
Abstract
Background
More than half of cardiovascular mortality occurs outside the hospital, mainly due to consistently low survival rates from out-of-hospital cardiac arrest.
Methods
This is a prospective, nested, case–control study derived from the Västerbotten Intervention Programme and the World Health Organization’s Multinational Monitoring of Trends and Determinants in Cardiovascular Disease study in northern Sweden (1986–2006). To determine predictors for sudden cardiac death risk factors for cardiovascular disease were compared between incident myocardial infarction with sudden cardiac death (n = 363) and survivors of incident myocardial infarction (n = 1998) using multivariate logistic regression analysis.
Results
Diabetes had the strongest association with sudden cardiac death out of all evaluated risk factors (odds ratio (OR) 1.83, 95% confidence interval (CI) 1.30–2.59), followed by low education (OR 1.55, 95% CI 1.19–2.01), high body mass index (OR 1.05, 95% CI 1.02–1.08) and male sex (OR 1.42, 95% CI 1.001–2.01).
Conclusions
The pattern of risk factors for incident myocardial infarction is different among survivors and those who die within 24 hours. The risk factors that contribute the most to death within 24 hours are diabetes mellitus, high body mass index and low education level, and can be addressed at both the public health level and by general practitioners.
Introduction
Cardiovascular mortality is the leading cause of death, but reducing this mortality is challenging. Sudden cardiac death (SCD) is at the core of this challenge, as at least two-thirds of these cases occur out of hospital1–4 and overall survival from a cardiac arrest is less than 10%,5–7 constituting approximately 20% of the total mortality. 8 Thus, those suffering from incident myocardial infarction (MI) with SCD do not benefit from the last few decades of medical advancements in secondary prevention. 9 Consequently, the main potential in reducing mortality from SCD lies outside hospital settings, and primary preventive measures are the most promising strategy for improving survival rates. 10 Many studies present methods for stratifying SCD risk among other risk groups, such as post-MI, structural heart disease, heart failure and diabetes.11–14 Post-mortem studies on SCD have demonstrated a wide range of underlying conditions,15,16 which indicates that SCD cannot simply be viewed as a severe onset of the typical MI. The traditional risk factors for incident MI may differentiate between those who survive more than 24 hours (i.e. MI survivors) and those who present with SCD. Cohort data are available but there are no population-based data on the risk markers for SCD or studies comparing the risk factors in MI survivors and those who succumb from post-MI SCD. Identifying the risk factors for SCD and their relative importance among previously healthy individuals is the first logical step to initiating preventive measures that can improve survival. Therefore, our aim was to study the risk factors for SCD based on the hypothesis that the pattern of risk factors for MI is different in survivors and those who die within 24 hours.
Materials and methods
Study population
The study population was derived from the Västerbotten Intervention Programme (VIP) 17 and the World Health Organization’s (WHO) Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA) study in northern Sweden. 18 Both VIP and MONICA are health examination programmes for cardiovascular disease and diabetes with participation rates of 59% and 77%, respectively. The data collection methods in the VIP and MONICA study regarding cardiovascular risk markers were similar. The designs of the VIP and MONICA study have previously been described in detail.17,18 All MI events in northern Sweden are registered in the population-based MONICA registry according to standardised WHO and MONICA criteria and based on reports from hospitals or general practitioners, as well as hospital discharge records and death certificates. 18 All prospective cases of first MI in VIP and MONICA participants between 1986 and 2006 were identified in the MONICA registry. Post-MI deaths were classified as SCD if they occurred within 24 hours of the onset of symptoms.
A prospective, nested case–control study design was used. Subjects with a history of MI before the health examination were excluded, as experiencing a MI may influence the studied determinants. Up to four controls matched by sex, age (±2 years) and year and type of health examination were selected for each case. A total of 2361 cases of incident MI and 8502 controls were identified. Of the incident MI cases, 363 experienced SCD.
Baseline variables
Smoking habits were classified into ‘daily smoking’ or ‘non-smoking’ (including previous smokers and occasional smokers). Body mass index (BMI) was calculated as weight in kilograms divided by height in metres squared. Hypertension was defined as a systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg, or reported use of anti-hypertensive medication during the past 14 days. Blood samples were taken after a minimum 4-hour fast and analysed for total cholesterol and plasma glucose using a bench-top analyser (Reflotron, Boehringer Mannheim GmbH Diagnostica, Germany). Since 2005, a HemoCue bench-top analyser (Quest Diagnostics) has been used for glucose values. An oral glucose tolerance test was performed with a 75 g oral glucose load according to WHO standards. Diabetes was defined as self-reported disease on a questionnaire or a fasting glucose ≥7 mmol/L and/or a 2-hour post-load plasma glucose ≥11.0 mmol/L (≥12.2 mmol/L in the VIP, as capillary plasma was drawn). Education level was dichotomised into 9 years of compulsory education or a higher level of education.
Statistical analysis
Using logistic regression we analysed the associations between risk factors and MI, comparing SCD cases and MI survivors. Multivariate models included the traditional cardiovascular risk factors age, smoking, diabetes, education level, BMI, cholesterol level and systolic blood pressure. Univariate conditional logistic regression including a single potential risk variable was used to analyse crude odds ratios (ORs) and 95% confidence intervals (CIs) for each potential risk factor based on the matched case–control sets. The multivariate model included smoking, diabetes, education, BMI, cholesterol level and systolic blood pressure. The case–control sets were matched for age and sex. The statistical computations were carried out in SPSS for Windows (versions 15 and 17; SPSS Inc., Chicago, IL, USA). The study was approved by the research ethics committee of Umeå University. All participants provided informed consent.
Results
A total of 363 MI cases with SCD and 1318 controls matched for screening time, age and sex were included with 1998 MI survivors and 7184 matched controls. Of the 2361 MI cases, 16% of the men and 14% of the women presented with SCD; 288 (79%) of the 363 SCD cases occurred out of hospital. No significant difference was found in the time from screening to event between SCD cases and MI survivors (P = 0.67).
Baseline characteristics of 1507 men and 491 women with myocardial infarction without sudden death and 284 men and 79 women with myocardial infarction with sudden death.
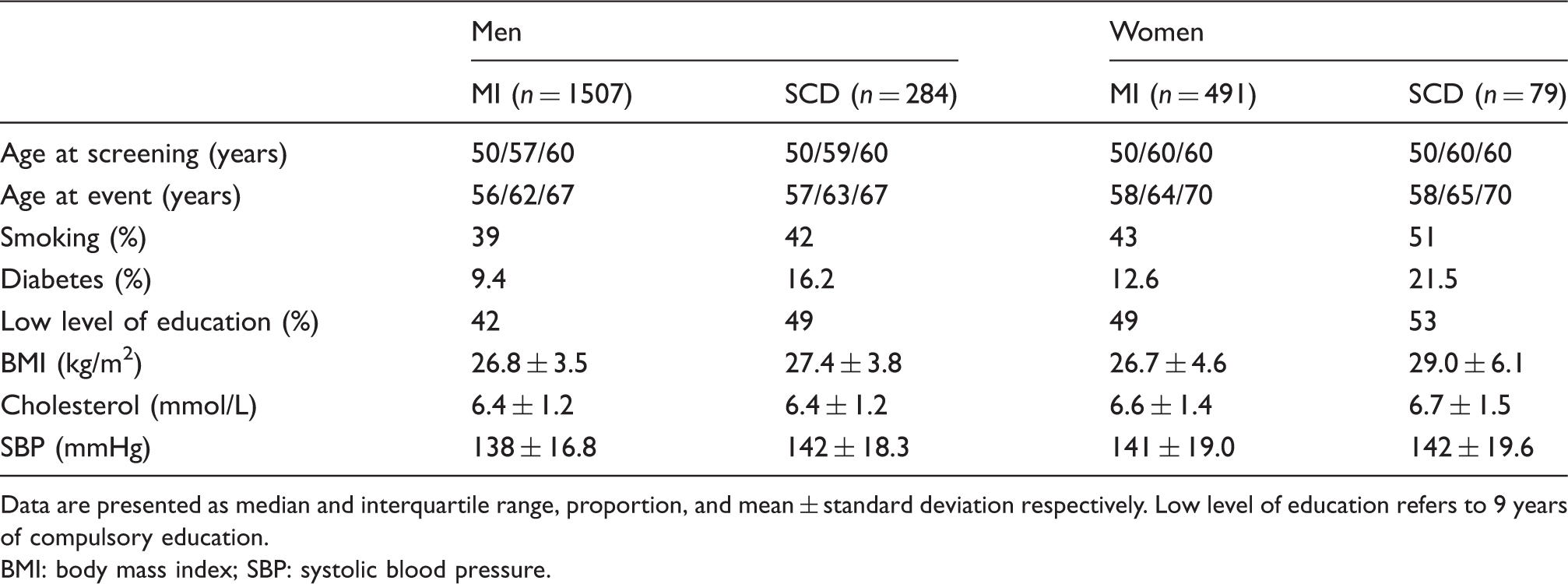
Data are presented as median and interquartile range, proportion, and mean ± standard deviation respectively. Low level of education refers to 9 years of compulsory education.
BMI: body mass index; SBP: systolic blood pressure.
Univariate and multivariate logistic regression analysis of incident myocardial infarction with sudden cardiac death compared to 24-hour survival.
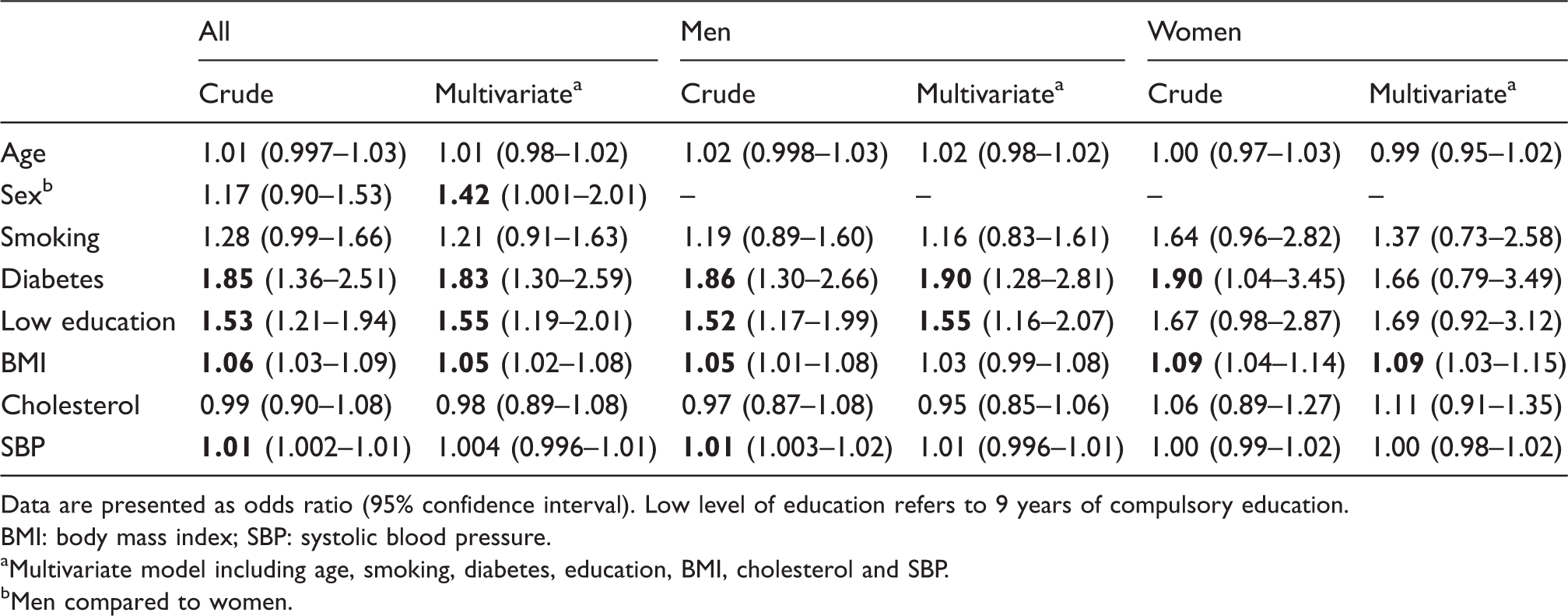
Data are presented as odds ratio (95% confidence interval). Low level of education refers to 9 years of compulsory education.
BMI: body mass index; SBP: systolic blood pressure.
Multivariate model including age, smoking, diabetes, education, BMI, cholesterol and SBP.
Men compared to women.
Univariate and multivariate conditional logistic regression analysis of incident myocardial infarction with or without sudden cardiac death.
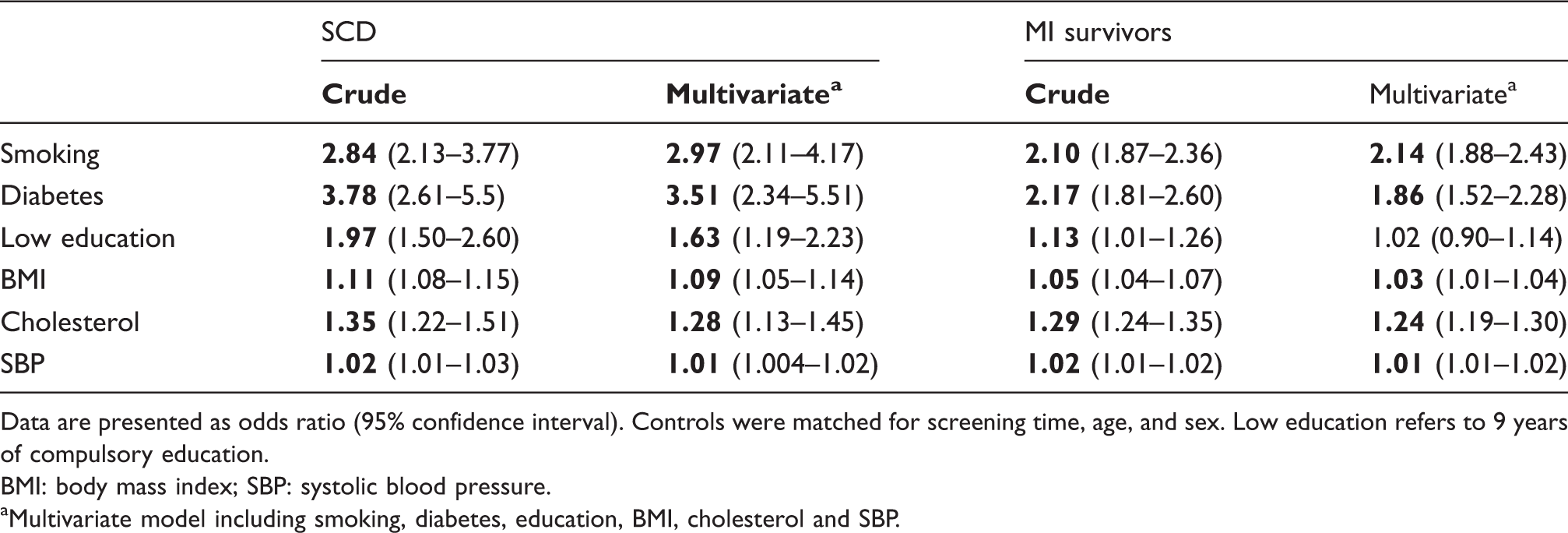
Data are presented as odds ratio (95% confidence interval). Controls were matched for screening time, age, and sex. Low education refers to 9 years of compulsory education.
BMI: body mass index; SBP: systolic blood pressure.
Multivariate model including smoking, diabetes, education, BMI, cholesterol and SBP.
To analyse the combined effect of the risk factors on SCD, we constructed four groups based on the presence of pairs of the selected dichotomised risk factors in a conditional logistic regression analysis. The presence of diabetes mellitus and low education versus none of these had an OR of 6.33 for SCD compared to matched controls (95% CI 3.70–10.8). The risk for SCD among persons with diabetes mellitus and smoking had an OR of 8.45 (95% CI 4.25–16.8) compared to non-smokers without diabetes. Finally, smokers with low education had an OR of 4.45 (95% CI 3.00–6.58) compared to non-smokers with higher education.
Univariate conditional logistic regression analysis of myocardial infarction with or without sudden cardiac death.
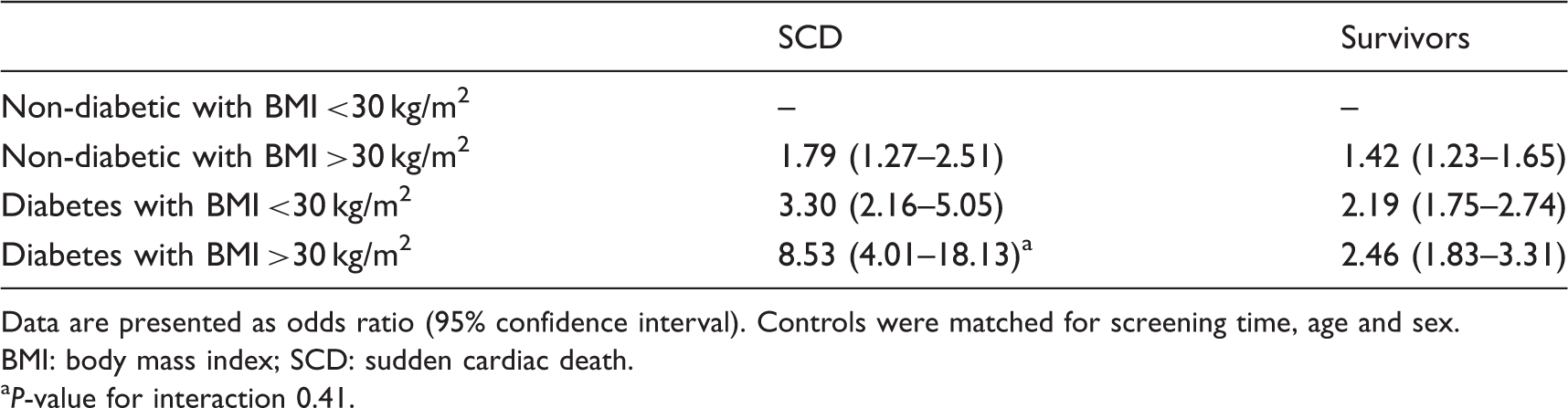
Data are presented as odds ratio (95% confidence interval). Controls were matched for screening time, age and sex.
BMI: body mass index; SCD: sudden cardiac death.
P-value for interaction 0.41.
Discussion
Our main finding in the present study is that the risk factors for dying within 24 hours of the onset of an incident MI compared to surviving is diabetes, low education level, high BMI and male gender. The combination of BMI >30 kg/m2 and diabetes was associated with an 8-fold increased risk of SCD compared to matched controls without MI. Our findings are in line with previous research and provide further evidence that both diabetes and obesity increase the risk of SCD. A recent meta-analysis of 10 prospective and four case–control studies reported a 2-fold increased risk of SCD among people with diabetes. 13 A Swedish cohort study from Göteborg found diabetes more common among fatal than non-fatal coronary events. 19 Other cohort studies have similarly found associations between diabetes and SCD, 3 and several mechanisms have been suggested. The increased risk of MI and SCD in patients with diabetes mellitus may be related to inflammation, diabetic cardiomyopathy and diabetic autonomic neuropathy with subsequent arrhythmia.13,20 Previous cohort studies have shown up to 2 to 3-fold increased risk for SCD among obese patients,21–23 supporting our results. The mechanism of increased SCD among obese individuals could be mediated through several mechanisms, such as haemodynamic disturbances, hypertension and left ventricular hypertrophy or cardiac electrical abnormalities. 21
For patients with incident MI admitted alive to the hospital, the odds of survival are good.9,24,25 The vast majority of patients who die from cardiovascular events do so out of hospital. Implantation of implantable cardioverter defibrillators in individuals at very high risk of SCD is one option, but is limited to a selected high-risk group. Early awareness of warning signs, early cardiopulmonary resuscitation, and public access to automated external defibrillators are important strategies, but they have limitations. Public access defibrillation requires early detection of out-of-hospital cardiac arrest and the presence of ventricular fibrillation or flutter. 26 Thus, the potential for improving MI survival rates is outside the hospital, mainly involving primary prevention.
Our study shows that lifestyle factors are important not just for the risk of developing incident MI, but also for early prognosis, and that the strongest contributors may be modified in the general population. We identified three possible ways to decrease the risk attributable to these risk factors in the general population and selected high-risk groups. These strategies aim to lower out-of-hospital cardiovascular mortality.
First, the factors most strongly associated with an early bad prognosis, diabetes and obesity should be addressed through preventive lifestyle and public health interventions to avoid or delay disease. In public health interventions, improving the education level of the population is important, especially to encourage and support further education beyond 9 years of compulsory school. Public health interventions reach the entire population and will also decrease overall MI incidence.
Second, the early detection and treatment of type 2 diabetes mellitus is important, especially among those with BMI >30 kg/m2, who have an 8-fold increased risk of dying within 24 hours of their first MI. In the analysis of blood glucose levels sampled approximately 5 years before the SCD event, 50% of the individuals with diabetes were not treated or stated that they did not have diabetes. Delayed diagnosis and treatment may have contributed to the fatal outcome of incident MI. Previous studies have shown that impaired fasting plasma glucose increases the risk of SCD 1.51-fold. 27
Third, medical treatment of the remaining cardiovascular risk factors in the general population should be addressed. At this point, reducing cholesterol levels and hypertension are important ways to improve not only early prognosis, but also long-term prognosis, and reduce overall MI events. Smoking cessation should be encouraged at all levels of the health care system. A cardiovascular risk prevention strategy among risk groups with a high incidence of diabetes was associated with better prognosis and could be a suitable model for the general practitioner. 28
However, further studies are needed to confirm our findings and verify that our suggested measures are effective at reducing the out-of-hospital cardiovascular mortality. Studies with interventions in high-risk subjects with diabetes and obesity are especially important. To the best of our knowledge, this study is the first prospective, nested, case–control study investigating whether the established cardiovascular risk factors for incident MI are different between survivors and those who die within 24 hours. We also want to emphasise that we studied incident MIs, as these patients are not subject to secondary preventive medication or other interventions that may affect the studied risk factors.
Our study is unique for two reasons. Firstly, it includes all incident MI cases with SCD, even those who died before being admitted to hospital care and cases in which no cardiopulmonary resuscitation was attempted. This is especially important as a majority of cardiovascular deaths4,11,14,27 occur outside hospital settings. Secondly, questionnaires, BMI, blood pressure, blood samples and other data were collected during a health examination prior to the SCD events.
Our study has some limitations. We only had 79 female SCD cases, limiting the gender analysis. The participants in this study were mainly middle-aged Caucasians from northern Sweden. Therefore, the results cannot be applied to other populations with certainty. We have adjusted our results for traditional risk factors but not biomarkers, and as such we cannot exclude the possibility that biomarkers, such as C-reactive protein, affected the results.
Conclusion
The pattern of risk factors for MI is different among survivors and those who die within 24 hours. Except for the male sex, all risk factors associated with death within 24 hours can be addressed at both the public health level and by general practitioners.
Footnotes
Author contribution
DL, SE and JH contributed to the conception or design of the work. JA, PW, DL, SE and JH contributed to the acquisition, analysis, or interpretation of data for the work. JA drafted the manuscript. JA, PW, DL, SE and JH critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.