) presentations in acute coronary syndrome (ACS) patients.
Methods:We analyzed hospital readmissions and emergency room presentations in RESPONSE, a multicenter, randomized clinical trial in 754 post-ACS patients. In total, 375 patients were randomized to the NCPP (interventions), consisting of 4 visits in 6 months, focusing on 1) healthy lifestyles, 2) biometric risk factors, 3) medication adherence, 4) counseling and motivation, on top of usual care. Controls received usual care only. Out main outcome was cardiac and non-cardiac hospital readmissions, interventions, and ER presentations in the first year post-ACS.
Results:During 1-year follow-up, there were no differences between interventions and controls in the number of readmissions for ACS (17 vs. 21, p=ns), acute interventions (12 vs. 17, p=ns), or elective interventions (48 vs. 50, p=ns). However, non-cardiac admissions and ER presentations were significantly less frequent in interventions as compared to controls (41 vs. 87, p<0.001).
Conclusion:Non-cardiac hospital admissions and ER presentations were markedly lower in patients attending the NCPP. Our findings may indicate that counseling and support provided by the NCCP decrease anxiety, increase confidence, or both. These effects contribute to the cost-effectiveness of post-ACS NCCPs.
10653.
P580
The impact of an exercise program based on nordic walking on patients with a recent acute coronary syndrome
R Dalmau1, JM Carrera Pons2, A Castro Conde1, M Marin Santos1, S Espinosa1, A Araujo3, MD Hernandez3, C Vindel3, H Arranz3, JL Lopez Sendon1
1University Hospital La Paz, Madrid, Spain
2Escuela de Esqu?aspirineo, Huesca, Spain
3University Hospital La Paz, Department of Cardiology, Cardiac Rehabilitation Unit, Madrid, Spain
Topic: Sports cardiology
Purpose:Both sedentarism and non-adherence to exercise are growing problems in our modern society. Nordic walking (NW) is an attractive option of aerobic exercise, in which brisk walking is complemented with coordinated arm movements using special poles. This technique allows the patient to exercise both upper and lower muscles. NW is adaptable to most patients, and is not an expensive activity. We analysed the impact of a cardiac rehabilitation program (CRP) based on NW on the adherence to exercise among patients with a recent acute coronary syndrome (ACS).
Methods:80 successive patients referred to a CRP after a recent admission for ACS were randomized 1:1 to receive either a standard exercise program (indoor exercise with bicycle or treadmill) or a NW program (NW sessions outdoor). All patients were offered 16 sessions of exercise supervised by a physiotherapist (75 min, 2 per week during 8 weeks), with a recommendation of doing similar exercise on their own, in order to complete 5-6 days/week of training. Life style group education sessions were offered as well. A symptom-limited treadmill test was performed at baseline, and at 3 and 6-month follow up visits. Adherence to exercise was analysed at the 6-month follow up visit.
Results:we found no differences in baseline characteristics: mean age 56,1, 87,5% male, mean LVEF 53%, mean basal exercise capacity 8,2 METS. 61,3% of patients were sedentary at baseline. At the end of the program an improvement in functional capacity was reached in both groups, with no significant differences. At the 6-month follow up visit, 90% of patients claimed to do exercise, with no significant differences in the number of days/week nor hours/week between groups. Only 19% of patients of the NW group continued to practice NW.
Conclusions:NW is an attractive outdoor sport activity, it can be practiced in a group and it involves more muscle groups than conventional walking. Despite a good acceptance during the CRP, NW did not improve adherence to exercise in coronary patients.
NW group
Control group
p
METS Baseline
8.1
8.3
NS
METS 6-month
11.5
11.4
NS
N of hours of training/week (6-month)
5.8
6
NS
Non-adherence to exercise (6-month)
7,7%
2,4%
NS
P583
Hospital-based and telemonitoring guided home-based training program: effects on exercise tolerance and qol in patients with heart failure, receiving crt therapy
E Smolis-Bak1, R Dabrowski1, E Piotrowicz1, T Chwyczko1, I Kowalik1, B Kazimierska1, B Jedrzejczyk1, K Gepner1, H Szwed1
1National Institute of Cardiology, Warsaw, Poland
Background:Cardiac resynchronization therapy with defibrillator function (CRT-D) along with an optimal medical therapy improves symptoms, cardiac efficiency, quality of life (QoL) and prognosis in patients with heart failure (CHF). The aim of the study was to assess the effects of exercise training, hospital-based and home-based with telemonitoring (TELE) on the levels of exercise capacity, QoL and prognosis in patients with advanced CHF and CRT-D.
Methods:The study was conducted in 52 patients, aged 45-75 years (mean 62 ±9.3), with CHF, NYHA III, with CRT-D. Group CRT-Ex (n=26) underwent initial exercise training in the hospital setting and continued training program at home with TELE (8 weeks). The CRT-Control group (n=26) consisted of patients who had no rehabilitation after discharge.
Results:After 3-4 months the CRT-Ex group achieved better results in VO2 peak, VCO2 peak and treadmill test duration. But after 12 months the improvement in most of the measurements was maintained in the CRT-Control group, while in the CRT-Ex group the measurements returned to the baseline values. In the CRT-Ex group the distance in a six-minute walk test (6-MWT) significantly increased at 3 months compared to baseline. At 12 months, the distances remained similar. No significant differences were observed between two groups in distances of 6-MWT. Echocardiographic evaluation showed significant reduction of left ventricular dimensions and improvement in the ejection fraction, in both groups ( CRT-Ex group, p=0.0213 and CRT-Control group, p=0.0001). Significant improvement in all domains of QoL was observed in the CRT-Ex group, while the CRT-Control patients declared only higher energy levels and less pain. Intensity of TELE-guided home-based exercise training was low. Most of the pts did not continue exercise training after completing the TELE-guided programme. In the 12-month follow-up there were no differences in the mortality or hospitalization rates between the groups.
Conclusions:A structured exercise training program in the hospital setting and further home-based with telemonitoring was safe option of treatment and improved physical fitness, quality of life and echocardiographic parameters in patients with NYHA III CHF and CRT-D. However, patients starting home-based cardiac rehabilitation with telemonitoring must be confident that their knowledge of physical exercise and its impact on their health, continuous access to the monitoring centre staff and telemonitoring guidance guarantee safety of the training programme.
P584
Dance provides greater gain cardiorespiratory fitness and less chance of sexual dysfunction than conventional rehabilitation program.
AI Gonzales1, SW Sties1, HO Braga1, GD Carvalho1, LS Mara1, AS Netto1, DP Lima1, PAB Araujo1, AV Souza1, T Carvalho1
1State University of Santa Catarina, Florianopolis, Brazil
Topic: Sports cardiology
Purpose:There is a relationship between sexual dysfunction and cardiovascular diseases, being the physical exercise effective in the treatment of both. The ballroom dancing has provided cardiovascular effects similar to those of conventional exercise, and it is plausible the hypothesis that can also benefit sexual function. The aim of this study was valuate sexual function and physical performance in hypertensive and coronary cardiovascular rehabilitation and ballroom dance practitioners.
Methods:Cross-sectional study with 102 individuals of both sexes (67.6% men), divided into three groups: ballroom dance practitioners (BDG; n = 34; 66.47 ± 6.66 years), cardiovascular rehabilitation participants (CRG; n = 34; 66.61 ± 6.3) and sedentary (SG; n = 34; 66.17 ± 6.73). The men were evaluated for sexual function by International Index of Erectile Function (IIEF), and women for Index of Female Sexual Function (IFSF); and cardiorespiratory capacity determined by cardiopulmonary exercise testing. In statistical analysis was used Korgomorov-Smirnov test, Mann-Whitney, Kruskal-Wallis and logistic regression analysis, considered confidence interval of 95%, adjusted for gender with significance level of 5%.
Results:Men and women ballroom dance practitioners showed less possibility to present sexual dysfunction (OR= 0.352; p = 0.020; OR= 1.05; p = 0.041, respectively). In the BDG was observed peak VO2 and VO2 in the first threshold, higher than the other groups (<0.001), and VO2peak 16% higher than the CRG and 21% higher than the SG.
Conclusion:Men and women coronary and hypertensive ballroom dance practitioners had higher cardiorespiratory capacity and reduced chance of sexual dysfunction, compared to participants in conventional rehabilitation program and sedentary.
P585
The NOR-COR (NORwegian CORonary) study: identification of CHD patients with poor adherence to secondary prevention and their perceived needs for follow-up
J Munkhaugen1, E Sverre1, K Peersen2, E Gjertsen1, T Liodden2, L Gullestad3, JE Otterstad2, J Perk4, E Husebye1, T Dammen5
Background:Randomized intervention studies on secondary prevention show varying results in patients with coronary heart disease (CHD) and 40-70% of these patients do not participate in cardiac rehabilitation or receive optimal secondary prevention. New strategies are therefore needed. A better understanding of the non-compliant patient and his/her perceived needs may be important for improving the intervention strategies.
Topic: Sports cardiology
Purpose:The NOR-COR projects identify underserved, high risk CHD patients with poor adherence to secondary prevention and low participation in rehabilitation programs, and reveal their perceived needs for secondary preventive follow-up. The first study tests whether illness attribution influences CHD patients`perceived needs for follow-up, and the associations to age, education, drug adherence, risk factor control, time since the event, type of event, somatic and psychosocial comorbidity.
Methods:A cross-sectional, observational study was designed to explore a large number of cardiovascular, behavioural, psychosocial, and health care related factors in patients with a coronary event (myocardial infarction, percutaneous coronary intervention, and/or coronary by-pass operation) from 2011-14. An extensive self-report questionnaire, clinical examination and laboratory data were included. CHD patients, nurses, preventive cardiologists, and researchers in epidemiology and psychosomatic medicine contributed to development of the questionnaire and a pilot test on 20 random selected CHD patients has been performed. Patients who refused study participation will be asked to give their consent to compare journal data (age, gender, type and number of events, risk factors, and somatic and psychiatric comorbidity) with those participating.
Results:From the catchment (380,000) of two representative Norwegian hospitals (Drammen and Vestfold), we identified 1608 patients aged 18-80 years with established CHD. After excluding 291 patients, 1317 patients were invited, and 1125 (85.4%) participated. Preliminary results including current participation in primary and secondary programs, perceived needs for further secondary preventive follow-up, beliefs regarding what caused their CHD, illness attribution and risk factor perceptions will be presented at EuroPRevent 2015.
Conclusion:The study will provide new insights that may be useful for increasing participation in secondary prevention and improving patient information programs. Moreover, this may promote the development of tailored prevention programs applying to patient groups with different perceived needs and behaviour profiles.
P586
The influence of water-based training on arrhythmia in patients after myocardial infarction with preserved left ventricular function.
I Kubacka1, MB Bilinska Maria2, RB Baranowski Rafal2, EP Piotrowicz Ewa3, RB Piotrowicz Ryszard1
1Institute of Cardiology in Anin, Cardiac rehabilitation and noninvasive electrocardiology, Warsaw, Poland
2Institute of Cardiology in Anin, Dept. of Arrhythmia, Warsaw, Poland
3Institute of Cardiology in Anin, Telecardiology Center, Warsaw, Poland
Topic: Sports cardiology
Purpose:Water immersion may cause adverse cardiovascular events, e.g. arrhythmia in post MI patients. So far there have been rather few reports on arrhythmia induced by water training in CAD patients. The aim of the study was to assess the influence of exercise training in moderately cold water on arrhythmia in patients after myocardial infarction (MI) with preserved left ventricular function.
Methods:62 post MI men, mean age 50.9±7.9 years with preserved LV function(EF 57.8±22.6 %), underwent 16 40-minute swimming pool trainings (SPT) twice a week in water at 28-30 ?C. Each subject underwent 24h Holter on-land monitoring (Holter-24) before SPT and twice in-water Holter monitoring (Holter-W) performed with a waterproof pack during SPT. Before and after SPT cardiopulmonary exercise test (CPET) was performed. Arrhythmic events (mean number of VEBs and SVEBs per patient) were assessed during selected 55-min periods of Holter-24 and Holter-W. Moreover, the evaluation included the percentage of men who developed arrhythmia during CPET versus Holter-24 and versus Holter-W.
Results:SPT significantly improved patients' physical capacity, pVO2 increased by 15.3% (p<0.05). During SPT 36 (58%) men developed VEBs and 39 (62%) SVEBs. No complex arrhythmia was recorded. The mean number of VEBs per patients on Holter-W and Holter-24 did not differ significantly (4.93±16 vs 6.92±20) but the number of SVEBs recorded in Holter-W was significantly higher (3.63±9.6 vs 0.12±3.3, p<0.05). SPT provoked arrhythmia much more often than did CPET (VEBs, p<0.05 and SVEBs, p<0.01) and normal daily activity assessed during Holter-24 (VEBs, p<0.01and SVEBs, p<0.01).
Conclusions:SPT generated arrhythmia significantly more often than did CPET and normal daily activity. SPT is an effective and safe form of physical training in men after MI with preserved LV function.
P587
Baseline factors determining the continuation of physical activity 12 months after cardiac rehabilitation
R Pinto1, M Tavares-Silva1, G Pestana1, AR Godinho1, J Rodrigues1, V Araujo1, JA Rocha2, F Parada2, MJ Maciel1
1Sao Joao Hospital, Cardiology, Porto, Portugal
2Sao Joao Hospital, Physical Medicine and Rehabilitation, Porto, Portugal
Topic: Sports cardiology
Purpose:Cardiac Rehabilitation Programs have gained tremendous importance in the prevention of cardiovascular disease. However, the long term benefits are dependent on the ability of the participants to continue unsupervised regular physical activity after the phase II has ended. The aim of this study was to determine the factors that influence the physical activity habits 12 months after the phase II of the Cardiac Rehabilitation Program. Knowledge of this factors can allow the development of more tailored programs.
Methods:The study included 147 patients from a single center referred to CRP after an ACS, from whom 12 month data for physical activity was prospectively assessed by the International Physical Activity Questionnaire (IPAQ). Baseline risk factors, demographic, psychosocial and physical variables were collected at the start of the program and regularly throughout. The IPAQ was administered before the start of the program and at 12 months. We performed logistic regression to the baseline variables deemed to possibly have an impact on the levels of physical activity at 12 months Results:Patients' mean age was 53.±9.1 years, 12% of whom were females. At the beginning of the program 80.5% of the patients reported low levels of activity, while at 12 months this percentage decreased to 38.1%. Using univariate analysis, female sex OR 0.233 (CI 0.083-0.657), being unemployed OR 0.353 (CI 0.139-0.929), the Physical function of the SF-36 OR 1.05 (1.009-1.099) and the Intensity of the first exercise teste in METS OR 1.378 (1.150-1.661) have shown to be significant predictors for the intensity of physical activity at 12 months.
Conclusions:Despite the well-known effects of a CRP after an ACS, a significant proportions of patients does not maintain regular physical activity. Both social, demographic and baseline exercise capacity factors influence this outcome.
P588
The effect of high interval training in acute myocardial infarction patients with drug eluting stent
C Kim1, HE Choi2
1Inje University, Sanggye Paik Hospital, Seoul, Korea, Republic of
2Inje University, Haeundae Paik Hospital, Pusan, Korea, Republic of
Topic: Sports cardiology
Purpose:Peak oxygen uptake (VO2peak) is a strong predictor of survival in cardiac patients. The aim of this study was to compare the effects of high interval training (HIT) and moderate continuous training (MCT) on VO2peak and to identify the safety of HIT in acute myocardial infarction (AMI) patients with drug-eluting stent (DES).
Methods:Twenty-eight AMI patients with DES were randomized to either the HIT or MCT groups, and exercise training started within 3 weeks after PCI, three times per week for 6 weeks at the hospital and usually with a minimum of 1 week or three sessions of MCT mode before starting HIT. The HIT group exercised for a total of 45 minutes. The program consisted of a 10-min warm-up at 50–70% of HRR, followed by four times four minutes intervals of walking on a treadmill at 85–95% of HRR with three active pauses of 3-min of walking at 50–70% of HRR, and a 10-min cool-down at 50–70% of HRR. The MCT group exercised for a total of 45 minutes. Their program consisted of a 10-min warm-up, followed by 25-min walk on a treadmill continuously at 70–85% of HRR, and a 10-min cool-down. All training sessions were supervised by medical staff and monitored by ECG, heart rate, and BP using a telemetry monitoring system, and subjective rate of perceived exertion. All study subjects received a symptom-limited exercise tolerance test (ETT) using the modified Bruce protocol including a pretest an average of 17.07 days (HIT group) and 18.57 days (MCT group) after AMI. Follow-up tests were performed after completing the 6-week exercise training. Primary outcome was VO2peak at baseline and after CR.
Results:Both HIT and MCT groups showed significant increases in VO2peak and heart rate recovery, and significant decreases in serum levels of low-density lipoprotein cholesterol and high-sensitive C-reactive protein after 6 weeks of training. The 22.16 % improvement of VO2peak in the HIT group was significantly greater than the 8.48 % improvement of that in the MCT group (P = 0.021). There were no cardiovascular events related with both HIT and MCT.
Conclusion:HIT is more effective than MCT for improving VO2peak in AMI patients with DES. These findings may have important implications for more effective exercise training in CR program.
P589
Effect of Eccentric Endurance Training in subjects after recent cardiovascular surgery.
F Maslowsky1, M Pribetich1, E Milani1, G Lo Bello1, A Mazzola1, C Franzin1, S Sarzi Braga1, R Pedretti1
1IRCCS Foundation Salvatore Maugeri, Department of Cardiology, Tradate, Italy
Introduction:Eccentric muscle work is a part of our daily activities; usually people use eccentric muscle work during walking, and in particular when walking downhill, to convert potential energy into heat. Eccentric muscle action is characterized by a low metabolic demand for a high power output. Recent studies have drawn attention to the benefits of eccentric muscle training in patients with coronary artery diseases. Aim this study evaluated the effects of eccentric endurance training (EET) in male/female (2/18) subjects (age range 61,5 ± years) after recent cardiac surgery i.e. coronary artery by-pass or cardiac valves replacement Methods:Twenty consecutive patients were participating in the inpatient cardiac rehabilitation program at our institute. Ten patients were randomized in concentric endurance training (CET) and ten in EET. Six minute walking test (6MWT) quality of life (EuroQol) Visual analogic scale (VAS) for leg pain, Borg RPE-scale (0-10 rating) were performed before and after the training period. EET or CET was integrated into a standard comprehensive rehabilitation program such that light calisthenics, stretching and relaxation procedures were identical for all subjects. CET group was underwent one session a day with speed at 80% of speed reached at 6MWT and positive inclination of degrees 5%, whereas the EET group was trained with speed at 80% of speed reached at 6MWT and negative inclination of 5% degrees. The mean of training session was 11,8 ± 5,5 for the two group; CET and EET were carried out five times per week for half an hour.
Results:No muscular injury was reported and no rhythm troubles were found during training. No patients reached rate of perceived exertion over 10, the two groups was homogeneous for type of surgery, age, EF, Hemoglobin content and number of training session. No significant difference was found in two groups in distance during 6MWT, quality of life, leg pain and heart rate, while significant difference was found in in Borg RPE scale in EET group, EET group reported a significantly lower fatigue level than that perceived by the ECT Group.
Conclusion:eccentric exercise training is feasible in middle-aged patients with recent cardiac surgery and without musculoskeletal complication. The results indicate small but not significant improvement in walk capacity whereas significant differences in reduction of fatigue to perform the same work. Because the small energy demand relative to the force produced, eccentric training may be an attractive alternative for patients with limited cardiovascular exercise tolerance.
P590
Effects of exercise training after an acute coronary syndrome on echocardiography evaluation and health status.
A R Godinho1, AS Correia1, I Rangel1, A Rocha2, J Rodrigues1, V Araujo1, F Macedo3, MJ Maciel3
1University of Porto, Cardiology, Porto, Portugal
2University of Porto, Physical Medicine and Rehabilitation, Porto, Portugal
3Faculty of Medicine University of Porto, Cardiology, Porto, Portugal
Despite the role of both diastolic and systolic function in prognosis after acute coronary syndrome (ACS), diastolic function is often overlooked in comparison to improvement of ventricular systolic function and health status. An adequate cardiac rehabilitation program (CRP) after ACS can improve global and cardiac mortality. We studied echocardiography parameters and EuroQol5D scale, before and after CRP, in patients who had ACS and were included on CRP.
Methods:Study of 121 patients who completed a two month CRP consisting of biweekly exercise training sessions, nutrition counseling and psycho-educational group intervention. Patients were enrolled between January 2011 and December 2012. All subjects underwent echocardiography and EuroQol5D scale before and at the end of the CRP.
Results:Mean age was 53.8 years (SD 9.1) and 81.8 % were male. ACS with ST-segment elevation occurred in 53,8% of cases while 36,8% were admitted with ACS without ST-segment elevation. The majority of patients had one vessel coronary disease (63,2%), with 18.8% having 2-vessel disease, and most underwent percutaneous revascularization (90,6%). Most patients were medicated with angiotensin- converting - enzyme inhibitor(80,3%) and beta blockers (90,6%). The EuroQol5D scale improved after CRP (p=0,000). The mean of left ventricular systolic function (LVSF) before CRP was 58,5% (DP 8,5) and after 60,5% (DP 8,0), p<0,001. When we analyzed separately the patients with reduction of LVSF (Ejection Fraction (EF) <55%) (n=26), mean was 46,1% (DP 7,6) before CRP and improved for 51,1% (DP 10,4) after CRP , p=0,000 as well as patients with normal LVSF (FE=55%) (n=95), mean before CRP was 62,1% (DP 4,5) and after 63,3% (DP 4,5), p=0,021. At the end of CRP there was no significant differences on echocardiography diastolic parameters like E/A [1,18(DP 0,3) versus 1,23(DP 0,3)]; before and after CRP, respectively; p=0,123, deceleration time [215,1 msec (DP 44,9) versus 215,6 msec (DP 56,8 ); p=0,935], E/E` [8,46 (DP 2,8) versus 8,36(DP 2,5); p=0,616], left auricular diameter [38,9 mm (DP 3,9) versus 39,2 mm (DP 3,6); p=0,194]. There was also no significant improved on right ventricular systolic function (RVSF) after CRT: peak systolic velocity [13,36 cm/s (DP1,9) versus 13,33cm/s (DP 2,0); p=0,884] and TAPSE [23,19 mm (DP 4,3) versus 23,78 mm (DP 3,6); p=0,582] , Conclusion:Diastolic function and RVSF did not change significantly after CRP on patients who had ACS, but the program improved health status and LVSF. So, cardiac rehabilitation can be of value and should be implemented after ACS.
P591
Ballroom dancing improves functional capacity in cardiac rehabilitation phase III outpatient program
E Venturini1, M Siragusa1, L Lo Conte1, R Testa1
1Department of Cardiology - Civic Hospital , Cecina (LI), Italy
Topic: Sports cardiology
Purpose:aerobic exercise can improves, functional capacity in cardiac patients (P). The longer the duration of physical activity, the greater its effectiveness. The conventional forms of exercise offered in Cardiac Rehabilitation (CR) can be little attractive. Therefore we evaluate, in a preliminary outpatient program (OP), the ballroom dancing (BD) as a strategy to increase physical activity and adherence to exercise.
Methods:we studied 10 P after myocardial infarction (9 men, mean age 64±10 y) enrolled in a CR OP of BD. Dance sessions were performed in an external gym 2 times a week for 8 weeks, lasting 1 hour. The maximal intensity of training was calculated as the HR corresponding to 75-85% of the peak reached during the exercise stress test (EST). At the entry and at the end each P underwent EST and echocardiogram. In each session, were measured basal and maximal exercise blood pressure (BP). All the P completed the protocol.
Results:the BD OP significantly improved the total duration of EST by 11%. The Rate Pressure Product increase by 8% and also the intensity of energy expenditure, in METs (+7%) and in Watts units (+10%), p not significant. The BP during maximal exercise, and the diastolic basal BP were statistically reduced; also basal SBP fell down, but not significantly. Ejection fraction and E/A ratio improved but not statistically. There were no untoward events.
Conclusions:an OP of CR based on BD can increase functional capacity with a better control of BP at rest and during exercise. The hypotensive effect of BD allows it to tackle a greater exercise time, limiting the effort energy expenditure. The short duration of the study may explain the neutral effect on echocardiographic parameters. The emotional dimension of dancing, adds value to the aerobic exercise, improving adherence to the physical activity. BD can be useful, safe and at low-cost in CR Phase III OP, combined with traditional aerobic exercise or in alternative in P, who prefer dancing to other forms of exercise.
Entry
End
p
Entry
End
p
EST
579±115
645±138.3
<.0008
SBP exer.
162.2±14.3
152.4±9.7
<.0009
RPP
24005±3238
26145±4641
ns
DBP exer.
87±3.8
80.5±1.1
<.0007
METs
6.6±1.5
7.1±1.6
ns
SBP basal
148.1±18.8
132.8±12.5
ns
Watt
139.2±24.4
153.±32.2
ns
DBP basal
80.5 ±5.8
74.2 ±6.7
<.002
P592
Feasibility of an exercise stress test as an indicator of disease severity in cardiac rehabilitation patients
A Salzwedel1, A Rieck1, H Voller1
1University of Potsdam, Center of Rehabilitation Research, Potsdam, Germany
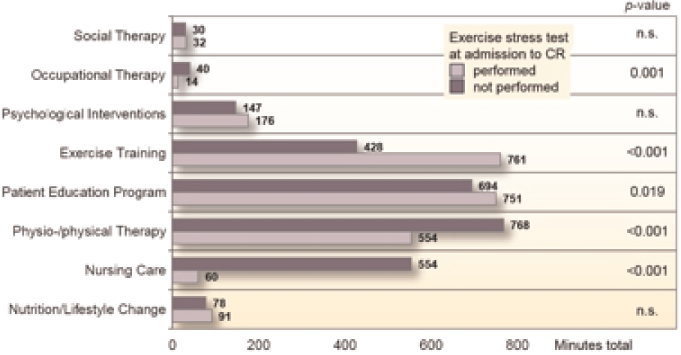
Introduction:Training is a core component of cardiac rehabilitation (CR). There is evidence for large benefit of CR for patients with low exercise capacity at admission. But patients without baseline values were not sufficiently considered. Therefore, we aimed to identify predictors for the feasibility of an initial exercise stress test (EST).
Methods:In a prospective multicenter registry, 1094 patients (71±7 years, 78% men) were enrolled (9 days after hospital stay), predominantly after CABG (33%), PCI (21%), and heart valve replacement (14%). We analysed sociodemographic and clinical variables (e.g. risk factors, comorbidities, complications, 6-min walking distance [6MWD]) with respect to the feasibility of an EST. In addition, we considered therapy volume (total minutes) in different categories (e.g. training, nursing care, patient education).
Results:166 patients (15%) were not able to perform an initial EST. In multivariable logistic regression, the probability of obtaining an EST was significantly higher for men (OR 1.89, p=0.01), a longer 6MWD (per 10m, OR 1.07, p<0.01), higher education level (OR 2.85, p<0.01), but lower for patients with diabetes mellitus (OR 0.48, p<0.01), NYHA-class III/IV (OR 0.27, p<0.01), osteoarthritis (OR 0.39, p<0.01), and a longer hospital stay (OR 0.97, p=0.02). Age had no effect (p=0.67). Patients who did not perform an EST received less therapy units of training and education but more units of nursing car and physiotherapy (Fig).
Conclusion:Feasibility of an initial EST early after an acute cardiac event is an indicator of disease severity. Routine EST will help to better tailor CR to the needs of patients with poor health status. However, there is a justified need not only for exercise based, but also for the comprehensive, interdisciplinary CR.
Total therapy volume during CR
P593
Exercise-based cardiac rehabilitation for adults after heart valve surgery
K Laerum Sibilitz1, SK Berg1, L Tang1, SS Risom1, C Gluud2, J Lindschou2, L Kober1, C Hassager1, RS Taylor3, AD Zwisler1
1Rigshospitalet, Department of Cardiology, Copenhagen, Denmark
2Rigshospitalet - Copenhagen University Hospital, Copenhagen Trial Unit, Copenhagen, Denmark
3University of Exeter, Health Services Research, Exeter, United Kingdom
Background:Exercise-based cardiac rehabilitation may benefit heart valve surgery patients. This systematic review of randomised trials aims to assess the benefits and harms of exercise-based cardiac rehabilitation in adults following heart valve surgery.
Methods:This Cochrane systematic review was conducted according to our published protocol. We included randomised trial irrespective of publication date, type, language and status investigating exercise-based interventions compared with no exercise intervention or treatment as usual in adults who had undergone heart valve surgery. Two review authors independently extracted data and assessed the risk of bias. We undertook meta-analyses and trial sequential analyses to assess the risk of random errors.
Results:We identified 2 trials published in 1987 and 2004 with a total of 148 participants. Both trials had high risk of bias. There was inadequate evidence to determine the impact of exercise-based rehabilitation on the primary outcomes of mortality, serious adverse events, or health-related quality of life, or secondary outcomes (left ventricular ejection fraction, New York Heart Association class, return to work, costs, or cost-effectiveness). However, we did find that, compared with control, exercised-based rehabilitation may increase the secondary outcome of exercise capacity (-0.47 standard deviation units, 95% CI -0.81 to -0.13, p=0.006, I2 statistic=0%).
Conclusions:This Cochrane review suggests that exercise-based rehabilitation for adults after heart valve surgery compared with no exercise, may improve exercise capacity. Further randomised trials with low risk of bias are needed in order to assess the impact of exercise-based rehabilitation on patient-relevant outcomes including mortality and quality of life.
P594
Clinic results in a modern cardiac rehabilitation unit
J A Alarcon1, C Del Bosque1, FJ Madruga1, J Reparaz1, X Arrazola1, M Lavado1, M Rocandio1, F De La Cuesta1
1Donostia Hospital, Donostia, Spain
Background:It is well known the benefit of cardiac rehabilitation (CR) in terms of morbidity and mortality. We present the results of our Cardiac Rehabilitation Unit (CRU), analyzing the data on control of different cardiovascular risk factors (CVRF) just before recruitment( Pre-Program:PP) and after completing the programme in CRU(FP), and MACE during the programme and 1 year after the hospital admission with ACS(acute coronary sindrome).
Methods:In our CRU ,coordinated by cardiologist, we performe strict control of CVRF and stratification of patients, we have also smoking cessation programme , nursing consultation, gym work (with nurse and physiotherapist on-site and telemetry- ECG) with continuous and intervalic aerobic exercise and strength exercise (50% of MR for a total of 9 muscle groups,including dumbbells, floor exercises and leg press machine) ,rehabilitation physician and clinical psychologist, and educational sessions with the patients. We have treated 1160 patients referred from December 2008-February 2014 : 53% STEMI, NSTEMI 36%, 7% stable angina, 4% other . In total, 45% low risk, medium risk 32%, 23% higher risk (according to criteria of the AACVPR). 83% male. Mean age 58 years (29-82a) .We have analyzed the latest 124 patientes treated between July 2013 and February 2014(no differences in basal features with global group) Results:Blood pressure (average): PP 136/75, FP 129/72.Heart rate<70bpm PP68%, FP 86%. Waist circumference > 102 cm in men: PP46%, FP31% ; > 88cm in women: PP65%, FP 35% .Weight loss(this data in non-smokers): 69% of patients (-2,7Kg on average), weight gain 21% of patients (mean +1,4kg), equal 10%.Smoking cessation at 7 months (6-9) from admission with acute coronary syndrome(ACS): 78% (confirmed by co-oximetry) . In diabetic patientes, HbA1c (%) : a) <7: PP56%, FP75%, b) 7-8% PP13% ,FP13 c)> 8: PP31% ,FP12%. LDL-C <70 mg / dl: 25% PP, FP40%; LDLc 70-100mg / dl: PP43% FP 48%. HDL> 45 mg / dl: 35% PP, FP 54% .Functional capacity (METs, on average): PP 9METs vs FP 11.7 . PREDIMED diet adherence: PP 7/14, FP 12/14 .We had no cardiovascular mortality nor acute miocardial infarction(AMI) during the program. At one year from index ACS, only one cardiovascular death(intracranel hemorrage), and no newer AMI.
Conclusions:good control of CVRF is achieved with modern CR programmes with a clear benefit added to conventional cardiac pre-program control. We must implement the use of CR, still underused in our environment.
P595
Added value of physiotherapy in patient receiving Left Ventricular Assistance Devices.
M Lamotte1, E Mkeidze1, G Van Nooten2, M Antoine2
1Erasme Hospital (ULB), Physiotherapy and cardiac surgery department, Brussels, Belgium
2Erasme Hospital (ULB), Cardiac surgery department, Brussels, Belgium
Background:: LVAD are more and more efficient and proposed to an increased amount of heart failure patient. Actually, 25000 devices have been implanted around the world and approximately 2000 are now implanted yearly. Those devices allows not only to reduce the mortality of the patient, but also lead the patient on a more optimal status for the transplantation when, only the "bridge to transplant" indication is recognized. Waiting for the Expert flow chart of the ESC, exercise guidelines or recommendations for exercise training in such a population are not clearly established and actually based on CHF recommendation. Supervision parameters need to be clarified. Our study present the rehabilitation proposed in our centre. This rehabilitation is divided in post-operative intra-hospital phase and in ambulatory exercise training sessions. Our population is composed by 50 patients implanted on a period of three years, by a continuous "HeartWare®" device. Exercise capacity variable are obtained during a maximal cardiopulmonary exercise testing (CPET). A sub-group of patients follows a structured rehabilitation.
Results:The physiotherapy proposed during the immediate post-operative period (means hospital stay is 4 weeks) is a "classical" post-operative program for heart surgery patient and consist of respiratory physiotherapy, mobilisation and ambulation. The ambulatory phase's program consists of interval training on bicycle ergometer, treadmill, rowing machine, step based on the CPET results (workload, not HR or blood pressure not accurate in this kind of patient), and different resistance training exercises realised progressively at 75 % of 1-RM. The mean stay in ICU is 7 days, patients are discharged from the hospital after a mean of 28 days. The exercise capacity (VO2p) of our patient at one month after implantation is 46 % of PV, for a RER of 1.27. At 6 and 12 month, VO2p is at 60 and 57% of PV. We observe a large variation between our patient in terms of VO2p : for example, at 6 month, from 33 to 98 % of PV. An important factor that explains those differences is the participation to a readaptation program as illustrate on a sub-group of our patient who did it regularly (VO2p : 67 versus 45 % of PV).
Conclusion:: LVAD allows the patient to recover an active life and allow them to follow a structured rehabilitation. The exercise capacity is severely depressed in some patient, but increase during the first 6 month. Only patient following a structured program of exercise recover significantly. Our study demonstrates the feasibility and the efficacy of exercise training in such patient.
P597
Quality of life on long-term follow-up after acute coronary ischemia
N Pogosova1, V Vygodin1, A Karpova1, Y Pozdnyakov1
1National Center for Preventive Medicine, Moscow, Russian Federation
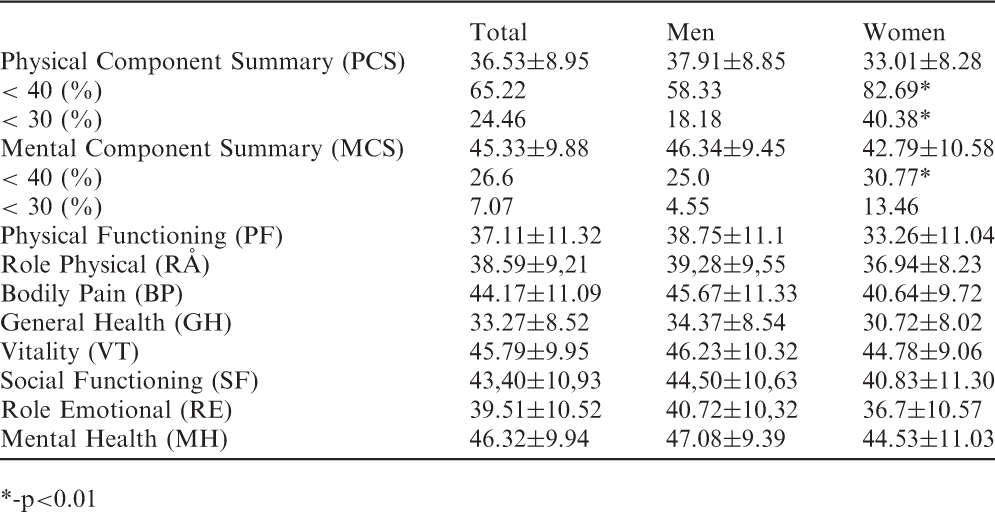
Low quality of life is known to be associated with poor prognosis in patients after cardiovascular events. The aim was to study the gender-specific differences of quality of life in coronary heart disease patients on long-term follow-up.
Methods:190 consecutive patients (aged 35-80) hospitalized for acute coronary ischemia (ACI) to a city hospital were identified retrospectively and interviewed in average 2 years after the event. Quality of life (QL) was studied by means of EQ-5D and SF-12v2 questionnaires.
Results:10.5% patients (mean age 64,5±10,9) died: 3.2% in hospital and 7.4% during follow-up. 82.1% patients were interviewed. The total QL EQ-5D score at the end of follow-up was 0,7±0,19 (0,6±0,18 in women and 0,7±0,19 in men). According to the SF-12v2 questionnaire women had significantly lower QL after ACI as compared to men. This finding was true for both integral parameters of QL and most subscales of QL (Table 1). Especially low QL was found in women older 60 years.
Conclusions:Quality of life in women is substantially lower 2 years after ACI. This could be result of lower participation of women in cardiac rehabilitation programs, higher drop-out of these programs, and need special attention.
*-p<0.01
Total
Men
Women
Physical Component Summary ( PCS )
36 . 53±8 . 95
37 . 91±8 . 85
33 . 01±8 . 28
< 40 (%)
65 . 22
58 . 33
82 . 69 *
< 30 (%)
24 . 46
18 . 18
40 . 38 *
Mental Component Summary ( MCS )
45 . 33±9 . 88
46 . 34±9 . 45
42 . 79±10 . 58
< 40 (%)
26 . 6
25 . 0
30 . 77 *
< 30 (%)
7 . 07
4 . 55
13 . 46
Physical Functioning (PF)
37 . 11±11 . 32
38 . 75±11 . 1
33 . 26±11 . 04
Role Physical (RO
38 . 59±9,21
39,28±9,55
36 . 94±8 . 23
Bodily Pain (BP)
44.17±11.09
45.67±11.33
40.64±9.72
General Health (G H)
33 . 27±8 . 52
34 . 37±8 . 54
30 . 72±8 . 02
Vitality (VT)
45 . 79±9 . 95
46 . 23±10 . 32
44 . 78±9 . 06
Social Functioning ( SF )
43,40±10,93
44,50±10,63
40 . 83±11 . 30
Role Emotional ( RE)
39 . 51±10 . 52
40 . 72±10,32
36 . 7±10 . 57
Mental Health (MH)
46 . 32±9 . 94
47 . 08±9 . 39
44 . 53±11 . 03
P598
Supplementation with resveratrol does not affect muscle oxidative capacity in coronary artery disease patients in the short term.
A Avila1, M Diaz2, E Coeckelberghs1, L Vanhees1, V Cornelissen1
2Manchester Metropolitan University, Health Care Science, Manchester, United Kingdom
Resveratrol is a polyphenol phytoalexin derived from red grapes, peanuts and berries with many functions including anti-inflammatory, antioxidant and immunomodulatory effects. In vivo studies have shown that resveratrol improves mitochondrial function. In humans, the oxidative capacity of skeletal muscles decreases with aging partly as a consequence of a lower number of mitochondria units. Hence, we hypothesize that resveratrol might improve oxidative capacity in humans by improving mitochondrial function. Exercise-onset VO2 kinetics has been shown to be a reliable tool for the evaluation of oxidative capacity of skeletal muscle. Therefore, we aimed to assess the effect of short term supplementation with resveratrol on muscle oxidative capacity, by means of exercise-onset VO2 kinetics in coronary artery disease patients Methods:A controlled single blind cross-over study was performed to investigate the immediate effect of resveratrol on muscle oxidative capacity in 10 coronary artery disease patients (9 men, mean age 67.2 ± 7.45 years, mean BMI of 27.1 ± 4 kg/m2) participating in phase 3 of cardiac rehabilitation. Patients completed two blinded exercise sessions which included two six-minute constant load bouts at 30% of their maximal load, separated by a 6-minute recovery rest interval. The first session was performed after placebo supplementation; the second was performed after resveratrol supplementation (3 days, 1 g/day). Oxygen uptake (VO2 mL/min) was measured breath-by-breath and averaged every 10 seconds. Muscle oxidative capacity was assessed by calculation of exercise onset oxygen uptake kinetics and expressed as mean response time (MRT). Statistical analyses were performed by means of Wilcoxon Test. Statistical significance was set at P<0.05.
Results:Muscle oxidative capacity, expressed as MRT, median 46.3 (24.37-92.35) under placebo didn't change significantly following short-term resveratrol supplementation, median 42.3 (22.5-69.55 MRTs; p=0.67). VO2 steady-state median 1194 (756-1585ml/min) didn't change after resveratrol supplementation, median 1101 (756-1628ml/min; p=0.67). No effect of resveratrol was observed for Oxygen Deficit (p=0.85) or actually achieved VO2 (p=0.76). No adverse effects were reported following resveratrol supplementation.
Conclusions:In patients with coronary artery disease, the results of the present study suggest that in the short-term resveratrol does not improve muscle oxidative capacity. However, further studies are warranted with longer treatment time to elucidate the potentials of resveratrol on muscle metabolism and oxygen on kinetics.
P599
Effects of a physical rehabilitation program for impaired ambulatory function in patients older than 80 years: the Ambulatory Independent Discharge for Elderly (AIDE) project
H Obata1, T Izumi2, A Uehara2, H Watanabe1, T Minamino1
1Niigata University, Niigata, Japan
2Niigata Minami Hospital, Niigata, Japan
Background:Japan is thought to have the highest proportion of elderly people in the world; 26% are aged 65 years or above, and 13% aged 75 years or above. Accordingly, there are a large number of elderly persons with impaired gait who need rehabilitation. The Ambulatory Independent Discharge for Elderly (AIDE) project is our original rehabilitation program based on cardiac rehabilitation methods for restoration of independent gait in elderly inpatients. In this study, we studied the effects of AIDE rehabilitation in ambulatory function in very elderly patients, aged over 80 years.
Methods:AIDE rehabilitation is comprised of prescribed, progressive aerobic, resistance, and balance trainings. In order to continue daily trainings at home after discharge, resistance and balance trainings were performed using the participants' own bodyweight, and not a special machine. AIDE rehabilitation was performed in inpatients who had ambulatory impairments during hospitalization. We compared the effects of AIDE rehabilitation program on gait speed and various physical performance measurements between patients aged from 60 to 79 years (elderly group) and those aged 80 years or above (very elderly group).
Results:This study included 69 consecutive inpatients who received AIDE rehabilitation with patients' own body weight (20 patients in elderly group, 49 patients in very elderly group). The mean age was 86 ± 4 years, and 28 patients (57%) were women. Decreased gait speed <0.8 m/s was more common in very elderly group (63%) than elderly group (33%). Low knee extension strength <0.4 kgf/kg body weight was common in very elderly group (77%) than elderly group (53%); However the frequency of short functional reach <30 cm, and short one-leg standing duration <15 s were similar between two groups. By AIDE rehabilitation during 32 ± 20 days, the mean walking speed was significantly improved in both groups. The physical performance measurements including knee extension strength, functional reach, and one-leg standing duration were also improved in both groups. The improvement of gait speed was similar between very elderly group (36 ± 41%) and elderly group (35 ± 38%). The frequency of patients who restored independent gait at the time of discharge was similar between very elderly group (28%) and elderly group (24%).
Conclusions:The simple exercise program of AIDE rehabilitation project, mainly by using the participants' own bodyweight, was effective in restoration of independent gait in elderly patients regardless of age.
P600
The influence of training modalities on the effect of exercise training in patients with coronary artery disease: a meta-analysis
J J Kraal1, T Vromen1, HMC Kemps2, G Van Valkenhoef3, J Kuiper3, N Peek4
1Academic Medical Center, University of Amsterdam, Department of Medical Informatics, Amsterdam, Netherlands
2Maxima Medical Centre, Department of Cardiology, Veldhoven, Netherlands
3University Medical Center Groningen, Department of Epidemiology, Groningen, Netherlands
4University of Manchester, Department of Health eResearch Centre, Manchester, United Kingdom
Topic: Sports cardiology
Purpose:Exercise training in patients with coronary artery disease (CAD) improves their exercise capacity and long-term survival. However, training modalities (intensity, frequency, duration) differ between studies and it is unclear which training modality is most effective for improving exercise capacity. Therefore, we conducted a meta-analysis to study the influence of the different training modalities on the effect of exercise training.
Methods:A systematic search was conducted in MEDLINE and EMBASE for papers published between 1 April 2007 and 1 September 2013, addressing CAD patients performing aerobic exercise training during cardiac rehabilitation. We included randomized studies that compared aerobic exercise training programs with other training regimes or with usual care, and that evaluated peak oxygen uptake as outcome measure. We performed univariate random effects meta-regressions on each of the following training modalities: training intensity (% heart rate), session duration (minutes), weekly session frequency, program duration (weeks), session energy expenditure (EE, intensity*duration), weekly EE (frequency*session EE) and total EE (program duration*weekly EE). The resulting models were ranked according to their fit.
Results:A total of 14 studies were included, involving 747 patients. Overall, training intensity appeared to be the best predictor for improvement in exercise capacity. Peak oxygen consumption improved with 3.3 ml VO2.min-1.kg-1 for each 10% increase in exercise intensity (95%CI 1.35 to 5.32 ml VO2.min-1.kg-1, p=0.001). Total EE and weekly EE were significantly associated with exercise capacity as well (p=0.002 and p=0.020 respectively), while session EE, program duration and session duration were not. Weekly session frequency showed borderline significance (p=0.051). However, for all training modalities there was considerable heterogeneity in effect size (I2 ranging from 69% to 84%), indicating that there was unmeasured confounding.
Conclusions:In CAD patients, exercise intensity appears to be the most important determinant of the improvement in exercise capacity after physical training. However, the considerable heterogeneity demands a cautious interpretation of the results.
P601
Predictors of improvement of autonomic nervous system function in patients after cardiac rehabilitation
P Rio1, A Abreu1, R Soares1, R Pereira-Da-Silva1, S Aguiar Rosa1, A Viveiros Monteiro1, I Rodrigues1, M Afonso Nogueira1, T Alves1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Autonomic nervous system (ANS) can be evaluated, in the clinical practice, by measuring resting heart rate (RHR), heart rate recovery (HRR) or heart rate variability (HRV) during exercise test. These parameters have prognostic significance in secondary prevention. The aim of the present study is to assess the cardiac rehabilitation (CR) benefit on ANS and to determine which factors are associated with its improvement.
Methods:Retrospective analysis of consecutive patients (pts) who underwent CR program (2004-2013), in a single center. 24-hour Holter HRV study, cardiopulmonary exercise testing (CPET), echocardiogram and blood tests were performed at baseline and after 36 exercise training sessions. The following parameters were evaluated: standard deviation of NN intervals (SDNN), ms, HRR, RHR, peak HR, bpm, peak oxygen uptake (pVO2), mL/Kg/min, production (VE/VCO2) slope, left ventricular ejection fraction (LVEF), %, glycaemia, sedimentation velocity (SV), high sensitive protein c reactive (hs-CRP), cholesterol level and natriuretic peptides. We studied the association of CAD risk factors, CPET, echocardiogram and blood tests parameters with SDNN, HRR and RHR improvement.
Results:We analysed 208 pts, 85% male, mean age 56.7±10.4 years. Of these, 113 pts (55%) had ST-elevation myocardial infarction (STEMI) diagnosed. There were significant differences between pre- and post-CR values in: SDNN (120.5±41.2 vs 127.5±42.1, p=0.022), HRR (23.9±13.8 vs 26.7±12.4, p=0.029), basal HR (71.4±11.1 vs 69.3±10.6, p=0.01), peak HR (136.4±21.7 vs 139.2±21.9, p=0.025), HR reserve (64.9±21.3 vs 69.9±21.6, p<0.001), pVO2 (25.4±6.8 vs 27.4±7.2, p<0.001), VE/VCO2 (26.1±5.4 vs 24.4±4.8, p=0.049), LVEF (53.1±11.4 vs 54.7±10.5, p=0.031). Baseline non-obese (OR 2.75, 95% CI 1.4-5.4, p=0.004), hypertension (OR 1.87, 95% CI 1.0–3.5, p=0.047) and beta-blocker use (OR 4.84, 95% CI 1.1–22.3, p=0.043) were associated with RHR improvement; baseline non-diabetes (OR 3.4, 95% CI 1.4–8.7, p=0.009), LVEF > 35% (OR 4.6, 95% CI 1.1–20.3, p=0.044) and E/A ratio < 1 (OR 2.8, 95% CI 1.2–6.3, p=0.017) were associated with SDNN improvement; baseline reduced hs-CRP levels (OR 0.98, 95% CI 0.97–1, p=0.031), increased HDL (OR 1.04, 95% CI 1–1.07, p=0.021) and normal LVEF (OR 2.1, 95% CI 1.1–4.3, p=0.034) were associated with HRR improvement.
Conclusion:CR program induced a positive modulation of the ANS function in different clinical settings. The absence of diabetes and obesity, as well, as the presence of normal LVEF and high HDL-cholesterol level predicted larger benefit on ANS balance.
P602
Cardiac rehabilitation effectiveness: how good is it in stable coronary artery disease?
P Rio1, A Abreu1, R Soares1, S Aguiar Rosa1, T Pereira-Da-Silva1, I Rodrigues1, A Viveiros Monteiro1, G Portugal1, M Afonso Nogueira1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Cardiac Rehabilitation (CR) programs are effective in improving functional capacity and in reducing total and cardiovascular mortality. It is not completely clarified which groups of patients (pts) benefit more with exercise training. The aim of the present study is to compare the impact of CR in different clinical settings of pts with coronary heart disease and evaluate specifically the gain obtained in stable coronary artery disease (CAD) patients.
Methods:Retrospective analysis of consecutive CAD pts who underwent CR program (2004-2013), in a single center. 24-hour Holter HRV study, cardiopulmonary exercise testing (CPET), echocardiogram and blood tests were performed at baseline and after 36 exercise training sessions. Exercise sessions were performed in hospital, three times a week, 60 minutes duration. The following parameters were evaluated: standard deviation of the average of NN intervals (SDNN), ms, basal heart rate (HR), peak HR, HR recovery, HR reserve, peak oxygen uptake (pVO2), %, left ventricular ejection fraction (LVEF), %, sedimentation velocity (SV), mg/dL, high density cholesterol (HDL), mg/dL, and natriuretic peptides (NT_proBNP), pg/mL. Patients were divided and analysed according previous event, in three groups: ST-elevation myocardial infarction (STEMI), non-STEMI and stable CAD.
Results:We analysed 192 pts, 85% male, mean age 56.3±10.12 years. Of these, 113 pts (59%) had STEMI, 52 pts (27%) had non-STEMI and 27 pts (14%) had stable CAD. There were significant differences between pre- and post-CR values in: basal HR (71.2±10.6 vs 68.8±10.3, bpm, p=0.009), peak HR (137.7±21.8 vs 141.7±20.7, bpm, p=0.002), HR recovery (23.7±13.8 vs 27.6±12.2, bpm, p=0.003), HDL (38.5 ±10.6 vs 41.5±9.8, mg/dL, p<0.001), SDNN (120.1±40.4 vs 127.9±42.3, ms, p=0.015) and in the variables showed on the table. There were significant differences pre- and post-CR, between pts with STEMI and stable CAD in SV (?% 9.2 ±72.6 vs -17.9 ±45.1, p=0.042), NT_proBNP (?% -46.6 ±46.2 vs -0.1 ±65.9, p=0.007), pVO2 (? 10.2 ±30 vs -0.8 ±20.6, p=0.029) and LVEF (?% 4.5 ±16.6 vs 9.7 ±13.8, p=0.048).
Conclusion:Cardiac rehabilitation program induced significant improvement of functional capacity, autonomic nervous system, cardiac function, HDL, and systemic inflammation in different clinical settings of coronary heart disease. Patients with stable CAD, although achieving less benefit in functional capacity, obtained a greater benefit in systolic function and in systemic inflammation reduction than patients with acute coronary syndromes.
P603
The benefits of using short combined aerobic-resistance training versus load match aerobic training for cardiorespiratory responses in coronary heart disease
PM Lepretre1, R Feron2, M Bulvestre1, T Porcher2, M Ghannem2
1University of Picardie Jules Verne, UFR-STAPS, Lab. Physiological Adaptations to Exercise and Rehabilitation (APERE), EA-3300, Amiens, France
2Centre de réadaptation Cardiaque , Tracy-Le-Mont, France
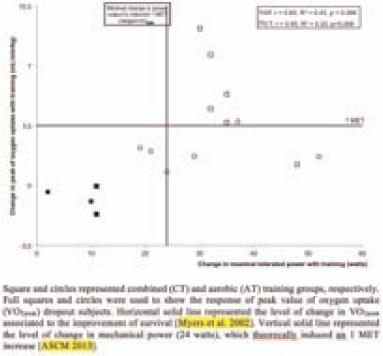
Exercise was a component of secondary prevention in cardiac rehabilitation but its beneficial effects seemed to depend of type, duration and intensity of physical activity. To compare the effect of exercise modalities on cardiorespiratory responses, 16 men with coronary heart disease (59.2±6.5y, 1.75±0.07m, 84.3±14.9kg, LVEF: 0.53±0.08) performed 4 weeks of exercise rehabilitation based on combined aerobic – resistance training (CT, n=8) or aerobic training (AT, n=8) with similar training load, quantified using the session rating of perceived exertion. Maximal tolerated power (MTP), peak values of oxygen uptake (VO2peak) and heart rate and VO2 associated at the ventilatory anaerobic threshold (VAT) were determined during an incremental cycling exercise. Both training induced significant increases in VO2peak (15.5±2.8 vs. 19.2±5.3 mL.min-1.kg- 1, and 15.9±4.1 vs. 17.3±4.4 mL.min-1.kg-1, for CT and AT, respectively, p<0.05)) and MTP (CT: 110.4±24.9 vs. 139.6±24.8 watts and AT: 109.0±27.8 vs. 133.3±36.9 watts, p<0.01). In each group, a closer look at individual data show that training effects on VO2peak occurred in 6 out of 8 subjects (figure). In these subjects, improvements in VO2peak were larger after CT (+33.9 ± 17.9 % of pre-training VO2peak, i.e. +5.3 ± 2.8 mL.min-1.kg-1) than observed after AT (+13.4 ± 4.7 % of pre-training VO2peak, i.e. +2.0 ± 1.0 mL.min-1.kg-1) (p<0.01). Such observations could not be made for MTP (p>0.05). VO2 associated to VAT was significantly improved after CT but not after AT. In conclusion, these results suggested that short CT and AT programs improved cardiorespiratory responses with different central and peripheral adaptations. This might be taken into account for exercise rehabilitation according initial patient limitations.
Change in VO2peak with training
P604
Mindfulness training in post-myocardial infarction patients with elevated depressive symptoms: a pilot study of feasibility and effectiveness
O Lundgren1, P Garvin2, L Nilsson1, M Kristenson2, L Jonasson1
1Linkoping University, Department of medical and health sciences, division of cardiovascular medicine, Linkoping, Sweden
2Linkoping University, Department of medical and health sciences, division of community medicine, Linkoping, Sweden
Topic: Sports cardiology
Purpose:Depression is associated with an increased risk of recurrent cardiac events in patients with previous myocardial infarction (MI). Still, it remains a challenge to identify patients with depressive symptoms and offer appropriate treatment. In this study, we first investigated whether depressive symptoms remained one year after an MI. Secondly; we tested the feasibility and effectiveness of mindfulness-based stress reduction (MBSR) in post-MI patients with elevated depressive symptoms.
Methods:Depressive symptoms were assessed by using the CES-D scale in 160 consecutive patients, one and twelve months after an MI. Based on these results, we defined an inclusion criterion for depressive symptoms and started a new screening of 171 patients. Patients were invited to participate in an 8-week MBSR group intervention. CES-D scores and GAD-7 scores (anxiety) were determined before and after the program.
Results:The first screening showed CES-D scores of median 7 (IQR 3;12) at 1 month, and remained unchanged after 12 months, median 7 (3;12). In the second screening, 79 patients with CES-D scores > 7 at 1 month were invited to participate in MBSR. Twenty-nine patients accepted, of whom 24 started MBSR and 16 completed the full program. In this group, mean CES-D scores were 19.2 (median 18) at screening, 19.8 (18) pre-MBSR and 13.3 (14) post-MBSR; a decrease by 33 %, (p=0.006). Mean GAD-7 scores changed from 7.5 (median 7,5) to 4.3 (4.5) after the intervention; a decrease by 43% (p=0.004).
Conclusions:Data from the yearlong follow-up of post-MI patients showed unchanged levels of depressive symptoms. We invited patients with CES-D > 7 to an 8-week MBSR intervention and found that 20 % accepted to participate and also completed the program. Depressive symptoms and anxiety were significantly reduced, lending support to MBSR as a promising tool for selected post-MI patients.
P605
Recognition of depression in medical settings
N Pogosova1, A Kursakov1, V Vygodin1
1National Center for Preventive Medicine, Moscow, Russian Federation
Depression is a well established cardiovascular risk factor. Depression and even minor depressive symptoms are associated with lower medication adherence and worse prognosis. Although depression is highly prevalent, it is still underdiagnosed and undertreated. The use of short screening questionnaires may improve the recognition of depression in different medical settings. The Patient Health Questionnaire (PHQ -9) has become increasingly popular in research and practice over the past decade in a number of countries, and have not been adapted for Russian-speaking populations before the current study.
Aim:We conducted this study to evaluate the validity of the Russian version of PHQ-9 as a screening tool for detecting depression in a sample of general medical practice patients.
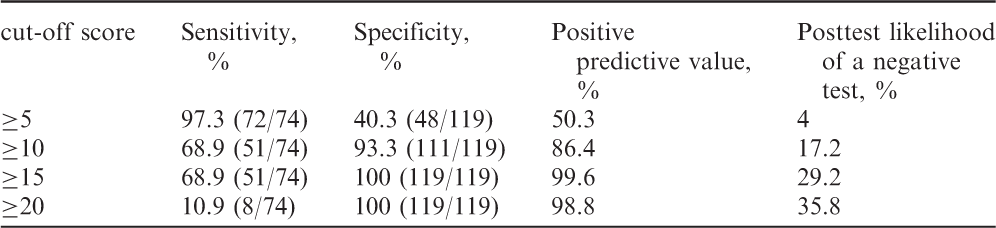
Methods:193 consecutive patients (63 men and 130 women; mean age 34.6+11.4 years) attended a general medical practice setting completed the PHQ-9 questionnaire and then were interviewed by a psychiatrist in a blind manner. The gold standard was the structured diagnostic interview, based on the International Classification of Diseases-10 criteria for depressive episode. Statistical analysis has been done to estimate sensitivity, specificity and positive predictive value and posttest likelihood of a negative test.
Results:The results are presented in the Table 1. The optimal cut-off point for detecting depression was 10 (with sensitivity of 68.9% and specificity of 93.3%).
Conclusions:The brief Patient Health Questionnaire (PHQ-9) was found to have acceptable screening properties for detecting depression in the primary care setting for cuff-of point 10.
cut-off score
Sensitivity, %
Specificity, %
Positive predictive value , %
Posttest likelihood of a negative test, %
=5
97.3 (72/74)
40.3 (48/119)
50.3
4
=10
68.9 (51/74)
93.3 (111/119)
86.4
17.2
=15
68.9 (51/74)
100 (119/119)
99.6
29.2
=20
10.9 (8/74)
100 (119/119)
98.8
35.8
P606
The effects of thyroid hormones and inflammatory markers on health-related quality of live in coronary artery disease patients admitted for cardiac rehabilitation program
J Brozaitiene1, N Mickuviene1, M Staniute1, N Kazukauskiene1, R Bunevicius1
1Behavioral Medicine Institute, Lithuanian University of Health Sciences, Palanga, Lithuania
The aim of the study was to evaluate the effects of thyroid hormones and inflammatory markers on health-related quality of live (HRQoL) in coronary artery disease (CAD) patients depending on the severity of the disease.
Methods:640 CAD patients, 2 weeks after acute myocardial infarction (MI) or unstable angina pectoris, admitted for rehabilitation program (RP), were invited in the study. All patients (mean age 58±9 years, 76% male) were evaluated for demographic, clinical data, the New York Heart Association (NYHA) class and HRQoL using the 36-item Short Form Medical Outcome Questionnaire (SF-36). Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety (HADS-A) and depression (HADS-D) symptoms. Serum concentrations of high sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), thyroid hormones: free T3 (T3), free thyroxine (T4), reverse T3, total T4 were analyzed. Univariate and multivariate linear regression models were used to examine relationships between all thyroid hormones, inflammation markers and HRQoL separately for NYHA I-II and NYHA III class patients.
Results:In sum, 420 patients (63%) were after MI, 429 (67%) – after percutaneous coronary intervention, 521 (81%) were NYHA I-II, 119 (19%) – NYHA III class. Multivariate linear regression analyses, adjusted for gender, age, angina pectoris class, HADS-A and HADS-D score revealed that in NYHA I-II class patients higher hs-CRP (?-.097, p<.05), IL-6 concentrations (?-.141, p<.01) were associated with poorer physical functioning, lower IL-6 - with less pain (?-.088, p<.05) and higher free T3 (?.093, p<.05) - with fewer role limitation due to physical problems. In NYHA III class patients, after controlling for potential confounders, higher concentrations of hs-CRP was associated with more role limitations due to emotional problems (?-.212, p<.05), more expressed pain (?-.224, p<.05). Better perception of mental health was related with higher reverse T3 (?.183, p<.05), lower free T3 (?-.173, p<.05), and greater energy/vitality - with higher reverse T3 (?.208, p<.05).
Conclusions:In CAD patients post-acute cardiac events with NYHA I-II class admitted for RP higher concentrations of hs-CRP, IL-6 and lower free T3 are associated with poorer physical problems and pain components of HRQoL. In NYHA III class patients lower reverse T3 level is associated with worse mental health, lower energy/vitality and elevated levels of hs-CRP, IL-6 – with poorer mental and increased pain components of HRQoL. This research was funded by the European Social Fund under the Global Grant measure, Grant VP1-3.1-SMM-07-K-02-060.
P607
Smoking cessation intervention after acute myocardial infarction, predictors of relapse
R A Mori Junco1, R Dalmau Gonzalez Gallarza1, A Castro Conde1, O Gonzalez Fernandez1, C Alvarez Ortega1, Z Blazquez Bermejo1, J Caro Codon1, I Ponz De Antonio1, JL Lopez Sendon1
1University Hospital La Paz, Cardiology, Madrid, Spain
Background:Taking into account the burden of tobacco in cardiovascular prognosis, smoking cessation is a priority in secondary prevention programs. We analysed the predictors of relapse of a smoking cessation intervention in coronary disease patients.
Methods:448 smoker patients (85,5% male) referred to a cardiac rehabilitation program after a recent admission for acute myocardial infarction were analyzed. Most of them were heavy smokers (mean consumption of 24,5 cig/day, 41,2 pack-year). The intervention was based in an average of 3 individual visits during the first 3 months, one group session, and one follow-up visit after 6 months. Diet and exercise counselling was given. First line smoking cessation pharmacotherapy was offered to all patients as a possibility. Smoking abstinence was confirmed with co-oximetry at 3 and 6-month follow-up visits. A multivariate analysis was performed in order to study the predictors of relapse.
Results:mean age was 53.6, 57% were hypertensive, 23% diabetic, 60% dislipidaemic, 27% obese and 7% had been previously diagnosed with chronic obstructive pulmonary disease (COPD). Pharmacotherapy for smoking cessation was requested in 31%, varenicline was used in 57% of them, nicotine replacement therapy in 33% and bupropion in 10%. Patients lost to follow-up (3% at month 3, 6% at month 6) were considered as having relapsed. Abstinence rate was 76,6% at month 3, and 71% at month 6. Following a multivariate analysis, the predictors of relapse were found to be the number of cigarettes smoked per day, the number of pack-year, the use of smoking cessation drugs, dropping out of the program, and having a previous condition of COPD.
Conclusion:smoking cessation interventions after an acute myocardial infarction are effective. A high degree of motivation facilitates the abstinence even in the absence of pharmacotherapy. A high degree of addiction and dependence, the need of smoking cessation drugs, lack of adherence and a previous condition of COPD were predictors of relapse.
Abstinence
Relapse
p
Cig/day
23,2
29,5
<0,001
Pack-year
38,4
51,6
<0,001
Non adherence to the program
6,3%
29,5%
<0,001
Pharmacotherapy use
19,8%%
54,3%
<0,001
P608
Effects of smoking cessation on autonomic nervous system among patients attending a cardiac rehabilitation program
P Rio1, A Abreu1, R Soares1, T Pereira-Da-Silva1, A Viveiros Monteiro1, S Aguiar Rosa1, I Rodrigues1, M Afonso Nogueira1, P Pinto-Teixeira1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Tobacco use leads to an increased sympathetic nerve activity and therefore a dysfunction of autonomic nervous system (ANS). These alterations may play an important role in the relation between smoking and mortality. Smoking cessation alone has been associated with ANS improvement. The objective of this study is to evaluate the effect of cardiac rehabilitation (CR) and smoking cessation on ANS in patients (pts) with coronary artery disease (CAD).
Methods:Retrospective analysis of CAD pts who underwent CR program (2004-2013), in a single center. 24-hour Holter HRV study and cardiopulmonary exercise testing were performed at baseline and after 12-week training program. Exercise sessions were performed three times a week, 60 minutes duration. The following parameters were evaluated: standard deviation of the average of NN intervals (SDNN), resting heart rate (RHR) and heart rate recovery (HRR) in the first minute. Pts were analysed according to tobacco use and smoking cessation.
Results:We analysed 168 pts, 85% male, mean age 57.3±10.4 years. Of these, 47% were smokers and 61% of these quit smoking. According to non-smoking vs smoking patients, there were no significant differences, between basal values of: RHR (72 ±11 vs 71±11, p=ns), HRR (24±12 vs 22±12, p=ns), SDNN (115±38 vs 121±43, p=ns). In the group of persistent smoking there were not significant difference between pre and post-CR values of: RHR (70 ±11 vs 71±11, p=ns), HRR (25±12 vs 25±12, p=ns), SDNN (117±37 vs 115±36, p=ns). There were significant differences between pre and post-CR values of RHR, HRR and SDNN, in non-smokers patients and those who quit smoking. This analysis is shown on the table.
Conclusion:Non-smoking and smoking cessation significantly enhances cardiac autonomic function in patients with coronary artery disease after a cardiac rehabilitation program. Instead, patients who sustained smoking habits have not improved the autonomic nervous system.
*for the differences between the two groupsCR = cardiac rehabilitationns = not significant
Non-smoking
Smoking Cessation
Parameters
Before CR
After CR
Variation, %
p value
Before CR
After CR
Variation, %
p value
p value*
Resting HR ( bpm )
72 ± 11
69 ±9
- 2.3 ±16
0.004
71 ± 9
67 ±10
-6.2 ±10
0.01
0.038
HR recovery ( bpm )
24 ±11
29 ± 12
4.2 ± 12
0.001
24 ±10
32 ±14
6.9 ± 12
0.02
ns
SDNN ( ms )
115 ±38
128 ±44
16 ±40
0.002
121 ±31
134 ±38
13 ±29
0.03
ns
P609
Differences in lipid profile between current smokers and non smokers after acute myocardial infarction
Z Blazquez Bermejo1, R Mori Junco1, R Dalmau1, A Castro1, C Alvarez1, J Caro Codon1, I Ponz De Antonio1, D Gemma1, SO Rosillo1, JL Lopez-Sendon1
1University Hospital La Paz, Cardiology, Madrid, Spain
Topic: Sports cardiology
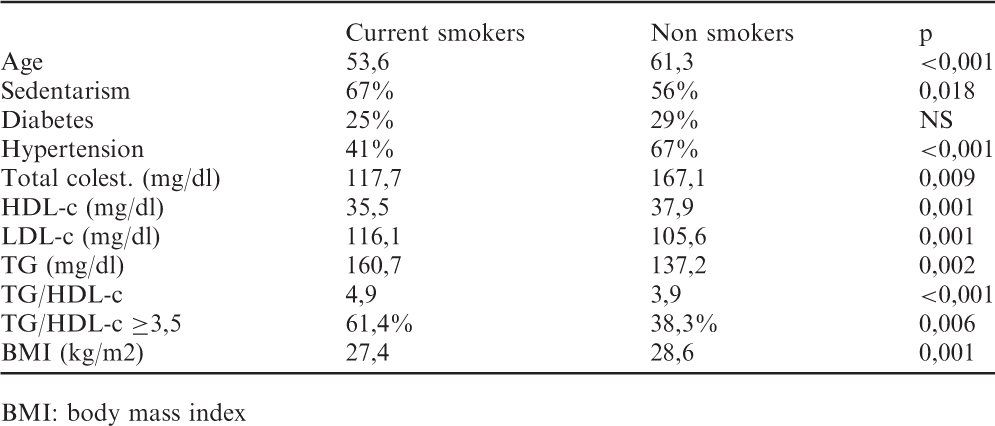
Purpose:Smoking is an important risk factor of cardiovascular disease, whose deleterious effect is enhanced by the induction of smoking-related l?d abnormalities. We compared the l?d profile of patients with a recent acute myocardial infarction (AMI) according to their smoking status.
Methods:611 patients admitted to a cardiac rehabilitation program after an AMI were analyzed. 84% were male, 57% current smokers, 22% former smokers. We analyzed the lipid profile from a fasting blood test performed during admission. Results (see table): Active smokers with AMI were on average 8 years younger, nevertheless sedentarism was more prevalent in smokers. Obesity was more prevalent in non smokers, but obesity and being overweight were also common conditions in active smokers, despite the anorexic properties of nicotine. L?d profile in current smokers was particularly unfavorable, with significantly lower level of HDL cholesterol (HDL-c), and higher level of triglycerides (TG). Smokers were more likely to have HDL=35 mg/dl (57% vs 40%, p<0,001), and TG>150 mg/dl (41% vs 29%, p=0,003). The TG to HDL ratio, an accepted predictor of insulin resistance when =3,5, was significantly higher in smokers.
Conclusion:Active smoking is commonly related to other lifestyle abnormalities, whose interaction promotes a particularly atherogenic l?d profile, and a higher insulin resistance. Besides the smoking cessation intervention, a complete lifestyle correction should be a target in secondary prevention programs.
BMI: body mass index
Current smokers
Non smokers
p
Age
53,6
61,3
<0,001
Sedentarism
67%
56%
0,018
Diabetes
25%
29%
NS
Hypertension
41%
67%
<0,001
Total colest. (mg/dl)
117,7
167,1
0,009
HDL-c (mg/dl)
35,5
37,9
0,001
LDL-c (mg/dl)
116,1
105,6
0,001
TG (mg/dl)
160,7
137,2
0,002
TG/HDL-c
4,9
3,9
<0,001
TG/HDL-c =3,5
61,4%
38,3%
0,006
BMI (kg/m2)
27,4
28,6
0,001
P611
Strong correlation of central hemodynamic and peripheral skeletal muscle function in stable heart failure patients
C Deluigi1, M Nil1, D Herzig1, J-P Schmid1, P Eser1, M Wilhelm1
1Bern University Hospital, Cardiology, Bern, Switzerland
Background:Reduced exercise capacity is a prominent limiting symptom in patients with congestive heart failure (CHF), and attributable to both central and peripheral factors. We aimed to investigate the relationship between peak oxygen uptake (VO2), cardiac output (CO), and peripheral muscle function in chronic, stable CHF patients.
Methods:CHF patients, who had completed a 3-months outpatient cardiac rehabilitation program at our institution within the last 5 years were contacted. Clinically stable patients with a history of CHF of at least 6 months were included. A cross-sectional observational study design was chosen. Participants underwent a symptom limited cardiopulmonary exercise test (CPET) for assessment of peak VO2, followed by isometric knee-extension force measurements (Fmax) and peripheral quantitative computed tomography for measurement of thigh cross-sectional muscle area (CSAthigh). During a separate session, stress hemodynamic measurement by means of inert gas rebreathing (IGR) was performed to assess maximum CO. Parameters were indexed for body weight, body surface area or CSAthigh, as appropriate. Correlations were assessed using Pearson's R.
Results:A total of 27 patients were included in the study. Isometric knee-extension force data was of sufficient quality in 25, and data of CO measurements in 17 patients. Mean age was 63±9 years, mean body mass index 28.1±5.7 kg/m2, resting left ventricular ejection fraction was 35±11%. During CPET, peak VO2 was 17.7±5.2 ml*min-1*kg-1 (range 9.8 to 28.9 ml*min-1*/kg-1), and maximum work rate was 1.39±0.57 W*kg-1. IGR revealed a resting cardiac index (CI) of 1.5±0.3 L*min-1*m-2, and a peak CI of 4.9±1.1 L*min-1*m-2. Fmax was 444.8±159.1 N, Fmax*kg-1 was 5.3±1.5 N*kg-1, and Fmax*CSAthigh-1 was 5.4±1.3 N*cm-2. There were significant correlations of peak VO2 with absolute parameters: peak work rate (r =0.926, p<0.001), CO (r=0.839, p<0.001), and Fmax (r=0.854, p<0.001), and also for peakVO2*kg-1 with normalized parameters: peak CI (r =0.793, p<0.001), Fmax*kg-1 (r=0.793, p<0.001), and Fmax*CSAthigh-1 (r=0.676, p<0.001). The duration of CHF showed no correlation with exercise capacity and parameters of muscle function.
Conclusion:In our sample of chronic, stable CHF patients, exercise capacity was strongly related to both central and peripheral factors. This may be due to reciprocal adaptation of hemodynamic and muscular parameters over time.
P612
Exercise NT-pro-BNP and global longitudinal strain in systemic lupus erythematosus patients
G Gusetu1, D Pop1, D Pop-Mindru1, D Zdrenghea1
1University of Medicine and Pharmacy, Cluj-Napoca, Romania
Background:Systemic lupus erythematosus (SLE) patients present many times myocardial involvement, this being recommended to be early detected to optimize the treatment and to avoid or postpone the cardiac decompensation.
Methods:There were studied 41 SLE patients, 46±11.79 years, 75.6% females and 20 healthy controls 48.2±9.82 years, 75% females. All SLE patients did not present clinical heart diseases. All subjects were submitted to an echo Doppler examination diastolic and systolic function, including global longitudinal strain (GLS) being determinated. All SLE patients but not healthy controls performed a cardiopulmonary exercise testing (CPE) on cycloergometer, peak exercise capacity being determined. Before exercise, at peak effort and two hours after exercise venous blood samples were obtained and NT-pro-BNP determined using ELISA method.
Results:The LVEF was more than 50% in all healthy controls and SLE patients. In turn global longitudinal strain was significantly less in SLE patients (19.15%±1.21 vs 20.45%±1.49, p=0.045). 38.9% of SLE patients presented diastolic dysfunction, in this group GLS being less than in patients with normal diastolic function (18.77±0.84 % vs 19.49±0.91%). This suggest an early involvement of systolic performance, more important in patients with already diastolic dysfunction. During CPE the patients performed a mean 74.77%±10.96% of predicted VO2 Max. The mean values of NT-pro-BNP were: 134.15±64.2pg/ml at rest, 190.17±134.20 pg/ml at peak effort and 233.22±161.13 pg/ml post effort, p>0.005. No correlation was registered between GLS and peak VO2, being known the absence of correlation between systolic performance and exercise capacity even in heart failure patients. In turn it was a negative significant correlation between GLS ant NT-pro-BNP at peak effort (r=-0.499) and post exercise (r=-0.513).
Conclusion:The results suggest that exercise NT-pro-BNP can be used together with GLS for early detection of systolic dysfunction in SLE patients.
P614
The presence of glucose metabolic disorders and subclinical renal insufficiency in patients with ischemic heart disease
S Kostic1, I Tasic2, D Djordjevic2, D Lovic3, D Mijalkovic4
1Institute for Therapy & Rehabilitation "Niska Banja", Niska Banja, Nis, Serbia
2University of Nis, Medical Faculty, Nis, Serbia
3Clinic for internal disease InterMedica-dr Lovic, Nis, Serbia
4Clinic for internal disease "Kardiomedika", Nis, Serbia
Microalbuminuria is the earliest indicator of renal disease attributable to diabetes. Several studies has shown microalbuminuria to be predictive of total mortality and cardiovascular mortality and morbidity.
Topic: Sports cardiology
Purpose:To evaluate the presence of glucose metabolic disorders and subclinical renal insufficiency in patients with ischemic heart disease Metod:The study included 142 patients, with coronary heart disease (mean age 64,01±8,6 years, 108 (76 %) men,) who were in a rehabilitation at the Institute for Treatment and Rehabilitation "Ni?ka Banja". For all patients there was determined: presence of risk factors for cardiovascular disease (hypertension, hyperlipidemia, smoking, diabetes, obesity, gender, age), laboratory analyses, anthropometric measurements, creatinine clearance (CrCl) using Cocroft – Gault equation, eGFR, albumin/creatinine ratio (ACR), oral glucose tolerance test (OGTT) for subjects without diabetes.
Results:According to the presence of diabetes patients were divided into two groups. The first group (I) consisted of subjects without DM, n=99 (69,7%), the second (II) group patients with DM, n=43 (30,3%). The first group had a significantly higher average number of risk factors (p<0,0001) but no significant differences in age and the presence of hypertension. Abnormal OGTT was found in 43 (43,4%) of patients from the first group: 19 (19,2%) had diabetes, 24 (24%) impaired glucose tolerance and was correlated with age. Decline in CrCl (< 89 ml/min) was found in 58% patients I gr. vs 63 % in II gr., <60 ml/min in 24,4:25,6%, n.s. Abnormal ACR was found in 34(34%) of patients I gr. vs 18 (41%) in II gr., n.s. There was no significant difference in mean creatinine and CrCl (I gr. 84±29 vs II gr.79,8±23) between the two groups.
Conclusion:Patients with unknown history of diabetes have a high incidence of glucose metabolic disorders and subclinical renal insufficiency. OGTT and ACR can identify individuals with subclinical disease requiring a more aggressive treatment of risk factors and more intensive therapy.
P617
Depression and cardiovascular disease in the diabetic patient: probably more than just a fling
SL Mosteoru1, G Mut-Vitcu2, R Timar2, S Mancas1, D Gaita1
1University of Medicine Victor Babes, Cardiology, Timisoara, Romania
2University of Medicine Victor Babes, Diabetes, Nutrition and Metabolic disorders Department, Timisoara, Romania
Recent studies have brought to light that people with diabetes mellitus (DM) have twice the risk compared to the general population of developing long-term symptoms of depression, which represents a risk factor for coronary heart disease. We have designed a study aimed at uncovering if depressed diabetic patients have a higher incidence of cardiovascular complications and have also evaluated the relationship between the presence of depression and glycemic control in patients suffering from diabetes mellitus. We have conducted a cross-sectional study on 1346 patients suffering from DM admitted to the Diabetes Department of the Emergency County Hospital between January and December 2012. All relevant information was extracted from patient charts: demographic data, DM type and duration, DM treatment, weight status, HbA1c, presence of cardiovascular complications. Out of the 1346 patients included in our study 54% were males. 8.5 % of the entire population has been also diagnosed with depression. Depression was found in 7.9% of patients with type 1 DM, while the prevalence of depression was 8.6% in the type 2 DM category. There was statistical significance between diabetes mellitus and depression (p < 0.05). The mean value of HbA1c was 9.2% in patients suffering from both DM and depression and 8.9% in diabetic patients only. Patients with DM and depression were able to achieve the < 8% HbA1c target in 29.31% of the cases, while those without depression in 32.59% of the cases. Our conclusions highlight the need for active screening for depression in diabetic patients due to the potential of this complication being overlooked and also in order to ensure that preventive action is taken. Further research is necessary to disentangle causal relationships among depression, diabetes complications, cardiovascular disease and mortality.
P620
Prevalence of unknown polyvascular arterial disease in patients with coronary artery disease and its impact on the major adverse events
S Kostic1, I Tasic2, D Djordjevic2, D Lovic3, D Mijalkovic4
1Institute for Therapy & Rehabilitation "Niska Banja", Niska Banja, Nis, Serbia
2University of Nis, Medical Faculty, Nis, Serbia
3Clinic for internal disease InterMedica-dr Lovic, Nis, Serbia
4Clinic for internal disease "Kardiomedika", Nis, Serbia
Topic: Sports cardiology
Purpose:The aim of the study is to evaluate the prevalence of polyvascular arterial disease (carotid and peripheral disease) in patients with coronary artery disease and its impact on the major adverse events.
Methods:The study involved 100 patients with coronary heart disease (mean age 59.7± 10 years, 55% men) who were in a rehabilitation at the Institute. For all patients there was determined: presence of risk factors for cardiovascular disease (hypertension, hyperlipidemia, smoking, diabetes, obesity, age), laboratory analyses, anthropometric measurements, ankle–brachial index (ABI), carotid ultrasound imaging and coronarography. ABI was calculated as the ratio of pressure in the pedal segments of tibial arteries to that in brachial artery. Intraluminal lesions carotid artery were documented using B-mode imaging and defined as carotid intima-media thickness (CIMT) and plaques as focal intimal protuberances.
Results:The average number of risk factors was 2,79±1,03, the most common were hypertension 80.0% and dyslipidaemia 86.0%. The average number of atherosclerosis involved coronary blood vessels was 2.22±0.81. All the patients had atherosclerotic changes, in 46.0% observed in three blood vessels, in 30.0% in two, and in 24.0% in one vessel. The average value of ABI was 1.02±0.21, ranged from 0.71 to 1.50. Patological value ABI was found in 59(59%) patients, 41,0% had reduced ABI values (=0.9), 18.0% higher values (>1.3). The average value of CIMT was 0,98±0,21. Abnormal CIMT values ?128;??128;?were observed in 51% of patients, 71% had one or more carotid plaques with an average stenosis 35,3±20,8%. Carotid stenosis higher than 50 % had 17 % patients. Polyvascular disease (PVD) - the changes in coronary, carotid and peripheral arteries at the same time, was found in 47(47%) participants. There was a significant correlation between the presence of PVD and age, the average number of risk factors and the presence of diabetes. After 4 years, a major adverse cardiac event (MACE) had 13(16.7%) patients; 3(3.8%) patients had cardiac death, 5% myocardial infarction, 5% new PCI and 2,5% stroke. Among patients with polyvascular disease MACE were significantly higher 10 (21%) v.s 3 (5,6%), p=0,02.
Conclusion:Patients with ischaemic heart disease often have multiple arterial disease. Patients with PVD are at higher risk for future cardiovascular events.
P622
Abnormal findings in resting electrocardiograms and their association with hypertension.
A Piwonska1, W Piotrowski1
1Institute of Cardiology, Warsaw, Poland
Topic: Sports cardiology
Purpose:the evaluation of abnormal findings in resting electrocardiograms (ECGs) of hypertensive persons (treated or untreated) compared to healthy persons, and the association between the ecg findings and hypertension status.
Methods:random sample of 2783 men and 2835 women, aged 35-64, examined in the frame of Pol-MONICA study in 1984, 1988, and 1993. Hypertension (HT) was defined as BP = 140/90mmHg or hypotensive treatment. Resting ECGs were coded using Minnesota code. The following ECG categories were created: abnormal Q wale (Q), ST depression (ST), abnormal T wave (T), AV blocks, His bundle branch blocks (HBBB), left ventricle hypertrophy (LVH), arrhythmia (atrial flutter or fibrillation (ARR), and ischemic ECG findings (IEF: Q or ST or T).
Results:HT was found in 1515 (54.4%) men and 1345 (47.4%) women. In hypertensive persons the most often observed ECG finding were HBBBs (10% In both genders), and additionally in men T (4.2%), Q (3.3%) and ST (2.4%), and in women T (5.8%) and ST (3.5%). Abnormal findings were 3-times more often found in hypertensive persons compared to normotensives, except for HBBBs, AV-blocks in both genders, and additionally ARR in men. IEF were significantly more often observed in persons with HT compared to healthy persons (men: 6.9% vs 2.8%, p=0.001; women: 7.9% vs 4.2%, p=0.001). Analyzing 3 groups: persons with treated HT, persons with untreated HT and healthy persons we found the highest percentage of persons with abnormal ECG in the group of persons with treated HT. ST and T in men and T in women occurred significantly and independently of coronary artery disease history and age associated with HT status.
Conclusions:Abnormal ECG findings were observed significantly more often in resting electrocardiograms of hypertensive persons compared to healthy persons, and most often in persons with treated hypertension. Abnormal T wave and ST depression occurred significantly associated with hypertension independently of age and the history of coronary artery disease.
P623
Ethnic differences in self-reported risk profile of stroke survivors in urban suriname
A V Jarbandhan1, S M Baldew1, F S Diemer2, J Q Aartman3, G A Van Montfrans3, G P Oehlers2, L M Brewster3, J R Toelsie4, H E J Veeger5, L Vanhees1
1Catholic University of Leuven, Department of Rehabilitation Sciences, Leuven, Belgium
2Academic Hospital Paramaribo, Department of Cardiology, Paramaribo, Suriname
3Academic Medical Center of Amsterdam, Vascular Medicine, Amsterdam, Netherlands
4Anton de Kom University of Suriname, Physiology, Paramaribo, Suriname
5VU University, Faculty of Human Movement Sciences, Amsterdam, Netherlands
Topic: Sports cardiology
Purpose:Describe ethnic disparities in cardiovascular risk factors among stroke survivors.
Methods:1478 persons aged 18-70 years participated in the HELISUR study. Participants were asked about their history of hypertension, diabetes, smoking, hypercholesterolemia and TIA. Logistic regression explored the association between ethnicity and the prevalence of stroke.
Results:Stroke was reported by 4.1% South Asians, 3.6% Creole, 2.0% Indonesian and 1.8% Maroons. The first exploratory logistic regression analyses showed that South Asians have a significant 2.5 times higher chance of experiencing stroke compared to Maroons. Other comparisons between ethnic groups appeared not to be significant.
Conclusion:Preliminary findings show that significant ethnic disparities may exist in stroke prevalence. Multiple regression analyses should be performed to account for potential confounding effects of CVD risk behavior. Future results should indicate whether targeted secondary prevention will be necessary to decrease differences among South Asian stroke survivors.
Significance level was set at 0.05
Ethnic groups
South Asians (N=544)
Creole (N=388)
Indonesian (N=150)
Maroons (N=396)
Stroke crude prevalence (%) (N)
4.1 % (22)
3.6% (14)
2.0% (3)
1.8% (7)
Age-groups: 30-40 years
2.8
1.2
3.7
2.1
40-50 years
3.6
3.8
2.0
1.6
50-60 years
6.5
10.9
4.3
2.3
60-70 years
11.2
2.4
0
6.2
Gender (M/F) (N)
17/5
8/6
1/2
2/5
Smoking (%)
7.3
6.7
1.8
3.2
Hypertension (%)
6.4
8.6
3.4
7.6
Diabetes mellitus (%)
11
10.8
0
6.2
TIA (%)
25
41.6
100
14.2
Hypercholesterolemia (%)
8.1
6.8
0
0
Logistic regression
Significance
OR
Creole compared to South Asian
0.73
0.89
Indonesian compared to South Asian
0.25
0.49
Maroons compared to South Asian
0.05
0.43
P625
Age gradient of carotid intima-media thickness and plaques and their prospective determinants in women of elder age in a general population
S K Malyutina1, YU Polekhina2, A Ryabikov1, S Shakhmatov1, M Bobak3
1Institute of Internal Medicine SB RAMS, Novosibirsk, Russian Federation
2Novosibirsk State Medical University, Novosibirsk, Russian Federation
3University College London, London, United Kingdom
Objective:Carotid intima-media thickness (CIMT) and atherosclerotic carotid plaques (CP) are proven predictors of cardiovascular outcomes and are strongly associated with aging. The pattern of age gradient of these phenotypes and their determinants are sex- and population specific, have not been well studied in women. In this prospective study, we examined the age gradient and the prospective determinants of the structural characteristics of carotid arteries in older women in a Russian population sample.
Methods:A random population sample of women in Novosibirsk, Russia was examined twice over 8.5 years interval (n=338, aged 45-69 years old at baseline and 52-79 years old at the repeated survey). Cardiovascular risk factors were measured at both occasions. In the second survey, we measured mean-mean CIMT on the far wall of both common carotid arteries and identified CP with high-resolution ultrasound. CP were categorized as absent, single and multiple. Linear regression analysis was applied for analysis of cross-sectional and prospective associations.
Results:The mean value of CIMT was (M±SE) 0,79±0.01mm, the frequency of any CP was of 54%. CIMT increased by 0.06-0.07mm per age decade, the frequency of CP increased from 31% at age 52-59 to 73% at age 70-79. In cross-sectional analysis, CIMT was positively associated with age, systolic blood pressure (SBP) and history of treated diabetes. Prospective predictors of CIMT included age, SBP and menopausal status at baseline. In cross-sectional analysis, CP were positively associated with age, SBP, smoking, history of cardiovascular diseases (CVD) and negatively associated with alcohol intake. Prospective predictors of CP included age, SBP, low-density lipoprotein cholesterol (LDL-C) and smoking at baseline.
Conclusion:In this population sample of women aged 52-79 in Russia, the increment of CIMT comprised 0.06-0.07mm per age decade and the frequency of CP doubled in older age decade in studied age range. Age, SBP and menopausal status at baseline predicted CMIT 8.5 years later, while age, SBP, smoking, and LDL-C at baseline predicted CP. These factors contribute to the age gradient in vascular ageing and carotid wall lesion in elder women in Russian population. The study is sponsored by the the Russian Scientific Foundation (#14-45-00030).
P626
Changes in the etiology of congenital heart disease in the Korean population
SY Jang1, EY Ju2, SR Seo3, JY Choi4, DK Kim4, SW Park4
1Samsung Medical Center, Division of Cardiology, Department of Medicine, Center for Cardiovascular and Stroke Imaging, Seoul, Korea, Republic of
2Seoul National University, Graduate School of Public Health, Seoul, Korea, Republic of
3The National Health Insurance Service, Seoul, Korea, Republic of
4Samsung Medical Center, Division of Cardiology, Department of Medicine, Cardiovascular Imaging Center , Seoul, Korea, Republic of
Objective The aim of this study is to assess changes in the causes of congenital heart diseases between 2006 and 2013 in Korea. Research Design and Methods Data were collected from the National Health Insurance Corporation in Korea from 2006 through 2013. These data consisted of primary diagnoses related to congenital heart disease diagnosed regardless of other conditions. Congenital heart disease included congenital malformations of cardiac chambers and connections (Q20: Q20.0~20.9), congenital malformations of cardiac septa (Q21: Q21.0~21.9), congenital malformations of pulmonary and tricuspid valves (Q22: Q22.0~22.9), congenital malformations of aortic and mitral valves (Q23: Q23.0~23.9), other congenital malformations of heart (Q24: Q24.0~24.9), congenital malformations of great arteries (Q25: Q25.0~25.9), congenital malformations of great veins (Q26: Q26.0~26.9), other congenital malformations of peripheral vascular system (Q27: Q27.0~27.9), and other congenital malformations of circulartory system (Q28: Q28.0~28.9). The age-standardized prevalence of congenital heart diseases was calculated with the direct method using the estimated Korean population in 2010 as the reference. Results For male, the age-standardized cumulative prevalence of Q20, Q21, Q23, Q24, and Q26 in over 65 years was 0.02, 0.05, 0.16, 0.09, and 0.01 per 100,000 persons in 2006 and 0.27, 1.69, 0.79, 1.03, and 0.06 in 2013. For female, the age-standardized cumulative prevalence of Q21, Q22, Q24, and Q26 in over 65 years was 0.09, 0.42, 0.21, 0.004, and 0.01 per 100,000 persons in 2006 and 14.9, 1.08, 1.28, 1.03, and 0.04 in 2013. The age-standardized cumulative prevalence of Q25, Q27, and Q28 did not change dramatically between 2006 and 2013 year in over 65 years.
Conclusions:The overall age-standardized cumulative prevalence of Q20, Q21, Q23, Q24, and Q26 in male and Q21, Q22, Q24, and Q26 in female increased between 2006 and 2013, especially in those older than 65 years. These changes should be considered in future designs of cardiovascular healthcare services in rapidly aging countries.
P629
Role of the waist/height ratio in the cardiometabolic risk assessment, classified according to body mass index
R Rodrigues1, R Palma Dos Reis2, A Pereira1, S Gomes1, AC Sousa1, M Rodrigues1, I Ornelas1, S Borges1, D Pereira1, MI Mendonca1
1Hospital Dr. Nélio Mendon? Research unit, Funchal, Portugal
2New University of Lisbon, Cardiology, Lisbon, Portugal
Background:Body Mass Index (BMI) is widely used to assess the impact of obesity on cardiometabolic risk but it does not always relate to central obesity. The WHtR (waist/height), is a contant anthropometric marker of central adiposity, has been advocated as a superior indicator of cardiometabolic risk.
Methods:Cross-sectional cardiometabolic risk factor variables on 2555 adults (23.6% female and 76.4% male), 30-65 years of age were used. Based on BMI, the population was classified as obese if BMI was>30 (n=1759, 68.8%) and non obese if BMI <30 (n=796, 31.2%). The risk profiles of each group based on the WHtR (<0.6, no central obesity versus = 0.6, central obesity) were compared.
Results:24.9% of the non obese group were centrally obese (WHtR =0.6) and 10.1% among the obese were not (WHtR < 0.6). 32.2% of the non Obese with Central Obesity group had Type 2 Diabetes, as compared to 15.7% of the non Obese without Central Obesity (P<0.0001). 74.7% of the non Obese with Central Obesity had metabolic syndrome as compared to 36.7% of the non Obese without Central Obesity (p < 0.0001). On multivariate analysis the non obese with central adiposity were 1.78, 1.4, and more likely to have significant adverse levels of tryglicerides, glucose and 0.55 less times to have higher HDL, respectively. In the obese group, those without central obesity were 3.49 times likely to have significant adverse levels of HDL cholesterol (p < 0.0001), as compared to those with central obesity.
Conclusion:In our population WHtR was found to further stratify cardiometabolic risk factor levels beyond BMI percentile category alone. It not only detects central obesity and related adverse cardiometabolic risk among non obese population, but also identifies those with predisposition to Glucose metabolism impairment, which has implications for primary care practice.
P630
Heterogeneity of cardiovascular risk factors and disease characteristics and cardiovascular outcomes in patients with rheumatoid arthritis across 10 countries
A G Semb1
1Diakonhjemmet Hospital, Oslo, Norway
Topic: Sports cardiology
Purpose:Patients with rheumatoid arthritis (RA) have an increased risk of cardiovascular disease (CVD). CVD risk scores for the general population do not accurately predict CVD events in RA. Heterogeneity of traditional CV risk factors and RA characteristics across various countries may be associated with varying impacts on CVD events. We aimed to compare the impact of classical CV risk factors and RA characteristics on CVD outcomes in RA patients from 10 countries.
Methods:RA cohorts from 13 rheumatology centers in UK, Norway, Netherlands, US, Sweden, Greece, South Africa, Spain, Canada and Mexico were compared. Data on CV risk factors and RA characteristics were collected at baseline for each cohort; CVD outcomes were collected prospectively using standardized definitions. Cox models with random effects for center were used to compare the impact of CV risk factors and RA characteristics on CVD events. Classical CV risk factor effects were adjusted for age and sex; RA characteristic effects were adjusted for age, sex and CV risk factors.
Results:5685 RA patients without prior CVD were included (mean age: 55 [SD: 14] years, 76% female). During a mean follow-up of 6.1 years (31155 person years), 476 patients developed CVD events. RA duration varied by center: 4 with early RA (<1 year), 7 established (mean 9-13 years) RA and 2 with both. Mean age varied from 37 to 61 years (younger in the early RA cohorts - p<0.001); females varied from 66% to 90% (p<0.001). 2 cohorts consisted of Hispanics, the rest Caucasians. CVD event rates varied across countries with the lowest observed in Norway and UK and the highest in South Africa, Netherlands, US-Mayo and Sweden. Age effects were fairly consistent (hazard ratios [HR] ranged from 1.6-1.8 per 10 year increase in age), but male sex varied from no effect to a doubled effect (HR=1.0-2.3). Varied effects were also seen for current smoking (HR=1.1-2.1), hypertension (HR=0.6-2.0), total cholesterol: high-density lipoprotein ratio (HR=0.9-1.2) and diabetes mellitus (HR=0.7-2.8). Effects were also varied for RA characteristics, including rheumatoid factor and/or anti-citrullinated protein antibody seropositivity (HR=0.7-1.4), disease activity score [DAS28] (HR=0.9-1.2) and RA disease duration (HR=0.7-1.1 per 10 years).
Conclusions:Major heterogeneity exists in CVD event rates and in the effects of classical CV risk factors and RA characteristics on CVD outcomes among patients with RA across different countries. This must be considered in the generation of a CVD risk calculator for RA that will be generalizable to patients in different countries.
P631
Trajectories of traditional risk factors and novel biomarkers before the onset of type 2 diabetes, the Doetinchem Cohort Study
G Hulsegge1, AMW Spijkerman1, HA Smit2, YT Van Der Schouw2, WMM Verschuren1
1National Institute for Public Health and the Environment (RIVM), Bilthoven, Netherlands
2University Medical Center Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, Netherlands
Topic: Sports cardiology
Purpose:To examine whether trajectories of risk factors and biomarkers differ for those who develop type 2 diabetes and controls over a follow-up of 15-to-20 years.
Methods:A total of 350 incident type 2 diabetes cases (self-reported and/or random glucose =11.1 mmol/L) were identified between 1987 and 2012 in a prospective population-based cohort of 7,768 adults aged 20-59 years at baseline. At the wave that type 2 diabetes was ascertained for cases and the same wave for age- and sex-matched controls, retrospective trajectories were analysed using generalized estimating equations.
Results:In general, 15-20 years before case ascertainment levels of risk factors and biomarkers were similar for those with type 2 diabetes and controls. However, trajectories in HDL-cholesterol, triglycerides, body mass index, waist circumference, random glucose, alanine aminotransferase, gamma glutamyltransferase, uric acid and C-reactive protein were significantly worse for those with type 2 diabetes (P-value for interaction<0.10). For example, compared to controls, increases in body mass index were 3 times larger for men and 4 times larger for women with type 2 diabetes (Figure 1). In contrast, trajectories in blood pressure, total cholesterol, albumin and estimated glomerular filtration rate were similar. Differences between men and women were small, but differences in trajectories of alanine aminotransferase and gamma glutamyltransferase were somewhat larger in men, while differences in triglycerides and uric acid were larger in women.
Conclusions:Our results add knowledge about the pathophysiological changes that lead to the development of type 2 diabetes. Unfavourable changes in risk factors and biomarkers occured among all adults but were much larger in those with incident type 2 diabetes.
Figure 1
P632
Ethnic differences in arterial stiffness - the HELIUS study
MB Snijder1, K Stronks1, CO Agyemang1, WB Busschers1, RJ Peters2, BJ Van Den Born3
1Academic Medical Center of Amsterdam, Department of Public Health, Amsterdam, Netherlands
2Academic Medical Center of Amsterdam, Department of Cardiology, Amsterdam, Netherlands
3Academic Medical Center of Amsterdam, Department of Internal and Vascular Medicine, Amsterdam, Netherlands
Topic: Sports cardiology
Purpose:Well-known ethnic differences in cardiovascular risk exist, which may be explained by ethnic differences in arterial stiffness. Our aim was to assess ethnic differences in arterial stiffness, and to explore whether these differences are acquired during life by studying whether they are accounted for by conventional cardiovascular risk factors and whether they increase with age.
Methods:Data of 1535 Dutch, 1368 South-Asian Surinamese, 1584 African Surinamese, and 1203 Ghanaian participants of the HELIUS study (aged 18-70 years) were used. Arterial stiffness was assessed by duplicate pulse wave velocity (PWV) measurements using the Arteriograph system.
Results:Linear regression showed that South-Asian Surinamese had higher PWVs as compared with Dutch (age-adjusted mean difference (95% CI) was 0.55 (0.38-0.72) m/s in men and 0.77 (0.56-0.98) m/s in women). These differences were largely, but not completely, explained by conventional risk factors (MAP, HT, diabetes, BMI, WHR, total cholesterol, HDL, smoking). Furthermore, these ethnic differences were not found at young age (<35 years). African Surinamese and Ghanaians had higher PWVs as compared with Dutch across the entire age range (ranging from 0.19 (0.01-0.37) m/s in African Surinamese men to 1.13 (0.92-1.34) m/s in Ghanaian women), but these differences disappeared after adjustment for risk factors (except in Ghanaian women).
Conclusion:PWV levels paralleled the well-known ethnic differences in cardiovascular risk. Our results support the hypothesis that higher PWV in South-Asian and African ethnic groups are acquired during life due to higher exposure to cardiovascular risk factors.
P633
Association between hepatic steatosis, serum transaminases and risk for atrial fibrillation
MRP Markus1, PJ Meffert2, W Lieb3, M Koch3, SE Baumeister2, SB Felix4, M Doerr4, G Targher5, H Voelzke2
1University Medicine of Greifswald, DZHK (German Centre for Cardiovascular Research), Greifswald, Germany
2University Medicine of Greifswald, Institute for Community Medicine, Greifswald, Germany
3Christian-Albrechts-University Kiel, Institute of Epidemiology, Kiel, Germany
4University Medicine of Greifswald, Department of Internal Medicine B, Greifswald, Germany
5University of Verona, Department of Medicine, Verona, Italy
Topic: Sports cardiology
Purpose:Atrial fibrillation (AF) is a common heart rhythm abnormality that affects up to 2% of the general adult. On the other hand, unfavorable lifestyle behaviors such as the increase in sedentary lifestyles, and high caloric food intake are accompanied by the increase in the prevalence of obesity, dysglycemia, diabetes and hepatic steatosis (HS). HS is the most common cause of elevated serum transaminase levels and is now regarded as a pathogenic component of the metabolic syndrome. The aim of our large population-based study was to examine the associations of ultrasonographically determined HS and elevated serum transaminases with the risk of prevalent AF.
Methods:Cross-sectional data of 3,039 men and women, aged 20-81 years, from the population-based Study of Health in Pomerania (SHIP-0) was used. HS was defined as the presence of a hyper-echogenic ultrasound pattern of the liver. Three liver transaminases were measured photometrically: alanine transaminase (ALT), aspartate transaminase (AST) and gamma-glutamyl-transaminase (GGT). Presence of AF was ascertained by resting electrocardiograms.
Results:AF was present in 46 individuals (1.51% of the whole cohort). After adjustment for age, sex, height and weight, individuals with HS had no significant higher risk for prevalent AF when compared with those without HS (odds ratio [OR] = 1.27; 95% confidence interval [CI], 0.63 to 2.57; p=0.510). In contrast, the risk for prevalent AF increased with higher transaminases levels. The adjusted (for age, sex, height and weight) -ORs for prevalent AF, per 1-SD increase in each serum transaminase, were 1.50 (95% CI: 1.14 to 1.97; p=0.003) for ALT, 1.41 (95% CI: 1.15 to 1.73; p=0.001) for AST and 1.38 (95% CI: 1.21 to 1.57; p<0.001) for GGT, respectively. Sensitivity analyses with additional adjustments for ejection fraction, myocardial infarction, valvular heart disease, left ventricular hypertrophy, alcohol consumption, systolic blood pressure, Hb1ac and use of antihypertensive and antidiabetic medication did not change the overall results.
Conclusions:Our results indicate that, in a general population, increased serum transaminase levels are significantly associated with a higher risk of prevalent AF, while the ultrasonographic diagnosis of HS is not. A possible explanation for these findings is that the adverse effects of increased levels of inflammatory mediators released by a steatotic and inflamed liver (NASH, which is typically characterized by increased serum transaminase levels) are more important for the association with AF than the simple presence of fat inside the liver.
P634
Low efficiency of current guidelines: low diagnostic performance of non-invasive ischemia testing in patient with intermediate pretest probability
P Rio1, T Pereira-Da-Silva1, R Ramos1, C Barbosa1, M Afonso Nogueira1, P Pinto-Teixeira1, A Viveiros Monteiro1, A Fiarresga1, D Cacela1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Background:Non-invasive ischemia testing (NIST) is recommended in symptomatic patients with intermediate pretest probability (IPP) of obstructive coronary artery disease (OCAD) for triage for invasive cardiac catheterization (ICA). Purpose: We sought to determine the predictors of CAD in a contemporary sample of patients with intermediate pretest probability and assessed the incremental diagnostic value of NIST. Methods:Among patients referred for elective ICA in a single tertiary-care center (2006 -2011), those with an IPP were retrospectively identified. To understand the relative value of the factors in predicting OCAD, a model of stepwise logistic regression analysis was performed starting with Framingham risk score (FRS), symptomatic status, left ventricular (LV) function and finally the NIST results by this specific order. The discriminatory power of this model was assessed by the area under de ROC curve (AUC). Results:From a total of 2600 patients, 525 were included: 61.6 ±10.2 years, 61.7% female, 20% diabetics, mean 10-year Framingham risk 14.4%, 20.6% typical angina and 7% of LV dysfunction. NIST was performed in 82.5% (56% treadmill exercise ECG, 38.3% SPECT). At ICA only 105 patients (20%) had obstructive CAD. Independent predictors of OCAD included male gender (OR 3.49; 95% CI, 1.36-9.93), presence of typical angina (OR 37.59; 95% CI, 12.59-112.27), smoking (OR 3.83; 95% CI, 1.42-10.32), and LV dysfunction (OR 6.78; 95% CI, 2.35-19.58), (all p<0.01). Stepwise analysis shown in the figure. Conclusions:A low proportion of patients with IPP were found to have OCAD. The incorporation of NIST in the previous models had no significant effect over the clinical evaluation. To increase the predictability of CAD in this population another tests are needed.
Predictability of CAD
P635
Peak VO2 and physical health predict survival after heart transplantation
M Yardley1, O E Havik2, I Grov1, A Relbo1, L Gullestad1, K Nytroen1
1Oslo University Hospital, Department of Cardiology, Rikshospitalet, Oslo, Norway
2University of Bergen, Department of Clinical Psychology, Bergen, Norway
Topic: Sports cardiology
Purpose:Does physical capacity predict survival in heart transplant (HTx) recipients? Method:This retrospective study investigated two different HTx populations regarding predictors for long-term survival. Cohort1 includes patients who completed a VO2peak test during their annual follow-up between 1990 and 2003. Cohort2 includes patients who completed a SF-36 v1 questionnaire between 1998 and 2000. Background information and other central variables were collected from our center's HTx database. Results:Cohort1; N=132, Mean age: 51(12) years, Men: 92%, Median time after HTx: 2(4) years, Mean VO2peak: 19,9(5,3) ml/kg/min, Mean years under observation: 15(6). Cohort2; N=133, Mean age: 54(11) years, Men: 78%, Median time after HTx: 5(6) years, SF-36 Median Physical Component Sumscore (PCS): 90 (30), Mean years under observation: 15(5). Predictive variables were analysed using cox regression (enter method) based on p-values<0.2 from univariate regression and clinical aspects. The two best predictive models (adjusted for gender) were: Cohort1; Age (p=0.005), VO2peak (p=0.016), Ischemic time (p=0.021) and Cardiac Output (p=0.052). Cohort2: Age (p<0.001), years after HTx (p<0.001), PCS (p=0.003), Smoking (p=0.003), and cardiovascular disease (p=0.079). Other univariate significant predictors that did not reach statistical significance in multivariate regression were: Etiology of HTx, donor age, BMI, ejection fraction, blood pressure, creatinine, Hgb and SF-36 Mental Component Sumscore. Kaplan-Meier analysis showed that groups divided by median VO2peak and PCS had significantly different survival-time.
Conclusion:VO2peak level and self-reported physical health are both strong predictors for survival in HTx recipients. VO2peak is a crucial measurement, and should be more frequently used after HTx.
Survival-time divided by groups
P637
Effects of physical exercise and regular training in renal transplantation
L Stefani1, GM Mascherini1, CP Pedri1, LF Francini1, MG Gianassi1, IC Corsani1, AP Pacini1, EM Minetti1, GG Galanti1
1University of Florence, Florence, Italy
Topic: Sports cardiology
Purpose:Regular physical exercise contrasts metabolic syndrome. The study aims to assess the effects after 6 months of individualized moderate exercise training program,in renal solid organ recipients.
Methods:14 renal transplant recipients were submitted to Cardiopulmonary Test, echocardiographic exam, ca skin fold, bioimpedance analysis and test of strength for the lower anf higher limbs .Exercises consisted in 30 minutes of aerobic training , 3 times a week, and 2 sets of 20 repetitions at 35% of the maximum load for each. Results:EF is significantly enhanced. The anaerobic threshold improved . Skin folds were significantly reduced at pectoral level. Conclusion:A short period of mixed aerobic and resistance exercise , improves cardiovascular performance and reduces risks factors linked to the visceral fat. Any other effects on other will need of a longer follow - up .
T 0
T6
p value
Age
51.6±6.2
Time from transplant (yrs)
6.2±6.1
Anthropometrics
Weight (Kg)
69.8±12.2
69.2±12.8
NS
BMI (kg/m2)
23.4±3.5
23.2±3.5
NS
Skin fold
Pectoral (mm)
13.3±7.1
6.4±3.8
<0.01
Abdomen (mm)
16.0±9.4
12.4±8.6
< 0.05
Body Composition
Fat Mass (%)
15.1±6.8
12.4±5.5
< 0.05
Fat Mass (kg)
10.1±4.9
8.4±4.5
< 0.05
Aerobic Threshold
VO2(mlO2/kg/min)
11.1±7.9
10.5±6.1
NS
Anaerobic Threshold
VO2(mlO2/kg/min)
14.5±6.9
19.2±10.0
<0.05
P640
Severe blood pressure spikes during 24hr ambulatory blood pressure monitoring, more common than we think?
P Ting1, LH Wong2
1National Heart Centre, Singapore, Singapore
2University College Cork, Cork, Ireland
Topic: Sports cardiology
Purpose:Ambulatory blood pressure measurement (ABPM) is becoming increasingly important in the management of hypertension. Apart from the average BP, BP variability and exaggerated morning surges have been shown to be independent predictors of cardiovascular risk. While modest increase in morning waking BP is believed to be physiological, less is known about BP spikes that may occur during other parts of the day. We describe the frequency and characteristics of extreme blood pressure spikes during 24 hour ABPM at our Institution.
Methods:We conducted a retrospective analysis of 220 subjects who had 24 hour ABPM performed within a 5 month period in 2013 at a single hospital for suspected or known hypertension. Severe spikes in BP were defined as SBP=180mmHg or DBP=110mmHg or an increase in the BP =30mmHg above the day or night time average. Subjects with one or more severe spikes in BP were labeled as "Spikers", and those without "Non-spikers". Both groups were compared, and the characteristics of the spikes analysed.
Results:"Spikers" made up 54.5% (120) of the total subjects and on average had 5.3 spikes each. Age, BMI, gender and ethnicity were not significantly different between groups. "Spikers" tended to have higher average systolic (142 vs. 131mmHg, p<0.01) and diastolic pressures (85 vs. 78mmHg, p<0.01), and systolic variability (SD 14 vs. 11mmHg, p<0.01). Of the 80 subjects with normal average systolic blood pressure (<135/85mmHg), 38.8% (31) were "Spikers". Nocturnal dipping status was not significantly different between the two groups. Spikes were not restricted to the mornings, but occurred throughout the day, even at night. Spikes also often did not occur with concomitant rises in heart rate. Conclusions:In our study cohort, severe spikes in blood pressure were common and not limited to just morning surges. Poorer average BP control and greater variability were associated with more spikes, however it is important to note that significant spikes can also occur with normal or mildly elevated average BP. The pathophysiologic mechanism and clinical significance of frequent severe blood pressure spikes needs to be further studied.
P642
Correlation of sugar sweetened beverage consumption with cardiovascular risk factors in Mexican adolescents
M A Gomez Martinez1, VCA Vergara Castaneda2, CML Castillo Martinez1, MVM Martinez Valdivia2
1National Institute of Medical Sciences and Nutrition Salvador Zubiran, Mexico City, Mexico
2University La Salle, Mexico City, Mexico
Background:Mexico has positioned itself as the largest consumer of soft drinks , registering an increase of 12 % between 2000 and 2009. Beverages intake represents a large share of total energy consumption.It has been proposed that the consumption of sweetened beverages is associated with increased prevalence of overweight and obesity as well as other cardiovascular risk factors, including hypertension.
Objective:To determine the relationship between the consumption of sugar sweetened beverages with cardiovascular risk indicators in a community of adolescents in Mexico City.
Material and methods:A cross sectional study including adolescents aged 11-16 years was conducted in Mexico City; anthropometric measurements (weight, height, and waist circumference) were taken as well as blood pressure according to AHA recommendations and a 24h recall was obtained. Body mass index and Waist to Height Ratio were calculated. T student test and Spearman correlations were performed.
Results:242 adolescents were evaluated, the average aged was 12 ± 1.9 y, 50.4% of population were boys. 45% of sample presented a higher value for WtHR and 27% was classified with abdominal obesity according to waist circumference, without differences between gender. Mean systolic blood pressure was higher in boys compared with girls (103.11.4 ± 11.4 vs 99.8± 10.5; p<0.05), meanwhile no differences were found in diastolic blood pressure. Also, higher prevalence of hypertension was observed in men than women (13.9 vs 11.7 % ; p < 0.05). Excessive consumption of sugars was recorded with a value of 5 ± 5.8 servings a day, being higher in males ( 5.6 ± 6.8 servings per day ) compared to women ( 4.4 ± 4.4 servings per day) and from these , soft drinks and juices are consumed by an average of 2.39 ± 4.5 and 1.29 ± 2.3 servings per day, respectively. No relations to BMI to weight, BMI and sugar sweetened drinks were found.A good correlation between the consumption of soft drinks and juices with waist circumference (r = 0.523 was found ; r = 0.463 ; p < 0.001 , respectively) and a high correlation between soft drink and juices consumption and systolic blood pressure (r = 0.985 p < 0.001; r = 0.987 ; p < 0.001, respectively). Meanwhile the correlations for diastolic blood pressure and soft drinks and juices intake were r=0.987 and r=0.613, both with a p<0.001.
Conclusions:The prevalence of cardiovascular risk factors are higher than the reported in the national surveys in this target population. The soda consumption and juice is associated with SBP and DBP. In relation of SBP it was associated with sex and weight.
P644
Alimentary fats and hypertension in a urban high school adolescents in Mexico City
M A Gomez Martinez1, CML Castillo Martinez1, VCA Vergara Castaneda2
1National Institute of Medical Sciences and Nutrition Salvador Zubiran, Mexico City, Mexico
2University La Salle, Mexico City, Mexico
Background:The different types of consumed fatty acids in diet; saturated and the index n6/n3 can be related in the development of SBP and DBP, respectively. On the other hand the systemic hypertension has been associated with anthropometric parameters, like waits to height ratio. Previous studies only a few has report the indexn6/n3 associated with hypertension in this particular age but no in adolescence.
Objective:To examine the relation between saturated fats, the index of fatty acids omega 6 and omega 3 with hypertension diagnosis among high school adolescents.
Methodology:247 adolescents were evaluated on a cross sectional study, in public high school of low socioeconomic status in México City. BP was measured according to the TASK FORCE and National Health and Examination Survey from United States. A 24-hour intake recall was obtained. Subjects were classified in high saturated fat intake group (HIG) if >10% of the total energy intake and the recommended intake group (RIG) <10% of the total energy intake, also the Reason n6/n3 with more of recommended consumption > 4:1. Also the anthropometric measures were performed: weight, height, waist circumference according toãÎ..and waist–to-height ratio (WtHR) was calculated.
Results:Mean age was 11±.5years, the prevalence of diastolic hypertension is 65.8% and systolic hypertension is 21%, for other hand the systolic blood pressure (SBP) was 120 ± 20.5 mmHg blood pressure (DBP) 80 ±15 mmHg. The 70% belonged to HIG group and 29% of the RIG group for saturated fats. When these groups were compared prevalence of systolic hypertension was 1% in RIG group vs 4.6% HIG (p=0.030), in diastolic blood pressure the values was 60 vs 65 mmHg in a HIG and RIG total fats (p= 0.048). Also the index n6/n3 it was 10/1 in our study when in the literature report 4/1, we compare this index between the hypertensive diastolic vs normotensive subjects (p=0.034).
Conclusion:Prevalence of hypertension among high school adolescents is higher than reported in Mexican surveys as well as a high fat diet intake. The systolic hypertension was associated with saturated fats, in another hand the diastolic hypertension was associated with index n6/n3.
P645
Hypertension, and awareness and treatment of hypertension in Europe. Results from the EHES Pilot Project
HK Tolonen1, S Giampaoli2, K Kuulasmaa1, JS Mindell3, S Mannisto1, CM Dias4, P Koponen1
1National Institute for Health and Welfare (THL), Helsinki, Finland
2Superior Institute of Health, Rome, Italy
3University College London, London, United Kingdom
4National Health Institute Doutor Ricardo Jorge, IP, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Prevalence of raised blood pressure has been defined as one of the target indicators for the World Health Organization Global Action Plan for the prevention and control of non-communicable diseases. Therefore, it is important to be able to monitor changes in population level hypertension prevalence, as well as changes in awareness and treatment of hypertension. We assessed the prevalence, and awareness and treatment of hypertension using standardized methods in defined adult populations in 12 European countries.
Methods:The European Health Examination (EHES) Pilot Project was conducted in 2009-2012(the Czech Republic, Finland, Germany, Greece, Italy, Malta, the Netherlands, Norway, Poland, Portugal, Slovakia and UK/England planned and prepared for their national health examination survey (HES) and conducted a fieldwork pilot survey among adults aged 25-64 years in at least 1-2 towns/regions. Standardized measurement protocol and questionnaire were used to obtain information on blood pressure, hypertension treatment and awareness of hypertension.
Results:The prevalence of hypertension was on average 33% among men and 23% among women. Among hypertensives, 51% of men and 70% of women were aware of their condition, and 31% of men and 40% of women were on drug treatment. Of those on treatment, 59% of men and 61% of women had their blood pressure under control. There was large variation in prevalence of hypertension, and awareness and treatment of hypertension between surveys.
Conclusions:Our pilot findings indicate that there is still a need for improvement in prevention and primary care, to better meet the needs for detection, monitoring and control of hypertension at the population level. Nationally representative data from European countries are needed to monitor hypertension status and to allow better evaluation of possible effects of national health care systems and treatment guidelines on observed differences between surveys.
P646
Relation between the severity of the obstructive sleep apnea and serum copeptin levels in prehypertensive patients
C Dursun Akkoyun1, A Akyuz1, R Alp1
1Namik Kemal University Faculty of Medicine, Tekirdag, Turkey
Topic: Sports cardiology
Purpose:We sought to evaluate the serum copeptin levels in newly diagnosed prehypertensive patient with obstructive sleep apnea syndrome (OSAS).
Methods:Eighty-four prehypertensive patients were evaluated with polysomnography and divided in to two as OSAS (n=41) and control (n=43) groups. Serum copeptin levels were measured with ELISA method.
Results:Lowest SpO2 was 77±8% in OSAS group and 90±5% in the control group (p<0.001). Mean apnea hypopnea index (AHI) was 26.8 (6-102) in OSAS group and 2 (1-4) in the control group (p<0.001). Copeptin levels were significantly higher in OSAS group compared to control group (146 (93-739) pg/ml vs. 111 (33-253) pg/ml, respectively, p<0.001). Regression analysis have revealed that AHI and lowest SpO2 were related to serum copeptin levels (unstandardized ? 1.02±0.40, p=0.014 and unstandardized ? -3.1± 0.9, p=0.048 respectively).
Conclusion:According to results of our study serum copeptin levels are higher in prehypertensive patients with OSAS compared to control group. Therefore in the assessement of the severity of OSAS, serum copeptin level can be used as a biochemical marker in addition to polysomnographic findings.
Is there an improvement in the degree of control of patients with chronic ischemic heart disease in the last 5 years? Statin use in the BARIHD study
O Ferreiro Uriz1, E Rodriguez Moldes1, JL Gomez Vazquez1, MJ Vazquez Lopez1, E Outeirino Lopez1, A Castro Cives1, T Vazquez Rodriguez1, R C Vidal Perez1, F Otero-Ravina1, JR Gonzalez-Juanatey1
1University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
Topic: Sports cardiology
Purpose:In the chronic phase of coronary artery disease (CAD) it is not clear whether the degree of control of risk factors has shifted in recent years by the influence of changes in clinical practice guidelines and the best use of drug resources in particular statins. We evaluated whether there has been an improvement in these aspects for the long term in a cohort with chronic ischemic heart disease (CIHD) followed by primary care physicians (PCP).
Methods:BARIHD was a cross-sectional multicentric study made with the collaboration of 73 PCP. The PCP included during February 2007,patients(p) that fulfil the inclusion criteria: coronary artery disease (CAD) with at least 1 year of follow up since diagnosis, diagnosis clear established (stable angina-SA, unstable angina-UA or myocardial infarction-MI) in a discharge summary from cardiology department. Follow-up was done by clinical review and we applied as control criteria the ESC guidelines of Stable Coronary Artery Disease. We compared the current situation with 5 years ago when the cohort started.
Results:1038p were included, the differences in the degree of control achieved by cohort are shown in the table. The only difference was found in the LDL-Cholesterol parameter. The use of lipid-lowering drugs was 88.9% in 2007 and 85,2% in 2013 % (p=0.016). In 2013 we found no statin use in 172p (16.6%), and the reasons were good control (47.1%), myopathy (1.7%), intolerance (6.4%) and other causes (44.8%).
Conclusions:There is still room for improvement in all control parameters. We found a significant improvement in LDL control, despite a striking percentage of patients not receiving statins with a CIHD.
NS: No significant
2007 (%)
2013 (%)
p-Value
Blood pressure control
61,7
65,5
NS
LDL-Cholesterol <70 mg/dl
8,4
20,8
<0,001
Triglycerides <200 mg/dl
88,9
88,4
NS
HDL Cholesterol >40 mg/dl ?153; or >45 mg/dl ?153;?
63,2
61,8
NS
Absence of obesity
60,0
59,7
NS
Active smoking
10,7
7,3
NS
P649
The relationship between the achievement of the target values of lipids and observance of healthy lifestyle in patients with moderate cardiovascular risk
V S Gurevich1, SA Urazgildeeva1, MV Musalevskaya2, AA Temirov3, AV Tregubov4
1Saint-Petersburg state university, Saint-Petersburg, Russian Federation
2North-west state medical university, Saint-Petersburg, Russian Federation
3Almazov's Federal Center of Heart, Blood and Endocrinology, Saint-Petersburg, Russian Federation
4Saint-Petersburg State University, Medical Faculty, Saint-Petersburg, Russian Federation
Purpose of this study was to investigate the effect of adherence to physical exercise and dieting on the effectiveness of lipid-lowering therapy in patients with moderate cardiovascular risk.
Methods:The case record forms of 1023 out-patients with initially elevated lipid levels were analyzed. Evaluation of cardiovascular risk was performed with usage of SCORE tables at first visit and after 1 year of follow up. Adherence to lipid-lowering therapy and achieving the target values ?128;??128;?were estimated based on the records in the outpatient charts. Also a selective survey of out-patients during annual visit was performed.
Results:Only 35% of patients at the initial examination were aware of their level of lipids. It has been found that the recommendations to correct diet received about 95 % of all patients of moderate cardiovascular risk on SCORE scale and 25% of them were recommended statins. Only half of patients on lipid-lowering therapy advised physical activity. Physical exercise along with diet and lipid-lowering therapy was prescribed by doctors for 78 % of men and 32% of women. At the same time it was found in a selective survey of out-patients that the compliance with the newly prescribed physical activity demonstrated 62% of women and only 27% of men. Adherence to medication as well as the achievement of lipid level targets was positively correlated with compliance for physical activity (r = 0.480) and diet (r = 0.330). Interruption of statin treatment occurred in 9 % of cases and was not associated with exercise intolerance.
Conclusions:The recommendations for physical exercise were less common than those for diet in patients of moderate cardiovascular risk. Adherence to diet and exercise in these patients was associated with effective lipid-lowering therapy
P650
Association of lone severe primary hypertriglyseridemia with syndrome X and its effect on angiographic myocardial perfusion in presence of normal coronary arteries
O Beton1, H Kaya2, E Saricam3, H Yucel2, A Zorlu2, HE Pamukcu1, LD Asarcikli1, Z Kucuksu4, MB Yilmaz2
1Diskapi Yildirim Beyazit Education and Research Hospital, Ankara, Turkey
2Cumhuriyet University, Cardiology, Sivas, Turkey
3Cag Hospital, Cardiology, Ankara, Turkey
4Mengucek Gazi Training and Research Hospital, Erzincan, Turkey
Topic: Sports cardiology
Purpose:Hypertriglyceridemia has been considered as a risk factor for cardiovascular diseases(CVD). However, triglyceride levels are influenced by many clinical and lipid risk factors. When triglyceride levels are adjusted by these variables, its effect as a risk factor becomes minimal or negligible. Therefore, its association with CVD is uncertain. Myocardial blush grade (MBG) has been developed as a simple angiographic parameter to describe the effectiveness of microvascular perfusion. Aim of our study is to evaluate the possible relationship of lone severe primary hypertrigliseridemia(LSPH) with syndrome X and its effect on MBG in the presence of normal coronary arteries.
Methods:Total of 1795 consecutive patients who had fasting blood triglyseride level of =500mg/dl were included in our study. Patients scheduled to undergo coronary angiography(CAG) were included in the study. Exclusion criterias were previous MI, HF, coronary artery ectasia, DM, hypertension, valvular heart disease, cardiomyopathy, conduction disturbances, impaired renal or liver function, presence of secondary casuses of hypertriglyceridemia, impaired blood glucose and BMI>30 kg/m2. In all patients, extracardiac causes of chest pain, including musculoskeletal and esophageal causes, were ruled out. The diagnosis of syndrome X was based on the presence of typical exercise induced angina pectoris, transient ischemic ST-segment depression (>1 mm) during exercise, and angiographically normal coronary arteries in the absence of left ventricular hypertrophy and systemic hypertension. Patients with hypertriglyseridemia divided into 2 groups, patients with syndrome X (group 1) and patients without syndrome X (group 2). Control subjects who had normal lipid profile and normal coronary arteries were included in the study (group 3). Indication for CAG in group 2 and 3 was typical chest pain. Treadmill exercise ECG was negative in group 2 and 3.
Results:Fifty two, 42 and 45 patiens were included in group1, group 2 and group 3, respectively. Mean age and gender ratio were similar in three groups. Mean triglyseride, LDL and HDL levels were 590.4±144.4, 96.6±37.7, 35.0±11.8 in patients with hypertriglyseridemia and these levels were similar in group 1 and 2. Total MBG score of coronary arteries were 7.9±0.5, 8.2±0.6 and 8.8±0.4 in group 1, group 2 and group 3, respectively (p<0,001).
Conclusion:It was shown for the first time that LSPH has association with syndrome X. LSPH causes imparement in angiographic myocardial perfusion which could explaned by endothelial dysfunction. LSPH should be taken into account as CAD when planning medication.
P651
The association of EPA AA ratio with subclinical atherosclerosis in different generations without DM Multi-slice CT study
Y Suzuki1, S Murase1, O Matsuda1, A Murata1, M Ehara1, T Ito1
1Nagoya Heart Center, Nagoya, Japan
Objective:Eicosapentaenoic acid (EPA) of the omega-3 polyunsaturated fatty acids (?#137;-3 PUFA) family plays important roles in the prevention of cardiovascular disease (CVD), while, arachidonic acid (AA) of the ?#137;-6 PUFA family promotes inflammatory and prothrombotic influences. However, there have been few reports investigating the relationship between plasma EPA/AA ratio and the prevalence of coronary atherosclerosis in multi-slice CT (MSCT) study. The aim of this study was to investigate the association between the plasma EPA/AA ratio and the prevalence of subclinical atherosclerosis in different generations without DM.
Methods:This study consisted of consecutive 230 suspected coronary artery disease (CAD) patients from 40's- to 70's-year-old underwent 128-MSCT. They all were non-DM patients without any lipid-lowering intervention. To examine the plasma fatty acid level, blood samples were obtained. We investigated the prevalence of coronary plaque based on MSCT findings and patients were divided into different generations (40's; N=31, 50's; N=48, 60's; N=72, 70's; N=79). We investigated the association between the plasma EPA/AA ratio and the prevalence of subclinical coronary atherosclerosis.
Results:The results are shown in the table. The plasma EPA/AA ratio was significantly higher in the older generation. In all generations except 70's, the plasma EPA/AA ratio was significantly lower in the patients with coronary artery plaque. The ROC analysis showed the cut-off value of the plasma EPA/AA ratio, sensitivity, and specificity as shown in the table.
Conclusions:In non-DM young patients with suspected CAD, the low plasma EPA/AA ratio was significantly associated with a high prevalence of subclinical coronary atherosclerosis.
Table
P653
Effect of low doses of long chain n-3 PUFA intake on daytime heart rate variability: results from the MARINA study.
AM Pinto1, WL Hall1, TAB Sanders1
1King's College London, Diabetes & Nutritional Sciences, London, United Kingdom
Topic: Sports cardiology
Purpose:Heart rate variability (HRV), a term that refers to a range of parameters that reflect the variability in the length of the interbeat interval (IBI), is regarded as an indirect measure of cardiac autonomic function, and it may be influenced by long-chain n-3 polyunsaturated fatty acids (n-3 PUFA): eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Low HRV indicates reduced functional regulation of heart rate (HR) by the autonomic nervous system and is a powerful predictor of sudden cardiac death. This study tested the hypothesis that supplementation with low doses of n-3 PUFA equivalent to consuming 1, 2 or 4 portions of oily fish per week increases daytime HRV in non-smoking healthy men and women (aged 45-70y).
Methods:The MARINA study (ISRCTN66664610) was a parallel design, randomised controlled trial that compared the intake of 0.45, 0.9 and 1.8g/d of encapsulated EPA + DHA-rich triacylglycerols with matched placebo capsules containing an oleic acid-rich triacylglycerol consumed for 1y. Actiheart monitors (CamNtech Ltd, Cambridge, UK) were fitted following a clinic visit and heart rate IBI were recorded over 24h following a 1 month run-in on placebo and at 6 and 12 months following randomisation to treatment. Data was processed from day-time and night-time periods separately using Actiheart 4 (v.4.0.91) and Kubios HRV software (v.2.1). Complete data on the HRV parameters (frequency domain, time domain and non-linear) were available for 214 participants (89 men, 125 women). Nocturnal (sleep-time) data has been reported previously; here we report the results of the daytime data analysis. The following HRV parameters are reported: SDNN, estimates of overall variability; high frequency (HF) power, a short-term component of HRV reflecting vagal modulation; and SDANN and very low frequency (VLF) power, indicating longer-phase variability.
Results:No significant treatment effects were found for the different components of daytime HRV and there was a large variation in the data, in contrast to the night-time data showing statistically significant increases in longer-phase components of HRV (SDANN, VLF and Ti) following n-3 PUFA supplementation compared to placebo.
Conclusions:Daytime data was collected from subjects under ambulatory conditions and subject to the influence of a number of external stimuli that are difficult to control, unlike night-time data where external stimuli is reduced. If we are to detect subtle dietary effects on HRV we need to control the degree and number of external stimuli. These results have important implications for the design of future studies.
P654
Changes in fat intake in adult Warsaw population in the 28 year period
A Waskiewicz1, A Aranowska1, D Szczesniewska1
1National Institute of Cardiology, Warsaw, Poland
Topic: Sports cardiology
Purpose:Studies results indicate a relationship between the intake and type of dietary fats and the occurrence of cardiovascular diseases. Evaluation of changes in fat intake and fat sources in the diet consumed by an adult Warsaw residents in 1984-2012 years.
Methods:Independent, representative population samples of Warsaw residents aged 35-64 were examined in the frame of Pol-MONICA Projects (in 1984 year - 2552 persons; 1988 year - 1381 persons; 1993 year - 1460 persons; 2001 year – 843 persons) and WAW-KARD (in 2012 year - 614 persons). Nutrition patterns were assessed by interview of food intake in the 24-hours before the study.
Results:In 2012 in comparison to 1984, 23% decrease in fat and 40% decrease in dietary cholesterol consumption in men and women was noticed. However, in relation to saturated (SFA) and polyunsaturated (PFA) fatty acids (expressed as percentage of energy) course of changes in 1984-2001 and 2001-2012 was different. In the first period there was 20% decrease of SFA and 70% increase of PFA, in the second one the reversal of the trend was observed - increase SFA (men 13% and woman 20%) and decrease PFA (by 5% and 13%). Above mentioned changes resulted in course of atherogenicity level of diet as expressed by Keys score, significant reduction in 1984-2001 (men 56,5 to 43,0 and woman 56,7 to 41,7), and then increase in 2012 (respectively to 47,7 and to 49,3) was noted. This was associated with changes in preferences the type of fat used spreads and cooking. At first, after the growing interest in margarine and oils which was the cause of the increase in consumption of vegetable fats, the trend has been reversed, and again became more popular butter.
Conclusions:A positive tendency in fat consumption observed in 1984-2001 was further until 2012 inhibited and even reversed.
P656
Body mass index, insulin-like growth factor 1 and other factors in children with insulin resistance
A Tohatyova1, E Joppova1, N Fatulova1, D Stromplova1, I Schusterova2
1Safarik University, Faculty of Medicine, Kosice, Slovak Republic
2East-Slovak Institute of Cardiovascular Diseases, Kosice, Slovak Republic
Topic: Sports cardiology
Purpose:Adult study showed an inverse association between the insulin-like growth factor I (IGF-I) and the risk of impaired glucose tolerance or diabetes mellitus. These data suggested a protective effect of IGF-I against the development of metabolic syndrome. However, there are only few data in children population. Aim of our study was to association between IGF-I and obesity and insulin resistance (IR).
Methods:In 21 child (mean age 13.38 ± 2.69) with IR and 34 (mean age 12.32 ± 4.5) controls without IR, insulin-like growth factor 1 (IGF-l), growth hormone (HGH), hepatic enzymes, uric acid, lipids were measured. For the diagnosis of IR, 3.16 was used as the cut-off value of homeostasis model assessment of insulin resistance (HOMA-IR). Presence of metabolic syndrome was determined according to IDF 2007 criteria.
Results:In children with IR, there were only significant differences in body mass index (BMI) (p < 0.001), and body weight (p < 0.001). No differences were found in IGF-1 in spite of correlations of HOMA-IR with some of MS components; positive correlation with BMI (p < 0.001), body weight (p= 0.001), and with uric acid (p = 0,037), and negatively with HDL cholesterol (p = 0.031).
Conclusions:IR in childhood is s related to normal IGF-1 children and it seems that BMI and body weight both are more associated with IR than IGF-l. More study is required to elucidate biological mechanism of this complex relationship.
P657
Improved cardio-metabolic risk factors at three months after laparoscopic sleeve gastrectomy in morbidly obese individuals
RS Gavril1, AC Oprescu2, A Gherasim1, LI Graur1, L Mihalache1, SS Padureanu1, M Graur1
1"Grigore T. Popa" University of Medicine and Pharmacy, Iasi, Romania
2St Spiridon University Hospital, Diabetes, Nutrition and Metabolic Diseases, Iasi, Romania
Topic: Sports cardiology
Purpose:Obesity is correlated with increased cardio-vascular risk. However, pharmacological therapy for weight loss is scarce, and diet and exercise is insufficient for morbidly obese patients. Currently, bariatric surgery is the most efficient treatment for these patients. While Roux-en-Y gastric by-pass is the "gold-standard" procedure, the newer laparoscopic gastric sleeve (LGS) is beginning to show comparable results with fewer complications and long-term nutritional deficits. The aim of this study was to assess the modification in cardio-vascular risk factors in obese subjects after LSG.
Methods:We studied a group of obese patients who underwent LSG during 2013-2014 in our hospital. We evaluated the following clinical and biological parameters before and three months after surgery: body mass index (BMI), waist circumference (WC), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose, glycated haemoglobin (HbA1c), total cholesterol, HDL-cholesterol, triglycerides and uric acid. The study conformed to the principles of the Declaration of Helsinki.
Results:We studied a group of 28 patients (21 women), mean age of 41.4±11.7 years. Anthropometric and metabolic parameters improved significantly at three months after surgery, except for HDL-cholesterol, but the decrease in SBP and DBP was not statistically significant, as can be seen in Table 1.
Conclusions:LSG produced a significant weight loss after three months and had beneficial effects on metabolic parameters. SBP and DBP were not as much influenced by the weight reduction.
*mean value+/-standard deviation
Parameter
Before LSG*
3 months after LSG*
Sig. (p)
BMI (kg/m2)
43.2±6.9
33.8±6.7
<0.001
WC (cm)
126.6±18.2
107.6±17.9
<0.001
SBP (mmHg)
130±16.8
129±17.5
0.391
DBP (mmHg)
79.3±9.2
74±11.4
0.638
fasting plasma glucose (mg/dl)
116.4±43.3
98.9±21
0.013
HbA1c (%)
5.9±0.7
5.6±0.8
0.054
total cholesterol (mg/dl)
200.6±40
197.4±43
0.041
HDL-cholesterol (mg/dl)
45.9±12.6
44.5±12.7
0.014
triglycerides (mg/dl)
142±64.7
123.7±53.7
0.097
uric acid (mg/dl)
6.3±1.1
5.5±1.5
0.078
P659
Adipokine and incretin levels in metabolically healthy obese patients
M Boyarinova1, O Rotar1, E Moguchaya1, E Kolesova1, K Sysoev2, E Vasilieva1, V Yudina1, V Solntsev1, A Konradi1
1Federal Almazov Medical Research Centre, Saint Petersburg, Russian Federation
2Saint Petersburg Pavlov State Medical University, Saint Petersburg, Russian Federation
Objective:Obesity is believed to be associated with cardiovascular and metabolic complications; while a small proportion can be considered "metabolically healthy" obese (MHO) individuals, who have normal insulin sensitivity, lipid profile, and blood pressure. Absence if inflammation and neurohumoral activation can be an explanation for such phenomenon. The aim of the study was to assess the adipokine and incretin levels in obese individuals with and without metabolic disorders.
Design and methods:1600 relatively healthy bank employers were screened for metabolic syndrome (MS) in Saint-Petersburg (Russia). 155 participants were randomly selected out of subjects who had at least one component of MS and had no established cardiovascular events and severe concomitant diseases. Informed consent was obtained from all participants. Anthropometry and blood pressure measurement were performed according to standard protocols. Fasting plasma glucose and lipid profile were determined (Hitachi-902). Adipokines and incretins were measured on BioPlex Protein Array System (BioRad, USA). Insulin resistance (IR) was calculated using the HOMA IR formula. The threshold level for IR was considered 2,7. Metabolic health was defined as the presence of 0-1 cardiometabolic abnormalities according to the Wildman criteria, 2008. Nonparametric statistic was applied.
Results:From 155 subjects only 65 participants had obesity according to body mass index = 30 kg/m2: 10 participants were MHO (group 1) and 55 had metabolic disorders (group 2). Groups were matched for sex and age. The mean age was 47.6 years in the group 1 and 49.0 – in the group 2. There were no significant differences in levels of ghrelin, GIP, GLP-1, resistin, insulin and leptin between groups. Significantly different levels of PAI-1 13425.4 (7518.9; 30570.7) vs 33291 (13265.0; 48860.1) pg/ml, p = 0.04, and visfatin 388.4 (6.8; 625.1) vs 1354.0 (354.4; 2061.7) pg/ml, p = 0.006. Both were higher in the obese patients with metabolic disorders.
Conclusions:Visfatin and plasminogen activator inhibitor 1 are considered as pro-inflammatory markers and are related to endothelial dysfunction and atherosclerosis. Increase of these adipokines in obese patients might contribute to association of obesity with metabolic abnormalities.
P660
Cardiovascular risk reduction in obese patients submited to bariatric surgery persists over time
M Faustino1, S Bravo Baptista1, M Nedio1, C Monteiro1, E Lourenco1, V Gil1, C Morais1
1Hospital Prof. Dr. Fernando Fonseca, EPE, Amadora, Portugal
Topic: Sports cardiology
Purpose:Obesity associates with increased cardiovascular risk. Bariatric surgery (BS) has been demonstrated to result in relevant weight loss in the first moths after surgery and consequent improvement of most obesity-associated cardiovascular risk factors. However questions remain if this benefit persists long term. This study aims to evaluate long-term evolution of anthropometric and laboratorial parameters and functional capacity on a cohort of obese patients, submitted BS.
Methods:Patients were prospectively examined before BS (Eval1), 6 month (Eval2) and 3 years after BS (Eval3). Anthropometric parameters, lipid profile and glycaemia were obtained and a six-minute walk test (6mWT) was performed.
Results:Forty-one obese patients were included (mean age 46 years ±11; 38 women); The median time between BS and Eval2 was 217 days (IQR 93) and between Eval2 and Eval3 was 918 days (IQR 343). Results are presented in the table1. Weight and BMI continued to improve between Eval2 and 3, as did glucose and CRP values. The gain obtained in LDL-C values was not lost and HDL-C increased even further in Eval3.
Conclusion:The effect of BS on body weight persists after 3 years, with additional benefit. The initial improvement of metabolic and hemodynamic parameters and functional capacity, that accompanied weight loss, not only persisted but also improved additionally at 3 years, even after a very important weight loss had occurred.
Analysis (Eval2 vs Eval1) and (Eval3 vs Eval2). *p< 0.0001; **p=0,017; § p=0,015 (number of patients on anti-hypertensive therapy Eval1-11, Eval3-5); #p=0,0036;
Eval1
Eval2
Eval3
Anthropometric parameters
IMC (Kg/m2)
42.9±4.0
29.6±3.6*
27.4±3.1*
Weigh (kg)
113.5±12.8
78.5±11.8*
72.6±10.3*
Heart rate (1/min)
70.0±8.9
61.7±10.3*
61.0±7.5
Systolic blood pressure (mmHg)
129±16
124±21
135±22 §
Laboratorial parameters
Glycaemia (mg/dl)
100 (28)
85(8)*
82 (10)#
Total cholesterol (mg/dl)
194.4±45.4
169.2±304*
177.0±29.7
LDL cholesterol (mg/dl)
123.8±39.2
100.7±25.3*
95.4±26.9
HDL cholesterol (mg/dl)
45.9±10.2
51.8±13.0*
64.7±15.6*
High sensitive CRP(mg/ml)
1.33(1.54)
0.64 (1.05)*
0.29 (0.02)*
6mWT
Distance (m)
454±93
524±76*
539±77
P662
Return to work after acute coronary syndrome in independent workers
F Latil1, M-C Iliou2, C Boileau1, C Lechien1, P Ha-Vnh1, C Guimond1
1Service medical RSI, Paris, France
2Corentin Celton - APHP, Cardiac Rehabilitation and secondary prevention, Issy Les Moulineaux, France
Introduction:Failure in return to work (RTW) after an acute cardiac syndrome (ACS) can turn a medical success into turmoil such as job loss, weight gain or depression. The aim of this study was to assess the frequency and cause of delayed RTW after a first ACS in independent workers.
Methods:154 consecutive patients (independent craftsmen or shopkeepers) who underwent a first hospitalisation for acute coronary syndrome (ACS) were included.Primary outcome was RTW at 90 days. For patients who had not resumed work at90 days, social, medical and psychological processes were investigated via self-report questionnaires and medical examination.
Results:Among the 154 patients, 63 (40%) did not RTW on time at 90 days, as stated by the national guide-line. Among these 42 for medical, administrative or psychological reasons but 21 of those (15.7%) were ready to resume, had no reason to stand-by and were only waiting for the go-ahead from the cardiologist. Secondary outcome: uptake in medical knowledge of the disease was better 70,7 % , than the occupational knowledge (53.4%) Conclusion:We suggest that, a lot of the stand-by patients could resume work sooner if on time decision and education were implemented.
P663
Gender related differences in psychological distress and polyvascular disease in patients with coronary artery disease
A N Sumin1, EV Korok1, OI Raich1, RA Gayfulin1, AV Bezdenezhnyh1, OL Barbarash1
1RAMS Scientific-Research Institute for Complex Studying of Cardiovascular Diseases, Kemerovo, Russian Federation
Background:No doubt, polyvascular disease (PolyVD) worsens treatment outcomes in patients with coronary artery disease (CAD). Current medical literature report that PolyVD patients are more likely to have type D (distressed) personality, compared to patients with isolated atherosclerotic lesions. However, the impact of gender related differences on the relationship between psychological distress and PolyVD are still poorly understood.
Objective:To study the prevalence of psychological distress based on the presence of PolyVD and gender.
Material and methods:709 patients with stable CAD were examined and treated in the NII KPSSZ for the period from 1 February 2009 to 31 January 2010. Patients were assigned into four groups according to their gender and the presence of PolyVD: Group 1 – females without PolyVD (n = 108), Group 2 – females with PolyVD (n = 23), Group 3 – males without PolyVD (n = 471), Group 4 – males with PolyVD (n = 107). PolyVD was diagnosed as a combination of stenotic lesions >50% of two or more arteries. Trait anxiety levels were assessed with the Spielberger-Hanin anxiety test. Depression severity was assessed with the Depression Scale.
Results:Severe psychological distress is associated with unfavorable psychological profile in PolyVD patients of both genders. They had higher levels of depression and trait anxiety, compared to patients with isolated coronary lesions (Table 1).
Conclusion:CAD patients presenting with PolyVD had higher levels of depression and anxiety, regardless of gender. The relationship between psychological distress and PolyVD may be regarded as one of the factors affecting the prognosis in CAD patients.
PolyVD – polyvascular disease; * - p<0.05 in comparison with females without PolyVD; # - p<0.05 in comparison with females suffering from PolyVD; $ - p<0.05 in comparison with males without PolyVD
Indicators
Females without PolyVD (n=108)
Females with PolyVD (n=23)
Males without PolyVD (n=471)
Males with PolyVD (n=107)
p
Levels of depression
51.5 [48;54]
55 [49;57]*
53 [48;56]#
54 [49;56]*$
0.029
Trait anxiety levels
30.5 [29;35]
35 [31;43]*
32 [29;40]
34 [30;44]
0.006
P664
The psychological status of youngsters
I N Ryamzina1, AS Ragel2
1Perm State National Research University, Perm, Russian Federation
2Perm State Medical Academy, Perm, Russian Federation
Topic: Sports cardiology
Purpose:It is actual to discuss a role of psychological abnormalities in a development of cardiovascular disease (CVD). The aim of present study was to assess a psychological status of youngsters.
Methods:The study involved 160 students of the Medical Academy (53 males). Age of the respondents was 23.22 ± 0.17 years. HADS test was performed to identify anxiety and depression. Also we studied traditional CVD risk factors: body mass index (BMI), blood pressure (BP), glucose and cholesterol levels, tobacco-smoking and volume exercise Results:According to HADS test results 14.7% of the students observed subclinical anxiety and 7.35% clinical anxiety, 47.7% subclinical depression and 8.82% - clinical. The students indicated a high overload of educational process. 20% of them complained on weakness and fatigue, 8% - on decrease of capacity of work. Duration of sleep was less than 7 hours in 38.4% of the students. The average systolic blood pressure (SBP) was 113.68 ± 1.82 mm Hg, diastolic blood pressure (DBP) - 71,62 ± 0,99 mm Hg. BP = 140/90 mm Hg was found in 5.88%. It should be noted that the SBP was increased in students with significant anxiety / depression and decrease of physical activity.
Conclusion:Our data show that psychological abnormalities (anxiety and depression) are associated with arterial hypertension in youngsters. There is a need to promote a healthy lifestyle, including psychological support of the students. We suppose that a correction of educational program could be useful in this case.
P666
Implications of Literacy for health for blood pressure
M Cunha1, LS Nunes2, A Dias1, O Ribeiro1
1CI&DETS, Superior Health School , Polyrechnic Institute of Viseu, Viseu, Portugal
2Escola Nacional de Sa??a, Lisboa, Portugal
Topic: Sports cardiology
Purpose:This research aims to show how blood pressure is influenced by health literacy, salt intake habits, the use of sugar and herbs and spices in cooking.
Methods:A descriptive and transversal study was undertaken to collect data on a selected sample of 508 Portuguese individuals, aged 44-48. It was used the European Health Literacy Survey Questionnaire, (HLS- EU-Q) Health Literacy Survey in Portuguese (HLS-EU-PT) and a survey was created on salt intake, as well as on herbs and spices in cooking. Blood pressure was also measured.
Results:The majority of people who participated in the survey (35.83%) have both normal diastolic (PAS >130mmHg) and systolic blood pressure (PAD>85 mmHg); about 32.28% have high blood pressure, Stage 1 Hypertension, (systolic > 140-159 and diastolic > 90-99 mmHg). The participants who had a salt intake superior to the recommended maximum of 5 g/day got higher diastolic blood pressure measurements. Higher blood pressure levels were found in individuals who consumed either high levels of sugar (men 36 g/day and women > 20g/day) or did not use herbs and spices in cooking. Although participants who consume too much salt or sugar and those who do not use herbs and spices got higher blood pressure measurements, statistical differences among the groups are considered to be not significant. These data demonstrate that participants with inadequate health literacy, have higher blood pressure levels, have poorer health and suffer from more heart diseases when compared to those with good health literacy.
Conclusions:The study confirms that health status is directly correlated to literacy skills. Although there is no statistical significance, health literacy has an effect on blood pressure levels. Thus, it is both pertinent and necessary to invest in literacy as a promoter of this health indicator, while valuing clinical relevance.
P667
Gender and nationality effect on quality of life after beta-blocker up-titration in patients with heart failure: results from the CIBIS-ELD trial
HD Duengen1, E Tahirovic1, C Zelenak1, T Trippel1, M Fritschka1, V Celic2, S Apostolovic3, B Pieske1, ML Chavanon4, C Herrmann-Lingen4
2University Clinical Hospital Center "Dr Dragisa Misovic-Dedinje", Cardiology Department; Faculty of Medicine, University of Belgrade, Belgrade, Serbia
3Clinical Center of Nis, Cardiology, Nis, Serbia
4Georg-August University, Department of Psychosomatic Medicine and Psychotherapy, Gottingen, Germany
Objective:Previous research showed that quality of life (QoL) is based on the patient's emotional and social situation and characteristics of the treatment setting. Assumptions are that cultural aspects might influence the perception of psychosocial treatment aspects, but they have rarely been taken into account. In order to probe effects of cultural background on QoL independent of clinical improvement due to beta-blocker up-titration, we analyzed QoL data from the Cardiac Insufficiency Bisoprolol Study in Elderly (CIBIS-ELD).
Methods:German (G) and Serbian (S) patients were randomly assigned in CIBIS-ELD trial to up-titration with bisoprolol or carvedilol. The physical and psychosocial component scores on the short-form health survey (SF36) were recorded at baseline and after 3 months. Besides the design factors Sex, Nation and Time, all analyses accounted for age and clinical parameters such as NYHA functional class (I-II vs. II-IV) at baseline, objective physical performance in the 6-min walk test, LVEF, initial medication and final dosage of study medication at follow-up (0, ?155;, ¼, ½, >½ of the targeted dose). Complete data were available for 136 G (67 f) and 426 S (117 f). We controlled the number of unplanned visits and its interaction with NYHA class and nation in order to rule out QoL differences of that origin.
Results:Comparison of data showed that in both sexes and nations, both physical and mental QoL scores improved from baseline to follow up (d>.17, ps<=.001). However, differences in sexes have been noticed: men reported better both physical and mental QoL, F>6.6, ps<.01. When comparing the effect of nation: S showed a greater response on physical and mental QoL compared to G (S d=0.3-0.34 vs. G d=0.07-0.12). It was also shown that cultural differences in treatment response were strongest for facets that are less affected by beta-blockers. Treatment effects associated to NYHA class were only observed on physical QoL, F=9.38, p=.002. For patients in NYHA classes III-IV the treatment resulted in a lager improvement of physical QoL than for NYHA I-II and their physical QoL was not different from that of patients with less severe heart failure at follow-up anymore, p>.10.
Conclusion:This researched showed clear cultural differences in QoL change: S showed a stronger positive response to treatment compared to G. This effect might be associated with national differences when it comes to prevention and health care service or cultural aspects related to the perception of interpersonal factors as nation effects were more pronounced on the psychosocial than on the physical QoL facet.
P668
Hurdles and expectations towards preventative measures in urban women (from the BEFRI study): tailoring prevention to selective needs
S Oertelt-Prigione1, U Seeland1, M Ruecke1, V Regitz-Zagrosek1
1Charité - Universit?medizin Berlin, Institute of Gender in Medicine, Berlin, Germany
Topic: Sports cardiology
Purpose:Preventative measures and lifestyle changes are essential strategies towards population health. We sought to explore lifestyle measures, uptake barriers and expectations in the female urban population, as well as subjective health information sources to define overall subgroup patterns in lifestyle choices.
Methods:Within the BEFRI (Berlin Female Risk Evaluation) study, we enrolled 1062 women aged 25-74 years. Participants completed questionnaires and attended an extensive clinical examination. Lifestyle factors, subjectively perceived hurdles and expectations and health information sources were elicited. Behavioral patterns, wishes and hurdles were evaluated in multivariate analysis using social, economic and clinical variables as independent explanators.
Results:49.6% of the study participants reported lifestyle measures (e.g. weight control, physical activity, relaxation techniques, smoking cessation etc.) in the last 12 months, with no significant age-related differences. Target groups were successfully addressed, e.g. overweight and diabetic women more frequently engaged in weight management effort (adjusted, OR = 3.9, C.I.= 1.7-9.3 and OR = 4, C.I.= 1.5-10.8). Subjectively perceived hurdles for participation varied. Older women (OR= 1.8, C.I.= 1.0-3.4 for each of 5 age strata) and women with hypercholesterolemia (OR= 3.4, C.I.= 1.3-8.9) feared of inability to change. Overweight women (OR=3.2, C.I.=1.3-8.1) and women living alone (OR=2.4, C.I.= 1.1-5.8) feared lack of physical ability. Expectations diverged, e.g. social rewards were most relevant in women living alone, proximity to work for women with children and higher earning brackets and opportunity to perform measures at home for overweight women and women with a history of tumor disease. Health information sources also differed. Physicians and pharmacists were only reported as primary sources if frequent access was granted, i.e. women having had medical contact in the last three months or with frequent follow-up visits. Magazines and newspapers were the main source for older women and TV for women with low-income jobs. Internet consultation for health information significantly decreased with income (OR=0.8, C.I.= 0.7-0.9, for each of 5 wage brackets).
Conclusions:Our analysis identified specific patterns, expectations and limitations for the uptake of preventative lifestyle measures by different subgroups of urban women. These data, combined with the reported differences in information access, should be taken in consideration for the development of future information campaigns and for general health counseling.
P669
Sports history and timing of first myocardial infarction in normal weight men younger than 65 years
P Eser1, C Janggen1, C Graeni1, L Raeber1, M Wilhelm1
1Preventive Cardiology & Sports Medicine, University Clinic for Cardiology, University Hospital Berne, Berne, Switzerland
Background/Aim:Regular physical activity delays the onset of atherosclerosis through positive modification of cardiovascular risk factors (CVRF). However, vigorous exercise may lead to acute plaque rupture and premature myocardial infarction (MI) in patients at risk. Our retrospective cohort study assessed sports history and age at first MI in young to middle aged normal weight men with MI.
Methods:The registry of consecutive percutaneous coronary interventions (PCI) at the University Hospital Bern was analyzed from March 2009 until January 2012. Male patients with acute MI between 18 and 65 years and body mass index =25kg/m2 were included. Sports history was assessed by telephone interview. Patients were grouped according to starting age with sports =1 h/week outside school sports (EARLY:<18 years, CONTROL:=18 years or never). Cumulative lifetime training hours, CVRF and circumstances of MI were recorded. The primary end-point was age at first MI. Sub-group analyses were performed for two age groups (20-55 years vs. 56-65 years). Groups were compared by independent t-, Mann-Whitney, or Chi square test, as appropriate.
Results:Of 4394 consecutive patients who underwent PCI, 212 fulfilled the inclusion criteria and were interviewed (EARLY 133, 62.7% and CONTROL 79, 37.3%). Age at first MI was significantly lower in EARLY compared to CONTROL. This was solely due to the earlier onset of first MI in the subgroup of 20-55 years (mean ± SD 46.8 ± 6.0 vs. 49.8 ± 4.6 years; p=0.006), while the subgroup of 56-65 years showed no differences (60.0 ± 2.9 vs. 60.5 ± 2.6; p=0.49). The proportion of exercise-related acute MI was not different between the groups (11.3% vs. 12.6%; p=0.66). In EARLY mean yearly training hours were higher than in CONTROL for both subgroups (p<0.001). Patients in EARLY had fewer CVRFs (1.7 vs 2.2; p=0.003). Fewer EARLY patients had hypertension or hypercholesterinemia (p=0.011), but groups were comparable for diabetes mellitus and family history. Smoking was equally high in EARLY and CONTROL (58% and 59%). For the subgroup 20-55 years, patients in EARLY exhibited more frequently one-vessel disease and ST-elevation MI (51.9% vs. 31.0%; p=0.027, and 76.5% vs. 57.1%; p=0.026, respectively).
Conclusions:Unexpectedly, in patients aged 55 and younger, occurrence of first MI was 3 years earlier in those who started regular sports activity before age 18, despite a more favorable CVRF profile. Exercise may exhibit negative effects on an endothelium altered by smoking and/or in the presence of genetic risk factors.
P670
Early and late aortic propagation velocity values in STEMI patients after successful primary PCI
M Yaman1, O Beton2, HE Pamukcu2, A Aksakal1, A Hakan1, S Aktag1, O Yucel1, O Dogdu3
1Samsun Education and Research Hospital, Samsun, Turkey
2Diskapi Yildirim Beyazit Education and Research Hospital, Ankara, Turkey
3Firat University, Cardiology, Elazig, Turkey
Aim Atherosclerosis is a generalized disease that mainly manifested in medium-sized vessels and also present in the great vessels, such as the thoracic aorta. Atherosclerosis leads to arterial stiffness. M-mode propagation velocity of the descending thoracic aorta or aortic velocity propagation (AVP) is a novel method for the measurement of the aortic stiffness. It is not known yet whether AVP value could change after effective treatment in STEMI patients. We aimed to investigate the difference between early and late values of AVP after successful primary PCI in STEMI patients.
Methods:A total of 100 consecutive patients without previously known coronary artery disease who presented with STEMI without hemodynamic comprimise and undergone successful primary percutaneous coronary intervention (PCI) were selected prospectively. Presence of more than 50% lesion in coronaries other than culprit vessel and hemodynamic comprimise in ICU after primary PCI were exclusion criterias. Transthorasic ecocardiography (TTE) was performed to all of patients after primary PCI at 12-24 hour in ICU (early measurements) and during the third month control (late measurements) after discharge. All patients received guidelines based optimal medical therapy during hospital stay and after discharge. Doppler echo, 2D and AVP measurements were recorded. Haematological and serum biochemical parameters of the study group were recorded.
Results:The study group was consisted of 77 male and 23 female patients with 175.6±120.4 min symptom onset-to-balloon time. There was no difference between 2D echocardiography measurements between early and late evaluations. AVP values increased at late control in all patients. Mean AVP values were 33.7± 11.6 cm/sn and 44.4±10.5 cm/sn at early and late measurements, respectively (p<0.001). Increase of AVP value (difference between early and late) was more prominent in patients with hypertension(n=49) in comparison with patients without hypertension, 12.5±7.2 cm/sn and 8.9±8.7 cm/sn, respectively (p=0.027). While, this difference is not significant between patient with and without diabetes mellitus. There were significant correlations between difference of AVP and neutrophil lymphocyte ratio between early and late measurements (r = ?.699, P < 0.001).
Conclusion:It was shown for the first time that AVP values could improve after successful treatment in STEMI patients. Increments in AVP values were closely correlated with decrements in neutrophil lymphocyte ratio. It can be postulated that AVP has strong relationship with acute inflammatory process
P671
Impact of cardiovascular polypill based therapy on healthy lifestyle behavior
R Webster1, C Bullen2, A Patel3, A Rodgers1, V Selak2, S Thom4
1The George Institute for Global Health, Cardiovascular, Sydney, Australia
2National Institute for Health Innovation, Auckland, New Zealand
3The George Institute for Global Health, Office of the Chief Scientist, Sydney, Australia
4Imperial College London, London, United Kingdom
Background:The effectiveness of a polypill strategy in improving adherence to recommended CVD preventive medications has been established. However there are concerns that this strategy may deflect attention from lifestyle measures of prevention. The Single Pill to Avert Cardiovascular Events (SPACE) collaboration is a prospective, individual participant data meta-analysis of three trials conducted from 2009 to 2013 comparing polypill-based care with usual care in patients with established CVD or similarly high risk. Patients in the SPACE trials knew they were taking the polypill. This setting enables assessment of changes in beneficial lifestyle behaviours in those who were randomised to the polypill group.
Aim:To assess the effect of polypill-based care on CVD preventive lifestyle behavior.
Methods:The SPACE trials include: UMPIRE (India, n=1000; Western Europe, n=1004), Kanyini-GAP (Australia, n=623) and IMPACT (New Zealand, n=513). The 3 trials had similar protocols and used the same polypill (containing aspirin, lisinopril, simvastatin and either atenolol or hydrochlorothiazide). Analyses were conducted on a combined dataset using a log-binomial model with treatment group as a fixed effect and trial as a random effect. Analysis of continuous measures used a linear mixed model (baseline value and treatment arm as fixed effects) and a random trial intercept and random trial-by-treatment interaction.
Results:At 12 months, no difference was seen between polypill and usual care groups for BMI (mean difference 0.0 kg/m2, 95% CI -0.1 to 0.2, p=0.68), waist circumference (mean difference 0.1cm, 95% CI -0.3 to 0.5, p=0.73), smoking (RR 0.96, 95% CI 0.81 to 1.14, p=0.65), or quitting smoking before month 12 (RR 1.00, 95% CI 0.66 to 1.51, p=0.99). Similar findings were seen in high-risk primary prevention and secondary prevention patient populations, with tight confidence intervals around a null effect on BMI, waist circumference and smoking measures in both groups.
Conclusions:These data provide the first randomised evidence that use of a polypill does not adversely impact beneficial lifestyle behaviour in both primary and secondary prevention populations.
P672
Effect of preventive measures for major metabolic parameters in patients with non-alcoholic fatty liver disease and cardiovascular risk
OV Kolesnikova1, VD Nemtsova2
1L.T.Malaya Institute of Therapy, Cardiology, Kharkiv, Ukraine
2Kharkiv National Medical University, Cardiology, Kharkiv, Ukraine
The purpose - the dynamic assessment of the preventive measures impact on the main metabolic parameters in patients with nonalcoholic fatty liver disease (NAFLD) in combination with obesity with low and moderate cardiovascular risk (CVR).
Materials and methods:In 184 patients aged 40-62 years with NAFLD and obesity with low and moderate CVR was studied the effect of a personalized diet with a gradual reduction of daily energy intake (400 kcal every 2 weeks) and with the dose of physical activity to 250 minutes or more per week in combination with strength training 90 minutes a week on the main of basic anthropometric, metabolic (lipid profile) and hormonal (adiponectin, resistin) parameters and the relative value of CVR. In addition, ursodeoxycholic acid (UDCA) at a dose of 1000 mg/day was recommended to all patients. Evaluation of the data was performed directly before treatment and after 12 months. Adiponectin, resistin, insulin, tumor necrosis factor-a (TNF-a), C-reactive protein (CRP) in serum were determined by enzyme immunoassay. Assessment of the hepatic steatosis degree and the measurement of the thickness of carotid intima-media complex (IMT) were performed by ultrasound scanner.
Results:Under the influence of the lifestyle modification in NAFLD patients with low and moderate CVR was obtained significant improvement of basic anthropometric parameters: body mass index and waist circumference reduction (p = 0.0000), levels of systolic and diastolic blood pressure (p = 0.005 and p = 0.004, respectively). A significant improvement of the hormonal (increase of the adiponectin level, decrease of the resistin, TNF-a, CRP levels, p <0.005) and metabolic (increased cholesterol of HDL and decreased triglycerides (p=0,05), a significant reduction in insulin levels (p = 0.0002) parameters was shown. Moreover, 50% of studied patients that have reduced body weight at 10% of the initial, showed optimal results of these indicators. There was a significant tendency in the decreasing of IMT values (p = 0.02). Clinically significant result in the dynamics of 12 months observation was a redistribution in groups of studied patients the level of CRV - increase the part of patients with low CVR (54.76%) compared to the moderate CVR (45.23%), p = 0.01, a significant decrease in median relative CVR (p = 0.03).
Conclusions:Timely individual prevention of cardiovascular diseases in patients with NAFLD significantly improves the basic metabolic indexes and reduces the degree of CVR, which is essential in prevention of the complications development and improve life quality.
P673
HRV spectra shed light upon heart rate control during sleep
R M Negoescu1, I-E Csiki1
1Institute of Public Health Bucharest, Bucharest, Romania
Background:Autonomic control of heart during sleep is poorly understood: e.g. occurrence of arrhythmias in certain stages contrasts the protection brought about by higher vagal tone.
Methods:9 normals 19-31 y were studied during 2 nonconsecutive nights by EEG (O1–O2), oblique EOG, ear temperature, thermistor respiration, ear lobe plethysmogram, and lead II ECG producing RR series. Sleep stages were scored every minute cf. conventional criteria, and power spectra of 256 second-long quasi-stationary RR epochs were got by: 1) resampling at 0.5 s; 2) mean substraction and normalization; 3) zero padding towards 512 points; 5) Sande-Tukey FFT. Power was summed over adjacent bands as follows: VLF/nonstationarity&trends (.007–.035Hz), LF/vasomotor (–.166), HF/respiratory (–.39), and total (.007– .5).
Results:Table 1 shows data from 41 RR spectra as per stages 1+2 = NREM1 (shallow, n=as shown), 3+4 = NREM2 (profound), and REM, one spectrum per stage. P points to non-matched/2 tails Wilcoxon. Discussion. Results show increase of HF with sleep deepness and converse trend in LF. REM features tachycardia bursts alternating with low variability bradycardia "plains" that jointly elicit enrichment of VLF and VF. While plains evoke sinus arrhythmia attenuation under mental loading while vigil, burst pattern and mean RR slightly lower vs NREM2 suggest a sympathetical revival. Increased dual autonomic tone (IDAT) in REM evokes early reports of Skinner & Guilleminault on arrhythmic potential of high level dual balance under ischemia and of REM in coronary pts.
Conclusion:In REM, medullary centers are perhaps overridden by a neural inflow of cortical origin on an IDAT background, arguing for REM interpretation as a wakefulness sui generis promoting arrhytmias in certain cases. NREM to REM reciprocal dynamics of HF and VLF powers may conceivably help the automatic sleep scoring.
variable/stage
REM (12)
P
NREM1(21)
P
NREM2(8)
P
REM(12)
mean RR [ms]
1192
NS
1238
NS
1261
<.02
1192
SD [ms]
113.8
<.02
93.8
NS
84.6
<.03
113.8
total power [a.u.]
0.38
<.001
0.21
<.03
0.15
<.001
0.38
VLF power/total
0.392
<.001
0.207
NS
0.164
<.001
0.392
LF power/total
0.285
NS
0.278
NS
0.200
<.005
0.285
HF power/total
0.280
<.001
0.457
NS
0.607
<.001
0.280
P674
The relation of ambulatory heart rate with all-cause mortality among middle-aged men: a prospective cohort study
E Clays1, M Lidegaard2, F Kittel3, K Van Herck1, G De Backer1, D De Bacquer1, A Holtermann2, M Korshoj2
1Ghent University, Ghent, Belgium
2National Research Centre for the Working Environment, Copenhagen, Denmark
3Free University of Brussels (ULB), Brussels, Belgium
Topic: Sports cardiology
Purpose:The aim of this study was to investigate the association between average 24-hours continuously measured ambulatory heart rate and all-cause mortality, while adjusting for resting clinical heart rate, cardiorespiratory fitness, occupational and leisure time physical activity as well as classical risk factors.
Methods:A group of 439 male workers free of baseline coronary heart disease and aged 40-55 years from the prospective Belgian Physical Fitness Study was included in the analysis. Data were collected by questionnaires and clinical measurements and examinations from 1976 to 1978. All-cause mortality was collected from the national mortality registration with a mean follow-up period of 16.5 years, with a total of 48 events.
Results:After adjustment for all before mentioned confounders in a Cox proportional hazards regression analysis, a significant increased risk for all-cause mortality was found among the tertile of workers with highest average ambulatory heart rate compared to the tertile with lowest ambulatory heart rate (Hazard ratio = 3.21, 95 % confidence interval: 1.22-8.44). No significant independent association was found between resting clinic heart rate and all-cause mortality.
Conclusions:The study indicates that average 24-hour continuously measured ambulatory heart rate is a strong predictor of all-cause mortality independently from resting clinic heart rate, cardiorespiratory fitness, physical activity and other classical risk factors among healthy middle-aged workers.
P675
Self-reported psychosocial stress and risk of atrial fibrillation - From The Birkebeiner Ageing Study
M Myrstad1, AH Ranhoff1, DS Thelle2, EE Solberg1
1Diakonhjemmet Hospital, Oslo, Norway
2University of Oslo, Oslo, Norway
Topic: Sports cardiology
Purpose:Psychosocial stress increases the sympathetic tone and is a risk factor for coronary heart disease (CHD). Autonomic imbalance is among the suggested underlying mechanisms for AF among endurance-trained individuals, but an association between stress and atrial fibrillation (AF) has not been established. Therefore, we explored the association between stress and risk of AF among male non-elite senior cross-country skiers and men from the general Norwegian population.
Methods:The study was designed to investigate the association between endurance exercise and risk of AF. In order to cover the broad range from physical inactivity to repeated participation in a long-distance endurance competition, this cohort study was based upon 2 distinct cohorts: 3114 men who had previously completed the 54-kilometer Birkebeiner cross-country ski race and 1185 men who had participated in a population-based health study. Altogether 4999 men aged >53 years were invited to take part in the study. Stress during the previous 5 years was self-reported by questionnaires and categorized into "No-", "Periodical-" and "Continuous" stress. Self-reported AF was confirmed by electrocardiograms (ECGs) reviewed from medical records.
Results:3712 men (74%) participated in the study (mean age 66 (53-92) years). 254 cases of AF were confirmed by ECG. After multivariable adjustments, the adjusted odds ratios for AF were 1.66 (95% confidence interval (CI) 1.23-2.23) for periodical and 1.81 (CI 0.98-3.33) for continuous stress.
Conclusions:Self-reported stress at home during the previous 5 years was positively associated with AF. However, as AF might have preceded stress, this study is not designed to conclude about the direction of the association or causality.
P676
Cardiovascular risk factors: underdiagnosis before admission due to acute coronary syndrome.
B Samaniego Lampon1, E Hernandez Martin1, G Alvarez Cuervo1, A Arias Suarez1, V Cabrera Garcia1, M Fernandez Garcia1, I Garcia Ruiz1, M Martin Suarez1, S Morala Gonzalez1, E Segovia Martinez De Salinas1
1Hospital de Cabuenes, Cardiology Department, Gijon, Spain
Topic: Sports cardiology
Purpose:To be aware and to control cardiovascular risk factors is essential to prevent cardiovascular events. We analyse the underdiagnosis of major cardiovascular risk factors in very high risk cardiac patients admitted for acute coronary syndrome (ACS), by collecting risk factors that patients are known to present and studing their real prevalence.
Methods:Descriptive study including 50 patients with ACS from December 2013 to March 2014. We conducted a survey at admission to register the prevalence of known or treated hypertension, diabetes or dyslipidemia, smoking habits and body mass index. We took the mean of blood pressure measurement at 8 am, before morning medication, on two consecutive days and considered hypertension if =140/90. We used fasting plasma glucose and glycated haemoglobin to establish the diagnosis of diabetes or pre-diabetes. As LDL-cholesterol is recommended as target for treatment and the LDL-cholesterol goal depends on total cardiovascular risk (CVR), we estimated the CVR before the ACS using the ESC classification based on the SCORE chart and compared LDL-cholesterol levels to goals. We evaluated again the CVR before the ACS, taking into account the unknown new diagnosed risk factors, and compared the two estimations.
Results:Mean age was 68 ± 13 years, 74% of patients were male. A previous cardiovascular event was suffered by 38% of patients. The percentage of current smokers was 32%, with 32% being ex-smokers and 36% having never smoked. Obesity was present in 6% of cases, overweight in 54%. Hypertension was known or treated in 48% of patients, diabetes in 30% and dyslipidemia in 42%. Based on the data obtained during hospitalization, the real prevalence was 62% for hypertension, 42% for diabetes and 72% for dyslipidemia. We also found pre-diabetes in 16% of patients. Attending only to the previously known risk factors, the CVR before admission was very high in 58%, high in 14%, moderate in 24% and low in 4% of patients. Taking into account the new diagnosed risk factors, 12% of cases were reclassified to a superior level of CVR: 3 patients changed from high to very high risk level, 1 patient from moderate to high and 2 patients from moderate to very high.
Conclusions:Major cardiovascular risk factors were remarkably infradiagnosed and undertreated before admission for acute coronary syndrome, with 14% of new diagnosis of hypertension, 12% of diabetes, 16% of pre-diabetes and 30% of patients with LDL-cholesterol above goals.
P677
New-onset chronic obstructive pulmonary disease and its clinical significance among patients with STEMI
OLGA Polikutina1, EVGENY Bazdyrev1, OLGA Barbarash1
1Federal State Budgetary Institution Research Institute for Complex Issues of Cardiovascular Diseases, kemerovo, Russian Federation
Topic: Sports cardiology
Purpose:To study the incidence of new-onset chronic obstructive pulmonary disease and its clinical significance among patients with ST-elevated myocardial infarction (STEMI).
Materials and methods:154 STEMI patients were enrolled into the study. All the patients underwent pulmonary function test with bronchodilatatory test performance and body plethysmography. The level of ultra-sensitive C-reactive protein (CRP) at 10-14th days from the beginning of STEMI clinical implications was determined.
Results:34 (22%) out of 154 patients were known to have a history of COPD. Among 120 patients without a history of pulmonary pathology, 24 (20%) patients revealed new-onset irreversible post-bronchodilatatory respiratory obstruction and were diagnosed with COPD as a result of our examination. All the patients with new-onset chronic obstructive pulmonary disease had respiratory symptoms of varying intensity before the present hospitalization, but they didn't seek for medical help. Among STEMI patients with concomitant COPD the lower values of diffusing lung capacity were registered, however there were higher values of CRP. Recurrent myocardial infarction, early postinfarction angina were registered more often and the degree of pneumonia incidence during the hospital phase of myocardial infarction reached significant differences.
Conclusion:It is necessary to perform screening spirometry in order to identify COPD among patients with CAD, which will allow to reduce the risk of complications and improve the prognosis in this group of patients.
P679
Kidney injury: an important predictor to remember in acute coronary syndrome
R Ferreira1, J Neves1, A Gonzaga1, M Bastos1, J Santos1
1Centro Hospitalar do Baixo Vouga, Cardiology, Aveiro, Portugal
Topic: Sports cardiology
Purpose:Morbidity associated with chronic kidney disease (CKD) has increased with the growth of aging populations. CKD is strongly associated with increased mortality rate and accelerated cardiovascular disease.
Methods:Retrospective observational analysis of 431 patients admitted on a coronary intensive care unit with acute coronary syndrome for 2 consecutive years. Patients were followed-up until the 31st october 2013 or until another event (new acute coronary syndrome, stroke, heart failure, arrhythmia or cardiac death).
Results:431 patients were included, 72.4% were male, with mean age of 67 ± 13 years, 33.2 % with kidney injury on admission. The multivariate Cox analysis adjusted for potential confounders (sex, hypertension , diabetes, dyslipidemia, obesity , family history, previous events, kidney injury and anemia) showed that the only variables that remained as independent predictors of new events were the existence of previous events (HR 1.759; 95% CI 1335-2138 with p = 0:00), kidney injury (HR 0572; 95% CI 0340-0961, p = 0.035), and anemia (HR 0.484; 95% CI 0.265- 0.883 with p = 0.018 ) . Dividing patients into two groups based on the presence of kidney injury, we found that patients with kidney injury had higher values ?128;??128;?of systolic blood pressure and heart rate at admission; they had more advanced Killip class and more often had episodes of atrial fibrillation. Kaplan- Meier's survival curves showed that these patients had worse event-free survival (log rank of 10,912 with p < 0.001).
Conclusion:The presence of kidney injury was one of the most important predictors of new cardiovascular events, highlighting the importance of early identification of these patients in order to adopt individualized therapeutic strategies to prevent new cardiovascular events and to reduce the progression of kidney disease.
P680
Cardiovascular disease knowledge, health behaviors, physician communication, health self-efficacy and health education in ultra-orthodox jewish female teachers
E Langner-Leiter1, K Greenberg1, M Donchin2, M Nubani1, S Siemiatycki3, C Lotan1, D Zwas1
1Hadassah University Medical Center, Cardiology Department, Jerusalem, Israel
2Hadassah-Hebrew University, Braun School of Public Health, Jerusalem, Israel
3Bishvilaych, The Evelyne Barnett Womens Medical Center, Jerusalem, Israel
Topic: Sports cardiology
Purpose:The Ultra-Orthodox Jewish (UOJ) community represents 10% of Israel's population. UOJ women engage in lower levels of health behaviors (HB) and have higher rates of diabetes and obesity. Barriers are likely cultural, religious and socio-economic (i.e. large families, modesty, restricted exposure to secular media and education, and poverty). Research in this population is scant. This study explored cardiovascular disease (CVD) knowledge, HB (i.e. diet and physical activity (PA)), and physician communication (PC) in UOJ female teachers and investigated the relationship of health self-efficacy (HSE) and health education (HE) to HB.
Methods:As part of an ongoing health promotion program, 285 female UOJ high school teachers from 3 schools in Israel completed questionnaires. Questions included demographic, HB and knowledge items and a HSE scale. HE was defined as self-reported education or training in nutrition and PA. Knowledge items included correct identification of heart attack symptoms (HASx) and correct identification of CVD risk factors. PC was defined as having one's physician discuss specified topics.
Results:Teachers' age range was 21-71, mean number of children was 6 (range= 0-17), 37% were below poverty level, 32% were overweight and 17% were obese. Thirty four percent reported >150 minutes/week of moderate PA, 11% reported >75 minutes/week of vigorous PA, 26% reported eating >5 fruits and vegetables/day, and 19% reported eating >3-4 servings of whole grains/day. Transfat usage was 41%. Only 2% correctly identified all HASx and 2% all CVD risk factors. Knowledge of CVD risk factors and HE in nutrition were each associated with eating >5 fruits and vegetables/day (p=.045 and p=.01) and less transfat (p=.094 and p=.056). HE in PA was associated with engaging in >75 minutes/week of vigorous PA (p=.002). PC about weight or nutrition were each associated with eating the recommended servings of fruits and vegetables (p=.008 and p=.002) and whole grains (p=.016 and p=.062). PC about exercise was not associated with PA. HSE was associated with eating the recommended servings of whole grains and fruits and vegetables, less transfat, and engaging in the recommended amount of moderate and vigorous PA (p=.076, p<.0001, p=.051, p=.004, p=.0007).
Conclusions:This study is the first investigating HSE, HE, CVD knowledge, PC, and HB in an UOJ population. UOJ teachers reported engaging in moderate to low levels of PA and healthy eating as well as limited CVD knowledge. Exposure to HE, PC, and increased HSE may improve the rates of these preventive health behaviors.
P681
Association of earlobe crease with cardiovascular risk factors and diseases: the CoLaus study
M Aligisakis1, P Vollenweider2, P Marques-Vidal2
1University of Lausanne, Lausanne, Switzerland
2University Hospital Centre Vaudois (CHUV), Lausanne, Switzerland
Background:Earlobe crease (ELC) has been associated with cardiovascular disease (CVD) or risk factors (CVRF). However, the associations were usually limited to a small number of CVRF and the mechanisms involved are poorly understood.
Methods:Data from the population-based CoLaus study (n=4635, 46.7% men) conducted between 2009 and 2012 in Lausanne, Switzerland.
Results:Presence of ELC was associated with age, male gender, higher body mass index (BMI), abdominal obesity, hypertension, higher glucose and insulin levels, diabetes, insulin resistance, dyslipidaemia (especially lower HDL cholesterol and higher triglycerides levels), metabolic syndrome (MS) and history of CVD. In multivariate analyses adjusting for age and gender, ELC remained significantly associated with abdominal obesity [odds ratio and (95% confidence interval) 1.20 (1.02; 1.42)]; hypertension [1.41 (1.18; 1.67)]; diabetes [1.43 (1.15; 1.79)]; high HOMA-IR [1.53 (1.18; 1.99)]; lower HDL cholesterol and higher triglycerides levels (p-value < 0.05), MS [1.28 (1.08; 1.51)] and history of CVD [1.55 (1.21; 1.98)]. However, when BMI was added to the model, only the associations between ELC and hypertension [1.30 (1.08; 1.56)], glucose level (p-value <0.05) and history of CVD [1.55 (1.21; 1.98)] remained significant.
Conclusion:In this community-based sample we observed a significant association between ELC and some classical cardiovascular risk factors (particularly higher BMI and hypertension) but also with a positive history of CVD.
P682
Evaluation of oral anticoagulation therapy in patients with atrial fibrillation and high thromboembolic risk
M Zlatar1, D Matic1, B Zlatar2, D Jelic1, M Marjanovic3, T Potpara3, M Gajic4
1Cardiology Clinic, Emergency Department, Clinical Center of Serbia, Belgrade, Serbia
2City Institute of Public Health, Belgrade, Serbia
3Cardiology Clinic, Clinical Center of Serbia, Belgrade, Serbia
4University of Belgrade, School of Medicine, Institute for Medical Statistics and Health Research, Belgrade, Serbia
Topic: Sports cardiology
Purpose:Anticoagulation is the cornerstone of therapeutic measures for prevention of thromboembolic complications in patients with atrial fibrillation. This therapy is particularly important to apply in patients with atrial fibrillation and high thromboembolic risk. The aim of our study was to investigate the use of anticoagulation in patients with atrial fibrillation and high risk of thromboembolic complications.
Methods:Our study included 229 patients with electrocardiographic evidence of atrial fibrillation who were treated in cardiology ambulance of Emergency Center in Belgrade from 1/2009 to 12/2012. Thromboembolic risk was assessed according to CHADS2 score. In high thromboembolic risk considered patients with CHADS2 score =2.
Results:Out of 229 patients included in our study who had proven atrial fibrillation and high thromboembolic risk, anticoagulant therapy was performed in 100 patients (43.7%). There was no statistically significant difference between patients receiving oral anticoagulant therapy compared to patients without oral anticoagulant therapy in terms of demographics (age and sex) and the presence of other risk factors and co morbidities (smoking, hypertension, hyperlipidemia, diabetes mellitus, congestive heart failure, previous stroke, chronic renal failure and hyperthyroidism). Patients who received oral anticoagagulant therapy had more frequently coronary artery disease (31.0% vs. 17.0%; p = 0.013), prior myocardial infarction (18.0% vs 7.8%; p = 0.019), control examination by internal medicine specialist (61.0% vs. 21.7%; p = 0.000) and less frequently received oral antiplatelet therapy (16.0% vs. 69.0%; p = 0.000) than those without anticoagulant therapy.
Conclusion:In our study, oral anticoagulation is not prescribed in a large percentage of patients with atrial fibrillation and in high thromboembolic risk as it was recommended by European Guidelines. Patients receiving oral anticoagulant therapy had more frequently coronary artery disease, history of myocardial infarction, are often controlled by a physician specializing in internal medicine and less frequently received concomitant antiplatelet therapy than those without anticoagulation.
P683
Cardiovascular risk in the working population of Ryazan region (Meridian-Ro study)
E Philippov1, S Iakushin1
1Ryazan State Academician I.P. Pavlov Medical University, Ryazan, Russian Federation
In Russia, cardiovascular mortality remains very high, which has a significant impact on life expectancy. It is comparable to CVD mortality in Finland 70s and is different from the present (2011) is more than 2.5 times. Back in the 50s, it was shown that the main contribution to the development of CVD risk factors contribute, so the conventional concept of mortality reduction is to fight with them. Their prevalence in the Russian Federation are high, however, in some regions still remains unknown.
Objective:To investigate the prevalence of major risk factors for CVD in the region and their complex influence on cardiovascular risk.
Methods:The study included 1622 human urban and rural population aged 25-64 years without diagnosed CHD (mean age - 43,4 ± 11,4 years, 46.2% male) randomly selected by sectional sample. They conducted a survey on a standardized questionnaire, electrocardiogram, measurement of blood pressure, heart rate, waist circumference, height, weight, intake of biological samples for the determination of biochemical risk profile, a comprehensive assessment of cardiovascular risk. The study was an open, prospective, cross-sectional.
Results:It was found that 4.3% of persons surveyed had very high 10-yrs risk on a scale HeartSCORE (city - 4.3%, rural - 4.2%, p> 0.05). The high risk group had a total of 15.0% (city - 14.1%, rural - 17.9%, p> 0.05), moderate - 54.9% (city - 53.8%, country side - 58 2%, p> 0.05), the lowest - 25.8% (city - 27.9%, rural - 19.7%, p> 0.05). The study was 17.7% rural and 13.4% urban with atherosclerosis and related diseases. When evaluating the biochemical markers, it was found that the CRP (6.89 vs. 5.7 mmol / l, p = 0.0001), LDL (3.55 vs. 3.28 mmol / l, p = 0.05), cholesterol (5.65 vs. 5.16 mmol / l, p = 0,05) and uric acid (335 against 302 mmol / l, p = 0.0001) were higher in the high risk group. In addition, HDL were lower in the high risk group (1.25 vs. 1.33 mmol / l, p = 0.05). In the analysis of medical consultations in the high-risk group showed significant greater number of outpatient visits (82.8% vs. 73.5%, p = 0.0001), appeals by ambulance (20.2% vs. 10.0%, p = 0.0001) and hospitalization (24.5% vs. 14.2%, p = 0.0001).
Conclusion:The prevalence of high-risk individuals on a scale HeartSCORE in Ryazan region was 19.3%. Significant impact on the risk is the presence of hypertension and dyslipidemia. Persons at high risk on a scale HeartSCORE had more adverse biochemical profile and more likely to seek medical care.
P685
Gender specific differences in cardiovascular risk and their impact on left ventricular ECG parameters in primary prevention
M E Moellenberg1, C Berndt2, D Dellweg2, D Horstkotte1, KP Mellwig1
1Department of Cardiology, Heart and Diabetes Center North Rhine-Westphalia, Ruhr University Bochum, Bad Oeynhausen, Germany
2Fachkrankenhaus Kloster Grafschaft, Department of Pulmonology, Intensive Care and Sleep Medicine, Schmallenberg, Germany
Topic: Sports cardiology
Purpose:The aim of the present study was to analyse gender specific prognostic differences of cardiovascular risk factors (CVRF) in primary prevention and their impact on left ventricular ECG parameters.
Method:In 529 basically German employees (Age 30 - 65 years, ?153;? 49 %, ?153; 51 %) common CVRF were obtained and ECG (CardioLine®) was automatically analyzed. As parameter for left ventricular alterations we used the averaged r-amplitude in I and aVL ((I+aVL)/2) (avR-Amp), which has found to be a more appropriate tool to assess early left ventricular alterations than Sokolow-Lyon index. The avR-Amp was correlated for gender regarding CVRF like age, LDL/HDL ratio, BMI, mean arterial pressure (MAD), HbA1C, trigycerides and nicotine. Furthermore, we correlated avR-Amp to PROCAM and HEART Score.
Results:Males presented a higher percentage of CVRF earlier in life than females ( table). Furthermore, there was a significant correlation of avR-Amp to the following risk factors: age (?153;?p=0.001, ?153; p<0.0001), LDL/HDL-ratio (?153;? p=0.013, ?153; p=0.0005), BMI (?153;? p<0.0001, ?153; p<0.0001), MAP (?153;? p=0.002, ?153; p<0.001), HbA1C (?153; p=0.02), triglycerides (?153;? p<0.0001, ?153; p<0.001), PROCAM-Score (?153;? p=0.002, ?153; p<0,0001) and Heart-Score (?153; p<0.0001). No correlation was found between avR-Amp and HbA1C (?153;? p=0.211), nicotine (?153;? p=0.29, ?153; p<0.430) and Heart Score (?153;? p=0.2). The Sokolow-Lyon index neither correlated to the CVRF mentioned above nor to the PROCAM and HeartScore.
Conclusion:The averaged r-amplitude seems to be an appropriate ECG parameter to evaluate cardiovascular risk in primary prevention. Due to the absence of threshold values for this approach only dynamic changes in the course may allow an evaluation.
LDL/HDL > 3
BMI>30 kg/m²
MAD > 107 mmHg
HbA1C > 6.5%
Triclycerides > 150 mg/dl
Nicotine
PROCAM Score > 10%
Heart Score > 3%
females
8%
8%
18%
0.4%
23%
29%
1.2%
2.3%
males
73%
17%
27%
3.4%
55%
36%
14.2%
20%
P686
Epicardial adipose tissue and cardiac simpathetic derangement in heart failure patients
V Parisi1, T Pellegrino2, G Pagano1, A Bevilacqua1, G Ferro1, G Rengo1, D Leosco1, A Cuocolo2, P Perrone Filardi2, N Ferrara1
1University of Naples Federico II, Department of Translational Medical Sciences , Naples, Italy
2Federico II University of Naples, Advanced Biomedical Science, Naples, Italy
Topic: Sports cardiology
Purpose:Adrenergic overactivity represents an hallmark of heart failure (HF). It induces cardiac beta-adrenergic receptor dysfunction and sympathetic myocardial denervation. Epicardial adipose tissue (EAT) is a local source of hormones, cytokines, and vasoactive substances. EAT increase is associated with adrenergic overactivity and with sympathovagal imbalance, detected by heart rate variability. In the present study, we aimed to evaluate in HF patients the relationship between EAT thickness and cardiac sympathetic nerve derangement assessed by 123I-metaiodobenzylguanidine (123I-MIBG).
Methods:N.110 patients (mean age 64.74±10.50 yrs) with systolic HF (mean ejection fraction, 38.1±9.3) underwent echocardiographic evaluation of EAT thickness and 123I-MIBG planar [early heart to mediastinum ratio (H/M) and late H/M] and SPECT imaging [total defect score (TDS)]. EAT was also measured in n. 27 controls matched for age, gender, and BMI.
Results:EAT thickness was increased compared to controls (8.6±2.55 mm vs 5.57±1.16 mm; p<0.001). EAT thickness significantly correlated with early H/M (r= -0.3; p<0.001) and late H/M (r= -0.3; p<0.001), and TDS (r=0.7; p<0.001). At multivariate analysis, EAT and left ventricular ejection fraction (LVEF) were both predictors of TDS and late H/M, while EAT was the only predictor of early H/M. We also evaluated the additional predictive value of EAT on 123I-MIBG parameters utilizing a model of increasing global chi-square (Figure 1, Model 1 includes age, sex, NYHA, ischemic etiology, diabetes, hypertension, dyslipidemia).
Conclusions:The present study indicate that EAT thickness is increased in HF, shows a strong correlation with cardiac sympathetic derangement, and improves the predictive value on MIBG parameters when added to clinical variables and LVEF.
P689
Gender inequality in a population presenting with suspected paroxysmal atrial fibrillation and potential impact on diagnosis
PJ Howlett1, M Mahmoudi1, J Morritt2, L Greswell2, R Jabr1, CH Fry3, EW Leatham2
1University of Surrey, Faculty of Health and Medical Sciences, Guildford, United Kingdom
2Royal Surrey County Hospital, Cardiology , Guildford, United Kingdom
3University of Bristol, Bristol, United Kingdom
Topic: Sports cardiology
Purpose:Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia. Paroxysmal AF (PAF) comprises approximately half of AF cases and poses an equivalent risk of thromboembolism compared to other AF sub-types. It is well established that AF is more common in males than females. In spite of this, it is also recognised that men access healthcare service less readily than women. We aim to determine whether gender difference impacts on attendance and ultimately diagnosis of PAF in an arrhythmia screening clinic.
Methods:Patients attending the clinic and meeting the following criteria were recruited: suspected PAF (defined as palpitations or detection of an irregular pulse); aged 40 years and over; no previously documented atrial arrhythmia; sinus rhythm confirmed with a 12-lead ECG; no significant electrolyte disturbance. Participants were issued with an automated cardiac event recorder for 1-week, deemed standard practice (R Test Evolution 4, Novacor). They also used a handheld ECG monitor (OMRON Portable ECG Monitor HCG-801), recording 30-second segments twice-daily and with relevant symptoms, for a 12-week period. Recordings were analysed by a blinded cardiologist.
Results:177 patients attended the clinic, 120 of whom were female (68%). 134 (75%) participants were subsequently recruited with a mean age of 66 years. A significant majority of participants were female (n=91, 68%; p = 0.004, Fisher's). 83% were referred with palpitations and 17% with detection of an irregular pulse. 90% of participants completed the study and 99% of recordings were suitable for analysis. Atrial arrhythmias were identified in 32 patients (24%). Of these cases, 26 were diagnosed with PAF, 5 with atrial flutter and 1 with atrial tachycardia. A higher proportion of atrial arrhythmias were diagnosed in women than men (n=21, 66%; p = 0.3).
Conclusions:Significantly less men present to a screening clinic for PAF than would be expected statistically and, as a likely consequence, a reduced rate of detection is observed in this gender. Future health campaigns to promote awareness of AF should target the male population.
P690
Gender does not determine prognostic differences in a cohort with chronic ischemic heart disease, data from long-term follow-up of the BARIHD study
O Rego Ojea1, M Otero Mata1, A Lado Llerena1, R Besada Gesto1, M Sanchez Loureiro1, I Pazos Del Olmo1, C Caneda Villar1, R C Vidal Perez1, F Otero-Ravina1, JR Gonzalez-Juanatey1
1University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
Topic: Sports cardiology
Purpose:The outcome differences in the chronic phase of coronary artery disease (CAD) by gender are controversial. We assessed the influence of gender on long-term prognosis in a cohort with chronic ischemic heart disease (CIHD) followed by primary care physicians (PCP).
Methods:BARIHD was a cross-sectional multicentric study made with the collaboration of 73 PCP. The PCP included during February 2007,patients(p) that fulfil the inclusion criteria: coronary artery disease (CAD) with at least 1 year of follow up since diagnosis, diagnosis clear established (stable angina-SA, unstable angina-UA or myocardial infarction-MI) in a discharge summary from cardiology department. Follow-up was done by clinical review or telephone contact and death or CV events were recorded, as well as the cause of death.
Results:1038p with a complete follow up after a median follow up of 2304 [2-2612]days. 73% (758p)male sex, first diagnosis of CAD: male vs. female SA (21 vs.29.3%,p<0.001), UA (19.3 vs.27.9%,p<0.001) and MI (59.8 vs. 42.9%,p<0,001), time of evolution after the 1st diagnosis was higher in male 8.2±6.3 vs. 6.9±5.2 years. Women were older (mean age 72.4±10.5) and had a worse risk profile, with more hypertension (78.9%), diabetes (34.6%).There were no differences in dyslipidaemia, atrial fibrillation, stroke or prior heart failure, but women had less COPD and more valvular and kidney disease (glormerular filtration<60 defined by MDRD). Less coronariography were performed in women (78.9%vs.67.9%). There was no difference in medical treatment. Outcome by gender without differences (table) Conclusions:Gender was not related with differences in the long-term prognosis for patients with CIHD
CV: Cardiovascular
Mortality (%)
CV Mortality (%)
CV admissions (%)
CV Death and/or CV admissions(%)
Men (n=758)
194 (25.6)
103 (13,6)
294 (38,8)
317 (41,8)
Women (n=280)
66 (23.6)
39 (13,9)
100 (35,7)
111 (39,6)
P691
Educational level and risk profile and risk control in patients with established coronary heart disease
J Bruthans1, O Mayer2, D De Bacquer3, D De Smedt4, ? Reiner5, K Kotseva6, R Cifkova1
1First Faculty of Medicine, Charles University and Thomayer Hospital, Center for Cardiovascular Prevention, Prague, Czech Republic
2Faculty of Medicine Pilsen, Charles University, Czech Republic, 2nd Department of Internal Medicine, Pilsen, Czech Republic
3University Hospital , Department of Public Health , Ghent, Belgium
4Ghent University , Department of Public Health , Ghent, Belgium
5University Hospital Center, University Zagreb, Department of Internal Medicine, Zagreb, Croatia
6National Heart and Lung Institute, Imperial College , International Centre for Circulatory Health, London, United Kingdom
Objective:To ascertain in which way conventional risk factors, compliance with recommended risk factor control and medication, and the effect of medication were associated with education in patients with established coronary heart disease (CHD).
Methods:The EUROASPIRE IV study was a cross-sectional survey undertaken 2012-2013 in 24 European countries to ascertain how recommendations on secondary CHD prevention are being followed in clinical practice. Consecutive patients, men and women <80 years of age who had been hospitalized for an acute coronary syndrome or revascularization procedures, were identified retrospectively. Data were collected through an interview with examinations at least six months after hospitalization.
Results:A total of 7937 patients (1934 women) were evaluated. Patients with primary education were older, with a larger proportion of women. In women only, body mass index, waist circumference, systolic and diastolic blood pressure, fasting triglycerides, and fasting glucose were negatively associated with educational level. The control of risk factors, as defined by JES 4 and JES 5 guidelines, was significantly better with higher education for current smoking (p=0.001), overweight and obesity (p=0.047 and p=0.029 respectively), low physical activity (p<0.001) and low HDL-cholesterol (p=0.011) in men, and for obesity (p=0.005), low physical activity (p=0.001), low HDL-cholesterol (p=0.023), diabetes (p<0.001) and high blood pressure (p=0.001) in women. Taking high education as reference, a significantly higher risk was observed in men for overweight (OR 1.22 and 1.29 for secondary and primary education), smoking (OR 1.30 and 1.55), low HDL (OR 1.33 for primary education) and low physical activity (OR 1.72 for primary education) and in women for overweight (OR 1.50 for primary education), obesity (OR 1.74 for primary education), diabetes (OR 1.53 and 2.22, for secondary and primary education, respectively), high blood pressure (OR 1.36 and 2.06), low HDL (OR 1.6 for primary education) and low physical activity (OR 1.88 and 2.75). The patients with primary and secondary education were more often treated with diuretic and antidiabetic drugs (p=0.014 and p=0.020 respectively). Compared to the previous EUROASPIRE II report (1999-2000), the differences in cardiovascular risk factors prevalence and control according to educational level remained similar.
Conclusions:Particular risk communication and control are needed in secondary CHD prevention for patients with lower educational status. This substudy was supported by IGA, Ministry of Health, Czech Republic, grant No NT/13186
P692
The association between perceived ethnic discrimination and the components of the metabolic syndrome across ethnic minority groups
MUZ Ikram1, MB Snijder1, CO Agyemang1, CO Agyemang1, AH Schene2, K Stronks1, RJG Peters3, AE Kunst1
1Academic Medical Center of Amsterdam, Department of Public Health, Amsterdam, Netherlands
2Radboud University Medical Centre, Department of Psychiatry, Nijmegen, Netherlands
3Academic Medical Center of Amsterdam, Department of Cardiology, Amsterdam, Netherlands
Topic: Sports cardiology
Purpose:To investigate whether perceived ethnic discrimination (PED) is associated with metabolic syndrome and its individual components across ethnic minority groups, and to assess the contribution of PED to the metabolic syndrome.
Methods:Cross-sectional data from the HEalthy Living In an Urban Setting (HELIUS) study were collected from January 2011 until July 2014, including 2186 South-Asian Surinamese, 2059 African Surinamese, 1685 Ghanaians, 2162 Turks, and 2117 Moroccans aged 18-70 years living in Amsterdam, the Netherlands. PED was measured using the Everyday Discrimination Scale. Metabolic syndrome was defined according to the harmonised definition. Analyses were done with logistic regression, adjusted for potential confounders (demographics, education and other psychosocial stressors) and mediators (health behaviours and depression). Population attributable fractions (PAF) were used to calculate the contribution of PED to metabolic syndrome.
Results:PED was significantly positively associated with metabolic syndrome in the total sample (odds ratio 1.06; 95% confidence interval 1.00-1.13), South-Asian Surinamese (1.12; 0.98-1.28), African Surinamese (1.15; 1.00-1.32), and Moroccans (1.19; 1.03-1.37). In these groups, PED overall tended to have positive associations with all individual components of metabolic syndrome. The PAFs were 5% in South-Asian Surinamese and Moroccans, and 7% in African Surinamese.
Conclusion:PED contributes to metabolic syndrome and has positive associations with the individual components of metabolic syndrome in some ethnic minority group. Public health policies should explicitly focus on ethnic discrimination to improve cardiovascular health of ethnic minority groups.
P694
Contribution of cardiac electrophysiologic testing for etiologic ischemic stroke of undetermined causes in young adults
MB Bouame1, A Mekarnia1, MT Bouafia1
1Central Hospital of the Army, Algiers, Algeria
Introduction:Despite the recently described new syndromes, about a third of ischemic stroke (AIC) in young adults remains unexplained. The works, Attuel, Four Ducrocq and suggest the cause of ischemic stroke (AIC) unexplained young adults, the role of atrial vulnerability (VA), substratum of paroxysmal atrial fibrillation (PAF) we studied prospectively in 121 patients.
Patients-Methods:Patients 17 to 55 victims admitted to AIC services Neurology and Internal Medicine, are subject to a systematic review referred to etiological. An electrophysiological study was performed ear in case of unknown aetiology in patients consenting, as described by Attuel, within 90 days after the AIC. In addition to the usual parameters were measured conduction time intra atrial refractory periods, latent vulnerability index, prior to the completion of atrial stimulation Programmed:In this study, the vulnerability has been refined over the outbreak of supra ventricular arrhythmia (FA, Flutter, TA) sustained (> 1 min), or other supra ventricular rhythm disorder in the presence of minors disturbed settings. Clinical, neuroimaging and embolic recurrence were compared by chi 2 test or Fischer, according to the presence or absence of atrial vulnerability.
results:Of 121 patients, mean age 40.89 years, Sex ratio 1.63, 53 (43.8%) had a positive atrial vulnerability in the form of time and FA 22 10 flutter and atrial tachycardia times 9 times. There is no evidence of significant difference in the type and location of the AIC, with a significant difference against tobacco (risk = 2.4), birth control pills (risk = 3.6), the presence> 70 ESA on holter ECG (risk = 3.7) and septal defects (PFO and / or ASIA with a risk = 2.89). On a mean follow up of 06 months, 12 patients presented with cerebral embolic recurrence in the 10 + VA group and 02 patients in the VA-group, as predictors multi analysis varied VA inducible and pathological holter Conclusion:With a sensitivity of 83% and a specificity of 61% and a negative predictive value of 97%; The presence of inducible atrial vulnerability with a pathological ECG Holter (ESA) exposed to a high risk of recurrence and embolic requiring anti-arrhythmic therapy and discussion of anticoagulant treatment.
P695
The role of Holter monitoring in the examination of young elite athletes
L Makarov1, V Komoliatova1, I Kiseleva1, N Fedina1, D Bessportochny1
1Center for Syncope and Cardiac arrhythmia in children and adolescents of FMBA of Russia. DKB # 38, Moscow., Russian Federation
Athletes are special professional group with regular increased stress of the cardiovascular system and accordingly the risk of cardiac complications, the most serious of which is Sudden Cardiac Death (SCD). Holter monitoring (HM) one of the first informative method for detection of the cardiac pathology. Few studies are devoted to daily heart rhythm in athletes. Aim of the study was reveal role of HM in examination of the young elite athletes.
Methods:HM (MARS, GE Healthcare, USA) were performed in 86 from 500 young elite athletes, members of national teams 12 - 18 years old. Indication for HM were arrhythmias, syncope, QT prolongation, family history sudden death and other abnormalities during prescreening examination before competition. We excluded cardiomyopathy and other structure and organic diseases of the heart.
Results:Were revealed ABV block 1- 3 degree in 13 – 15% (one hockey player had one episode asymptomatic AVB III at night period with pause 7789 mc. Supravenricular extrasystolies were detected in all athletes from single till 20000, ventricular arrhythmias were revealed in 13 athletes (15%). One athlete with VT had 3 transient major criteria of the ARVC/ARDV (epsilon wave, negative T in the right precordial leads, VT). Maximum prolongation of the QT interval were detected at the second part of the night and not exceed 530 ms (normal value less than 480 ms). HM informative in examination of elite young athletes. Possibly it would be useful to use HM more actively for routine screening at young elite athletes.
P696
Effect of hemoglobin concentration on left ventricular mass in healthy adolescent athletes
H Krysztofiak1, A Folga2
1Mossakowski Medical Research Centre, Warsaw, Poland
2National Center of Sports Medicine, Warsaw, Poland
According to the Fick's law, concentration of hemoglobin affects the arterio-venous difference and consequently the oxygen uptake. Lower concentrations of hemoglobin ([Hb]) in women than in men, seem to be responsible for their lower than in men maximal oxygen uptake during exercise. Reduced [Hb] causes a compensatory cardiovascular response and can induce cardiac growth. However, there is little information about the relationship between hemoglobin concentration and left ventricular mass in young people without heart disease. The aim of this retrospective, cross-sectional study, was to evaluate the influence of hemoglobin concentration on the cardiac growth in adolescent athletes. In particular, in relation to sex. Healthy athletes, 69 boys (B) and 19 girls (G), age range 9-19, practicing different sports, who underwent echocardiography and laboratory tests with determination of [Hb], during pre-participation examination in sports medicine center, were included in this study. The groups B and G were of a similar age (13,5±2,8 vs. 13,6±2,8 yrs; p=0,95). Left ventricular mass (LVM), indexed to body surface area (LVM/BSA) and to height raised to an exponential power of 2,7 (LVM/H2,7) were calculated. Analysis of correlation of LVM indexes with [Hb] were performed in both groups. Unpaired t-tests were performed to compare the value of indexes below and above median for [Hb] within both groups. The [Hb] was significantly lower in G vs. B (13,2±0,7 vs. 14,1±1,2 g/dL; p<0,005). It was high, significant, negative correlation of LVM/H2,7 with [Hb] (r2=0,43; p<0,005) and intermediate, significant, negative correlation of LVM/BSA with [Hb] (r2=0,31; p<0,05) in girls group (G). There were no correlation of LVM indexes with [Hb] in boys (B). In comparison of value of the LVM indexes below and above the median for [Hb] within groups, the both LVM indexes were significantly higher below the median (n=10) vs. above the median (n=9) in group G (LVM/H2,7: 31,5±3,2 vs. 27,7±3,0 g/m(2,7), respectively; p<0,05 and LVM/BSA: 73,7±5,9 vs 66,3±8,4 g/m2, respectively; p<0,05). There were no age difference in the below vs. the above the median sub-group in G (13,7±3,3 vs. 13,4±2,4 yrs, respectively; p=0,85). In boys, there were no differences of LVM indexes, in the sub-groups relative to their median for [Hb]. Hemoglobin concentration seems to be an important factor in cardiac growth, especially in female athletes. The lower concentrations of hemoglobin correspond to the higher LVM indexes. This effect can be explained by referring to Fick's law. However, why this effect was not observed in male subjects requires further study.
P697
Cardiac adaptation in elite cyclists; overlap with disease phenotypes.
T Keteepe-Arachi1, A Malhotra1, G Mellor1, H Dhutia1, L Miller1, R Narain1, K Prakash1, V Gabus1, M Papadakis1, S Sharma1
1St George's University of London, St Geor, London, United Kingdom
Topic: Sports cardiology
Purpose:Regular, intensive exercise results in structural cardiac adaptations that in extremes may mimic cardiac pathology. The type of exercise affects the degree to which these adaptations occur. The aim of this study was to examine differences in cardiac adaptation between elite endurance cyclists and elite non-endurance athletes.
Methods:Between 2009 and 2013, 39 elite endurance cyclists underwent 12-lead ECG and echocardiography as part of pre-participation screening. They were compared to 39 age, sex and ethnicity-matched elite athletes from a variety of non-endurance disciplines including football, rugby and cricket.
Results:The cyclists exhibited significantly greater measurements of all echocardiographic parameters with the exception of ejection fraction (EF), compared to non-endurance counterparts (Table). Extremes of left atrial diameter (>45mm) were noted in 10% (n=4) cyclists. Left ventricular cavity dimensions (LVEDd) considered to overlap with dilated cardiomyopathy (DCM) (>60mm) were identified in 33% (n=13) of cyclists. Left ventricular hypertrophy (>12 mm) was present in 31% (n=12) of cyclists but none exceeded a maximal wall thickness of 14mm. No cyclist exhibited an EF <50%.
Conclusions:Our data confirms that endurance athletes exhibit more pronounced cardiac adaptation compared to non-endurance counterparts. A significant proportion exhibits LVEDd that overlaps with DCM making differentiation between physiology and pathology challenging in endurance athletes with ECG anomalies or symptoms.
Echocardiographic parameter
Endurance Athletes (Cyclists) Mean Values (standard deviation)
Range (mm)
Non-Endurance Athletes Mean Values (standard deviation)
Range (mm)
p value
LA diameter (mm)
40 (±3.2)
34-51
35 (±3.5)
27-42
<0.001
Ao diameter (mm)
35 (±3.2)
30-42
31 (±3.6)
22-39
<0.001
LVEDd (mm)
59 (±3.9)
53-74
54 (±3.4)
47-63
<0.001
IVS thickness (mm)
11 (±1.0)
9-13
9 (±1.2)
7-11
<0.001
PW thickness (mm)
10 (±0.8)
9-14
9 (±1.1)
7-11
<0.001
EF (%)
62 (±6.1)
50-73
52 (±9.1)
39-76
NS
P698
Right ventricular structure and function in senior and scholar elite footballers
D Oxborough1, E Popple1, J Somauroo1, S Sharma2, V Utomi1, R Lord1, R Cooper3, J Forster4, K George1
1Liverpool John Moores University, Sports and Exercise Science, Liverpool, United Kingdom
2St George's University of London, Cardiology, London, United Kingdom
3Liverpool Heart and Chest Hospital, Liverpool, United Kingdom
4Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom
Topic: Sports cardiology
Purpose:To determine whether the extent of RV structural and functional adaptation is mediated by age in professional footballers.
Methods:We recruited 20 senior and 20 scholar professional footballers at three Premier League Clubs. All players underwent 2D, Doppler, tissue Doppler and strain (e) echocardiography with a focused assessment on the right heart. A range of structural and functional indices were derived and indexed allometrically where appropriate. Peak RV e, strain rate (SR) and time to peak e and SR were also calculated. All data were compared between groups as well as against normal values.
Results:Allometrically scaled RVOTplax was significantly larger in the senior compared to the scholar players (25.5 ± 2.2 mm[m]0.31 and 23.2 ± 3.6 mm[m2]0.31, P = 0.02). Individual and absolute values for the RV outflow tract measured in a parasternal long axis orientation (RVOTplax) and the basal inflow (RVD1) were often above the normal range cut-offs (40% and 20 % for RVOTplax (see figure) and 50 % and 25 % for RVD1 in senior and scholar players respectively). All functional parameters were within normal limits, however systolic SR (SRS) was lower in the senior players compared to scholar players (-1.4 ± 0.30 l/s and -1.3 ± 0.16 l/s, p = 0.015 respectively) with a moderate correlation to indexed RVOTplax (r = 0.314).
Conclusions:Some degree of RV structural adaptation occurs in both senior and scholar football players, with senior players having significantly larger RVOTplax dimensions. Although senior players have slightly lower peak SRS than scholar players, all global e and SR are within normal ranges.
P699
Screening in female athletes: The outcomes of the largest mandatory pre-participation screening programme for women in the UK.
A Malhotra1, L Robinson1, S Cheadle2, A Sood1, J Ariyaratnam1, R Birt1, R Mehta2, M Papadakis1, I Beasley2, S Sharma1
1St George's University of London, Cardiac and Vascular Sciences Research Centre, London, United Kingdom
2The Football Association, Medical Department, Wembley Stadium, London, United Kingdom
Topic: Sports cardiology
Purpose:Women are participating in greater numbers at the highest levels of sport. The Football Association (FA) runs the largest, mandatory pre-participation screening (PPS) programme for female athletes in the UK. With a health questionnaire, 12-lead electrocardiogram (ECG) and echocardiogram (echo), the programme strives to identify athletes with an underlying cardiac condition that increases their risk of sudden cardiac death (SCD) with exercise. The aim of this study was to evaluate the outcomes of this unique process for female athletes.
Methods:Between June 2009-May 2014, 426 female footballers were screened at national team selection. Each player completed a screening questionnaire and underwent an ECG and echo that was reviewed independently by 2 cardiologists. All abnormal cases were further evaluated comprehensively at a dedicated sports cardiology clinic.
Results:The footballers were aged 17.8±2.4 years with a follow-up period of 3.8 years. 402 players (94.4%) were cleared to participate after initial screening. 24 (5.6%) required further evaluation. An abnormal ECG accounted for half of referrals for further evaluation, while an abnormal echo accounted for the other half. A cardiac condition was identified in 13 (3.1%) players (Table 1). 1 player was advised not to continue playing football. Of the remaining 11 in whom a condition was not identified, 9 were discharged and 2 kept under annual surveillance.
Conclusions:Although The FA's cardiac PPS programme is effective at identifying pathology in elite female footballers, our data suggest that the majority of these were detected by echo, consisting largely of minor valvular pathologies though a bicuspid aortic valve was found in 2 players . While no condition was diagnosed in those with ECG repolarisation anomalies, only one serious case was identified by ECG for which disqualification was advised. Further refinement of the process is required to reduce the false positive burden of ECG screening in female athletes.
Yearly review All clear Yearly review Yearly review
Repolarisation (10)
T wave inversion V1-V3 (x7) T wave inversion V1-V5 (x3)
Yearly review Yearly review
Structural (4)
Trabeculated left/ right ventricle Atrial septal defect (x3)
All clear All clear
Electrical (2)
Long QT (borderline) Long QT Syndrome
Yearly review Advised not to participate
P700
Myocardial contractility dynamics of the LV during staged maximal exercise testing in adolescent elite footballers as measured by 2-D strain echocardiography
G E Pieles1, L V Gowing2, A G Stuart3, C A Williams2
1Bristol Heart Institute, NIHR Cardiovascular Biomedical Research Unit, Bristol, United Kingdom
2Sport and Health Sciences, University of Exeter, Exeter, United Kingdom
3Bristol Royal Infirmary, Bristol Congenital Heart Centre, Bristol, United Kingdom
Topic: Sports cardiology
Purpose:Cardio-pulmonary exercise testing (CPET) is a recommended secondary screening tool in youth athletes but cannot assess cardiac function. Left ventricular (LV) training adaptation in youth athletes has so far only been reported at rest and no data exists describing myocardial dynamics during exercise. We have performed CPET with simultaneous echocardiography using 2-D speckle-tracking-echocardiography to describe LV contractility response.
Methods:14 male professional football academy players (mean age 15.4±.8y; stature 176.9±8.4cm; body mass 64±8.5kg) underwent echocardiography at rest, during exercise and recovery (rec) while completing an incremental CPET on a recumbent cycle ergometer (25W?153;3min increments). Echocardiography at rest was performed following Football Association screening guidelines. LV contractility was serially assessed during exercise and recovery measuring longitudinal (LS) and circumferential (CS) systolic 2-D strain.
Results:End-diastolic LV (LVWT) and septal (VS) wall thickness and LV end-diastolic diameter (LVEDD) were as follows: LVWT 10.1±1.4 (8.1–12.6)mm; VS 9.8±1.5 (7.8–12)mm; LVEDD 46.9±3.9 (42-55)mm. Systolic and diastolic function at rest were normal. Athletes achieved a peak oxygen uptake (VO2peak) of 51.7±6.2 ml/min/kg and a max work rate of 203±25W, HRpeak exercise was 177.9±7.9bpm. LS and CS showed a linear relationship with significant differences across increasing work rates compared to rest and recovery. LV LS and CS increased significantly from rest to peak exercise (p<0.01) with significant moderate Pearson's correlations between LSrest and LSpeak (r=0.64, p=0.01) and CSrest and CSpeak (r=0.7, p=0.01). There was significant moderate correlation between LSpeak and LSrec (r=0.57, p=0.04) and CSpeak and CSrec (r=0.56, p=0.04). LSpeak significantly correlated to HRmax (r=0.59, p=0.03). A positive, yet non-significant correlation existed between LSpeak and work-rate (r=0.45, p>0.05). Weak and non-significant correlations were found between LSpeak and VO2max, LSpeak and work-rate and LVPWd with LSpeak and CSpeak (r=-0.2–0.4, p>0.05) but not between LVEDD and LSpeak or CSpeak.
Conclusion:LV longitudinal and circumferential systolic motion both contribute to the linear contractility response to maximal CPET in adolescent elite footballers. LV resting contractility but not LV diameters correlate to exercise contractility in this cohort. CS and LS during exercise and recovery might allow differentiation between physiological and pathological cardiac exercise response in athletes with borderline or abnormal resting echocardiographic parameters.
P702
Dynamics of echocardiographic and electrocardiographic findings in child and adolescent athletes
T Svanishvili1, E Tataradze1, N Chabashvili1, Z Sopromadze1, M Sopromadze1, L Malania2, E Chumburidze2, Z Kakhabrishvili1
1Tbilisi State Medical University, Tbilisi, Georgia, Republic of
2LTD "City Sport" medical-diagnostic center, Tbilisi, Georgia, Republic of
Topic: Sports cardiology
Purpose:The purpose of our study was to observe dynamics of electrocardiographic (ECG) and echocardiographic findings among child and adolescent athletes, considering there is a limited amount of data available concerning this subject in medical literature.
Methods:We observed 140 male athletes aged 6 to 13 years, who underwent regular semi-annual pre-participation screening during several years, using ECG and echocardiography. 16 children and adolescents were evaluated for four consequent years, 50 - for three years, 54 - for two years and 30 - for one year. Control group was made up of 44 healthy non-athletes of the same age range.
Results:Among the athletes, a distinct trend was noted towards increase of heart dimensions during the observational period, namely there was a linear increase of mean values of thickness of interventricular septum, thickness of posterior wall of the left ventricle and left ventricular end-diastolic volume, from 5.85 mm to 7.60 mm, from 6.07 mm to 8.20 mm and from 36.13 ml to 38.30 ml, respectively. While the rate of growth of three above-mentioned parameters was somewhat slower in the control group, the difference was not statistically significant (5.83 to 7.20 mm; 5.70 o 7.60 mm and 36.00 to 38.06 ml, respectively). When comparing the athletes of the same age categories, we could not find a significant difference in heart sizes with respect to duration of engagement in sports activities; as an example, mean thickness of interventricular septum among 13-year old boys with 2-year experience of sports participation was 7.21 mm, while the same value in athletes with 4-year experience was 7.75 mm, but the difference was not statistically significant. It is noteworthy that mild degree of mitral valve regurgitation (MVR) was found in 32% of athletes, as compared to only 15% in the control group. As for ECG changes, incomplete right bundle branch block (RBBB) was found in 34% of athletes and 18% of non-athletes (statistically significant difference).
Conclusion:Based on our study results we can conclude that significant myocardial hypertrophy does not occur in athletes aged up to 13 years and the rate of growth of heart dimensions does not exceed the rate in non-athletes of the same age; besides, in this age group, heart sizes do not correlate with duration of sports participation. No significant ECG changes can be observed. Increased prevalence of MVR in athletes is notable and requires further investigation.