
Abstract
Background
Reduced telomere length is a measure of biological aging that is predictive of cardiac events in adults, and has been mechanistically implicated in the onset and progression of atherosclerosis. We sought to describe the early life factors associated with leukocyte telomere length in early childhood, and to determine whether telomere length measured during early childhood is associated with arterial wall thickening later in childhood.
Design
A longitudinal birth cohort recruited antenatally in Sydney from 1997 to 1999.
Methods
Leukocyte telomere length was measured in 331 children at age 3.6 years (SD 1.0); of whom 268 children without diabetes had carotid intima-media thickness assessed by ultrasound at age 8 years.
Results
Male sex, younger paternal age and higher maternal body mass index were associated with shorter telomere length in early childhood, which in turn was associated with greater carotid intima-media thickness at age 8 years (standardised β = −0.159, P = 0.01). There was a graded association across quartiles of telomere length (Ptrend = 0.001) with the highest odds of elevated intima-media thickness (>75th percentile) being in children with the shortest telomeres (odds ratio 4.00 (95% confidence interval 1.58 to 10.14) relative to those with the longest telomeres, P = 0.003). This association remained after adjustment for early life risk factors (Ptrend = 0.001).
Conclusions
Reduced telomere length in early childhood is independently associated with arterial wall thickness in later childhood, suggesting that reduced telomere length during early childhood may be a marker of vascular disease risk.
Keywords
Introduction
Reduced telomere length, a measure of biological aging that is predictive of cardiac morbidity and mortality in adults,1,2 has been proposed as a plausible mechanistic component of the onset and progression of early atherosclerosis. 3 Established risk factors for reduced telomere length include older age, male sex and younger paternal age. 4 However, early life predictors of telomere length have not previously been well described.
Carotid intima-media thickness (IMT) is an established non-invasive measure of subclinical atherosclerosis, which in adults is associated with the risk of incident cardiovascular events. 5 Carotid IMT is an age-appropriate measure of structural vascular health in children, being associated with putative early life risk factors, including poor fetal growth and excessive weight gain in infancy and established cardiovascular risk factors in childhood including obesity, low high-density lipoprotein (HDL)-cholesterol, type 1 diabetes and increased blood pressure. 6 Telomere length has previously been demonstrated to be associated with carotid IMT in adulthood. 7 However, it is contentious as to whether reduced telomere length is involved in the onset and progression of early atherosclerosis, or solely in more advanced atherosclerotic lesions. 8 We hypothesised that telomere length in early childhood would be an independent predictor of carotid IMT in later childhood.
Accordingly, we first sought to describe the factors associated with leukocyte telomere length in early childhood, and thence to determine whether telomere length measured at that time predicts arterial wall thickening later in childhood.
Methods
Participants
Participants (n = 616) were enrolled antenatally (between September 1997 and December 1999) into the Childhood Asthma Prevention Study (CAPS), a randomised trial of dietary omega-3 supplementation and/or avoidance of house dust mite exposure during the first 5 years in children considered ‘at risk’ of developing atopy and/or asthma. 9 Participants had at least one parent or sibling with symptoms of asthma; exclusion criteria included infants from a multiple pregnancy, and those born before 36 weeks’ gestation. Participants were studied as part of the trial at birth, 18 months (n = 554), 3 years (n = 526) and 5 years of age (n = 516), and subsequently at age 8 years (n = 450) as part of an ongoing longitudinal birth cohort comprising the original trial participants.
Consent was obtained for leukocyte genomic DNA collection either at 18 months, 3 years or 5 years of age, with sufficient DNA extracted and leukocyte telomere length analysed in 331 participants. These participants were included in an analysis of early life predictors of telomere length in early childhood. Of the 450 participants who attended the 8-year study visit, consent was obtained for vascular testing in 405 children without diabetes, 268 of whom also had data for telomere length from early childhood.
Established cardiovascular risk factors, including systolic blood pressure, HDL-cholesterol, non-HDL-cholesterol and C-reactive protein, were assessed using standardised methods at the 8-year study visit (see Supplemental Methods).
This study complies with the Declaration of Helsinki. The human research ethics committees of the University of Sydney, the Children’s Hospital at Westmead and Sydney South West Area Health Service have approved the research protocol, and informed consent was obtained from a parent or legal guardian of all participating children.
Leukocyte telomere length
Leukocyte genomic DNA was extracted from peripheral venous blood samples using a salting-out method, 10 and quantified by UV-Vis Spectrophotometry (NanoDrop 2000, NanoDrop Technologies, USA).
The mean leukocyte telomere length in genomic DNA samples was measured using multiplex quantitative real-time polymerase chain reaction (qPCR). 11 Briefly, two series of quadruplicate qPCR reactions were performed for each standard and sample in a total volume of 15 μl, in clear 96-well plates on a CFX96 real-time PCR detection system (Bio-Rad Laboratories, USA). Five serial dilutions of a reference sample (leukocyte DNA from an adult woman) spanning 75–1.92 ng (2.5 × serial dilution) were run on each plate. For each sample, the following were determined: the amount of reference DNA that matched the experimental sample for copy number of the telomere template (T); and the amount of reference DNA that matched the experimental sample for copy number of the albumin template (S). The telomere to single copy gene (T/S) ratio was then calculated, corresponding to the relative telomere length of DNA. 11 The results of all four replicates were averaged, and the average calculated for each sample from the two series of qPCR.
The median intra-assay coefficient of variation was 5.3%. The inter-assay repeatability coefficient was 1.02 units, 12 and the median inter-assay coefficient of variation was 9.9% (see Supplemental Figure 1).
Parental characteristics and early life exposures
Standardised questionnaires were used to assess parental age, education and maternal smoking status during pregnancy approximately 4 weeks prior to delivery, breastfeeding status 6 months after birth and evidence of asthma and atopy at each study visit. Maternal and paternal height and weight were measured at the 8-year visit; if only one parent attended the study visit, a standardised protocol was provided to assist home assessment of the non-attending parent.
Birth weight and length were recorded from hospital records. At subsequent study visits, weight was measured to the nearest 0.1 kg using calibrated electronic scales and height to the nearest 0.5 cm using a stadiometer. Disproportionate weight gain during infancy was defined as the residual of weight gain from birth to 18 months on the change in height over the same period derived from sex-stratified linear regression, and as such is a measure of weight gain in kilograms above or below the weight gain predicted from stature growth. 13 The body mass index (BMI) z-score at the time of DNA sample collection was calculated based on US growth charts. 14
Carotid IMT
Common carotid artery IMT was assessed 0–1 cm proximal to the carotid bulb by high resolution ultrasound at the 8-year study visit (see Supplemental Figure 2). 15 Briefly, right and left carotid arteries were scanned by a single sonographer following a standardised protocol. Loops were captured for blinded offline analysis by a single experienced observer. Carotid IMT was assessed along a ∼1 cm long region of the far wall of the artery, proximal to the carotid bulb. The maximum carotid IMT, the thickest point from either the right or left carotid, was used for analysis, given evidence of greater relevance to cardiovascular risk, 5 the focal nature of early lesions, 16 and stronger associations with risk factors in children. 13
Measurement of carotid IMT was repeated by the single experienced observer for 50 randomly selected participants; the intra-observer repeatability coefficient was 41 µm, 12 and the intra-observer coefficient of variation was 1.4% (see Supplemental Figure 3).
Statistical analysis
Compared with those participants who were not included in the current analysis, the children reported here had older parents and there was some evidence that they gained more weight during infancy (see Supplemental Table 1).
Associations with early childhood telomere length and carotid IMT at age 8 years were determined by multivariable linear and logistic regression. All multivariable models were adjusted for sex, age at DNA collection, randomised study group and parental education. Multivariable models with carotid IMT as the outcome were additionally adjusted for age at carotid IMT assessment. An early life risk factor model was further adjusted for birth weight, gestational age, disproportionate weight gain during infancy, asthma and atopy. Quartiles of age-adjusted telomere length were derived using the residuals method. To assess the linear trend, telomere quartiles were numbered from lowest to highest, and analysed as a continuous variable. Elevated carotid IMT was defined as maximum carotid IMT greater than the 75th percentile. No sex-related differences were present (data not shown). The distribution of telomere length was skewed and hence was transformed (Ln[telomere length]/Ln[2]) for parametric analysis. Non-linear associations were examined using centered quadratic variables.
Statistical analysis was undertaken using IBM SPSS Statistics (version 21.0; IBM Corp., USA), and statistical significance inferred at a two-sided P value < 0.05.
Results
Participant characteristics (n = 331).
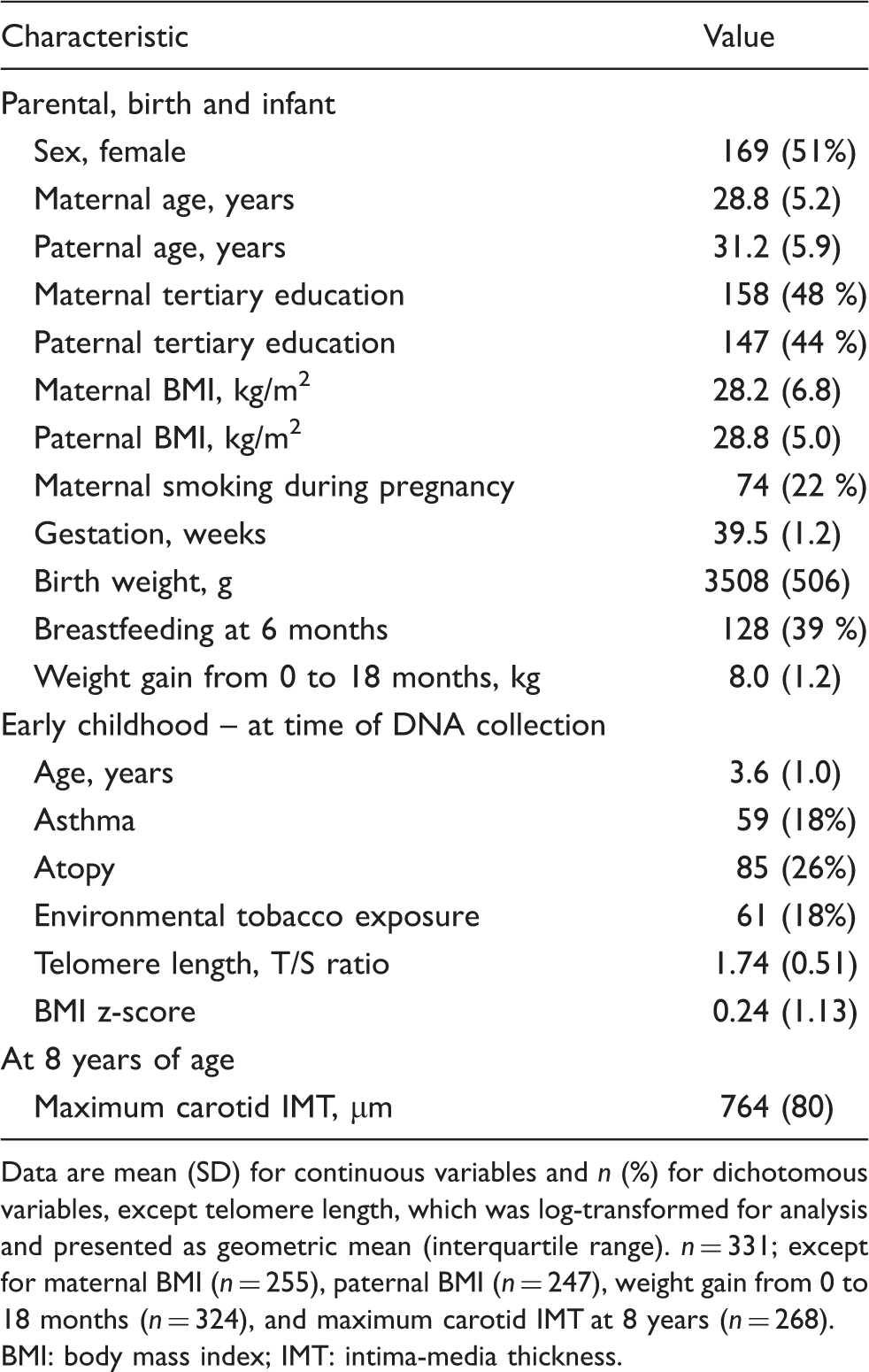
Data are mean (SD) for continuous variables and n (%) for dichotomous variables, except telomere length, which was log-transformed for analysis and presented as geometric mean (interquartile range).
n = 331; except for maternal BMI (n = 255), paternal BMI (n = 247), weight gain from 0 to 18 months (n = 324), and maximum carotid IMT at 8 years (n = 268).
BMI: body mass index; IMT: intima-media thickness.
Predictors of leukocyte telomere length during early childhood
Associations with telomere length during early childhood – minimally adjusted models.
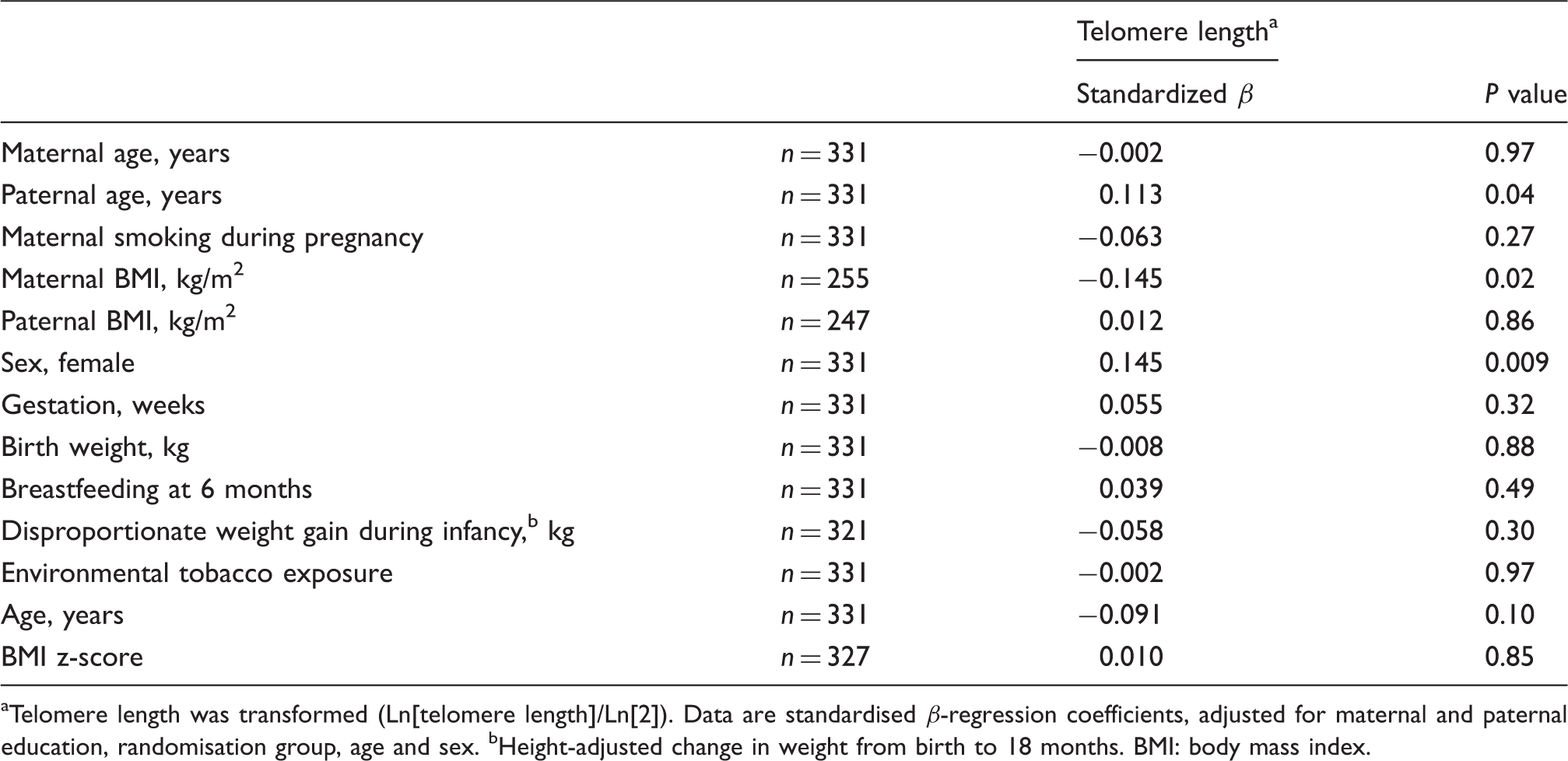
Telomere length was transformed (Ln[telomere length]/Ln[2]). Data are standardised β-regression coefficients, adjusted for maternal and paternal education, randomisation group, age and sex. bHeight-adjusted change in weight from birth to 18 months.
BMI: body mass index.
Leukocyte telomere length during early childhood and carotid IMT during later childhood
Shorter telomere length during early childhood was associated with greater carotid IMT at age 8 years, independent of early life risk factors (birth weight, gestational age, disproportionate weight gain during infancy, asthma and atopy, see Supplemental Table 3 and Supplemental Figure 5). Adjustment for established cardiovascular risk factors and evidence of atopy and/or atopy at age 8 years (systolic blood pressure, HDL-cholesterol, non-HDL-cholesterol, and C-reactive protein) did not modify the association (−31 µm (95% confidence interval (CI) −61 to −2) per doubling of telomere length, P = 0.04). The association was similar after excluding those participants randomly assigned to the omega-3 supplementation group (−18 µm (95% CI −53 to 16) per doubling of telomere length), or those who had developed asthma and/or atopy at the time of IMT analysis (−18 µm (95% CI −52 to 16) per doubling of telomere length).
There was a graded association with elevated IMT across quartiles of leukocyte telomere length, translating to a four times increased odds of elevated IMT in those with the shortest telomeres, compared to those with the longest telomeres (P = 0.003; see Figure 1). Adjustment for early life risk factors did not markedly affect this association (Ptrend = 0.001 across quartiles of telomere length).
Leukocyte telomere length in early childhood and elevated IMT at age 8 years. Data presented as odds ratios (95% CI) for elevated IMT (carotid IMT > 75th percentile). P value is Ptrend across age-adjusted telomere length quartiles. Adjusted for age at carotid IMT assessment, age of DNA collection, sex, study randomisation, maternal and paternal education. IMT: intima-media thickness; CI: confidence interval.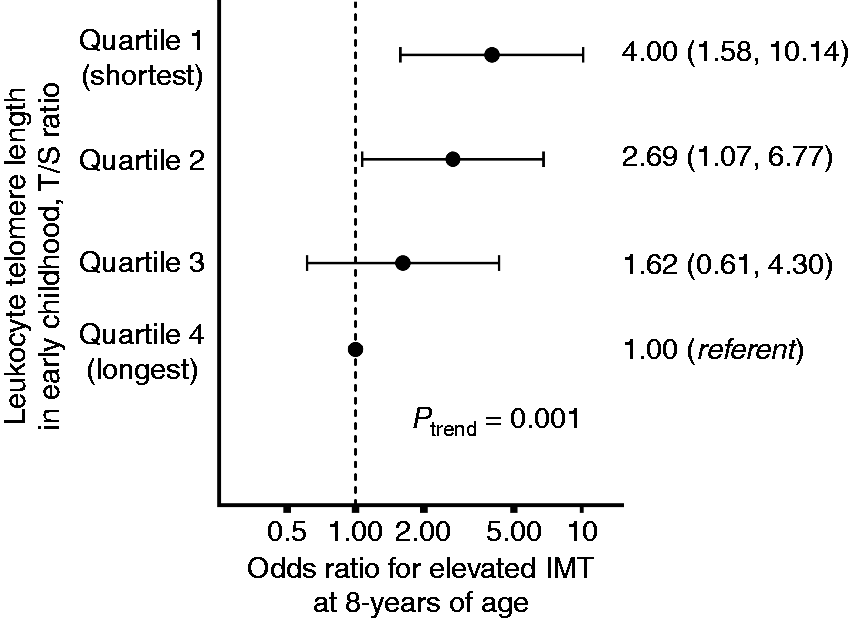
Discussion
In this study, we demonstrate that shorter telomere length in early childhood is a predictor of higher carotid IMT in later childhood, such that those with the shortest telomeres (lowest quartile) were substantially more likely to have elevated IMT (highest quartile) later in childhood. The effect size was such that carotid IMT was on average 30 microns higher in children with the shortest telomeres in early childhood than in those with the longest telomeres; an effect size similar to that previously described for type 1 diabetes in children of a similar age. 17
The association of shorter telomere length in early childhood with thicker carotid walls in later childhood suggests that reduced telomere length may be a biological mechanism affecting the onset and progression of the initial stages of atherosclerosis, or that they have a shared aetiology. 18 Putative mechanistic links may involve the senescence of vascular smooth muscle cells due to oxidative DNA damage and inflammatory pathways. 19
A number of studies have described the association of reduced leukocyte telomere length with increased cardiovascular events. A recent meta-analysis demonstrated that adults in the shortest third of telomere length have a 30–83% higher risk of coronary heart disease than those in the longest third. 20 While there is controversy regarding reverse causation,1,2,20 a recent study utilising Mendelian randomisation techniques calculated that a 1 SD increase in leukocyte telomere length due to a genetic risk score derived from seven leukocyte telomere length associated single-nucleotide polymorphisms, was associated with a 5–35% lower risk of coronary artery disease. 21 In combination with our observed association of reduced telomere length with an established biomarker of subclinical atherosclerosis in early childhood, these findings argue against reverse causation.
We assessed telomere length using qPCR, which correlates closely with the length of terminal restriction fragments by southern blot. 11 Other aspects of telomere biology, such as telomerase and telomerase reverse transcriptase, are associated with improved cardiac structure and function in experimental models 22 and coronary calcium in humans. 23 We did not assess these other aspects of telomere biology, and as such cannot ascertain whether they have similar effects on arterial wall thickness in childhood.
Established risk factors for reduced telomere length in adults and older children include male sex, adiposity, aging and younger paternal age.4,24,25 Here we demonstrate that risk factors for shorter telomere length in early childhood include younger paternal age, higher maternal adiposity and male sex, with weaker evidence for older age. Gestational age was not associated with leukocyte telomere length, although our study only included participants born at term. Preterm birth is associated with increased blood pressure and atherosclerotic vascular disease;26,27 future studies may determine whether telomere length is altered in children born preterm.
This population previously participated in a randomised trial on the basis of being at increased risk of developing asthma, although their cardiovascular risk profile is similar to a community-based cohort of similar age from the same geographical region.15,28 We have previously shown that asthma is not associated with altered carotid IMT at 8 years of age in this study, 15 consistent with other findings in young children. 29 Nonetheless, our results were independent of asthma status and were similar in the non-asthmatic participants. Future studies may confirm whether similar associations are observed in the general population.
Strengths of the current study include the longitudinal design and antenatal recruitment, allowing standardised assessment of birth characteristics and early indices of growth. Weaknesses include the lack of arterial IMT and cardiovascular risk assessment at the time of telomere sampling, although carotid IMT is not commonly used as a marker in children under 5 years of age, 30 and the relatively low percentage (45%) of the initial study participants with complete data for both leukocyte telomere length in early childhood and carotid IMT at 8 years of age. However, the largest number lost to follow-up occurred in the first 18 months; only 19% of participants from whom DNA was collected did not have carotid IMT assessed, on average 5 years later. As the birth and parental characteristics did not markedly differ from those not included in the current analysis, we believe that this is unlikely to have significantly biased the findings. While we observed statistically significant associations, participant numbers were relatively low, particularly given that telomere length has greater variability in childhood. 31 The variability of the telomere length assay was within the published range for laboratories with considerable expertise in this measure. 32 Treatments in early life may partly contribute to the observed association, although we believe this is unlikely to be a major contributor given that similar results were observed in stratified analysis excluding all participants with asthma and/or atopy. Furthermore, despite the longitudinal study design, causality cannot be ascertained, with the observed association potentially relating to the cumulative burden of putative risk factors for both shorter telomeres and increased carotid IMT, such as aspects of early childhood nutrition or passive smoke exposure.
In conclusion, reduced telomere length in early childhood is independently associated with greater arterial wall thickness in later childhood. This suggests that shorter telomeres during early childhood may be a biological marker of vascular disease risk. Future studies may determine the causality of such an association, and whether assessment of telomere length in early life may be useful in identifying individuals at risk of later cardiovascular events.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MRS contributed to the development of educational resources for AstraZeneca, relating to the clinical management of type 2 diabetes. GBM serves on an advisory board to Novartis, and has received grant funding from AstraZeneca and GlaxoSmithKline. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cooperative Research Centre for Asthma, Department of Health, Children’s Hospital at Westmead, and the National Health and Medical Research Council of Australia Project and Program Grants (grant numbers 222722 and 482800), contributions of goods (oil supplements) were made by Nu-Mega Ingredients Pty Ltd, Australia, goods (margarines and cooking oils) were provided at reduced cost by Goodman Fielder Foods, Australia, a fellowship from the National Health and Medical Research Council of Australia (no. 1004474 to MRS).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.