
Abstract
Background
Metabolic syndrome is the most important risk factor for developing cardiovascular disease and type 2 diabetes. The aim of this review was to systematically assess and perform a meta-analysis of the effects of yoga on the parameters of metabolic syndrome.
Methods
MEDLINE/PubMed, Scopus, the Cochrane Central Register of Controlled Trials and IndMED were searched and screened from their inception through to 8 March 2016 for randomised controlled trials on yoga for patients with metabolic syndrome. Risk of bias was assessed using the Cochrane risk of bias tool.
Results
Seven trials with a total of 794 participants were included. No effects of yoga on resolution of metabolic syndrome, diastolic blood pressure, triglycerides, high-density lipoprotein cholesterol and fasting plasma glucose were found, but yoga was superior to usual care for waist circumference (standardised mean difference (SMD) = −0.35; 95% confidence interval (CI) = −0.57 to −0.13; p < 0.01) and systolic blood pressure (SMD = −0.29; 95% CI = −0.51 to −0.07; p = 0.01). However, these effects were not robust against selection bias. No intervention-related adverse events were reported.
Conclusion
Based on the results of this meta-analysis, no recommendation can be made for or against yoga in order to influence the parameters of metabolic syndrome. Despite methodological drawbacks, and until further research is undertaken, yoga can be preliminarily considered as a safe and effective intervention for reducing waist circumference and systolic blood pressure in individuals with metabolic syndrome who are not adhering to conventional forms of exercise.
Keywords
Background
Metabolic syndrome is a major health problem in industrialised countries worldwide 1 and mainly results from a sedentary lifestyle, high levels of subjective stress and inadequate diet. Different definitions of metabolic syndrome have emerged that base the diagnosis on varying criteria. However, almost all definitions require the presence of central obesity, elevated blood pressure, elevated plasma glucose and/or dyslipidaemia. 2 Insulin resistance and adipose tissue dysfunction are thought to be the primary mediators of metabolic syndrome. 3 Metabolic syndrome is associated with numerous comorbidities 2 and is among the most important risk factors for cardiovascular disease and type 2 diabetes mellitus. 4 While drug therapy is recommended for metabolic syndrome only as a secondary intervention, the primary management approach for metabolic syndrome is a healthy lifestyle, including a change in dietary composition and an increase in physical activity. 5 A complementary lifestyle intervention that includes both components and is gaining increased popularity worldwide is yoga.
Yoga is rooted in Indian philosophy and has been a part of traditional Indian spiritual practice for millennia. 6 Yoga traditionally is a complex intervention that comprises not only physical activity, but also advice for breathing exercises, meditation and advice for a healthy and ethical lifestyle. While the ultimate goal of traditional yoga has been described as uniting mind, body and spirit, it has become a popular means of promoting physical and mental well-being.6,7 In North America and Europe, yoga is most often associated with physical postures (asanas), breathing techniques (pranayama) and meditation (dhyana), and different yoga forms have emerged that put varying levels of focus on physical and mental practices. 6 In North America and Europe, yoga is gaining increased popularity as a therapeutic intervention. Approximately 14 million adult Americans (more than 6% of the population) reported that yoga had been recommended to them by a physician or therapist. 8 Indeed, approximately 80% of American yoga practitioners (more than 16 million people) reported that they had started practice explicitly to improve their health. 9 Yoga is a combination of exercise, controlled breathing and relaxation, often combined with specific diet and lifestyle advice. It has been tested in the prevention and rehabilitation of cardiac diseases10,11 and has been shown to improve several components of metabolic syndrome.11,12 Thus, the aim of this review was to systematically evaluate and perform a meta-analysis of the available data on the efficacy and safety of yoga as an adjunct treatment for patients with metabolic syndrome.
Methods
This review was planned and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 13 and the recommendations of the Cochrane Collaboration. 14
Eligibility criteria
Types of studies
Randomised controlled trials (RCTs), randomised cross-over studies and cluster-randomised trials were eligible. No language restrictions were applied.
Types of participants
Studies on adult patients (≥18 years) with a diagnosis of metabolic syndrome were eligible. No restrictions were made regarding diagnostic criteria; however, differences in studies using standardised diagnostic criteria such as the US National Cholesterol Education Program Adult Treatment Panel III (NCEP), 15 the American Heart Association (AHA), 16 the International Diabetes Federation (IDF) 17 or the World Health Organization (WHO) criteria 18 were compared with studies that used unclear or inadequate diagnostic criteria in a sensitivity analysis.
Types of interventions
Experimental
Studies on yoga interventions, including at least one of physical activity, breath control, meditation and/or lifestyle advice (based on yoga theory and/or traditional yoga practices) were eligible. No restrictions were made regarding yoga tradition, length, frequency or duration of the programme. Studies on multimodal interventions that included yoga amongst others were excluded. Studies allowing individual co-interventions were eligible (i.e. studies allowing patients to continue their individual treatment by their respective physician were not excluded as long as all study groups were allowed to do so).
Control
Studies comparing yoga to usual care, exercise or other active non-pharmacological control interventions were eligible.
Types of outcome measures
To be eligible, studies had to assess the resolution of metabolic syndrome (i.e. the number of patients who no longer met the diagnostic criteria for metabolic syndrome) or at least one other primary outcome based on internationally recognised diagnostic criteria: waist circumference, triglycerides, high-density lipoprotein (HDL) cholesterol, systolic blood pressure, diastolic blood pressure and/or fasting plasma glucose. Safety was defined as a secondary outcome.
Search methods
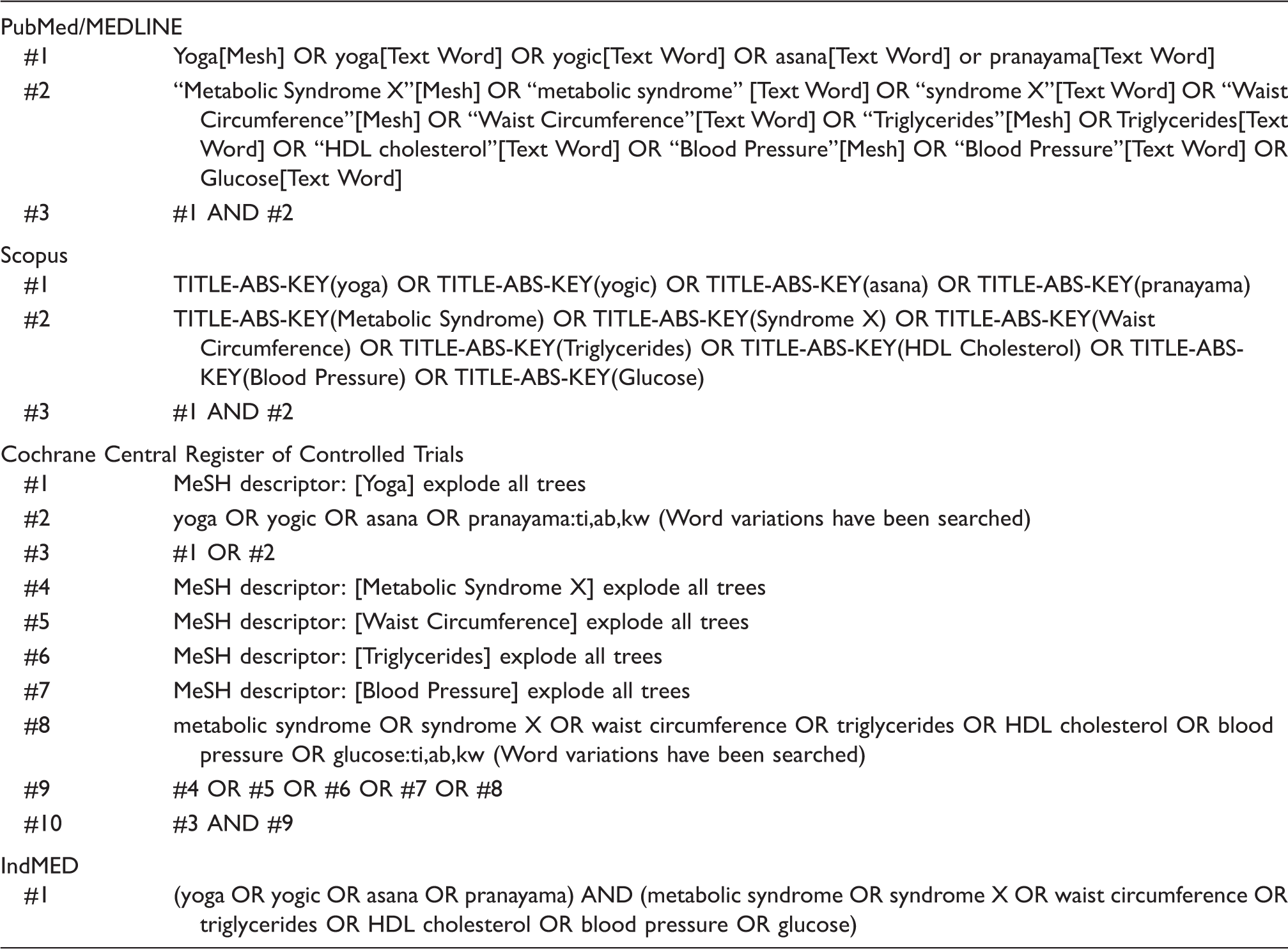
Complete literature search.
Abstracts were screened and selected independently by two reviewers (HC and RL), and potentially eligible articles were read in full by two reviewers (HC and RL). Disagreements were settled through a discussion with a third reviewer until consensus was reached. If necessary, additional information was obtained from the authors of the primary study.
Data extraction and management
Data on patients (e.g. diagnostic criteria, age, gender and ethnicity), methods (e.g. randomisation and allocation concealment), interventions (e.g. yoga type, frequency and duration), control interventions (e.g. type, frequency and duration), outcomes (e.g. outcome measures and assessment time points) and results were extracted independently by two reviewers (HC and RL) using an a priori-developed data extraction form. Disagreements were settled through discussion with a third reviewer until consensus was reached.
Data analysis
Assessment of overall effect size
Meta-analyses were conducted using Review Manager 5 software (version 5.1, The Nordic Cochrane Centre, Copenhagen, Denmark) by random effects models. In order to be able to perform a meta-analysis on a specific outcome, at least two RCTs had to have assessed this outcome (i.e. if a specific outcome was assessed in only one RCT, no meta-analysis was performed; if it was assessed by two or more RCTs, a meta-analysis was performed). Separate meta-analyses were conducted for comparisons of yoga to different control interventions. For dichotomous outcomes, odds ratios (OR) with 95% confidence intervals (CIs) were calculated. For continuous outcomes, standardised mean differences (SMDs) with 95% CIs were calculated as the difference in means between groups, divided by the pooled standard deviation, using Hedges’ correction for small study samples. 14 Where no standard deviations were available, they were calculated from standard errors, CIs or t-values, 14 or attempts were made to obtain the missing data from the studies’ authors by email. A negative SMD (i.e. lower values in the yoga group) was defined as indicating beneficial effects of yoga compared to the control intervention for all outcomes except for HDL cholesterol, where a positive SMD (i.e. higher values in the yoga group) was defined as indicating beneficial effects. If necessary, values were inverted. 14 Cohen’s categories were used in order to evaluate the magnitude of the overall effect size with SMD = 0.2–0.5 being small, SMD = 0.5–0.8 being medium and SMD > 0.8 being large effect sizes. 20
Assessment of heterogeneity
The I2 statistic was used in order to analyse the statistical heterogeneity between studies. The magnitude of heterogeneity was categorised as I2 = 0–24% being low, I2 = 25–49% being moderate, I2 = 50–74% being substantial and I2 = 75–100% being considerable heterogeneity.14,21 The χ2 test was further used in order to assess whether differences in results are compatible with chance alone. Given the low power of this test, when only few studies or studies with low sample sizes are included in a meta-analysis, a p-value ≤ 0.10 was regarded as indicating significant heterogeneity. 20
Subgroup analyses
Subgroup analyses were initially planned for the type of yoga intervention (yoga interventions including physical postures vs. yoga interventions without physical postures). As all studies included yoga postures, subgroup analyses could not be performed.
Assessment of risk of bias in individual studies and across studies
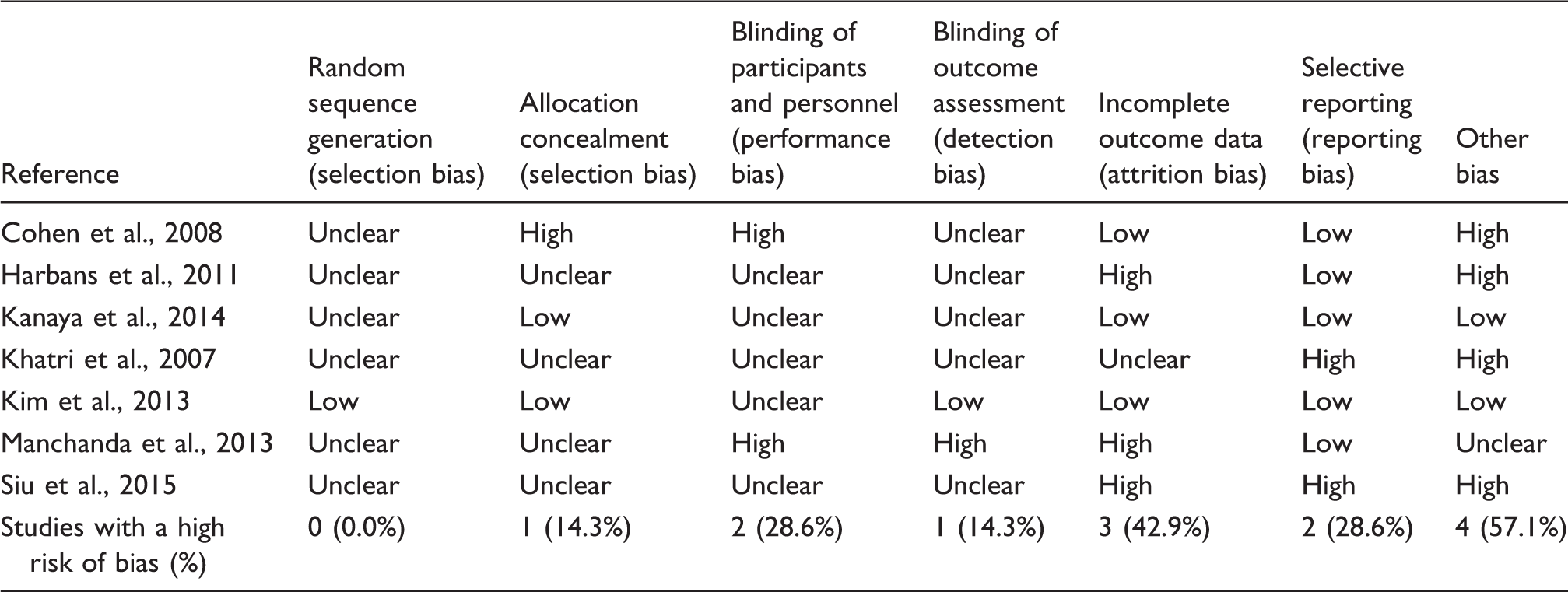
Risk of bias was assessed independently by two reviewers using the Cochrane risk of bias tool. 14 This tool assesses the risk of bias on seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias. For each domain, risk of bias was assessed as low, unclear or high. Disagreements were settled through discussion with a third reviewer until consensus was achieved.
In order to test the robustness of significant results, sensitivity analyses were conducted by including only studies with a low risk of bias in the following domains: selection bias (random sequence generation and allocation concealment), detection bias (blinding of outcome assessment) and attrition bias (incomplete outcome data). Initially, further sensitivity analyses were planned that would include only studies that used standardised diagnostic criteria and would exclude studies that used unclear or inadequate diagnostic criteria. As all studies that were included in meta-analyses used standardised diagnostic criteria, these sensitivity analyses could not be performed.
Assessment of publication bias was initially planned using funnel plots generated by Review Manager software;14,22 however, as fewer than 10 studies were included in each meta-analysis, funnel plots could not be analysed.
Results
Literature search
Twelve full-text articles were assessed for eligibility; four were excluded because they were not randomised23,24 or were not focused on metabolic syndrome.25,26 Eight full-text articles reporting on seven RCTs involving a total of 794 patients met the inclusion criteria and were included in the qualitative analysis (Figure 1).27–34 One study did not report post-intervention data for the control group; as the missing data could not be obtained from the studies’ authors, this study was not included in the meta-analysis.
31
Two further studies had unique control groups that could not be pooled with other control groups in meta-analyses.29,30 All full-text articles were published in English.
Flowchart of the results of the literature search.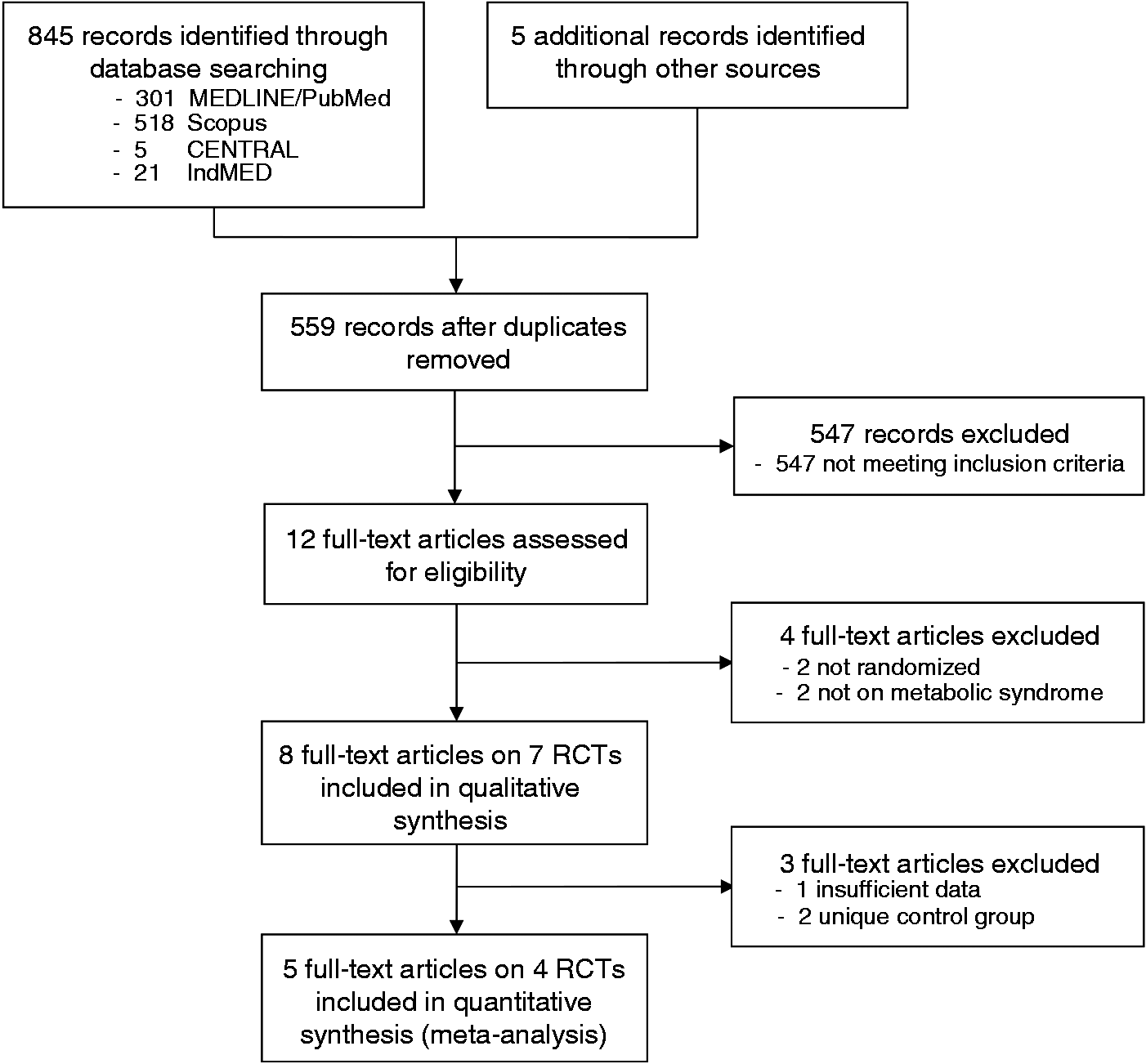
Study and participant characteristics
Sample characteristics.
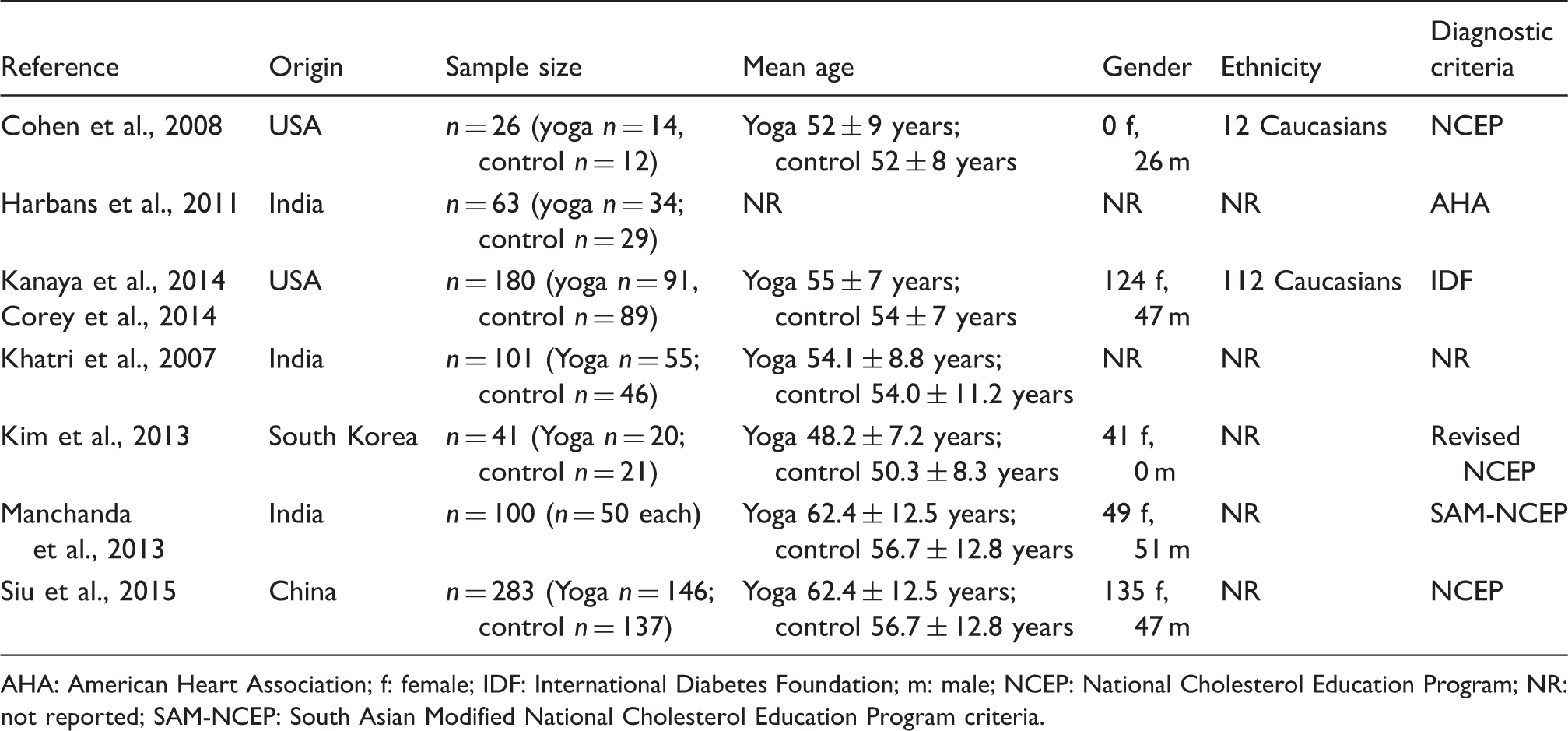
AHA: American Heart Association; f: female; IDF: International Diabetes Foundation; m: male; NCEP: National Cholesterol Education Program; NR: not reported; SAM-NCEP: South Asian Modified National Cholesterol Education Program criteria.
Characteristics of the included studies.

Intervention group characteristics
One study used Hatha Yoga, 32 one used restorative yoga 30 and the remaining studies did not report the yoga style used. Two studies did not further outline the content of the yoga intervention29,31 and the remaining studies all used yoga postures. In four studies, pranayama and meditation or relaxation were additionally used,27,32–34 and one study additionally used lifestyle advice. 33 The duration of yoga programmes ranged from 8 weeks to 1 year with a median of 30 weeks; frequency of yoga interventions ranged from one weekly to two daily (median: 3 weekly) yoga sessions of 45–90 (median: 60) minutes in length.
Control group characteristics
Five RCTs compared yoga to usual care or no specific treatment.27,31–34 One RCT used stretching exercises; the yoga and exercise interventions were exactly matched for programme length, frequency and duration of the sessions. 30 One trial compared yoga to herbal medicine. 29 The latter two RCTs could not be included in the meta-analyses.
Outcome measures
Only one RCT assessed the resolution of metabolic syndrome as the number of patients who no longer met the diagnosis of metabolic syndrome after the study intervention. 34 All seven studies assessed waist circumference, triglycerides, HDL cholesterol and systolic and diastolic blood pressure. All but one study 29 also assessed fasting plasma glucose. Regarding safety, only one study explicitly assessed adverse events;27 one study assessed clinically significant adverse events;29 and one study assessed drop outs due to side effects. 32
Risk of bias in individual studies
Risk of bias assessment.
Analysis of overall effect
Primary outcomes
In the single study assessing the resolution of metabolic syndrome, 37 out of 84 patients in the yoga group and 34 out of 94 patients in the untreated control group no longer met the diagnostic criteria for metabolic syndrome (OR = 1.48; 95% CI = 0.81–2.70; p = 0.20).
34
Meta-analyses revealed evidence of the short-term effects of yoga compared to usual care on waist circumference (SMD = −0.35; 95% CI = −0.57 to −0.13; p < 0.01) and systolic blood pressure (SMD = −0.29; 95% CI = −0.51 to −0.07; p = 0.01), but not for diastolic blood pressure (SMD = −0.20; 95% CI = −0.42 to 0.02; p = 0.07), triglycerides (SMD = −0.02; 95% CI = −0.24 to 0.20; p = 0.89), HDL cholesterol (SMD = 0.17; 95% CI = −0.36 to 0.70; p = 0.53) or fasting plasma glucose (SMD = 0.03; 95% CI = −0.19 to 0.25; p = 0.80) (see Figure 2). One RCT compared yoga to exercise and found group differences favouring yoga for fasting plasma glucose only.
30
Another compared yoga to a herbal medicine compound, but did not include statistical tests for group differences.
29
Forest plots of overall effect sizes for all outcomes.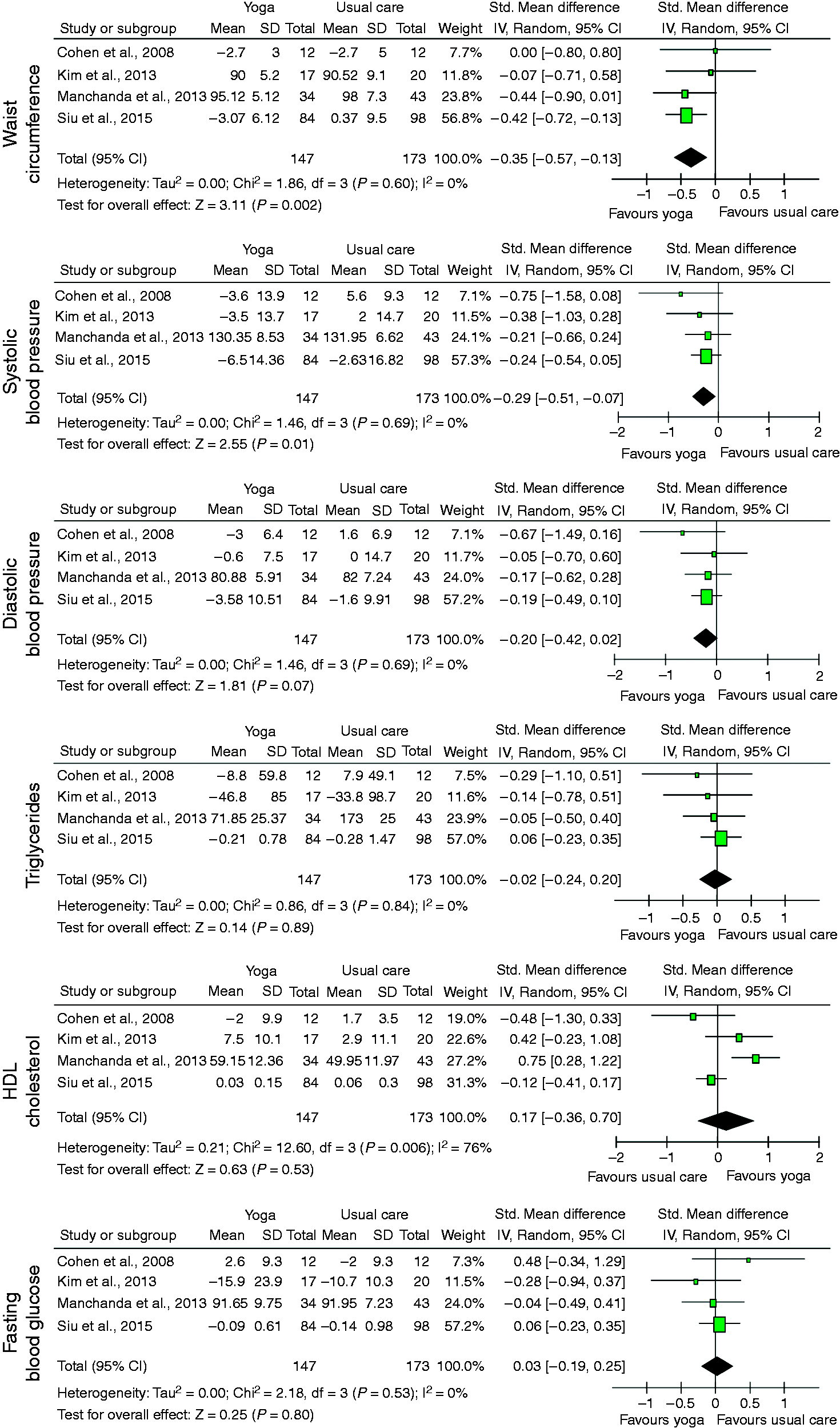
Safety
Three RCTs reported safety-related data. One of those reported adverse events and reported that there were no adverse events. 27 Another study reported on clinically significant adverse events and reported that no such events occurred during the research period. 29 One further RCT reported reasons for drop outs and reported that no trial patient dropped out due to intervention side effects. 32
Sensitivity analyses
A low risk of selection bias 32 and a low risk of detection bias each only appeared in one study. 32 No effects remained significant if only this study was included in the analysis. In studies with a low risk of attrition bias,27,30,32 the effect of yoga compared to usual care on systolic blood pressure did not change substantially (SMD = −0.52; 95% CI = –1.03 to −0.01; p = 0.05). No other effects remained significant.
Discussion
Summary of evidence
In this systematic review of seven randomised trials on yoga in patients with metabolic syndrome, evidence for the beneficial effects of yoga on waist circumference and systolic blood pressure was found. No effect was robust agianst selection and detection bias, and only the effect on systolic blood pressure was robust against attrition bias. Yoga appeared to be safe; however, the reporting of safety was insufficient.
To the best of our knowledge, no systematic review and/or meta-analysis on yoga for patients with metabolic syndrome has been conducted so far. However, several reviews exist with thematic overlap. Chu et al. 36 conducted a review of the effects of yoga on modifying risk factors in cardiovascular disease and metabolic syndrome. They included 32 RCTs in meta-analyses and found significant improvements for weight, systolic and diastolic blood pressure, HDL and low-density lipoprotein cholesterol and triglycerides, but not for fasting blood glucose. Contrary to our present review, these authors included healthy participants with increased risk factors and patients with chronic diseases (i.e. coronary artery disease, diabetes or metabolic syndrome), which results in different outcomes. Anderson and Taylor, 37 on the other hand, included different mind/body therapies, and they did not conduct a meta-analysis. Their conclusion that mind/body practices may be potentially effective for components of metabolic syndrome is therefore based on qualitative analysis of the trials.
Innes and colleagues 12 conducted a review of the protective effects of yoga on risk indices associated with insulin resistance and cardiovascular disease. They identified 70 uncontrolled trials, controlled trials and RCTs and reported beneficial effects on risk factors, such as glucose tolerance and insulin sensitivity, lipid profiles and blood pressure. Cramer et al. 11 investigated the effects of yoga on cardiovascular risk factors in the general population and high-risk disease groups. They also found beneficial effects on waist circumference, systolic and diastolic blood pressure, cholesterol and triglycerides, HbA1c and insulin resistance. However, both of these reviews were more comprehensive than the current meta-analysis and included healthy participants and other risk factor patients without metabolic syndrome, but no subgroup analysis on patients with metabolic syndrome was conducted. Therefore, the effects on those parameters may have been present primarily in other patient samples and cannot be directly applied to patients with metabolic syndrome. Furthermore, several of the trials in metabolic syndrome have been published only recently. This meta-analysis adds value to the current literature as the first meta-analysis in this subgroup to provide syndrome-specific results for yoga.
Strengths and weaknesses
To the best of our knowledge, this is the first systematic review and meta-analysis that is available on yoga for metabolic syndrome. The strengths of this review include its adherence with PRISMA guidelines, the comprehensive literature search and the inclusion of yoga trials in a predefined patient sample. The primary limitation of this review is the paucity of eligible trials and the small overall sample size within the meta-analysis. Another major limitation is the insufficient reporting and/or low methodological quality of the studies included, limiting the interpretability of the results. Finally, no unpublished studies or studies published in ‘grey literature’ were included. The usefulness of including unpublished trials is still under debate. 14 Being meant to address publication bias, few unpublished trials can normally be located for systematic reviews and the located studies may be an unrepresentative sample of all unpublished studies.14,38 Investigators are often unwilling to provide unfavourable results, while they are more willing to provide favourable results; thus, publication bias may still remain an issue. 14 Moreover, unpublished studies tend to be of lower methodological quality than published studies 39 and normally lack peer review. 14 It might be regarded as a further limitation that EMBASE was not searched and that no librarian was involved in the literature search, although there is no consensus on these issues.
Implications for further research
Firstly, more trials focusing on yoga and metabolic syndrome are warranted in order to conclusively judge its potential in that collective. Specifically, more studies assessing the resolution of metabolic syndrome through yoga are needed. Secondly, given that one of the main drawbacks of this review was the insufficient reporting of trial methodology, authors of prospective research studies should further improve the reporting of yoga trials and adhere to standard reporting guidelines (e.g. Consolidated Standards of Reporting Trials (CONSORT)). 40 Further trials should ensure rigorous methodology is followed, including a priori sample size calculations in order to prevent negative results due to a lack of power. They should further ensure adequate randomisation, allocation concealment, intention-to-treat analysis and blinding of at least outcome assessors. 40
Yoga trials should improve their reporting of safety. Even though no evidence for serious yoga-associated adverse events or an accumulation of adverse events have been found in RCTs reporting on safety, 35 two-thirds of trials had not bothered to report or discuss safety. Yoga has occasionally been associated with serious adverse events. 41 Patients who are overweight and who have hypertension and/or prediabetes may especially require modifications of yoga practice. This should be an additional focus of further trials.
A recent meta-analysis of yoga for hypertension found that yoga might effectively reduce both systolic and diastolic blood pressure, but only if meditation and/or breathing techniques are the main component of the intervention. 42 Given that this current meta-analysis found no effects of yoga on diastolic blood pressure, it might be worthwhile to compare the antihypertensive effects of the different yoga components (i.e. posture, breathing and meditation) in patients with metabolic syndrome. In addition, more research is needed that compares yoga to other active interventions, such as conventional exercise.
Implications for clinical practice
The findings of this meta-analysis can be applied to patients with metabolic syndrome only. Based on the results of this meta-analysis, no recommendation can be made for or against yoga influencing the parameters of metabolic syndrome in patients with metabolic syndrome. Despite the methodological drawbacks of the included trials, yoga can be preliminarily considered to be a safe and effective intervention in order to reduce waist circumference and systolic blood pressure. Yoga might be considered as an alternative approach for patients who are not adhering to conventional forms of exercise.
Footnotes
Author contribution
HC and RL contributed to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; and drafted the manuscript. JL and GD critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was supported by a grant from the Rut- and Klaus-Bahlsen-Foundation. The funding source had no influence on the design or conduct of the review; the collection, management, analysis or interpretation of the data; or in the preparation, review or approval of the manuscript.