
Abstract
Objective
The objective of this study was to determine time trends in the implementation of European guidelines on the management of cardiovascular disease prevention in people at high cardiovascular risk.
Methods
Cardiovascular disease prevention as reflected in the primary care arms of the EUROASPIRE III and IV surveys were compared in centres from Bulgaria, Croatia, Poland, Romania and the United Kingdom that participated in both surveys. All patients were free of cardiovascular disease but considered at high cardiovascular disease risk since they had been started on blood pressure and/or lipid and/or glucose lowering treatments. They were interviewed and examined by means of standardized methods ≥6 months after the start of therapy.
Results
EUROASPIRE III comprised 2604 and EUROASPIRE IV 3286 subjects whereof 76% and 56% were interviewed. There were no major differences between the two surveys in age, gender, centres and reasons for inclusion. The prevalence of smoking was similar between EUROASPIRE III and IV. The proportion of smokers who did not intend to quit was significantly greater in EUROASPIRE IV compared with III. The prevalence of overweight or obesity was high and identical in both surveys. No significant differences were observed in physical activity. In participants not on blood pressure lowering treatment an elevated blood pressure was observed in 47% in both EUROASPIRE III and IV. In participants not on lipid lowering drugs the low-density lipoprotein cholesterol was ≥2.5 mmol/l in 87% and 88% in EUROASPIRE III and IV respectively. In participants free from known diabetes fasting plasma glucose was ≥7 mmol/l in 12% and 18% in EUROASPIRE III and IV. In subjects with known arterial hypertension blood pressure was at or below guideline recommended targets in 28% in EUROASPIRE III and 35% in IV. In participants on lipid lowering drugs the low-density lipoprotein cholesterol was < 2.5 mmol/l in 28% and 37% in EUROASPIRE III and IV. Glycated haemoglobin was < 7.0% in participants with known diabetes in 62% and 60% in EUROASPIRE III and IV.
Conclusions
The results from EUROASPIRE III and IV clearly demonstrate that the control of modifiable risk factors in people at high cardiovascular disease risk remains poor.
Introduction
Primary prevention of atherosclerotic cardiovascular disease (CVD) remains a major challenge in Europe and in other places in the world. In observational cohort studies it has been repeatedly shown that CVD is less likely to occur in the presence of healthy lifestyles.1,2 In randomized controlled intervention studies in persons with arterial hypertension, hypercholesterolaemia or diabetes the control of these risk factors was clearly associated with the prevention of CVD events.3-5 European guidelines on CVD prevention in clinical practice summarize how, when and in whom prevention strategies should be developed. Joint European Societies Task forces regularly update these guidelines and the last update was published in 2012. 6
In the EUROASPIRE surveys the implementation of these guidelines in clinical practice is examined. There have been four such surveys until now. The hospital arms of these surveys deal with secondary prevention in coronary patients.7-10 In the primary care arms that have been undertaken since the third EUROASPIRE (EA III) survey the implementation of the guidelines is looked at in subjects still free from but at high risk of developing CVD. 11
The present report compares results from the EA III primary care arm with those from the same participating centres in the EUROASPIRE IV (EA IV) with the objective to examine whether changes have taken place regarding lifestyles and risk factor detection and management over a period of eight years.
Patient population
Primary care centres from the same geographical regions that participated in both EA III and IV surveys were selected: these centres were located in Bulgaria (mainly centres in Sofia) , Croatia (centres in Zagreb), Poland (centres in Krakow town and two surrounding rural districts), Romania (centres in Timisoara) and the United Kingdom (centres in Hull in EA III and in London in EA III and IV). In principle general practices were identified from a convenience sample organized differently in each country according to the structure of the local health services. The governing principle of the sample was that any patient being treated for hypertension, dyslipidaemia or diabetes had an approximately equal chance of being included. In these practices consecutive patients, men and women aged ≥18–<80 years without a history of coronary or other atherosclerotic disease were identified if they had been prescribed one or more of the following therapies: (i) blood pressure lowering and/or (ii) lipid lowering and/or (iii) glucose lowering treatments (diet and/or oral and/or injectable) since >6 months but <3 years prior to the date of identification. Persons sampled by each of these treatments might have been using one or more of the other therapies.
Information on eligibility criteria was obtained from medical records according to local possibilities in each of the primary care centres. Eligible persons were invited to attend a visit where trained research assistants conducted a standardized interview.
Methods
At the time of interview venous (fasting) blood was drawn for serum total and high-density lipoprotein cholesterol (HDL-C), triglycerides, and glycated haemoglobin (HbA1c) while low-density lipoprotein cholesterol (LDL-C) was calculated according to Friedewald’s formula. The central laboratory was the Disease Risk Unit, National Institute for Health and Welfare, Helsinki, Finland, which is accredited by the Finnish Accreditation Service and fulfils the requirements of the standard SFS-EN ISO/IEC 17025:2005. Venous blood samples were taken in a sitting position with light stasis into a tube containing clot activator (Venosafe, Terumo Europe, Leuven, Belgium) for lipid assays and into a potassium EDTA tube (Venosafe) for HbA1c assay. Serum was separated by centrifuging at 2000 × g for 10 min at room temperature. After that serum was aliquoted into two bar-code-labelled tubes and stored together with whole EDTA blood tubes locally at a minimum of –70 ℃ and then transported frozen to the central laboratory where all measurements were performed on a clinical chemistry analyser (Architect c8000; Abbott Laboratories, Abbott Park, Illinois, USA). Total cholesterol and HDL-C and triglycerides were analysed in serum, and HbA1c in whole blood with the following methods: enzymatic method for total cholesterol, a homogenous method for direct measurement of HDL-C, an enzymatic glycerol phosphate oxidase method for triglycerides, an immunoturbidimetric method for HbA1c and an enzymatic hexokinase method for plasma glucose in EA III; the laboratory takes part in the Lipid Standardization Program organized by CDC, Atlanta, Georgia, USA and External Quality Assessment Schemes organized by Labquality, Helsinki, Finland. During the course of the study (two months in 2013), the coefficient of variation (mean ± SD) and systematic error (bias) (mean ± SD) were 1.3% ± 0.2 and 1.7% ± 1.1 for total cholesterol, 1.6% ± 0.5 and –1.5% ± 1.6 for HDL-C, 2.3% ± 0.1 and –1.2% ± 2.6 for triglycerides, and 1.9% ± 0.1 and 1.4% ± 0.2 for HbA1c, respectively.
In EA IV plasma glucose was analysed locally with a photometric point-of-care technique (Glucose 201 + , HemoCue®, Ängelholm, Sweden). Regression analysis between the HemoCue® instrument and standard isotope dilution gas chromatography-mass spectrometry (IDGC-MS) showed a slope of 1.051 (95% confidence interval (CI): 1.031 to 1.071) an intercept of –0.222 (95% CI –0.016 to –0.428; r = 0.994). The mean deviation was 0.24 mmol/l (2.0%). Values obtained with the HemoCue® instrument were in 69% within 5%, in 91% within 10%, and always within 14.3% of the IDGC-MS method. The HemoCue® method is cholesterol sensitive due to the measurement in very small volumes with higher levels of glucose with lower cholesterol. Therefore the glucose values were corrected according to the formula: HemoCue® glucose + 0.22 × (total cholesterol – 5 mmol/l). The values were converted from whole venous blood to plasma applying the formula by Carstensen: 12 plasma glucose = 0.558 + 0.119 × whole blood glucose. Standardized use of the equipment was assured through central training of the data collectors, and retrieval of HemoCue®-cuvette storage information and validation sheets from a selection of the participating centres..
Height and weight were measured in light indoor clothes without shoes (SECA scales 701 and measuring stick model 220). Obesity was defined as a body mass index (BMI) ≥30 kg/m2.
Waist circumference was measured using a metal tape applied horizontally at the point midway in the mid-axillary line between the lowest rim of the rib cage and the tip of the hip bone (superior iliac crest) with the patient standing. Central obesity was defined as a waist circumference of ≥88 cm for women and ≥102 cm for men.
Blood pressure was measured twice on the right upper arm in a sitting position using an automatic digital sphygmomanometer (with Omron M5-1 in EAIII and Omron M6 in EAIV) and the mean was used for all analyses. According to the manufacturer (OMRON Healthcare (UK) Ltd) no conversion formula is required for blood pressure measurements obtained by Omron M6 and Omron M5-I.
Breath carbon monoxide was measured in ppm using a smokelyser (Bedfont Scientific, Model Micro 4 in EA III and Micro + in EA IV). Smoking at the time of interview was defined as self-reported smoking, and/or a breath carbon monoxide exceeding 10 ppm.
Higher educational level was considered in individuals who had completed college or university or had a postgraduate degree.
The outcome measures were changes in the proportions of high-risk individuals achieving lifestyle, risk factors and therapeutic targets for CVD prevention.
The EA III primary care arm survey took place in 2006–2007 and the EA IV primary care arm survey in 2014–2015.
Data management
In both EA III and IV data were collected electronically and submitted via Internet to the data management centre (Euro Heart Survey for EA III and the EuroObservational Research Programme for EA IV, European Heart House, Sophie Antipolis, France). Data were checked for completeness, internal consistency and accuracy. All data were stored under the provisions of the National Data Protection Regulations.
Ethical approval
National coordinators were responsible for obtaining approval by the local ethics committee. Written informed consent was obtained from each participant by the investigator by means of a signed declaration. The research assistants signed the case record form to confirm that informed consent was obtained and stored the original of the signed declaration of consent in the patient file.
Statistical analyses
Descriptive statistics were used to estimate the frequency of risk factors, lifestyles and drug use by survey, country, gender, age and reason for inclusion. In the statistical analysis, the clustering of patients within countries was taken into account according to multilevel modelling. Potential confounding due to differences between surveys in distributions of age and gender was adjusted for in these models. Because of the limited number of centres within countries, centre was not considered as a separate level in the multilevel analysis. The assumption that time trends in risk factor frequencies would be parallel between countries is unrealistic. By use of random coefficients in the models, we allowed differences between surveys to vary between countries. p-values for evaluating the null hypothesis of equal risk factor frequencies between surveys were based on Wald-type tests. All statistical analyses were done with SAS statistical software (version 9.4) (PROC GLIMMIX).
Results
In EA III and EA IV respectively 2604 and 3286 eligible persons were identified in the medical records of the primary care practices; 1985 and 1842 individuals participated in the visits of respectively EA III and IV, representing an interview rate of respectively 76% and 56%. The lower interview rate in EA IV was mainly due to a higher proportion of people who did not respond to any of the invitation procedures. Non-participants were younger in EA III (64% < 60 years of age compared with 57% in the participants) but this was also the case in EA IV (62% < 60 years of age in the non-participants compared with 49% in the participants); female persons participated more in EA III (60% of the participants were female in EA III compared with 50% in the non-participants) but this was also the case in EA IV (54% of the participants were female compared with 46% in the non-participants).
Distribution of age, gender, centre and reason for inclusion.
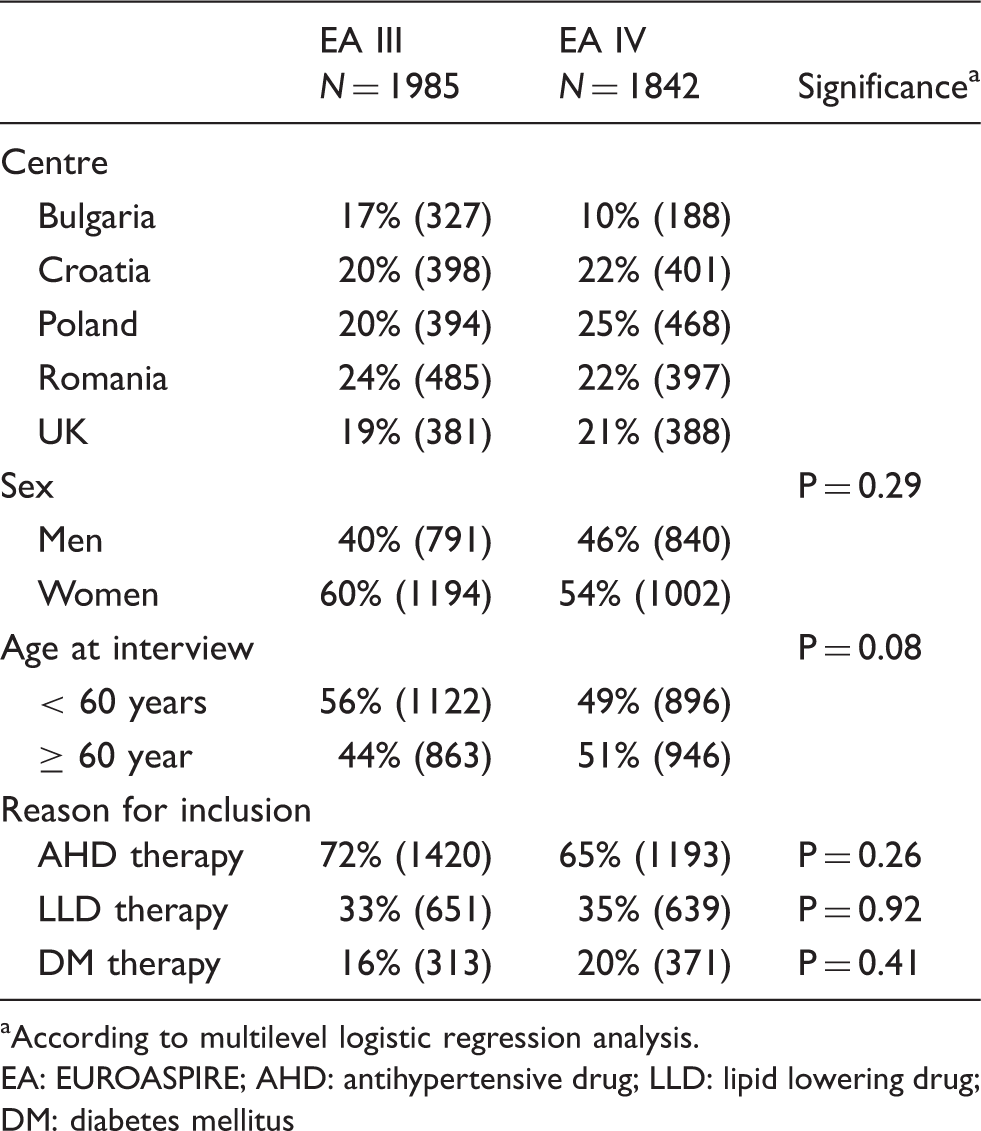
According to multilevel logistic regression analysis.
EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
Prevalence of smoking a at interview and intention to quit.
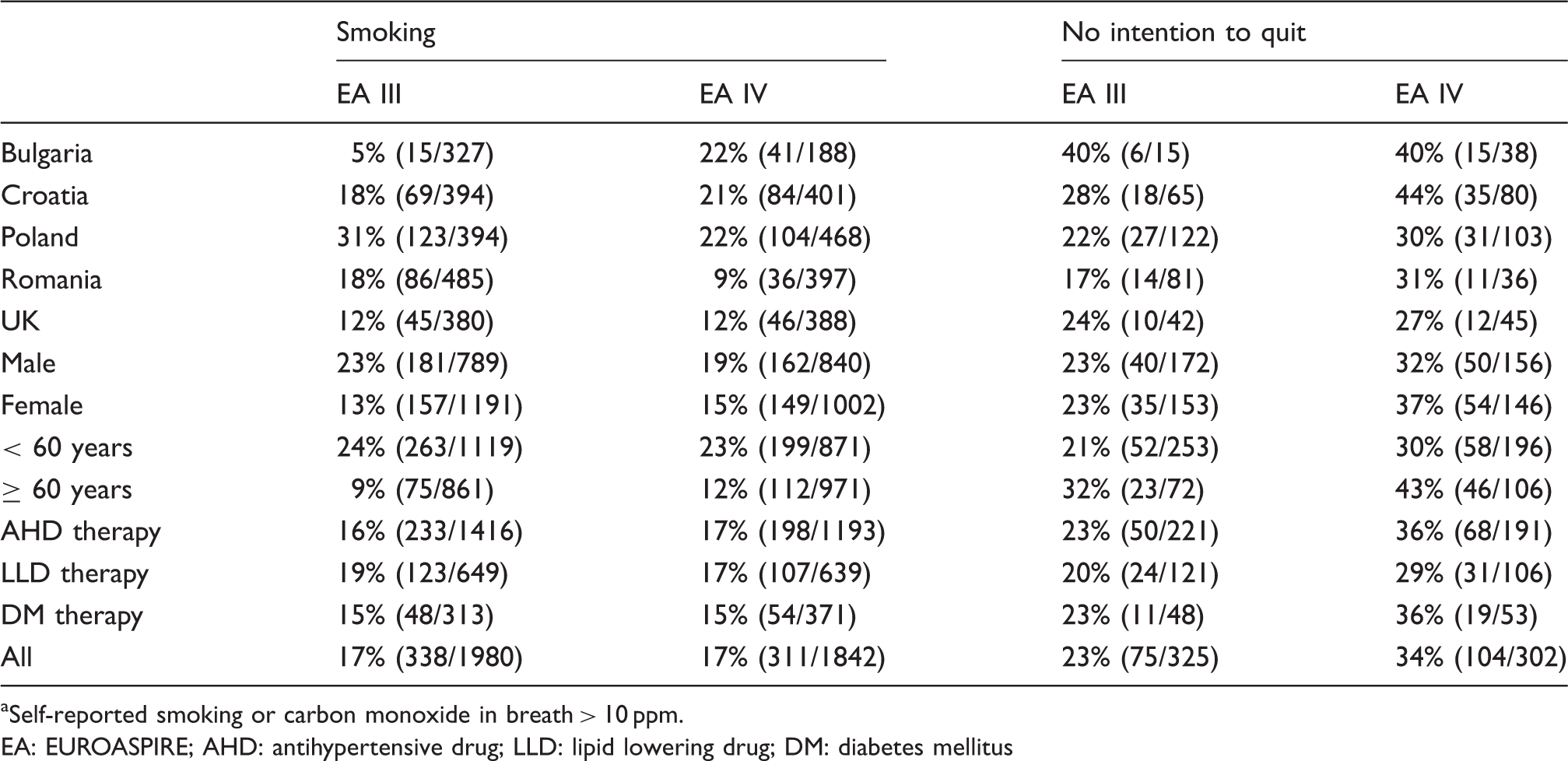
Self-reported smoking or carbon monoxide in breath > 10 ppm.
EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
The participants who were smokers at the interview were asked if they intended to quit in the coming months. The proportion without any intention to quit increased significantly (p = 0.0039) and such increase was observed in four of the five centres (Table 2).
The prevalences of overweight and obesity were high. Of the participants in both EA III and EA IV 82% had a BMI of ≥ 25 kg/m2 and respectively 44% and 43% a BMI ≥ 30 kg/m2. These prevalence rates as well as their changes differed largely between centres; for instance the prevalence of obesity was present in 65% of the participants in EA III in the centres from Bulgaria and dropped to 50% in EA IV; in contrast the prevalence of obesity was 37% in EA III in the centres from Romania and this increased to 47% in EA IV. Central obesity (waist circumference ≥88/102 cm in respectively women/men) was also frequently observed and tended to increase (59% in EA III to 62% in EA IV, p = 0.053) with large variations between centres increasing, for instance, from 57% to 65% in those in Croatia and from 47% to 58% in those in Poland.
Among participants with BMI ≥ 30 kg/m2, the proportion answering positively to questions regarding awareness and actions taken or planned.
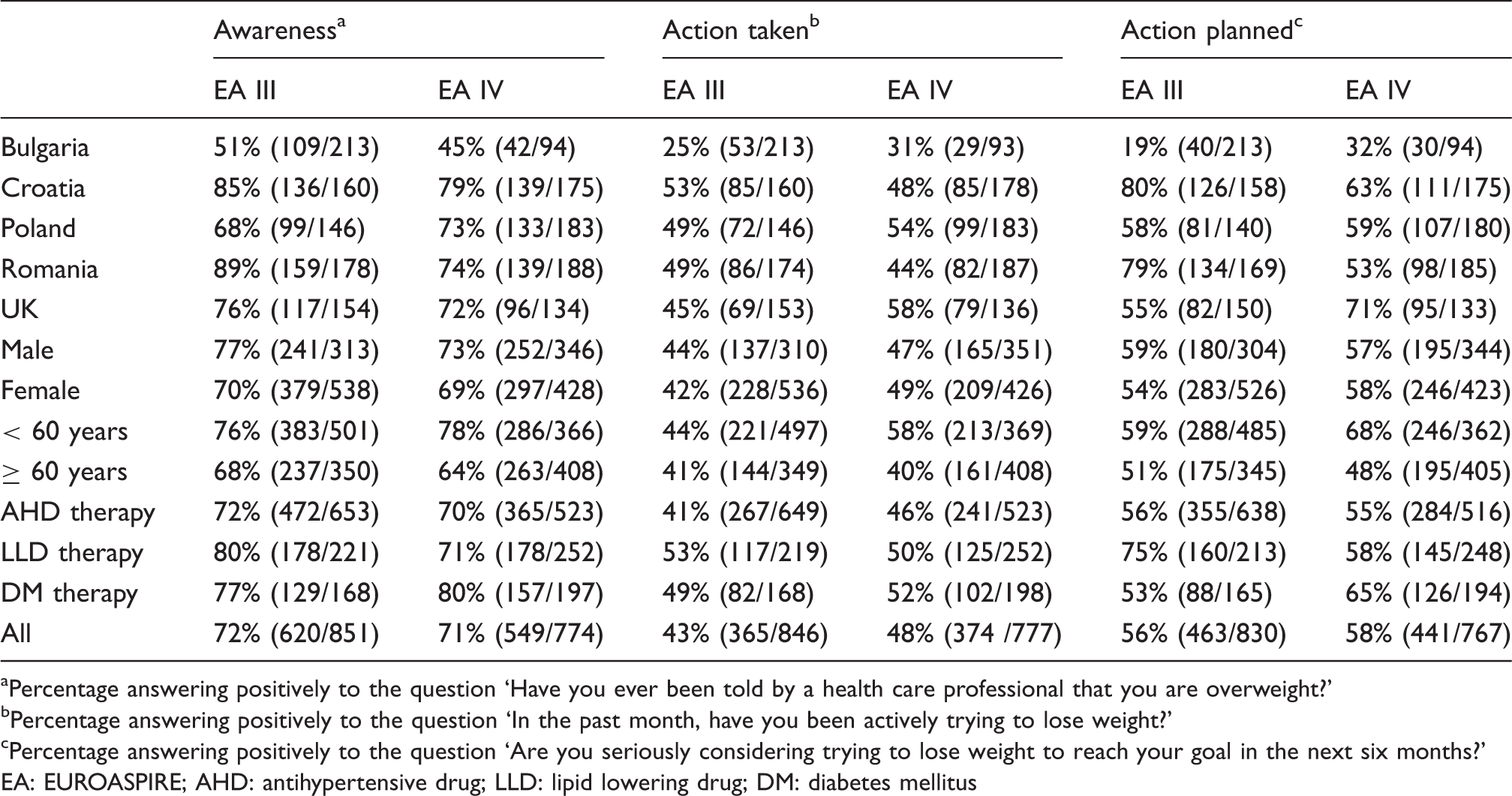
Percentage answering positively to the question ‘Have you ever been told by a health care professional that you are overweight?’
Percentage answering positively to the question ‘In the past month, have you been actively trying to lose weight?’
Percentage answering positively to the question ‘Are you seriously considering trying to lose weight to reach your goal in the next six months?’
EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
The participants in EA III and EA IV were asked: ‘Which of the following four alternatives describes your level of activity outside work in the best way? No physical activity weekly / Only light physical activity in most weeks / Vigorous physical activity at least 20 minutes once or twice a week / Vigorous physical activity for at least 20 minutes three or more times a week.’
Proportions of participants engaging in vigorous physical activity outside work for ≥ 20 min at least three times per week.
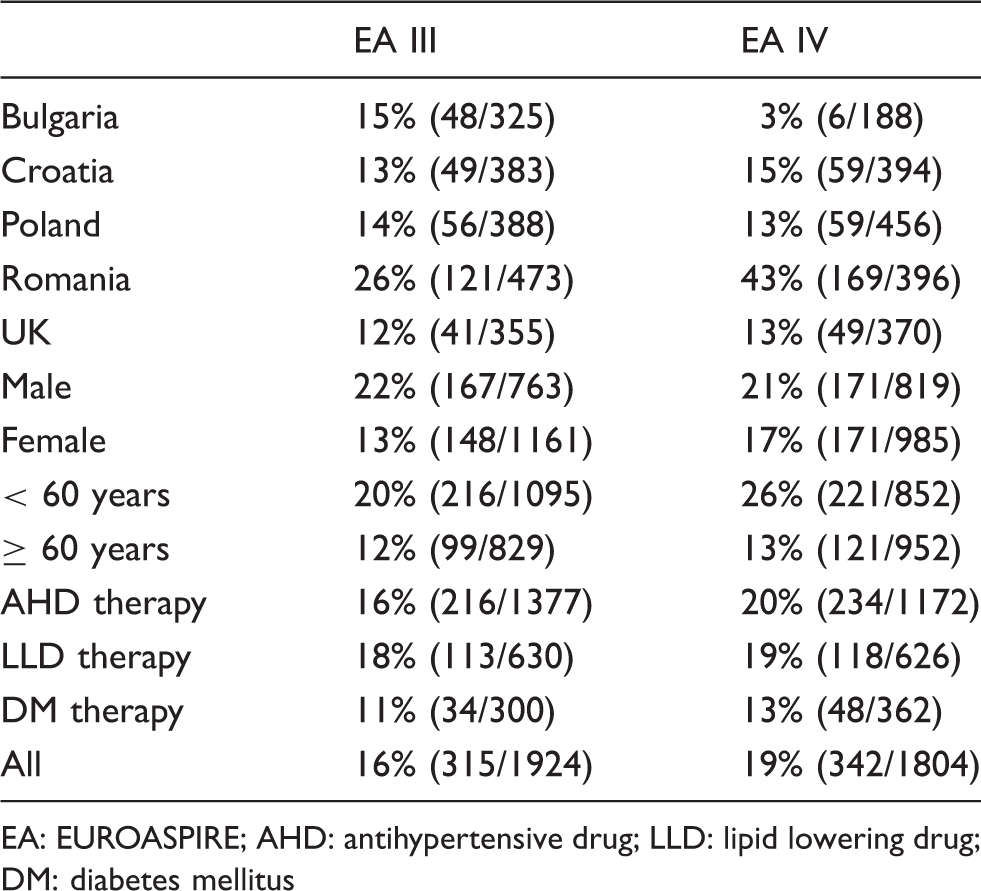
EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
Control of blood pressure.
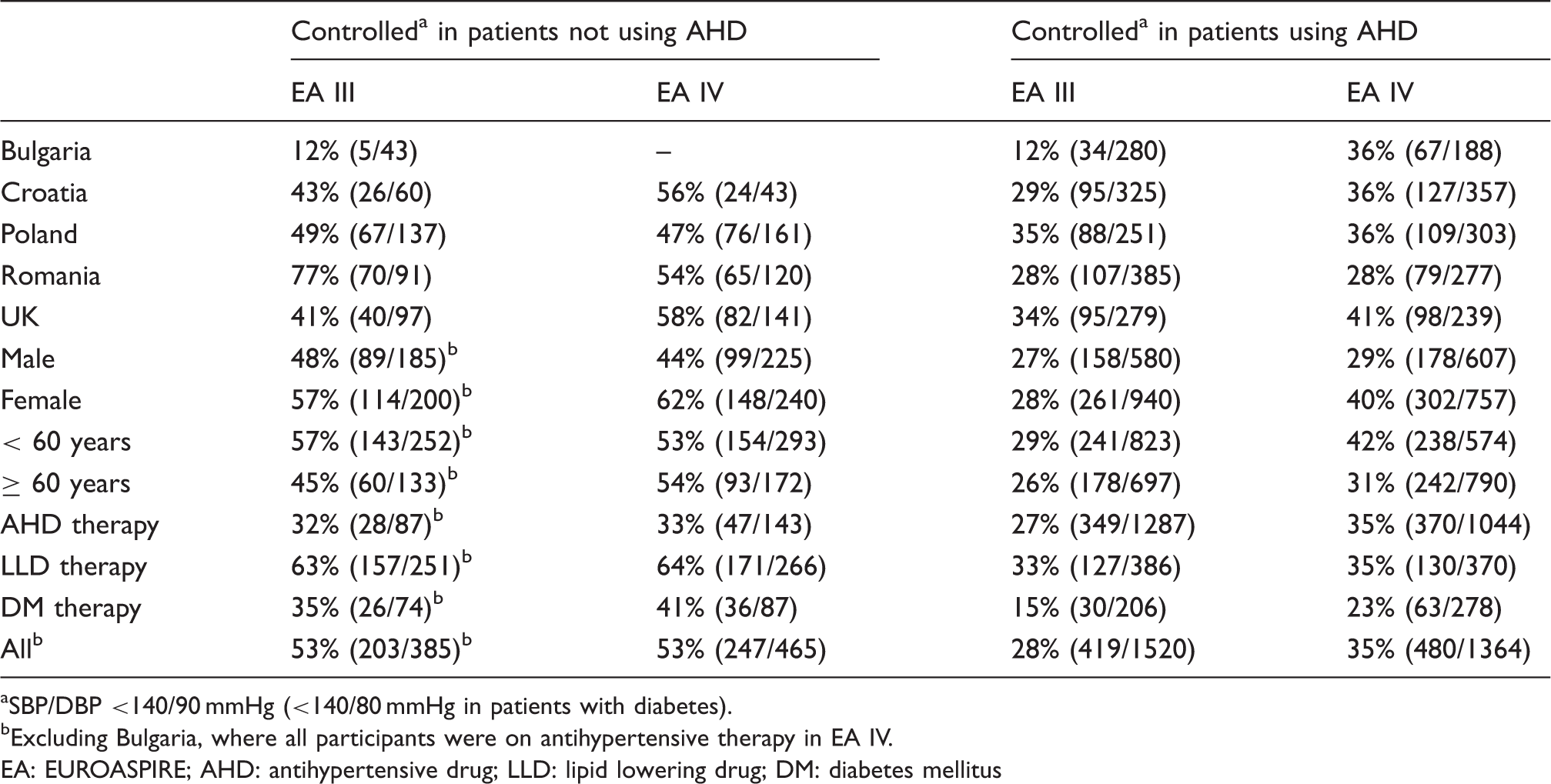
SBP/DBP <140/90 mmHg (<140/80 mmHg in patients with diabetes).
Excluding Bulgaria, where all participants were on antihypertensive therapy in EA IV.
EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
Among the participants not on lipid lowering drugs a large proportion did not reach the LDL-C target recommended for high-risk subjects in the European guidelines: 6 in men 87% and 88% had a LDL-C ≥ 2.5 mmol/l in respectively EA III and EA IV. In women these proportions were respectively 92% and 89%. These proportions were comparable in the young and the old and in all centres (results not shown).
Therapeutic control of LDL-C and diabetes.
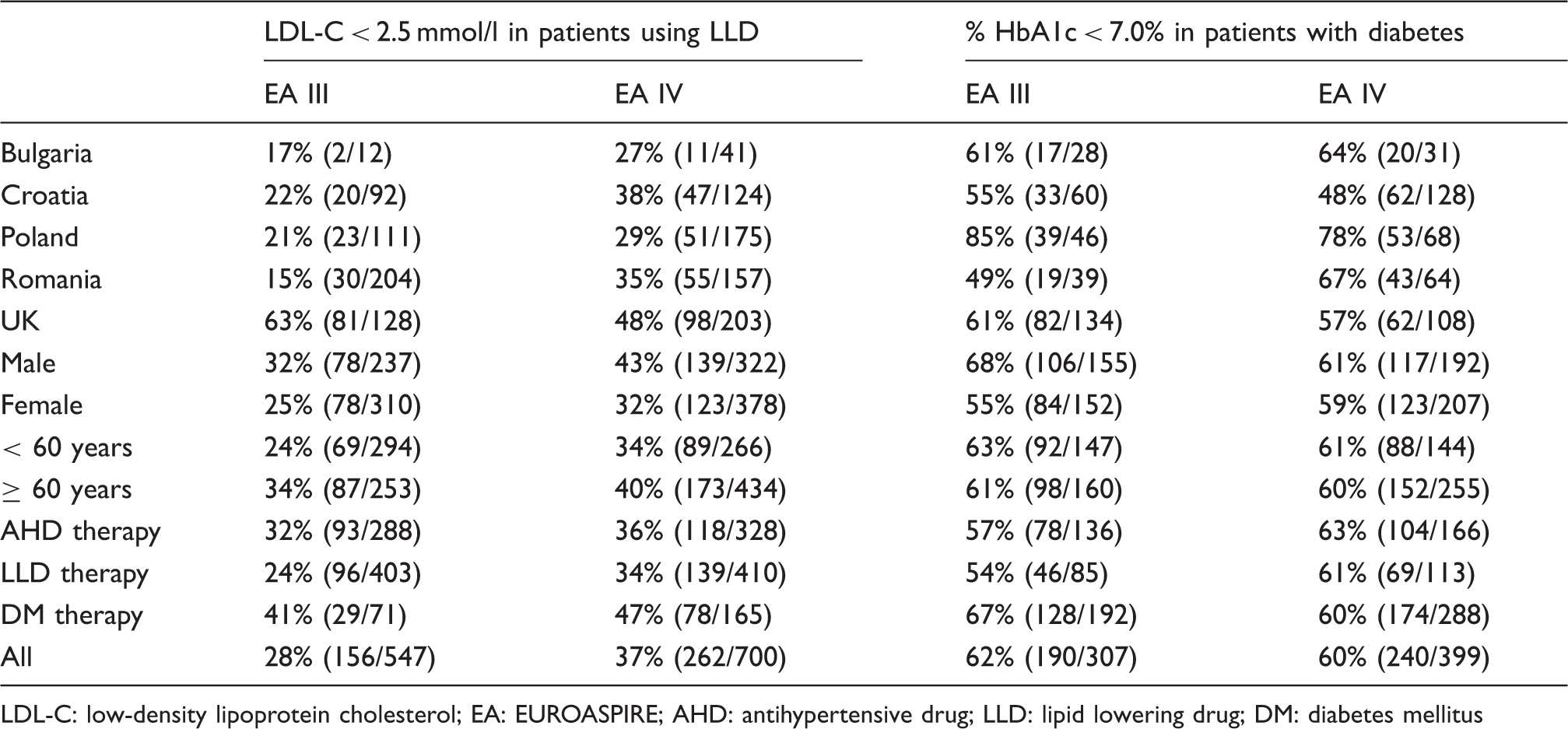
LDL-C: low-density lipoprotein cholesterol; EA: EUROASPIRE; AHD: antihypertensive drug; LLD: lipid lowering drug; DM: diabetes mellitus
In the participants not known or treated for diabetes, an elevated fasting glucose level ≥ 7 mmol/l was observed in 12% and 18% in respectively EA III and EA IV (p = 0.09). In those in whom no diabetes was reported at the visit 36% had impaired fasting glycaemia (fasting glucose ≥ 6.1 but lower than 7 mmol/l) both in EA III and in EA IV.
The therapeutic control of diabetes in the participants known and treated for diabetes is presented in Table 6. The proportion of participants with self-reported diabetes and a HbA1c of < 7% did not change significantly from EA III to EA IV (p = 0.75).
The proportions of patients achieving simultaneously a fasting glucose level of < 7 mmol/l, a blood pressure of < 140/90 mmHg (< 140/80 mmHg in patients with diabetes) and a LDL-C of < 2.5 mmol/l were 5.4% (86/1598) and 6.3% (106/1679) in respectively EA III and EA IV (p = 0.26).
Discussion
Despite impressive reductions in coronary heart disease (CHD) mortality in several European countries during the past decades, CHD remains a main cause of premature mortality, disability-adjusted life years lost and health care costs. Primary prevention of CHD is possible and therefore the actual situation remains a great challenge to public health. The major modifiable risk factors have been identified and relate to lifestyle and if needed to the use of drugs to control arterial hypertension, dyslipidaemia and diabetes mellitus. This is to our knowledge the first comparison over time regarding the implementation of primary prevention in independent samples of subjects at high CHD risk using standardized methods in comparable regions of Europe. The design and methodology of EA III and EA IV were strict and comparable; the participation rates were, however, different between the centres and over time probably in relation to differences in the application of the recruitment procedures due to varying and changing primary care health structures and organization. The centres that participated in both surveys are not necessarily representative for the countries they come from and the five countries not representative for Europe. Accordingly the results are of particular relevance for the participating centres and countries. Another limitation has to do with the large heterogeneity in the changes that occurred within and between centres; this makes the interpretation of the overall results difficult. This heterogeneity may have to do with differences between and within centres in how prevention of CVD is organized, how this is supported by the national health insurance systems and with differences in socio-economic situations that affect lifestyles and management of CVD prevention.
Given these limitations the results from EA III and EA IV clearly demonstrate that the control of the main modifiable risk factors was and remains poor.
Nearly 25 years after the introduction of Joint European Societies’ guidelines on CVD prevention in clinical practice, no significant change was seen over a period of eight years in the prevalence of smoking, physical inactivity, overweight and obesity, with more than 80% of persons at high cardiovascular risk being overweight or obese. The proportion of the smokers who intend to quit even decreased significantly and only half of the obese persons had tried or had the intention to lose weight. Particularly frustrating is the decrease of the smokers who intend to quit considering all the efforts invested in smoking cessation in Europe. 13
The 2012 Joint European Societies’ guidelines on CVD prevention in clinical practice recommend that healthy adults of all ages should spend 1–2.5 h/week on vigorous intense exercise. 6 Similar recommendation is based upon all available data given by the European Association for Cardiovascular Prevention and Rehabilitation. 14
In all day practice, as reflected in this survey, less than one in five of the participants exercises regularly in accordance with this recommendation without any change over time. Finally there were no improvements in the control of elevated blood pressure, LDL-C and diabetes. However, it should be emphasized that a large heterogeneity was found in all these results between participating centres.
Similar findings were reported from the EURIKA study, carried out in 2009 in 12 European countries among 7641 individuals aged ≥50 years with at least one cardiovascular risk factor but free of CVD. In that study only 39% of the participants treated for hypertension achieved a target of <140/90 mmHg (<130/80 mmHg if diabetes) and a between countries range of 32.1–47.5%. 15 With a less stringent goal for blood pressure at <140/80 mmHg for the participants with diabetes, the EA IV results are even worse, with only 35% below target and a range between centres of 29–41%. The change over time is overall not significant, but this may be due to the large heterogeneity between centres. There were, however, indications that in some instances treatment of subjects with hypertension could be improved more than in others by either combination therapies and/or improvements in drug combination choices and in the doses of medications used.
In EURIKA the participants treated with lipid lowering drugs had a total cholesterol <5 mmol/l and a LDL-C <3 mmol/l (<2.5 mmol/l if diabetes) in 41.2% (between countries range 24.3–68.4%). Using a unique goal for LDL-C at <2.5 mmol/l the results in EA IV compared with EA III improved in all centres except in the UK where, despite a drop, the proportion of subjects at goal is still the highest in EA IV. In the Irish Longitudinal Study of Ageing statins were used in only 19.7% of the participants aged 50–64 years, free of diabetes and CVD but with a Systematic COronary Risk Evaluation risk of ≥5%/10 years; 16 in only 15% of them the LDL-C target of < 2.5 mmol/l was reached.
In EURIKA control of diabetes was defined as a HbA1c of <6.5% and 36.7% of the patients with diabetes achieved that goal (between countries range 23.4–48.4%). With the HbA1c target now at <7.0% the proportion achieving that goal in EA IV is better (60%) but not improved compared with EA III and the differences between the centres are again substantial.
The between-centres variation in attainment of treatment targets may be due to differences in clinical and socio-economic characteristics of the participants, in adherence to CVD prevention guidelines and in healthcare systems between countries. The wide range of drug treatments used across countries suggests important differences in drug prescription policies or market penetration. 17
Among the participants selected in the study because of treated arterial hypertension a large proportion also had elevated LDL-C. Similarly among those treated for dyslipidaemia a large proportion also had elevated blood pressure. This seems to indicate that clinicians still think in a unifactorial way about prevention although it has been clearly shown that CVD is multifactorial in origin and elevated blood pressure and dyslipidaemia have been linked to each other in several studies.18-20 Thus, despite effective control of one risk factor, multifactorial lifestyle measures are clearly needed to address the level of residual risk that exists in most of these persons. This is even more important in the presence of diabetes and its pre-state impaired glucose tolerance.
Regarding gender differences in changes over time in the control of risk factors it seems that in women hypertension became less undetected and better controlled, that the control of elevated LDL-C has improved but less than in men and that the control of diabetes did improve slightly while it fell back in EA IV in men.
The control of hypertension and of dyslipidaemia changed more favourably in the participants aged <60 years compared with those who were older.
Given these results there is a clear demand to improve the implementation of what is recommended in the European Society of Cardiology prevention guidelines; this requires actions at the level of different domains that were identified in a systematic review on the subject: guidelines related factors, individual health professional factors, patient factors, professional interactions, incentives and resources, capacity for organizational change and social, political and legal factors. 21 All this has to be developed at the level of the community in consideration of the large socio-economic and cultural diversities between European countries.
Footnotes
Acknowledgements
The primary care arms of the EA III and IV surveys were carried out under the auspices of the European Society of Cardiology, Euro Heart Survey (EUROASPIRE III) and EURObservational Research Programme (EUROASPIRE IV). The EUROASPIRE Study Group is grateful to the administrative staff, physicians, nurses and other personnel in the primary care practices in which the survey was carried out and to all patients who participated in the surveys. The sponsors of the EUROASPIRE surveys had no role in the design, data collection, data analysis, data interpretation, decision to publish, or writing the manuscript. Members of EUROASPIRE other than the authors are listed in Appendix 1.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ZR received honoraria for lectures and advisory boards from Amgen, Sanofi and Synageva. GDB, DDB, LR, DG, BG, NG, SM, DM and DW have no interests to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AP declares that the Polish part of the study was supported by the grants of Polish Ministry of Science and High Education (project No: 2 P05D 008 30 and Polish National Science Committee (contract: DEC 2011/03/B/NZ7/06101). KK had grant support from the European Society of Cardiology for the submitted work. The following companies have supported the EUROASPIRE III programme: AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Merck/Schering-Plough, Novartis, Pfizer, Sanofi-Aventis, Servier; and the EUROASPIRE IV programme: Amgen, AstraZeneca, Bristol-Myers Squibb and AstraZeneca, F Hoffman-La Roche, GlaxoSmithKline, and Merck Sharp & Dohme.