
Abstract
Background
Adherence to multiple cardiovascular (CV) medications is a cornerstone of coronary heart disease (CHD) management and prevention, but it is sub-optimal worldwide. This review aimed to examine whether interventions improve adherence to multiple CV medications in a CHD population.
Design
This study was based on a systematic review and meta-analysis according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
Methods
Randomised controlled trials were identified by searching multiple databases and reference lists. Studies were selected if they evaluated interventions aiming to improve adherence to multiple CV medications targeting a CHD population and if they provided an appropriate measure of adherence. Interventions were classified as complex or simple interventions. Odds ratios (ORs) were calculated and pooled for a meta-analysis. Risk of bias, heterogeneity and publication bias were also assessed.
Results
Sixteen studies (10,706 patients) were included. The mean age was 62 years (standard deviation (SD) 3.6) and 72% were male. In a pooled analysis, the interventions significantly improved medication adherence (OR 1.52; 95% confidence interval (CI) 1.25–1.86; p < 0.001) and there were no significant differences based on intervention type (complex vs simple), components categories and adherence method. There was moderate heterogeneity (I2 = 61%) across the studies. After adjusting for publication bias, the effect size was attenuated but remained significant (OR 1.35; 95% CI 1.09–1.68).
Conclusion
Interventions to improve adherence to multiple CV medication in a CHD population significantly improved the odds of being adherent. Simple one-component interventions might be a promising way to improve medication adherence in a CHD population, as they would be easier to replicate in different settings and on a large scale.
Keywords
Introduction
Medication adherence is defined as the process by which the patients take their medication as prescribed by their healthcare professionals.1,2 Although medication adherence is the preferred term, 1 other terms such as compliance or concordance have been commonly used in the literature. Adherence to a combination of long-term cardiovascular (CV) medications is a cornerstone of coronary heart disease (CHD) management and prevention. However, adherence to these medications is sub-optimal worldwide.3–5 It is known that medication adherence decreases with time 6 and a recent meta-analysis found that only 60% of nearly two million participants had an overall good adherence (adherence ≥ 80%) to CV medications. 7 Therefore, to improve adherence to evidence-based CV medications and achieve the subsequent reduction in morbidity, mortality and costs, there is a need for interventions that improve the medication-taking behaviour of CHD patients.
CHD is a singular medical condition and it can have positive or negative effects in the patients’ life. 8 While a fear of a heart attack may have a positive effect on medication adherence, the complexity of guideline-recommended CV medication regimens is a well-recognised barrier to adherence for patients with CHD. 9 Previous reviews assessing interventions to improve medication adherence are limited in terms of addressing these specific details related to CHD. Reviews have tended to include a broad patient population with a variety of medical conditions10,11 or patients with CV disease but with a focus on hypertension and heart failure.12,13 In addition, previous reviews have focussed on one specific class of CV medication, such as lipid-lowering, 14 or on one specific type of intervention such as multi-professional interventions 15 or reminder packaging. 16 To our knowledge, no previous review has evaluated interventions to improve adherence to multiple CV medications in a CHD-specific population.
Our primary aim was to examine whether interventions improved patients’ adherence to multiple CV medications, by reviewing randomised controlled trials (RCTs) that assessed any type of intervention aimed at improving adherence in a CHD population compared to usual care or no intervention. In addition, we aimed to determine which types of intervention components were present in the interventions; whether the interventions improved clinical outcomes; whether they were cost-effective and the degree of patient’s satisfaction with the interventions.
Methods
Protocol and registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines and followed the methods pre-specified and documented in a protocol. The review was registered in the International prospective register of systematic reviews (PROSPERO) Registry CRD42015016694.
Study inclusion criteria
Randomised controlled trials with individual or cluster randomisation were considered for inclusion if the study population comprised adults (over 18 years) with a diagnosis of CHD, including previous acute coronary syndrome (myocardial infarction and unstable angina), stable angina, percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery (CABG). Studies were excluded if some participants in the study did not have an established diagnosis of CHD, for example studies that comprised a mixed population including participants with established CHD and participants with an estimated high risk of CV diseases (≥15%), and if they involved psychiatric and institutional patients (to avoid potential external controls over adherence). Studies were eligible if the main objective of the intervention was to improve patient’s adherence to multiple CV medications or if a broader intervention, such as in cardiac rehabilitation programmes, had a core component focused on improving medication adherence. Only studies with interventions targeting patients and consumers were included. Studies investigating interventions to improve adherence to only one specific class of CV medication, e.g. statins, were excluded as it is recommended that CHD patients take a combination of CV drugs concomitantly.17–19
Medication adherence is defined as the extent to which patients take medications as prescribed, therefore we only included studies that provided sufficient information about the extent to which patients were adhering to their drug regimen (e.g. whether there were any missed doses). We excluded studies that reported only prescription rates (e.g. whether the patient was prescribed a particular medication by their physician) and medication use rates (e.g. a Yes/No type of question about whether the patient is taking the prescribed medication). We included studies using any method of adherence, including indirect (e.g. pill count, prescription refill rate, electronic monitoring), direct (tracer substances in blood or urine) and subjective measures (e.g. self-report questionnaires). Other proxy measures for adherence included physiological indicators (e.g. cholesterol, blood pressure), health outcome indicators (e.g. quality of life, morbidity, mortality), adverse effects and cost evaluations, if reported in association with medication adherence outcomes in the main paper.
Search strategy
Five databases (Medline, CENTRAL, PsycINFO, EMBASE, CINAHL) were searched on 6 February 2015 and re-searched on 21 July 2015 with no language restriction. A date limit (1 January 1995 to year 2015) was applied to ensure that only contemporary evidence was reviewed. The database search strategy was developed in collaboration with a librarian. Search terms included patient compliance, treatment refusal, adherence, non-adherence, coronary disease, myocardial ischemia, myocardial infarction, percutaneous coronary intervention and coronary artery graft bypass (Supplementary Material, S1). Appropriate RCT filters were used to maximise identification of randomised controlled trials. Additional articles were obtained through manual search of reference lists and by contacting experts in the field.
Study selection
One author (KS) carried out the database searches. Two authors (KS, SK) independently screened all titles and abstracts. Full-text articles of potentially relevant studies were assessed independently by the same authors using a pre-determined eligibility assessment form. A study was included if it met all inclusion criteria. Any disagreement was discussed and resolved by consensus; and a third reviewer (JR) was consulted in case of an unresolved disagreement. A reference management system (Endnote X6 - Thompson Reuters) was used to identify and remove duplicate references, which was verified by manual search.
Assessment of risk of bias
Assessment of risk of bias of the included studies was done independently by two authors (KS, SK) using the Cochrane ‘Risk of Bias’ tool. 20 The main sources of systematic bias in trials were assessed: selection bias, performance bias, detection bias, attrition bias and reporting bias. Random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and selective reporting were coded into low, high or unclear risk of bias. The method used to measure adherence was also considered, as some methods are more likely to be biased than others.
Data extraction
The relevant data from the included articles were extracted using a pre-designed electronic spreadsheet that was developed and test-piloted for this review. One author (KS) extracted the data and a second author (SK) checked it for accuracy. Extracted data included study characteristics (design, date, aim, sample size, country, recruitment, inclusion and exclusion criteria), participants’ characteristics (CHD diagnosis, age, gender), intervention characteristics (intervention and comparator descriptions, number of intervention groups, CV medication targeted, mode of delivery, professional delivering the intervention, number and time points of intervention delivery), adherence measures (number, type and definition of adherence outcome), adherence outcomes (outcome data and statistical significance, time point reported) and other outcomes (type and definition of outcome, outcome data and statistical significance). When study results were reported at more than one time point, the last time point results were recorded. When two or more articles reported results from the same study, both articles were considered together for more complete data extraction. Authors were contacted for missing, incomplete or unclear data.
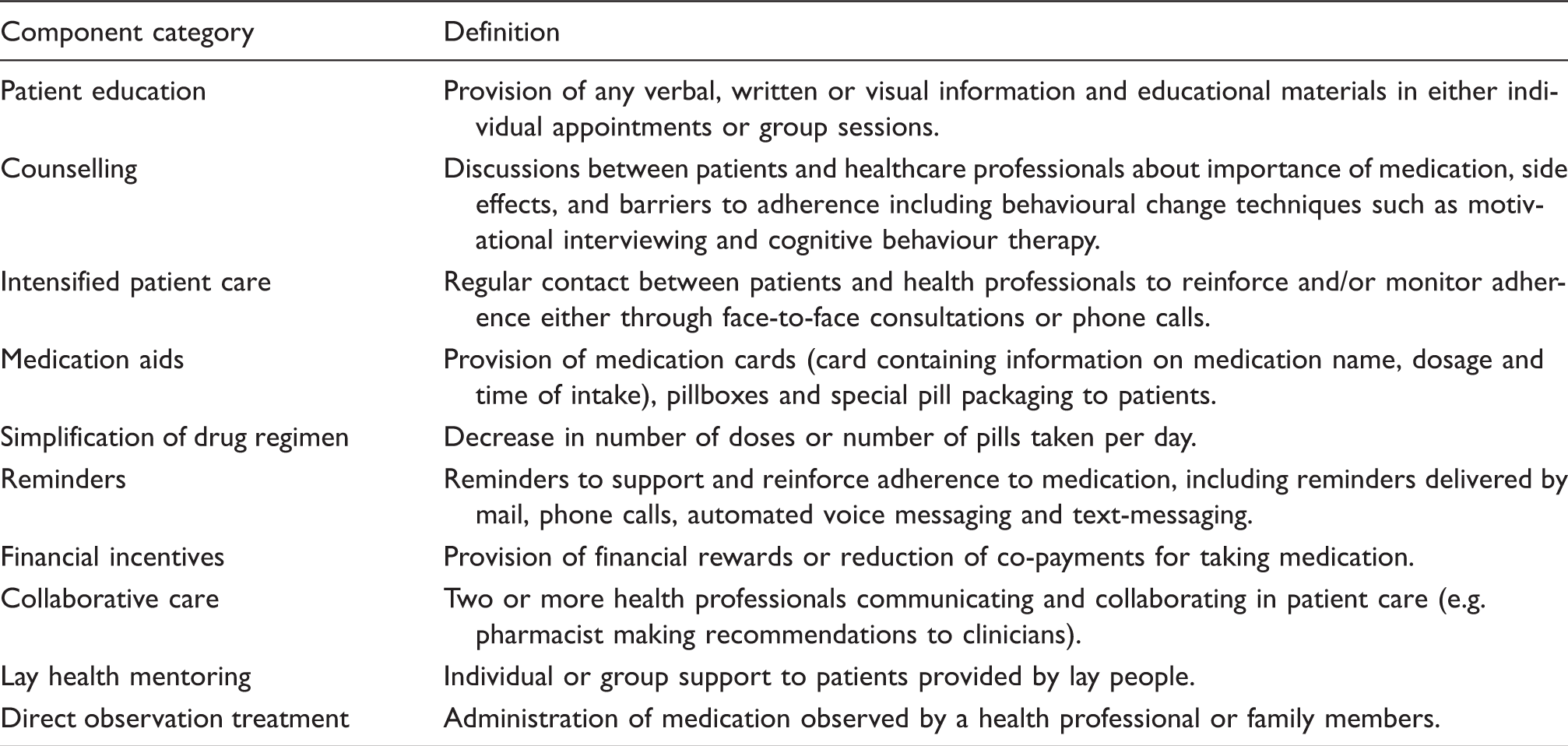
Categories of interventions’ components.
Analysis and synthesis
Overall study and participant characteristics were summarised as means or medians for continuous data and as frequencies and proportions for categorical data. We used a software program (Comprehensive Meta-analysis, Version 3.3.070) to pool the data for a meta-analysis. We calculated the odds ratio (OR) of being adherent with 95% confidence interval (CI) for each study and used a random-effects model to pool the estimates. We used the overall adherence to all CV medications measured in the study to calculate the OR. For studies that did not report an overall adherence, we combined the adherence to each individual drug to get an overall estimate of adherence, which is a recommended approach when multiple outcomes are reported within a study. 22 For studies with multiple groups, we computed a summary effect for the groups with active interventions and analysed the data in a single pair-wise comparison (intervention vs control), which is also the recommended approach. 23 We assessed heterogeneity between the studies by calculating the I2 statistic. An I2 statistic exceeding 50% with p-value < 0.05 was interpreted as representing substantial heterogeneity. 24 We assessed publication bias by using the funnel plot symmetry and Egger regression intercept. An asymmetric funnel plot with an Egger test p-value < 0.05 was interpreted as indicative of publication bias. We used the trim-and-fill method by Duval and Tweedie to impute the missing studies. 25 To investigate heterogeneity, we performed subgroup analysis based on intervention type (complex vs simple), components categories (only for components that were present in more than half of the included studies) and type of adherence methods (self-report vs other more objective methods). We also performed sensitivity analysis excluding studies assessed with low quality (defined as having a high or unclear risk of bias in any of the source of bias criteria, excluding blinding of participants).
There is no gold standard for measuring medication adherence and defining a patient as adherent. Being adherent was defined as per the definition used in each individual trial. For studies that reported more than one type of adherence method, we used the most objective measure, according to the pre-defined hierarchy: medication event monitoring system (MEMS), prescription refills, pill count and self-report. If studies reported more than one self-report method, we used the measure that provided the percentage of doses taken. We used results presented in either continuous or dichotomous scales, as this is acceptable approach 26 and has been done by others.27,28 For studies that reported the results in both types of scale, we selected the continuous scale over the dichotomised scale.
Results
The search retrieved 4766 references from all sources (Figure 1). After exclusion of duplicates, 3758 titles and abstracts were screened and 3670 were excluded. Eighty-eight full-text articles were assessed for eligibility and 71 articles were excluded for several reasons detailed in Figure 1. Seventeen articles reporting 16 studies that met all the eligibility criteria were included in this review.
Flowchart of selection of included articles. CV: cardiovascular.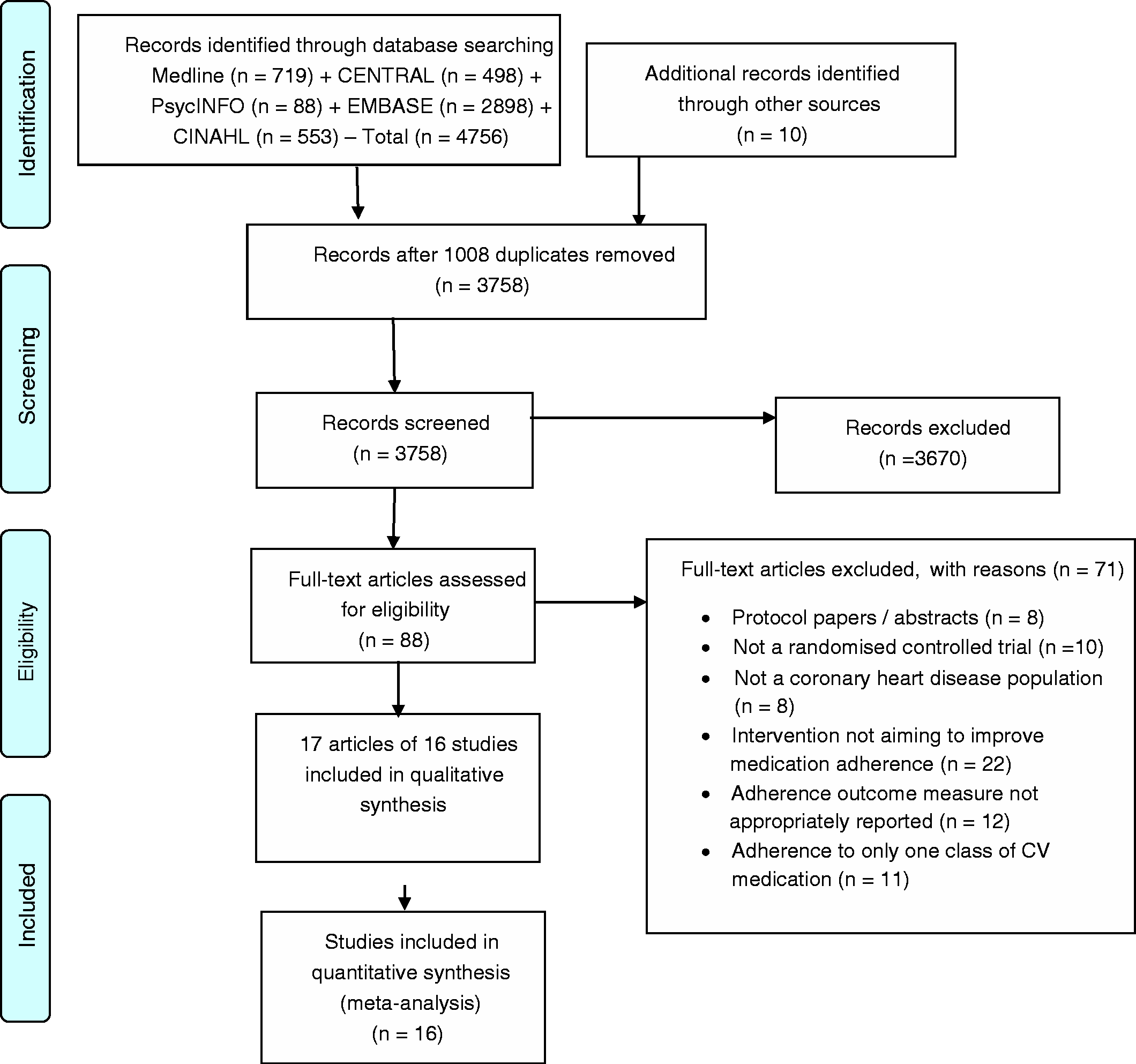
Characteristics of included studies
Study characteristics and adherence measures.

ACS: acute coronary syndrome; CABG: coronary artery bypass surgery; CG: control group; CHD: coronary heart disease; CMA: continuous multiple-interval; CMG: cumulative medication gap; IG: intervention group; IQR: interquartile range; M: male; MARS: Medication Adherence Report Scale; MEMS: medication event monitoring system; MI: myocardial infarction; MMAS: Morisky Medication-taking Adherence Scale; MPR: medication possession ratio; PCI: percutaneous coronary intervention; PDC: proportion of days covered; RCT: randomised controlled trial; SD: standard deviation.
Proportion of days covered ((number of days of medication supply available/total number of days during study period) × 100).
Pill count ((no. of pills dispensed–no. of pills returned)/no. of pills prescribed × 100).
Medication possession ratio ((number of days of medication supply available/days of eligibility for the medication) × 100).
Cumulative medication gap (number of days of medication supply not available/days of eligibility for the medication).
Continuous multiple-interval (number of days of medication supply obtained/total number of days between refill records).
Intervention components of included studies.
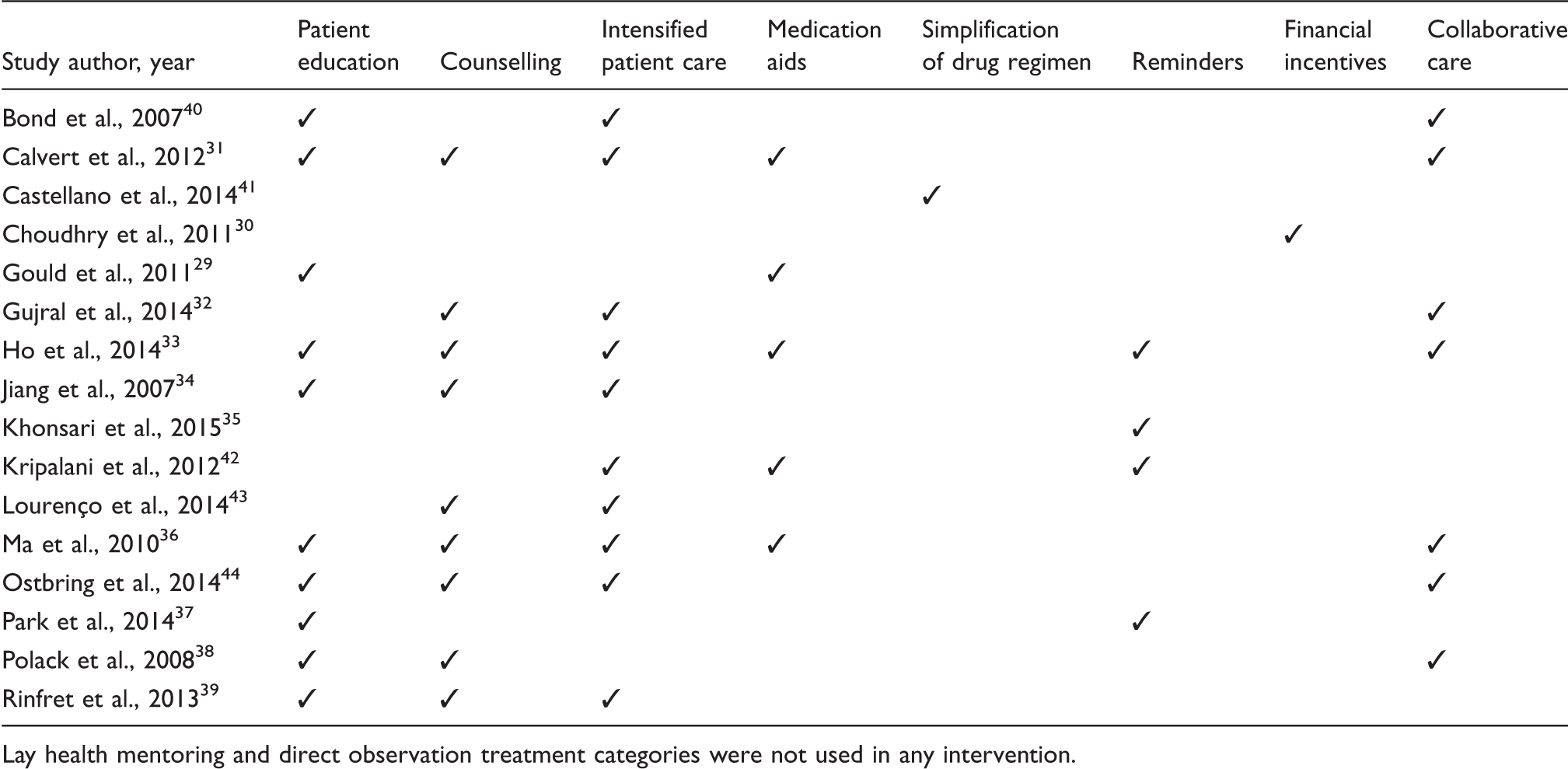
Lay health mentoring and direct observation treatment categories were not used in any intervention.
In terms of adherence measures, the majority of studies reported self-report measures, while seven used prescription refills, one used pill count 39 and one used MEMS (Table 2). 35 Trials reported adherence in either a continuous and dichotomous scale. The majority of the trials reported a threshold of 75–80% to be considered as adherent. 35 Half of the trials reported overall adherence,34,35,38,40-44 four trials reported adherence to individual classes of medications32,36,37,39 and four trials reported both.29–31,33
Effects of interventions
Medication adherence
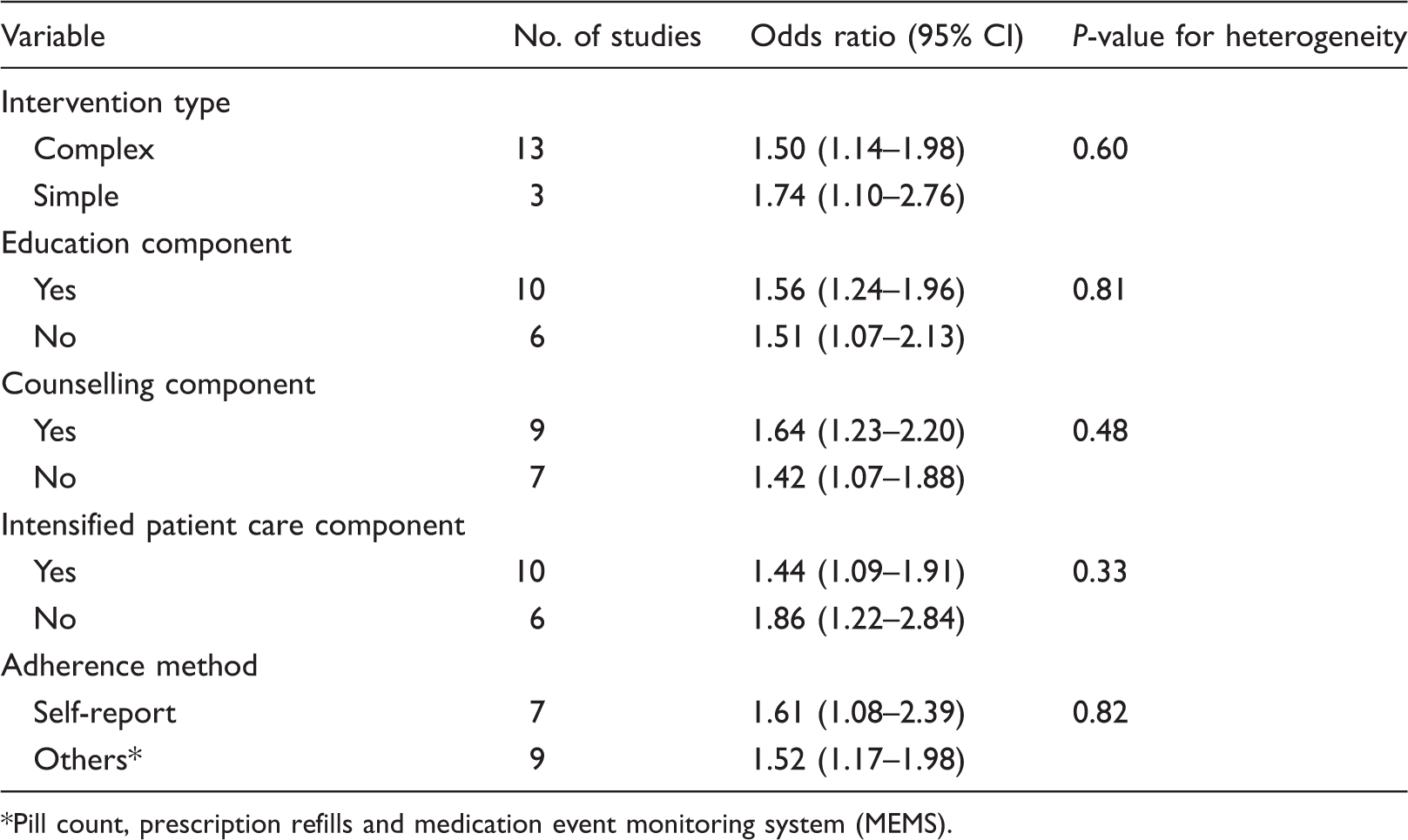
In a pooled analysis of 10,706 patients, the delivery of an intervention, irrespective of its type, significantly improved medication adherence (OR 1.52; 95% CI 1.25–1.86; p < 0.001) (Figure 2). The interventions were similarly effective when the analysis was restricted to only high quality studies (OR 1.70; 95% CI 1.20–2.41; p = 0.003) (Supplementary Material, S3). There was moderate heterogeneity (I2 = 61%; p = 0.001) across the studies. We investigated the heterogeneity by conducting subgroups analysis in which we did not find any significant differences based on intervention type, components categories and type of adherence method (Table 4). Publication bias was detected by funnel plot asymmetry (Supplementary Material, S4), however the Egger regression coefficient was not significant (one-tailed p = 0.06), possibly due to low power. Using the trim-and-fill imputation for missing studies, the adjusted effect size was attenuated but remained significant (OR 1.35; 95% CI 1.09–1.68).
Meta-analysis of the effect of interventions on medication adherence. CI: confidence interval. Effects of the interventions on medication adherence in sub-groups stratified by intervention type, components categories and type of adherence method. Pill count, prescription refills and medication event monitoring system (MEMS).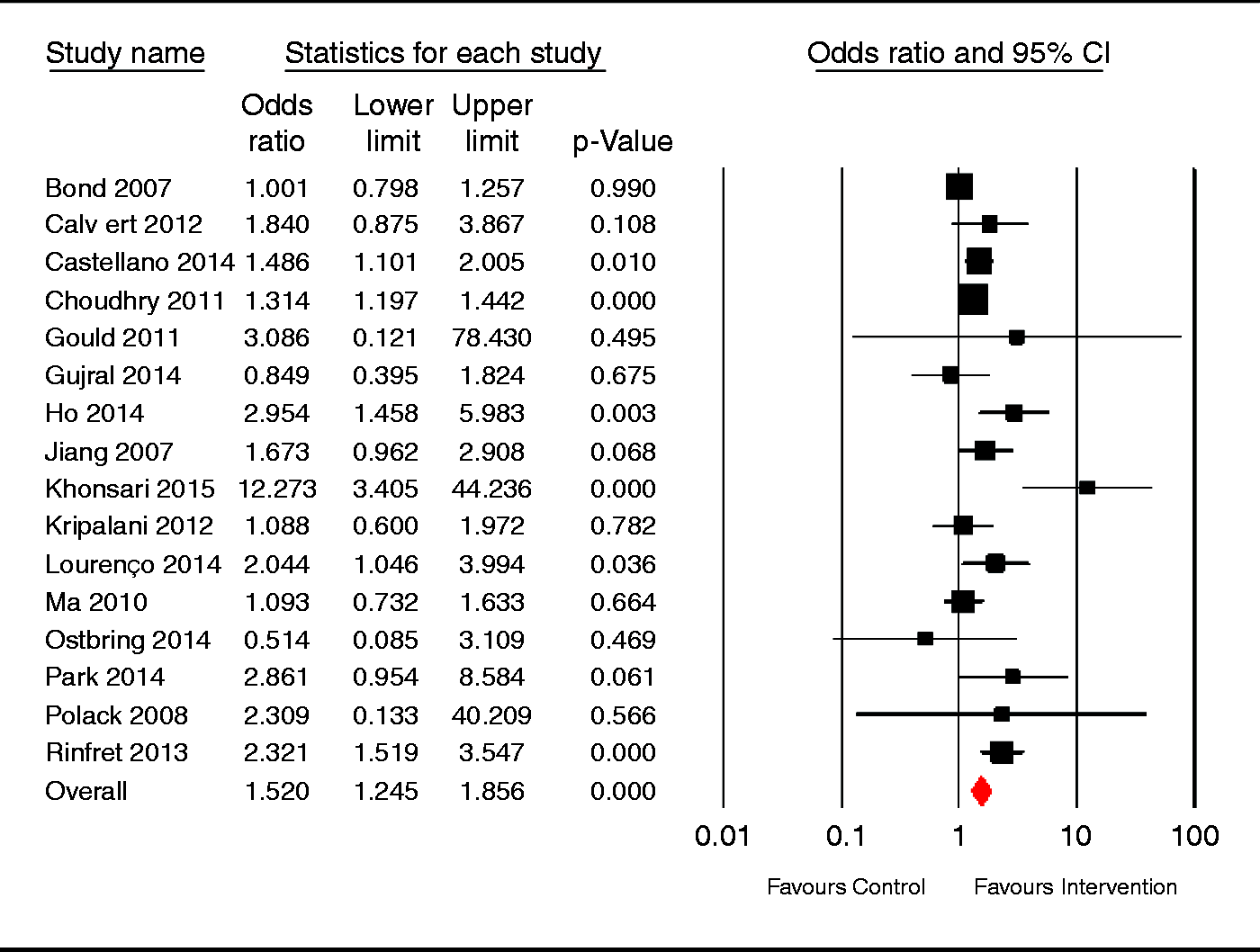
Other outcomes
Few studies reported other outcomes. For clinical outcomes, there was no statistically significant difference in three trials,33,36,41 while one trial reported greater reduction in total and low-density lipoprotein (LDL)-cholesterol. 34 In four trials, there was no significant difference in CV events, re-hospitalisation and death,33,35,39,41 while one study showed significant reductions in major vascular events or revascularisation in the intervention group. 30 In terms of costs, two trials reported no statistical difference in total costs between groups,30,33 while one trial reported higher costs due to pharmacists’ training in the intervention group. 40 In terms of patient’s satisfaction, two trials reported high satisfaction with pharmacist and nurse interventions,29,40 while two trials reported that a text-messaging intervention was useful and helped the majority of intervention patients to take their medication.35,37
Assessment of risk of bias
Overall, the majority of studies was classified as having low or unclear risk of bias across all main sources of bias, not taking into account blinding of participants and personnel as this was impractical due to the nature of the interventions (Figure 3 and Supplementary Material, S5). Eleven trials provided information about adequate random sequence generation and nine adequate allocation concealment. Eleven trials reported blinded outcome assessors or used objective measures of adherence (prescription refills and MEMS) and hence, were classified as having low risk for blinding of outcome assessment. In terms of incomplete outcome data, seven trials were classified as unclear risk, raising a concern about trial results being biased; while all included trials, except one, had low risk of bias in selective reporting.
Risk of bias assessment summary.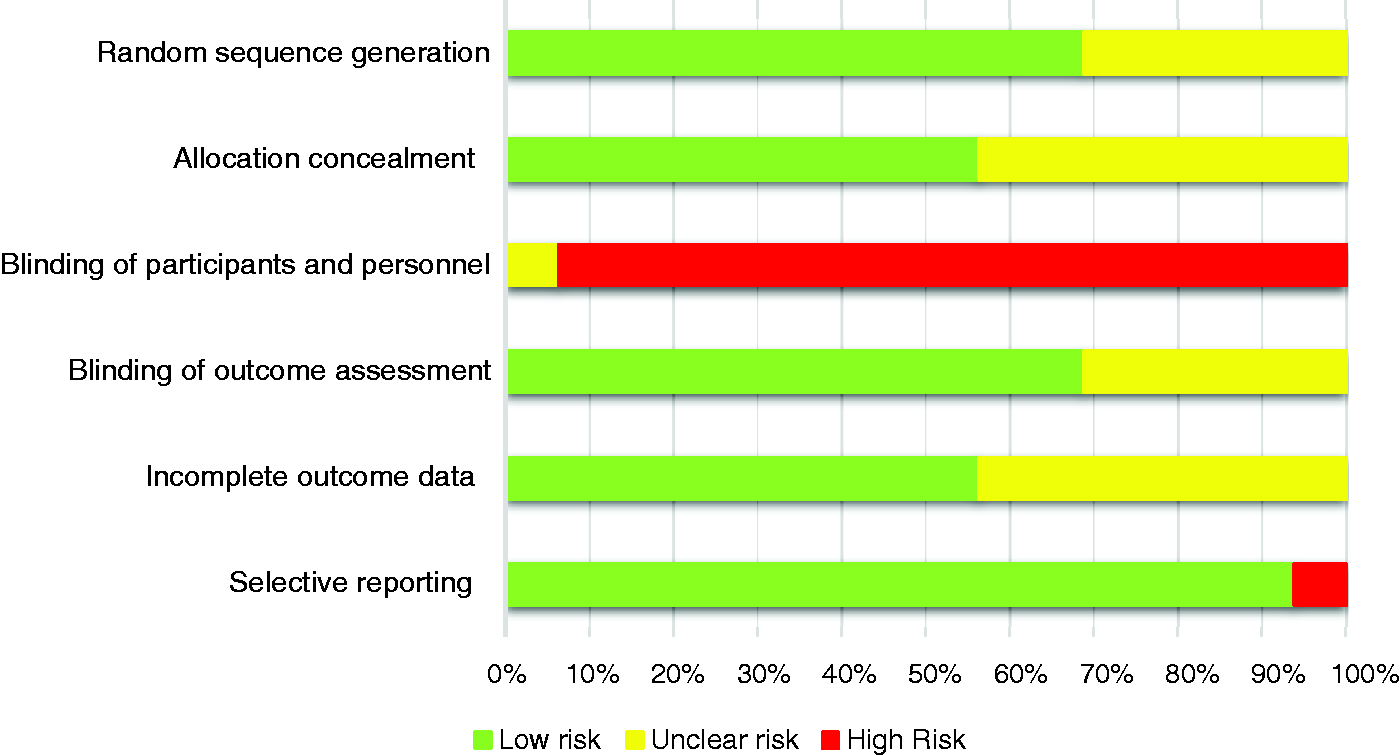
Discussion
In this review, we assessed 16 studies that investigated the effectiveness of interventions to improve adherence to multiple CV medications in a CHD population. We found that the interventions significantly improved medication adherence by increasing the odds of being adherent to the CV medications by 50%. This means that if we assume that 60% of the patients are adherent to CV medications 7 then implementing an intervention, irrespective of its type, could increase the percentage of adherent patients to around 70%. We also found that the interventions were diverse and that the majority were complex, comprising two or more components. Due to this diversity, our review was unable to ascertain which types of interventions would definitely improve adherence, however the subgroup analysis suggest that there is no difference between complex and simple interventions, as well as between interventions that include patient education, counselling and intensified patient care components compared with those interventions without these components.
A previous Cochrane review also found that interventions to improve adherence to medications in any medical condition are mostly complex. 10 The disadvantages of complex interventions are that they are difficult to compare and be replicated, thereby possibly increasing costs and making implementation in routine practice difficult. Our results showed that simple interventions might be as effective as more complex ones. In our review, three trials used simple interventions by delivering text-message reminders, simplifying the drug regimens using a polypill and by using co-payments to reduce the burden of medication costs in the patients’ life. Other reviews have found that text-messages27,45,46 and polypills 47 can improve adherence in a wide range of diseases. An interesting common factor between these three interventions is that they do not require dedicated personnel to deliver them. Cutrona et al. have previously reported that person-independent interventions were successful in improving adherence to CV medication. 48 These findings highlight that simple interventions not requiring dedicated personnel to deliver them might be a promising way to improve medication adherence in a CHD population, as these interventions are easier to replicate in different settings and on a large scale. Future studies comparing the effects of complex and simple interventions on adherence will help confirm this hypothesis.
Importantly, medication adherence in a CHD population must be viewed within a broader context of CV risk management that includes a concomitant focus on lifestyle changes, such as smoking cessation, regular physical activity and a healthy diet. In this review, we included only two studies that investigated interventions classified as broader interventions. Although cardiac rehabilitation programmes generally aim to improve medication adherence in a CHD population, few studies report a core component of the programme dedicated to achieve this goal and the majority do not measure and report the adherence outcome appropriately. The results of this review emphasise that cardiac rehabilitation and prevention programmes should include a dedicated strategy for medication adherence promotion, meanwhile promoting lifestyle changes.
Our review has identified important limitations of medication adherence research in a CHD population. The lack of a gold standard method contributes to the lack of uniformity in measuring adherence, resulting in difficulty in assessing and comparing different interventions. In this review, studies reported different methods for measuring adherence, therefore to pool the data we had to combine these different methods, always considering the most objective measure reported according to our previously pre-specified hierarchy. In addition, international guidelines17–19 recommend that patients with CHD adhere to multiple CV medication concomitantly. However, in our review, some studies only measured adherence to individual classes of CV medication, which were combined into an overall adherence to all CV medication in our meta-analysis. It is important to emphasise that future studies should aim to improve the overall adherence to all CV medication, as an overall improvement is more likely to be associated with clinical and health benefits than improvements in adherence to aspirin only, for example.
We also acknowledge that our results might have been limited by our rigorous inclusion criteria and the low quality of more than half of the trials. In addition, our review was not able to demonstrate that the significant improvement in medication adherence would be translated into concurrent benefits in clinical and health outcomes, as these outcomes were only reported in a few of the included studies. Therefore, we recommend that future medication adherence research always includes clinical measures to ensure this translation from medication adherence into clinical outcomes.
Conclusion
Interventions to improve adherence to multiple CV medication in a CHD population significantly improved the odds of being adherent. The interventions were diverse and mostly complex, however the complex interventions were found to have similar results when compared to simple one-component interventions. These simple interventions might be a promising way to improve medication adherence in a CHD population, as they would be easier to replicate in different settings and on a large scale. However, benefits in clinical outcomes and cost-effectiveness need to be determined by future research.
Footnotes
Acknowledgments
The authors acknowledge the role of Jeremy Cullis at the University of Sydney who contributed to the design of the search strategy, and Laurent Billot at The George Institute for Global Health who provided guidance and advice in the statistical analysis. Information about this work will be presented as a poster at the World Congress of Cardiology and Cardiovascular Health on 6 June 2016 in Mexico City, Mexico.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KS is funded by a University of Sydney International Postgraduate Research Scholarship. JT is funded by a University of Sydney Australian Postgraduate Award. RW is funded by a National Heart Foundation Post-doctoral Fellowship (APP100493). CKC is funded by a Career Development Fellowship co-funded by the National Health and Medical Research Council (NHMRC) and National Heart Foundation, and a Sydney Medical Foundation Chapman Fellowship (APP1033478). JR is funded by a Career Development and Future Leader Fellowship co-funded by the NHMRC and the National Heart Foundation (APP1061793). JC is an investigator on NHMRC programme grant (ID1052555).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.