Cardiac rehabilitation (CR) in octogenarians after transcatheter aortic valve implantation (TAVI) or surgical aortic valve replacement (AVR) for aortic stenosis: safety, performance and outcome
F Tarro Genta1, E Eleuteri2, F Bertolin1, Z Bouslenko1, C Taglieri1, M Tidu1, P Giannuzzi2
1Salvatore Maugeri Foundation, IRCCS, Division of Cardiac Rehabilitation, Turin, Italy
2Salvatore Maugeri Foundation, IRCCS, Division of Cardiology Rehabilitation, Veruno, Italy
Topic: Sports cardiology
Purpose:to compare safety, performance and outcome of octogenarians attending residential CR after TAVI or AVR with biological prosthesis.
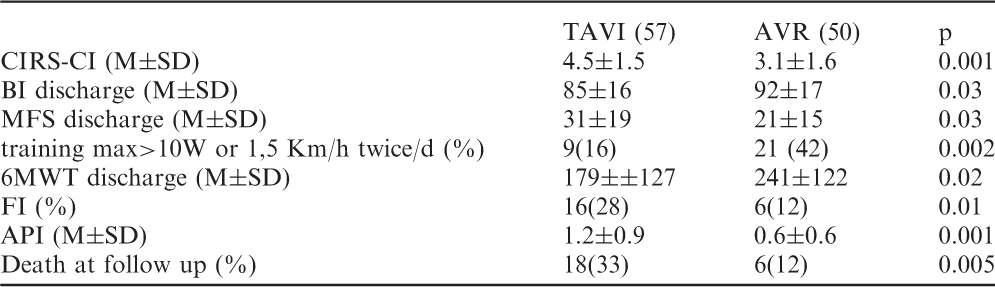
Methods:from January 2010 to April 2013 57 consecutive TAVI (28% male, age 85±3, 25 Edwards, 32 CoreValve) and 50 consecutive AVR (42% male, age 82±2 ) aged =80 years were admitted to a 3-week CR training program (walking, up to 30 minutes of cycling or treadmill session twice daily, respiratory training). Co-morbidity (cumulative illness rated state-comorbility index) (CIRS-CI) score, Echocardiography on admission, Disability (Barthel Index) (BI), Morse Fall Scale score (MFS), Six minute walking test distance (6MWT) on admission and at discharge were assessed; a frail index (FI) at discharge was defined as the presence of at least two of the following: 6MWT <200m, BI <75, MFS=50.
Results:Compared to AVR, TAVI were older, more frequently female, had higher CIRS-CI and higher degree of aortic prosthetic insufficiency (API) on 0-3 scale . TAVI as AVR could attend safely CR training; nevertheless TAVI could tolerate a significantly lower workload with lower performance at 6MWT at discharge compared to AVR even if 6MWT gain was similar in both groups. Disability, MFS and FI were higher in TAVI at discharge even if they had significant disability improvement during CR At follow up (range 12-36 months) death occurrence was significantly higher in TAVI (p=0.01) (Table).
Conclusion:In octogenarians after TAVI o AVR CR is safe favoring disability recovering and safe discharge at home. Nevertheless TAVI can tolerate reduced training workloads maintaining at discharge a higher fragile profile which influence survival at late follow up compared to AVR.
TAVI (57)
AVR (50)
p
CIRS-CI (M±SD)
4.5±1.5
3.1±1.6
0.001
BI discharge (M±SD)
85±16
92±17
0.03
MFS discharge (M±SD)
31±19
21±15
0.03
training max>10W or 1,5 Km/h twice/d (%)
9(16)
21 (42)
0.002
6MWT discharge (M±SD)
179±±127
241±122
0.02
FI (%)
16(28)
6(12)
0.01
API (M±SD)
1.2±0.9
0.6±0.6
0.001
Death at follow up (%)
18(33)
6(12)
0.005
P751
The influence of cardiac rehabilitation on tolerance to physical loading and myocardial vascularization in patients after heart transplantation
V A Sujayeva1
1Republican Scientific and Practical Centre of Cardiology, Minsk, Belarus
Aim:to study the changes of microvasculature and tolerance to physical loading (TPL) in patients after heart transplantation (HT) with different ways of physical rehabilitation (PR) in the different times after HT. Object: 38 patients aged from 21 to 61 year (on the average 44.6±12.1 years) after HT, without cardiac transplant rejection >R1 according to ISHLT classification. In each patients were performed 3 tests: the I test was done at 15.1±8.8 days after HT, the II test – at 6.4±2.1 months after HT and the III test – at 12.0±0.6 months after HT. Each test included both endomyocardial biopsy (EMB) with calculation of the average number of vessels in the 10 fields of vision and Bicycle Spiroergometry Test (BST). The patients were randomized in 2 gropes after HT. 18 pts in the age 46.5±2.6 years were randomized to the Main Grope (MG), 20 pts in the age 47.1±2.4 years were randomized to the Control Grope (CG) (p>0.05). In the MG we used original program of PR, the physical rehabilitation in the CG performed by the routine way.
Results:The character of microvasculature according to EMB data was similar in MG and CG at I test. The average number of vessels in 10 fields of view was 69.5±17.4 in MG and 68.0±13.3 – in CG (p>0.05). In the MG and CG at II test we established opposite tendencies in the character of myocardial vascularization. In the MG the number of vessels no significant decreased from 69.5±17.4 at I test to 63.7±12.4 - at the II test (p>0.05). On the contrary in CG the number of vessels no significantly increased from 68.0±13.3 to 70.8±15.6, respectively (p>0.05). In the III test above mentioned reorganization of microvasculatury remained. The number of vessels in MG was 65.2±3.3 (less than at I test, p>0.05), in CG - 77.9±7.0 (more than at I test, p>0.05). The number of vessels in MG became significantly less than in CG (p<0.05). We studied how the number of vessels connected to TPL in patients after HT. We revealed that increasing in the number of vessels established in CG accompanied by the decreasing both in TPL and Maximal oxygen consumption (VO2 max). In contrast decreasing in the number of vessels revealed in MG accompanied by the increasing both TPL and VO2max (p<0.05).
Conclusion:Growth of myocardial vascularization after HT accompanied by the decreasing both of the tolerance to physical loading and maximal oxygen consumption. Developed program of physical rehabilitation contributed to contain the growth of vascularization and of increase of aerobic physical working capacity.
P752
Transition to home in heart failure: theres an app for that
L Houston-Feenstra1, W Dysinger1, M Kagoda1, S Chatterjee2, N Alnosayan2, A Alluhaidan2
1Loma Linda University Medical Center, Loma Linda, United States of America
2Claremont Graduate University, School of Information and Technology, Claremont, United States of America
Why do heart failure (HF) patients fail to adhere to prescribed medications/ lifestyle recommendations? Evidence suggest that lack of effective and training for patient/families challenge successful transition to home due to conflicts generated by pressure within the patient's home environment. This pilot is a multidisciplinary project, including information systems professionals, clinicians, and patients working together to develop/evaluate a customized mobile phone application (app). Using, home based monitoring of daily weights, blood pressure, heart rate, blood glucose, and a dash board of cumulative data accessed daily by clinicians. A built in algorithm identifies patients' risk for re-admission based on changes in their vital signs or self-reported symptoms defined by clinical staff as representing best practices pathways decision points. 7 patients with a clinical diagnosis of HF, with documentation of at least one HF admission in the past 14 months were recruited to trial the App. Outcome Data: HF related hospitalizations; emergency department/urgent care visits, weight, blood pressure, and Minnesota living with heart failure quality of life. 120 day data analysis: mean compliance rate for daily measurements = 68.5%. Quality of life improved 43%, 3 HF readmissions prevented, changed one admission from an acute ICU readmission into a short stay guided HF admission, accomplished by early identification of symptoms that unmanaged would have resulted in a more serious and lengthy admission. This integrated innovative system has demonstrated improved accountability and outcomes in the enrolled participants. Patient input at 120 days resulted in system revisions. New system data analysis to continue.
P753
Muscle mass change and its predictors during exercise-based cardiac rehabilitation
JM Patrick1, DW Harris2, FM Wise1
1Caulfield Hospital, Melbourne, Australia
2Caulfield Hospital, Aspex Consulting , Melbourne, Australia
Topic: Sports cardiology
Purpose:Loss of muscle mass and strength is associated with reduced functional status and can become a major health issue. While resistance exercise has been shown to improve muscle mass in the general population, there is little evidence regarding the impact of cardiac rehabilitation on muscle mass. The aim of this study was to evaluate muscle mass change in cardiac rehabilitation patients, and identify potential determinants.
Methods:A sample of 288 consecutively admitted cardiac rehabilitation outpatients (mean age: 61.9 years SD 11.3; 22.6% female) were recruited to this study. They completed the Hospital Anxiety and Depression Questionnaire, stationary bike assessment and 6 minute walk test, and were weighed using body composition scales, on admission to and discharge from a six week outpatient cardiac rehabilitation program.
Results:One hundred and thirty-four subjects (46.5% of the sample) gained muscle mass from admission to discharge, with a mean gain of 1.7kg muscle (SD 1.9). An ordinary least squares linear regression with backward elimination was conducted and revealed that change in muscle mass was predicted by a combination of initial body fat percentage, waist measurement, anxiety, depression and sex, with an adjusted R2of 29%. Initial muscle mass, initial exercise capacity and age were not predictors. There was a positive correlation between fat loss and muscle gain during rehabilitation.
Conclusion:During cardiac rehabilitation, men were more likely than women to increase muscle mass, while this change was less likely in patients who were anxious or depressed. Initially higher percentage body fat predicted better muscle mass gain; this relationship requires further investigation. While the explained variance was modest and more research into predictors of muscle mass change is warranted, this preliminary study suggests that certain patient groups (e.g. women, depressed/anxious patients) may benefit from greater assistance from staff to achieve maximum benefits from exercise-based cardiac rehabilitation, particularly resistance exercises.
P754
Heart rate plus 20 or 30: an appropriate method for prescribing exercise intensity for heart failure patients in cardiac rehabilitation?
JL Reed1, AZ Blais1, AL Pipe1, RD Reid1
1University of Ottawa Heart Institute, Prevention and Rehabilitation, Ottawa, Canada
Topic: Sports cardiology
Purpose:Patients with heart failure (HF) are a growing population within cardiac rehabilitation (CR). Guidelines recommend HF patients work at 40-60% of their heart rate reserve (HRR) for the first 3 weeks of an exercise program, and 50-80% HRR thereafter. Maximal exercise testing, the gold standard for determining individual exercise prescription, is often impractical due to costs, expertise and technological resources required. Presence of co-morbidities and varying patient characteristics further complicates exercise prescription. The purpose of this study was to compare a common, practical method of prescribing exercise intensity for in-patient CR programs, resting HR plus 20 or 30 beats per minute [RHR+20, RHR+30], to % HRR derived from maximal exercise testing in HF patients with varying functional capacities during the first 3 weeks and latter 9 weeks of a 12 week out-patient CR program.
Methods:HF patients completed a baseline maximal exercise test and had their height, body weight and waist circumference assessed. Resting and exercise HRs were measured during each (n=24) exercise session.
Results:33 patients (4 females, 29 males; mean±SD = age: 59±10 yrs; height: 172±9 cm; BMI: 29.3±4.5 kg/m2; waist circumference: 130.7±10.6 cm; VO2peak: 20.9±6.1 ml?153;kg?153;min-1) with HF (ejection fraction: 26.7±5.3%) participated in this study. During weeks 1-3 and exercise at RHR+20, 55% of patients were at less than 40% HRR, 26% were at 40-60% HRR and 19% exceeded 60% HRR. At RHR+30, 16% of patients were at less than 40% HRR, 45% were at 40-60% HRR and 39% exceeded 60% HRR. During weeks 4-12 and exercise at RHR+20, 74% of patients were at less than 50% HRR, 19% were at 50-80% HRR and 7% exceeded 80% HRR. At RHR+30, 37% of patients were at less than 50% HRR, 41% were at 50-80% HRR and 22% exceeded 80% HRR.
Conclusions:RHR+20 appears to be an ineffective method for HF patients to achieve recommended exercise intensities of 40-60% HRR or 50-80% HRR. However, RHR+30 may be more promising given the greater number of HF patients that achieved 40-60% HRR during the first 3 weeks (45% vs. 26%) and 50-80% HRR the latter 9 weeks (41% vs. 19%) of CR when compared to RHR+20. The potential for overprescribing should be monitored. Exercise intensity prescriptions based solely on HR are likely to impose variable cardiometabolic demands in HF patients, especially in those taking HR blunting medications. It may be therefore beneficial to use additional tools (e.g. Talk Test) in conjunction with RHR+30 to prescribe and monitor exercise intensity for HF patients with varying functional capacities.
P755
Erectile dysfunction in cardiac rehabilitation: response and impact on cardiac morbimortality
M Tavares Da Silva1, G Pestana1, R Pinto1, J Rodrigues1, R Godinho1, JA Rocha2, V Araujo1, F Parada2, MJ Maciel1
1Sao Joao Hospital, Cardiology, Porto, Portugal
2Sao Joao Hospital, Physical Medicine and Rehabilitation, Porto, Portugal
Topic: Sports cardiology
Purpose:Erectile dysfunction (ED) is a strong predictor of coronary heart disease (CHD). ED and CHD have common risk factors, such as age, diabetes, dyslipidaemia, hypertension and smoking. In fact, ED severity correlates with the severity of heart disease. Participation in a cardiac rehabilitation program (CRP) after an acute coronary syndrome (ACS) has been shown to exert beneficial effects on risk factor profile and future cardiovascular morbidity and mortality. The aim of this study was to evaluate the effect of a CRP in the severity of ED in patients who suffered an ACS and to predict the cardiovascular outcome in these patients.
Methods:The study included 320 male patients consecutively referred to a CRP after an ACS. Erectile function was assessed using the International Index of Erectile Function. ED was classified according to the severity: >21: absence or mild ED; 12-21: mild to moderate ED; <12: moderate or severe ED in order to evaluate its prognostic impact. Morbidity and mortality data were obtained from hospital records, remote internet-access to primary care and other institution's records using a nation-wide health data platform. ED severity was compared before and after conclusion of the CRP using Wilcoxon signed-rank test. The composite endpoint included cases of all cause mortality, new hospital admission for ACS, stroke or heart failure and/or revascularization procedures. Prognostic significance of ED severity was evaluated using cox-proportional hazards model.
Results:Patients' mean age was 54.0±9.5 years. There were 124 (38.8%) patients with no ED or only mild ED, 135 (42.2%) patients with mild to moderate ED and 61 (19.0%) patients with moderate to severe ED. We found no difference in the severity of ED before [P50(P25-P75):20(14-23) and after [19 (14-23)] the participation in the CRP (p=0.98). In a mean follow-up of 28.9±16.8 months, a total of 26 (8.1%) events were identified: 16 (5%) admissions for ACS, 18 (5,6%) revascularizations, 2 (0.6%) admissions for stroke, 1 (0.3%) admission for heart failure and 2 (0.6%) deaths. Events were more common in patients with moderate to severe ED compared with the other two groups, with double the risk compared to those with mild to moderate ED, even adjusted for age, diabetes, hypertension, previous CHD, and ?blocker therapy (p=0.02).
Conclusions:Despite the well-known effects of a CRP after an ACS, participation in a PRC is not associated with an improvement in ED. The severity of ED might be a marker for more advanced cardiovascular disease and higher risk for subsequent fatal and non-fatal cardiovascular events.
P756
Alterations in erythrocyte internal components induced by cardiac rehabilitation
K Gwozdzinski1, A Pieniazek2, J Czepas1, J Brzeszczynska1, A Jegier3, L Pawlicki4, R Irzmanski4
1University of Lodz, Department of Molecular Biophysics, Lodz, Poland
2University of Lodz, Department of Thermobiology, Lodz, Poland
3Medical University of Lodz, Department of Preventive Medicine, Lodz, Poland
4Medical University of Lodz, Department of Internal Medicine, Lodz, Poland
Topic: Sports cardiology
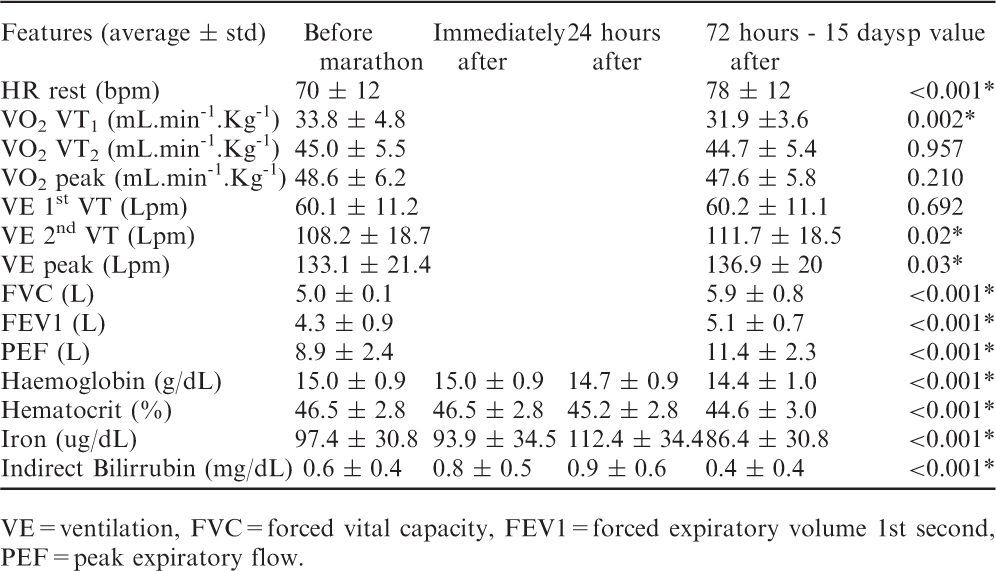
Purpose:Cardiac rehabilitation (CR) is recommended to patients with ischaemic heart disease (IHD). CR may be effective owing to its main factor, i.e. physical activity. Exercise affects the human body due to induction of moderate oxidative stress and related changes. We employed a physical exhaustion cycling test to examine the properties of internal components of erythrocytes in men with IHD before and after cardiac rehabilitation.
Methods:All parameters were measured in venous blood taken before, immediately after and 1h after 6 min cycling test performed by male volunteers with IHD and balanced diet (non-smokers, non-drinkers): age (52.2 ± 6.4 years); height (172 ± 3 cm), weight (84.2 ± 12.9 kg), BMI (28.3 ± 4.2). All experiments were designed according to the principles of the Declaration of Helsinki of the World Medical Association. The conformational state of haemoglobin was investigated by spin-labelling method and the levels of glutathione reduced (GSH) and total thiols were studied before and after cardiac rehabilitation. Two spin labels, MSL and ISL, were applied for the studies of conformational changes in Hb structure.
Results:From EPR spectra the relative rotational correlation time (Tc) was calculated as an indicator of conformational changes in Hb structure. Generally, this parameter did not change during exercise before and after cardiac rehabilitation. However, both spin labels attached to haemoglobin showed a slight decrease in rotational correlation time after cardiac rehabilitation. The level of total thiols dropped significantly after exercise before CR and remained at the comparable level 1 h later. After CR the decrease induced by exercise was approx. two times lower. We have also observed that exercise induced a decrease in the level of GSH, before and after CR. However, opposite results were obtained 1 h after exercise. Before CR, the decrease was continued, while after CR, 1 h after exercise a large increase in GSH level was detected.
Conclusions:These results indicate that cardiac rehabilitation does not influence the conformational state of haemoglobin. On the other hand, it improves significantly the level of GSH, despite the decrease in the level of total thiols. Acknowledgment: This study was supported by the grant N404 178440 from the Polish Ministry of Science and Higher Education.
P757
Cardiac rehabilitation role in improving HDL cholesterol
P Pinto-Teixeira1, P Rio1, A Abreu1, S Rosa1, A Monteiro1, I Rodrigues1, M Nogueira1, T Silva1, R Soares1, R Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Topic: Sports cardiology
Purpose:Low levels of high density lipoprotein (HDL) cholesterol are associated with increased cardiovascular risk and are frequent among patients (pts) with coronary heart disease (CHD). Currently available drugs do not robustly raise HDL cholesterol leaving an important role to lifestyle interventions such as physical activity and weight reduction. In this study we sought to evaluate the impact of a 12-week cardiac rehabilitation (CR) program on HDL cholesterol levels.
Methods:We retrospectively analysed the series of consecutive pts who underwent a single centre CR program comprising of 36 in-hospital exercise sessions, occurring three times per week (60 minutes duration). We recorded the total cholesterol (TC), HDL, low lipid lipoprotein (LDL) and triglyceride (TG) levels before and after the 12-week CR program and assessed the differences between them. Stratification analysis was performed for those with baseline HDL levels below or greater than 40mg/dL.
Results:208 pts completed CR program, 85% male, mean age 57.3±10.4 years, 92% had CHD. There was significant improvement on post-CR HDL cholesterol levels (38.9±10.7 vs 41.6±11.1 p<0.001). There were no relevant differences concerning TC, LDL or TG cholesterol levels pre and post-CR. On subgroup analysis, pts with baseline HDL < 40mg/dL had significant improvement on their HDL cholesterol levels pre and post-CR when compared with those with baseline HDL > 40mg/dL (20.3% vs -1,8%, p<0.001).
Conclusions:Cardiac rehabilitation significantly improves HDL cholesterol in patients with low baseline HDL levels (< 40mg/dL).
*for the differences between the two groups.ns = not significant
Baseline HDL < 40 mg/ dL
Baseline HDL > 40 mg/ dL
Parameters
Before CR
After CR
Variation (%)
p value
Before CR
After CR
Variation (%)
p value
p value*
Total cholesterol (mg/ dL )
146.9±30.3
153.7 ±31.9
6.7
0.035
171.3 ±36.5
164.2 ±32.6
-2.2
0.09
0.006
HDL (mg/ dL )
31.4 ±5.7
37.0 ±7.6
20.3
<0.001
48.4 ±8.4
47.1 ±9.7
-1.8
0.237
<0.001
LDL (mg/ dL )
92.8 ±27.2
95.9 ±27.6
7.2
ns
108.0 ±30.5
104.9 ±26.9
0.9
0.382
ns
Triglycerides (mg/ dL )
121.1 ±60.7
122.7 ±75.2
7.4
ns
108.8 ±59.9
111.2 ±60.5
-12.6
0.710
ns
P758
Efficacy of phase II cardiac rehabilitation on exercise capacity and renal function in patients with cardiovascular diseases and chronic kidney disease
Y Iso1, H Kitai1, J Kowaita1, E Kyuno1, H Maezawa1, H Suzuki2
1Showa Univ. Fujigaoka Rehab. Hosp., Yokohama, Japan
2Showa Univ. Fujigaoka Hospital, Yokohama, Japan
Objectives:Cardiac and renal diseases are common and frequently coexist, so called cardio-renal syndromes, to significantly increase mortality and morbidity. Efficacy of exercise therapy for cardiovascular disease (CVD) is well recognized, and thus the importance of cardiac rehabilitation (CR) is reflected in guidelines of clinical cardiology. On the other hand, there is a general fear that exercise training might deteriorate renal function in patients with chronic kidney disease (CKD) because heavy bouts of exercise may cause a transient fall in renal blood flow. Therefore, the aim of this study was to investigate the effect of phase-II CR on exercise capacity and renal function in the CVD patients with CKD.
Methods:and Results:Sixty seven CVD patients who participated in a 5-month CR program were studied. Causes of the CVD were as follows: chronic heart failure (n= 24), acute myocardial infarction (n= 25) and stable angina pectoris (n= 18). Cardiopulmonary exercise testing was performed before and after the CR program, and peripheral blood was collected at the beginning and 3-month after completion of the program. Estimated glomerular filtration rate (eGFR) less than 60ml/min/1.73m2 was defined as CKD. In patients with severe CKD (eGFR<50, n= 19), peak oxygen uptake (VO2) at the baseline was lower than in the patients with mild CKD (eGFR50-60, n= 14) and without CKD (n= 34). Phase-II CR significantly increased the peak VO2 levels in the patients with and without CKD, whereas the CR did not alter the eGFR from phase-II to –III in each group. We found that changes in the eGFR was inversely associated with age (r= -0.355, p< 0.05). When the patients with CKD were divided into the elderly (age>70, n= 20) and the non-elderly (age<70, n=13) groups, the non-elderly group showed significant increases in the eGFR levels.
Conclusion:Taken together, exercise training in phase-II CR improved exercise capacity and did not deteriorate renal function in the patients with cardio-renal syndromes. Results of this study also suggest that age may influence the recovery of renal insufficiency by exercise therapy.
P759
Does ischemic heart disease affects sexual function in women?
I Cunha1, S Viamonte1, C Matos1, AR Correia1, A Barreira1, P Fernandes1, S Torres1
1Centro Hospitalar do Porto, Porto, Portugal
Topic: Sports cardiology
Purpose:Sexual dysfunction after ischemic heart disease is well documented in men; in the female this issue is recent and literature is scarce, despite being a prevalent problem. The purpose of this study was to analyse sexual function in female patients before and after a cardiac event and identification of factors that interfere with it.
Methods:Unicentric, observational, prospective, cohort trial. Selected female patients, oriented to Cardiac Rehabilitation Program conducted in the first 3 months after hospitalization for acute coronary syndrome, during 2013-2014. Patients older than 70 years, and women without active sex life were excluded. Sociodemographic and clinical data on heart disease and cardiovascular risk factors were collected. Functional capacity was estimated in Metabolic Equivalents (MET) obtained in a maximal treadmill exercise stress test. Anxiety and depression levels were evaluated by the Hospital Anxiety and Depression Scale (HADS). For evaluation of sexual function, a self-reported questionnaire was applied. Results:50 patients (mean age: 59±10.1 years) were enrolled, 81.3% hypertensive, 37.5% diabetic, 40.6% smokers and 65.6 % dyslipidemic. Exercise capacity estimated by MET was 7.18±2.25. HADS scores showed an average of 11.62±4.66 for anxiety and 8.15±4.69 for depression. Data collected through the questionnaire applied found that 75.0% resumed sexual activity after the event, 25.0% of these more than 8 weeks after. The majority (73.9%) decreased the frequency of sexual activity with approximately 54.2% referring a low degree of satisfaction. 66.7% denied cardiovascular symptoms during sexual activity, but 92.0% women's and 95.8% of partners expressed concern about the possibility of having a heart attack or sudden death during the same. Statistically significant relationship between anxiety levels and depression levels with the resumption of sexual activity was found (p=0.023 and p=0.008, respectively) as well as between levels of depression and the time at which it was taken up (p=0.025).
Conclusions:This study clearly demonstrates the negative impact of a cardiovascular event in women's sexual function. The concern shown regarding the repetition of symptoms during sexual activity, shared by the woman and partner, demonstrates the need to clarify the couple. Sexual dysfunction should be addressed in the Cardiac Rehabilitation Programs, and an interventional attitude is required towards the organic dysfunctions potentially aggravating this dysfunction.
P760
Peripheral vascular disease is a leading risk factor of adverse events after myocardial infarction
A Simon1, I Tiringer2, I Berenyi1, E Gelesz1, G Veress1
1Balatonfured State Cardiology Hospital, Balatonfured, Hungary
2Institute of Behavioral Medicine, PTE AOK, Hungary, Pécs, Hungary
There are so many known risk factors that can influence the prognosis after myocardial infarction. Peripheral artery disease (PAD) is a marker of extended atherosclerosis and in this way may be a sign of poor prognosis after myocardial infarction. We aimed to investigate the role of presence of PAD disease among conventional risk factors in risk stratification in subjects, who entered Phase II cardiac after their myocardial infarction. 302 patients (age 61.9 +- 12.2 years, 61.9 % men) were entered in our analysis, who participated in phase inpatient II cardiac rehabilitation program after their myocardial infarction (either STEMI or NSTEMI). Actual smoking, diabetes mellitus, hypertension, depression (assessed by Hospital Anxiety and Depression Scale), left ventricular ejection fraction (LVEF), signs of heart failure were treated as conventional risk markers. Age, gender, CCS an NYHA classifications were also taken into account in Cox proportional hazard model. Mortality and occurrence of death, nonfatal myocardial infarction, PCI or stroke (MACE) were treated as endpoints.
Results:36 patients (11.9%) had PAD in their medical history or diagnosed during rehabilitation treatment with ankle-brachial index (ABI). Patients with PAD had higher NYHA class (2.11 +- 0.83 vs. 1.83 +- 0.70, P = 0.03), higher CCS class (1.11 +- 0.96 vs. 0.75 +- 0.78, P = 0.012), higher prevalence of diabetes mellitus (41.7 vs. 24.4 %, P = 0.026) and heart failure (33.3 vs. 16.2 %, P = 0.015). No significant difference in age, gender, hypertension, depression, actual smoking and ejection fraction was found. Kaplan-Meier analysis reveled marked difference in mortality (9/36 vs. 16/264, P<0.0001) and borderline difference in the occurrence of MACE (14/36 vs. 61/264 cases, P=0.05) during the follow up of 477 +- 98 days. Cox proportional hazard model identified hypertension as only significant predictor of mortality (HR: 4.0001 95%CI: 1.056-15.161; P = 0.041), while age (HR: 1.061, 95%CI: 0.990-1.136, P=0.093), LVEF (HR: 0.0953 95%CI: 0.904-1.005, P = 0.077) and PAD (HR: 3.489, 95%CI: 0.920-13.234, P = 0.066) showed a tendency toward higher mortality. MACE was predicted by PAD only (HR: 2.402 95%CI: 1.120-5.148, P = 0.024).
Conclusion:PAD is an important prognostic factor of adverse events after myocardial infarction. Active search of PAD in medical history and use of ABI in patients during rehabilitation can identify those subjects, who need more powerful optimalization of lifestyle and medical treatment.
P761
Complexity of heart rate variability during orthostatic position in patients with coronary artery disease
RP Simoes1, MO Gois1, VC Kunz1, A Porta2, AM Catai1
1Federal University of Sao Carlos, Physical Therapy, S?Carlos, Brazil
2University of Milan, Department of Technologies for Health, Milan, Italy
Topic: Sports cardiology
Purpose:to evaluate the complexity of heart rate variability (HRV) during orthostatic position in patients with coronary artery disease (CAD) with and without diabetes mellitus (DM).
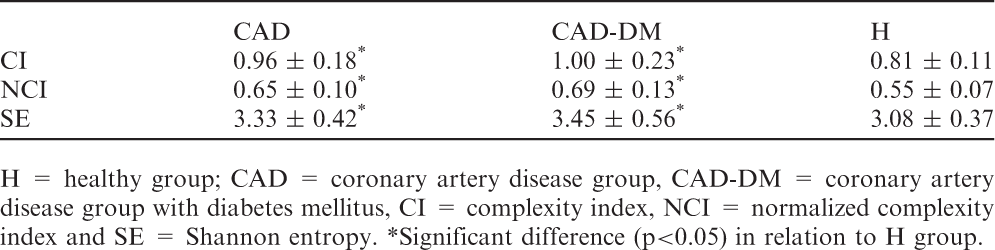
Methods:we evaluated 56 men between 45 and 65 years and separated into 3 groups: 1) coronary artery disease patients without diabetes mellitus (CAD group, n = 20); 2) coronary artery disease patients with type 2 DM (CAD-DM group, n = 16); and 3) healthy individuals (H group, n = 20). All patients of CAD and CAD-DM groups had a diagnosis of CAD confirmed by coronary angiography examination and the patients with type 2 DM had a diagnosis according to the criteria of American Diabetes Association. The recording of R-R interval (R-Ri) of the electrocardiogram were performed with the subjects at rest in the orthostatic position in a period of 15 minutes. The R-Ri registration was performed using the BioAmp FE132 and Power Lab 8/35 system, ADInstruments. Regarding data analysis, 256 consecutives data points were used in the analysis. Conditional entropy was assessed with the complexity index (CI) and this index was normalized by the Shannon entropy (SE) of the R-R series to obtain a normalized complexity index (NCI), thus expressing complexity in terms of dimension less units. A higher value of CI, NCI and SE reflect greater complexity of the series and is associated with better cardiac parasympathetic modulation.
Results:Regarding pharmacological treatment, 16 subjects of the CAD group and 15 of CAD-DM group used beta-blocker drugs. The table shows higher values of CI, NCI and SE of CAD and CAD-DM groups compared to group H.
Conclusion:Complexity indices of HRV was higher in CAD and CAD-DM groups possibly due to pharmacological treatment.
H = healthy group; CAD = coronary artery disease group, CAD-DM = coronary artery disease group with diabetes mellitus, CI = complexity index, NCI = normalized complexity index and SE = Shannon entropy. *Significant difference (p<0.05) in relation to H group.
CAD
CAD-DM
H
CI
0.96 ± 0.18*
1.00 ± 0.23*
0.81 ± 0.11
NCI
0.65 ± 0.10*
0.69 ± 0.13*
0.55 ± 0.07
SE
3.33 ± 0.42*
3.45 ± 0.56*
3.08 ± 0.37
P762
Preventive versus culprit-only percutaneous coronary intervention in st-elevation myocardial infarction patients with multivessel coronary disease and chronic obstructive pulmonare disease.
J Ramazanov1, T Batyraliyev2, I Pershukov3, Z Karben2, A Omarov4, L Shulzhenko5, B Sidorenko6, Y Belenkov7
1Central Hospital of Oil Workers, Cardiology, Baku, Azerbaijan
6Presidential Medical Center , Moscow, Russian Federation
7M.V. Lomonosov Moscow State University, Moscow, Russian Federation
Background:Although previous studies have suggested clinical benefits of complete revascularization in patients with multivessel coronary artery disease, it still controversial whether preventive percutaneous coronary intervention (PCI) leads to better clinical outcomes in the clinical setting of ST-segment elevation myocardial infarction (STEMI),especially in patients with comorbidities, such as chronic obstructive pulmonary disease (COPD). Material and Methods:We analyze data of relevant studies published through September 2014. Studies were searched and identified in the electronic databases. Primary endpoint was all-cause mortality at the longest follow-up.
Results:From 917 initial citations, 7 randomized trials and 24 observational studies with 47,630 patients (8,216 preventive and 39,414 culprit-only) were included in this study. Subgroup of patients with COPD was 1,834 (227 preventive and 1,607 culprit-only). There were no significant differences in all-cause mortality (odds ratios {OR},1.02; 95%CI, 0.75-1.36; p=0,89), MI (OR, 1.09; 95%CI, 0.58-1.78; p=0.61), and repeat revascularization (OR, 0.74; 95%CI, 0.48-1.03; p=0.8), between the two groups (complete vs culprit-only). Comparison of preventive PCI versus culprit-only PCI group disclosed ORs for MACE of 0.83 (95%CI, 0.57-1.23; p=0.29). Stratified analysis according to the different strategy demonstrated a significantly lower incidence of all-cause mortality of COPD patients with staged PCI compared with culprit-only or multivessel PCI during the index procedure.
Conclusions:Preventive PCI strategy did not reduce adverse outcomes when compared with culprit-only revascularization in STEMI patients with multivessel disease and COPD, while a significantly lower all-cause mortality was observed with staged PCI compared with culprit-only PCI or multivessel PCI during the index revascularization.
P763
Physical training improves oxidative stress status in people living with HIV-AIDS: a pilot study
M Karsten1, LF Deresz1, CM Scholer2, PIH Bittencourt Jr2, MLR Ikeda2, P Dal Lago1
1Universidade Federal de Ci?ias da Sa?e Porto Alegre, Sciences of Rehabilitation, Porto Alegre, Brazil
2Federal University of Rio Grande do Sul, Porto Alegre, Brazil
Topic: Sports cardiology
Purpose:Higher levels of oxidative stress may contribute to increased cardiovascular risk in people living with HIV/AIDS (PLWHA). Thus, the main goal of this study was to evaluate the effects of physical training on markers of oxidative stress in PLWHA who at the same time were undergoing highly active antiretroviral therapy (HAART).
Methods:Virologically suppressed patients received the same HAART and other medication for a period of at least six months. All participants performed three sessions per week for eight weeks (24 sessions) of Aerobic (AT), Resistance (RT) or Concurrent Training (CT) (defined by block randomization). Aerobic training consisted of 40 minutes on a treadmill, resistance training was three sets of 10-12 repetitions of seven exercises and concurrent training comprised of 20 minutes on a treadmill in addition to a single set of the seven resistance exercises. Oxidized/Reduced Glutathione ratio (GSSG/GSH) measured in erythrocytes and thiobarbituric acid–reactive substances (TBARS) measured in plasma samples, were used as oxidative stress markers. A paired t-test was used to determine the differences in physiological parameters between baseline and post training values. The Cohen's d was used to measure a standardized Effect Size. Statistical significance was defined as p= 0.05.
Results:Eight volunteers completed the training protocol: three in AT, three in RT and two in CT. Data pooled analysis showed an increase in VO2peak after the training protocol (29.14±5.34 – 32.48±5.75 p=0.04; d=0.6). All subjects who performed resistance exercises (RT and CT) showed increases (69±30%) in muscle strength after the protocol training and there were no differences between performing single or multiple sets to gain muscle strength. The GSSG/GSH ratio and TBARS values decreased after the training protocol (Log GSSG/GSH = -1.26±0.57 – -1.54±0.65, p=0.01, d = 0.46; Log TBARS= 0.73±0.35 – 0.43±0.21 p=0.01, d = 0.35).
Conclusions:the results of this study confirm the benefits of physical training on aerobic and muscular fitness and decrease oxidative stress in PLWHA, supporting the hypothesis that physical training is an effective therapy to reduce cardiovascular risk factors in this population.
P764
Pacients with heart failure have lower muscle power of the lower limbs
AS Coimbra1, RM Cascon1, F Caramez1, M Varella1, PA Azevedo1, MA Santos1, SF Borges1
1EPVM - UNIMED RIO, Cardiac Rehabilitation, Rio de Janeiro, Brazil
Introduction:The loss of muscle mass, especially in the lower limbs, is a feature very present in patients of cardiac rehabilitation programs. It is proved that the muscular power (MP) has a direct relationship with functional capacity in the elderly where there is a natural loss of this variable with the aging process. Especially in elderly patients with heart failure (HF) muscle mass loss of lower limb contributes to the poor prognosis and evolution of the disease.
Topic: Sports cardiology
Purpose:To evaluate the MP of the lower limbs of patients with and without HF participating in a cardiac rehabilitation program.
Methods:Thirty-six elderly, 16 with HF (72 ± 6.51y, 76.8 ± 4.8 kg, 171 ± 9.48 cm), beginners in cardiac rehabilitation exercise program, in Rio de Janeiro, Brazil were evaluated in MP to enter the program. To analyze the absolute and relative muscle sink body weight of the lower limbs, we used half squat exercise (body weight), where the forward speed to lift the seat from a 90 ° knee through FITRODYNE® equipment (Fitronic Bratislava, Slovakia) , the evaluation result was obtained in watts (W) to complete MP and watts per kilogram (W/kg) relative to MP.
Results:Heart failure patients shows a lower absolute (A) and relative (R) MP compared with no HF patients (A 362.41±18,57W - 438.92±22.33W p=0.015.) (R 4.69±0.23W/kg - 5.90±0.23W/kg p=0.001).
Conclusions:- Patients with heart failure have great loss of muscle mass in the lower limbs, a fact that contributes to bad prognosis of the disease. Cardiac rehabilitation programs should enhance the strength training of the lower limbs, focusing on gaining power, improving the quality of life and the prognosis as the disease. More studies should be conducted in order to identify the best methodology for the training of these patients.
P765
The role of cardiac rehabilitation patients with left ventricular assist devices.
A Zielinska-Meus1, K Oleszczyk1, B Spinczyk1, K Bugajska-Sysiak1, T Sykosz1, M Cichosz1, B Leszczynska-Bolewska1, I Cogiel1, J Pacholewicz2
1Upper Silesian Rehabilitation Center "Repty", Department of Cardiac Rehabilitation, Tarnowskie Gory, Poland
2Silesian Center for Heart Diseases (SCHD), Departament of Cardiac Surgery and Transplantology Medical University of Silesia, Zabrze, Poland
The left ventricular assist devices (LVADs) implantation is one of treatment method for patients in end-stage heart failure which brings new complications: pulmonary and pericardis effusion, anxiety, weight increase. The aim of this study was to asses the role of standard rehabilitation program in patients with LVADs.
Patients and methods:24 men - mean age 50±9,4 after implantation left ventricular assist device in Silesian Center of Heart Diseases in Zabrze were admitted to cardiac rehabilitation unit in Upper Silesian Rehabilitation Center in Tarnowskie Gory for supervised cardiac rehabilitation program between 2010 - 2014. All patients were in New York Hart Association class IV before implantation and ejection left ventricular fraction was below 20%. All patients underwent residential cardiac rehabilitation with duration 20±8 days (from 11-28 days). The program of rehabilitation consisted of: morning exercise, aerobic training, interval endurance aerobic training (cycle ergometer - monitoring training), resistant training, brisk walk. The exercises were limited by rating of perceived exertion (RPE) – 10-11. The body mass was also monitoring as a result of proper diuretic drug administration, but also as a result of muscle mass increase. Descriptive statistic were expressed as median and standard deviation for continuous variables. Comparison between variables in each patients were done by Student's t-test for pair samples. P value<0,05 was considered as statistically significant.
Results:The reason of the end stage heart failure was ischemic cardiomyopathy (40% patients) and dilated cardiomyopathy (60%). The mean time from implantation of left ventricular devices to admission to the cardiac rehabilitation unit was 48,7±23 days. The ICD was implanted in 90% of patients as a primary prevention of sudden cardiac death. Before rehabilitation the walking distance in 6 min test was mean 328m±89,9 m, after rehabilitation 391±73,8 m (p<0,05). Mean distance rise was 74,5 m. The level of exercise tolerance satisfaction increased and it was depend on length of stay in cardiac program. The serum level of creatinine and blood count didn't change during rehabilitation.
Conclusions:Early post-hospital rehabilitation in patients with LVADs influences positively on subjective and objective improvement. The exercise tolerance improvement is significant and depend on length of stay on cardiac rehabilitation unit. The training heart rate observation during exercise training is impossible and subjective scale method control need patient to be high motivated for exercises.
P766
Has beta-blocker therapy a continuous incremental benefitial effect after primary percutaneous coronary intervention?
A T Timoteo1, S A Rosa1, P Rio1, A V Monteiro1, M L Ferreira1, R Cruz Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
Background:It has been previously shown that beta-blocker (BB) therapy has a beneficial impact in patients with stable coronary artery disease as well as with acute coronary syndrome, particularly ST-elevation acute myocardial infarction (STEMI). However, in the more recent era of preferred reperfusion therapy with primary percutaneous coronary intervention (PCI), studies are scarce.
Methods:Study of consecutive patients admitted at a single-centre coronary care unit for a STEMI and successfully treated with primary PCI within 24 hours from the onset of STEMI. Patients who received oral BB and who did not were compared. Our primary end-point was all-cause mortality at one-year follow-up.
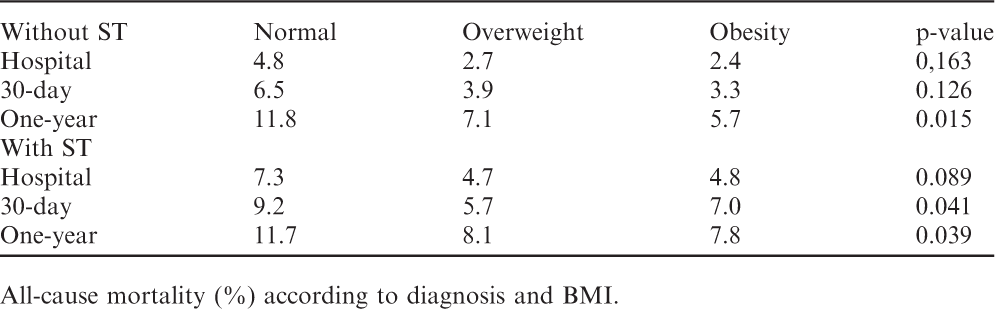
Results:We included 607 patients, mean age 62 ± 13 years, 76% males. In this group, 84% received BB shortly after admission and these patients were younger, had higher heart rate, systolic blood pressure, estimated glomerular filtration rate and lower GRACE risk score. All the other baseline characteristics were similar. In-hospital (3.1% vs. 17.7%), 30-day (3.9% vs. 18.8%) and on-year mortality (4.7% vs. 20.8%) was significantly lower (p<0.001) in patients that received BB (adjusted HR 0.37, 95% CI 0.19 – 0.72, p=0.004). However, analysing only patients that survived to discharge (n=574, 77% males, 61 ± 12 years, 82% with BB), no difference was observed in one-year all-cause mortality between patients with and without oral BB at discharge (1.7% vs. 2.9% respectively, p=0.425; adjusted HR 0.77, 95% CI 0.17 – 3.62, p=0.745).
Conclusions:In the subset of patients with STEMI treated by primary PCI, although BB remains protective for short-term mortality, the incremental benefit is no longer observed after discharge. These results suggest that in patients with STEMI in the PCI era, the impact of medical therapy might be attenuated.
P767
Predictors for better functional capacity of patients in cardiac rehabilitation program
J Matos1, S Viamonte1, S Magalhaes1, C Branco2, I Cunha1, A Barreira1, P Fernandes1, S Torres1
1Hospital Center of Porto, Porto, Portugal
2Institudo de Ciencias Biomedicas Abel Salazar, porto, Portugal
Introduction:The cardiac rehabilitation programs (CRP) play a significant role in management of heart diseases, resulting in an improvement in patients physical activity and quality of life and a decrease of health costs. A significant part of its effectiveness is due to the positive impact on the functional capacity, improving prognosis.
Objective:The aim of this study was to determine the predictors for better outcome of functional capacity in individuals admitted in CRP Material and methods:Retrospective cross-sectional descriptive study of patients who initiated CRP between January 2008 and December 2013. The dependent variable was the increase in metabolic equivalents (METs) in exercise test at the beginning and end of phase II of the program. The independent variables were age, gender, dyslipidemia, diabetes mellitus, hypertension, smoking habits, body mass index, sedentarism (assessed by the International Physical Activity questionnaire) and the diagnosis. The variables were analyzed by univariate and multivariate linear regression model with significance level of 0.05 for reject null hypothesis.
Results:The sample included 1399 patients; 1125 (80.4 %) finalized the Phase II of the program. The average age was 61 years, 76% were male and 24% female, 62% were admitted to the program for acute coronary syndrome, 14% after coronary angioplasty and 10% after coronary artery bypass grafting. The prevalence of dyslipidemia was 71%, diabetes mellitus 38%, hypertension 61%, obesity 18%, smoking habits 31% and physical inactivity 63%; 93% of participants had a favorable functional evolution registered in METs with average increase 1.45 METs and standard deviation 1.19). Patients admitted in CRP after CABG had better improvement in functional capacity with average increase of 1.90 METs and standard deviation 1.43. Compared with acute coronary syndrome patients admitted after CABG had on average a additional benefit of 0.44 METs. Patients with diabetes mellitus showed a worse outcome of functional capacity. Patients between 45 and 65 and older than 65 years old had a better outcome of functional capacity than the other groups. The remaining variables had no significant influence on functional capacity.
Conclusion:This study reinforces the relevance of CRP in secondary prevention of cardiovascular disease. It is necessary to extend the evaluation of predictors of response to the PRC to a multifactorial context in order to maximize the effectiveness of these programs.
P768
The association of cardiac autonomic function and oxygen uptake in the cardiovascular elastic function of patients following acute myocardial infarction
A Ogawa1, K Shimizu2, T Ymamoto3, K Terayama1, T Akiba1, H Kiyokawa2, T Nakagami2, H Maruoka4, K Nakagawa1, K Shirai3
1Sakura Medical Center, Department of Rehabilitation, Sakura-City, Chiba, Japan
2Sakura Medical Center, Department of Internal Medicine, Sakura-City,Chiba, Japan
3Sakura Medical Center, Department of Vascular Function, Sakura-City,Chiba, Japan
4Saitama Prefectural University, Graduate School of Health and Medical Welfare, Koshigaya-City,Saitama, Japan
Background:The etiology of ischemic heart disease shows a reduction in cardiovascular elasticity features, such as arteriosclerosis. The prognosis of heart disease is associated with oxygen uptake and heart autonomic nervous function. However, the relationship between cardiovascular elastic function, cardiac autonomic function and oxygen uptake is not fully elucidated.
Topic: Sports cardiology
Purpose:The purpose of this study was to investigate the relevance of cardiovascular elastic function, cardiac autonomic function, and oxygen uptake. Methods?#154;The subjects were patients who carried out Cardiac Rehabilitation (CR) after an emergency coronary angioplasty for acute myocardial infarction between August 2012 and September 2014. We measured the Cardio-Ankle Vascular Index (CAVI) as the vascular elasticity function and the oxygen uptake during Cardio Pulmonary Exercise Tests (CPX) and 123-IMIBG, as well as myocardial scintigraphy (MIBG) as cardiac autonomic function at discharge. Analysis was carried out to investigate the association of each parameter in the Pearson product-moment correlation coefficient or Sparman rank correlation coefficient. The significance level was set at 5%.
Results:?Subjects 21 patients (3 female), mean age was 64.7 ± 9.1 years old. The MIBG was only measured in about half of the subjects (12 people). CAVI and Peak VdotO2 showed an inverse correlation?=-0.601?#140;P<0.01?#137;.CAVI and MIBG H / M ratio showed an inverse correlation?=-0.579?#140;P<0.05?#137;,and the MIBG Washout Rate was correlated?=0.581?#140;P<0.05?#137;.
Conclusion:In the present study, cardiac autonomic function and oxygen uptake were shown to be associated with cardiovascular elastic function. Cardiovascular elastic function plays the role of providing a steady blood supply to the whole body following the pulsatile flow from the heart. Therefore, vascular distensibility that was linked to systolic elastic function is impaired by arteriosclerosis. This causes the peripheral circulation of blood volume to decrease. An increase in sympathetic activity decreases the skeletal muscle vasodilator in the periphery and decreases the amount of oxygen supply to skeletal muscle. The reduction of oxygen uptake is due to these factors.
Limitation:The impact of age was undeniable and this is a limitation of this study. A study excluding the impact of age would be preferred. We think further investigations containing more subjects are needed.
P770
Using of physical and cardiorespiratory training for prophylaxis of sudden cardiac death after myocardial infarction
I A Leonova1, S Boldueva1, M Samokhvalova1, I Yarmosh1
1North-Western Sate Medical University named I.I. Mechnikov, St-Petersburg, Russian Federation
Sudden cardiac death (SCD) is the main reason of mortality during one year after myocardial infarction (MI). Independent predictor of SCD after MI is the vegetative imbalance. Heart rate variability (HRV) is a widely used method for an assessment of a condition of vegetative nervous system. Possibilities of medicament impacts on a vegetative imbalance are limited, actual search of alternative methods of impact on HRV, such as physical trainings (PT) and cardiorespiratory training (KRT) is very important.
The purpose of this study:the assessment of changes of vegetative regulation of HR at patients with MI, receiving standard methods of treatment, sessions of KRT and PT in early period after MI.
Material and methods:89 patients with IM in early period of disease at the age from 40 till 70 years were surveyed. The 1-st main group consisted from 29 people by whom KRT (5–10 sessions) was carried out. The assessment of efficiency and safety of KRT was carried out on a clinical picture and on parameters of HRV before, after and during KRT. The 2-nd main group was created from 30 patient by whom aerobic PT on bicycle was carried out. Both study groups received standard therapy. Control group (CG) consisted of 30 patients receiving only standard therapy.
Results:During carrying out of KRT, and after KRT worsening of clinical picture at patients of the 1-st main group was not observed. 4 patients from group of PT were excluded due to angina pectoris and signs of heart failure. HRV analysis at patients of the main group showed that after end of KRT decrease in an index of tension (p<0,05), increase in an indicator of the general dispersion of HR (p<0,05), and also a tendency to increase of vagal part of total power during spectral analysis (p=0,05) was observed. Normalization of HR and arterial pressure (AP), growth of cardiorespiratory index and index of a variation took place, cardiorespiratory synchronization was restored. Persons from CG had no such changes. After the termination of PT in patients of 2-nd AP and HR has decreased while in the CG, opposite, accrued. Upon termination of PT at patients from 2-nd main group (4 months after IT) reliable increase in the general HRV parameters at the expense of parasympathetic (SD, dRR) and sympathetic (lgLF and LFn) influences was found; the share of humoral and metabolic influences (%VLF) decreased against a distinct tendency to the general improvement of HRV. Persons from CG had no such changes.
Conclusion:PT and KRT are safe and effective methods, allowing to improve vegetative regulation after MI
P771
Association of early exercise capacity with different biomarkers in coronary artery disease patients admitted for exercise-based rehabilitation program
J Brozaitiene1, N Mickuviene1, N Kazukauskiene1, J Burkauskas1, I Duoneliene1, R Bunevicius1
1Behavioral Medicine Institute, Lithuanian University of Health Sciences, Palanga, Lithuania
The aim of the study was to evaluate associations of early exercise capacity (EC) with different biomarkers in coronary artery disease (CAD) patients admitted for exercise-based rehabilitation program (RP).
Methods:In sum, 640 CAD patients, 2 weeks after acute coronary syndromes (acute myocardial infarction (MI) or unstable angina pectoris), admitted for RP were invited to participate in the study. All patients (mean age 58±9 years; 76% male) were evaluated for demographic, clinical, psychological and echocardiographic characteristics. Cardiovascular functional status was assessed according to the New York Heart Association (NYHA) class. Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety (HADS-A) and depression (HADS-D) symptoms. Evaluation of early EC testing was performed using a stationary bicycle ergometer with rising workload by 25 watts (W) every 3-minutes. Subjects were exercised to their self-determined maximal capacity or until the appearance of cardiovascular symptoms. Serum concentrations of thyroid hormones: free T3 (T3), free thyroxine (T4), reverse T3, total T4, thyroid stimulating hormone (TSH), natriuretic peptide NTpro-BNP and inflammation markers: high sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6) were analyzed. Univariate and multivariate linear regression (enter method) models were used to examine relationships between early EC and biomarkers separately for NYHA I-II and NYHA III class patients.
Results:Four hundred two patients (63%) were after acute MI, 429 (67%) – after percutaneous coronary intervention, 521 (81%) were NYHA I-II and 119 (19%) – NYHA III class. The mean EC was 70.8±29.2 W. In univariate regression analysis almost all biomarkers were significantly associated with early EC in all NYHA classes. After adjusting for gender, age, angina pectoris class, HADS-A and HADS-D score, in NYHA I-II class patients higher EC was associated with lower concentrations of NTpro-BNP (?-.222, p<.001), IL-6 (?-.121, p<.01) and total T4 (?-.111, p<.05). Controlling for potential confounders, in NYHA III class patients early EC was associated with NTpro-BNP (?-.198, p<.05) concentration.
Conclusions:In patients after acute coronary syndromes admitted for exercise-based rehabilitation program higher level of the early EC in NYHA I-II class patients is associated with lower concentrations of NTpro-BNP, IL-6 and total T4. The lower level of the EC in NYHA III class patients remained associated with higher concentration of NTpro-BNP. This reserch was funded by the European Social Fund under the Global Grant measure, Grant VP1-3.1-SMM-07-K-02-060.
P772
The effects of posture and relaxation training on sleep, dyspnoea, pain and, quality of life in the short-term after cardiac surgery: a pilot study
B Akinci1, I Yeldan2, Z Bayramoglu3, T B Akpinar3
1Biruni University Faculty of Health Science, Division of Physiotherapy and Rehabilitation, istanbul, Turkey
2Istanbul University , Faculty of Health Science Division of Physiotherapy and Rehabilitation, Istanbul, Turkey
3Florence Nightingale Hospital, Cardiovascular Surgery Department, Istanbul, Turkey
Topic: Sports cardiology
Purpose:To evaluate the effects of a 2-week posture and relaxation training(PRT) program on sleep quality, daytime sleepiness, dyspnoea, pain and quality of life (QoL) in patients who underwent cardiac surgery.
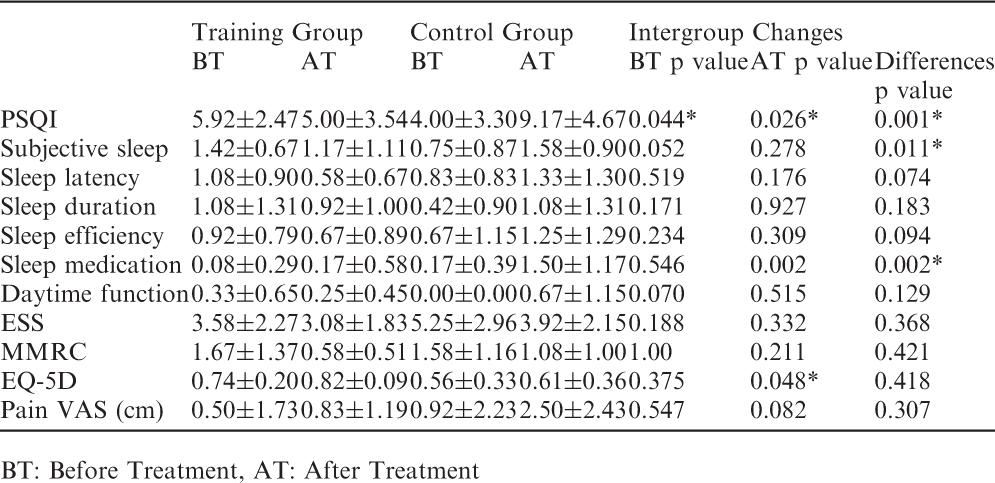
Methods:Twenty-four patients were randomized into the control (n = 12) or training groups (n = 12). The control underwent a conventional post-operative rehabilitation program. The training group underwent PRT in addition to post-operative rehabilitation. Treatment duration was 30 min, twice a day for 2 week. The outcome measures were Pittsburgh Sleep Quality Index (PSQI), Epworth sleepiness scale (ESS), Modified Medical Research Council Dyspnea (MMRC), Euro Quality of Life-5D and visual analogue scales (VAS). The study was performed in accordance with the Declaration of Helsinki of the World Medical Association.
Results:After treatment, there were statistically significant negative changes in the PSQI score, subjective sleep quality, sleep medication usage, sleep disturbance and VAS scores in the control. The training group showed a significant improvement in the MMRC score. Additionally, the PSQI, subjective sleep and sleep medication usage scores showed significant improvements in favour of the training group after treatment.
Conclusion:PRT have beneficial effects to maintain sleep quality, reduce sleep medication usage, alleviate dyspnoea and pain and increase QoL in cardiac surgery patients.
BT: Before Treatment, AT: After Treatment
Training Group
Control Group
Intergroup Changes
BT
AT
BT
AT
BT p value
AT p value
Differences p value
PSQI
5.92±2.47
5.00±3.54
4.00±3.30
9.17±4.67
0.044*
0.026*
0.001*
Subjective sleep
1.42±0.67
1.17±1.11
0.75±0.87
1.58±0.90
0.052
0.278
0.011*
Sleep latency
1.08±0.90
0.58±0.67
0.83±0.83
1.33±1.30
0.519
0.176
0.074
Sleep duration
1.08±1.31
0.92±1.00
0.42±0.90
1.08±1.31
0.171
0.927
0.183
Sleep efficiency
0.92±0.79
0.67±0.89
0.67±1.15
1.25±1.29
0.234
0.309
0.094
Sleep medication
0.08±0.29
0.17±0.58
0.17±0.39
1.50±1.17
0.546
0.002
0.002*
Daytime function
0.33±0.65
0.25±0.45
0.00±0.00
0.67±1.15
0.070
0.515
0.129
ESS
3.58±2.27
3.08±1.83
5.25±2.96
3.92±2.15
0.188
0.332
0.368
MMRC
1.67±1.37
0.58±0.51
1.58±1.16
1.08±1.00
1.00
0.211
0.421
EQ-5D
0.74±0.20
0.82±0.09
0.56±0.33
0.61±0.36
0.375
0.048*
0.418
Pain VAS (cm)
0.50±1.73
0.83±1.19
0.92±2.23
2.50±2.43
0.547
0.082
0.307
P775
Is double-limb stance balance impaired by a single exercise session in middle-aged and elderly subjects?
CG Araujo1, CV Duarte2, FA Goncalves2, GC Pessoa2, SL Rhem2, BC Silva2
1Federal University of Rio de Janeiro, Heart Institute Edson Saad/CLINIMEX, Rio de Janeiro, Brazil
2Exercise Medicine Clinic - CLINIMEX, Rio de Janeiro, Brazil
Topic: Sports cardiology
Purpose:Balance is one of the key components of physical fitness and of upmost importance in older subjects due to their potential to influence in the probability of falls. Balance exercises are often prescribed to older adults and included in their routine exercise sessions. While there is an impressive body of research about the acute effects of exercise on several cardiovascular and muscular variables, much less is known about the effects of a single exercise session on balance. The aim of this study was to analyze the impact of an exercise session on the static double-limb stance of middle-aged and elderly subjects.
Methods:A convenience sample of 122 patients (70% men) aged between 51 e 92 years old and regularly attending a supervised exercise program, most of them due to secondary prevention of coronary artery disease, voluntarily participated in this study. Double-limb stance was assessed in two conditions: with open (OPEN) and closed (CLOS) eyes. Results were obtained by measuring the distance moved by the center of pressure in 10-s before and within 10 minutes after 60-75 minutes of a comprehensive exercise session – 30-40 min of moderate to vigorous aerobic and 30-35 min of muscle training (8-12 exercises 2x6-8 reps at maximal possible eccentric speed) & flexibility and balance exercises. Further analysis was carried out by stratifying subjects according three age-groups: 51-65 (N=37), 66-74 (N=45), 75-92 (N=40) years of age.
Results:There was no difference between static double-limb stance before and after exercise in both conditions (mean ± SEM): OPEN (m) = 28.31 ± 0.53 and 27.91 ± 0.49 (p=.36) and CLOS (m) = 37.72 ± 1.11 and 35.60 ± 1.21 (p=.08). Similarly, there were no differences for before-after measurements when the three age-groups were separately analyzed (p>.05).
Conclusions:These data indicated that static double-limb stance balance, as reflected by 10-s measurements with open and closed eyes, was not significantly affected by a vigorous exercise session, even in the older subjects. In this context, the risk of fall immediately after an exercise session seems to do not be increased and so, no special caution or recommendation need to be undertaken before they return to workplace or to home.
P779
Borg CR-10 scale is not useful to identify ventilatory anaerobic threshold: an analysis based in 1429 adults
C G S Araujo1, FA Goncalves2, CV Duarte2
1Federal University of Rio de Janeiro, Heart Institute Edson Saad/CLINIMEX, Rio de Janeiro, Brazil
2Exercise Medicine Clinic - CLINIMEX, Rio de Janeiro, Brazil
Topic: Sports cardiology
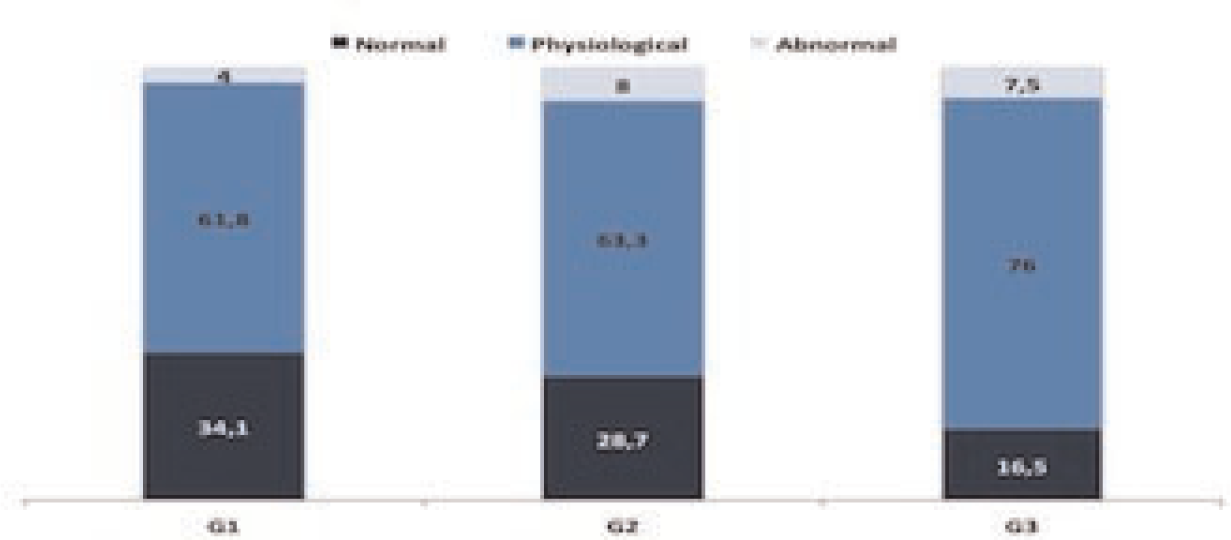
Purpose:Ventilatory anaerobic threshold (VAT) is an important physiological variable with clinical, epidemiological and sport implications; however, its routine use is limited by the requirement of expired gas analysis during cardiopulmonary exercise test (CPET) for its determination. This study assess if there is a specific value in the Borg category ratio scale (CR-10) that represents the VAT.
Methods:1429 adults (72% men) aged between 18 and 89 years old (53 ± 15) performed a maximal cycling CPET with an individualized ramp protocol. VAT was characterized at the work intensity (%VO2max and %HRmax) in which a first non-linear increase in ventilation occurred. Borg scale was questioned at every minute of CPET and the corresponding Borg VAT value identified. Analyses were undertaken for several variables: age, sex, clinical condition (asymptomatic, coronary heart disease and other diseases) and past exercise/sport history at childhood, adult life and last 5 years.
Results:Borg VAT value ranged from 0 to 10 with values from 3 to 5 occuring in 46% of the subjects (figure). Borg VAT value was unrelated to age (r=-.01, p=.60). It was similar between healthy and unhealthy subjects (p=.53), but was slightly higher for women as compared to men, respectively, 4.27±0.07 and 3,98±0.11 (p=.03). There was a tendency to modestly higher Borg VAT values for those more physically active (p=.09). The correlation coefficients between Borg VAT value and %VO2max and %HRmax at VAT, although significant, were too low, respectively, r=.16 and r=.12 (p<.01), to present any major relevance.
Conclusions:Despite physiologically both plausible and appealing, there was not a single Borg value able to precisely identify or reflect the occurrence of VAT.
P780
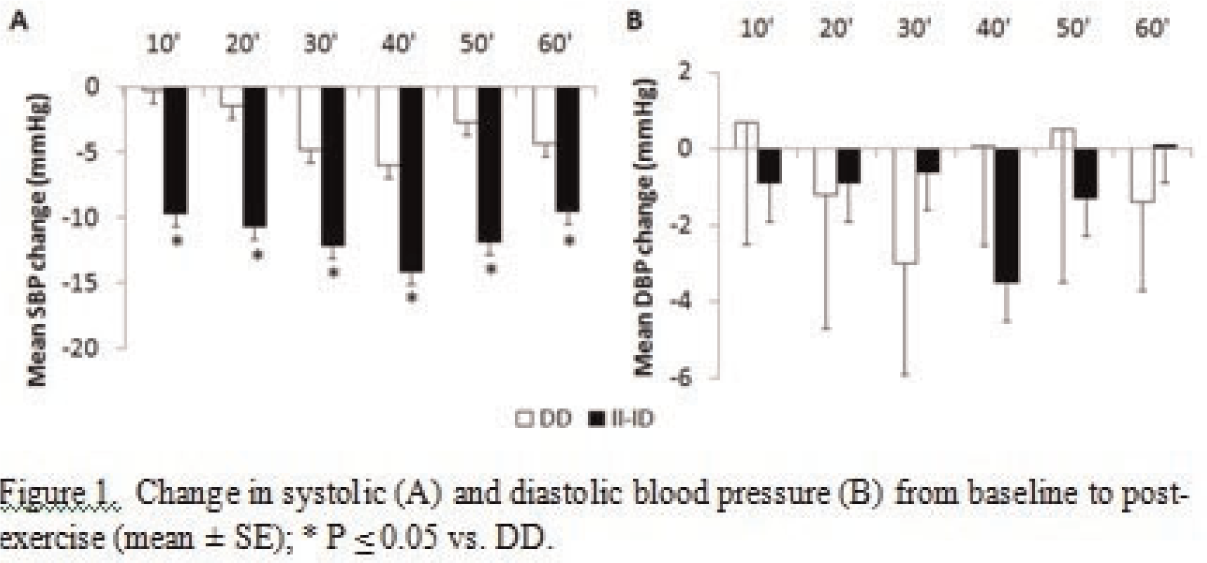
ACE polymorphisms are associated with post-exercise hypotension in hypertensive patients: a pilot study
K Goessler1, V Cornelissen2, EM Oliveira3, GF Mota3, MD Polito4
1CAPES Foundation Education of Brazil, Bras?a, Brazil
2KU Leuven, Leuven, Belgium
3University of S?Paulo, S?Paulo, Brazil
4State University of Londrina, Londrina, Brazil
The adoption of a healthy lifestyle is an essential component in blood pressure (BP) management. Both acute and chronic exercises have been shown to lower BP, especially in hypertensive individuals. However, not all individuals respond similarly to exercise. Limited data suggest that polymorphisms of the angiotensin converting enzyme (ACE)-gene can interfere with the exercise induced acute BP reductions. The aim of this pilot study was to evaluate the effect of the ACE polymorphism on post-exercise hypotension in medicated hypertensive patients. Baseline measurements of office BP were performed after 15 minutes of seated rest in 43 hypertensive patients (14 men; mean age 69.9±9.3 years). Then, all participants performed one walking session of 45 minutes at 60-75% of heart rate reserve. Following this exercise session, office BP was measured every 10 minutes for one hour by means of an automatic device. ACE genotyping was performed by means of polymerase chain reaction; and the ACE gene was classified into three types: I/I, I/D and D/D. Carriers of the I allele were compared to individuals with ACE D/D polymorphism. At baseline, systolic BP (p=0.21) and diastolic BP (p=0.94) were similar for both groups and averaged 133.4±16.1 / 84.3± 9.0 mmHg. Both groups showed a significant reduction in systolic BP following the walking session (p <0.01). However, the reduction in systolic BP was significantly larger at all-time points for individuals with an I allele compared to the individuals homozygous for the D allele (Figure 1A). There were no significant changes in diastolic BP following exercise (p=0.75) (Figure 1B). The present study suggests that the ACE-gene is associated with acute BP reductions following exercise. Larger randomized controlled trials are warranted to confirm our findings.
10127. Figure 1
P783
Metabolic and pshycological aspects as consequences of sports interruption in ex--elite athletes
L Stefani1, VDT Di Tante1, MY Matan1, GG Galanti1
1Department of Experimental and Clinical Medicine, University of Florence, Italy, Department of Experimental and Clinical Medicine, University of Florence, Italy, Florence, Italy
Introduction:Regular sports activity has positive impact in reducing risks factors but few data are available about eventual disadvantages when physiologically stopped. The study aims to verify, by a questionnaire, the consequences of sports interruption in two different kind of world's countries.
Material Methods:23 elite ex- athletes (17 M and 3 F )aged 52.4 ± 16.6 yr including 16 Italian and 4 Israelian, retaired from various sports disciplines (2 sailing , 7 soccer , 3 cycling , 2 combat sports , 2 fencing , 3 swimming and 1 tennis ) were investigated. The EQ- 5D was used a measure of health status and translated into Hebrew and English in evaluating any co-morbidity, quality of life and physical and mental health. They stopped to participate in national and international competitions or had significantly reduced physical activity. Morbility , self-care , usual activities , pain/discomfort were analyzed. Each parameter was investigated at 3 different levels:L 1 - no difficulty, L 2 - some difficulty, L 3 - serious difficulties. The numerical scale ranging from 1 to 10 .A Questionnaire Hospital Anxiety and Depression Scale ( HADS ) was also used .
Results:Time of inactivity was 20 yr. 4 suffered of arrhythmias , 3 had cancer ( oral cavity, breast and melanoma ), 1 had an exercise-induced asthma , and 1 was affected of diabetes. Only 12 (60% ) do not take any drugs , while 5 take a single drug and 2 more than 3 medications ; 2, > 70 yr, were submitted to a coronary bypass . 6 (30 % ) had a post- orthopedic surgery. The BMI was of 24.8 ( ± 2.6 SD). 9 were overweight and 1 was obese ; 50% had a normal BMI. 9 (45%) were smokers, no one had reported to consume alcohol, 3 were hypertensive and 1 had hypercholesterolemia and hypertriglyceridemia. For the anxiety/depression balance, 6 (30 %) showed a risk of developing an anxiety disorder, 3 had an effective anxiety (15 % ).The rest had normal values (11 % ) .Only 2 (10%) were at risk od depression while the rest of the athletes had a normal score.
Conclusions:Athletes maintain a correct lifestyle rather healthy, however they accumulated several cardiovascular risks factors largely represented by an increase in BMI. A predominant difficulty is due to the presence of pain and to those psycological aspects particularly depression and anxiety , that inducing a reduction of quality of life . The cause of these aspects cannot be exclusively explained by "the absence of the sport," but probably has a multifactorial etiology related to their new life style habits
P784
Connection of risk factors and hemodynamic characteristics in men with type D personality
A Miroshnichenko1, I Osipova2, O Antropova2, N Pyrikova2, A Zaltsman1
2Altay State Medical University, Barnaul, Russian Federation
Objective:determine the type D personality, his connection with risk factors and hemodynamic reactivity in men without cardiovascular disease.
Materials and Methods:We observed 99 drivers and their assistants. "Distressorny" type D personality is determined by questionnaire DS-14. Checklist DS-14 includes subscales NA - «negative affectivity" and SI - «social inhibition" in assessing 10 points or higher on each of the subscales determines the type D personality. To assess the hemodynamic reactivity conducted a stress test "Mathematical account" and score from visit to visit variability in blood pressure (BP) within one year. Were identified 2 groups: 1st - person with personality type D (n = 14) and group 2 - without type D personality (n = 85).
Results:The incidence of type D personality in men was 14%. Men with type D personality more likely to smoke by 38% (p < 0,01) and 28% more likely to have hypercholesterolemia (p < 0,01) and did not differ in abdominal obesity. In individuals with type D personality during the test "Mathematical account" observed a more pronounced increase of systolic BP (sBP), diastolic BP (dBP) and heart rate (HR), sBP at 7 mm larger, dBP by 5.6 mm higher, HR above 4.6 (p < 0,001). Reveals an increase of the visit to the visit BP variability. More was the rise in dBP, which was combined with an increase in dBP during the stress test and had a moderate positive correlation (r = 0,5; p = 0,01).
Conclusions:In men with type D personality more frequency of smoking and hypercholesterolemia. Type D personality is associated with increased sBP, dBP and HR, but to a greater extent with the dBP, which is an unfavorable prognostic factor for cardiovascular disease and cardiovascular complications in men.
P786
Predictors of one-year unfavorable prognosis in patients with st-segment elevation myocardial infarction
S Pomeshkina1, N Ardashova1, N Lebedeva1, O Barbarash2
1Federal State Budgetary Institution Research Institute for Complex Issues of Cardiovascular Diseases, Rehabillitation Laboratory, Kemerovo, Russian Federation
2Federal State Budgetary Institution Research Institute for Complex Issues of Cardiovascular Diseases, Kemerovo, Russian Federation
Objective:To identify predictors of one-year unfavorable prognosis in patients with ST-segment elevation myocardial infarction (MI).
Material and Methods:412 patients with MI admitted to the hospital were included in the study. Of them, 152 (37%) patients suffered form diabetes mellitus (DM) and 260 (63%) - without DM. The level of depression (D) was assessed on day 7 of the in-hospital-stay using the Zung Self-Rating Depression Scale (signs of D>49 scores; normal range without D <49 scores). The following assessment end-points one year after MI were selected: death, the number of readmissions for progressive angina and myocardial infarction. The prognosis was considered unfavorable, if at least one cardiac adverse event occurred. Statistical analysis was performed using PASWStatistics (SPSS) statistical software and Statistica 8.0 (StatSoft) software. P <0.05 was considered statistically significant.
Results:One-year unfavorable prognosis was observed in 300 (73%) patients. Univariate analysis showed that the risk of one-year poor prognosis increased by 2.8-fold in the presence of acute heart failure Killip III-IV (p = 0.011), by 2.5.-fold - in depression (p = 0.032 ); by 2.1-fold – in DM (p = 0.038), by 1.4-fold in males (p = 0.041), by 1.3-fold in patients older than 65 years (p = 0.043), by – 1.25-fold in smokers (p = 0.032) and by 1.1-fold in case of prior MI (p = 0.044). Multivariate logistic regression analysis identified the following significant predictors of one-year poor prognosis for MI: congestive heart failure, Killip III-IV (OR, 9.5; 95% CI 5.3-12.9; p <0.05), depression (OR 8.7; 95% CI 6.1-11.6, p <0.05), diabetes (OR, 7.4; 95% CI 2.1-16.3; p = 0.002). The predictive power of the regression model was estimated using the ROC-curve (sensitivity of 78%, specificity of 85%). The area under the ROC-curve reached 0.837, indicating a high predictive power of the model.
Conclusion:The multivariate regression analysis suggested the presence of acute heart failure, Killip III-IV, depression (> 49 scores on the Zung scale) and diabetes in the in-hospital period to be significant predictors of one-year unfavorable prognosis in patients with myocardial infarction.
P788
Diagnosis of diabetes mellitus and prediabetes is improved by repeated measurements in patients with acute coronary syndrome
TA Bjarnason1, ES Oskarsdottir2, SO Hafthorsson2, LB Kristinsdottir2, I Olafsson2, K Andersen1
1Landspitali University Hospital, Department of medicine, division of cardiology, Reykjavik, Iceland
2Landspitali University Hospital, Reykjavik, Iceland
Background:Type 2 diabetes (DM2) and prediabetes are established risk factors for coronary artery disease that often go undetected among patients with acute coronary syndromes (ACS). Recent guidelines have recommended oral glucose tolerance test (OGTT) as the most reliable screening tool for prediabetes and DM2 in this patient population. The aim of this study was to determine whether the diagnosis of impaired glucose metabolism could be improved by repeated measurements of glucose metabolism before hospital discharge and 3 months later.
Methods:The Study populations were patients with ACS admitted to a single center coronary care unit with no previous diagnosis of DM2. Glucose metabolism was evaluated with fasting glucose in plasma (FGP), HbA1c and a standard two hour OGTT with 75 mg glucose. Measurements of glucose metabolism were made before hospital discharge (day 2-4 of hospital stay) and repeated three months later. The highest value determined whether patients were classified as having normal glucose metabolism (NGM), prediabetes or DM2.
Results:One hundred and fifty four patients (male 80.5%, mean age 63 years) with no previous diagnosis of DM2 were consecutively included in the study. During hospital stay, 46.8, 40.2, and 13.0% were classified as having NGM, prediabetes or DM2, respectively. Three months later, 40.3, 50.0, and 9.7% were classified as having NGM, prediabetes or DM2, respectively. When combining the results from hospital stay and 3 months later, 28.6, 53.9 and 17.5% were classified as having NGM, prediabetes or DM2, respectively. The classification for glucose metabolism remained the same in 59.7% of patients, 18.2% got better and 22.1% got worse between measurements.
Conclusion:The prevalence of impaired glucose tolerance in patients with ACS and previously undiagnosed diabetes was higher 3 months after hospital stay than during hospitalization. The diagnostic yield was considerably improved by combining results from hospital stay and 3 months later.
P789
Factors associated with above average clinical inertia in treating T2DM patients in primary care
V Bralic Lang1, K Kranjcevic2, B Bergman Markovic3
1Private GP office affiliated to Department of Family Medicine, University of Zagreb, Zagreb, Croatia
2Healthcare Centre Zagreb-Zapad, Family Medicine, Zagreb, Croatia
3Department of Family Medicine, University of Zagreb School of Medicine, Zagreb, Croatia
Background:Clinical inertia is widespread and represents a failure of health care providers to initiate or intensify therapy when indicated. A conjunction of patient's with physician's and health care system's factors is required in order to disentangle true clinical inertia from apparent clinical inertia.
Topic: Sports cardiology
Purpose:To determine factors associated with above average clinical inertia in a given medical consultation, based on variables related to the patient, physician and health care setting.
Methods:National, multicentre, observational, cross-sectional study in primary care. Each family physician (FP) provided professional data and collected clinical data on 15-25 type 2 diabetic (T2DM) patients. Clinical inertia was defined as a consultation in which treatment change based on HbA1c% levels was indicated but did not occur.
Results:449 FPs collected data on 10275 patients. Mean clinical inertia per FP was 55.6% (26.17) of consultations. Patient-related variables accounted for approximately 6% of variance of clinical inertia, while FP-related variables explain 3.3% and health care system's variables explain 3.8% of the variance (Nagelkerke R2= 0.060; 0.033; 0.038). Main FP-related factors associated with clinical inertia above average (cut-off value at 56% of patients) were as follows: oral anti-diabetic drug initiated by diabetologist and years of working experience >23. Main patient-related factors were higher percentage of HbA1c, sedentary lifestyle and smoking habit and main health care setting factor was working status of FP with those who work in private practice outside health care centres or health care center employee beeing more clinically inert.
Conclusions:Patients with worse glycemic control, sedentary lifestyle and smokers experience more clinical inertia and the FPs with more years of working experience are more likely to act inert. More research on causes of clinical inertia, including all aspects of care, should be conducted to achieve more effective diabetes control.
P790
Diabetes mellitus is seriously underdiagnosed after an acute coronary syndrome: results from the RESPONSE randomised clinical trial
HT Jorstad1, WJM Scholte Op Reimer1, JGP Tijssen1, RJG Peters1
1Academic Medical Center, Amsterdam, Netherlands
Topic: Sports cardiology
Purpose:To study the prevalence of undiagnosed Diabetes Mellitus (DM) in post-acute coronary syndrome (ACS) patients.
Methods:Diabetes screening took place in 754 patients in the RESPONSE trial, a multicenter, randomized clinical trial. DM was defined as fasting glucose 1x =11.0 mmol/L or 2x =7.0 mmol/L, or HbA1c 1x =6.5%. Patients were randomised to a structured Nurse Coordinated Prevention Program (?128;?interventions') or to usual care alone (control). As there were no differences between interventions and controls, the 2 are combined in the present analysis. Overall, patients were screened for DM 3 to 7 times in the first 12 months. Results were presented to their treating physicians. Our main outcome was newly diagnosed DM and undiagnosed DM based on clinical records.
Results:At baseline (post-ACS), 101 patients had a diagnosis of DM. At 12 months, 19 additional patients had been diagnosed with DM. In addition to all 120 diagnosed diabetics, as many as 48 patients (29% of all diabetics) remained undiagnosed, in spite of fulfilling the criteria for the diagnosis of DM and these findings being presented to treating physicians.
Conclusion:Despite meeting the criteria for DM, 29% of post-ACS patients with DM were not diagnosed correctly, even after referral to their treating physicians for this purpose. Diagnosis and treatment of DM in post-ACS patients may be greatly improved.
P791
The use of antithrombotic drugs in patients with acute coronary syndromes: the results of a National Registry data.
D Caldeira1, G Morgado1, AC Gomes1, I Cruz1, B Stuart1, C Martins1, H Pereira1
1Hospital Garcia de Orta, Department of Cardiology, Almada, Portugal
Topic: Sports cardiology
Purpose:Antithrombotic drugs are the cornerstone of Acute Coronary Syndrome (ACS) treatment. The use and combination of some of these drugs are markers of quality in ACS care. Therefore, we intended to characterize and evaluate the antithrombotic therapy of ACS patients during hospitalization and at discharge, based on a National ACS Registry data.
Methods:We used data from the ACS National Registry on consecutive patients registered between October 2010 and October 2013. Demographic and clinical characteristics of the population were evaluated. The proportion of patients who were treated according to European guidelines regarding: 1) the inpatient use of dual antiplatelet therapy with ASA and P2Y12 antagonists; 2) the use of low molecular weight heparin (LMWH) and unfractionated heparin (UFH) during the same episode [this is not recommended by ESC guidelines];, 3) the use of LMWH, UFH, fondaparinux and bivalirudin according to the type of SCA. We also estimated the cumulative number of antithrombotic drugs used during hospitalization and discharge.
Results:We assessed data for 8186 patients with ACS were included in the National Registry. About 92.0 % of these underwent dual antiplatelet therapy with aspirin and clopidogrel (regardless of other antithrombotic drugs) during hospitalization. Approximately 14.9 % of patients had both LMWH and UFH in the same hospitalization episode. In patients with ACS without ST-segment elevation (NSTEMI) the use of fondaparinux, LMWH and UFH was respectively 19.2 %, 70.9 % and 17.1 %. In patients with ACS and ST-segment elevation (STEMI) reported the use of bivalirudin was 0.7 %, 50.4% for LMWH, and 46.7% for UFH. During hospitalization, 58.5% of patients had 3 antithrombotic agents. The most common combination was aspirin, clopidogrel and LMWH (overall 38.2%; NSTEMI 49.7%; STEMI 23.1%). At discharge, dual treatment with aspirin and clopidogrel was prescribed in 80.6 % of the cases. About 3.0 % of patients received triple antithrombotic therapy (aspirin, clopidogrel and oral anticoagulant). This registry has included a small proportion of patient receiving the new P2Y12 receptor antagonists such as ticagrelor or prasugrel.
Conclusions:A high proportion of patients received dual antiplatelet therapy in the hospital; however the share of patients with this therapy prescribed at discharge decreased significantly. A considerable number of patients with ACS had in the same inpatient episode both LMWH and UFH. The proportion of fondaparinux and bivalirudin used in NSTEMI and STEMI, respectively, is low.
P792
What do Russian physicians do for stroke prevention in patient with atrial fibrillation: the results of medical documentation analysis
RM Linchak1, AM Nedbaikin2, OG Kompaniets3, D S Komkov1
1State Research Centre for Preventive Medicine, Moscow, Russian Federation
2Cardiologic Dispensary of Bryansk Region, Bryansk, Russian Federation
3Kuban State Medical University, Krasnodar, Russian Federation
Topic: Sports cardiology
Purpose:To evaluate Russian physicians` strategy for antithrombotic drugs prescription in patients with atrial fibrillation Methods:There were analyzed 571 outpatient cards in three regions of Russia (Moscow, Bryansk, Krasnodar). We assessed the strategy for antithrombotic drugs prescription in atrial fibrillation and for those patients who taking warfarin we additionally evaluate INR control rate.
Results:According to data received during outpatient cards analysis the most of patients (53,7% in total) with high stroke risk have been receiving antithrombotic drugs (aspirin alone 49,4%, clopidogrel alone 2,5%, aspirin+clopidogrel 1,8%). Furthermore, 13,3% of patients haven't been receiving any antithrombotic drug. The rest of their (33%) have been taking different anticoagulants including warfarin (25,2%), rivaroxaban (3,4%), dabigatran (2,3%), warfarin+aspirin (1,9%), dabigatran+aspirin (0,2%). From those patients who have been taking warfarin only 19,6% have controlled INR monthly. But 21% haven't ever done it. From those who have been controlling INR monthly only 44% had INR in the target range.
Conclusion:Our study showed that the most of patients with atrial fibrillation taking antiplatelets for stroke prevention, one of 4 patients receiving warfarin and nearly 5% of patients receiving "novel" anticoagulants. From those who are taking warfarin only 44% get effective INR control. So, in total only about 10% of patients with atrial fibrillation receiving effective therapy for stroke prevention.
P793
May the combustion not checked of urban refusals increase the cardiovascular risk?
M L De Rosa1, M Cerini2, L Cerini3
1University Hospital Federico II, Naples, Italy
2Nuclear Dept, Politecnico of Milan , Milan, Italy
3Economics and Menagment of Innovation andTechonology,Bocconi University, Milan, Italy
Background:A cardiovascular health (CH) survey of 1203 persons (P)in households located near the hazardous waste disposal sites, Campania, region of Southern Italy, was conducted from 2009 until today to assess whether rates of adverse CH outcomes were elevated among P living near the sites Methods:Data included a household questionnaire, medical records of reported cardiovascular diseases (CD) certificates and hospital admission for CD from our database Results:The study areas appeared similar with respect to mortality, cancer incidence, and pregnancy outcomes. In contrast, rate ratios were greater than 1.5 for 2 of 19 reported disease, i.e., angina pectoris, and strokes. Prevalence odds ratios for 23 symptoms (S) were uniformly greater than 1.0, and 12 S had odds ratios greater than 1.5: anginal pain, deep, frightening, sometimes burning, typically triggered by physical activity ,dyspnea with a feeling of suffocation, pale skin, the state of anguish and terror of P, accompanied by palpitations, faintness, marked fatigue, nausea ,vomiting. The apparent broad-based elevation in reported disease and S may reflect increased perception or recall of conditions by P living near the sites. There are few data on the full range of regulated community air pollutants (CAP) as PM2,5, sulfur and nitrogen dioxide, carbon monoxide and ozone. The our study considered all CAP and found cardiovascular risk associated only with PM2.,5 concentrations, which might derive from uncontrolled burning of municipal solid waste in particular sites of our region. Our analysis demonstrated a relationship between increased levels of eventual fine particulate CAP and higher rates of death and complications from cerebrovascular and CD, depending not only on which city a P lived in but also on where in that city P lived Conclusions:Combustion not checked of urban refusals releases a number of toxic substances, most in small quantities and at extremely low levels. Because of the wide range of CAP, the different pathways of exposure, long-term low levels exposure, and the potential for synergism among the CAP, concerns remain about potential CH but there are many uncertainties involved in the assessment:
P794
The beta blockers in stable chronic heart failure - two years of experience from CIBIS ELD study
S Apostolovic1, D Stanojevic1, R Jankovic-Tomasevic1, S Salinger-Martinovic1, D Djordjevic-Radojkovic1, M Damjanovic1, M Pavlovic1, E Tahirovic2, HD Dungen2
1Clinic for Cardiovascular Diseases, Nis, Serbia
2Charite - Campus Virchow-Klinikum, Department of Internal Medicine-Cardiology, Berlin, Germany
Introduction:CIBIS ELD study included 876 patients from Germany and South Eastern Europe with chronic heart failure (CHF). The average patients' age was 73 years, 58.5% were male, and 63% had systolic CHF. We gradually increased the dose of carvedilol or bisoprolol for 3 months to the maximal tolerated dose.
Aims and results:In the subsequent CIBIS ELD FOLLOW UP 24 MONTHS study 75.7% of our patients were alive, 20.9% died and 3.3% were lost to follow up. The aim of this sub-study was to investigate whether the patients were on beta-blocker after the end of titration. For 172 patients we do not have data on used beta blocker. 89.1% of patients from whom we could get data had beta blocker in therapy and 84.9% of them did not change beta blocker since the end of titration period (carvedilol or bisporolol). The most common reasons for excluding beta blocker from therapy were bradycardia (0.7%), hypotension (0.5%), decision of general practitioner (0.5%) and in 2% of patients the reason was unknown. We found that the average doses of beta blockers were significantly lower (bisoprolol - 5 mg vs. 10 mg and carvedilol - 3.125 mg vs. 50 mg). Majority of patients (59.7%) were in NYHA class II, 22.1% in NYHA class I, 14.7% in NYHA class III and only 3.5% in NYHA class IV. The average systolic pressure was 136.6±21.7 mmHg and diastolic 77.5±12.3 mmHg, while the average heart rate was 69.8±12.6/min. 68.3% of patients were not hospitalized due to worsening heart failure in the previous 12 months, while 0.5% of patients had 6 hospitalizations during the same period. The average number of hospitalizations during 24 months was 0.51±0.992. We did not find significant difference between having or not beta blocker in therapy among patients in different NYHA classes, with or without peripheral edema (22.5% vs.75.6%), dyspnea at exercise (74.3% vs. 25.7%), jugular venous distension (1.9% vs. 89.1%), pulmonary rales (2.6% vs. 79.5%), number of hospitalizations due to heart failure, while all patients with dyspnea at rest (8.3%) had beta blocker therapy vs. those without (?=4.369, p=0.019).
Conclusion:24 months after the end of titration period we found that majority of our patients had stable CHF and that they had unchanged beta blocker in therapy. Type of beta blocker was the same while the dose was significantly lower since the end of titration. Patients had normal blood pressure and heart frequency. Beta blockers remain the cornerstone in CHF therapy with an accent on symptoms/blood pressure/heart frequency guided dosage.
P795
Behavior cardiovascular risk factors prevalence in randomly selected Russian population aged 25-44 years
Y Balanova1, A Kontsevaya1, S Shalnova1, A Deev1, A Konradi2, O Rotar2, Y Zhernakova3, E Oschepkova3, S Boytsov1
1National Research Center for Preventive Medicine, Moscow, Russian Federation
2Federal Almazov Medical Research Centre, Saint Petersburg, Russian Federation
3Russian Cardiology Research and Production Complex, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:To evaluate the prevalence of behavior cardiovascular risk factors among randomly selected respondents aged 25-44 years in Russian population.
Material and methods:A cross-sectional survey - Epidemiology of cardiovascular diseases in different regions of Russian Federation (ESSE-RF) was carried out in randomly selected males (N=3284) and females (N=4041) aged 25-44 years in 12 Russian regions (Volgograd, Vologda, Voronezh, Ivanovo, Kemerovo, Samara, Orenburg, Tomsk, Tyumen, St.Petersburg, Republic of North Ossetia-Alania), response rate>80%. Standard epidemiology methods and criteria were used. A person was considered to be a current smoker if smoke at least one cigarette per day; alcohol abuse was considered in males drank =168 g of ethanol per week, females =84g. Obesity was defined as body mass index>30kg/m2. Dietary habits were assessed by questionnaire.
Results:Current smoking prevalence was higher for males than females: 47.8 vs 19.2% in the 25-34-year age group, 44.6 vs 17.2 % in the 35-44-year age group. Prevalence of alcohol abuse was also higher for males, the highest prevalence was observed in the 35-44-year age males (9.3%), p<0.005. The highest prevalence of physical inactivity was noted in females, p<0.005 (for example in age group 25-34 – 46.8%). Prevalence of obesity increased with increasing age (males: from 14.3% in the 25-34 -year age group to 26.6% in the 35-44-year age group; females: from 10.5% i to 24.5% respectively, p<0.0005). Excess salt intake was revealed in half of the surveyed (males: 25-34 – 51.8%; 35-44 –55.2%; females – 47.0% and 45.5% respectively). The highest prevalence of low vegetables and fruits intake was found in males aged 25-34 – 57.2%, p<0.005; low fish and seafood consumption – in females aged 25-34 – 45.2%, p<0.005.
Conclusions:Prevalence of behavior cardiovascular risk factors among randomly selected Russian population aged 25-44 years is high. Reducing of cardiovascular risk prevalence is a very important resource for CVD mortality decreasing in RF.
P796
Lack of association between meat intake and 10-year (2004-2014) cardiovascular disease outcomes in acute coronary syndrome patients: The Greek study of acute Coronary Syndrome.
M Kouvari1, V Notara1, D B Panagiotakos1, Y Kogias2, P Stravopodis3, G Papanagnou4, S Zombolos5, Y Mantas6, C Pitsavos7
1Harokopio University, Athens, Greece
2Cardiology Clinic, General Hospital of Karditsa, Karditsa, Greece
3Cardiology Clinic, General Hospital of Zakynthos Island, Zakynthos, Greece
4Cardiology Clinic, General Hospital of Lamia, Lamia, Greece
5Cardiology Clinic, General Hospital of Kalamata, Kalamata, Greece
6Cardiology Clinic, General Hospital of Chalkida, Chalkida, Greece
7Hippokration Hospital, University of Athens, Athens, Greece
Topic: Sports cardiology
Purpose:There is very recent literature suggesting that red meat consumption is not associated with cardiovascular disease (CVD) outcomes in the general population, whereas processed meat seems to exert its harmful role. However, there is limited knowledge regarding the effect of meat consumption on cardiac outcomes among CVD patients. We sought to evaluate the association of long-term red meat consumption with CVD outcome of patients who have had suffered an Acute Coronary Syndrome (ACS).
Methods:From October 2003 to September 2004 a sample of 2.172 ACS consecutive patients from 6 major Greek hospitals was selected. In 2013-14, the 10-year follow-up was performed in 1.918 participants (88% participation rate). Logistic regression models were applied to evaluate the effect of red meat consumption (as assessed by using a validated semi-quantitative food frequency questionnaire) on CVD incidence.
Results:No association was observed between red meat intake and CVD incidence, after taking into account various potential confounders; in particular, red meat intake 1-2 times/week was not associated with development of CVD (odds ratio=0,881, 95% confidence interval 0,543, 1,429, p=0,607), similarly, 3-5 times/week [0,869 (95%CI 0,530, 1,425, p=0,577)] and >5 times/week [0,785 (95%CI 0,445, 1,385, p=0,404)].
Conclusion:Red meat consumption seems to have no influence on the prognosis of ACS patients; suggesting that the dietary management of ACS patients should, probably, focus on other components of saturated fat intake, such as restriction of processed meat.
P797
Time limiting definitions misclassify SUD victims
C A Nwosu1, N D Mehta1, I W Pursell1, R J Simpson1, P Nanavati1, M E Lewis1, O O Osehobo1, J P Mounsey1, E H Chung1
1University of North Carolina Hospitals, UNC Division of Cardiology and Cardiac Electrophysiology, Chapel Hill, United States of America
Standard definitions of sudden unexpected death (SUD) may place an over reliance on witnessed death, timing of symptom onset and time since last seen alive; leading to under reporting of SUD incidence, mischaracterization of its predictors and misclassification of individuals at greatest risk. To address these potential concerns, we calculated the annual incidence of SUD in a North Carolina (NC) cohort based on clinical presentation rather than time limits and then recalculated it using published criteria. SUDDEN is a prospective study of SUD. Emergency Medical Services in Wake County, NC referred consecutive presumed SUD subjects. Medical and public records were collected and a panel of 3 cardiologists reviewed all data to determine SUD victims. A systematic literature review identified 5 studies that calculated SUD incidence; their criteria were applied to our cohort. Incidence rates were adjusted for timing, witnessed death, age, cause of death, attempted resuscitation, and survivor status. Discrepancies between the criteria were analyzed. Figure 1 shows estimated SUD incidence for each of the published studies compared to SUDDEN. SUDDEN criteria estimated a 3-fold higher incidence. Two thirds of subjects with SUD would have been excluded if witnessed death or short duration of time since last seen alive are required. Qualitative assessment shows overwhelmingly that African Americans, females, and the socioeconomically deprived are excluded in previous studies. Incidence of SUD varies greatly by criteria. Timing limiting criteria are imprecisely characterized and often unknown. Excluding victims by these criteria under reports the incidence of SUD and overlooks underserved populations. Understanding the incidence and predictors of SUD will help in prevention.
SUDDEN (Figure 1)
P798
Physical activity and sport participation for people with long-term illness
N Heron1, ME Cupples1, F Kee1, MA Tully1
1Queen's University of Belfast, Department of General Practice, Belfast, United Kingdom
Topic: Sports cardiology
Purpose:Physical activity is recommended for optimal prevention of cardiovascular disease(CVD) and participation in sport is associated with improved well-being. However, people with long-standing illness/disability are less likely to participate in sport than others. Evidence of factors associated with their participation is limited and the best approach to encourage participation is unknown. This study aimed to identify sport participation levels and their correlates, among adults with long standing illness/disability in Northern Ireland, where CVD prevalence is high. Method:Using routinely collected data in annual surveys of population samples from 2007 to 2011, descriptive statistics were derived. Chi-squared tests were used to compare characteristics of those with a long-term illness/disability and those without long-term health problems. Uni-variate binary regression analysis for the whole sample and those with a long-standing illness/disability, using sport participation as the dependent variable, was performed and variables with a p-value of 0.1 or less were taken into a multi-variate analysis.
Results:The sample included 13,683 adults; 3550(26%) reported having long-term illness/disability. Fewer of those with, than without, long-term illness/disability reported sport participation in the previous year (868/3550(24.5%) v 5615/10133(55.6%)). Multi-variate analysis showed that, for those with long-standing illness/disability, being single and less socio-economically deprived correlated positively with sport participation. For both those with long-standing illness/disability and the full sample, sport participation correlated positively with being male, aged <56 years, access to a household car/van, sports club membership, health ?128;?fairly good' or ?128;?good' in the previous year, doing paid/unpaid work, and living in an urban location. For the full sample but not those with long-standing illness/disability, sport participation correlated positively with being a non-smoker, higher educational status and personal internet access. Of note, personal internet access was less for those with, than without, long-term illness/disability (41% v 70%).
Conclusions:Efforts to promote physical activity in sport for those with long-standing illness/disability should target older people, married females, those who live rurally, and those who are socio-economically deprived and report their health as ?128;?not good'. Implementation of initiatives should not rely on the internet, to which these people may not have ready access, to help support their sport participation and physical activity in optimal CVD prevention.
P799
Relation between knowledge on cardiovascular disease (CVD) risk factors and the risk of death in urban residents.
A Wasniowska1, M Kozela2, A Pajak2
1John Paul II Hospital, Department of Diagnostics, Krakow, Poland
2Institute of Public Health, Department of Epidemiology and Population Studies, Krakow, Poland
Low education is associated with the higher risk of death, in particular from cardiovascular disease (CVD). Less is known, to what extent this relation is explained by the better knowledge on CVD prevention and to what extent it is explained by the other characteristics which are related to higher socioeconomic status of people with high education.
Objective:to assess the relation between knowledge on risk factors and the risk of death from all causes Methods:the study group was a random sample of 3544 persons selected from a population of urban residents at age 45-64 years. Knowledge on CVD risk factors was assessed by a set of 15 standard questions. Participants were followed for up to 15 years. Information on deaths was obtained from the municipal registry. Cox proportional hazards model was used. Statistical significance was assessed at the level of p<0.05.
Results:1152 men and 1158 women were included in the analysis (participation rate: 66% and 65% respectively). Only 39% of men and 34% of women had less than secondary education. Most of risk factors were identified correctly by at least 90% participants. However, noticeable proportion of participants considered protective factors or lifestyle characteristics as risk factors. The median time of follow-up was 14,35 years (interquartile range =14.30-14.39). Survival analysis involved 31.188 person years. There were 211 deaths in men and 96 in women. After adjustment for age, men with low level of knowledge on risk factors had higher risk of death by 40% compared to men with high level of knowledge. The relation was significant after adjustment for occupational activity and marital status. However adjustment for education attenuated the association. After stratification by education, in men with secondary education or higher, an inverse, independent of age, relation between the knowledge on risk factors and the risk of death was found (HR=1,60, 95% CI=1.04-2,48). In this group, the differences in the exposures to risk factors were in favor for persons with more knowledge on risk factors but were insignificant. In men with low education and in women risk of death was not associated with knowledge on risk factors.
Conclusions:In urban population with high level of education, the association between knowledge on CVD risk factors and the risk of death depended on sex and education. Lower level of knowledge on risk factors was associated with a higher risk of death only in men with secondary or higher education. This association could not be explained by differences in the exposure to main CVD risk factors.
P800
Sudden unexpected death: variability in reporting between the United States and Germany
O Osehobo1, M Lewis1, C Virus2, I Pursell1, C Nwosu1, J Mounsey1, E Chung1, R Simpson1
1University of North Carolina Hospitals, UNC Heart & Vascular, Chapel Hill, United States of America
2University of North Carolina Hospitals, McAllister Heart Institute, Chapel Hill, United States of America
ICD-10 coding was developed in order to provide uniform classification of disease and to accurately guide the appropriate allotment of resources towards prevention. However, country-specific modifications of the manual and differences in methodologies can result in inconsistent reporting of conditions such as sudden unexpected death (SUD). To elucidate the specific areas of inconsistencies, we examined the distribution of ICD-10 codes of SUD across two Western industrialized countries. Death certificates in Germany and the United States (US) for 2011 were compared by ICD-10 categories for SUD. These codes were designed to classify the order, type, and association of events resulting in death. Subjects between 20 and 64 years old whose deaths were attributed to diseases of the circulatory system (I05-I09, I11, I20-I52) and unknown causes of death (R96-R99) were included. In 2011, among those aged 20 to 64 years, there were 133,808 deaths (20.6% SUD) in Germany and 639,276 deaths (19.5% SUD) in the US. However, the reported causes of these SUDs differ between the two countries. In Germany, reports of unknown cause of death were 5 times higher than in the US (see Figure). In the US, there was a higher reported incidence of death attributed to hypertensive or atherosclerotic disease. Germany and the US have similar rates of SUD. Underreporting of unknown causes of death and overreporting of hypertensive and atherosclerotic disease in the US appear to account for most of the difference in the distribution of the etiologies of SUD between Germany and the US. Variability in application of ICD-10 codes may impair our understanding of the diverse risk factors for sudden death.
P801
Ethnic differences in chronic kidney disease in theNetherlands
C O Agyemang1, MB Snijder1, DN Adjei1, L Vogt1, BJ Van Den Born1, JJ Ujcic-Voortman1, P Modestie2, RJ Peters1, K Stronks1
1Academic Medical Center of Amsterdam, Public Health, Amsterdam, Netherlands
2University of Florence, Florence, Italy
Background:Chronic kidney disease (CKD) is increasingly recognized as a major public health and clinical burden. Evidence suggests important ethnic differences in kidney diseases mainly in the USA, but the data among various ethnic groups in Europe, particularly Mediterranean and Sub-Saharan African, are lacking. We sought to assess differences in the prevalence of CKD between European Dutch and the various ethnic minority groups in Amsterdam, the Netherlands. Furthermore, we assessed whether the convention risk factors contributes to the observed differences.
Methods:Baseline data from the HELIUS study were used including 1849 European Dutch, 1711 South-Asian Surinamese, 1879 African Surinamese, 1337 Ghanaians, 1852 Turks, and 1252 Moroccans aged 18-70 years. CKD status was assessed using the new Kidney Disease: Improving Global Outcomes (KDIGO) classification. Comparisons among groups were made using proportions and age-adjusted prevalence ratios.
Results:The age-standardised prevalence of CKD was higher in all the ethnic minority groups ranging from 4.7% (95% CI, 3.7-5.6%) in African Surinamese to 8.3% (6.8%-9.5%) in Turkish compared with European Dutch (3.1%; 2.3-3.8%). After multivariable adjustment, except for African Surinamese, prevalence ratios were higher in Turkish (1.79; 1.31-2.45), South Asian Surinamese (1.55; 1.16-2.06), Moroccans (1.41; 1.00-2.00), and to a lesser extent in Ghanaian (1.35; 0.98-1.86) people than European Dutch. Similar higher prevalence rates were found when the CKD was stratified into moderate risk and high risk. However, the differences among the risk group were mainly explained by differences in education level, smoking, hypertension, BMI, diabetes, and hypercholesterolemia.
Conclusions:Our findings indicate a higher prevalence of CKD in ethnic minority groups than in European Dutch. The differences in high risk CKD group were mainly explained by modifiable risk factors suggesting that effective public health and clinical interventions to reduce these modifiable risk factors may help to reduce ethnic inequalities in CKD.
P802
The effect of moderate red wine consumption on 24-h blood pressure trajectory in type 2 diabetes; a six-month randomized controlled intervention trial
Y Gepner1, Y Henkin2, D Schwarzfuchs1, R Golan1, R Durst3, I Shelef2, I Harman-Boehm2, M J Stampfer4, A Rudich1, I Shai1
1Ben-Gurion University of the Negev, Department of Public Health, Beer-Sheva, Israel
2Ben-Gurion University of the Negev, Soroka University Medical Center, Beer-Sheva, Israel
3Hadassah University Medical Center, Jerusalem, Israel
4Harvard Medical School, Boston, United States of America
Aims:Observational studies report inconsistent associations between moderate alcohol intake and blood pressure (BP). In a 6-month randomized controlled trial we assessed the effect of initiating moderate red wine consumption on 24h-dynamics BP, specific time-intervals of BP, and its interaction with a common genetic variant of alcohol-dehydrogenases (ADH) among patients with type-2-diabetes.
Methods:We randomly assigned 54 type-2-diabetes patients, alcohol abstainers, to initiate consumption of 150ml dry red-wine or mineral-water at dinner. Both groups were guided to adhere to Mediterranean diet, without caloric restriction. We measured 24h ambulatory-blood-pressure-monitoring (ABPM) and ADH1B polymorphism.
Results:Participants (age=57yrs;85% men;24h blood pressure=129/77mmHg) had 92% six-month retention. After 6-month intervention, average 24hr BP did not differ between the wine and water groups. The ABPM decreased in the red-wine group at midnight (3-4 hours after wine intake: systolic BP: red-wine=-10.6mmHg vs. mineral-water=+2.3mmHg; p=0.031) and the following morning at 7-9AM (systolic BP: red-wine:-6.2mmHg vs. mineral-water:+5.6mmHg; p=0.014). Among the red-wine consumers, only the individuals who were homozygous for the gene encoding ADH1B*2 variant (Arg48His;rs1229984,TT, fast ethanol metabolizers), exhibited a significant decrease in mean 24h systolic BP (-8.0mmHg vs. +3.7mmHg; p=0.002) and pulse pressure (-3.8mmHg vs. +1.2mmHg; p=0.032) compared to heterozygotes and homozygous for the ADH1B*1 variant (CC, slow metabolizers). No genetic interaction was observed for the water group.
Conclusions:Initiating moderate red-wine consumption at dinner in type-2-diabetics may have modest hypotensive effects within several hours after its consumption, and the following morning. The genetic interaction uncovers a personalized/precision-medicine factor regulating the hypotensive effect of red-wine in diabetes.
P803
Pregravid cardiovascular risk factors in the prediction of gestational hypertension and preeclampsia. A cohort Norway and Medical Birth registry of Norway Linkage study
G Egeland1, K Klungsoyr1, N Oyen2, GS Tell2, O Naess3, R Skjaerven2
1Norwegian Institute Of Public Health, The Cardiovascular Registry, Bergen, Norway
2Dept of Global Public Health and Primary Care, Bergen, Norway
3Norwegian Institute of Public Health, Division of Epidemiology, Oslo, Norway
Topic: Sports cardiology
Purpose:To evaluate the extent to which preexisting CVD risk factors predicted gestational hypertension and preeclampsia.
Methods:Female participants in Cohort Norway (CONOR) health surveys, 1994-2003, were prospectively followed via record linkages to the Medical Birth Registry of Norway (through 2012) for ascertainment of gestational hypertension (without proteinuria) and preeclampsia. Those with preexisting hypertension or a multiple birth pregnancy were excluded leaving 14,615 singleton pregnancies for analyses. Multivariate multinomial regression included important covariates: age, smoking, parity, baseline blood pressure, preexisting diabetes, a history of gestational hypertension and preeclampsia in a prior pregnancy, and time between CONOR and delivery. Results Mean (SD) age at baseline was 28 yrs (4.4) and the mean length of follow-up was 4.6 yrs (3.5). Gestational hypertension was noted for 251 and preeclampsia for 455 pregnancies. Overweight and obesity, a family history of diabetes, women's preconception diabetes, and baseline blood pressure were significant risk factors for both gestational hypertension and preeclampsia. However, for preeclampsia, numerous other CVD risk factors were significant: high total/HDL-C ratio (>5)(OR=1.8, 95% CI 1.2-2.6), high nonHDL-C (4th quartile vs. 1st quartile OR=1.7, 95% CI 1.2-2.4), high triglyceride (4th quartile vs. 1st quartile OR=1.9, 1.4-2.6), and a family history of myocardial infarction (OR=1.9, 1.4-2.5) and stroke (OR=1.6, 1.1-2.4). Further, weekly light physical activity reduced and binge drinking increased risk for preeclampsia but no associations were observed between these parameters and gestational hypertension.
Conclusion:Our findings support that pregnancy is a "stress test" for women with underlying familial and acquired CVD risk. The CVD risk factors significant for preeclampsia, but not for gestational hypertenstion, suggest a potential role of these risk factors in placentation/placental perfusion, and maternal responses to a poorly perfused placenta.
P804
Alcohol consumption and incidence of atrial fibrillation and heart failure: prospective findings from the MOLI-SANI study
A Di Castelnuovo1, S Costanzo1, L Rago2, A De Curtis1, M Persichillo1, M Bonaccio1, F Bracone1, MB Donati1, G De Gaetano1, L Iacoviello1
1IRCCS, Mediterranean Neurological Neuromed Institute, Pozzilli, Italy
2Epicomed Research Srl, Campobasso, Italy
Purpose The connection between ethanol intake and atrial fibrillation (AF) or heart failure (HF) remains controversial. We assessed the hypothesis that alcohol consumption predicts onset of AF or HF.
Methods:We analyzed 22,420 (47% men, age=35) AF or HF–free individuals randomly recruited from the general population included in the MOLI-SANI study, for whom complete data on HF, AF and alcohol were available. The cohort was followed for a median of 4.2 years (91,930 person-years). Alcohol intake was categorized in former, never, occasional (<1 gr/day) drinkers and in four categories of consumers with different intake (Table). Incident cases were identified through linkage to the regional archive of hospital discharges. The end of follow-up was 31/12/2011. Hazard ratios (HRs) were calculated using Cox-proportional hazard models (Table). Results We identified 546 incident cases of HF and 352 of AF. In comparison with never drinkers, both former or occasional drinkers showed an equal risk of developing HF (Table). Drinking at various amount of alcohol revealed a J-shaped protection against HF, with a 25% (95%CI: 1% to 44%) maximum protection at 2-4 drinks a day, independent from common confounders (Table). Concerning AF, we failed to observe any association of alcohol with onset of it. Very similar results were obtained after restriction of the analyses to only men/women or to type of alcoholic beverages (wine, beer or liquor).
Conclusions:Consumption of alcohol in moderation prevent the incidence of heart failure of 25%, whereas it was not associated with development of atrial fibrillation.
*Adjusted for age, sex, smoking, education, income, physical activity, body mass index, total calories intake, history of cardiovascular disease, hypertension or diabetes
Former drinkers
Never drinkers
Occasional drinkers
1-12 gr/dy
13-24 gr/dy
24-48 gr/dy
>48 gr/dy
N
750
6051
1427
4499
3447
4111
2135
Heart Failure (546/22420, 2.44%)
Rate of event
32 (4.3%)
125 (2.1%)
31 (2.2%)
90 (2.0%)
88 (2.6%)
118 (2.9%)
62 (2.9%)
Hazard Ratios*
1.10 (0.75-1.63)
-1-
1.05 (0.71-1.57)
0.86 (0.65-1.13)
0.79 (0.60-1.06)
0.75 (0.56-0.99)
0.80 (0.56-1.15)
Atrial Fibrillation (352/22228, 1.58%)
Rate of event
14 (4.0%)
69 (1.2%)
9 (0.6%)
59 (1.3%)
60 (1.7%)
93 (2.3%)
48 (2.3%)
Hazard Ratios*
0.88 (0.49-1.57)
-1-
0.57 (0.28-1.14)
1.07 (0.75-1.52)
0.96 (0.67-1.38)
1.09 (0.77-1.54)
1.14 (0.75-1.72)
P805
Heart failure following incident acute myocardial infarction (AMI); the effect of time from and age at AMI hospitalization - a CVDNOR project
G Sulo1, O Nygaard2, SE Vollset1, J Igland1, E Sulo1, G Egeland3, M Ebbing3, GS Tell1
1Department of Global Public Health and Primary Care, Bergen, Norway
2Haukeland University Hospital, Department of Heart Disease, Bergen, Norway
3Norwegian Institute of Public Health, Department of Health Registries, Bergen, Norway
Topic: Sports cardiology
Purpose:Coronary heart disease is the main cause of heart failure (HF), which is associated with high mortality. We aimed at analyzing the occurrence of HF beyond the acute phase of AMI as a function of age and time from AMI hospitalization, using patients hospitalized for an incident (first) AMI in Norway during 2001-2009.
Methods:Patients hospitalized for a first AMI were retrieved from the Cardiovascular Disease in Norway project. They were followed for a new hospitalization with a diagnosis of HF (ICD-10 code I50) through 2009. Gender-specific incidence rates (IR) per 1000 person-years were calculated by time from and age at AMI hospitalization.
Results:A total of 102 975 AMI patients (60.8% men) were included. Women were on average 8 years older than men [74.8 (12.8) vs. 66 (13.7) years]. In 20.6% of the cases, HF was present at arrival or developed during the AMI hospitalization. Among the remaining patients, 76378 (93.4%) were discharged alive. During a median follow up of 2.6 years, 9707 patients (12.7%) were hospitalized for an episode of HF. Overall, HF incidence rates (95% CI), per 1000 person-years, were 33.5 (32.6 - 34.4) for men and 53 (51.4 – 54.6) for women. Rates were highest during the first year following the AMI [66 (63.6 – 66.5) in men and 98.8 (94.6 – 103.8) in women]. After the third year the incidence rates dropped to nearly 1/3 and remained stable throughout follow up (Figure). HF incidence rates were strongly influenced by age at AMI hospitalization, in men ranging from 8.9 (3.7 – 21.4) among 20-29 year-olds to 156.3 (137.1- 178.1) in those 90 + years, in women ranging from 0 in 20-29 year-olds to 146.7 (134 – 160.4) in those 90+ years.
Conclusion:- HF is a common complication following AMI. It follows a time-dependent fashion and is strongly influenced by age.
P807
Variables of negative ischemic exercise test improve prediction of subclinical carotid atherosclerosis based on traditional cardiovascular risk scoring
N Katamadze1, L Berstein1, Y Grishkin1
1North-western state medical university named after I.I.Mechnikov , Saint-Petersburg, Russian Federation
Topic: Sports cardiology
Purpose:We studied the value of negative exercise test in asymptomatic pts in prediction of the extent of carotid atherosclerosis compared to that of a standard cardiovascular risk scoring algorithm.
Methods:This cross-sectional study included 217 pts aged 54,3±8 years (48% females) with =1 traditional cardiovascular risk factors and no evidence of clinical atherosclerotic disease. Cardiovascular risk was estimated by SCORE algorithm. All pts underwent ultrasound imaging of 3 extracranial carotid segments including measurement of intima-media thickness (cIMT), detection of atherosclerotic plaque and calculation of total plaque area (TPA). Exercise treadmill test was performed by Bruce protocol; only subjects with negative ischemic test results were included.
Results:184 (85%) of pts had low or moderate risk (SCORE <5%). The IMT values were 0,8±0,15 mm in common carotid artery (CCA), 1,29±0,5 mm in bifurcation (BIF) and 0,82±0,4 mm in internal carotid artery (ICA). Carotid plaque was present in total of 83 (38%) participants. The median TPA was 0 [0,16] cm2. The level of risk by SCORE was positively associated with IMT measured in all three carotid sites and TPA (?0,04, 95% CI 0,04-0,05 for CCA; 0,07, 95% CI 0,04-0,09 for BIF; 0,03, 95% CI 0,02-0,04 for ICA; 0,04, 95% CI 0,03-0,05 for TPA, respectively, p<0,0001 for all regressions). R2of SCORE values for prediction of cIMT in CCA, BIF and ICA were 0,239, 0,063 and 0,036, respectively, and 0,158 for prediction of TPA. SCORE predicted the presence of plaque with AUC=0,706. In multivariable SCORE risk-adjusted regression models resting heart rate, peak systolic blood pressure, increase in heart rate and systolic blood pressure, exercise capacity independently predicted cIMT in all three sites and TPA. Models including these exercise test variables were inferior to SCORE in prediction of CCA cIMT and TPA with R2of 0,187 and 0,07 respectively, however worked better than SCORE in prediction of cIMT in BIF and ICA with R2of 0,083 and 0,077, respectively. There ability to predict a carotid plaque was similar to that of SCORE (AUC=0,704). Adding exercise test variables to SCORE value improved prediction of cIMT in all segments (R20,291, 0,124 and 0,083 for CCA, BIF and ICA, respectively) and TPA (R2=0,188) as well the presence of plaque (AUC=0,758).
Conclusions:Variables of negative ischemic stress test in asymptomatic pts with predominantly low or moderate cardiovascular risk improve detection of subclinical carotid atherosclerosis compared to standard risk assessment algorithm and thus may be of value for screening purposes.
P811
Telomere length and myocardial infarction, Is longer really better? the HUNT2 study.
IB Oyen Osthus1, J Nauman1, S Lydersen2, H Dalen1, U Wisloff1
1Norwegian University of Science and Technology, Institute of Circulation and Medical Imaging, Trondheim, Norway
2Norwegian University of Science and Technology, Regional Centre for Child and Youth Mental Health and Child Welfare, Trondheim, Norway
Topic: Sports cardiology
Purpose:As possible markers of biological age, telomeres have been related to age-related diseases such as myocardial infarction (MI). The association between telomere length (TL) and MI has so far been studied to limited degree, and found negative or no associations. Most of the data have been sampled post-event through case control studies, and the few prospective cohort studies have not excluded participants with previous cardiovascular disease, which is believed to be associated with shorter TL. The measure of TL in participants with previous CVD, which in case-control studies have been associated with shorter TL, represent a bias as previous CVD also is a risk factor for suffering a new CVD event. A prospective cohort of a population healthy at baseline may help unveil the role of telomeres in MI.
Methods:919 participants from a large Norwegian population-based cohort (HUNT-2) 65 years or older and free of known CVD, diabetes and hypertensive medications were followed for a mean of 11.5 years for incident of MI. DNA was extracted from blood leukocytes and mean relative TL measured by quantitative PCR.
Results:Hazard ratios (HR) for incidence of MI, using relative TL as a continuous variable in a Cox-regression model, showed a prominent higher risk of MI in participants with longer telomeres; with HR of 3.07 (95% CI; 1.57 to 5.99, p=0.001) in men, and 2.82 (95% CI; 1.23 to 6.50, p=0.02) in women. Compared with the bottom tertile of telomeres, HR of incident MI in top tertile of telomeres was 3.88 (95% CI; 1.56 to 9.62, p=0.003) in men and 3.11 (95% CI; 1.12 to 8.59, p=0.03) in women. Longer telomeres in participants 65 years or older seem to increase the incidence of MI in at baseline healthy participants. This indicates that telomere length as an indicator of cardiovascular risk may not be as simple as "the longer, the better".
P813
Regional features risk factors for heart disease: focus on arterial hypertension in the Ryazan region (Meridian-Ro study)
E Philippov1, S Iakushin1
1Ryazan State Academician I.P. Pavlov Medical University, Ryazan, Russian Federation
Arterial hypertension is one of the major risk factors that make a significant contribution to cardiovascular mortality. 35.5% of premature deaths in Russia is associated with hypertension.
Objective:To investigate the prevalence of hypertension and its treatment efficiency in the typical Russian region.
Methods:The study included persons aged 25-64 years. They conducted a survey on a standardized questionnaire, electrocardiogram, measurement of endothelial function, measurement of blood pressure, heart rate, waist circumference, height, weight, intake of biological samples for the determination of biochemical risk profile, a comprehensive risk assessment using the SCORE scale adapted for the Russian Federation. The study MERIDIAN-RO included 1622 people (1220 and 402 urban - rural population), of which 42.6% were male, 53.8% - women.
Results:The prevalence of hypertension was 45.9% among the urban population - 49.3%, among the rural - 44.8%. The average age of the population studied in the city was 47.5 (46,3-48,5) years in rural areas - 47.9 (46,5-49,3). Mean SBP / DBP was higher in urban than in rural areas (141.8 / 90.4 vs. 135.4 / 83.6 mmHg, p <0.001). At the risk of hypertension, according to our data, influenced: smoking (relative risk (RR) 1.23, 95% confidence interval (CI) 1,11-1,37), obesity (1.93; 1,73-2, 14), endothelial dysfunction (1,42; 1,15-1,75), diabetes (1.34; 1,16-1,54). Factors such as excessive alcohol consumption, salt consumption and passive smoking were not associated with the development of hypertension. 81.7% hypertensive patients taking medications. Patients who lived in the city took drugs in 82.2% cases in rural areas - 80.8%. Effectively treated with 41.0% patients. Equally effective control their blood pressure, men and women (50.1% of the total number of men / women). In the city the percentage of persons who reach the target values was higher and amounted to 54.0% against 39.4% in rural areas (p = 0.002). In patients with a low risk of blood pressure control percentage reached 65.3%, with a very high risk - 41.9%. Among patients taking antihypertensive medications, the share of fixed combinations amounted to 10.5%, combination therapy - 30.6% and monotherapy - 58.9%.
Conclusions:The prevalence of hypertension in the Ryazan region, slightly higher than in Russia, however, is characterized by a high percentage achieve target BP. However, despite that more than 1/3 of the patients have a high and very high 10-year risk of fatal. In pharmacotherapy celebrated small percentage of use of fixed combinations and high monotherapy.
P816
Correlation between score risk and blood pressure control
T Yaneva-Sirakova1, R Tarnovska-Kadreva1, L Traykov2, M Yaneva3
1Medical University of Sofia, Department of Internal Medicine-Cardiology, Sofia, Bulgaria
2Medical University Sofia, Department of Neurology, Sofia, Bulgaria
3Medical University of Sofia, Sofia, Bulgaria
Topic: Sports cardiology
Purpose:The purpose of this study is to find if there is a correlation between SCORE risk and blood pressure control. It is very important especially in the group of patients (Pts) with high cardio-vascular risk, in which it may be difficult to achieve target values.
Methods:We included 931 hypertensive Pts in the initial visit [347(37.27%) males, 584(62.73%) females] and 263(28.25%) [178 females (30.48% of the initially recruited), 85 males (24.49% of the initial number)] during the follow-up visit after at least 6 months (6-20, mean 12). The mean age was 65.90±10.00 years. All of the Pts were on combination hypertensive treatment. Blood pressure was recorded in the office, at home (HMBP), 450 of the Pts had ambulatory monitored blood pressure during the inclusion and 213 during the follow-up. Pts underwent also basic laboratory and echocardiography evaluation. SCORE for high risk countries was used to assess cardio-vascular risk. Comorbidities were also recorded and evaluated. SPSS 19 was used for the statistical analysis.
Results:198(21.26%) of the Pts had only one cardio-vascular risk factor – hypertension. The largest number 394(42.32%) of Pts were those, who had =3 cardio-vascular risk factors. 588 (71.44%) of the Pts were with high and very high SCORE result. There was a significant (p<0.0001) difference between the mean HMBP values of the groups with very high/high SCORE risk and those with moderate/low risk with the higher values for the very high and high cardio-vascular risk groups. There was no statistically significant difference between the mean values of HMBP of the groups with very high and high risk. In both groups HMBP was suboptimal controlled, respectively 143.72±17.6 mmHg and 142.44±16.17 mmHg for the systolic, 85.51±9.65 mmHg and 83.99±10.02 mmHg for the diastolic,58.21±13.81 mmHg and 58.44±13.32 mmHg for the pulse pressure. The HMBP in the groups with medium and low SCORE risk were in the target values and between both of them there wasn't significant difference.
Conclusion:Pts with very high and high cardio-vascular risk have suboptimal controlled blood pressure. It is significantly higher than the blood pressure of the groups with medium and low SCORE risk, which is in the reference range. A potential reason for this or consequence of it may be advanced target organ damage. Stricter control of blood pressure is needed for the groups for which it is the most important.
P818
Rosuvastatin improves arterial stiffness in patients with inflammatory joint diseases and carotid atherosclerosis: Results from the RORA-AS study
E Ikdahl1, S Rollefstad1, J Hisdal2, IC Olsen2, I Holme3, TR Pedersen4, TK Kvien5, AG Semb1
1Diakonhjemmet Hospital, Preventive Cardio-Rheuma Clinic, Department of Rheumatology, Oslo, Norway
2Oslo University Hospital, Aker, Section of Vascular Investigations, Oslo, Norway
3Oslo University Hospital, Ullev? Dept. biostatistics, epidemiology and health economics, Oslo, Norway
4Oslo University Hospital, Ullev? Centre of Preventive Medicine, Oslo, Norway
5Diakonhjemmet Hospital, Department of Rheumatology, Oslo, Norway
Background:Arterial stiffness, as pulse wave velocity (PWV) and augmentation index (AIx), are early risk markers of cardiovascular disease (CVD). Intensive statin treatment induces carotid plaque (CP) regression in patients with inflammatory joint diseases (IJD). We evaluated the effect of rosuvastatin treatment on arterial stiffness in IJD patients with CP.
Methods:The study population included 89 statin na? IJD patients (rheumatoid arthritis: 55, ankylosing spondylitis: 23, psoriatic arthritis: 11). All patients had ultrasound verified CP and received rosuvastatin therapy over 18 months. PWV and AIx were measured at baseline and end of the study. Change in PWV and AIx from baseline was assessed with paired t-tests. Logistic regression analyses were performed with PWV and AIx as outcome variables, defined as decrease or no change/increase during the study, to assess for associations with other outcome measures.
Results:From baseline to study end, mean (SD) AIx and PWV was significantly improved from 27.9 (7.7) % and 8.1 (1.6) m/s2, to 26.2 (8.2) % (p=0.03) and 7.8 (1.5) m/s2 (p=0.03), respectively. The logistic regression models revealed associations between: 1) PWV and change in systolic blood pressure (sBP) (p=0.008) and a lower area under the curve sBP (p=0.03), adjusted for antihypertensive medication. 2) AIx and change in CP height (p=0.03) and rosuvastatin dose (p=0.01). All associations were robust to adjustments for traditional CVD risk factors.
Conclusion:Rosuvastatin therapy significantly improved arterial stiffness in IJD patients with CP. The improvement was associated with sBP change, rosuvastatin dose and atherosclerotic regression.
Change in arterial stiffness parameters
P819
Hypertension treatment in patients with metabolic syndrome and type 2 diabetes
SF Farsky1, AS Striskova1, MB Borcin1
1Slovak League against Hypertension, Martin, Slovak Republic
According to last ESH 2013 guidelines systolic blood pressure (sBP) goals for patients with diabetes mellitus is <140 mmHg, diastolic blood pressure (dBP) goals for patients with diabetes <85 mmHg, and for patients with metabolic syndrome BP =140/90 mmHg. We have analyzed the database of 1595 consecutive patients visiting our department of cardiology and internal medicine clinic in years 2005-2014. The analysis included 13990 visit records, average number of visits per patient was 8,5+-7,0. Our goals were to evaluate effectivity of hypertension treatment as for as drug choice, decrease of sBP and dBP associated with certain drug, drug combination and therapeutic inertia in patients with metabolic syndrome and/or diabetes mellitus. Final number of patients for analysis who fulfilled inclusion criteria for interpenetration of both diagnoses was 570.
Results:By hypertension monotherapy were treated 15% patients, by 2-4 drug combination therapy 70% and by 5-6 drug combination 15% patients. The most frequent used drugs were perindopril (perin), nitrendipin (nitre), amlodipin (amlo), telmisartan (telmi), hydrochlorothiazid (hydro), rilmenidin and nebivolol (used >100 patients). The most significant decrease of sBP was associated with treatment by nitre, hydro, telmi and urapidil (>19mmHg).The most significant decrease of dBP was associated with treatment by nitre, hydro, telmi and verapamil (>10mmHg). The most significant decrease of both sBP and dBP was associated with treatment 3 drug combination of telmi+hydro+spironolacton (41 resp. 16mmHg), telmis+hydro+nitre (34 resp.15 mmHg) and telmi+hydro+urapidil (34 resp. 15 mmHg). At the last visit 281 from 413 patients at the first visit have had sBP >140 mmHg (68%) i.e. sBP control was 32%. At the last visit 76 patients from 217 at the first visit have had dBP >90 mmHg (35%) i.e. dBP control was 65%. Therapeutic inertia was calculated by evaluating of proportion of visits at which sBP was about the target for eligible visits minus the proportion of visits where the change was made in antihypertensive (AHT) medication (either medication type or dose) over the number of eligible visits, with the resultant value multiplied by the mean of difference between actual sBP and target value at clinic visits: TIQ= ((%>TARGET - %? AHT/visits)/visits)* mean sBP- target sBP. TIQ was counted at first 100 consecutive patients and the average value was 45+-114.
P820
Indapamide is superior to methyldopa in women with post-partum hypertension: results from a randomized, case-control 1-year study
IR Gaisin1, AS Iskchakova2, LV Shilina2, NI Maksimov1
1State Medical Academy, Izhevsk, Russian Federation
2Clinical Diagnostic Centre of the Udmurt Republic, Izhevsk, Russian Federation
Background:Hypertensive disorders in pregnancy have been recognized as an important risk factor for atherosclerotic cardiovascular disease in women. Therefore, lifestyle modifications, regular blood pressure control, and control of metabolic factors are recommended after delivery, to avoid complications in subsequent pregnancies and to reduce maternal cardiovascular risk in the future. There are no uniform recommendations for the treatment of post-partum hypertension yet.
Methods:In a case-control, open-label 1-year study, 30 post-partum hypertensive women [aged 23–39 years; body mass index 26.2±4.4 (SD) kg/m2; 10 with previous pre-eclampsia, 10 pre-existing hypertension, 10 pre-existing hypertension plus superimposed pre-eclampsia; 60% nursing mothers] were randomized 1:1 to receive either indapamide 1.5 mg daily or adjusted-dose methyldopa. No significant differences observed between two groups at baseline.
Results:After comprehensive follow-up, blood pressure was not found to differ substantially between indapamide and methyldopa groups (122.8±3.6/78.5±2.5 mmHg vs. 126.3±4.2/81.3±3.5 mmHg respectively, p=NS). No maternal and offspring adverse effects were registered in both groups. There was a significant difference in weight reduction, in favour of indapamide (–12.8 kg vs. –2.4 kg, p=0.042), as well as in decrease of microalbuminuria (–194.1 mg/24 h vs. –48.3 mg/24 h, p=0.0004) and left ventricular mass index (–28.4 g/m2 vs. –9.2 g/m2, p=0.035). No significant changes in lipid and glucose metabolism were found in both groups. Treatment with indapamide significantly improved endothelial function, non-invasively assessed by flow-mediated dilatation of the brachial artery using high-resolution ultrasound (+8.7% vs. +2.3%, p=0.022) and increased eGFR (+15.7 ml/min/1.73 m2 vs. +6.3 ml/min/1.73 m2, p=0.021). Moreover, indapamide demonstrated a good safety profile and led to high adherence to treatment. In both groups, no reduced milk production was observed.
Conclusion:The results of the study provide support for indapamide as an effective and safe therapy of post-partum hypertension.
P821
The prevalence of and risk factors for masked hypertension.
E Mcintyre1, D Brouillard1, U Jurt1, M Matangi1
1Kingston Heart Clinic, Kingston, Canada
Background:Masked hypertension (MH) is present when a patient (P) has a normal office BP (OBP), <140/90 and an abnormal average daytime (ADT) 24hr ABPM (=135/85) in the absence of antihypertensive drugs (AHD). MH is important as it is associated with increased cardiovascular risk. Our purpose was to determine the prevalence of MH and the risk factors predisposing to MH.
Methods:Our ABPM database was searched for all P with a normal OBP (<140/90) who were not taking AHD. We arbitrarily defined ADT ABPM to be between 7am and 10pm. P were divided into two groups based on their ADT ABPM. Group 1, average daytime ABPM was either =135/85, or =135 and <85 or <135 and =85 (MH) and group 2, ADT ABPM was <135/85 (normotensive). Only the first ABPM was used and any duplicates were removed from both groups. Chi-squared analysis was used to determine differences between proportions and relative risk for sex, obesity, smoking, diabetes, sleep apnea, alcohol excess and NSAID use. An unpaired t-test was used to detect differences between mean values. A p value of <0.05 was considered statistically significant.
Results:Of 17,869 ABPMs 1,007 P were normotensive and 215 P exhibited MH, prevalence 17.6%. P with MH were older, 51.8 ± 13.7 vs 49.6 ± 14.7 years (P<0.05), had higher ADT SBP, 135.6 ± 6.1 vs 121.3 ± 7.4mmHg (p<0.0001), higher ADT DBP, 83.7 ± 5.9 vs 73.7 ± 6.3mmHg (p<0.0001), higher OSBP, 133.8 ± 5.1 vs 129.9 ± 7.6mmHg (p<0.0001) and higher ODBP, 81.8 ± 6.4 vs 78.9 ± 7.5mmHg (p<0.0001). Systolic MH was present in 90 P (41.9%), systolic and diastolic MH was present in 51 P (23.7%) and diastolic MH was present in 74 P (34.4%), Chi-squared p=0.0605. The P characteristics are seen in Table 1.
Conclusions:MH occurs in 1 of every 6 P with a normal OBP and no AHD. MH is more common in males, diabetes, obesity and sleep apnea. P with MH were significantly older. P with MH have normal but significantly higher OSBP and ODBP compared to normotensives. Only home BP monitoring or 24hr ABPM can detect masked hypertension.
N
M/F
Obesity
Smoking
Diabetes
Sleep apnea
Alcohol
NSAIDs
Normal.
1007
377/630
412/595
96/911
23/984
55/952
20/987
61/946
Masked
215
117/98
112/103
21/194
12/203
24/191
6/209
21/194
P value
<0.0001*
<0.005
NS
<0.05
<0.005
NS
NS
RR (95% CI)
1.45 (1.26-1.68)
1.45 (1.14-1.85)
-
2.0 (1.25-3.23)
1.82 (1.27-2.60)
-
-
P822
Central blood pressure is elevated in youths with isolated systolic hypertension and influenced by classical risk factors
J Elmenhorst1, E Alvermann1, R Oberhoffer1
1Technische Universit? Institute of Preventive Pediatrics, M?, Germany
Topic: Sports cardiology
Purpose:Pediatric hypertension seems to be an underdiagnosed and thereby underestimated problem in Germany. In contrast isolated systolic hypertension in youth (ISH) seems to be a common condition. It is not clear if ISH in youths should be treated or not. Measurement of complementary central blood pressure in those individuals is recommended in adults. But little is known about central blood pressure in youths and the influence of classical cardiovascular risk factors.
Methods:In children from 8-18 years peripheral (pBP) and central systolic blood pressure (cSBP) were measured with an oscillometric device (Mobil-O-Graph, IEM, Germany) after 5-10min rest in supine position. Individual cardio-vascular risk factors were assessed in a questionnaire (adopted from KiGGS study). Participants were classified according to their pBP as normotensive (NT), high normotensive (HNT), hypertensive (HTN) or isolated systolic hypertensive (ISH). A child-adapted risk profile (low /elevated) was calculated with classical, non-invasive cardiovascular risks factors (smoking, media-consumption, physical activity and body mass index (measured)) based upon anamnestic information by the patient. Descriptive analyses are presented as mean±SD. For group differences an ANOVA (Bonferroni post-hoc) was performed; the significance level was set at p=0.05.
Results:From all participants (n=709; ?153;?: 47.8%) 66.4% were NT, 14.8% ISH, 10.7% HNT and 8.0% HTN. There are no significant differences in age and BMI z-score between the subgroups (except, ISH who are younger than NT). cSBP is the lowest in the NT group (101.5±8.6mmHG) followed by HNT (105.4±8.7mmHG), ISH (109.5±8.4mmHG), and highest in HTN (113.1±7.9mmHG). The subgroups differed significantly in cSBP z-score (percentiles corrected for age), however, in the post-hoc analysis no significant difference could be shown between ISH and HTN. In a second step we divided the blood pressure subgroups according to their risk profile: low risk (0-3 risk points; 69.2%) and elevated risk (4-8 risk points; 30.8%). In the low risk group highest cSBP was measured in HTN (p<0.001). In the high risk group highest cSBP could be observed in ISH and HTN without sig. differences between groups. In both groups cSBP was above the 90th percentile of cSBP.
Conclusions:Central systolic blood pressure is elevated in youths with hypertension and ISH. The condition is likely to deteriorate if the child has additional risk factors such as smoking, elevated BMI, inactivity, and extended media-consumption. These children might profit from intensified intervention strategies.
P823
LDL-C attainment rate among treated stable CHD patients: the dyslipidemia international study (DYSIS) II Ireland results
A Murphy1, T Kiernan2, B Seoighe3, A Flood3, AK Gitt4, M Horack4, V Ashton5, P Brudi5, D Lautsch6, B Ambegaonkar5
1National University of Ireland, Galway, Ireland
2University Hospital Limerick, Limerick, Ireland
3MSD, Dublin, Ireland
4Stiftung Institut fur Herzinfarktforschung, Ludwigshafen am Rhein, Germany
5Merck Sharp & Dohme Corp., Whitehouse Station, United States of America
6MSD, Wien, Austria
Topic: Sports cardiology
Purpose:Coronary heart disease (CHD) patients remain at very high risk of future cardiovascular events. Providing effective treatments for key risk factors, such as lipid abnormalities, hypertension and diabetes are vital to the reduction of future complications. DYSISII aims to identify unmet needs in lipid target achievements and prevalence of lipid abnormalities among stable CHD patients in Ireland currently being treated with lipid lowering therapy (LLT).
Methods:DYSIS II is a multicenter, observational cross-sectional chart review conducted in 4 outpatient care centers in Ireland from May 2013 to May 2014. Eligible adult patients had a documented history of CHD (past acute coronary syndrome (ACS) events must be >3 months before enrollment), full lipid profile available 0-12 months prior to enrollment, on LLT for =3 months or not treated at all, and were not participating in randomized clinical trials involving medication at the time of enrollment. Patient characteristics, risk factors, treatment patterns, and laboratory values were collected. Lipid target achievement for low density lipoprotein cholesterol (LDL-C) was assessed based on 2011 ESC/EAS guidelines.
Results:Among 296 stable CHD patients (82.1% male, mean age 69.8 ± 8.7 years), 80.8% had a previous coronary artery bypass graft or percutaneous coronary intervention, 59.1% family history of CHD, 52.0% history of ACS, 45.3% hypertension, 39.6% hypercholesterolemia, 36.3% BMI>30kg/m2, and 26.0% had type 2 diabetes mellitus. 97% (n=287) of patients were on statin (96.9%) or non-statin (17.8%) LLT, with only 40.4% achieving the <70 mg/dl LDL-C target. Mean atorvastatin-equivalent dose was 28 ± 20 mg/day. 14.6% of treated patients received combination therapy with 10.8% receiving ezetimibe plus a statin.
Conclusion:Approximately 60% of LLT treated stable CHD patients in Ireland did not achieve the recommended LDL-C target. Additional effective LLTs are needed among these very high risk patients to prevent future cardiovascular events.
LLT Treated Patients (n=287)
Low density lipoprotein (LDL) cholesterol
75.2 ± 24.8 mg/dl
Total cholesterol
150.3 ± 30.9 mg/dl
Triglycerides
131.3 ± 85.2 mg/dl
Non-HDL cholesterol
100.4 ± 28.6 mg/dl
P826
Differences in body composition, body-mass index, and cardiovascular risk between ethnic groups in Suriname
FS Diemer1, YC Haan2, GA Van Montfrans2, GP Oehlers1, LM Brewster3, LMW Nahar-Van Venrooij4
2Academic Medical Center of Amsterdam, Vascular Medicine, Amsterdam, Netherlands
3Academic Medical Center of Amsterdam, Internal and Vascular Medicine, Amsterdam, Netherlands
4Anton de Kom University of Suriname, Public Health, Paramaribo, Suriname
Topic: Sports cardiology
Purpose:To describe differences in body composition, BMI, and cardiovascular risk in a multi-ethnic population in urban Suriname.
Methods:Fat mass and fat-free mass were determined in 330 Surinamese adults from the running HELISUR study through bio-electrical impedance spectroscopy. BMI, waist-hip ratio (WHR), fat mass, and fat-free mass index for height squared were calculated. High-risk subjects were identified with the Framingham Risk Score. Kruskal-Wallis tests and Chi-squared tests were performed to test group differences. To compare continuous variables between two groups, we used the Mann-Whitney U test.
Results:Cardiovascular risk was higher in South-Asians and Indonesians than in people of African descent (Creole, Maroons) (Table 1). Although BMI did not differ in men, in particular South-Asian men showed higher fat mass and higher WHR compared to Creole (p=0.025; p=0.021) and Maroon men (p=0.151; p=0.003). Compared to South-Asian women, Creole and Maroon women showed higher BMI (p=0.001; p=0.043) and fat-free mass index (p<0.001; p<0.001) but not a higher fat mass (p=0.277; p=0.343) or WHR (p=0.371; p=0.128).
Conclusion:The results suggest a more favorable body composition in people from African descent compared to South-Asians, despite similar or higher BMI levels.
Prevalence of obesity among coronary patients according to the metric used.
R Dalmau Gonzalez-Gallarza1, A Castro Conde1, Z Blazquez Bermejo2, R Mori Junco2, C Alvarez Ortega2, A Roldan Sevilla3, J Nuche Berenguer3, I Montilla Padilla3, N Tovar Forero3, JL Lopez Sendon2
1University Hospital La Paz, Department of Cardiology, Cardiac Rehabilitation Unit, Madrid, Spain
2University Hospital La Paz, Madrid, Spain
3University Hospital 12 de Octubre, Department of Cardiology, Madrid, Spain
Topic: Sports cardiology
Purpose:Obesity prevalence has experienced a dramatic rise over the last decades, with a very important impact on cardiovascular prevention, as obesity promotes the onset of cardiovascular risk factors, and determines its control. Nevertheless, there is some debate about which is the best metric of obesity. We studied the prevalence of obesity in a cohort of coronary disease patients, according to the metric used, and the metabolic disturbances related to obesity. Methods:868 coronary disease patients referred to a cardiac rehabilitation program were analysed. Obesity prevalence was determined according to Body Mass Index (obese when BMI =30 kg/m2) or waist circumference (obese when =102cm for men, =88cm for women). We also analyzed the proportion of patients meeting NCEP ATP3 metabolic syndrome criteria according to their BMI and waist circumference category. Results:84% of patients were male, mean age 56,9 , 22,9% were diabetic, 50,9% hypertensive, 52,9% smokers, 56,4% sedentary, 59,4% had dyslipidemia. 26,0% were obese according to their BMI (25,7% of men, 27,4% of women, p=0,37). Considering waist circumference the proportion of obesity was larger: 46,5% in the global cohort (41,6% of men, 73,0% of women, p<0,001). 24,9% of patients met both obesity criteria. 95,2% of patients with BMI =30 kg/m2 had also abdominal obesity, but only 53,5% of patients with abdominal obesity had a BMI =30. Moreover, 29,4% of patients with BMI<30 had abdominal obesity. 85,2% of patients with abdominal obesity met at least two other criteria of metabolic syndrome, 88% of patients with BMI =30 met 3 or more criteria of metabolic syndrome.
Conclusions:despite the fact that both abdominal obesity and obesity according to BMI are common conditions in coronary patients, abdominal obesity is more prevalent, mostly in women, and it is often present in the absence of a BMI =30 kg/m2. Both obesity metrics are related to a high prevalence of metabolic disorders.
Abdominal obesity
BMI =30 kg/m2
Triglyceride =150 mg/dl
43,1%
51,1%
Fasting glucose =100 mg/dl
76,1%
82,0%
Hypertension
63,5%
68,6%
HDL-c <40 mg/dl in men or <50 in women
76,6%
83,1%
P828
Is the obesity paradox equally present in patients with and without ST-segment elevation acute coronary syndromes?
A T Timoteo1, S A Rosa1, T P Silva1, P Rio1, M Nogueira1, M L Ferreira1, R C Ferreira1
1Hospital Santa Marta, CHLC, Lisbon, Portugal
Background:Obesity paradox has been previously described in patients with cardiovascular disease, including acute coronary syndromes. Particularly patients with overweight and grade 1 obesity have a better outcome. We sought to evaluate if this paradox was equally present in patients with and without ST-segment elevation acute coronary syndromes (ACS).
Methods:Study of consecutive patients admitted at our intensive care unit from 2005 to 2013 for an ACS and included in a single-centre registry of ACS. Patient data was reviewed. They were divided in three groups according to body mass index: Normal (< 25 Kg/m2, n=973), Overweight (25 – 29 Kg/m2, n=1291) and Obesity (³ 30 Kg/m2, n=584). The primary outcome was one-year all-cause mortality but in-hospital and 30-day mortality was also evaluated.
Results:We included 2848 patients, with a mean age of 64 ± 13 years, 71 % males and 62% with a ST-elevation acute myocardial infarction. In the entire population, obesity paradox was confirmed, particularly in the Overweight group, for all the outcomes considered. In the group without ST elevation ACS, the paradox was only significant for long term mortality but with a consistent decay in mortality across all groups including the Obesity group (Table). For ST elevation patients the paradox for the Overweight group was present even for short-term mortality but in the Obesity group there was an increase or a stabilization of mortality incidence.
Conclusions:Although the obesity paradox is present for long-term mortality in both patients with and without ST-segment elevation ACS, the paradoxical reduction in mortality is more evident and consistent in the group without ST-elevation, where the Obesity group has a lower rate of mortality compared with the Overweight group.
All-cause mortality (%) according to diagnosis and BMI.
Without ST
Normal
Overweight
Obesity
p-value
Hospital
4.8
2.7
2.4
0,163
30-day
6.5
3.9
3.3
0.126
One-year
11.8
7.1
5.7
0.015
With ST
Hospital
7.3
4.7
4.8
0.089
30-day
9.2
5.7
7.0
0.041
One-year
11.7
8.1
7.8
0.039
P829
Bariatric surgery improves endothelial function in patients with prior dysfunction
M Faustino1, S Bravo Baptista1, M Nedio1, C Monteiro1, E Lourenco1, V Gil1, C Morais1
1Hospital Prof. Dr. Fernando Fonseca, EPE, Amadora, Portugal
Topic: Sports cardiology
Purpose:Bariatric surgery (BS) is associated with significant reductions in cardiovascular risk factors and global improvement in cardiovascular risk profile. After BS, an improvement in peripheral endothelial function (EF) assessed noninvasively was also reported. This study aims to evaluate the long-term evolution of EF, in a population of obese patients submitted to BS.
Methods:EF was evaluated by arterial peripheral tonometry. The reactive hyperaemia index (RHI) was assessed before BS (Eval1) 6 months (Eval2) and 3 years after the CB (Eval3). Values ?128;??128;?of RHI <1.7 (very high risk) or 1.7> RHI> 2.1 (high risk) were defined as endothelial dysfunction (ED).
Results:Sixty-eight obese patients were included (mean age 43.0 years ±10.7; 62 women). The median time between BS and Eval2 was 217 days (Interquartile range (IQR) 93) and between Eval2 and Eval3 was 918 days (IQR 343). A significant reduction in weight, waist circumference and body mass index was observed between Eval1 and Eval2 (43+/-4,6 vs. 29,7+/-3,5; p<0,0001), which is further accentuated in Eval3 (additional reduction to 27,4+/-3,1 kg, p>0,0001). The number of patients with endothelial dysfunction decreased significantly between Eval1 (32 patients, 47.1%) and Eval2 (25 patients, 36.8%, p = 0.013). Among the patients with endothelial dysfunction in Eval 1, fourteen patients were reassessed after 3 years (Eval3). In these patients a significant increase in the average value of IHR between Eval1 and Eval2 was documented (1.6 vs. 2.1, p <0.001), which was accentuated in Eval3 (2.3, P <0.001, compared with the Eval1). The number of patients with endothelial dysfunction decreased to eight patients in Eval2 and to four patients in Eval3.
Conclusion:A significant percentage of obese patients (47.1%) presents endothelial dysfunction before BS, in spite of being a young population. In this group, the BS is associated with a significant improvement in endothelial function, which persists over time (3 years). This may be one of the mechanisms contributing to the improvement of cardiovascular prognosis documented after BS, justifying further investigation.
P830
Effect of onion peel extract on endothelial function and endothelial progenitor cells in overweight and obese subjects
W Kim1, JB Kim1, JS Woo1, WS Kim1, HS Kim1, W Kim2
1Kyung Hee University Hospital, Seoul, Korea, Republic of
2Gwangju Veterans Hospital, Gwangju, Korea, Republic of
Topic: Sports cardiology
Purpose:Acute or chronic intake of polyphenol-rich foods has been reported to improve endothelial function. Quercetin, found abundantly in onion, is a potent antioxidant flavonoid. This study was designed to investigate whether consumption of onion peel extract (OPE) improves endothelial function in healthy overweight and obese subjects.
Methods:This study was a randomized, double-blind, placebo-controlled study. Seventy-two healthy overweight and obese participants were randomly assigned to receive a red soft capsule of OPE (100 mg/day, 50 mg bid; 36 subjects) or an identical placebo capsule (36 subjects) for 12 weeks. Endothelial function, defined by flow-mediated dilatation (FMD), circulating endothelial progenitor cells (EPCs) by flow cytometry, and laboratory test were determined at baseline and after treatment.
Results:Baseline characteristics and laboratory findings were not significantly different between the two groups. Compared with baseline values, the OPE group showed significantly improved FMD at 12 weeks (from 12.5 ± 5.2 to 15.2 ± 6.1, p = 0.002) whereas the placebo group showed no difference. Nitroglycerin-mediated dilation (NMD) did not change in either placebo or OPE group. EPC counts (44.2 ± 25.6 vs. 52.3 ± 18.6, p = 0.005) and the percentage of EPCs were significantly increased in the OPE consumption group. When FMD was divided into quartiles, rate of patients with endothelial dysfunction defined as lowest quartile (cutoff value = 8.6%) of FMD was improved from 26% to 9% by OPE consumption.
Conclusions:Mid-term administration of OPE induces an improvement in FMD and circulating EPCs counts.
P831
Correlation between weight perception and body mass index (BMI) in an urban Swiss population
N Rouiller Larpin1, P Marques-Vidal1, G Waeber1
1University Hospital Centre Vaudois (CHUV), Internal Medicine, Lausanne, Switzerland
Background:Several studies have suggested that weight perception is a stronger determinant in motivation to lose weight than measured body mass index (BMI).
Objective:To assess the prevalence and determinants of weight self-perception (underestimation and overestimation) in an adult urban Swiss population.
Method:Cross-sectional study conducted between 2009 and 2012 among subjects living in Lausanne, Switzerland. A total of 4895 participants (2605 women) aged 40 to 80 years were assessed. Height and weight were measured and body mass index (BMI) was calculated. Weight self-perception, nationality, educational and socio-economic status were collected through a questionnaire.
Results:Prevalence of overweight and obesity was 39% and 17%, respectively. Among normal weight (BMI<25kg/m2) subjects, overestimation of weight was significantly higher in women (19.6%) than in men (8.5%). One quarter of women and half of men with overweight considered themselves normal weight; the corresponding values for obese subjects were 7% and 10%. After multivariate analysis, the following factors were associated with a higher likelihood of weight underestimation: male gender: odds ratio and (95% CI) 3.07 (2.52-3.74); increasing age (p for trend<0.001); overweight: 22.6 (17.4-29.2); obesity: 5.32 (3.61-7.82); low education: 1.92 (1.48-2.48); Portuguese nationality: 2.11 (1.43-3.12); current smoking: 1.32 (1.04–1.68) and being diagnosed with overweight 5.54 (4.44-6.92), while formers smokers had a lower likelihood of underestimation: 0.75 (0.61-0.92). Inversely, male gender: 0.29 (0.21-0.39); increasing age (p for trend<0.001); low education: 0.51 (0.38-0.69) and Portuguese nationality: 0.62 (0.44-0.88) were associated with a lower likelihood of weight overestimation while being diagnosed with overweight was positively associated: 3.06 (2.18-4.3).
Conclusion:Over half of overweight men and one tenth of obese subjects inadequately estimate their weight. Weight misperception is a multifactorial concept which might preclude adequate management of BMI-related cardiovascular risk factors. Emphasis on adequate weight assessment and awareness is needed.
P833
Cognitive function and cardiovascular disease mortality in Poland. The HAPIEE Study.
A Dorynska1, M Kozela1, A Pajak1
1CMUJ - Institute of Public Health, Institute of Clinical Epidemiology and Population Studies, Krakow, Poland
Background:Decline in cognitive function (CF) is related to ageing. There is some evidence on the relationship between CF and cardiovascular risk factors but less is known on the relationship between CF and risk of cardiovascular death.
Topic: Sports cardiology
Purpose:To assess the relationship between CF and risk of death from cardiovascular disease (CVD).
Methods:Studied group was a random sample of men and women aged 45-69 years, selected from permanent residents of Krakow. Information on health status, CF, CVD risk factors, and health behaviours was collected using standardized questionnaire. CF was assessed using two components, e.g. verbal memory (VM) and semantic verbal fluency (SVF). Participants were classified into four subcategories of each component of CF, according to quartile values of the distribution. Information on deaths and their causes was obtained from the local registry, Central Statistical Office of Poland and by contacting participants' relatives. Causes of deaths were classified according to ICD-10 and included codes from I.01 to I.99. Relationship between CF and CVD mortality was assessed using Cox proportional hazards model. Statistical significance was accepted at the level of p<0.05.
Results:Median follow-up time was 7.06 years in men and 7.08 years in women. There were 189 new CVD deaths in men, and 97 in women. After adjustment for age, compared to participants with the best VM, participants with the worst VM had higher risk of CVD death (HR=1.90; 95%CI=1.07-3.36 in men, HR=2.21; 95%CI=1.01-4.84 in women). In men, the relationship between verbal memory and CVD mortality was partially explained by other CVD risk factors (hypertension, hypercholesterolaemia, diabetes, smoking, BMI and physical activity), while in women adjustment for CVD risk factors did not affect statistical significance. After adjustment for age, compared to participants with the best SVF, participants with the worst SVF had higher risk of CVD death (HR=1.71; 95%CI=1.00-2.90 for men, HR=3.40; 95%CI=1.41-8.19 for women), and similarly to verbal memory, the relationship was partially explained by classical CVD risk factors, but remained significant in women (HR=3.11; 95%CI=1.11-8.68).
Conclusions:Worse both VM and SVF increased risk of CVD death. In men, the relationships was partially dependent of exposure to other CVD risk factors.
P835
The relationship between the sleep quality and blood pressure values before and after therapy with rilmenidine
S Farsky1, RS Sidlo1
1Slovak League against Hypertension, Martin, Slovak Republic
The study was aimed at determining a potential correlation between the morning values of blood pressure and the sleep quality during the previous night in patients with fixed hypertension treated with medicaments, and at finding whether a therapy with rilmenidine has positive effects not only on the value of blood pressure, but also improves the sleep quality through decrease in the sympathicus activity. We have examined 993 patients with essential hypertension, that have not reached the target values of blood pressure in spite of a therapy with medicaments, and the abdominal obesity was found in 79% of the patients. The therapy with rilmenidine was added to their previous treatment, and the study duration was 3 months. At the beginning and at the end of the study, there were performed anthropometric and basic biochemistry examinations, a repeated measurement of the blood pressure and heart rate in 10 min intervals in outpatient departments of general practitioners, as well as an evaluation of the sleep quality according to the Athens Insomnia Scale questionnaire. After adding rilmenidine to their hypertension therapy, there was found a decrease in systolic pressure, diastolic pressure, heart rate and sleep quality. The decrease was highly significant (p<0.0001). The coefficients of correlation between the systolic blood pressure values and the sleep quality were 0.08 (p<0.0226) at the beginning of the study and 0.14 (p < 0.0001) at the end of the study, and were 0.08 (p<0.015) between the diastolic blood pressure values and the sleep quality at the end of the study. The coefficients of correlation between a difference of the systolic blood pressure values and a difference between results of the questionnaire at the beginning and the end of the study were -0.09 (p< 0.0064). Results of our study acknowledged a positive effect of rilmenidine in hypertension therapy due to a significant decrease of the blood pressure, slowing the heart rate and improvement of the sleep quality evaluated by the standardized questionnaire. In addition, interesting associations were found between the sleep quality and values of the systolic blood pressure, and partly also diastolic blood pressure before the start of therapy with rilmenidine and during the therapy. These results are in concordance with the actual literature data that demonstrated that a decreased length and an impaired quality of sleep have a negative effect on blood pressure values and occurrence of hypertension as well as the overall cardiovascular risk in adolescent and adults persons.
P836
A comparison of the prevalence and clustering of cardiovascular risk factors in the Netherlands and China
X Wang1, ML Bots1, AW Hoes1, F Yang2, I Vaartjes1
1University Medical Center Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, Netherlands
21st Hospital of Jilin University, International Health Promotion Center, Changchun, China, People's Republic of
Purposes:To compare the prevalence and clustering of major cardiovascular risk factors among adults in the Netherlands and China.
Methods:6,542 adults were recruited from 2001 to 2006 for the Utrecht Health Project (UHP), an ongoing cohort study among inhabitants of a newly developing area near Utrecht, the Netherlands. 37,141 employees who received health screening in the Hospital, Changchun, China were enrolled from 2003 to 2010. 3,850 residents from Dehui, another city from Northeast China were enrolled in 2007.
Results:In each age group, the Dutch population had higher levels of body mass index (BMI), systolic blood pressure, and total cholesterol compared to Chinese population. In the younger age group (18-44 years old), Dutch men and Chinese men had a similar BMI level. Age standardized prevalence of smoking and diabetes was higher in Chinese men than in Dutch men (P<0.05). For women the prevalence of smoking and excessive alcohol intake was highest in the Dutch (P<0.05). For both Dutch and Chinese adults, older participants and men were more likely to have clustering of cardiovascular risk factors. The current smoking-heavy drinking cluster was most common in Chinese young men (33.6%). While in Dutch young men, smoking commonly went together with hypercholesterolemia (19.8%). For Chinese young women, the obesity-hypertension cluster was most prevalent (37.8%), while the smoking-hypercholesterolemia cluster was common in Dutch young women (26.4%).
Conclusions:Cardiovascular risk profiles and clustering patterns are different between Caucasians and Asians and seem to differ between men and women. This calls for race and sex specific targeted prevention programmes.
P837
Clinical and economic assessment of the organizational model of primary prevention in a group of railway workers
N Pyrikova1, A Zaltsman1, I Osipova2, A Kontsevaya3
2Altay State Medical University, Barnaul, Russian Federation
3National Research Center for Preventive Medicine, Moscow, Russian Federation
The aim:to evaluate the position of the employer the feasibility of implementing the organizational model of primary prevention in a group of men of railway transport.
Material and methods:the drivers and assistant drivers 20-55 years. In the 1st group (n=224) implemented the organizational model of primary prevention of CVD - School health at the workplace and individual preventive counseling in the clinic and Wellness physical center of the locomotive depot; 2nd group (n=128) were under regular medical supervision (pre-trip inspections, examination and medical commission). Assess of CVD risk factors, temporary disability by CVD, the return on investment of the employer on the background of the implementation of the organizational model of primary prevention of CVD within three years from 2010 to 2012.
Results:In 2012 in the 1st group, in comparison with the 2nd, smoking rarer 1.5 times (p=0,0000), overweight and abdominal obesity at 1.2 times (p=0.05), hypercholesterolemia in 2 times (p=0,0000), physical inactivity 2.4 times (p=0,0000), excessive alcohol consumption 1.6 times (p=0,0000), inadequate consumption of vegetables at 14.8 times (p=0,0000). In 2010 costs in the 1st group were higher than in the 2nd, mainly due to the cost of implementation of the organizational model of primary prevention of CVD. In 2012 on the background of preventive activities in the 1st group the total costs of the employer for three years were less 40%, than 2nd; in the 1st group decreased the number of days of temporary disability by 34.6%, in the 2nd group increased by 8.7%. Thus, in 2012 in the 1st group identified the reduction of temporary disability, compared to 2nd, at 32 days, additional gross regional product produced by reducing days of temporary disability, was 1253,2 dollars. For each spent in 2010 the dollar return on investment of the employer was 4.65 dollars in the next three years (2012).
Conclusion:Implementation of the organizational model of primary prevention in a group of railway workers in the next three years leads to decrease smoking by 27.3%, abdominal obesity by 13%, hypercholesterolemia by 32.1%, physical inactivity by 43.8%, excessive alcohol consumption by 16.1%, insufficient consumption of vegetables 64.7%, reduction of days of temporary disability by CVD by 34.6%. The economic feasibility of the organizational model of primary prevention of CVD with the employer confirmed the return $ 4,65 of investment $ 1 dollar within three years.
P838
Sleep disordered breathing in heart failure: nocturnal desaturation as a novel prognostic marker. A prospective cohort study on 376 patients.
B Gellen1, F Canoui-Poitrine2, L Boyer3, A Le Thuaut2, A Covali-Noroc3, JL Dubois-Rande4, L Hittinger4, S Adnot3, S Bastuji-Garin2, T Damy4
1AP-HP - University Hospital Henri Mondor, Interventional Cardiology Unit, Department of Physiology, Creteil, France
2University Hospital Henri Mondor, Public Health Department and Clinical Resarch Unit , Creteil, France
3University Hospital Henri Mondor, Department of Physiology, Creteil, France
4University Hospital Henri Mondor, Department of Cardiology, Creteil, France
Sleep disordered breathing (SDB) is common in patients with HF with reduced ejection fraction (HFrEF). Increased apnoea-hypopnoea index (AHI) is predictive of poor outcome. Nocturnal desaturation (ND) is associated with increase in NT-proBNP. Prognostic value of ND in addition to AHI is still unknown. 376 consecutive patients with stable HFrEF were prospectively screened for SDB between 2005 and 2010 by polygraphy. SDB was defined by an AHI =5 and sleep apnea (SA) by an AHI=15. Mean age was 59±13y, LVEF 30%±6%, and AHI 18±10; 310 patients (82%) had SDB. The composite end-point of death, transplantation and LV assistance occurred in 98 patients (26%) within 3y. Minimal oxygen saturation (MOS), number of desaturations <90%/hour and time spent with oxygen saturation <90% were significantly associated with adverse events after adjustment for confounders, whereas AHI was not (Figure). Best MOS cut-off for poor outcome was =88%. Patients with MOS =88% without SA had similar event rates than those with MOS =88% with SA. Patients with MOS =88% had a significantly higher event rate than those with MOS >88% (p<0.01). Risk assessment using MOS of =88% in top of established prognostic markers of HFrEF yielded a net reclassification index (NRI) of 6%. In HFrEF, ND =88% is a stronger predictor of events than AHI, independently of the presence of SA. This suggests that risk assessment in HFrEF should include MOS, and that SDB treatment may also focus on patients without SA presenting ND.
Arterial hypertension
181 (48.1)
22 (43.1)
10 (52.6)
55 (46.6)
94 (50.0)
0,8
polygraphy parameters and events at 3y
Country
N
Age
Women %
Cardiac rehab %
Current Smoker %
Physical inactivity %
Hypertension %
Diabetes %
Overweight/obese %
BP<140/90mmHg
LDL<1.8mmol/L
Belgium
609
68
24.0
40.8
16.1
47.2
68.8
29.5
73.2
61.8
23.9
Croatia
1515
66
31.0
32.2
21.9
45.7
83.5
32.1
80.1
55.1
25.3
Denmark
300
66
28.0
*
23.7
74.7
63.6
*
74.1
62.5
37.5
Ireland
1831
64
23.5
66.0
15.5
31.0
58.7
18.4
80.2
60.8
45.7
Italy
1223
68
24.9
49.1
13.8
52.2
72.8
30.7
71.8
65.8
33.9
Saudi Arabic
1582
62
26.1
2.8
11.1
54.7
83.9
78.3
83.0
73.2
35.6
North Ireland
166
65
20.1
56.6
21.7
56.3
63.0
14.9
84.7
89.3
46.4
Romania
625
64
27.8
4.8
22.4
54.1
75.5
27.2
79.4
57.4
16.1
Russia
464
65
38.4
52.3
26.3
37.8
88.9
25.2
82.1
65.9
25.3
Taiwan
735
67
30.7
4.4
20.3
51.2
70.9
35.8
53.1
66.1
15.1
China
1152
67
45.3
1.5
13.5
43.7
81.2
42.8
43.8
71.3
14.4
P839
Survey of risk factors (SURF) phase I report
M Zhao1, MT Cooney2, IM Graham3
1University College London, Farr Institute of Health Informatics Research, London, United Kingdom
2St Vincent's University Hospital, Dublin, Ireland
3Trinity College Dublin, Dublin, Ireland
Topic: Sports cardiology
Purpose:Risk factor management in the secondary prevention of Coronary Heart Disease (CHD) has been shown to be sub-optimal. SURF, an international audit, is designed as a simple but efficient way to collect risk factor information on CHD prevention. It allows comparisons between regions and complements other risk factor audits. Method:Patients with established CHD, were included from 11 countries. All eligible patients aged over 18 were recruited during routine clinic visits. Data were collected on one page collection sheet or online server and included information of diagnostic category, cardiac rehabilitation, risk factors, physical measurements, and medical measurements. Results:A total of 10,202 patients (71% men) were enrolled. The mean age was 65 years. 17% of the participants were still smoking, 73% were overweight/obese and 47% were physical inactivity. The attendance of cardiac rehabilitation was poor and with wide regional variations. Two-thirds of participants has reached 140/90mmHg of blood pressure target and less than one-third achieved the 1.8mmol/L of LDL cholesterol target. Antiplatelet, anti-hypertensive agents, and lipid lowering agents were widely used. There were some discrepancies on European and Asian results. Conclusion:There data indicate poor control of risk factors in CHD prevention. Physical and medical measurement targets were not achieved. The attendance of cardiac rehabilitation was extremely low in Asia. More attention to lifestyle risk factors need to be addressed.
P840
Factors determining the development of long-term postoperative cognitive dysfunction in patients with type 2 diabetes undergoing coronary artery bypass grafting
O Trubnikova1, A Mamontova1, O Maleva1, I Kuhareva1, O Barbarash1
1Research Institute of Complex Issues of Cardiovascular Diseases, Kemerovo, Russian Federation
Topic: Sports cardiology
Purpose:To identify factors, contributing to the development of long-term postoperative cognitive dysfunction (POCD) in diabetic patients with coronary artery disease (CAD), who have undergone on-pump coronary artery bypass grafting (CABG).
Methods:114 male patients (55,9 ± 5,3 years), who have undergone elective on-pump CABG, were enrolled in the study. We assessed a neuropsychological status (attention, short-term memory and neurodynamics) of patients on days 7-10 before and on days 7-10 and 1 year after CABG. Early (7-10 days) and long-term (over 1 year) POCD was diagnosed in 20% decline in postoperative parameters on 20% of the tests performed preoperatively. Trait anxiety (TA) was estimated by Spielberger-Khanin's questionnaire. The factors relevant to the development of long-term POCD were the following: patient adherence to treatment, mild cognitive impairment (MCI), early POCD, left ventricular ejection fraction, levels of TA and the progression of carotid artery (CA) stenosis over 1 year after CABG (new / or a increased progression rate of previously diagnosed stenosis). Binary logistic regression was used to identify independent predictors (SPSS17, Binary logistic regression, forward stepwise logistic regression method). The model was validated using the ROC curve. Patient adherence to treatment was calculated as the integral index, estimating the Euclidean distance of each patient to the standard.
Results:The achievement of target levels of glucose, glycated hemoglobin, total cholesterol, high and low density lipoprotein cholesterol, triglycerides, smoking cessation and weight loss were included in the comprehensive assessment of treatment adherence. The progression of CA (B = -0,683, p = 0,045), ?A levels (B = -0,067, p = 0,036) and the integral index of patient adherence to treatment (B = -1,501, p = 0,042) were identified as significant factors, contributing to the development of long-term POCD in diabetic patients. The area under the ROC-curve was - 0.7, sensitivity of 0.7 and specificity 0.55.
Conclusion:The progression of CA stenosis, high ?A levels and low adherence to treatment in diabetic patients 1 year after CABG appear to be significant for the development of long-term POCD.
P841
Salt sensitivity and the visit to the visit variability diastolic blood pressure as early markers of masked hypertension
I Osipova1, A Miroshnichenko2, O Antropova1, N Pyrikova1, A Zaltsman2, V Kulikov1
1Altay State Medical University, Barnaul, Russian Federation
Objective:study of salt sensitivity and the visit to visit variability in diastolic blood pressure (dBP) in men with masked hypertension.
Materials and Methods:The study included 99 drivers and their assistants (mean age 43,3 ± 10,4 years). The masked hypertension detected by the test "Mathematical expense." The test was positive for growth in systolic blood pressure (sBP) > 7% and/or increment of heart rate (HR) > 10%. Identified 2 groups: the first group consisted of individuals with masked hypertension (n = 40, age 42,8 ± 9,8 years); second group - healthy (n = 59, age 42,3 ± 8,4 years). Sensitivity to salt was determined by the modified method RJ Henkin. Apply a set of test strips based on 12 dilution of sodium chloride at concentrations ranging from 0.0025 to 5.12%. The level of sensitivity to salt: 0,0025-0,08% - lower threshold; 0.016% - the average; 0,32-5,12% - high. Variability was defined as diastolic blood pressure from visit to visit BP variability within one year. The analysis of the major risk factors.
Results:Average values ?128;??128;?of the level in the two groups correspond to the low level of sensitivity. The level of salt sensitivity in men with masked hypertension aged 20-39 years was 0,02 ± 0,015%; in persons over 40 - 0,08 ± 0,05% (4-fold increase, p <0,008). The level of salt sensitivity in healthy aged 20-39 years was 0,01 ± 0,005%; in persons over 40 - 0,03 ± 0,01% (increase by 3 times, p < 0,01). According to the results of analysis of variance (Kruskal-Wallis criterion) revealed significant differences depending on the level of sensitivity to salt and smoking (p = 0,03), abdominal obesity (p = 0,04), age (p = 0,002), family history of CVD (p = 0,002) and increased dBP (p = 0,004). When comparing men with masked hypertension with healthy revealed that the masked hypertension mean dBP higher than in the daytime at 4 mm Hg (p = 0,008), at night - 5 mm Hg (p = 0,03), on a visit to visit variability in dBP higher than in the daytime and at night (p = 0,004). From visit to visit variability in dBP was the main independent predictor of masked hypertension in men (p < 0,0001). When included in the model is the level of sensitivity to salt predictive value increased 2-fold (p = 0,001).
Conclusion:In men with masked hypertension compared to healthy an increased level of salt sensitivity, which is associated with increased from visit to visit variability in diastolic blood pressure. It has a pathogenetic substantiation and leads to early onset of cardiovascular disease.
P842
Different success rates in lifestyle related risk factors in the first year after acute coronary syndrome
M Minneboo1, M Snaterse2, S Lachman1, H Jorstad1, W Scholte Op Reimer2, R Peters1
1Academic Medical Center, University of Amsterdam, Department of Cardiology, Amsterdam, Netherlands
2Amsterdam University of Applied Sciences, School of Nursing, Amsterdam, Netherlands
Topic: Sports cardiology
Purpose:Lifestyle improvements are difficult to achieve in secondary prevention programs after an acute coronary syndrome (ACS). We evaluated patients with a single lifestyle risk factor (LSRF) (smoking, obesity or physical inactivity) to study differences in success rates.
Methods:We analysed data from RESPONSE, a multicentre randomised controlled trial. Patients (18-80 years) were randomised within 8 weeks after hospitalization for an ACS, to a nurse coordinated prevention program (NCPP) in addition to usual care (intervention) or to usual care alone (control). The intervention consisted of 4 visits within six months, and addressed guideline based risk factor management through medication and lifestyle modification. LSRF's were smoking, overweight (BMI>25) and physical inactivity. Success was defined as no LSRF at 12 months follow-up.
Results:754 participants were included in the RESPONSE study, of whom 278 patients had a single lifestyle risk factor. There was no significant difference in LSRF between the intervention and the control group, both at baseline and at follow-up. Therefore, results are combined. Overweight was the most prevalent risk factor at baseline and remained largely unchanged. The highest success rates were achieved in physical activity and smoking cessation (table).
Conclusion:Success rates differ substantially, overall it is most difficult to achieve weight reduction compared to physical activity and smoking cessation. There is a clear need for more effective interventions, particularly regarding weight reduction.
Baseline
12 months
Risk Factors
Prevalence n (% of total)
Success n (% of subgroup)
Smoking only
68
24%
19
28%
BMI>25 only
132
47%
12
9%
Inadequate physical activity only
78
28%
34
44%
n (% of total)
278
100%
65
23%
P844
Risk factors and their impact on velocity parameters of cardiac electrical activity in chronic alcoholics during acute alcohol withdrawal
AS Gorbunova1, SYU Levashov1
1South-Ural State Medical University, Chelyabinsk, Russian Federation
Objective:to evaluate prevalence of risk factors in patients with alcoholism and their impact on velocity parameters of heart electrical activity Methods:a cross-sectional study of men (n=114), alcohol addicted, aged 35-55 years, with acute alcohol withdrawal compared with healthy controls of the same age (n=34). Patients underwent clinical examination, biochemical tests, ECG, first ECG derivative, Holter monitoring. Key quantitative parameters of first ECG derivative - ventricular activation rate (VAR) and VAR irregularity index (VARII) were used in analysis. Algorithm of detection of first ECG derivative method was suggested by prof. Volkova E.G. Statistical analysis was performed using t-test for independent samples, Pearson's correlation and linear regression analyses. Results are performed as mean±SD.
Results:the prevalence of arterial hypertension was higher in study group (71% vs. 41%, p=0,028), no significant difference in prevalence of smoking between groups was found (59% vs. 38%, p=0,506). The prevalence of smoking among the groups differed not significantly (59 % vs. 38 %, p = 0,506). The level of total cholesterol in study group was lower than in controls (5,05 ± 1,06 vs. 5,54 ± 1,62 mmol / l, p = 0,006). Some electrocardiographic features, like broadening of QRS complex (0,093±0,101 vs. 0,077±0,013 msec, p=0,284) and prolongation of QT interval (0,405±0,045 vs. 0,388±0,026 msec, p=0,276) in study group were not statistically significant. Parameters of first ECG derivative were different in groups (VAR 38,8±2,2 in study group vs. 39,6±1,3sec-¹, p<0,05, VARII 27,3±12,8 vs. 19,2±7,1%, p<0,05). Data demonstrated that VAR in smoking alcoholics was lower than in non-smoking (37,9 ± 2,4 vs. 40,0 ± 1,1sec-¹,p = 0,003). Control group showed a similar nonsignificant trend. The presence of arterial hypertension in both groups was associated with increased VARII compared with those without hypertension (28,7 ± 14% vs. 23,3 ± 7,5%, p=0,047 in study group and 21,1 ± 9% vs. 17,6 ± 4,3%, p = 0,039 in control group). Data did not reveal correlation between hypercholesterolemia and velocity parameters of cardiac electrical activity.
Conclusions:Unfavorable cardiovascular risk profile in men with alcohol heart disease is associated with the direct toxic effects of alcohol and relatively high prevalence of cardiovascular risk factors in study group. The presence of arterial hypertension, in particular combined with smoking, is associated with worsening of velocity parameters of cardiac electrical activity. Hypercholesterolemia does not influence on velocity parameters of cardiac electrical activity.
P845
Temporal trends of risk profile among patients admitted with acute coronary syndrome
G Abreu1, P Azevedo1, C Arantes1, J Martins1, C Braga1, C Quina1, C Vieira1, J Marques1
1Hospital de Braga, Cardiology, Braga, Portugal
Background:Clinical practice focuses on the primary prevention of cardiovascular disease (CVD) through the modification and treatment of cardiovascular risk factors, in order to minimize long-term CVD risk.
Aim:To determine if there are differences in risk profile of patients admitted with acute coronary syndrome over time.
Methods:We analysed 4871 patients admitted consecutively in our coronary care unit with a diagnosis of ACS and included in a prospective registry, from January 2002 to October 2013. Patients were divided in 3 groups of 4 consecutive years: group 1 – from 2002 to 2005 (n=1245, 25.6%); group 2 – from 2006 to 2009 (n=1562, 32%); group 3 - from 2010 to 2013 (n=2064, 42.4%). For each group we studied the prevalence of conventional risk factors (CRF) including diabetes, hypertension, smoking and dyslipidaemia over time and compared findings according to sex and type of acute coronary syndrome.
Results:Women were less prevalent in group 3 (26.2% vs 26.9% vs 22.6%, p=0.006). Temporal trends of age and diabetes did not show statistic signify. Group 2 and 3 evidenced higher body mass index (26.48±4.0 vs 27.13±5.8 vs 27.15±4.67 kg/m2; p<0.001), had higher prevalence of dyslipidaemia (43.1% vs 49.2% vs 56.3%; p<0.001), smoking (39.4% vs 65.0% vs 64.4%; p<0.001) and hypertension (55.7% vs 65.0% vs 64.4%; p<0.001). We found at least 1 CRF in 92,4% of patients. The first temporal period had higher prevalence of 1 or 2 CRF, while two thirds of patients in group 3 had 2 or 3 CRF. Over time, hypertension was more prevalent in women (69.3% vs 77,4% vs 78.6%; p=0,007), on the other hand, smoking and dyslipidaemia occurred more often in men. It was observed an increasing tendency of smoking (44% vs 41.6% vs 54%; p<0.001) and dyslipidaemia (37.2% vs 45.3% vs 50.5%, p<0.001) over time. In those patients admitted with acute ST-elevation myocardial infarction (STEMI), it was observed an increased tendency on smoking. The last period registered LDL levels >100 mg/dl more often (66% vs 57% vs 68.8%; p=0.022), but higher control of systolic blood pressure below 140 mmHg (54.2% vs 59.6% vs 65.7%, p<0.001).
Conclusion:We found that the risk profile of patients presenting with acute coronary syndrome worsened over the years. In recent time, patients had more CRF, being smoking and hypertension the most prevalent cardiovascular risk factors.
P846
Are there differences in the degree of control of cardiovascular risk factors and secondary prevention treatments by gender? The BARIHD study
F Berrocal De Partearroyo1, B Capeans Gonzalez1, P Ramos Calvino1, C Pazo Paniagua1, C Besada Gesto1, R Castelo Dominguez1, A Ramos Gonzalez1, R C Vidal Perez1, F Otero-Ravina1, JR Gonzalez-Juanatey1
1University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
Topic: Sports cardiology
Purpose:Gender differences in relation with the degree of control of the CV risk factors and the secondary prevention treatment are still controversial in the field of the chronic phase of coronary artery disease (CAD). We assessed the influence of gender over these aspects in a long term follow-up of a chronic ischemic heart disease (CIHD)cohort followed by primary care physicians Methods:BARIHD was a cross-sectional multicentric study made with collaboration of 73 PCP. PCP included during February 2007,patients(p) that fulfil the inclusion criteria: coronary artery disease (CAD) with at least 1 year of follow up since diagnosis, diagnosis clear established (stable angina-SA, unstable angina-UA or myocardial infarction-MI) in a discharge summary from cardiology department. Follow-up was done by clinical review and we applied as control criteria the ESC guidelines of Stable Coronary Artery Disease.
Results:1038p were included, 73% male(758), first diagnosis of CAD: male vs. female SA(21 vs.29.3%,p<0.001), UA(19.3 vs.27.9%,p<0.001) and MI(59.8 vs.42.9%,p<0.001), time of evolution after the 1st diagnosis was higher in male 8.2±6.3 vs. 6.9±5.2 years, women were older(mean age 72.4±10.5) and had a worse risk profile, with more hypertension(78.9%), diabetes(34.6%). Differences by gender are showed in the table.
Conclusions:There is room for significant improvement in smoking cessation in men and increase physical activity in women that can lead to improved waist circumference in patients with CIHD.
Men (%)
Women (%)
p-value
Blood pressure control
66.9
61.8
0.141
LDL-Cholesterol <70 mg/dl
22.9
15.2
0.021
Triglycerides <200 mg/dl
88.0
89.5
0.525
HDL Cholesterol >40 mg/dl ?153; or >45 mg/dl ?153;?
61.1
63,7
0.510
Absence of obesity (BMI<30)
61.0
56.2
0.215
Absence of central obesity (<102 cm ?153;/88 cm ?153;?)
53.2
21.4
0.001
Active smoking
10
2.4
0.001
Antiplatelets
74.3
70.2
0.210
Statins
82.8
79.4
0.227
Betablockers
62.7
58.7
0.267
Exercise
46.2
32.0
0.001
P847
Predictors of heart failure occurrence in a population of acute myocardial infarction patients
I Sharka1, S Myftiu1, A Quka2, M Xhafaj1, A Shkoza3, L Cakerri3
1University Hospital Center Mother Theresa, Department of Cardiology & Cardiac Surgery, Tirana, Albania
2University Hospital Center Mother Theresa, Tirana, Albania
3University Hospital Center Mother Theresa, Department of Biomedical and Experimental Sciences, Tirana, Albania
Topic: Sports cardiology
Purpose:the aim of the study was to evaluate the level of heart failure in acute myocardial infarction patients in a tertiary cardiology center; their demographic and clinical background on hospital admission; and the main predictors in occurrence of heart failure during acute myocardial infarction hospitalization.
Methods:we prospectively analyzed demographic and clinical data on 397 consecutive AMI patients from January 2013 to May 2014; Framingham criteria were used to determine HF patients on admission and Killip class =2 at any time of hospitalization with follow-up extended to three weeks; valvular and nonischemic cardiomyopathies were excluded; a logistic regression model was used to define predictors of heart failure occurrence.
Results:heart failure was identified in 106 (26.7%) pts of our AMI population; heart failure group differed significantly from the rest regarding: age (69.1±11.2 vs 62.9±11.6, p<.0001); sex (male) (62.3% vs 82.4%, p<.0001); heart rate on admission (80.06±19.35 vs 70.64±11.13, p<0.001); systolic BP on admission (119.9±30.5 vs 130.9±24.2, p=.001); prior MI (21.7% vs 7.9%, p<.0001); glycemia on admission (168.5±83.3 vs 143±77.9, p=.007); prior HTN treatment (35.5% vs 64.5%, p=.031); prior coronary revascularization (10.4% vs 3.5%, p=0.012); peripheral vascular disease (11.4% vs 3.5%, p=.005); chronic renal disease (12.3 vs 4%, p=.005); EF (36.9±9.1 vs 57.2±5.7%, p<.0001); anemia (18.9% vs 7.9%, p=.003); AF occurrence (8.5% vs 1.8%, p=.003); no significant differences in HTN (p=0.923), diabetes (p=0.114), dyslipidemia (p=.987); presence of STEMI (.141); smoking (p=0.054). Independent predictors of HF occurrence in logistic regression were: EF OR 4.75 (95%CI:1.73 -13.03); prior revascularization OR 3.86 (95%CI:1.34- 11.1); peripheral vascular disease OR 2.14 (95%CI: 1.67-4.3); age OR 1.83 (95%CI: 1.25-3.16); sex OR 0.42 (95%CI: 0.23-0.76); prior MI OR 1.89 (95%CI: 1.12-4.03); systolic BP on admission OR 0.87 (95%CI: 0.63-0.91); anemia OR 1.67 (95%CI: 1.35-2.84).
Conclusions:regardless lowering trends in mortality following AMI, heart failure remains an important complication in our daily clinical practice; special attention should be paid to the most vulnerable population especially elderly pts, women, those with known coronary disease and comorbidities.
P848
The role of endothelial dysfunction in the development of different forms of coronary artery disease among women
I A Leonova1, S Boldueva1, V Feoktistova1, O Sirotkina1, A Lipunova1, L Gaykovaya1
1North-Western Sate Medical University named I.I. Mechnikov, St-Petersburg, Russian Federation
Summary:Currently, the leading role in the pathogenesis of coronary artery disease (CAD) is given any cause of endothelial dysfunction (ED). However, it remains an open question about severity of ED in various forms of ischemic heart disease.
bjective:To determine the level of circulating endothelial cells in women with atherosclerosis of the coronary arteries, women with "microvascular angina" and the women of the control group.
Materials and Methods:The study included 136 women, of whom 62 women with coronary heart disease due to atherosclerosis of the coronary arteries ( mean age 50,7 ± 6,4 years) 25 women with " microvascular angina " (mean age 57,3 ± 1,6 years) 49 women of the control group with no history of cardiovascular disease (mean age 52,3 ± 9,2 years). Determining the level of circulating desquamated endothelial cells (CEC ) was provided by flow cytometry.
Results:The average level of circulating endothelial cells in peripheral blood in women with coronary atherosclerosis was 7,4 ± 10,1 cells / ml in the group with CSX - 11,9 ± 9,8 cells / ml in the control group - 3,9 ± 3.0 cells / ml . When compared groups was found that significantly higher levels of CEC in both groups of women with coronary artery disease (group of the atherosclerosis with p = 0.003 for a group with CSX p < 0.00005 ) , wherein between the two groups of women with atherosclerosis and CSX also observed significant differences (p = 0.003) .
Conclusion:In our study, we demonstrated that endothelial dysfunction is the place to be in women with coronary heart disease due to atherosclerosis of the coronary arteries, and in women with cardiac syndrome X. In this case, a more pronounced ED dysfunction observed among women with CAD, as a result of microvascular disturbances.
P849
Prevalence of thyroid disease in patients with atrial fibrillation: Clinical practice evaluation to avoid complications associated with thyroid dysfunction
Atrial fibrillation( AF) is the most common arrhythmia in clinical practice and accounts for at least a third of hospitalisations due to cardiac rhythm disturbance. Paroxysmal and persistent AF affects 2.2 million Americans and 6 million Europeans. Patients with AF also have increased risk of impaired cognition, quality of life and exercise capacity, left ventricular dysfunction, and 5-fold increase risk of stroke resulting in increased health provision cost. Thyroid dysfunction which has the prevalence of 10-25% in elderly patients is one of the disabling treatable risk factors for AF and have been associated with significant increased risk of AF.Current guidelines advise aggressive treatment for patient with subclinical hyperthyroidism, as to prevent associated complications.
AIM:To assess the prevalence of thyroid disease in patients presenting with AF to our 150 beds midland hospital. Also to assess the management of their abnormal thyroid status.
Results:501 presentations including 110 patients were recorded over a period of 12 months. Mean age was 72 ±11 years (Range 41-94years). 21 patients were excluded due to missing data. Of 89 patients, they were 49 males and 40 females. Mean length of stay was 3 days ( range 1 – 16 days). Thyroid function status was assessed in 87% (n=77). 23.2% (n=16) had thyroid dysfunction; 5.9% ( n=1) had overt hyperthyroidism; 35.3% (n=6) had subclinical hypothyroidism and 58.8% (n=10) had under-reactive thyroid. 69.7% (n=62)of patients were hypertensive, 29.2% (n=26) had coronary arterial disease, 27.0%(n=24) had congestive heart failure, 24.7% (n=22) had ischaemic heart disease, 16.9% (n=15) were diabetic, 11.2% (n=10) had lower tract infection and 7.8% (n=7) had cerebro-vascular accident or transient ischaemic attack.
Discussion:In our audit, the prevalence of thyroid dysfunction tests abnormalities in patients admitted with known or new diagnosis of atrial fibrillation was 23.2%. This is significantly high compared to previous surveys. However, this is not a surprise because other surveys were performed in the community while our study involves acute hospital admissions, therefore, most of the patients will be acutely unwell resulting in abnormal thyroid function as a response to stressful body environment. Also our population is older and thyroid dysfunction is thought to be higher with increased age.
Conclusion:We recommend thyroid function assessment in all patients with AF to prevent complications associated with the disease. Patients with missing data of their thyroid status were called and their TSH was checked and were treated accordingly.
P850
Monocyte subsets in patients with severe aortic valve stenosis undergoing TAVI
SCD Au1, A Ludwig1, V Stangl1, G Baumann1, K Stangl1, B Hewing1
Purpose:Aortic valve stenosis (AS) represents a chronic inflammatory disease. Its pathogenesis shares profound similarities with atherosclerotic plaque development including the central role of macrophages in disease progression. Monocytes are the precursor of macrophages and individual monocyte subsets have been associated with cardiovascular risk. Therefore, we assessed the hypotheses that monocyte subsets differ in the presence of severe AS compared to an AS-free setting and may change by intervention of AS.
Methods:Classical (CD14++CD16-), intermediate (CD14++CD16+) and non-classical (CD14+CD16++) CD86 positive monocyte subsets and monocyte activation (median fluorescent intensity of CD11b) were determined by flow cytometry in peripheral blood from patients with severe AS (n=59) and matched AS-free controls (n=50). A follow-up evaluation of monocyte subsets and activation was performed in AS patients undergoing transcutaneous valve implantation (TAVI) 3 months after the procedure (n=18).
Results:There were no significant differences in the absolute monocyte counts between AS patients and controls. In contrast, AS patients exhibited a shift towards CD16+ monocytes subsets with a significant higher proportion (median [IQR] 6.7% [5.2-8.5%] versus 5.7% [4.6-6.7%]; p=0.003) and absolute counts (median [IQR] 39.9/µL [29.6-63.3/µL] versus 33.5/µL [24.4-44.0/µL]; p=0.015) of intermediate monocytes compared to controls. Classical and non-classical monocytes and monocyte activation did not differ significantly between the groups. There was no significant change in the distribution of monocyte subsets or in monocyte activation 3 months after TAVI compared to baseline.
Conclusions:We found preliminary evidence for a significant difference in the distribution of monocyte subsets in patients with severe AS compared to AS-free controls indicating an involvement of monocyte subsets in the pathogenesis of AS. Monocyte subsets and activation did not change after treatment of AS by TAVI within the first three months following the procedure.
P852
Use of SCORE charts among a population of immigrants from high risk european countries in an irish setting
L Tobin1, I Gibson2, G Flaherty1
1National University of Ireland, Galway, Ireland
2Croi West of Ireland Cardiac Foundation, Galway, Ireland
Topic: Sports cardiology
Purpose:Deaths due to cardiovascular disease (CVD) number 4 million annually in Europe with significantly higher mortality rates seen in Eastern Europe. Large numbers of citizens from Central and Eastern Europe migrated to Ireland in the last decade. There has been no research to date on the health status of these immigrants and the potential impact of migration on national and individual CVD risk levels. In addition there is currently no guidance from the European Society of Cardiology as to which SCORE chart is to be used for risk scoring in these migrant groups from high risk countries while resident in a low risk nation.
Methods:This study used convenience sampling to recruit subjects from the eligible non-national population of one Irish city. Adults over 18 years and from any of the high risk countries of Europe (according to the SCORE risk estimation tool) were invited to partake. Screening was offered in occupational and community settings; a non-fasting lipid profile and blood pressure measurements, subjective questioning regarding physical activity levels, alcohol consumption and smoking status. The SCORE risk tool and relative risk categorisation were used to calculate CVD risk.
Results:81 participants with a mean age of 41 years took part in this study. The majority were Polish (n= 72, 89%) and 54% (n=44) were male. Very high levels of hypertension (55%) and hypercholesterolaemia (61%) were observed in those aged = 40 years. High risk of fatal CVD was documented in 42% (n=16) of the older subjects when high risk or country-specific SCORE charts were used.
Conclusions:This study confirms the need for further investigation of the CVD risk profile of immigrants with many older migrants displaying significant risk levels. There is potential for serious under-estimation of risk when the low-risk SCORE chart is used.
LDL, low density lipoprotein
Characteristics
Mean
Standard Deviation
Recommended Clinical Target
Percent Not Meeting Target
Age (years)
40.6
13.3
Length of residency (years)
7.2
3.2
Systolic blood pressure (mmHg)
138.0
18.5
<140
37
Diastolic blood pressure (mmHg)
84.6
11.4
<90
22.1
Total cholesterol (mmol/l)
4.9
1.1
<5.0
42
LDL cholesterol (mmol/l)
2.8
1.0
<3.0
40
P853
Assessing the risk for cardiovascular diseases using Procam/HeartScore in hypertensive patients. A survey with 961 employees
S Hossain1, A Raethling1, T Bitter1, O Oldenburg1, R Gottfried1, F Buuren1, D Horstkotte1, KP Mellwig1
1Heart and Diabetes Center NRW, Ruhr-University of Bochum, Department of Cardiology, Bad Oeynhausen, Germany
Topic: Sports cardiology
Purpose:Hypertension has long been identified as important risk factor for a number of health problems. The excessive pressure on the artery walls caused by high blood pressure can damage your blood vessels, as well as organs in your body. The higher your blood pressure and the longer it goes uncontrolled, the greater the damage.The aim of the present project is to reveal the significance of hypertension as a risk factor for cardiovascular disease.
Methods:960 employees of different companies were investigated between May 2013 –September 2014. The cardiovascular risk was determined using the PROCAM score (allows the early detection of the risk of contracting a disease thereby providing the possibility of a timely prevention, especially in high risk groups whose disorders have not manifested clinically yet) and HeartScore (The tool for predicting and managing the risk of heart attack in Europe). We examined 388 women and 572 men (age 43±10.77 years). Increased systolic blood pressure (> 140 mmHg) was found in 367 employees (38.23%), increased diastolic blood pressure (> 90 mmHg) was found in 163 employees (16.98%).Increased systolic and diastolic blood pressure (> 140 / > 90 mmHg) was found in 138 employees (14.38%), only 63 of them (45.65%) were under antihypertensive therapy. The PROCAM-Score was > 20 in 5 employees of the hypertension group (3.62%) and in 4 employees of the non-hypertension group (0.71%). HeartScore was above 5 in 20 patients (14.49%) of the hypertension group and in 5 patients (0.88%) of the non-hypertension group. 156 employees (16.23%) were referred to their general practitioner, 101 (10.59%) to a cardiologist. Obese patients (BMI> 30) were found in 24.64 % of the hypertensive patients and in 8.11 % of the normotensive group. However there was a higher amount of smokers in the normotensive group (36.16%) compared to the hypertensive group (31.88%).The percentage of high LDL-Cholesterol levels was more than double in the hypertensive group (21.74 % vs. 9.17 %). The percentage of high HbA1c values was five times higher in the hypertensive group (11.59 % vs. 2.29 %).
Conclusion:Our Screening revealed that over 54 % with hypertension had no antihypertensive therapy so far. Although there was only a small percentage of hypertensive employees (~14%), the significant higher risk for cardiovascular disease was apparent in both score systems: The percentage of HeartScore = 5 was thirteen times higher and PROCAM = 20 was five times higher in the hypertensive group. Therefore extensive diagnostic measures in prevention are required.
P854
Cardiovascular prognostic predictive value of the TIMI, PAMI, CADILLAC, Zwolle primary PCI index and GRACE risk scores undergoing primary PCI
P Rio1, R Ramos1, T Pereira-Da-Silva1, M Afonso Nogueira1, P Pinto-Teixeira1, A Viveiros Monteiro1, A Fiarresga1, D Cacela1, L Sousa1, R Cruz Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Aims:There is a wealth of short-term mortality risk scores for ST-elevation myocardial infarction (STEMI). However, is not known weather these scores can predict long term mortality or other important prognostic markers. Our aim was to compare the predict value of several well-known risk scores for the occurrence of myocardial infarction (MI), target-vessel revascularization (TVR), non-elective cardiac readmission, cardiac death or all-cause mortality during a 5-year follow-up. Methods andResults:Patients who underwent primary PCI from January 2003 through August 2007 in a single tertiary-center were analysed (n=665) using a dedicated prospective STEMI database. TIMI, PAMI, CADILLAC, Zwolle primary PCI index and GRACE risk scores were calculated for each patient. We assessed the predictive accuracy of each of these scores for all cause and cardiac-death, reinfarction (re-MI), TVR, non-elective readmission at 1 and 5 years and also for non-elective cardiac readmissions at 30 days and 1 year, using the C statistic, which was obtained by means of logistic regression and ROC curves All-cause mortality was 22.1%, cardiac death 15.2%, re-MI 17.7%, TVR 12.3% and non-elective cardiac readmission 32.2% after at completion of 5-year follow up. The TIMI, PAMI, CADILLAC, Zwolle primary PCI index and GRACE showed a good predictive value for 30-days and 1-year mortality (C statistic range, 0.789-0.866) with a decreased in predictive value at 5-year all cause mortality (C statistic range, 0.744-0.793). The performance of these 5 scores was poor for both reinfarction and TVR (C statist range 0.417-0.473). The prediction of non-elective cardiac readmission at 30 days and 1 year after PPCI was weak (C statistic of 0.497 and 0,679, respectively). Conclusions:Risk scores provide good information for the stratification of 30-days and 1-year risk mortality in patients treated by primary PCI, but they fail when trying to predict reinfartion, TVR or non-eletive cardiac readmission. It is also necessary to find models for better prediction of mortality at long-term.
P855
Which patients benefit more from smoking cessation programme
C Ruivo1, D Fernandes2, L Pinto2, R Saraiva2, R Pires1, J Morais1
1Hospital Santo Andre, Cardiology, Leiria, Portugal
2Hospital Santo Andre, Internal Medicine, Leiria, Portugal
Introduction and Purpose:Smoking cessation (SC) is one of the most effective strategy towards the reduction of morbidity and mortality tobacco related. This study aims to describe patients, followed on this programme, in terms of demography and associated co-morbidities and correlate them with changes in tobacco consumption.
Methods:We retrospectively described and analyzed smoker patients referred to a SC appointment, from January 2013 to February 2014. Besides a counselling and motivational support, all patients initiated pharmacotherapy for smoking cessation. We compare the reduction of tobacco load between first and second appointments.
Results:93 patients were considered in the first appointment, however 22 (24%) missed their second appointment being therefore excluded. 71 smokers were evaluated, mean age was 49±12 years, 45 (63%) male. 38 (54%) patients had a cardiovascular risk factor other than smoking: dyslipidemia was present in 32 (45%) of them, high blood pressure in 23 (32%), BMI>25kg/m2 in 11 (16%) and Diabetes mellitus in 8 (11%). 53 (75%) had tobacco associated diseases: 23 (32%) had previous cardiovascular ischemic event (include acute myocardial infarction and stroke), 20 (28%) had respiratory disease, 4 (6%) had cancer and 6 (9%) had other tobacco associated disease. In analyses, 6 (8%) of the patient increased, 22 (32%) maintained, 25 (35%) reduced and 18 (25%) stopped smoking. The average tobacco load was 22±11 in first and 12±10 in second appointment. Table shows the average of cigarettes per day (cig/d)(±SD) reduced from first to second appointment and compares it between the presence and the absence of different diseases.
Conclusions:The success of SC programme is evident in individuals with previous cardiovascular disease. An additional motivational effort should be implemented for the remaining individuals not affected by any disease.
Presence
Absence
p-value
Any tobacco associated disease
13.4 (±13.5) cig/d
2.8 (±10.4) cig/d
p<0.001
Cardiovascular ischemic event
16.9 (±11.4) cig/d
7.7 (±13.5) cig/d
p<0.001
Dyslipidemia
14.1 (±13.9) cig/d
7.9 (±12.6) cig/d
P=0.026
High Blood Pressure
14.2 (±9.5) cig/d
8.9 (±14.8) cig/d
P=0.015
BMI>25kg/m2
18.2 (±12.5) cig/d
9.3 (±13.3) cig/d
P=0.011
Diabetes mellitus
16.3 (±5.2) cig/d
9.9 (±14.1) cig/d
P=0.027
P856
Factors influencing prevalence of smoking in a southern Indian province
A Geevar Zachariah1, S Harikrishnan2, M N Krishnan3, G Sanjay2, S Devika4, K R Thankappan5, P P Mohanan6, K Venugopal7
1Mother Hospital, Cardiology, Thrissur, India
2Sree Chitra Tirunal Institute for Sciences and Technololgy, Cardiology, Thiruvananthapuram, India
3Kozhikode Medical College, Cardiology, Kozhikode, India
4Christian Medical College, Biostatistics, Vellore, India
5Sree Chitra Tirunal Institute for Sciences and Technololgy, Public Health, Thiruvananthapuram, India
6Westfort Hitech Hospital, Cardiology, Thrissur, India
7Pushpagiri Medical College, Cardiology, Thiruvalla, India
Topic: Sports cardiology
Purpose:Kerala, southernmost state in India declared smoking in public illegal by a court judgement in 1999 much before India banned the same in 2008. However prevalence of smoking has not come down in this population. The purpose of this study was to find out current prevalence and factors influencing smoking in Kerala.
Methods:5167 participants (mean age 50.8 years, 40.1 % men) of Cardiological Society of India Kerala Coronary Artery Disease and its Risk Factors Prevalence (CSI Kerala CRP) Study were interrogated as to smoking habits, consumption of alcohol, educational status and standard of living by a structured questionnaire. The study was conducted in the year 2011. Participants were selected by multistage random sampling from rural and urban areas in the northern, middle and southern parts of the state.
Results:We found that the age standardized prevalence of smoking among men in Kerala was 28.05% with no significant difference between urban (30.45%) and rural (26.97%) areas (P=0.07). Smoking was significantly less prevalent in the 20 – 39 years age group (23.8%) compared to 40 – 59 years (33.8% p < 0.001) and 60 – 79 years (33.3% p < 0.001). We also noted a gradient in the prevalence of smoking with respect to educational status. It was 40.2 % among men with 0 – 4 years of education and 20.1% with > 10 years of education (p < 0.001). A similar but less pronounced gradient was noted with respect to standard of living index. Men with low standard of living index were found to have higher prevalence of smoking (34.3 %) compared to men with high standard of living index (23.5%) (p < 0.01). We also found significant relationship between alcohol use and smoking in this population. Men who admitted to consume alcohol had a prevalence of smoking of 40.6% compared to 14.7% smoking prevalence in those who did not admit to consumption of alcohol (p < 001). Among men currently smoking, 55.04 % started smoking between ages 20 to 30 years, 37.52% below 20 years of age and rest above 40 years of age. Mean age of initiation of smoking was 21 (SD 6.93). Smoking was found to be very uncommon among women in this study (0.18%).
Conclusions:Overall prevalence of smoking among men was high in Kerala. However prevalence was low among younger men and also those with higher levels of education and standard of living. Smoking was also low among men not consuming alcohol. Majority of men started smoking after twenty years of age. Smoking was very rare among women in Kerala. These findings may be relevant in formulating strategies to reduce smoking in Kerala.
P857
The delivery of smoking cessation advice to hospitalised smokers: A two-hospital survey
L Mellon1, NG Mcelvaney1, L Cormican2, A Hickey1, H Mcgee1, R Conroy1, L Ekpotu1, O Oghenjobu1, R Mcdonnell1
1Royal College of Surgeons in Ireland, Psychology, Dublin, Ireland
Purpose:Smoking is the single most preventable cause of disease, disability, and death. Hospitalisation is an ideal time to implement cessation interventions, and brief cessation advice from healthcare practitioners increases quit rates among hospitalised smokers. However, little is known about the extent inpatients receive such advice. This study aim determined the prevalence of smoking and cessation advice received by in-patients in two teaching hospitals in Ireland.
Methods:This study surveyed 1001 in-patients across two hospital sites, over a six month period. Demographic details, clinical history, smoking history, motivation to quit (Motivation to Stop Scale), cigarette dependence (Fagerstrom Test for Nicotine Dependence) and recent quitting history were assessed. Patients identified as smokers also consented to a follow-up telephone call at 3-months post-hospitalisation to establish post-discharge smoking behaviour, and establish if any quit attempts occurred. Self-reported quitters were asked to provide a breath sample using a carbon monoxide monitor (CO) to objectively assess smoking status at 3-months.
Results:Prevalence of smoking within the sample was 23.4% (235/1001). 20.6% (n=49) reported that they would like to receive smoking cessation advice whilst in hospital. Only 32% (n=75) reported that smoking cessation was discussed with them during admission. Smoking status of the patient was documented in 57% (n=132) of cases, however delivery of smoking cessation advice was documented in 2% (n=5) of cases. Attitudes towards smoking cessation were positive amongst hospitalised smokers. At 3 months, 17% of smokers reported smoking cessation, with 68% confirmed on CO test.
Conclusions:A strong, systematic focus on smoking cessation is needed in hospital settings. Although average dependence scores suggest that low-intensity interventions will probably suffice for most smokers, some vulnerable patients will require more intensive interventions.
P858
AMI is in the air: Relationship between tobacco sales and myocardial infarction incidence
C A Alvarez-Ortega1, J Fernandez-Bobadilla1, R Dalmau1, O Gonzalez1, R Mori1, Z Blazquez1, A Castro1, JL Lopez-Sendon1
1University Hospital La Paz, Cardiology, Madrid, Spain
The relationship between active and passive tobacco consumption and cardiovascular disease is well established, existing several studies that link tobacco consumption with the incidence of cardiovascular events. Some European countries have legislated banning tobacco consumption in public places, as is Spain, where two laws were promulgated in 2005 and 2010. Data suggest that these legislative measures had an impact in smoking rates among population. Based on that fact, it is to expect that tobacco sales would have a strong relationship with the incidence of AMI. The aim of this study is to analyse the relationship between tobacco sales and the incidence of AMI in Spain during the period 2002-2012.
Methods:We obtained data from the Spanish Tobacco Market National Commission of nationwide annual sales of 20-cigarret packages during 2002-2012. We also took data from the Spanish Hospital Morbidity Survey from that period of hospital morbidity rates for acute myocardial infarction (ICD-9-CM 410). A correlation analysis was made between number of 20-cigarrete packages sold per year per person and the hospital morbidity rates by diagnose.
Results:There was a positive correlation between 20-cigarrete packages sales and myocardial infarction discharge rate (Spearman rho 0.964, p<0.001). During period 2002-2012, there was a gradual reduction of tobacco sales and myocardial infarction. Conclusion:There is a strong correlation between tobacco sales and the incidence of AMI in Spain. These data support the hypothesis that legislative measures oriented to diminish tobacco consumption have a rapid effect on the incidence of AMI.
P859
A cohort study of early cardiologist consultation by telemedicine on the critical Non-STEMI inpatients
WISIT Wichitkosoom1, SUWANA Patee1
1cardiac center, medicine department, udonthani hospital, udonthani, Thailand
Objectives:To find out the more effect of early cardiologist consultation using a simple technology on the diagnosis and early proper management of patients with Non-STEMI at emergency department of district hospitals without cardiologist on site before transferred.
Methods:A cohort study was performed in the general hospital From 1 October 2012 – 30 September 2013 with 892 patients diagnosed with Non-STEMI. All patients mean aged 46.8 years of age who had been transferred because of Non-STEMI diagnosed, over a 12 week period of studied. Patients whose transferred, in addition to receiving proper care, were offered a cardiologist consultation with average time to Udonthani hospital 1.5 hour. The main outcome measure was length of hospital stay, mortality at 3 months, inpatient investigation, and transfer rate to the higher facilitated hospital were also studied.
Results:Hospital stay was significantly shorter for those didn't consult cardiologist (hazard ratio 1.19; approximate 95% CI 1.001 to 1.251; p = 0.039). The 136 cases were transferred to higher facilitated hospital. No statistically significant in overall mortality between the groups (p=0.068).
Conclusions:Early cardiologist consultant can reduce length of hospital stay for patients with cardiovascular conditions outside of cardiac center. The new basic technology can apply for the safety patient.
P860
Effect of education and telephone monitoring on exercise tolerance and health-related quality of life in patients with chronic heart failure: a prospective randomized controlled parallel-group study
D S Komkov1, R P Myasnikov1, N P Fedotova1, S A Boytsov1
1State Research Centre for Preventive Medicine, Moscow, Russian Federation
Topic: Sports cardiology
Purpose:To assess efficacy of education and telephone monitoring in patients with chronic heart failure.
Methods:The study included 40 patients with chronic heart failure discharged from hospital. They were randomized on telemonitoring (short-term educational program + active telephone calls by physician every 2 weeks in the first 3 months and then monthly) group (n = 20) and usual care group (n = 20). The period of follow-up was 9 months by the date of abstract submission. The study will be continued up to 12 months follow-up.
Results:At the start of study there weren't significant difference between telemonitoring and usual care groups on age (60.6 ± 14.7 and 56 ± 14.1 years, respectively; p = 0,32), Minnesota Living With Heart Failure Questionnaire (MLHF) score (65.6 ± 9.8 and 67.9 ±12.0, respectively; p = 0.64) and 6-min walk distance (207.9 ± 98.9 and 164.5 ± 59.27 m, respectively; p = 0.18). The left ventricular ejection fraction (LVEF) was significantly lower in the telemonitoring group (25,7 ± 9,3 % and 32,5 ± 11,3 % in usual-care group; p = 0,04). After 9-month follow-up the MLHF scores and 6-min walk distance were improved comparing to initial ones in both groups. Furthermore, MLHF scores in telemonitoring group was significantly lower (38.5 ± 9,5) than in usual-care group (47.4 ± 11,4, p < 0,001). 6-min walk distance was significantly longer in telemonitoring group (402,6 ± 62,2 and 298,8 ±99,3 m in usual-care group, p = 0,002). The LVEF, readmissions and mortality will be assessed after 12-month follow-up period.
Conclusion:Education and telephone monitoring improves health-related quality of life and exercise tolerance in patients with chronic heart failure.
P862
Traditional telehealth parameters are not as good as they pretend
K J G Schmailzl1
1Ruppiner Kliniken, Medizinische Klinik A, Neuruppin, Germany
Purpose We still do not know if and which parameters collected and transferred telemedically will provide useful prognostoc Information. Concerning chronic heart failure patients this is claimed above all for body weight. The relevance of other parameters like mean heart rate, blood pressure, oxygen saturation is unknown. Not least for that reimbursement of telemedicine remains uncovered.
Methods:We equipped 126 chronic heart failure patients with diaries, 50% of them having ICDs or CRT-Ds. We asked them to note - on a per diem base - their state of health ('good', 'fair', 'fairly poor", 'lousy'), to take their body weight, their blood pressure, and their pulse. We asked them to record the data into their individual diary. Follow-up was one year, during which we included all hospitalisations for heart failure associated reasons, ICD Shocks, and deaths. After all, we compared events occurred and prognostic parameters.
Results:There was no directed interrelationship between adverse events and: body weight, blood pressure, and pulse. Most adverse events were arrhythmias leading to hospitalisation, shock delivery or death. Exacerbated congestive heart failure (pulmonary edema) was relatively rare in our patients being on standard heart failure medication and in continous contact with their family doctor. Thge most valuable prognostic variable proofed to be their semi-quantitative self-assessment and - concerning the ICD/CRT-D patients - the frequency and complexity of arrhythmias that preceded an serious adverse event.
Conclusions:Traditional parameters in eHealth (like daily blood pressure) do not permit to predict serious adverse events in chronic heart failure patients. Even self-assessment of patients seems to be superior. The only parameter of prognostic value seems to be - at least in times of accepted standards of heart failure medication - the frequency and complexity of ventricular arrhythmias. Other parameters we should like to have seem to be be far more tricky and complex than these established ones.
P864
Hypertension in young adults after repaired coarctation of the aorta: a reason for concern in exercise?
A Monteiro1, A Abreu1, A Agapito1, SA Rosa1, P Rio1, I Rodrigues1, G Portugal1, PP Teixeira1, S Silva1, RC Ferreira1
1Hospital Santa Marta, Department of Cardiology, Lisbon, Portugal
Background:Postoperative follow-up of aortic coarctation (ACo) is often characterized by persistent arterial hypertension that is one of the causes of sudden cardiac death in this population. It has been suggested a residual narrowing at the site of surgical repair as a probable mechanism, however, a better understanding of the exercise hemodynamic response is needed. The purpose of this investigation was to study the impact of baseline hypertension after successful surgical repair of ACo using exercise stress doppler echocardiography.
Methods:Thirty consecutive patients (51.9% male) were studied after ACo repair (age at repair 3.3+/-2.6 years) and underwent, at 30.1 ± 8.25 years of age, an exercise treadmill testing with echocardiographic examination. The following parameters were evaluated: peak and mean doppler gradients and velocities in ascendant and descendent aorta (at rest and at maximum stress).
Results:All patients underwent test exercise (15.93 ± 4.0 minutes) with no severe complications such as syncope, ischemic or arrhythmic events. Forty-one percent of the patients had previous documented hypertension previous to exercise testing (Group A). At maximum stress, Group A presented a significant increase in peak gradient and velocity in descent aorta (respectively 20.2 ± 6.9 to 45.4 ± 23.9; p=0.027 and 2.0 ± 0.5 to 3.0 ± 1.0; p=0.020). In Group B, peak gradient and velocity in descent aorta also raised respectively from 25.9 ± 10.6 to 54.4 ± 17.2 (p<0.001) and from 2.63 ± 0.7 to 3.78 ± 0.42 (p=0.001). However, although overall similar uprise in doppler echocardiographic findings, when comparing both hypertensive and non hypertensive patients, no significant differences were found in descendent aorta parameters (?ak gradient 25.3±19.8 vs 27.9±18.3, p=0.730; (?ak velocity 0.79±0.9 vs 0.55±0.6, p=0.836). The same trend was verified in ascendant aorta values.
Conclusions:Hypertension at rest was moderately frequent despite apparently good surgical results after repair of AoC. Despite hypertensive patients revealed a significant increase in aorta doppler parameters, this didn't seem to be different or more danger as it was among patients with normal tensional values.
P866
Effects of a 2-week HIIT on the cardio and respiratory fitness of adult women
GE Pieles1, L Gowing2, AG Stuart3, CA Williams2
1Bristol Heart Institute, National Institute for Health Research (NIHR) Cardiovascular Biomedical Research Unit, Bristol, United Kingdom
2University of Exeter, Children's Health and Exercise Research Centre, Exeter, United Kingdom
3Bristol Heart Institute, Bristol Congenital Heart Centre, Bristol, United Kingdom
Background:High-intensity interval training (HIIT) has been found to induce significant skeletal and cardiac adaptations in males in as little as 2 weeks but limited research in active females. These adaptations have been observed using echocardiography and cardiorespiratory measurements. Therefore, the purpose of this study was to investigate the female training response of skeletal and/or cardiac adaptations from a 2-week HIIT programme.
Method:12 healthy female cyclists (mean age 46.5 ± 8.2 y) completed a stepwise exercise test to volitional exhaustion on a recumbent cycle ergometer before and after HIIT training. The training consisted of 6 sessions (5 maximal 30 s bout, 4 min recovery between each bout) over 12 days (+/- 2 days). Resting echocardiography assessed LV and RV function within one week pre and post HIIT using 2-D, pulse-wave tissue Doppler imaging and 2-D speckle tracking echocardiography (2-D STE). Images were acquired using a 4-MHz transducer, 2-D STE systolic circumferential strain (CS) analysis was performed at the rate of 30-90 frames per second from parasternal short axis view.
Results:There was a significant improvement in VO2max, with a mean increase of 10% post-training (p=0.006). In addition, HRrest, FS%, E' and TAPSE showed trends pre to post-training that are indicative of exercise-training adaptations.
Conclusion:Maximal oxygen uptake is significantly increased in a cohort of active females following a 2-week HIIT programme. A number of cardiac variables displayed discernible changes as a result of HIIT, whilst 2-D CS remained unchanged. Therefore, physiological change was evident in the VO2max, but the discernible changes in cardiac function were not evident and thus unlikely to be responsible for the improvement in aerobic power.
VARIABLE
PRE-TRAINING
POST-TRAINING
p VALUE
Maximal Oxygen Consumption (VO2max) (mL/min/kg)
41.4 ± 5.41
45.8 ± 6.40
0.006*
Volitional Exhaustion End Time (mm:ss)
23:30 ± 3:36
23:50 ± 3:52
0.962
Resting Heart Rate (HRrest) (bpm)
64.36 ± 9.23
59.91 ± 9.31
0.076
Resting Circumferential Strain (CSrest)
-24.91 ± 4.56
-25.77 ± 5.09
0.977
Fractional Shortening (%)
30.48 ± 3.26
33.38 ± 3.71
0.082
Tricuspid Annular Plane Excursion (TAPSE) (mm)
24.04 ± 3.13
26.41 ± 3.86
0.084
Peak Diastolic Myocardial Velocity (E') (cm/s)
9.09 ± 3.52
11.30 ± 2.40
0.094
P867
Utility of heart rate recovery in elite athletes: index of cardiopulmonary fitness?
L Millar1, G Finocchiaro1, K Prakash1, H Dhutia1, A Malhotra1, R Narain1, A Merghani1, V Gabus1, M Papadakis1, S Sharma1
1St George's University of London, Cardiovascular Sciences, London, United Kingdom
Topic: Sports cardiology
Purpose:Attenuated heart rate recovery (HRR) has been associated with increased cardiovascular morbidity and mortality. In contrast, an accelerated HRR is perceived as a marker of cardiovascular fitness and faster HRR has been reported in endurance athletes. There is, however, conflicting evidence relating to potential correlation of HRR with peak oxygen consumption (peak V02) in athletes. We sought to examine the role of HRR as an index of fitness in elite athletes and its association with peak V02.
Methods:Thirteen elite endurance athletes who participated in rowing, endurance running and cycling and 26 team sport players were recruited into the study. All athletes underwent echocardiography and cardio-pulmonary exercise test (CPET), in addition to standard pre-participation evaluation. Athletes were exercised to exhaustion on an upright cycle ergometer using a ramp protocol 20-30 W/min. Heart rate was recorded at baseline, peak exercise and 1 and 2 minutes into recovery.
Results:Endurance athletes demonstrated a higher peak V02 compared to team sport athletes (55.4±6.4 vs. 44.0±5.2 ml/kg/min, p<0.001). There was no difference in the mean HRR between endurance and team sport athletes neither at 1 minute (22.3±7.7 vs. 27.1±11.6, p=0.189) nor at 2 minutes (49±10.3 vs. 50.6±8.7, p=0.617) into recovery. In addition our analysis failed to demonstrate any correlation between HRR and a number of ECHO and CPET parameters, including left ventricular cavity size and wall thickness, indices of systolic and diastolic function, baseline and peak heart rate, baseline blood pressure, duration of exercise, peak VO2, VE/VCO2 and lactate threshold. Of importance, the range of HRR in athletes was wide (11-46 at 1 minute), with 23% (9/39) of athletes exhibiting a HRR <18.
Conclusions:In keeping with previous studies, this study demonstrated a higher peak V02 in endurance athletes compared to team sport athletes, indicating higher fitness levels. In contrast, HRR was similar in the two groups and did not demonstrate any correlation with peak VO2, questioning its value as an index of cardiovascular fitness in elite athletes. Nearly a quarter of the athletes had HRR considered pathological, highlighting the limited value of attenuated HRR as a predictor of cardiovascular morbidity in this group.
P868
The influence of sport related anaemia on the cardiopulmonary function in marathon runners
A P Sierra1, AD Da Silveira2, N Ghorayeb3, MFC Boaventura4, LCV Lemos3, CA Sierra3, MAPD Kiss5, R Stein2
1Nove de Julho University, Medicine Department, Sao Paulo, Brazil
2Federal University of Rio Grande do Sul, Exercise Cardiology Research Group, Porto Alegre, Brazil
3Institute Dante Pazzanese of Cardiology, Sao Paulo, Brazil
4Cruzeiro do Sul University, ICAFE, Sao Paulo, Brazil
5University of Sao Paulo (USP), School of Physical Education and Sport, Sao Paulo, Brazil
Introduction:The primary role of red blood cells is the transport of respiratory gases. If haemoglobin (Hb) decreases there is a reduction on exercise performance despite a compensatory increase in cardiac output.
Topic: Sports cardiology
Purpose:We analyze the relationship between "sports anaemia" and cardiorespiratory performance in amateur marathon runners.
Methods:74 male were evaluated twice by cardiopulmonary testing and spirometry, 3 weeks before and 3 to 15 days after the marathon. Hb, hematocrit, iron and bilirrubins were collected 24 hours before, immediately after, 24 and 72 hours after.
Results:Runners completed the marathon in 263.92 ± 36.93 minutes. The difference in Hb 24 and 72 hours after marathon was correlated with the difference in VO2 at the second ventilator threshold (VT2). Interestingly, the differences in VO2 in both thresholds were correlated with the changes in pulmonary capacity.
Conclusion:Marathon running induces a reduction in Hb, which is correlated with changes in ventilation. This compensation promoted by ventilation hinders the changes in cardiopulmonary capacity, although the decreased in the transport of respiratory gases seems to be a physiologic adaptation in the endurance athletes
Electrocardiographic adaptations to physical exercise: relation between military activity and competitive sport
H Dores1, R Fernandes1, S Ferreira1, A Silva1, MP Silva1, I Lopes1, MC Silveira1, E Rocha1, LB Carvalho1, J Monge1
1Hospital das For? Armadas, Cardiology, Lisbon, Portugal
Background:Military activity is characterized by intense physical exercise, and some military personnel are simultaneously competitive athletes. We aimed to analyze the electrocardiographic (ECG) findings of military personnel and the relation with involvement in competitive sport.
Methods and Results:Between May and November 2014, 1028 consecutive military were evaluated. According to the involvement in competitive sport, they were distributed into three groups: G1 – military activity only (n=678; 66%), G2 – past competitive sport (n=150; 14.6%) and G3 – present competitive sport (n=200; 19.5%). Among the baseline characteristics, black ethnicity was significantly more prevalent in G2 and male gender in G3. Individuals in the last group trained on average more 3 hours/week than G1 and G2. The ECG interpretation using the Seattle Criteria revealed: normal ECG – G1 34.1%, G2 28.7%, G3 16.5% (p<0.001); physiological findings – G1 61.8%, G2 63.3%, G3 76.0% (p=0.001); abnormal findings – G1 4.0%, G2 8.0%, G3 7.5% (p=0.039).
Conclusions:Although the frequent physical activity, the extension of ECG changes in military personnel is dependent of the involvement in competitive sport. These results reinforce the importance of the sports' history during military screening and ECG interpretation.
P871
Postural changes of QT interval in young elite athletes.
V Komoliatova1, L Makarov1, I Kisileva1, N Fedina1, D Besportochnii1
1Centre for Syncope & Cardiac Arrhythmias in Children & Adolescents of the Federal Medical-Biolo, Moscow, Russian Federation
Background:52% of LQTS carriers had a resting QTc in the normal or borderline range (R.W.Sy, 2012). Evaluation of the response of the QT interval to the brisk tachycardia induced by standing provides important information that aids in the diagnosis of LQTS. The changes of QT intervals immediately after standing in elite athletes haven't known. Aim of study was assessment of postural changes of QT interval in young elite athletes.
Methods:were examined 253 young elite athletes 14-18 (16.02±0.95) years old – members of national teams. Controls group was 125 healthy subjects (HS) 15.6±3.2 years old, not involved in sport. All of them were performed 12-lead in supine position and immediately after standing with measurement heart rate (HR), QT interval (manually) in V5 lead by method slope and calculated QTc interval using the Bazett's formula (QTc=QT/?154;RR). In standing position QT intervals were measured after 5-7sec after changes body position, when movement-related artifacts were disappeared. ?, ? and ?c were calculated as differences from HR, QTo and QTc in standing and supine position.
Results:All subjects have increasing HR immediately after standing, but there were significantly deference in this parameters between athletes and control groups (u=1511, z=2.19, p=0.02). HR immediately after standing was higher in HS, than in athletes (112±15 vs 85±14bpm, p<0.001), as QT interval (336±21 vs 392±32ms, p<0.01). We didn`t noted difference between QTc in standing position in athletes and nonathletes (460±32 vs 462±31, p>0,05) and ?c (57±33 vs 49± 38 ms, p>0.05). The maximum value of QTc in standing position in both groups didn`t exceed 500 ms and it lighting didn`t exceed 100 ms.
Conclusion:Elite athletes have a smaller increase in heart rate than those not involved in sports, and greater shortening of the QT interval immediately after standing. In elite athletes, as a subjects not involved in sports have the maximum value of QTc interval immediately after standing doesn't exceed 500ms and lighting of QTc interval doesn't exceed 100ms.
P872
Differentiating hypertrophic cardiomyopathy from physiological left ventricular hypertrophy: an echocardiographic and ECG approach
G Grazioli1, D Usin1, E Trucco1, M Sanz1, B Vidal1, S Montserrat1, J Gutierrez2, R Canal3, L Mont1, M Sitges1
1Barcelona Hospital Clinic, Barcelona, Spain
2Catalan Sports Council, Barcelona, Spain
3Futbol Club Barcelona, Barcelona, Spain
Background:Differential diagnosis of hypertrophic cardiomyopathy (HCM) from athlete's heart is challenging in mild-moderate left ventricular hypertrophy. The aim of the study was to assess ECG and echocardiographic parameters proposed for the differential diagnosis of HCM.
Methods:83 male subjects were included: control (n=40), athletes "grey zone" with IVS=13-15 mm (n=25), HCM with IVS 13-18 mm (n=18). The diagnosis of HCM was based on the results of comprehensive evaluation including familial evaluation, echocardiography and cardiac MRI. We performed an echocardiogram and an ECG. We calculated the Spatial QRS-T angle using the visual estimation of Kors' regression-related in all subjects.
Results:The baseline variables are shown in table 1. ROC curves were constructed to evaluate the diagnostic performance of HCM in each single criteria, the resulting area under curve (AUC) was: EDD (0.57), family history (0.61), TWI (0.68), Spatial QRS-T angle> 40 (0.76) and the ratio IVS/EDD > 0.27 (0.91). The Pearson's correlation between Spatial QRS-T angle > 40 and TWI was 0.67 (p 0.01). The combination of spatial QRS-T angle > 40 and IVS/EDD > 0.27 for diagnosis of HCM have an AUC was 0.76.
Conclusions:The best diagnostic criteria for HCM in echocardiography was the ratio IVS/EDD > 0.27 and in ECG was the spatial QRS-T angle > 40. No improvement in diagnostic accuracy by combining several parameters as spatial QRS-T angle and relation of IVS/EDD indexed.
TWI: T-wave inversion, LA: left atrial, EDD: left ventricle end diastolic diameter, IVS: inter ventricular septum
Control
Athlete grey zone
HCM
p- ANOVA
Age, years
32.1
25.5
34.6
0.17
LA, mm
32.7
38.0
42.5
0.001
EDD, mm
49.5
52.6
45.8
0.001
IVS, mm
9.50
13.20
16.11
0.001
IVS/EDD
0.19
0.25
0.51
0.001
Mass index
87.0
134.4
136.9
0.001
Spatial QRS-T angle
12.8
33.7
71.8
0.001
TWI, %
0
12
50
0.001
Family history, %
0
0
25
0.001
P873
Heart rate as an independent predictor of 3D derived strain components in top-level athletes: a real-time three-dimensional echocardiographic study.
F Lo Iudice1, V Schiano Lomoriello1, R Esposito1, C Santoro1, A Buonauro1, R Muscariello1, D De Palma1, B Trimarco1, M Galderisi1
1University Hospital Federico II, Naples, Italy
Topic: Sports cardiology
Purpose:To evaluate determinants of supernormal contractility of the athlete's heart using myocardial deformation parameters assessed by real-time 3-D echocardiography (RT3DE).
Methods:Twenty top-level competitive rowers (R) and 20 healthy young controls (C), matched for age (28 ± 6 and 28 ± 8 years respectively) underwent RT3DE quantification of left ventricular (LV) structure and function. Attention was paid to obtain a frame rate of at least 40% of the individual heart beating during the full volume recording. Accordingly, consecutive 4-beat ECG-gated subvolumes were acquired during apnea (multibeat acquisition) to generate the full-volume. LV end-diastolic volume (EDV), end-systolic volume (ESV) and ejection fraction (EF), sphericity index, LV mass index (LVMi), global longitudinal strain (GLS), global circumferential strain (GCS), global area strain (GAS) and global radial strain (GRS) were calculated off-line.
Results:The 2 groups were comparable for body mass index and diastolic blood pressure (BP) while systolic BP was higher (p<0.002) and heart rate (HR) lower (p<0.005) in R. LV EDV and ESV were greater in R (both p<0.0001) than in C, without significant difference of EF and sphericity index. LVMi was higher in R (75 ± 7 g/ m2) than in C (66 ± 7 g/ m2) (p<0.0001). GLS (-23.8 ± 3% in R and -21 ± 3% in C, p<0.005) and GAS (-36.7 ± 5% vs. -33.2 ± 4%, p<0.01) were higher in R than in C, while GCS and GRS did not differ significantly between the 2 groups. In the overall population HR was inversely related with LVMi (r = -0.49, p<0.0001) and both GLS (r = -0,43, p<0.005) and GAS (r = -0.34, p<0.01). After adjusting for body mass index, systolic BP and LVMi by separate multiple linear regression analyses, HR was an independent determinant of both GLS (standardized ?coefficient = -0.44, p=0.008) and of GAS (?= -0.37, p=0.03).
Conclusions:GLS and GAS are higher in top level athletes compared to normal healthy controls, despite a comparable LV ejection fraction between the two groups. Sinus bradycardia emerges as a major determinant of the supernormal myocardial deformation in the athlete's heart, independently from the increased LV mass.
P874
Training-induced atrial morphological and electrical remodeling: a prospective, longitudinal study in top-level athletes
F D'ascenzi1, M Solari1, M Biagi1, F Cassano1, M Focardi1, M Henein2, M Bonifazi3, S Mondillo1
1University of Siena, Department of Cardiovascular Diseases, Siena, Italy
2Umea University Hospital, Department of Cardiology, Umea, Sweden
3University of Siena, Department of Medicine, Surgery, and NeuroScience, Siena, Italy
Background:Biatrial enlargement is common in athletes and a further increase in biatrial size can occur in response to training. P-wave morphology seems to be unaffected by atrial size, however specific, longitudinal data are not available in top-athletes. Thus, the aim of this study was to investigate whether biatrial enlargement occurring in response to training is able to change the ECG pattern in athletes.
Methods:Fifty-five subjects were enrolled. Thirty-three professional, top-level athletes were evaluated at the beginning of the competitive season and after 6 months of training. Twenty-two sedentary subjects were used as controls. Athletes and controls were evaluated by ECG and both standard and 2D speckle tracking echocardiography.
Results:As expected, athletes had greater left atrial (LA) and right atrial (RA) size as compared with controls (p<.0001). After training, a further increase in LA and RA size was observed (p=.002 and p=.005, respectively). The increase in biatrial size was accompanied by an increase in both left and right ventricular size (p<.001 and p<.05, respectively). None of the participants fulfilled the criteria for RA enlargement. No significant differences existed between athletes and controls for criteria for LA enlargement, although 6% of athletes fulfilled these criteria. After training, despite an increase in LA size, the percentage of athletes fulfilling criteria for LA enlargement did not vary. Biatrial stiffness was normal both in athletes and in controls.
Conclusions:Despite a greater biatrial size as compared with controls and despite a further training-induced increase in biatrial dimensions, in top-level athletes ECG criteria for biatrial enlargement do not significantly vary with training. The finding of a normal biatrial stiffness suggests that, in absence of intra-atrial delay and in presence of a physiological global remodelling, no pathological findings can be detected at 12-lead ECG.
LA, left atrial; RA, right atrial.
Variable
Controls
Athletes
P value athletes vs. controls
P value pre- vs. post- training
Pre-training
Post-training
LA volume index, mL/m2
20.7 ± 4.7
27.1 ± 6.6
31.1 ± 8.2
.000
.000
RA volume index, mL/m2
17.3 ± 3.8
23.4 ± 6.3
26.4 ± 6.4
.000
.005
LA enlargement criteria
0%
6%
6%
.23
1.0
RA enlargement criteria
0%
0%
0%
1.0
1.0
P875
Cardiovascular disorders in paralympic athletes
M Bernardi1, MR Squeo1, F Quattrini2, A Vaquer2, E Lemme2, F Culasso1, A Spataro2, M S Link3, A Pelliccia2
1Sapienza, University of Rome, Department of Physiology and Pharmacologyl, Rome, Italy
2Institute of Sport Medicine and Science, CONI, Rome, Italy
3Tufts Medical Center, Medicine, CardioVascular Center, Cardiology , Boston, United States of America
Background:Exercise and sport participation programs for individuals with physical (motor and visual)impairments have exponentially grown, with an increasing number of them participating nowadays in competitive sport events, including Paralympic Games. Scarce scientific data, however, currently exist regarding the cardiovascular risk associated to competitive Paralympic sport.
Aim:To assess the type and prevalence of cardiovascular (CV) abnormalities, and the consequent possible risk for sport participation, in a large cohort of Paralympic athletes (PA).
Methods:267 PA (76%males), age 35±9 years, including 116 wheelchair bound PA (mostly with a spinal cord injury), 121 standing athletes with either amputation or poliomyelitis or other motor impairments and 30 PA with a visual impairment entered the study. PAcompeted in a spectrum of 18 Paralympic sport disciplines, and underwent a CV evaluation, prior to Paralympic Games, including history, PE, 12-lead resting and adapted maximal exercise test electrocardiography and echocardiography. Of this athletes'cohort, 105 PA participated in >2 consecutive Games, and had serial evaluations available over a 6±4 year follow-up period.
Results:Structural CV diseases were identified in 28 PA (11%), including dilated cardiomyopathy in 2 PA, hypertrophic cardiomyopathy in 1, isolated dilatation of aortic root in 3, valvular diseases in 8 (mitral valve prolapse in 5, bicuspid aortic valve in 3) and systemic hypertension in 14 (5%); finally, ventricular (polymorphic, couplets or NSVT) or supraventricular tachyarrhythmias (SVT, AF) were identified in 8 PA, in the absence of patents structural CV abnormalities. Over the follow-up, 6 athletes presented incidence of new diseases, including dilated cardiomyopathy in one and systemic hypertension in 5.
Conclusions:PA present an unexpected large prevalence of CV disorders, including cardiac conditions at risk, such as arrhythmogenic cardiomyopathies, dilated aortic root and primary ventricular tachyarrhythmias. This observation suggests that recommendations tailored to PA for pre-participation CV screening and safe sport participation are timely and appropriate