
Abstract
Background
Most exercise-related cardiac arrests in men aged ≥45 years are due to coronary artery disease (CAD). The current sports medical evaluation (SME) of middle-aged sportsmen includes medical history, physical examination and resting and exercise electrocardiography (ECG). We investigated the added value of low-dose cardiac computed tomography (CCT) – both non-contrast CT for coronary artery calcium scoring (CACS) and contrast-enhanced coronary CT angiography (CCTA) – in order to detect occult CAD in asymptomatic recreational sportsmen aged ≥45 years without known cardiovascular disease.
Methods
Following a normal SME (with resting and bicycle exercise ECG), 318 asymptomatic sportsmen underwent CCT and 300 (94%) had a low European Society of Cardiology Systematic Coronary Risk Evaluation (SCORE) risk. Occult CAD was defined as a CACS ≥100 Agatston units (AU) or obstructive (≥50%) luminal stenosis on CCTA. The number needed to screen (NNS) in order to prevent one cardiovascular event within 5 years with statin treatment was estimated.
Results
Fifty-two (16.4%, 95% confidence interval (CI): 12.7–20.8%) of 318 participants had a CACS ≥100 AU. The CCTA identified an additional eight participants with luminal narrowing ≥50% (and a CACS <100 AU). Taken together, CCT identified CAD in 60 (18.9%, 95% CI: 14.9–23.5%) of 318 participants. The 5-year estimated NNS was 183 (95% CI: 144–236) for CACS and 159 (95% CI: 128–201) for CACS combined with CCTA.
Conclusions
Coronary CT detects occult CAD in almost one in five asymptomatic sportsmen aged ≥45 years after a normal SME that included resting and bicycle exercise ECG. CACS reveals most of the relevant CAD with limited additional value of contrast-enhanced CCTA. The NNS in order to prevent one cardiovascular event compares favourably to that of other screening tests.
Keywords
Introduction
Sudden cardiac death is often the first manifestation of coronary artery disease (CAD). Regular physical exercise is recommended in order to reduce cardiovascular morbidity and mortality and is gaining popularity in the middle-aged.1–3 However, exercise transiently increases the risk of cardiovascular events, particularly in those with unknown cardiac disease. 4 More than 90% of exercise-related cardiac events occur in men, predominantly those aged 45 years and over, and these are mainly attributed to CAD.5,6 It follows that the main goal of the cardiovascular evaluation of older athletes is ruling out significant occult CAD. 2 The European Society of Cardiology (ESC) position paper on the cardiovascular evaluation of middle-aged/senior individuals engaged in leisure time sports activities advocates the use of maximal exercise testing. 7 This is now frequently performed in a sports medical examination (SME), in addition to medical history, physical examination, ESC Systematic Coronary Risk Evaluation (SCORE) risk calculation and resting electrocardiography (ECG), despite the low predictive value for CAD of both resting and exercise ECG in asymptomatic individuals.3,7,8 In addition, as exercise favourably influences cardiovascular risk factors (e.g. by reducing weight and blood pressure and improving the lipid profile), traditional cardiovascular risk scores may underestimate cardiovascular risk in persons who exercise regularly. 9 Coronary artery calcium scoring (CACS) provides a direct, non-invasive measure of CAD and is the strongest independent predictor of cardiovascular events in asymptomatic persons. 10 Absence of coronary artery calcium (CAC) is associated with a very low risk of cardiovascular events in asymptomatic and symptomatic individuals. CACS is increasingly used in order to expand upon risk stratification in asymptomatic persons with an intermediate risk of cardiovascular events (class IIa recommendation in ESC guidelines) and has been recommended as a first-line test over exercise testing or single-photon emission computed tomography in asymptomatic patients and those who are at a low risk of CAD. 11 Approximately half of asymptomatic middle-aged persons have subclinical atherosclerosis, defined as the presence of any CAC. In the absence of scientific evidence, no clear recommendations are available regarding the medical management of these individuals. 12
We aimed to evaluate the additional value of low-dose cardiac computed tomography (CCT) using both CACS and coronary CT angiography (CCTA) in order to detect occult CAD in asymptomatic middle-aged (≥45 years) sportsmen without known cardiovascular disease (CVD), who underwent bicycle exercise testing as part of a SME. Considering the much higher incidence of exercise-related cardiac arrests in men compared to women, we chose to enrol men only.5,6
Methods
Study design and population
The rationale and design of the Measuring Athlete’s Risk of Cardiovascular Events (MARC) study have been published. 13 The MARC study was approved by medical ethics committee and complies with the Declaration of Helsinki. Written informed consent was obtained from all participants. Men aged 45 years or older were eligible if they were asymptomatic, engaged in competitive or recreational leisure sports, were free of known CVD and had undergone a SME with bicycle exercise ECG that revealed no abnormalities, according to the responsible physician. Participants underwent a SME mainly for comprehensive assessment of exercise tolerance and were recruited with the help of regional sports physicians, who provided potential participants with information, including a flyer detailing the MARC study. Exclusion criteria were known CAD, contrast allergy and renal impairment. Baseline assessments were obtained during the SME. SME ECGs were reassessed by a cardiologist (AM) according to the Seattle Criteria for abnormalities unrelated to athletic training. 14 In line with a recent publication, left axis deviation and atrial enlargement were considered to be training-related normal variants. 15
Cardiac computed tomography
A low-dose CCT was performed using a 256-slice CT scanner (Philips Healthcare, Best, The Netherlands) with prospective electrocardiographic gating. A non-contrast coronary CT was acquired for CACS, followed by contrast-enhanced CCTA. 13 The American Heart Association 16-segment coronary artery model was used to analyse image quality, plaque characteristics and coronary lumen stenosis on CCTA.
Image analysis and definition of relevant CAD
CT scans were processed on a workstation (IntelliSpace Portal, Philips Healthcare) by experienced technicians, and assessed by one of two experienced cardiac radiologists (NHP, BKV) who were blinded to the SME findings. Presence of relevant CAD was defined as CACS ≥ 100 Agatston units (AU) on non-contrast CCT and/or ≥50% luminal stenosis on CCTA.16–18
Abnormal findings on CT were reviewed by consensus with at least two (sports) cardiologists and one radiologist in order to provide advice on the management of participants with relevant CAD or other incidental findings. In general, participants with CACS 100–400 AU without obstructive CAD were given lifestyle recommendations and recommended to initiate statin treatment.19,20 Participants with CACS ≥ 400 AU or coronary artery stenosis ≥50% were offered a cardiologist consultation to discuss management options.
Number needed to screen
The number needed to screen (NNS) in order to prevent one cardiovascular event within 5 years was computed based on the reciprocal of the prevalence of CAD (CACS ≥ 100 AU and/or stenosis ≥50%) multiplied by 100, multiplied by the number needed to treat (NNT) in order to prevent one cardiovascular event (angina pectoris, myocardial infarction, coronary revascularisation, resuscitated cardiac arrest, stroke or cardiovascular death) obtained from the Multi-Ethnic Study of Atherosclerosis (MESA). 21
Statistical analysis
Differences between normally distributed variables were analysed using the Student’s t-test and chi-square test. Non-normally distributed data were assessed by applying Mann–Whitney U and Kruskal–Wallis tests. Reclassification rates were based on the CCT results: CACS < 100, low (0–4%) and CACS ≥ 100, high (≥10%) 10-year risk of fatal cardiovascular events, respectively. 16
After univariable analysis of the relationship between participant characteristics and the presence of CAD, a multivariable analysis was conducted via a stepwise logistic regression analysis. Data analysis was performed using IBM SPSS statistics for Windows (version 20.0l SPSS, Inc., Chicago, IL). A two-sided value of p < 0.05 was considered statistically significant.
Results
Characteristics and computed tomography imaging findings of Measuring Athlete’s Risk of Cardiovascular Events participants (n = 318).
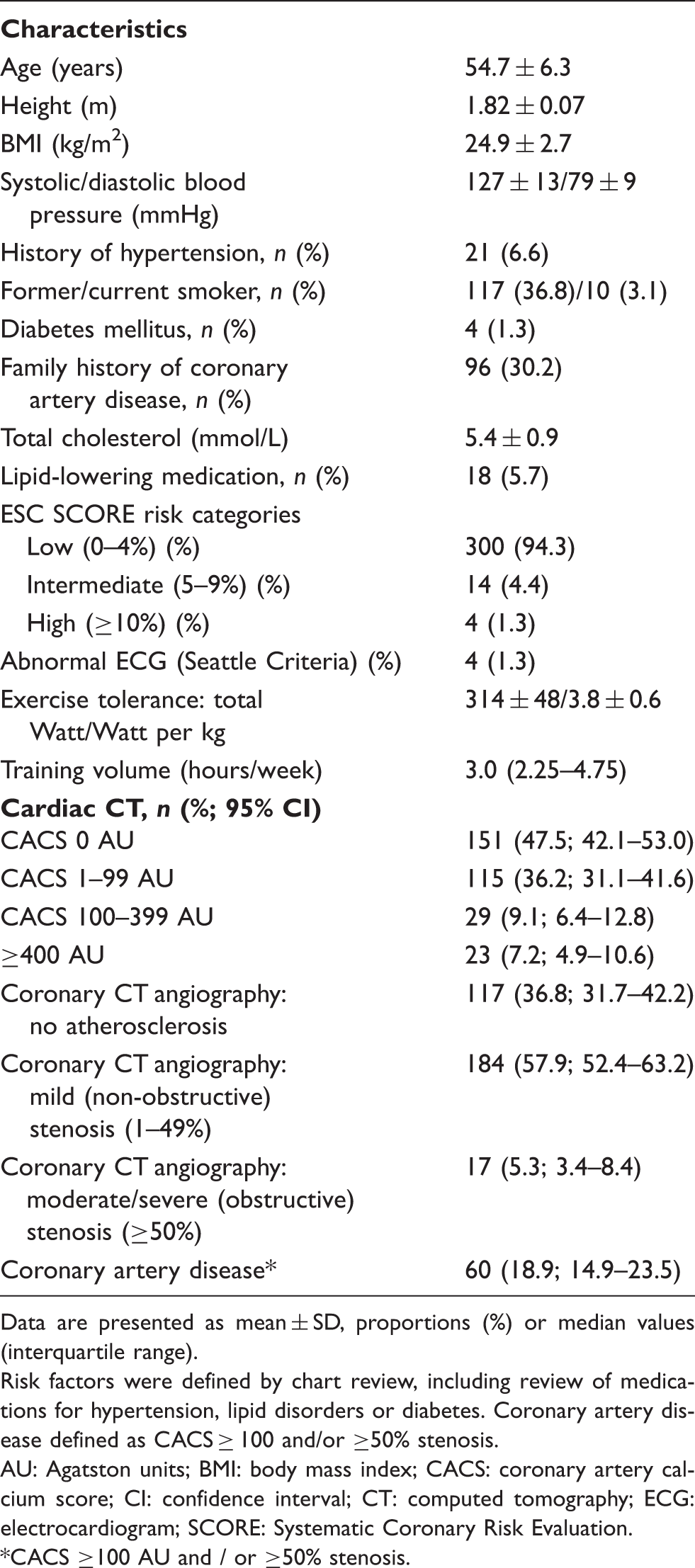
Data are presented as mean ± SD, proportions (%) or median values (interquartile range).
Risk factors were defined by chart review, including review of medications for hypertension, lipid disorders or diabetes. Coronary artery disease defined as CACS ≥ 100 and/or ≥50% stenosis.
AU: Agatston units; BMI: body mass index; CACS: coronary artery calcium score; CI: confidence interval; CT: computed tomography; ECG: electrocardiogram; SCORE: Systematic Coronary Risk Evaluation. *CACS ≥100 AU and / or ≥50% stenosis.
Three-hundred participants (94.3%) had a low (0–4%), 14 participants (4.4%) had an intermediate (5–9%) and four participants (1.3%) with diabetes had a high (≥10%) ESC SCORE risk. The participants were fit, with a mean maximal (bicycle) exercise capacity of 314 ± 48 Watt. Participants were predominantly engaged in high-dynamic, high-static sports (45% cyclists) and high-dynamic, low-static sports (36% long distance runners). Other sports included fitness (6%), speed/tour skating (5%), swimming/water polo (5%), rowing (1%) and tennis (1%).
ECG reassessment by a cardiologist revealed abnormal findings in four participants (complete left bundle branch block (n = 1), intraventricular conduction delay (n = 1), Q waves (n = 1) and QRS voltage criteria for left ventricular hypertrophy with abnormal repolarisation (n = 1)). The first two participants had no CAD on CCTA. The participant with Q waves underwent myocardial adenosine perfusion imaging that revealed no ischaemia or infarction. The fourth participant had long-standing hypertension without CAD or hypertrophy on CCTA.
Cardiac computed tomography
CCT results are also shown in Table 1. The total average radiation dose was 3.9 ± 0.9 mSv (1.0 ± 0.4 mSv for CACS and 3.0 ± 1.2 mSv for CCTA). No CAC was seen in 151 participants (47.5%), 115 (36.2%) had CACS 1–99 AU and 52 (16.4%) had CACS ≥ 100 AU. Stratification by age (45–54 years (n = 176), 55–64 years (n = 113) and 65–79 years (n = 29)) revealed increasing median CACS values (0, 16 and 39 AU, respectively; p for trend < 0.001), with accordingly lower rates of zero CACS (62%, 30% and 28%, respectively).
CCTA revealed no atherosclerosis in 117 (36.8%) and mild atherosclerosis in 184 (57.9%) participants. Seventeen (5.3%) participants had obstructive atherosclerosis (≥50% stenosis), with CACS < 100 AU in eight of them.
The combination of CACS and CCTA identified CAD in 60 (18.9%, 95% confidence interval (CI): 14.9–23.5%) participants, whose exercise capacity did not differ from those without CAD (303 vs. 317 Watt, p = 0.5). In univariable analysis, these 60 participants were significantly older, had higher body mass index (BMI) scores and cholesterol levels, more frequently had hypertension or a family history of CAD and more often were former smokers, and consequently had a higher ESC SCORE risk (data available in Supplemental Table 1). In a multivariable logistic regression model (see Supplemental Table 2), age (odds ratio (OR): 1.13, 95% CI: 1.07–1.19), BMI (OR: 1.19, 95% CI: 1.05–1.33), total cholesterol (OR: 1.75, 95% CI: 1.21–2.53) and family history of CAD (OR: 2.09, 95% CI: 1.10–4.01) remained independent predictors of relevant CAD on CCT.
Reclassification and NNS
With a CACS ≥ 100 AU as the cut-off (found in 52 (16.4%) participants), 46 of the 300 participants with low ESC SCORE risk were reclassified to higher risk and nine of the 14 participants with intermediate ESC SCORE risk were reclassified to low risk, resulting in 55 (17.3%, 95% CI: 13.5–21.8%) reclassifications. CCTA reclassified another eight (2.5%) participants to higher risk, resulting in an overall reclassification of 19.8% (95% CI: 15.8–24.5%).
The NNS in order to detect CACS ≥ 100 AU was 6.1 (100 × (1/16.4%)). Based on the 5–year NNT with a statin of 30,( 21 the NNS with CACS in order to prevent one cardiovascular event within 5 years is 183 (6.1 × 30) (95% CI: 144–236). Adding CCTA lowered the estimated NNS to 159 (95% CI: 128–201).
Additional cardiovascular workup/management of relevant CAD
Forty-three of the 60 participants with relevant CAD were given lifestyle recommendations and advised to contact their general practitioner in order to consider initiating statin treatment. The consensus panel recommended evaluation by a cardiologist in 17 (5.3%) participants with more severe CAD (CACS ≥ 400 AU and/or ≥50% stenosis). Nine participants underwent myocardial adenosine perfusion imaging, with no signs of ischaemia in seven and a positive perfusion scan in two that resulted in percutaneous coronary intervention (PCI). Four other participants underwent coronary angiography without prior myocardial perfusion imaging, which resulted in fractional flow reserve-guided PCI in two participants. The remaining four participants, after consultation with a cardiologist, opted for medical management without additional testing. In general, participants who were found to have relevant CAD were recommended to continue exercising, but to refrain from vigorous exercise. 22
Discussion
In this predominantly low-risk population (94% low ESC SCORE) of middle-aged sportsmen with a normal routine SME, CCT detected relevant CAD in almost one in every five participants. This reclassifies these persons to a higher risk of developing symptomatic CVD. Assuming a 5-year NNT (with statins) of 30 in order to prevent one cardiovascular event in individuals who are at high risk, this translates into a NNS of 159 (NNS of 183 if only CACS ≥ 100 AU is used).
The results demonstrate that both traditional cardiovascular risk assessment (ESC SCORE) and ECG exercise testing fail to reliably identify sportsmen with occult CAD. The fact that a considerable proportion of coronary events are attributed to non-obstructive lesions (with a high CACS reflecting the burden of multiple subclinical plaques that can become symptomatic) and the recent concept that more exercise-related cardiac arrests are caused by demand ischaemia in sportsmen with CAD than by acute plaque rupture provide a rationale for the identification of occult CAD in those who are (or aim to become) physically active.1,23
Comparison with other studies
Reference values for CACS are available from several population-based studies.24,25 Information on CCTA in asymptomatic/low-cardiovascular-risk persons is limited. Four studies have performed CCT in sportsmen (marathon runners).9,26–28
As expected, stratification by age revealed increasing median CACS in our participants, but their age-related values were generally lower than those of Caucasian men who are free of baseline CVD in the MESA and Heinz Nixdorf Recall (HNR) studies.24,25 MARC participants were younger, had a more favourable cardiovascular risk profile and more frequently had zero CAC (47.4%) than the MESA and HNR study subjects (32.1% and 18.1%, respectively). The MESA and HNR study subjects had higher BMI (28.1 and 27.9 vs. 24.9 kg/m2), were more often current/former smokers (11.9%/48.3% and 24.6%/45.2% vs. 3.1%/36.8%), more often had diabetes (4.4% and 5.7% vs. 1.3%) and hypertension (31.6% and 27.2% vs. 6.6%) and were more often treated with lipid-lowering medication (19.6% and 8.0% vs. 5.7%).
The prevalence of obstructive (≥50% stenosis) CAD in MARC (5.3%) was appreciably lower than that reported (25%) in the COroNary CT Angiography Evaluation For Clinical Outcomes: An InteRnational Multicenter Registry (CONFIRM) registry (mean age 58 ± 12 years) of persons without chest pain. 18 Apart from the greater age, the a priori likelihood of finding CAD was much higher in CONFIRM based on medical history and cardiovascular risk profile.
In a group of 108 German marathon runners, zero CACS was less common than in MARC (28.7% vs. 47.5%, p < 0.001). 9 Cardiovascular events nearly exclusively occurred in those with a CACS ≥ 100 AU, which was found more often than in MARC (36.1% vs. 16.4%, p < 0.001). 29 Apart from the slightly younger age (mean 54.7 ± 6.3 vs. 57.2 ± 5.7 years) and lower percentage of former and current smokers in our group (36.8% vs. 51.9%, p = 0.004; and 3.1% vs. 4.6%, p < 0.001, respectively), selection of participants may also play a role. The German study only enrolled persons who had run at least five marathons, whereas we recruited men aged ≥45 years from different sports disciplines with different training intensities. Two subsequent smaller studies in younger marathon runners (n = 50, mean age 52.6 ± 5.9 years and n = 25, mean age 55 ± 4 years) found lower numbers of CAD (10% and 8%).26,27 Six out of 44 (14%) asymptomatic athletes aged 30–60 years with ST-segment abnormalities during maximal exercise testing had a significant (>50%) coronary stenosis on CCTA, as compared to 5% of our sportsmen with a normal exercise test. 28
Implications
With the increasing number of middle-aged persons engaging in sports, our CCT results may apply to a considerable segment of the population. The low NNS in the general population in order to identify an individual with moderate CACS (≥100 AU) seems sufficient justification for extending CACS to lower-risk individuals in future guidelines, as CAC is also associated with risk of cardiovascular events among individuals with few or no risk factors. 10 The estimated NNS in MARC of 183 (CACS alone) or 159 (CACS combined with CCTA) in order to prevent one cardiovascular event in the next 5 years with statin treatment is low compared to other accepted screening tests, such as mammography to prevent a death from breast cancer in women aged 50–59 years (NNS 2451) or a cardiovascular event in mild-to-moderate hypertension (140–160 mmHg; NNS 279).30,31 The NNS would have been even lower if we had used the lower 21 instead of the higher 28 NNT estimate derived from the MESA study. 21
Investigating asymptomatic persons with CCT invariably raises issues. First, the prevalence of CCT-detected CAD depends on CAD definitions: our cut-off values (CACS ≥ 100 AU and ≥50% luminal stenosis) are commonly used in (population-based) studies.16–18 The prevalence of any CAD (i.e. non-zero CACS or any atherosclerosis on CCTA) was 63.2% (95% CI: 57.8–68.3%). Second, finding significant CAD may lead to additional diagnostic tests with extra costs and risks to asymptomatic persons. Severely calcified lesions can lead to misinterpretation of stenotic lesions and unwarranted further diagnostic testing or treatment. However, the Early Identification of Subclinical Atherosclerosis by Noninvasive Imaging Research (EISNER) study demonstrated that CACS compared with no scanning in asymptomatic volunteers could improve cardiac management without incurring significant downstream medical costs. 32 Third, without firm evidence-based guidelines, it is debatable how best to treat CAD in asymptomatic persons other than lifestyle modification. Many practitioners feel that any degree of CAD on CCT should be treated aggressively, and the threshold for statin treatment in order to prevent cardiovascular events is becoming lower in recent guidelines. For example, by applying the recent American College of Cardiology (ACC)/American Heart Association (AHA) guidelines to a European population aged 55 years or older, nearly all men (96.4%) would be eligible for statin treatment, compared to 66.1% when following the ESC guidelines. 33 Fourth, incidental findings, (e.g. pulmonary nodules) may lead to additional investigations. We used the Fleischner Society recommendations for solid and sub-solid pulmonary nodules on CT. 34 One participant was operated on for a malignant pulmonary sub-solid nodule found on CCT. Fifth, radiation is associated with a small dose-dependent increase in the risk of cancer. The mean radiation dose MARC participants received was 3.9 mSv: equivalent to 1–2 years of background radiation. Estimating the risk of cancer is difficult because there are no prospective data on the adverse events of radiation with the doses used for diagnostic purposes. 35 Being aware of these limitations, and without better estimates, the International Commission on Radiological Protection estimates that the risk of a dose of 10 mSv for a member of the public translates to a fatal cancer risk of five per 10,000 persons. 35 Limiting the investigations to CACS reduces the dose to 1 mSv, but technical developments are also lowering CCTA radiation doses substantially.
Limitations of our study require mentioning. First, although constituting a considerable number for a study of its kind, this remains a relatively small study of 318 selected men (all were Caucasian with college education). The fact that they consented to participate after undergoing a SME may have led to additional selection bias (e.g. those with a higher chance of CVD because of a positive family history). In order to investigate the possibility of selection bias, we compared our participants to a group of 725 unselected men aged ≥45 years who underwent a SME in 2012–2013 in another region of The Netherlands (Maxima Medical Centre, Veldhoven). The cohorts were remarkably similar (mean age 54.7 vs. 54.3 years, systolic blood pressure 127 vs. 129 mmHg, BMI 24.9 vs. 25.0 kg/m2, current smoking 3.1% vs. 5.1%, workload 314 vs. 309 Watt), indicating that our group is representative of sportsmen who undergo a SME.
Second, we used the NNT derived in the MESA cohort (estimated NNT across dyslipidaemia categories, mean age 62.0 ± 10.7 years) that is older than our group in order to calculate the NNS. 21 Athletes may also show less compliance with statins because of their myopathy side effects. 22 For these reasons, we chose the higher NNT estimate (30 rather than 23). 21
Third, our participants did not undergo echocardiography. The MARC study focused on CAD, and the probability of finding abnormalities in asymptomatic persons with a normal ECG and without heart murmurs on physical examination is low. 36 Nevertheless, careful ECG evaluation is warranted, as cardiomyopathies in older sportsmen can occur.
Fourth, non-invasive techniques in order to identify asymptomatic persons at increased risk (e.g. measurement of carotid intima media thickness, heart rate recovery after exercise and T wave alternans analysis) were not part of this study. 37
Our study’s main strength is that it is the first to examine the additional value of CACS and CCTA to a normal SME in asymptomatic middle-aged sportsmen with a low ESC SCORE risk in different sport disciplines. Our results demonstrate the limited value of traditional cardiovascular risk assessment and exercise testing in order to detect occult CAD in older sportsmen. CCT provides a more reliable risk assessment and will provide guidance to managing sportsmen who are found to have occult CAD in order to prevent (exercise-related) cardiovascular events.
Currently, no firm recommendations can be made regarding the routine use of CCT in the pre-participation evaluation of athletes aged ≥45 years. As the additional value of CCTA is limited in this study, due to its extra costs, contrast use and radiation, we suggest that a randomised study should investigate the hypothesis that the introduction of CACS in a SME setting reduces the incidence of (exercise-related) cardiac events in older athletes and is cost effective compared to exercise testing.
In conclusion, almost one in five asymptomatic middle-aged sportsmen, with a normal bicycle exercise test and predominantly low conventional cardiovascular risk scores, has occult CAD, and 87% of these abnormalities can be detected with CACS alone. The 5-year NNS with CCT in order to prevent one cardiovascular event appears to be much lower than for other screening strategies (183 for CACS and 159 for combined CACS and CCTA).
As both traditional cardiovascular risk assessment (ESC SCORE) and bicycle exercise testing do not reliably identify sportsmen with occult CAD, there is a need to further investigate the role of CCT in this setting.
Footnotes
Acknowledgements
We thank the participants, sports physicians, radiology technicians, Anneke Hamersma and Mireille Velthuis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: the MARC study was supported by unrestricted grants from the Foundations Wetenschappelijk Onderzoek Hart- en Vaatziekten and Bijstand of Meander Medical Center Amersfoort, the Röntgen Foundation Utrecht, Philips Healthcare and SPORTCOR, a Dutch databank for sports cardiology.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.