
Abstract
Background
Autonomic control of the cardiovascular system may be impaired in type 2 diabetes and is associated with increased morbidity and mortality. Parameters obtained during stress testing may reflect early stages of cardiac autonomic dysfunction and provide prognostic information in asymptomatic type 2 diabetes.
Methods
We performed maximal exercise treadmill testing in 594 patients with type 2 diabetes without known coronary heart disease. The prognostic significance of physiological parameters associated with autonomic dysfunction was assessed, including chronotropic incompetence (<80% heart rate reserve), abnormal heart rate recovery at 1 minute <18 beats/minute, and resting tachycardia >100 beats/minute. Cox proportional hazards analysis was used to determine the association of exercise parameters with a composite outcome of all-cause mortality, myocardial infarction or stroke.
Results
Resting heart rate >100 beats/minute was observed in 18% of patients, chronotropic incompetence in 30% and heart rate recovery at 1 minute <18 beats/minute in 35%. Over 79 ± 16 months, there were 72 (12%) events. Each parameter was significantly associated with event risk in an adjusted multivariate analysis: chronotropic incompetence (hazard ratio 1.89, 95% confidence interval 1.18–3.01; P = 0.008), resting heart rate ≥100 beats/minute (hazard ratio 1.97, 95% confidence interval 1.19–3.26; P = 0.008) and heart rate recovery at 1 minute <18 beats (hazard ratio 1.77, 95% confidence interval 1.12–2.81; P = 0.015). A progressive relationship between the number of abnormal parameters and event risk was observed (log rank P < 0.001).
Conclusions
Chronotropic incompetence, resting tachycardia and reduced heart rate recovery are independently and additively associated with long-term mortality, myocardial infarction or stroke in type 2 diabetes without known coronary heart disease.
Introduction
Diabetes mellitus is a major risk factor for both micro and macrovascular disease. 1 Cardiac autonomic neuropathy, a common complication of diabetes that is often overlooked, is associated with significant cardiovascular morbidity and mortality. 2 During its subclinical phase and early clinical stage, reduction in parasympathetic activity and sympathetic predominance may manifest by impaired heart rate (HR) variability, resting tachycardia and later, reduced exercise tolerance. 3 Non-invasive tests based on HR and blood pressure response to several physiological manoeuvres can be used to assess cardiac autonomic function. These tests, known as cardiac autonomic reflex testing (CART), include HR response to deep breathing, standing and valsalva, as well as blood pressure response to standing and sustained handgrip. 4 Although these tests are recommended for bedside screening of diabetes patients and are non-invasive, they require assessment of beat to beat HR variation, and in clinical practice are not broadly applied.
Exercise treadmill testing has served for decades as a useful test for screening asymptomatic individuals with type 2 diabetes for coronary artery disease. Its clinical utility is ongoing, despite the availability of advanced cardiac imaging modalities with better diagnostic capabilities. It additionally provides significant prognostic value in both the general population and in diabetes. 5 This prognostic utility is beyond that obtained from ST-segment analysis and the presence of angina. Exercise capacity and measures of cardiorespiratory fitness such as maximal metabolic equivalents (METs) and duration of exercise are well established independent predictors of cardiovascular morbidity and mortality in type 2 diabetes.6–9 Nevertheless, other non-ST segment parameters obtained during exercise testing are also associated with adverse prognosis in diabetes patients. 10 Among these predictors are HR-related markers reflecting cardiac autonomic nervous system dysfunction, including chronotropic incompetence, reduced heart rate recovery (HRR) and increased HR at rest.11–20
In the current study we aimed to investigate whether HR-related parameters that may reflect cardiac autonomic neuropathy are associated, both independently and additively, with myocardial infarction (MI), stroke or all-cause mortality, in asymptomatic subjects with type 2 diabetes without known coronary artery disease.
Methods
Study population
The study is part of an ongoing prospective study of cardiovascular outcomes in asymptomatic subjects with type 2 diabetes, enrolled between July 2006 and October 2008, who underwent cardiac computed tomographic angiography at study entry to examine coronary artery atheroma.21–23
That study is registered at ClinicalTrials.gov as NCT00321542. The current study included 594 patients of the parent study, in whom treadmill exercise testing was also performed at study entry.
Consecutive patients attending two regional diabetes clinics were screened for compliance with the study protocol, and family practitioners informed of the study protocol screened patients with type 2 diabetes for study participation. Patients providing informed consent to study procedures were enrolled. The index date for patient follow-up was the date of consent. Patients were included in the study if they fulfilled the following criteria: age 55–75 years, no history or symptoms of coronary artery disease or electrocardiographic signs of previous MI, and at least one of the following risk factors for a cardiovascular event: age greater than 60 years, history of hypertension, current smoking, family history of premature coronary artery disease in a first degree relative less than 55 years of age, cerebral, carotid or peripheral arterial disease, diabetic retinopathy or neuropathy or albuminuria (>30 mg/day) or duration of diabetes of at least 5 years from time of first diagnosis. Exclusion criteria were serum creatinine greater than 1.4 mg% (as computed tomographic angiography was part of the parent study protocol), chronic atrial fibrillation and inability to perform a treadmill exercise stress test.
The primary outcome was a composite of all-cause mortality, MI or stroke. Events were ascertained to July 2014 in all subjects, by phone calls and by reviewing patients’ electronic files and computerised records of health maintenance organisations. All events were adjudicated according to predefined diagnostic criteria, by an independent outcomes committee provided with patient hospital discharge reports, electrocardiograms and laboratory results from all hospitalised patients. The study protocol was approved by the Lady Davis Carmel Medical Center (Haifa, Israel) institutional review board. Study participants provided written informed consent.
Measurement of exercise testing parameters
All patients included in the current substudy performed at study entry a maximal graded treadmill stress test using a Bruce protocol. Exercise capacity was quantified as peak METs achieved. The software program of the treadmill (Marquette 2000; General Electric, Milwaukee, Wisconsin, USA) calculates METs based on the formula: METs = [(speed × 26.8 × 0.1) + (grade/100 × 1.8 × speed × 26.8) + 3.5]/3.5. Speed is entered as miles per hour, and grade as the percentage of the treadmill incline. Exercise termination was conducted in a standard fashion by rapid reduction in treadmill rate and incline followed by 10–20 seconds walking on the level before full stop. In the absence of an extended active cool-down period, HRR one minute after peak exercise (HRR1) less than 18 beats per minute (bpm) was defined abnormal. 24
Resting HR was recorded during the measurement of vital signs at rest, preceding the exercise testing. Predicted maximal HR was calculated as 220 – age. HR reserve was calculated as predicted maximal HR minus resting HR. The proportion of HR reserve used was then calculated as [(peak HR achieved minus resting HR)/HR reserve] × 100. Chronotropic incompetence was present if the latter was less than 80%.
Data analysis
Clinical characteristics, medications, blood tests results and exercise testing parameters are presented according to the occurrence of the composite event during follow-up. Continuous data are presented as means ± standard deviation or median and interquartile range (IQR), and categorical variables as numbers and percentages. The independent-samples t test was used to compare continuous variables or the Mann–Whitney test for skewed data, and the χ2 test was used to compare categorical variables. Fisher’s exact test was used in cases of small sample sizes.
To assess the effect of each of the exercise test parameters at baseline evaluation on the risk of all-cause mortality, MI or stroke, a Cox proportional hazards regression analysis was performed. Hazard ratios for the outcome event were calculated with 95% confidence intervals (CIs). Adjustment was made for age and sex, and in a separate model further adjustment was made for hypertension, body mass index, smoking status, total cholesterol, high-density lipoprotein and low-density lipoprotein cholesterol, glycated haemoglobin levels, hypertension drug therapy, statins, metformin and insulin therapy, duration of diabetes and the presence of microvascular disease.
Survival curves were plotted according to the number of tests for autonomic dysfunction with abnormal findings by the Kaplan–Meier method using the log-rank test for comparison between variables. The results were considered statistically significant when the two-sided P value was less than 0.05. SPSS statistical software version 20.0 was used to perform all statistical analyses.
Results
Study cohort
The study population included 594 type 2 diabetes patients who were asymptomatic, without known coronary artery disease. The mean age of the study participants was 63 ± 5 years (range 55–75) and 53% were women. Microvascular dysfunction was noted at baseline in 244 (41%) patients. The median duration of diabetes was 8 years (IQR 4–14), and 23% were treated by insulin therapy at study entry.
Baseline characteristics of study patients.
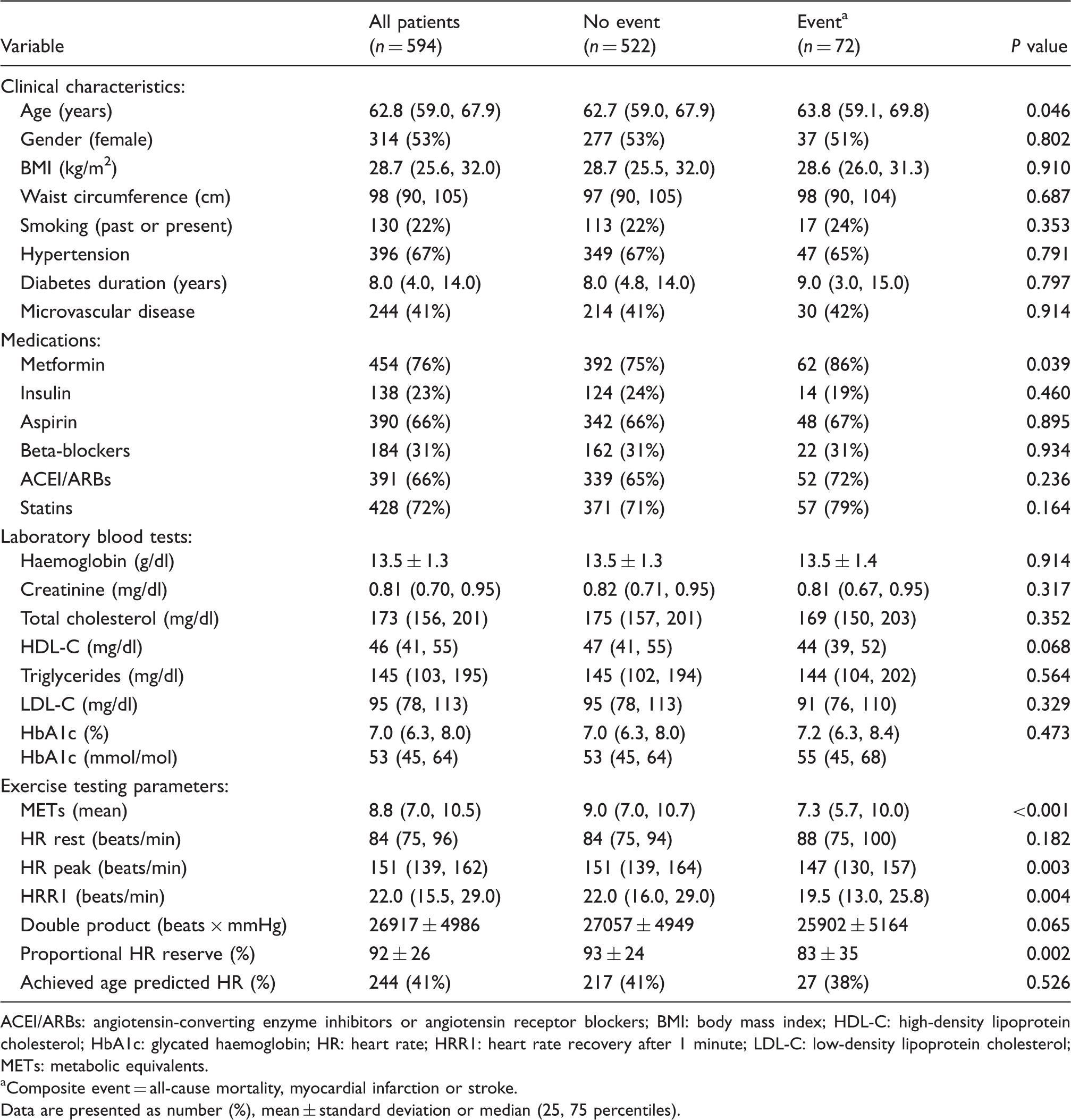
ACEI/ARBs: angiotensin-converting enzyme inhibitors or angiotensin receptor blockers; BMI: body mass index; HDL-C: high-density lipoprotein cholesterol; HbA1c: glycated haemoglobin; HR: heart rate; HRR1: heart rate recovery after 1 minute; LDL-C: low-density lipoprotein cholesterol; METs: metabolic equivalents.
Composite event = all-cause mortality, myocardial infarction or stroke.
Data are presented as number (%), mean ± standard deviation or median (25, 75 percentiles).
Prognostic value of exercise testing parameters
Variables associated with exercise treadmill testing are presented in Table 1. The exercise capacity estimated by METs, as well as peak HR achieved, HRR1 and proportional HR reserve were significantly lower in the event group. The double product also tended to be reduced. HR at rest was higher in the event group (median 88 bpm (IQR 75, 100) versus 84 bpm (IQR 75, 94)), but did not reach statistical significance.
Resting HR of 100 bpm or greater was evident in 18% of the study population, chronotropic incompetence (proportional HR reserve <80%) in 30% and HRR less than 18 bpm in 35% of the patients. There was no overlap between these three abnormal HR-related parameters in 40% of the attenuated HRR1 cases, 48% of the resting tachycardia cases and 53% of the chronotropic incompetence cases.
The occurrence of each of these abnormal HR-related parameters associated with cardiac autonomic dysfunction was significantly higher in the event compared to the non-event group (Figure 1).
Absolute rates of the composite eventa during follow-up, according to the presence/absence of each of the HR-related parameters.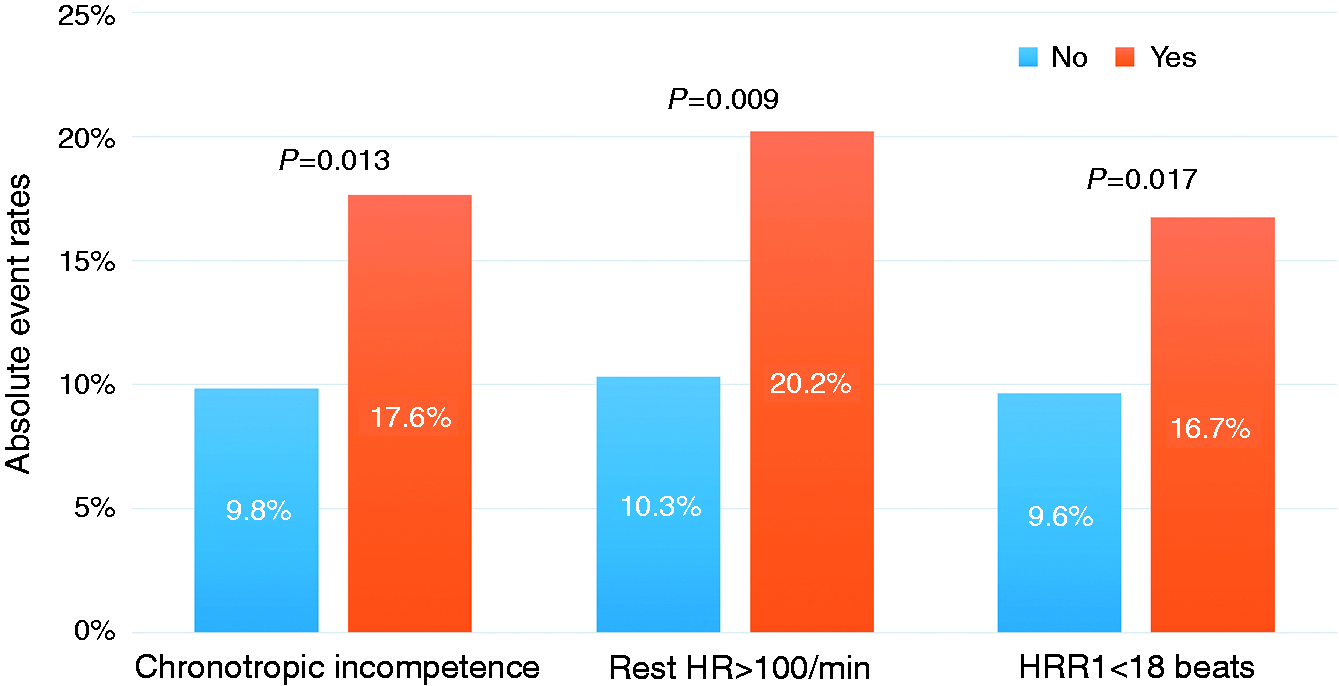
Hazard ratios for the composite event, a according to abnormal exercise treadmill testing parameters.
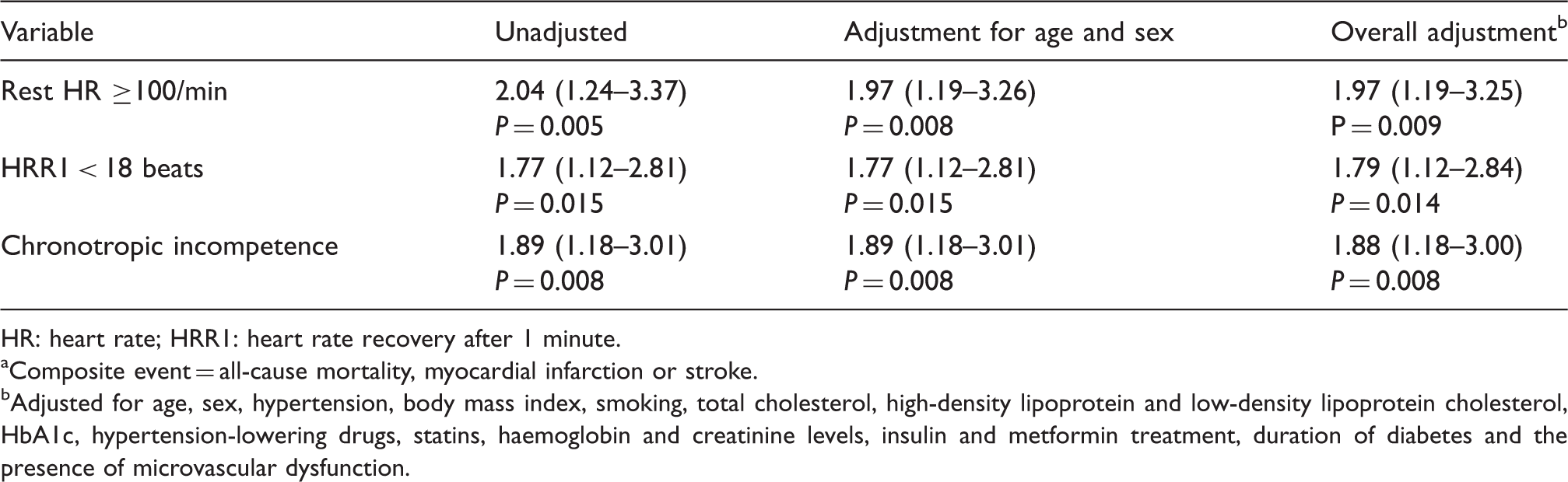
HR: heart rate; HRR1: heart rate recovery after 1 minute.
Composite event = all-cause mortality, myocardial infarction or stroke.
Adjusted for age, sex, hypertension, body mass index, smoking, total cholesterol, high-density lipoprotein and low-density lipoprotein cholesterol, HbA1c, hypertension-lowering drugs, statins, haemoglobin and creatinine levels, insulin and metformin treatment, duration of diabetes and the presence of microvascular dysfunction.
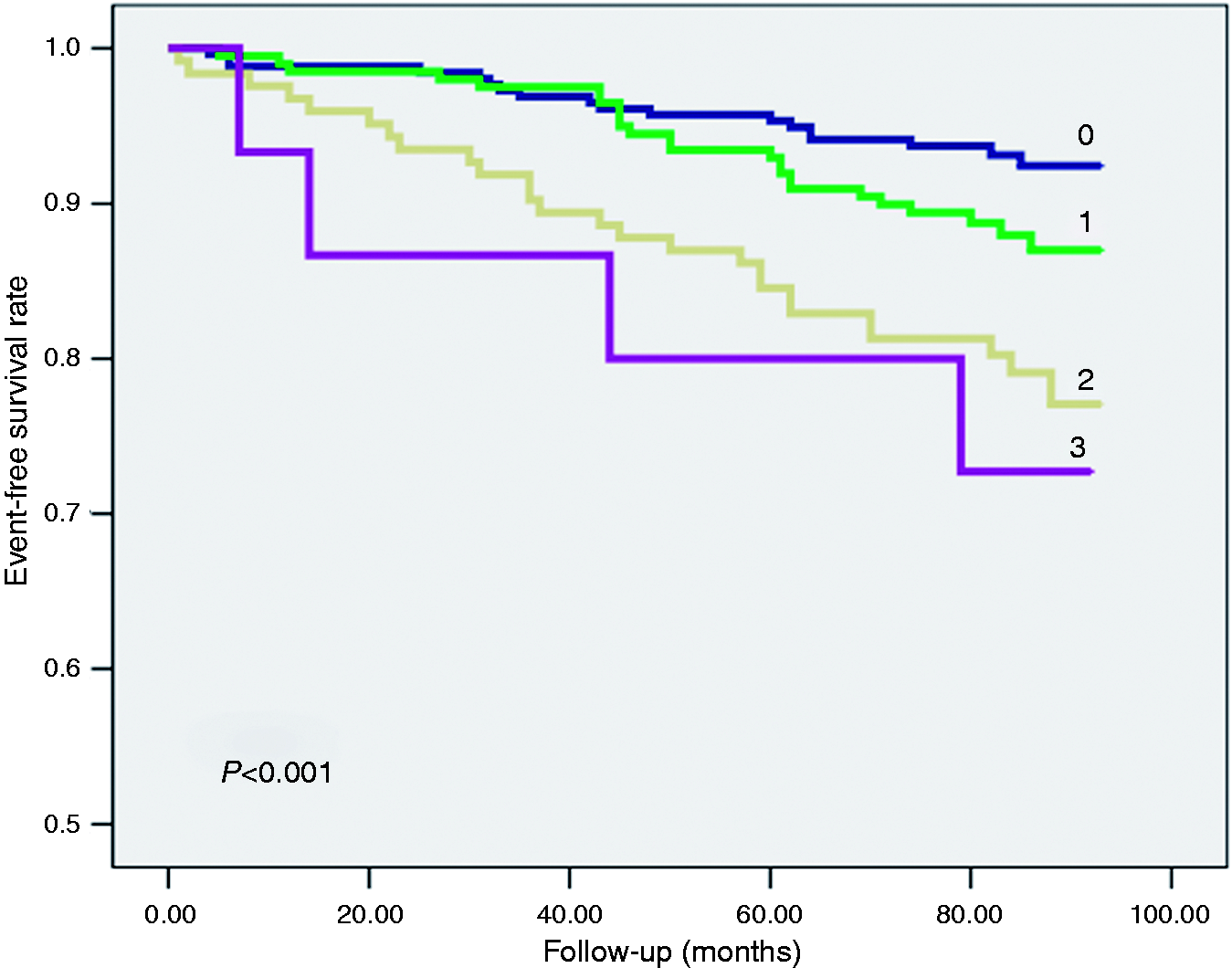
None of the abnormal HR-related parameters (HRR1 < 18 bpm, resting HR ≥ 100 bpm or chronotropic incompetence) was found in 256 patients (43.1%). One abnormal parameter was present in 200 patients (33.7%), two abnormal parameters in 123 (20.7%) patients, and only 15 patients (2.5%) had all three abnormal parameters. A progressive relationship between the number of abnormal parameters and outcome events was observed, from 7% absolute events in patients without any abnormal parameters to 27% in patients with all three abnormal parameters (Figure 2). The corresponding Kaplan–Meier event-free survival curves are presented in Figure 3; log-rank P < 0.001 for overall comparison. Compared to patients without any of the abnormal variables, the adjusted hazard ratio of diabetes patients with more than one abnormal HR-related parameter was 3.31 (95% CI 1.85–5.94; P < 0.001). Further adjustment for estimated METs achieved did not abolish the significance of the association with event risk (hazard ratio 2.10, 95% CI 1.10–4.01, P = 0.02).
Absolute eventa rates during follow-up, according to the number of abnormal HR-related parameters (0–3). Parameters include: (a) HRR1 <18 beats; (b) chronotropic incompetence; (c) rest HR >100/min. Event-free survival, according to the number of abnormal HR-related parameters (0–3). Adjusteda hazard ratios (95% CI) for event: no abnormal parameters = reference; one abnormal parameter: 1.73 (0.94–3.19), P = 0.07; two abnormal parameters: 3.14 (1.72–5.72), P = 0.001; three abnormal parameters: 4.11 (1.39–12.14), P = 0.011. Parameters include: (a) HRR1 < 18 beats; (b) chronotropic incompetence; (c) rest HR > 100/min.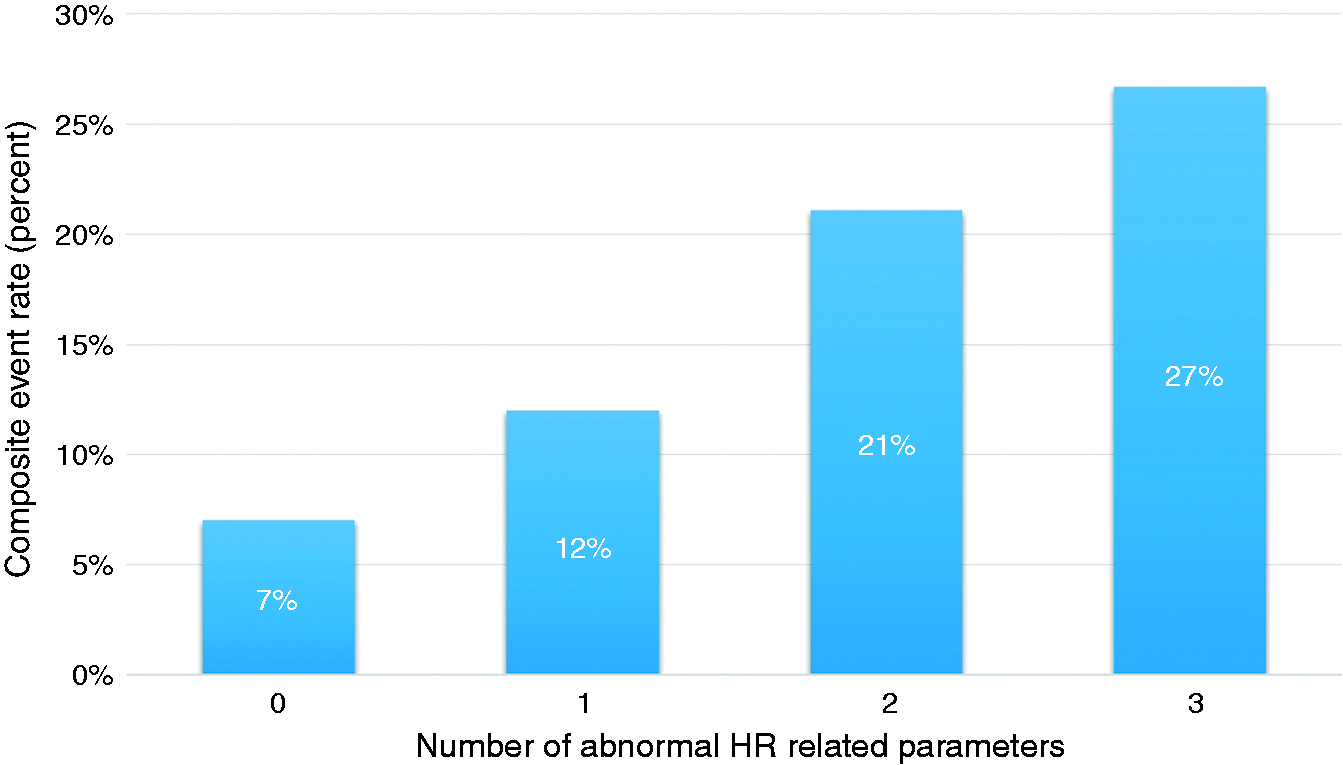
Discussion
The current study examined the prognostic utility of HR-related parameters that are associated with cardiac autonomic dysfunction and are easily measured in a clinical exercise laboratory. Resting tachycardia above 100 bpm, chronotropic incompetence and HRR of less than 18 heart beats during the first minute after achieving peak HR were each significantly and independently associated with all-cause mortality, MI or stroke in subjects with type 2 diabetes who were asymptomatic and without known coronary heart disease at study entry. The predictive value was progressive, with each abnormal parameter additively impacting long-term prognosis.
Cardiac autonomic neuropathy, in the setting of diabetes, is defined as the impairment of autonomic control of the cardiovascular system after the exclusion of other causes. 25 Its prevalence varies, increasing with age, glycaemic control and diabetes duration. Screening for cardiac autonomic dysfunction is recommended in asymptomatic type 2 diabetes, and clinical diagnosis is established on at least two abnormal CART tests, which are based on HR and blood pressure response to several manoeuvres. 25 Although CART-based diagnosis is recommended for screening patients with diabetes and can be performed at the bedside, it is not broadly applied in clinical practice. Considering the significant cardiovascular morbidity and mortality associated with the disease, additional tools that are simple to perform and commonly applied in diabetes are required for diagnostic and prognostic utility. Exercise treadmill testing is commonly performed in type 2 diabetes, and may serve as an appropriate modality for these objectives. Reduced HRR, chronotropic incompetence and resting tachycardia are early signs associated with cardiac autonomic dysfunction, which can be easily measured during routine exercise treadmill testing. Each of these HR-related parameters was reported in the literature to be associated with prognosis in type 2 diabetes.
The inability of the HR to rise in proportion to an increase in activity or metabolic demand is often clinically ignored, although it is not uncommon in patients with type 2 diabetes. This chronotropic incompetence is thought to derive from predominant activation of sympathetic nerves, which leads to downregulation of beta-adrenergic receptors in the sinus node, ultimately resulting in post-synaptic desensitisation and disturbed HR response during exercise. 26 The aetiology is probably complex, but involves impaired baroreflex sensitivity and cardiovascular autonomic neuropathy. Chronotropic incompetence is suggested to be significantly more prevalent in type 2 diabetes than in healthy individuals. 27 Similar to our cohort, among 1341 patients with diabetes mellitus referred for exercise testing, 36% had an impaired chronotropic response. 11 These individuals were at increased risk of total mortality, MI and coronary revascularisation, with an adjusted hazard ratio of 1.53 in a multivariate model. An additional study reported that chronotropically incompetent subjects with diabetes also have a higher frequency of cerebrovascular disease, comparable to the present study results. 12
The period of recovery after exercise is influenced by a combination of sympathetic withdrawal and parasympathetic reactivation. Data suggest that early HRR after exercise is predominantly due to parasympathetic reactivation, with sympathetic and non-autonomic components probably playing lesser roles. 28 A blunted HRR response derived from a standard exercise test was shown to provide high diagnostic accuracy for cardiac autonomic neuropathy in type 2 diabetes, as defined by cardiac reflex testing and HR variability. 29 In addition, hyperglycaemia was demonstrated to be strongly and independently associated with abnormal HRR.30,31 In accordance with our observation, several studies in populations with diabetes have shown that attenuated HRR response is significantly associated with adverse cardiovascular outcomes, including silent MI, cardiovascular and all-cause mortality.14–19
In addition to the above exercise-related measures of HR, we chose to evaluate the prognostic significance of resting HR as an early clinical sign of cardiac autonomic dysfunction. Resting HR is determined by the intrinsic sinus rate and is influenced by sympathetic and parasympathetic effects. It is simply measured and provides a global index of autonomic tone with important prognostic significance. 32 In the general population, as well as in type 2 diabetes, HR at rest was shown to be an independent predictor of cardiovascular and all-cause mortality.13,33,34 Of the three HR indices investigated in our cohort, resting HR greater than 100 bpm was the strongest predictor of the outcome event. This may reflect a progression to the clinical stage of cardiac autonomic neuropathy, with a relative increase in the sympathetic tone associated with vagal impairment. Nevertheless, resting tachycardia is a non-specific sign for cardiac autonomic dysfunction, and other conditions such as anaemia, heart failure or hyperthyroidism need to be taken into account.
Most previous studies have investigated only one exercise-related measure associated with the autonomic nervous system. A limited number of studies have evaluated and compared different exercise testing-related variables, and even less so examined the additive prognostic effect of combinations of several HR-related measures.35–42 These analyses have generally demonstrated a graded continuum of risk with the increase in the number of abnormal exercise testing parameters. However, these studies have commonly enrolled general populations referred for treadmill exercise testing, and not a clinically predefined cohort. In contrast to these studies, the current analysis demonstrates an additive prognostic effect of HR-related measures specifically in participants with asymptomatic type 2 diabetes who had at least one risk factor for cardiovascular disease. As cardiac autonomic neuropathy is a common complication of diabetes, the manifestation of subclinical HR abnormalities during exercise testing may provide important early prognostic information. It is possible that the association of the abnormal HR-related parameters with cardiovascular adverse outcomes is in part an expression of reduced functional capacity of these patients. However, adjustment for METs, a marker of exercise capacity, does not completely abolish this association, and accordingly the abnormality of the HR-related parameters may reflect an earlier stage of cardiac autonomic dysfunction.
There are several limitations to this study. The present study did not include subjects less than 55 years of age. All study participants were Caucasian, and recruited form a single healthcare system. In addition, the current findings may not be applicable to diabetes patients with established cardiovascular disease. These factors may limit the generalisability of the results to other populations.
Attenuated HRR, chronotropic incompetence and resting tachycardia are all associated with cardiac autonomic dysfunction in diabetes. Nevertheless, it is likely that these parameters are influenced by additional physiological and clinical determinants, which may not have been fully accounted for in this study. Moreover, these HR measures may have been affected by sinus node dysfunction (and arrhythmia). We excluded patients with atrial fibrillation, which may have modified the results. In addition, resting HR may have been influenced by withdrawal of beta-blockers prior to exercise testing and measurement of HR while standing. However, this is the routine clinical scenario prior to stress testing.
We did not compare or adjust the prognostic impact of the HR-related parameters to measures of exercise capacity, as exercise intolerance is associated with a more advanced clinical stage of cardiac autonomic neuropathy, and therefore may reflect a more progressive disease. Moreover, we did not analyse data on the total treadmill exercise test duration of each participant.
Our study has several strengths. The participation rate of both men and women was similar. The prospective design of the study enabled us to have a complete dataset for all participants, and to adjust for markers of disease severity such as the duration of diabetes, glycated haemoglobin levels and insulin therapy. Moreover, as noted, we have focused on individuals at risk with asymptomatic type 2 diabetes, a population among which cardiac autonomic neuropathy is more meaningful, in contrast to most other studies that recruited general referral populations.
Conclusions
In conclusion, resting tachycardia, chronotropic incompetence and reduced HRR are each significantly and additively associated with all-cause mortality, MI or stroke in asymptomatic type 2 diabetes patients without known coronary heart disease. These HR-related measures, which are simply obtained during a routine exercise treadmill test, may serve as an early warning sign for the development of cardiac autonomic neuropathy, a widely under-diagnosed complication of diabetes with significant prognostic implications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: a research grant from the European Foundation for the Study of Diabetes.