
Abstract
Background
Chronic aerobic exercise training is associated with improved endothelial function and arterial stiffness and favourable long-term cardiovascular effects.
Design
We investigated the acute effects of continuous moderate intensity aerobic exercise (CAE) and high intensity interval aerobic exercise (hIAE) on endothelial function and arterial stiffness in healthy participants.
Methods
Twenty healthy men were recruited to this cross-over study. They participated in two exercise sessions: (a) CAE, volume at 50% of maximum aerobic work for 30 minutes; and (b) hIAE, interval maximum aerobic work for 30 minutes. Endothelial function was evaluated by flow-mediated dilation in the brachial artery. The carotid femoral pulse wave velocity and the femoral dorsalis pedis pulse wave velocity were measured as indices of central aortic and peripheral arterial stiffness. Measurements were carried out before and immediately after each exercise session.
Results
There was no statistically significant difference in the baseline measurements before CAE and hIAE with respect to flow-mediated dilation, the carotid femoral pulse wave velocity and the femoral dorsalis pedis pulse wave velocity (p = NS). Both CAE and hIAE significantly improved the flow-mediated dilation compared with baseline (p < 0.001). Similarly, the femoral dorsalis pedis pulse wave velocity was improved after CAE and hIAE (p < 0.005), whereas the carotid femoral pulse wave velocity was not significantly affected (p = NS).
Conclusion
Both CAE and hIAE can favourably affect endothelial function, suggesting another cardioprotective effect of acute exercise. These types of aerobic exercise have a different impact on the central and peripheral arterial stiffness.
Keywords
Introduction
Endothelial function is a key regulator of the elastic properties of large vessels and an impaired endothelium is associated with unfavourable cardiovascular outcomes. 1 Increased large-artery stiffness is associated with problems in left ventricular function 2 and coronary blood flow. 3 The mechanical integrity of arteries has been identified as a marker of cardiovascular disease and as an independent prognostic marker of cardiovascular risk. 4
Physical inactivity is associated with increased oxidative stress, endothelial dysfunction and atherosclerosis, whereas physical training and aerobic capacity are associated with a low risk of cardiovascular disease and mortality.5–9 Aerobic exercise is therefore strongly recommended for both healthy people and for patients with cardiovascular disease to improve cardiovascular health and reduce the risk of premature death.6,10 However, recent clinical and epidemiological studies have shown that the beneficial effects of regular physical exercise depend on the volume or quantity of work carried out during exercise.10–12
If the total energy expenditure of exercise is maintained at a constant level, then exercise carried out at higher relative intensities has been found to induce larger increases in aerobic capacity and greater cardioprotective effects than exercise at moderate intensities.13,14 However, vigorous activity can also acutely and transiently increase the risk of sudden cardiac death and myocardial infarction in susceptible people. 15
The acute effects of aerobic exercise have received less attention and the reported results are conflicting. We investigated the acute effects of continuous moderate intensity aerobic exercise (CAE) and high intensity interval aerobic exercise (hIAE) on endothelial function and arterial stiffness in healthy participants.
Methods
Participants
Twenty healthy young men (mean ± SD age 22.6 ± 3.3 years) were recruited to this cross-over study. The characteristics of the participants are presented in Supplementary Table 1, available online. All the participants were non-smokers with no cardiovascular risk factor nor cardiovascular disease.
The exclusion criteria included any acute inflammatory, infectious or chronic disease, orthopaedic and/or neurological limitations to exercise, surgery during the intervention period or participation in another research study. None of the participants was taking any regular cardiovascular drugs (or growth hormone), antioxidant vitamin supplements, anti-inflammatory drugs or steroids.
Study design
Seven days before the first exercise session, the maximum aerobic work on a cycle ergometer was determined for the participants. Each of the 20 participants took part in two sessions (hIAE and CAE) with an interval of one week between each session. The participants were randomized to start with either an hIAE or CAE session; the participants who started with the hIAE session took part in a CAE session one week later and vice versa.
All participants attended after fasting at the same time (9 am) on the morning of each experimental session. They had avoided any intense physical activity for the previous 48 hours. The participants also refrained from caffeine and alcohol for 24 hours before each experimental session. All interventions and measurements were preceded by a preliminary period of >15 minutes of rest in a supine position in a quiet, darkened, temperature-controlled room at 22℃. The endothelial function and pulse wave velocity were evaluated with the participants resting in a supine position.
Endothelial function was evaluated before and immediately after each exercise session. Measurements of arterial stiffness with the pulse wave velocity were carried out before and 10 minutes after each exercise session. We choose a 10-minute time period because previous research has shown that exercise substantially alters arterial stiffness 10 minutes after the end of an exercise session. 16
Bioethics
All participants were informed about the aims of the study and gave their written informed consent. The study was approved by the local ethics committee of our institution and was carried out in accordance with the Declaration of Helsinki 1989.
Maximum aerobic work
Maximum aerobic work was measured one week before the first exercise session using a cycle ergometer (Cateye Ergociser, EC-3200, Cat Eye Co. Ltd, Osaka, Japan) and a graded cycle ergometer protocol during the morning. The aerobic capacity test was based on the adjusted YMCA Cycle Ergometer Protocol. 17 Participants started to cycle at 25 W at 50 revolutions per minute and every three minutes the resistance was increased by 25 W until the participants could no longer maintain the pedal cadence (the increase in resistance in the second three-minute stage was dependent on the first-stage heart rate 17 ). When the test was completed, the work resistance was gradually decreased and the participants continued pedalling for three to five minutes to prevent venous pooling.
Exercise sessions
Both hIAE and CAE were performed on the same cycle ergometer and started with a three-minute warm-up without loading. In the hIAE session, this was followed by 30 bouts of 30 seconds duration each at an intensity of 100% of the maximum aerobic work capacity, as measured during the maximum aerobic capacity test. A passive rest period of 30 seconds was allowed between bouts. To achieve an isocaloric protocol, the CAE involved continuously cycling for 30 minutes on the same cycle ergometer at 50% of the maximum aerobic work capacity. An isocaloric protocol was selected to generate a comparable total work load and energy expenditure between the hIAE and CAE sessions. The energy expenditure during cycling on a cycle ergometer is dictated by the mechanical power achieved. 18 The mechanical power in the hIAE session was double that in the CAE session, but the CAE session was twice as long (hIAE = 227.5 ± 44.8 W for 15 minutes; CAE = 113.7 ± 22.4 W for 30 minutes), which suggests an equal energy expenditure between protocols. These exercise protocols have been used before with the same reasoning. 19
Evaluation of endothelial function
The endothelial function was evaluated by estimating the flow-mediated dilation (FMD) in the brachial artery using a linear array ultrasound transducer as described previously. 20
Evaluation of central aortic and peripheral arterial elastic properties
The carotid femoral pulse wave velocity (cfPWV), an index of aortic stiffness, was calculated from measurements of the pulse transit time and the distance travelled between two recording sites (PWV = distance in metres divided by transit time in seconds) using a well-validated non-invasive device (SphygmoCor, AtCor Medical, Sydney, Australia), which allows online pulse wave recording and the automatic calculation of the PWV. 21
The femoral dorsalis pedis PWV (fdPWV), which is considered to be an index of peripheral arterial stiffness, was calculated from measurements of the pulse transit time and the distance travelled between two recording sites using the SphygmoCor system. Two different pulse waves were obtained simultaneously at two sites (over the right femoral artery and over the right dorsalis pedis artery). The distance was defined as the distance from the suprasternic notch to the dorsalis pedis artery minus the distance from the femoral artery to the suprasternic notch.
Statistical analysis
All variables were tested for a normal distribution of the data. Normally distributed data were expressed as mean ± SD values. To calculate the net increase in FMD, we subtracted the values before exercise from the values after exercise. To calculate the net improvement in cfPWV and fdPWV, we subtracted the values after exercise from the values before exercise. A paired sample t-test was used to test for intra- and inter-group differences between the means of normally distributed continuous variables. The Pearson correlation coefficient was used to test for correlations between normally distributed data. Exact values of p < 0.05 were considered to be statistically significant. All statistical calculations were performed using SPSS software (version 18.0; SPSS Inc, Chicago, IL, USA).
Results
Baseline measurements
There was no significant difference in baseline measurements before the CAE and hIAE sessions, as shown in Supplementary Table 2, available online.
Impact of different types of aerobic exercise on endothelial function
Supplementary Table 2, available online, shows that the FMD at baseline did not differ between the CAE and hIAE sessions. Compared with the baseline measurements, the FMD after the CAE and hIAE sessions was significantly improved (6.37 ± 1.48 vs. 8.57 ± 2.55%, p < 0.001 and 5.95 ± 1.78 vs. 8.48 ± 2.60%, p < 0.001, respectively) (Figure 1a and 1b). To assess whether the different types of exercise (CAE vs. hIAE) had different effects on the improvement in endothelial function, we calculated the net improvement in the FMD in the CAE and hIAE groups by subtracting the FMD at baseline from the FMD after exercise in each group. The CAE sessions resulted in a net improvement in the FMD of 2.19 ± 1.78% and the hIAE sessions resulted in a net improvement in the FMD of 2.53 ± 1.52%. There was no significant difference between the two types of exercise as shown by the paired t-test (p = 0.36) (Figure 1c). We examined the effect of the baseline arterial pressure on the improvement in the FMD. Supplementary Table 3, available online, shows that the baseline arterial pressure was not associated with a change in the FMD.
Box plots of flow-mediated dilation expressed as percentages. (a) Change in flow-mediated dilation (FMD) before and after continuous moderate intensity aerobic exercise (CAE). (b) Change in FMD before and after high intensity interval aerobic exercise (hIAE). (c) Change in FMD after CAE and after hIAE. Boxes represent interquartile range and the black line across the boxes represents the median value.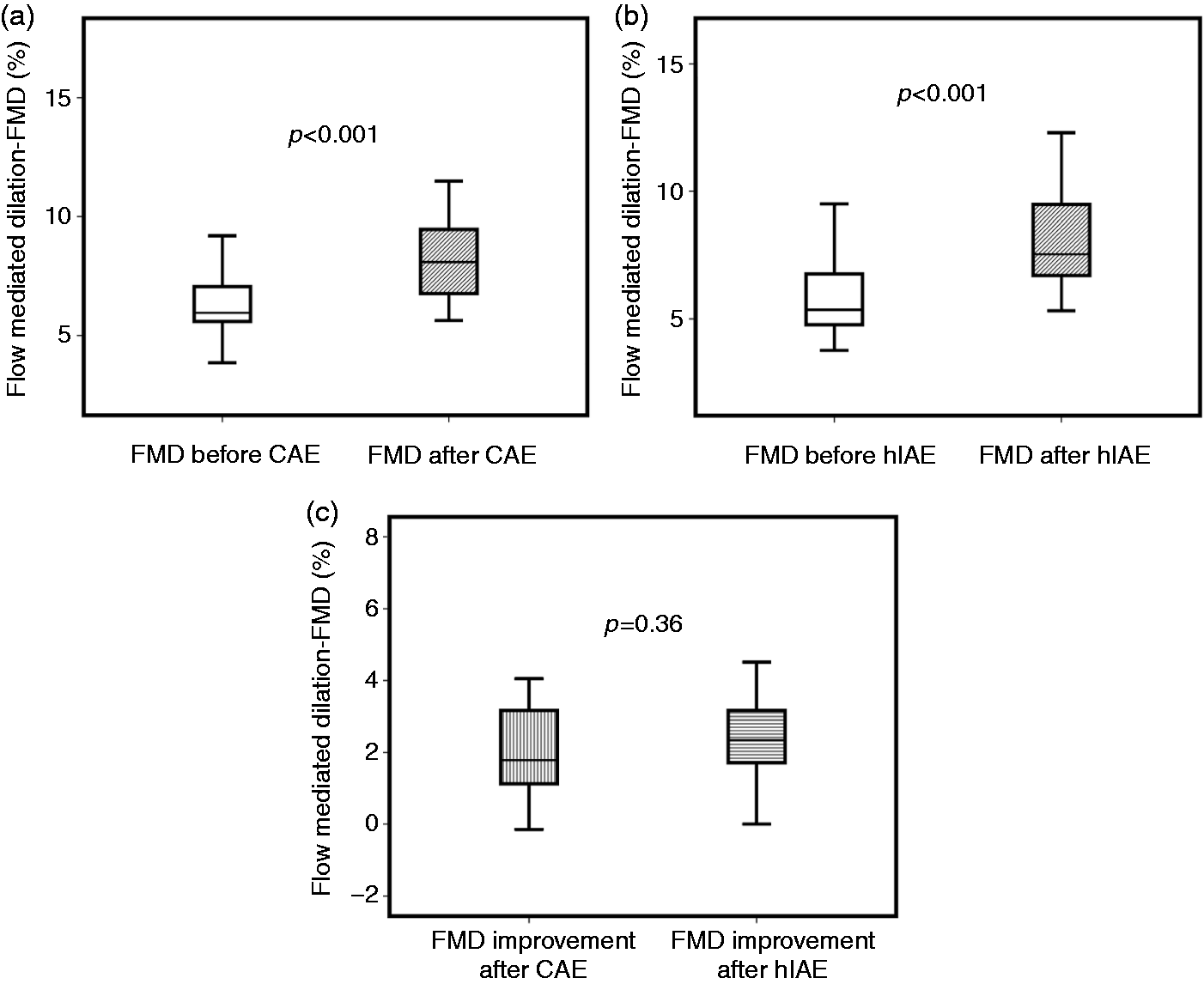
Impact of different types of aerobic exercise on arterial stiffness and pulse wave velocity
Carotid femoral pulse wave velocity
Supplementary Table 2, available online, shows that the cfPWV at baseline did not differ between the CAE and hIAE sessions. Compared with the baseline, the cfPWV was not significantly improved after the CAE sessions (5.87 ± 0.82 vs. 5.76 ± 0.63 m·s–1, p = 0.27) nor after the hIAE sessions (5.87 ± 0.67 vs. 5.80 ± 0.57 m·s–1, p = 0.40) (Figure 2a and 2b). There was no association of the improvement in the FMD after the CAE and hIAE sessions with changes in the cfPWV (Supplementary Table 4, available online). We examined the effect of the baseline arterial pressure in the changes in the cfPWV. Supplementary Table 3, available online, shows that the baseline arterial pressure was not associated with a change in the cfPWV.
Box plots of carotid femoral pulse wave velocity (cfPWV) expressed in m s–1. (a) cfPWV before and after continuous moderate intensity aerobic exercise (CAE). (b) cfPWV before and after high intensity interval aerobic exercise (hIAE). Boxes represent interquartile range and black line across the boxes represents the median value.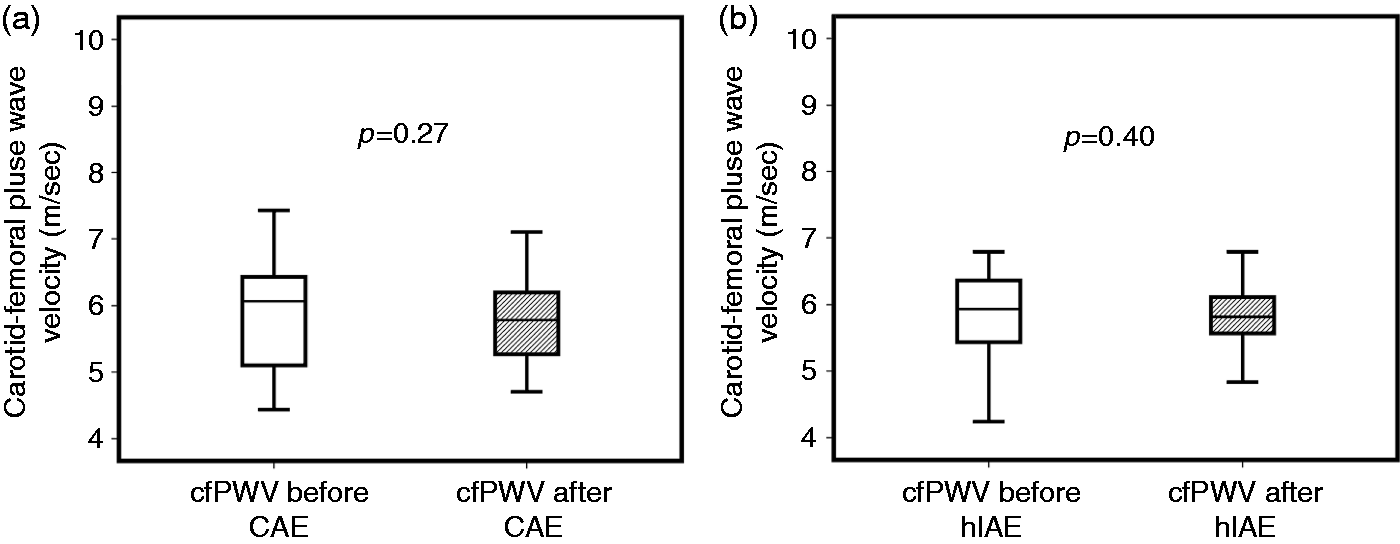
Femoral dorsalis pedis pulse wave velocity
Supplementary Table 2, available online, shows that the fdPWV at baseline did not differ between the CAE and hIAE sessions. Compared with the baseline, the fdPWV was significantly improved after the CAE sessions (9.27 ± 1.11 vs. 8.17 ± 1.48 m·s–1, p = 0.003) and after the hIAE sessions (9.14 ± 1.07 vs. 8.26 ± 0.8 m·s–1, p < 0.001) (Figure 3a and 3b). To assess whether the different types of exercise (CAE vs. hIAE) had a different effect on the improvements in the peripheral arterial stiffness, we calculated the net improvement in the fdPWV in the groups of CAE and hIAE by subtracting the fdPWV after exercise from the baseline fdPWV in each group.
Box plots of femoral dorsalis pedis pulse wave velocity (fdPWV) expressed in m s–1. (a) Change in fdPWV before and after, continuous moderate intensity aerobic exercise (CAE). (b) Change in fdPWV before and after high intensity interval aerobic exercise (hIAE). (c) Change in fdPWV after CAE and after hIAE. Boxes represent interquartile range and black line across the boxes represents the median value.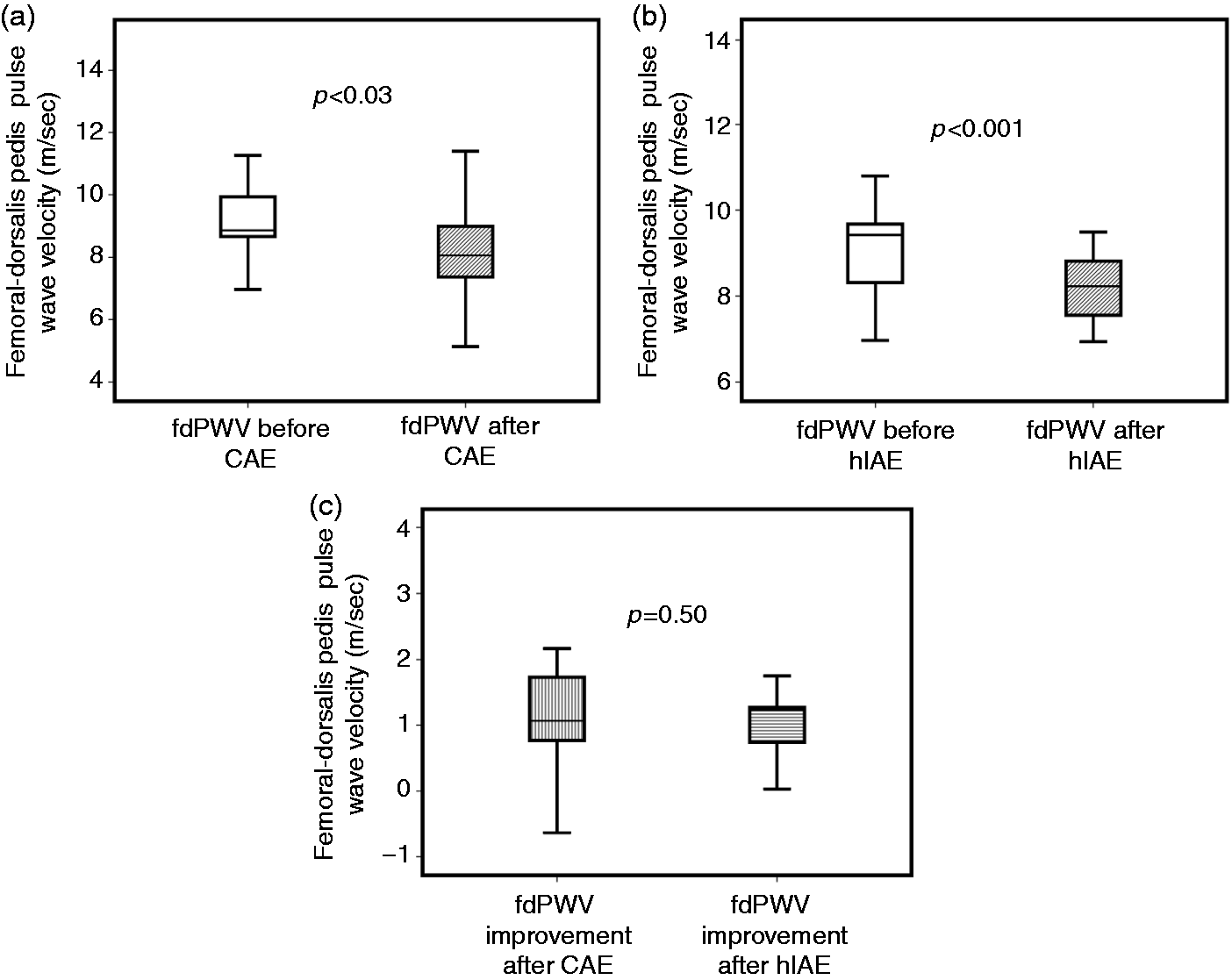
The CAE sessions resulted in a net improvement in the fdPWV of 1.10 ± 1.08 m·s–1 and the hIAE sessions resulted in a net improvement in the fdPWV of 0.89 ± 0.67 m·s–1. There was no significant difference between the two types of exercise using the paired t-test (p = 0.50) (Figure 3c).
The improvement in the FMD after the CAE sessions was significantly associated with the improvement in the fdPWV (r = –0.48, p = 0.04) (Supplementary Table 4, available online). However, the association between the improvement in the FMD and the fdPWV after the hIAE sessions did not reach statistical significance (Supplementary Table 4, available online). We examined the effect of the baseline arterial pressure on the improvement of fdPWV. Supplementary Table 3, available online, shows that the baseline arterial pressure was not associated with a change in the fdPWV.
Impact of different types of aerobic exercise on heart rate and blood pressure
We measured blood pressure and heart rate 10 minutes after the exercise sessions at the same time as the measurements of arterial stiffness. The differences between blood pressure and heart rate after the CAE and hIAE sessions are shown in Supplementary Table 5, available online, which shows that, although there was no difference in blood pressure after exercise, the heart rate of the participants was significantly increased after exercise.
Discussion
The rationale of this study was to evaluate the acute effects of CAE and hIAE sessions on endothelial function and arterial stiffness in healthy participants. We also compared the potentially different effect of these different types of aerobic exercise on endothelial function and arterial stiffness. Our results showed that, immediately after exercise, both types of exercise can favourably affect the endothelial function and peripheral arterial stiffness.
Acute impact of aerobic exercise on endothelial function
Both the CAE and hIAE sessions resulted in a significant improvement in the FMD compared with the baseline measurements, with no significant difference between the two types of exercise. In agreement with our findings, it has previously been shown that the intensity of aerobic exercise does not influence the FMD response. 22 Previous studies, however, included continuous high intensity aerobic exercise, not interval sessions as studied in this work. In contrast with our observations, Tyldum et al. 23 showed a greater improvement in the FMD after an hIAE session than after a CAE session. This could be explained by the different type of aerobic exercise (treadmill) used and the different intensities preferred.
The mechanisms by which aerobic exercise might influence endothelial function are multiple and complex. In the acute setting, it is suggested that exercise training increases blood flow and shear stress and therefore stimulates endothelial nitric oxide production.24,25 This is mainly achieved by increasing the phosphorylation of endothelial nitric oxide synthase.26,27 Adhesion molecules such as platelet endothelial cell adhesion molecule-1 and tyrosine kinase vascular endothelial growth factor receptor, which activate phophoinositide-3 kinase, can mediate endothelial nitric oxide synthase adaptations in exercise and shear stress. 28 The deformation of the endothelial glycocalyx by increased luminal forces, which allows direct signalling, is also important. 27
With respect to chronic adaptations to exercise, it is also possible that acute aerobic exercise increases reactive oxygen species, which may induce favourable endothelial adaptations, including the increased expression of superoxide dismutase and endothelial nitric oxide synthase. 29 Vascular endothelial growth factor receptor 2 and nuclear factor-κB have key roles in these biochemical pathways.26,27 Thus it is possible that the effects of acute exercise on the FMD reflect a combination of haemodynamic changes and nitric oxide endothelium-dependent mechanisms. 30
Acute impact of aerobic exercise on central and peripheral arterial stiffness
In this study, the CAE and hIAE sessions did not affect the cfPWV relative to the baseline measurements. Ranadive et al. 16 also found that there was no change in the cfPWV after maximum leg aerobic exercise. In contrast, Kingwell et al. 31 showed a reduction in the cfPWV after a single bout of moderate intensity cycling. This result occurred 30 minutes after exercise. Given that we measured the cfPWV 10 minutes after exercise, these conflicting findings could be attributed to the different times that the measurements were taken after exercise. Exercise stress tests resulted in an early increase in the cfPWV. 32
We also found that both the CAE and hIAE sessions significantly improved the fdPWV. Several previous studies agree with this finding, suggesting that decreased arterial stiffness should be expected to be induced in exercised limbs.16,32,33 As arterial stiffness is determined by both the properties of the arterial wall matrix and the vascular smooth muscle tone, an acute change in the arterial stiffness of the exercised limbs is probably mediated by an alteration in the vascular muscle tone with exercise, which is considered to be mainly induced by exercise-related regional factors, such as endothelium-derived hyperpolarizing factor.
34
Prostacyclin may induce the post-exercise decrease in arterial stiffness, given that its production, enhanced by an increase in shear stress in the regional vessels, attenuates neurogenic and myogenic vasoconstriction.
35
An increased shear stress can activate calcium ion channels and phospholipase activation, leading to the release of prostaglandin I2 and cAMP smooth muscle cell relaxation.
36
The observed changes in regional arterial stiffness seem to be independent of nitric oxide production because systemic nitric oxide synthase inhibition by the intravenous administration of NG-monomethyl-
In line with this evidence, Bia et al. 32 concluded that the alteration in regional arterial stiffness after an exercise stress test cannot by explained by blood pressure variations alone. It has been shown that a series of regional factors may account for the difference in the FMD reaction in the brachial and femoral arteries 39 and that the shear stress after cycling may significantly increase the diameter of the femoral artery compared with the diameter of the brachial artery, which may account for the observed difference in arterial stiffness and PWV.40,41 A recent meta-analysis focusing on studies of aerobic exercise concluded that the improvement in the brachial ankle PWV was based mainly on the improvement in the peripheral arterial stiffness and PWV. This was attributed to the greater shear stress enhanced release of nitric oxide in the peripheral exercising limbs and the nitric oxide production in small conduit arteries. 42 Similar results for central and peripheral arterial stiffness have been observed after acute resistance exercise, 43 which were also attributed to vasodilation of the exercising muscle beds. 31
Limitations
The primary purpose of this study was to investigate the acute effects of CAE and hIAE sessions on endothelial function and arterial stiffness in young healthy participants. Future studies are needed to explore the chronic vascular and metabolic effects of different types of aerobic exercise in older participants with cardiovascular risk factors.
Conclusion
CAE and hIAE sessions can favourably affect endothelial function in young healthy adults, suggesting another cardioprotective effect of exercise on the progression of atherosclerosis. These types of aerobic exercise have different effects on the central and peripheral arterial stiffness. Further studies are needed to elucidate the long-term impact of different types of aerobic exercise on cardiovascular health.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first two authors (G.S. and D.A.) contributed equally to this study. Gerasimos Siasos received a scholarship from the George D. Behrakis Research Fellowship Program. This scholarship had no involvement in the study design, in the data analysis, in the writing of the manuscript and in the decision to submit the article for publication. None of all the other authors have anything to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.